Embed Size (px)
Citation preview
Resuming the fight against
relapse of Plasmodium vivax
Professor J. Kevin Baird Head of Unit, Eijkman-Oxford Clinical Research Unit,
Jakarta, Indonesia &
Centre for Tropical Medicine Nuffield Department of Medicine
University of Oxford, United Kingdom
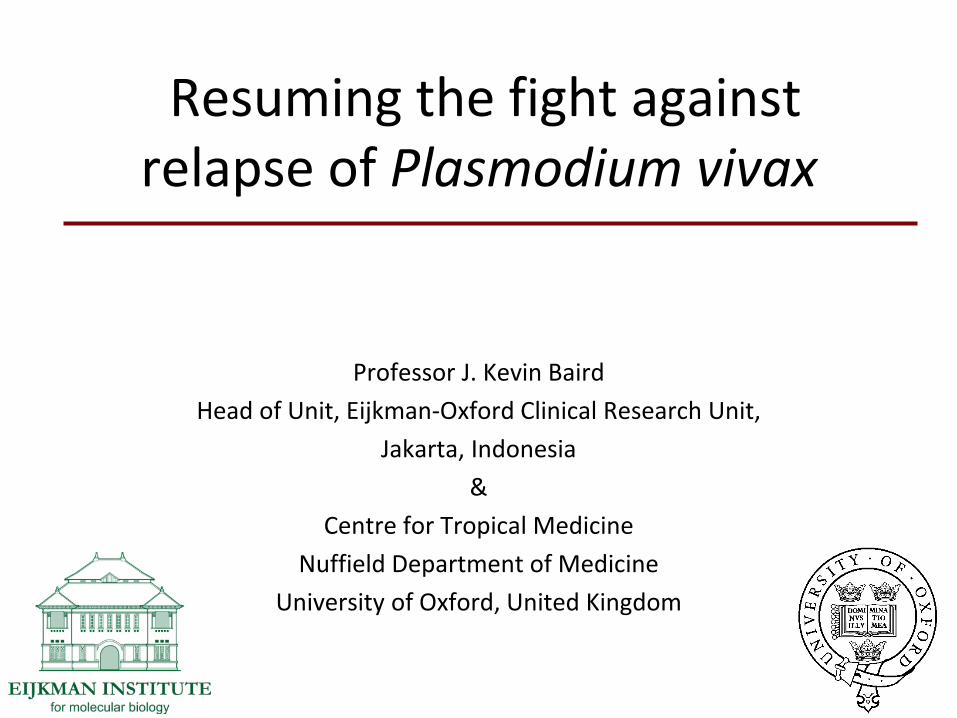
A global problem
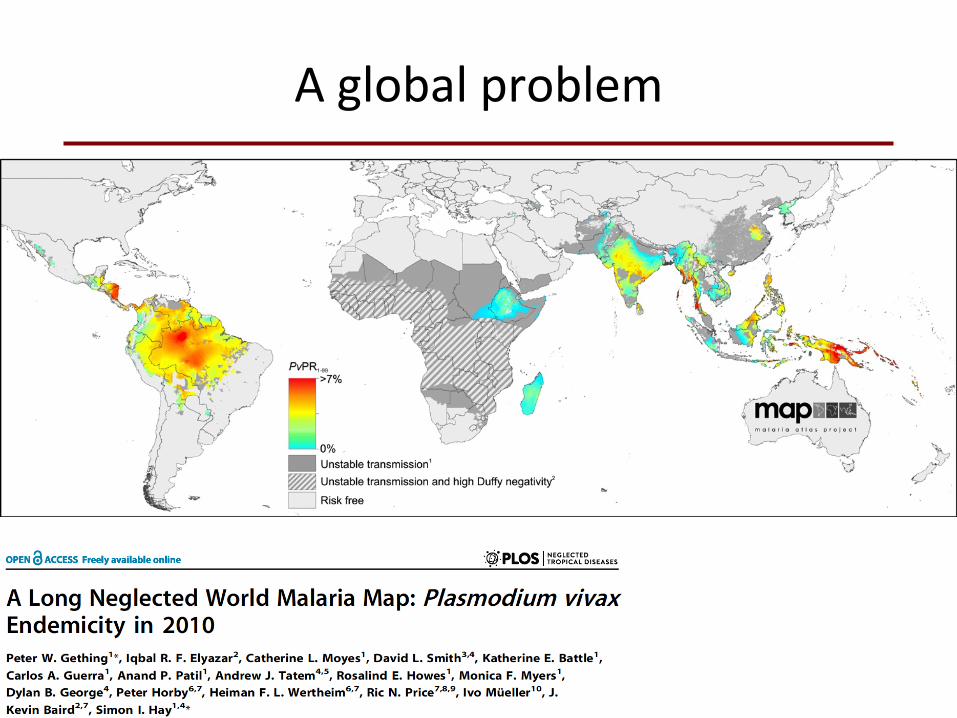
An Asia-Pacific problem
P. falciparum
P. vivax
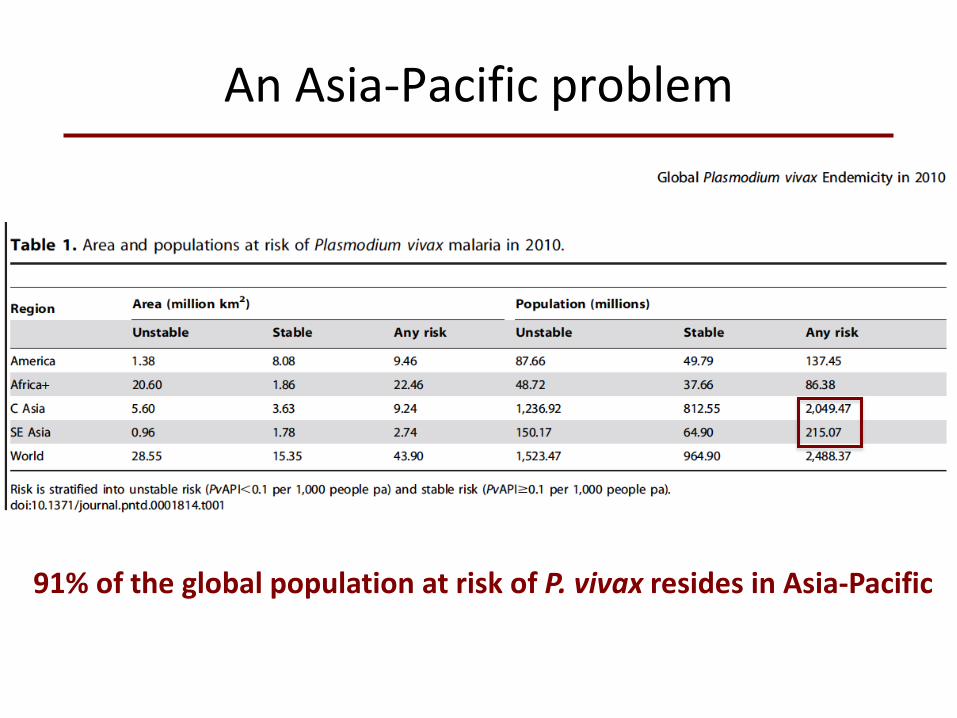
An Asia-Pacific problem
91% of the global population at risk of P. vivax resides in Asia-Pacific
A pernicious problem
Vivax malaria is often pernicious and life-threatening, NOT benign
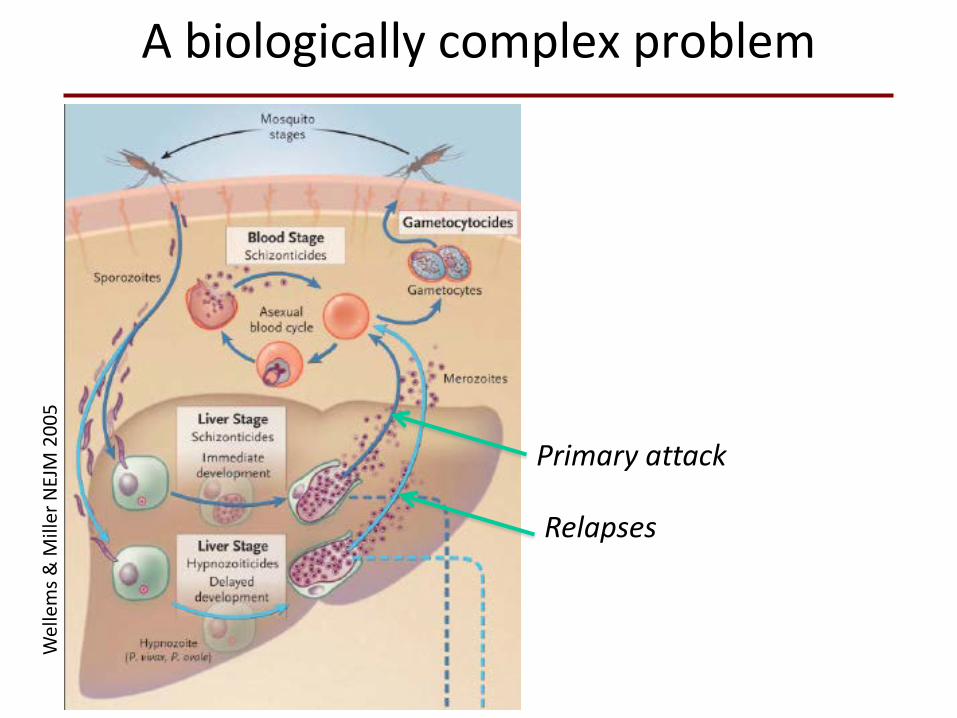
A biologically complex problem W
elle
ms &
Mill
er N
EJM
200
5
Primary attack
Relapses
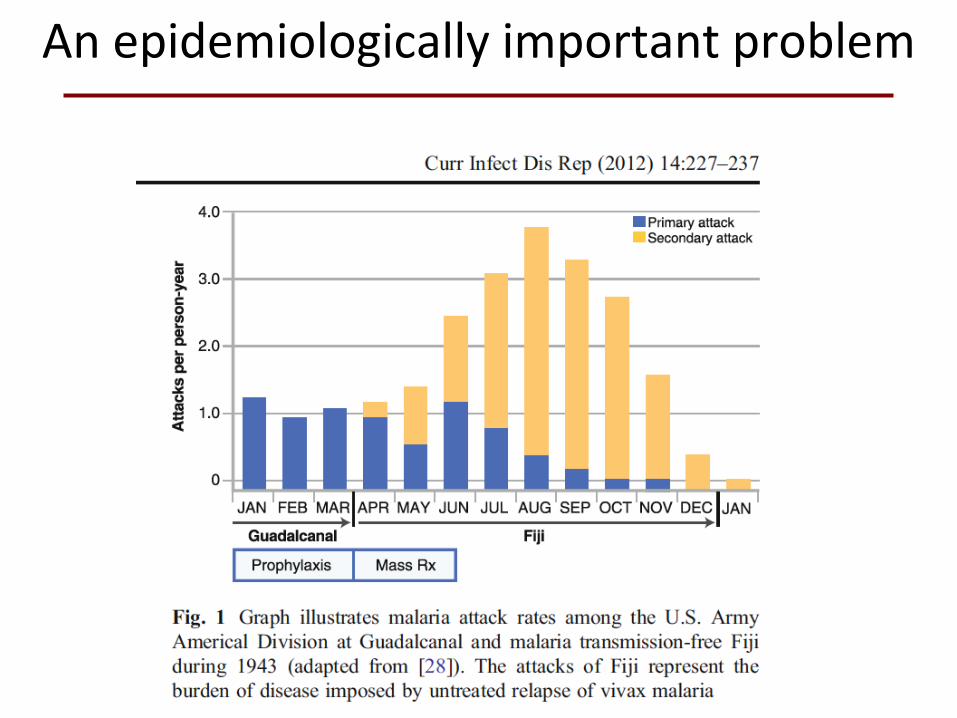
An epidemiologically important problem
The trouble with primaquine
• Licensed in 1952 in combination with chloroquine for radical cure of P. vivax
• Hemolytic toxicity in patients with glucose-6-phosphate dehydrogenase deficiency
• Doses distributed over 14 days to mitigate risk without screening for G6PD deficiency
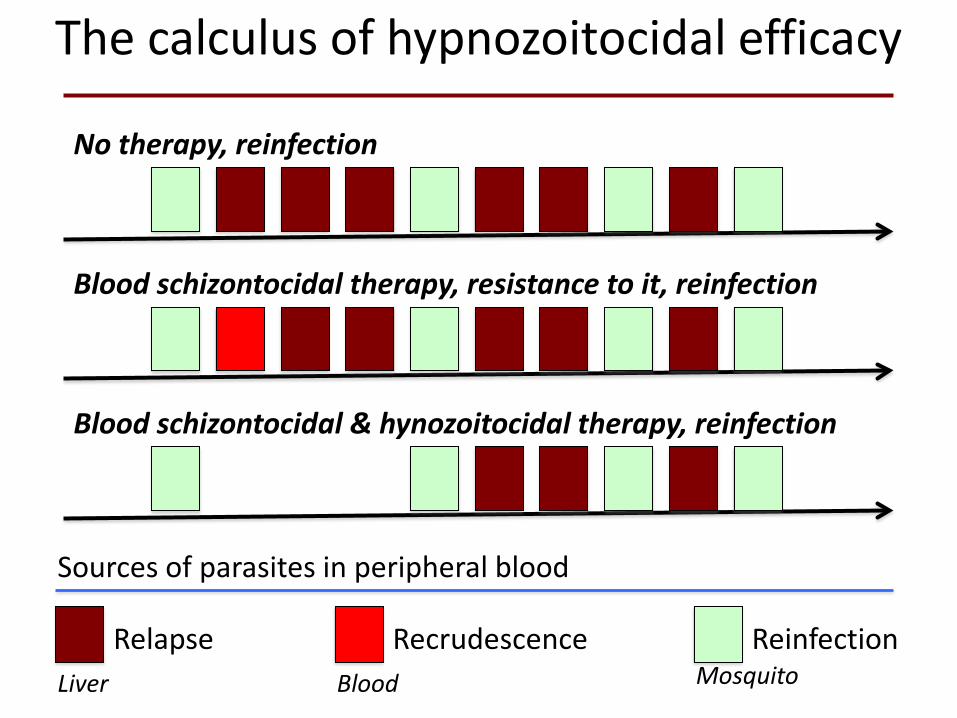
The calculus of hypnozoitocidal efficacy
Relapse Recrudescence Reinfection Liver Blood Mosquito
Sources of parasites in peripheral blood
No therapy, reinfection
Blood schizontocidal therapy, resistance to it, reinfection
Blood schizontocidal & hynozoitocidal therapy, reinfection
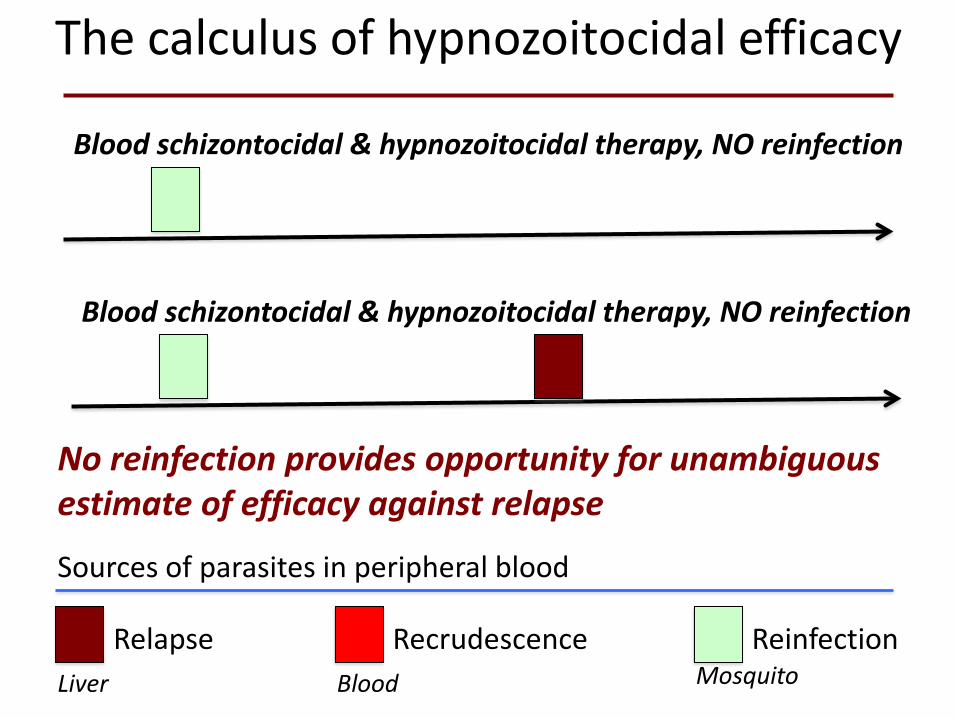
The calculus of hypnozoitocidal efficacy
Relapse Recrudescence Reinfection Liver Blood Mosquito
Sources of parasites in peripheral blood
Blood schizontocidal & hypnozoitocidal therapy, NO reinfection
Blood schizontocidal & hypnozoitocidal therapy, NO reinfection
No reinfection provides opportunity for unambiguous estimate of efficacy against relapse
A uniquely useful study population
• Indonesian troops routinely deployed to remote areas
• Movement in battalions of approx. 600 people for 6 months duty
• Often from densely populated & low malaria risk Java
• Often deployed to malaria high risk zones
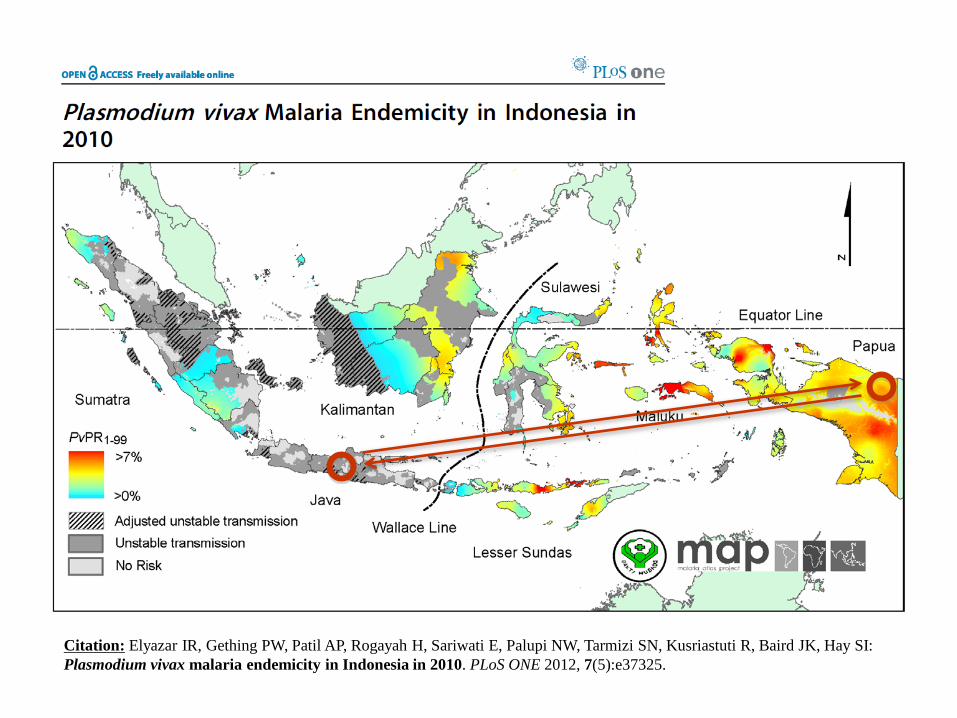
Citation: Elyazar IR, Gething PW, Patil AP, Rogayah H, Sariwati E, Palupi NW, Tarmizi SN, Kusriastuti R, Baird JK, Hay SI: Plasmodium vivax malaria endemicity in Indonesia in 2010. PLoS ONE 2012, 7(5):e37325.
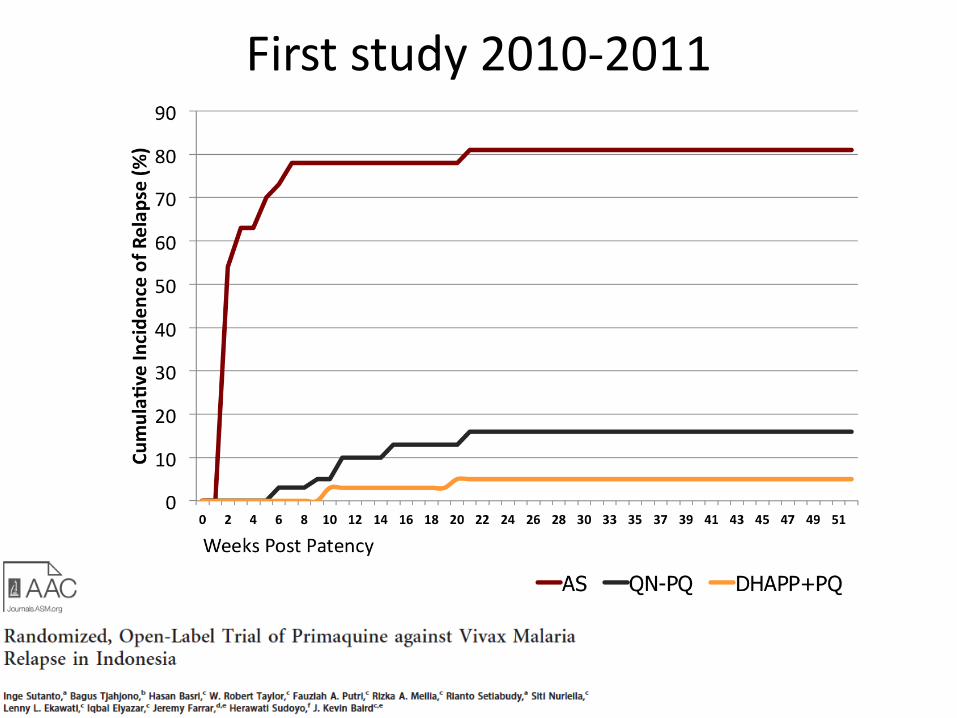
First study 2010-2011
Second study 2013-2014
• Estimate the therapeutic safety and efficacy of primaquine against relapse when combined with artesunate, artesunate-pyronaridine or with dihydroartemisinin-piperaquine
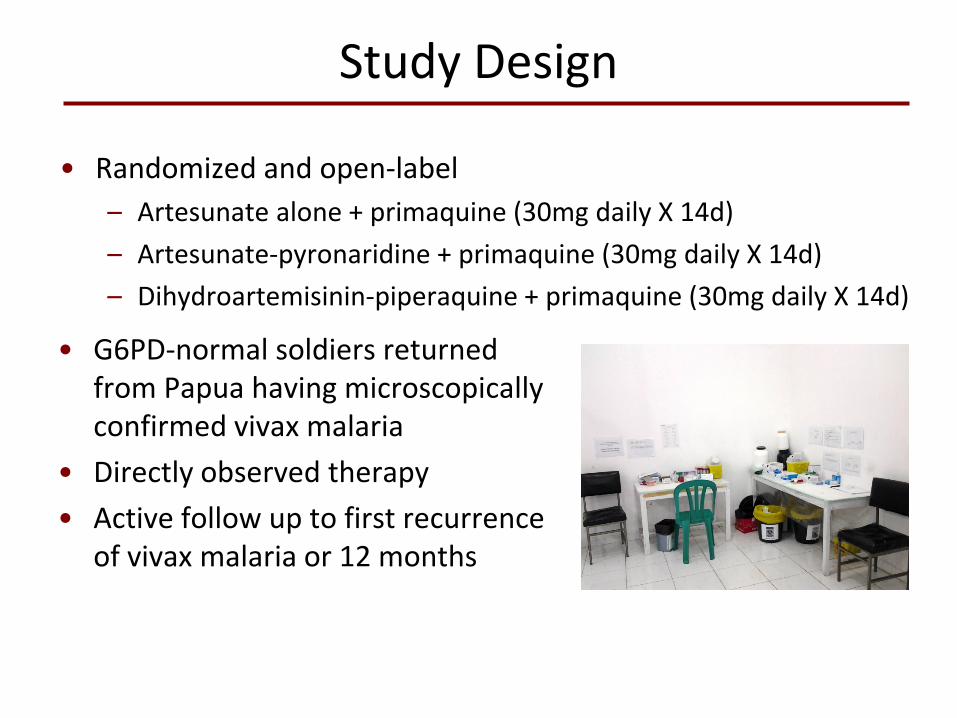
Study Design
• G6PD-normal soldiers returned from Papua having microscopically confirmed vivax malaria
• Directly observed therapy • Active follow up to first recurrence
of vivax malaria or 12 months
• Randomized and open-label – Artesunate alone + primaquine (30mg daily X 14d) – Artesunate-pyronaridine + primaquine (30mg daily X 14d) – Dihydroartemisinin-piperaquine + primaquine (30mg daily X 14d)
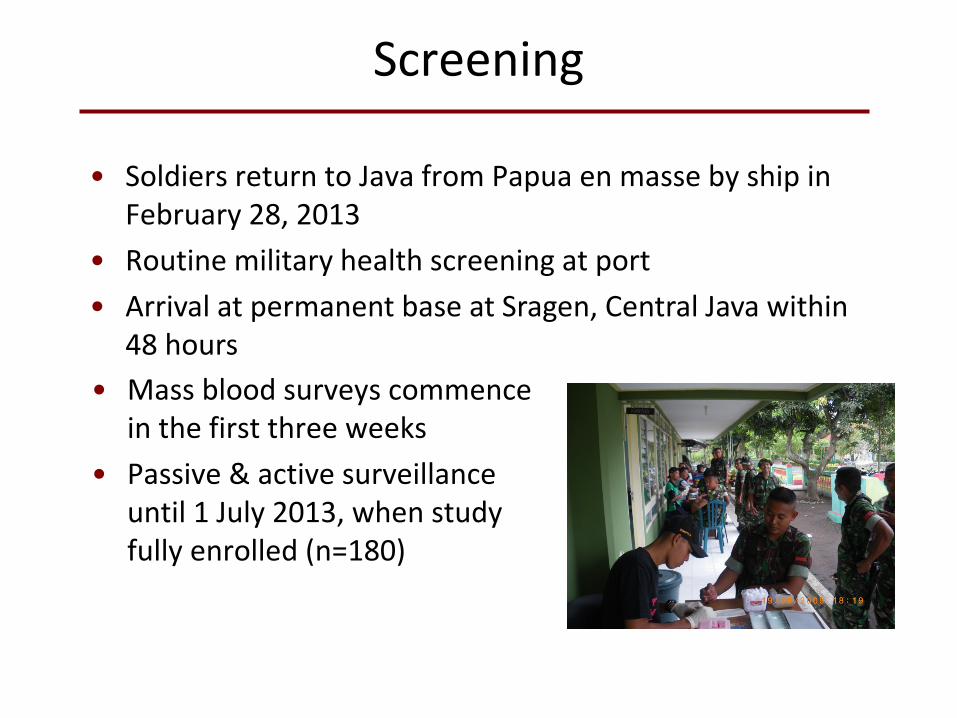
Screening
• Mass blood surveys commence
in the first three weeks • Passive & active surveillance
until 1 July 2013, when study fully enrolled (n=180)
• Soldiers return to Java from Papua en masse by ship in February 28, 2013
• Routine military health screening at port • Arrival at permanent base at Sragen, Central Java within
48 hours
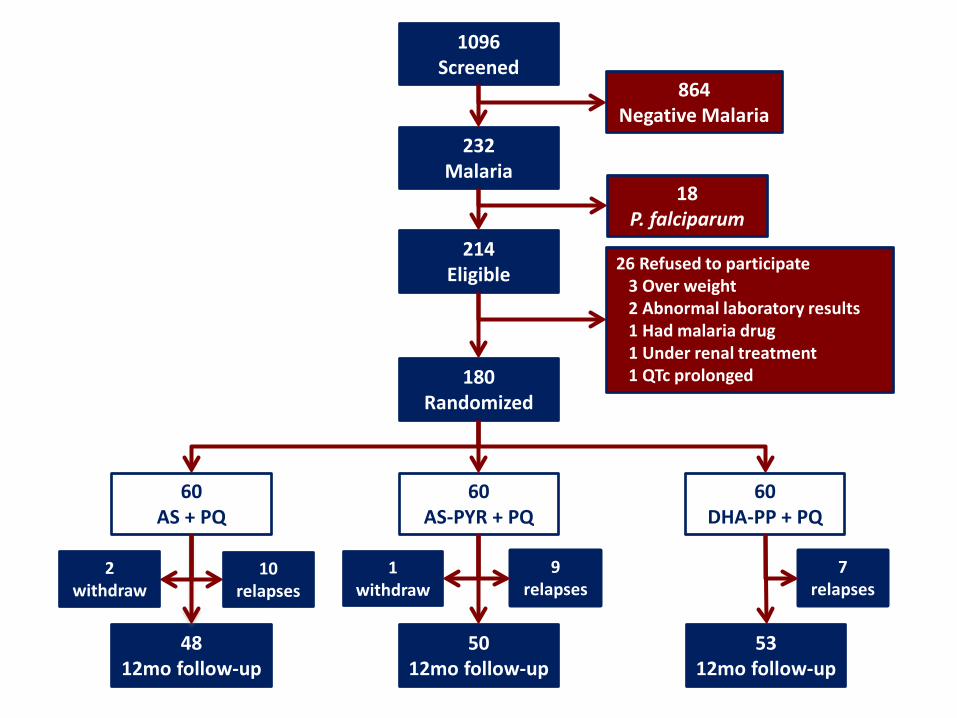
1096 Screened
232 Malaria
864 Negative Malaria
18 P. falciparum
214 Eligible
180 Randomized
60 AS + PQ
60 AS-PYR + PQ
26 Refused to participate 3 Over weight 2 Abnormal laboratory results 1 Had malaria drug 1 Under renal treatment 1 QTc prolonged
60 DHA-PP + PQ
48 12mo follow-up
50 12mo follow-up
2 withdraw
10 relapses
1 withdraw
9 relapses
7 relapses
53 12mo follow-up
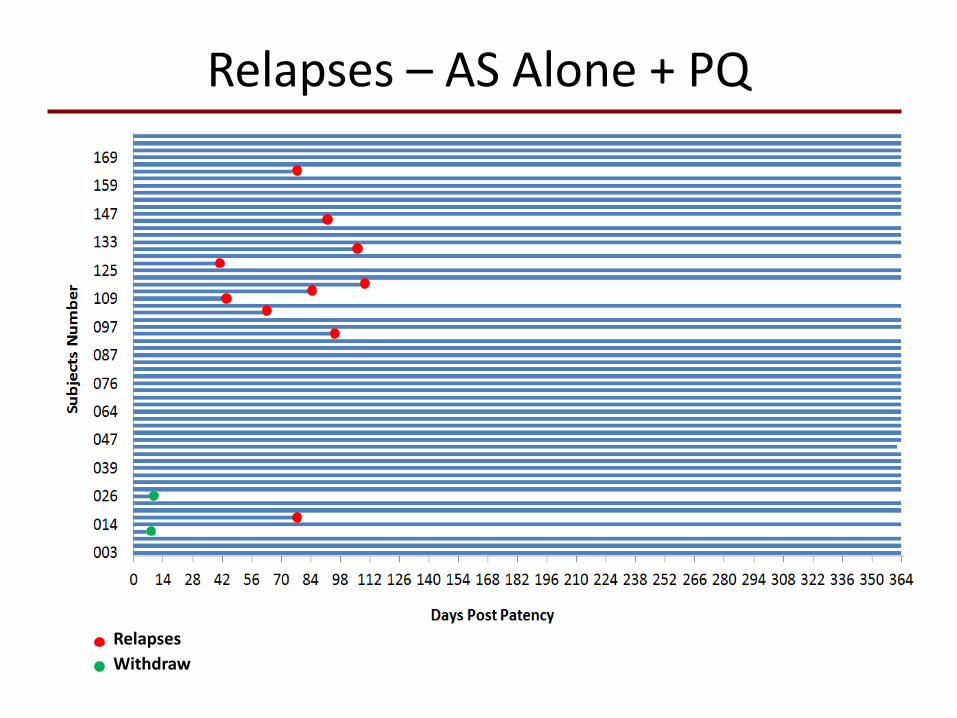
Relapses – AS Alone + PQ
Relapses Withdraw
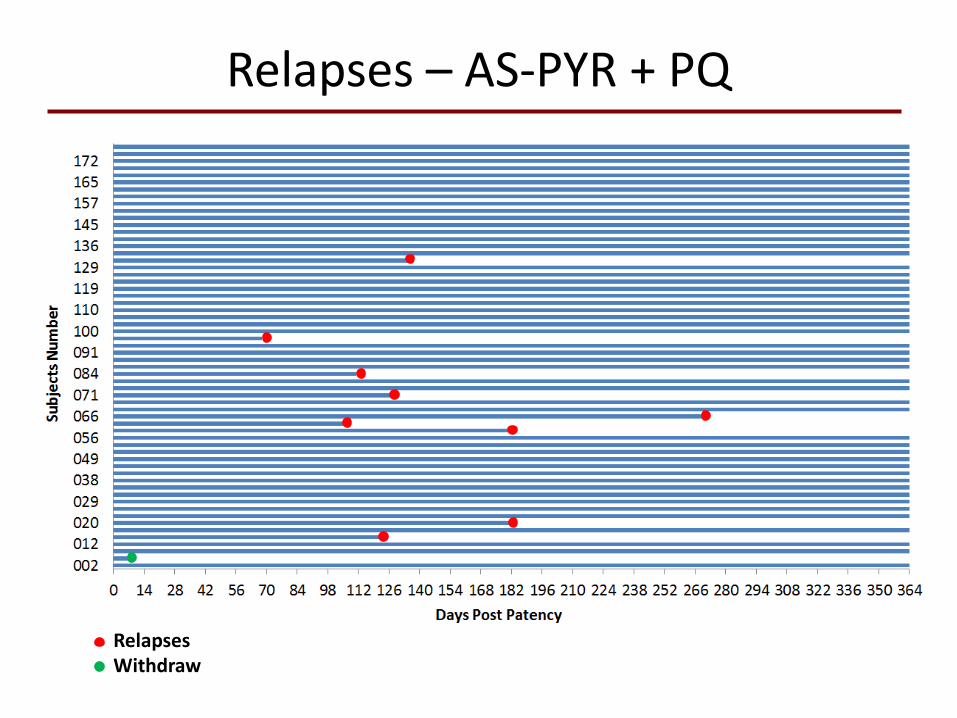
Relapses – AS-PYR + PQ
Relapses Withdraw
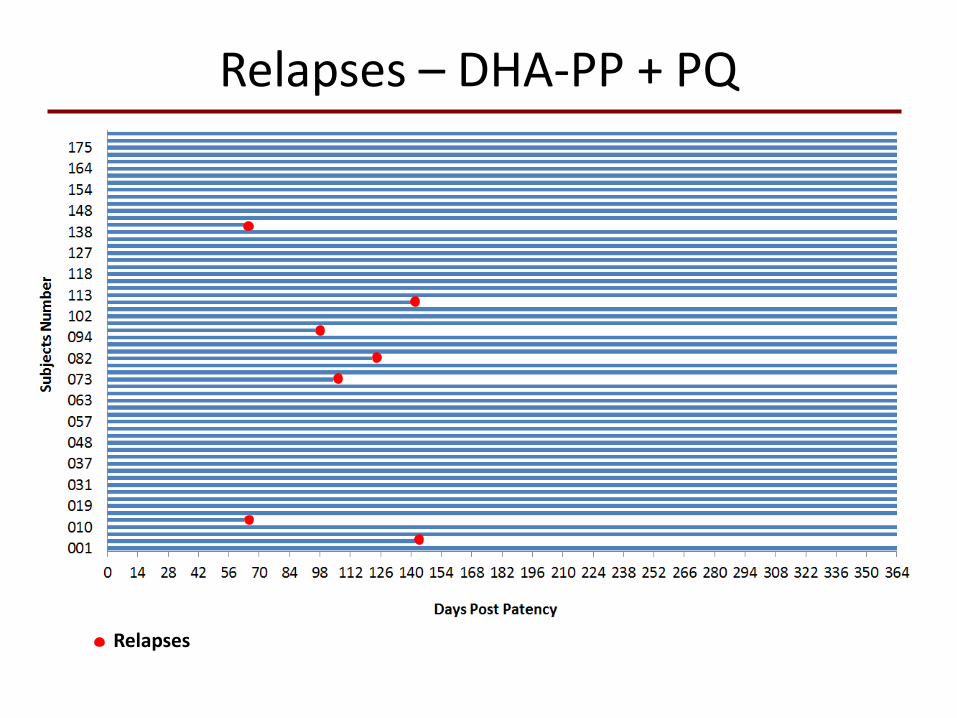
Relapses – DHA-PP + PQ
Relapses
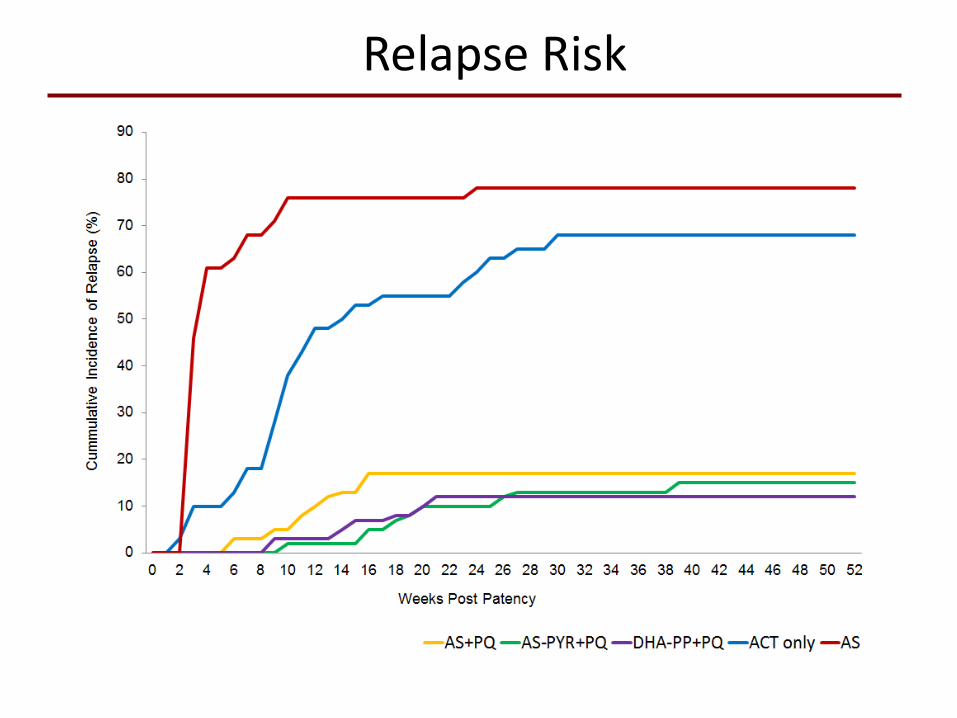
Relapse Risk
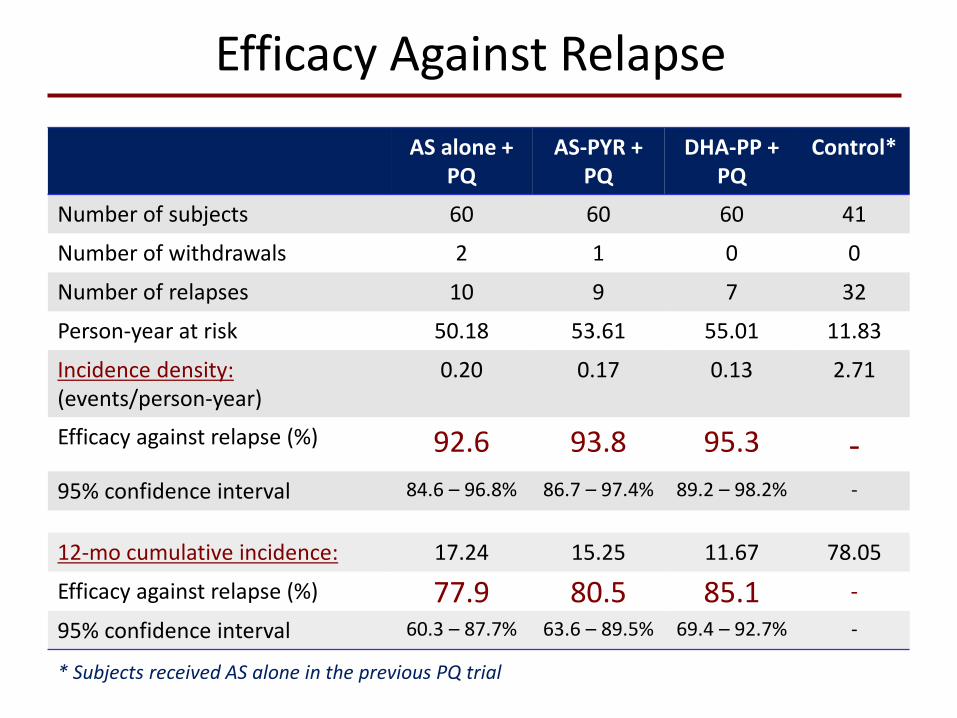
Efficacy Against Relapse
AS alone + PQ
AS-PYR + PQ
DHA-PP + PQ
Control*
Number of subjects 60 60 60 41
Number of withdrawals 2 1 0 0
Number of relapses 10 9 7 32
Person-year at risk 50.18 53.61 55.01 11.83
Incidence density: (events/person-year)
0.20 0.17 0.13 2.71
Efficacy against relapse (%) 92.6 93.8 95.3 - 95% confidence interval 84.6 – 96.8% 86.7 – 97.4% 89.2 – 98.2% -
12-mo cumulative incidence: 17.24 15.25 11.67 78.05
Efficacy against relapse (%) 77.9 80.5 85.1 -
95% confidence interval 60.3 – 87.7% 63.6 – 89.5% 69.4 – 92.7% -
* Subjects received AS alone in the previous PQ trial
Third study: 2016-2017
• Battalion returns from 6mo deployment to Papua, Indonesia approximately January 2016
• Positive for P. vivax all treated with DHA-PP and randomized to: • Tafenoquine single dose + placebo primaquine daily
for 14 days • Placebo tafenoquine single dose + Primaquine 14 daily
doses • Placebo tafenoquine single dose + placebo primaquine
daily for 14 days
Randomized, double-blind, double-dummy, placebo-controlled

Supporters
Funding & administration partners
Armed Forces of Indonesia
Faculty of Medicine University of Indonesia
Partner institutions