Embed Size (px)
Citation preview

Accepted Manuscript
Retro-Esophageal Brachiocephalic Artery Assessed by MRI: A Case Report andLiterature Review
Sharmila Udupa, MD, CM John F. Smythe, MD, FRCPC Derek T. Wong, MD. FRCPC
PII: S0828-282X(14)01400-7
DOI: 10.1016/j.cjca.2014.09.016
Reference: CJCA 1406
To appear in: Canadian Journal of Cardiology
Received Date: 4 August 2014
Revised Date: 4 September 2014
Accepted Date: 5 September 2014
Please cite this article as: Udupa S, Smythe JF, Wong DT, Retro-Esophageal Brachiocephalic ArteryAssessed by MRI: A Case Report and Literature Review, Canadian Journal of Cardiology (2014), doi:10.1016/j.cjca.2014.09.016.
This is a PDF file of an unedited manuscript that has been accepted for publication. As a service toour customers we are providing this early version of the manuscript. The manuscript will undergocopyediting, typesetting, and review of the resulting proof before it is published in its final form. Pleasenote that during the production process errors may be discovered which could affect the content, and alllegal disclaimers that apply to the journal pertain.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 1
Retro-Esophageal Brachiocephalic Artery Assessed by MRI: A Case Report and Literature Review
Short Title: Retro-Esophageal Brachiocephalic Artery – Literature Review
Sharmila Udupa MD,CM1, John F Smythe MD, FRCPC2, Derek T Wong MD. FRCPC1
1Division of Cardiology, Department of Pediatrics, University of Ottawa, Children’s Hospital of Eastern Ontario, Ottawa, Canada. 2Divison of Cardiology, Department of Pediatrics, Queen’s University, Kingston General Hospital, Kingston, Canada. Word Count: 1686 Corresponding Author: Sharmila Udupa, MD,CM Division of Cardiology, Department of Pediatrics Children’s Hospital of Eastern Ontario 401 Smyth Road Ottawa, Ontario Canada K1H 8L1 E-mail: [email protected] Telephone: (613) 737-7600 ext 2390 Fax: (613) 738-4835

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 2
Brief Summary
A right aortic arch with a retro-esophageal brachiocephalic artery is a very rare type of
vascular ring. We present a case of one such vascular anomaly diagnosed by cardiac
magnetic resonance imaging (MRI), with a review of all cases to date. Cardiac MRI can
be used as a primary diagnostic modality for anatomic assessment of the vascular ring,
as well as the hemodynamics of associated cardiac malformations in the pre-operative
setting.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 3
Abstract
A right aortic arch with a retro-esophageal brachiocephalic artery is a very rare type of
vascular ring. A case report with a review of published cases to date are presented.
Twelve publications from 1968 to 2014 describe a retro-esophageal brachiocephalic
artery in a total of thirteen patients. The mean age at diagnosis was 8.7 ± 16 years.
Four of the thirteen patients were male. Nearly half of the patients were symptomatic,
with dysphagia or respiratory difficulties. Ten patients (77%) had associated congenital
heart defects. Of the thirteen patients with a retro-esophageal brachiocephalic artery,
twelve had a right aortic arch, and only one patient had a left aortic arch associated with
complex congenital heart disease.
Investigations used in the diagnosis of the vascular ring include angiography,
esophagram, echocardiogram, and computed tomography. Only two cases confirmed
the diagnosis with magnetic resonance imaging but this was in the setting of complex
congenital heart disease.
In conclusion, a right aortic arch with a retro-esophageal left brachiocephalic artery is an
extremely rare form of vascular ring, often seen in association with other forms of
congenital heart disease. Cardiac MRI can be used as a primary diagnostic modality for
both the assessment of the vascular ring anatomy and the hemodynamics of associated
cardiac malformations in the pre-operative setting.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 4
Introduction
In general, vascular rings are a rare cardiac anomaly, however a right aortic arch with a
left retro-esophageal brachiocephalic artery is one of the rarest subtypes. Only a few
cases have been described in the literature, with minimal documentation of their age,
mode of presentation and association with other forms of congenital heart disease. We
present a case of one such vascular anomaly diagnosed by cardiac magnetic
resonance imaging, with a review of all cases to date.
Case
A six-month old boy was referred to our center with a diagnosis of a perimembranous
ventricular septal defect (VSD) and unclear aortic arch anatomy. He had initially been
assessed for a murmur in a peripheral center while hospitalized for a respiratory tract
illness.
Upon presentation to our center, there was no history of chronic respiratory or
gastrointestinal difficulties such as stridor, dysphagia or gastroesophageal reflux.
Physical examination revealed a normal blood pressure in all four limbs with no
evidence of an arm-leg gradient. Auscultation demonstrated a grade 3/6 pansystolic
murmur. Electrocardiogram revealed sinus rhythm and biventricular hypertrophy.
Echocardiography confirmed a moderate perimembranous VSD with evidence of left-

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 5
sided volume loading. There was evidence of right coronary cusp prolapse into the
VSD, without aortic insufficiency. Echocardiography at our institution failed to clearly
delineate the aortic arch anatomy, prompting further evaluation with cardiac magnetic
resonance imaging (MRI).
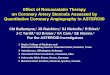
An outpatient cardiac MRI under general anesthetic revealed a right aortic arch with an
aberrant left retro-esophageal brachiocephalic artery (Figure 1). The first branch arising
from the right aortic arch was the right internal carotid artery, followed by the right
subclavian artery. The last branch off the descending aorta was the left brachiocephalic
artery which gave rise to the left internal carotid and subclavian arteries and had a retro-
esophageal course. In addition, the proximal base of the brachiocephalic artery
appeared prominent, reminiscent of a diverticulum of Kommerrell. This finding
supported the notion that the arterial duct originated from the brachiocephalic artery and
coursed towards the pulmonary trunk, thereby completing the vascular ring. There was
no evidence of tracheal compression. MRI also confirmed the hemodynamic
significance of the VSD, with a Qp:Qs ratio of 2.9:1 by phase contrast imaging.
Surgery was performed electively, and the aortic arch anatomy was confirmed at the
time of surgery – a right aortic arch with a retro-esophageal left brachiocephalic artery
and a left-sided arterial ligament connecting the left subclavian artery to the left
pulmonary artery, effectively completing the vascular ring. The VSD was closed and the
arterial ligament was divided without complications.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 6
Literature Survey
There have been a total of twelve publications from 1968 to 2014 describing a retro-
esophageal brachiocephalic artery in a total of thirteen patients (Table 1). The mean
age of diagnosis was 8.7 ± 16 years (median 1 year, range 0.002 – 61 years). Four of
the thirteen (30%) cases were male.
Nearly half of patients (46%) were symptomatic, with dysphagia or respiratory difficulties
attributable to the vascular ring. Symptomatic individuals had an average age of
presentation of 15.8 ± 20.7 years (median 9 years, range 0.1 – 61 years). Some of
these patients had associated congenital heart disease, however, it was felt that their
primary symptoms at presentation were due to the vascular ring.
Ten of the thirteen patients (77%) had associated congenital heart defects ranging from
isolated VSD in two (15%), common arterial trunk in two (15%), Tetralogy of Fallot in
one (7.5%), aortopulmonary window in one (7.5%), valvular aortic stenosis in one
(7.5%) and hypoplastic left heart complex in one (7.5%). The average age of
presentation for those with associated congenital heart disease was 3.5 ± 6.2 years
(median 0.375 years, range 0.002 – 19 years).
Of the thirteen patients with a retro-esophageal brachiocephalic artery, twelve had a
right aortic arch, and only one patient had a left aortic arch in the setting of complex

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 7
congenital heart disease. The strong association of right aortic arch and a retro-
esophageal brachiocephalic artery gives credence to the belief that its pathogenesis
may be related to abnormalities in outflow tract formation. In addition, the incidence of
associated congenital conotruncal lesions (30% of patients with Tetralogy of Fallot,
common arterial trunk, or aortopulmonary window) with a retro-esophageal
brachiocephalic artery in our review helps to further support this hypothesis. Only four
of thirteen cases in the literature were isolated vascular rings, highlighting the
importance of a thorough cardiac assessment to rule out other congenital heart defects
when presented with such a lesion.
Surgical intervention, consisting of ductal division, was linked to cases in which
symptoms were present or where complex cardiac disease co-existed. Only three out of
thirteen cases document no surgical intervention, likely due to the lack of associated
symptoms.
Discussion
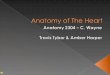
The development of various forms of vascular rings can be best understood through the
hypothetical pluripotent double aortic arch model proposed by Jesse Edwards in 1948
(Figure 2) (1). This hypothetical model consists of a double aortic arch with an arterial
duct on either side and the various head and neck vessels arising from their respective
arches. Embryologically, this model is based on the paired arteries seen within the five
pharyngeal arches that originate from the aortic sac and travel posteriorly to join with

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 8
the dorsal aorta (2). The various configurations of aortic arch anatomy can be explained
through persistence or regression of the various portions of this primitive aortic arch
substrate. The reader is directed to excellent reviews of cardiac embryology for further
detailed explanations. (2-5).
The formation of a right aortic arch with an aberrant left retro-esophageal
brachiocephalic artery is postulated to occur due to an interruption in the anterior portion
of the left branch of the aortic sac, proximal to the origin of the left common carotid
artery (1). The right aortic arch is formed by persistence of the right branch of the aortic
sac, the right aortic arch, and the right dorsal aorta. The left dorsal aorta persists and
connects to the distal portion of the left aortic arch, forming the retro-esophageal
brachiocephalic artery. Completion of the vascular ring occurs when a left sided arterial
duct or arterial ligament connects the aberrant left retro-esophageal brachiocephalic
artery to a pulmonary artery. This type of vascular ring is a rare entity, with very few
other cases described in the literature. A recent review of vascular rings at a single
institution listed an incidence of 3% of patients with this specific type of vascular ring (6).
Past reports have documented the use of angiography to diagnose a right aortic arch
with aberrant left retro-esophageal brachiocephalic artery. Other diagnostic
investigations include esophagram, echocardiogram, and until recently, computed
tomography. Only two cases confirmed the diagnosis with MRI but this was in the
setting of complex congenital heart disease. Following the use of MRI in confirming their

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 9
diagnosis, Moes et al concluded that MRI was their preferred tool for assessing vascular
rings (7).
Cardiac MRI has recently been described as the new gold standard for evaluation of
vascular rings (6), with significant benefit of vascular and extra-cardiac anatomical
delineation. Cardiac MRI allows for detailed anatomic imaging of the aortic arch with
high spatial resolution. In addition, it allows for multi-planar reconstruction and creation
of a 3-dimensional picture (Video 1) permitting clear visualization of the impact of the
vascular ring on adjacent structures. Furthermore, cardiac MRI does not use ionizing
radiation (unlike cardiac catheterization or CT) and is not limited by acoustic windows.
In our case, echocardiography was unable to resolve the aortic arch anatomy. All other
case reports have only utilized cardiac MRI for a purely anatomic diagnosis, thereby not
fully benefitting from its potential. Given that this anomaly is often associated with other
forms of congenital heart disease, MRI can also provide hemodynamic data and precise
anatomical assessment of associated lesions, imperative in surgical management of
these patients. In our case, cardiac MRI determined pulmonary-to-systemic blood flow
ratio, illustrating the hemodynamic significance of the VSD and necessity for its closure.
Conclusion
A retro-esophageal left brachiocephalic artery with right aortic arch is an extremely rare
form of vascular ring, with very few cases reported in the literature. This variant of a

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 10
vascular ring is often seen in association with other forms of congenital heart disease,
specifically those related to abnormalities of the outflow tracts. Our case illustrates how
cardiac MRI can be used as a primary diagnostic modality for both the assessment of
vascular ring anatomy and the hemodynamics of associated cardiac malformations in
the pre-operative setting.
Acknowledgements
None.
Funding Sources
None.
Disclosures
None.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 11
Reference List
(1) EDWARDS JE. Anomalies of the derivatives of the aortic arch system. Med Clin North Am
1948 July;32:925-49.
(2) Anderson RH, Webb S, Brown NA, Lamers W, Moorman A. Development of the heart: (3) formation of the ventricular outflow tracts, arterial valves, and intrapericardial arterial trunks. Heart 2003 September;89(9):1110-8.
(3) Anderson RH, Brown NA, Mohun TJ, Moorman AF. Insights from cardiac development relevant to congenital defects and adult clinical anatomy. J Cardiovasc Transl Res 2013 April;6(2):107-17.
(4) Anderson RH, Webb S, Brown NA, Lamers W, Moorman A. Development of the heart: (2) Septation of the atriums and ventricles. Heart 2003 August;89(8):949-58.
(5) Moorman A, Webb S, Brown NA, Lamers W, Anderson RH. Development of the heart: (1) formation of the cardiac chambers and arterial trunks. Heart 2003 July;89(7):806-14.
(6) Humphrey C, Duncan K, Fletcher S. Decade of experience with vascular rings at a single institution. Pediatrics 2006 May;117(5):e903-e908.
(7) Moes CA, Mawson JB, MacDonald C, Smallhorn J. Right aortic arch with retroesophageal left aberrant innominate artery. Pediatr Cardiol 1996 November;17(6):402-6.
(8) Grollman JH, Jr., Bedynek JL, Henderson HS, Hall RJ. Right aortic arch with an aberrant retroesophageal innominate artery: angiographic diagnosis. Radiology 1968 April;90(4):782-3.
(9) Garti IJ, Aygen MM. Right aortic arch with aberrant left innominate artery. Pediatr Radiol 1979 February 26;8(1):48-50.
(10) Rajaram PC, Hussain AT, Lakshmikanthan C, Vaidyanathan D, Subramanian N, Vasudevan S. Type D double aortic arch. Double aortic arch with interruption of its left component proximal to the site of origin of left common carotid artery. Angiology 1983 September;34(9):597-603.
(11) Schlesinger AE, Leiter BE, Connors SK. Computed tomography diagnosis of right aortic arch with an aberrant left innominate artery. J Comput Tomogr 1984 January;8(1):81-7.
(12) Maurus KE, Firmin RK, Leanage R. A rare anomaly of the aortic arch complex. Int J Cardiol 1988 July;20(1):149-51.
(13) Nakajima Y, Satomi G, Kawamura T, Nishibatake M, Nakazawa M, Takao A. Right aortic arch with aberrant retroesophageal innominate artery: a report of 2 cases and review of the literature. Int J Cardiol 1993 March;38(3):247-51.
(14) Ishizaka T, Allen SW, Strouse PJ, Ohye RG. Postductal origin of the left carotid, left subclavian, and aberrant retroesophageal right innominate arteries in truncus arteriosus with interrupted aortic arch. Pediatr Cardiol 2003 November;24(6):581-4.
(15) Sett SS, Mawson JB, Sandor GG. Repair in infancy of right aortic arch with aberrant left brachiocephalic artery in the setting of a variant of the hypoplastic left heart syndrome. Cardiol Young 2004 August;14(4):441-3.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 12
(16) Rios-Mendez RE, rauz-Martinez ME. [Chronic wheezing child and type "D" double aortic arch: case report]. Arch Argent Pediatr 2008 December;106(6):548-51.
(17) Fellmer PT, Bohner H, Wolf A, Roher HD, Goretzki PE. A left nonrecurrent inferior laryngeal nerve in a patient with right-sided aorta, truncus arteriosus communis, and an aberrant left innominate artery. Thyroid 2008 June;18(6):647-9.
(18) Kondrachuk O, Yalynska T, Yemets I. Right aortic arch with retroesophageal brachiocephalic artery. Cardiol Young 2009 June;19(3):292-3.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT
Udupa 13 Table 1: Summary of literature involving patients with a retro-esophageal brachiocephalic artery
Authors Year n Age Symptoms Modality for Diagnosis
Aortic Arch Sidedness Associated CHD Intervention
Grollman et al.(8;8)
1968 1 19 yrs Dyspnea on exertion
Esophagram and Arteriogram
Right Valvular aortic stenosis None
Garti et al.(9) 1979 1 9 yrs Dysphagia and recurrent URTI
Esophagram and Arteriogram
Right None Arterial Ligament Division
Rajaram et al. (10)
1983 1 5 yrs Recurrent URTI Angiogram Right PDA and bilateral pulmonary artery stenosis
PDA ligation
Schlesinger et al (11)
1984 1 61 yrs None - incidental on CXR
CT Right None None
Maurus et al (12)
1988 1 6 mos Heart failure Angiogram Right VSD and PDA PDA Ligation, and VSD closure
Nakajima et al (13)
1993 2 1 yr None - incidental on CXR
Angiogram Right Tetralogy of Fallot Tetralogy of Fallot repair
9 yr None - incidental on investigation for murmur
Angiogram and MRI
Right VSD None
Moes et al (7)
1996 1 5 wks Stridor and URTI
Angiogram Right ASD, PSD, aortopulmonary window and PDA
Complete repair
Ishizaka et al. (14)
2003 1 1 day Cyanosis Echocardiogram and MRI
Left Common Arterial Trunk (type II), single coronary artery, aortic arch interruption
Complete repair
Sett et al. (15) 2004 1 5 wks Cyanosis and failure to thrive
CT Right Severe mitral stenosis, large VSD, bicuspid aortic valve, arch hypoplasia, left superior vena cava
Norwood procedure
Rios-Mendez et al. (16)
2008 1 8 yrs Dyspnea and dysphagia
Esophagram and Arteriogram
Right None PDA ligation
Fellmer et al. (17)
2008 1 1 day Cyanosis Angiogram Right Common Arterial Trunk (Type I) Complete repair
Kondrachuk et al. (18)
2009 1 3 mo Dysphagia and dyspnea
CT Right PDA PDA ligation
Legend: CT: computer assisted tomography, CXR: chest radiograph, MRI: magnetic resonance imaging, VSD: ventricular septal defect, PDA: patent arterial duct, ASD: atrial septal defect, URTI: upper respiratory tract infection

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 14
Figure 1 Legend 3D volume rendered magnetic resonance angiogram of a right aortic arch with an aberrant left retro-
esophageal brachiocephalic artery. Note the prominent base of the brachiocephalic artery,
reminiscent of a diverticulum of Kommerrell, indicating that the arterial duct originated from the
brachiocephalic artery to connect to the pulmonary trunk, thereby completing the vascular ring. The
dotted line represents the location of the arterial ligament.
AAO: Ascending aorta; REBA: retro-esophageal brachiocephalic artery; PT: pulmonary trunk; DOA:
descending aorta.
Figure 2 Legend A. The hypothetical model for the double aortic arch proposed by JE Edwards. LAA: left aortic arch;
LCCA: left common carotid artery; LPA: left pulmonary artery; LSA: left subclavian artery; PT:
pulmonary trunk; RAA: right aortic arch; RCCA: right common carotid; RPA: right pulmonary artery;
RSA: right subclavian artery.
B. Formation of a right aortic arch with an aberrant left retro-esophageal brachiocephalic artery is
postulated to occur due to an interruption in the anterior portion of the left branch of the aortic sac,
proximal to the origin of the left common carotid artery. The right aortic arch is formed by persistence
of the right branch of the aortic sac, the right aortic arch, and the right dorsal aorta. The left dorsal
aorta persists and connects to the distal portion of the left aortic arch, forming the brachiocephalic
artery. Completion of the vascular ring occurs when a left sided arterial duct or arterial ligament
connects the aberrant left retro-esophageal brachiocephalic artery to a pulmonary artery. The red
lines indicate areas of regression.
[Reprinted from Paediatric Cardiology, 3rd Edition, Anderson RH, Baker EJ, Penny DJ, Redington AN,
Rigby ML, Wernovsky G [eds], “Vascular Rings, Pulmonary Arterial Sling, and Related Conditions”,
Yoo S-J and Bradley TJ, pp967-989, with permission from Elsevier; originally modified from Edwards

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPTUdupa 15
JE: Anomalies of the derivatives of the aortic arch system. Med Clin N Am 1948;32:925–948; and
Edwards JE: Vascular rings and slings. in Moller JH, Neal AN [eds]: Fetal, Neonatal, and Infant
Cardiac disease. Norwalk, CT: Appleton & Lange, 1990, pp 745–754.].
Video
Legend
3D volume rendered magnetic resonance angiogram of a right aortic arch with an aberrant left retro-
esophageal brachiocephalic artery. The prominent base of the brachiocephalic artery, reminiscent of
a diverticulum of Kommerrell, indicates that the arterial duct originated from the brachiocephalic artery
to connect to the pulmonary trunk.

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT

MANUSCRIP
T
ACCEPTED
ACCEPTED MANUSCRIPT