Embed Size (px)
Citation preview

British Journal of Ophthalmology, 1984, 68, 475-478
Retinal vascular remodelling in radiation retinopathyKENNETH G. NOBLE AND MARK J. KUPERSMITH
From the Department of Ophthalmology, New York University Medical Center, New York
SUMMARY A 34-year-old female developed bilateral radiation retinopathy three months afterexternal beam radiotherapy for pituitary adenoma. The clinical symptoms, fundus abnormalities,and microvascular pathology noted on fluorescein angiography resolved spontaneously over a fewmonths. The most dramatic aspect was the progressive improvement and partial reperfusion of theretinal capillary bed.
A retinopathy may follow radiation treatment forintraocular malignancies, for lesions adjacent to theeye, or for intracranial lesions. The latency period isvariable but is usually a few months to a few years.The abnormalities are probably a result of damage
to the retinal vessels resulting in obliterative endart-eritis. Clinical manifestations include microaneurysms,telangiectasias, haemorrhages and exudates (super-ficial and deep), vessel wall sheathing, capillary non-perfusion, and neovascularisation. Progression ofthese lesions is not uncommon.We report herein a case of radiation retinopathy
following external beam irradiation for pituitaryadenoma. On follow-up examination there wasdramatic resolution of many of the microvascularabnormalities.
Case report
A 34-year-old white female was diagnosed as havinga pituitary adenoma 11 years previously, at whichtime she underwent an intracranial subtotal removalof the tumor. The preoperative amenorrhoea andbitemporal visual field defect resolved after surgery.
In November 1978 she received external beamradiotherapy (4500 rads) to the remaining tumour forsymptoms of acromegaly (changes in facial contourand increasing hand size). Three months after therapyshe complained of spots in front of both eyes andprogressive visual blurring in the left eye. An increasein growth hormoneand an abnormal glucose tolerancetest prompted the diagnosis of diabetic retinopathyby the consulting ophthalmologist.
At the time of our initial evaluation in August 1979the visual acuity was 6/6- (20/20-) OD and 6/18(20/60) OS. The pupils were 4mm round and reactiveto light with a 2+ afferent pupillary defect OS. Theversions were full. Colour vision testing with theIshihara plates showed multiple errors in each eye,but they were more marked in the left eye. Tangentscreen visual fields showed a temporal defect to a3 mm red OD and a slight superotemporal depressionto a 3 mm white OS.The fundus examination revealed scattered post-
erior polar superficial haemorrhages and exudates,
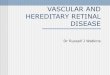
Correspondencc to Dr Kcnneth G. Noble, Department of Fig. I Initialexamination. Both eyesshowedsuperficialOphthalmology, New York University Hospital, 550 First Avenue, haemorrhages and exudates in the posteriorpole with aNew York, NY 10016, USA macularstarfigure in the left eye.
475
on January 18, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.7.475 on 1 July 1984. Dow
nloaded from

Kenneth G. Noble and Mark J. Kupersmith
Fig. 2A Fluorescein angiography. Large areas ofcapillarynon-filling were seen in the left eye which corresponded to theareas ofsuperficial haemorrhage and exudate.
which were more extensive in the left eye. There wasa macular star exudate in the left eye (Fig. 1). Thefluorescein angiogram showed extensive abnormali-ties in the retinal circulation, including large areasof capillary non-filling, focal microaneurysms, anddilated anastomotic channels. In the late-phase
Fig. 3A Seven-monthfollow-up examination. There isreperfusion ofthe retinal capillary bed with afew dilatedcapillaries evident in the macula.
Fig. 2B The latephaseshows intraretinal oedema and vesselwall staining.
angiogram there was evidence of posterior polarintraretinal oedema and staining of the vessel walls(Fig. 2).
After this examination she underwent a trans-phenoidal hypophysectomy with decompression ofthe chiasm. While the bitemporal field defects
Fig 3B The retinal oedema and vessel wallstaining is lessapparent.
476
on January 18, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.7.475 on 1 July 1984. Dow
nloaded from

Retinal vascular remodelling in radiation retinopathy
Fig. 4A One-yearfollow-up examination. Onfundusexamination there is little evidence oftheprevious injury saveforafew dilated tortuous retinal vessels.
improved the visual acuity remained unchanged.The fundus picture and fluorescein angiogram wereslightly worse in the left eye two months later. Inview of the extensive areas of retinal capillary diseasethroughout the posterior pole of the left eye it wasdecided that treatment with photocoagulation wouldnot prove beneficial for improving central vision.
In March 1980 the vision was 6/6- (20/20-) ODand 6/9 (20/30) OS. There were only a few superficialhaemorrhages and exudates in each eye, and themacular exudate had partially resolved. The angio-gram showed reperfusion ofmuch of the retinal capil-lary system (Fig. 3A). The retinal oedema was stillpresent but had considerably lessened, and there wasonly minimal vessel wall staining (Fig. 3B). One yearlater the vision was unchanged but the haemorrhagesand exudates had disappeared. There were a fewdilated tortuous vessels and focal microaneurysms ofthe left eye (Fig. 4).
Discussion
The retinopathy following radiation treatment to theeye and orbit has been well documented in a numberof reports. 1-7 The exact pathogenesis is uncertain. Itis known that irradiation of other organs can result ina vasculopathy consisting of thickened vessel walls,an endarteritis, and capillary atrophy. This is adelayed effect of radiation and may progress withtime.8 Histopathology of globes has revealedthickened hyalinised vessel walls.9-"
Clinically the retinopathy resembles the vascular
Fig. 4B Theangiogramshows capillary reperfusionwithout evidence ofretinal oedema.
changes seen in a variety of vaso-occlusive diseasessuch as diabetes, retinal vein obstruction, sickle cellretinopathy, or systemic hypertension, to name someof the more common aetiologies. Interestingly,retinal vascular disease-for example, diabetesmellitus-may potentiate the effect of radiation-induced retinitis. Chemotherapy also seems to havean additive effect. "The amount of capillary non-perfusion is con-
sidered to be a prognostic sign. When it occurs in themacula and affects the perifoveal capillary net, theprognosis for good central vision is grave. This is aresult of either retinal atrophy or persistent macularoedema. Capillary non-perfusion is a finding prior tothe appearance of intraretinal neovascularisation.Neovascularisation occurs at the interface of per-fused and non-perfused retina, growing into the non-perfused retina. A final complicating factor with pro-fuse areas of capillary non-perfusion is rubeosis iridisand haemorrhagic glaucoma.The treatment for diseases with capillary non-
perfusion has been to destroy ischaemic retina in anattempt to prevent new vessel formation or to hastenits regression. Panretinal argon laser photocoagula-tion has resulted in the complete regression of opticnerve and retinal neovascularisation in a case ofradiation retinopathy.'2The patient in this case report presents a number of
interesting findings. The onset of visual symptomsthree months after radiation therapy is an extremelyshort latency period. At this time her initial eyeexamination elsewhere prompted the diagnosis of
477
on January 18, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.7.475 on 1 July 1984. Dow
nloaded from

Kenneth G. Noble and Mark J. Kupersmith
diabetic retinopathy. Not only did the clinicalappearance resemble this common retinopathy, butthe abnormal glucose tolerance test (a result ofan increase in growth hormone) reinforced thisdiagnosis. Elevated blood glucose levels secondary toincrease in growth hormone may result in a minimalretinopathy of a few microaneurysms, but this neverproceeds to the marked retinopathy seen in thispatient. It is interesting to speculate whetherthis pituitary-induced diabetic state potentiated theeffects of radiation, as has been stated to occur indiabetes mellitus. "The most dramatic aspect was the partial reper-
fusion of the retinal capillary bed. The reperfusionwas noted seven months after the initial examinationand continued to improve when assessed one yearlater. The most plausible explanation for thissequence of events is that the radiation-inducedvessel wall oedema resulted in occlusion of thelumen. With resolution of this extra and intracellularswelling the lumen was reopened. Apparently thedegree of retinal hypoxia was insufficient to inducesecondary intraretinal neovascularisation.
Retinal vascular remodelling does occur in thehealing stages of obstructive vasculopathies (veinocclusion, sickle cell retinopathy, Eales' disease,retrolental fibroplasia, periphlebitis of variousaetiologies) and in the course of diabetic retinopathy.The reperfusion of the retinal capillary circulation tothe degree presented in this case is to our knowledgeunique.
Supported in part by grant 02179 from the National Eye Institute,and a grant from the National Retinitis Pigmentosa Foundation.
References
I Stallard HB. Radiant energy as (A) a pathogenic (B) a thera-peutic agent in ophthalmic disorders. Br J Ophthalmol 1933; 70(monog suppl VI): 67-79.
2 Moore RF. Prcsidcntial address. Trans Ophthalmol Soc UK1935; 55: 3-26.
3 Bedford MA, Bedotto C, MacFaul PA. Radiation retinopathyafter the application of a cobalt plaquc: report of three cases. BrJOphthalmol 1970; 54: 505-9.
4 Chee PHY. Radiation rctinopathy. Am J Ophthalmol 1968; 66:860-5.
5 Hayreh SS. Post-radiation retinopathy: a fluorcscencc fundusangiographic study. Br J Ophthalmol 197(0; 54: 705-14.
6 Shukovsky U, Fletcher GH. Rctinal and optic nervc complica-tions in a high dose irradiation technique of ethmoid sinus andnasal cavity. Radiology 1972; 104: 629-34.
7 Bagan SM, Hollenhorst RW. Radiation retinopathy afterirradiation of intracranial lesions. Am J Ophthalmol 1979; 88:694-7.
8 Berdjis CC. Pathology of irradiation. Baltimorc. Williams andWilkins, 1971: 377-407.
9 Howard GM. Ocular cffectswof radiation and photocoagulation.A study of 1(X) globes with retinoblastoma, somc of whichwere treatcd prior to enuclcation. Arch Ophthalnol 1966; 76:7-1).
1i) Egbert PR, Fajardo LF, Donaldson SS, Moazed K. Postcriorocular abnormalities after irradiation for retinoblastoma: ahistopathological study. BrJ Ophthalmol 1980; 64: 660-5.
11 Brown GC, Shields JA, Sanborn G, Augsburger JJ, Savino PJ,Schatz NJ. Radiation retinopathy. Ophthalmology 1982; 89:1494-150)1.
12 Chaudhuri PR, Austin DJ, Rosenthal AR. Treatment ofradiation retinopathy. Br J Ophthalmol 1981; 65: 623-5.
478
on January 18, 2021 by guest. Protected by copyright.
http://bjo.bmj.com
/B
r J Ophthalm
ol: first published as 10.1136/bjo.68.7.475 on 1 July 1984. Dow
nloaded from














![Blood Vessel Segmentation from Retinal Images · 2017-11-28 · Retinal images have been widely used for diagnosing vascular and non-vascular pa-thology in medical society [1]. Retinal](https://img.pdfslide.us/doc/110x75/5f0f643e7e708231d443edfb/blood-vessel-segmentation-from-retinal-images-2017-11-28-retinal-images-have-been.jpg)