Embed Size (px)
Citation preview

Int. Y. Oral Surg. 1976: 5:180-186
(Key words: sr~rgery, oral; impacted teeth, orthodontics)
Results of surgical exposure of impacted cuspids and bicuspids in relation to patients' somatic and dental maturation
MIKKO ALTONEN AND SINIKKA MYLL.~RNIEMI
Departments of Oral Surgery, Pedodo~ztics, and Orthodontics, Institute of Dentistry, University of Helsinki, Helsinki, Finland
ABSTraCT -- The aim of the study was to correlate the rate of post- operative eruption of impacted teeth after surgical exposure to the patients' somatic and dental development. This relationship was ana- lyzed in 31 patients with impacted cuspids or bicuspids, 12 of whom were over 25 and 19 under 21 years of age. Surgical uncovering of the impacted teeth was carried out and the degree of subsequent eruption was evaluated 4 months after the operation. On uncovering the crown was exposed as far as the cementoenamel junction and the surrounding bone was covered with mucous membrane. Dental age and growth rate were used as variables describing individual somatic and dental maturation. After surgical uncovering eruption took place in all but one tooth. Eruption was quicker and more complete i~ children who were still growing than in young adults. The eruption process was also more favorable in dentitions still under formation than in cases with completed dental development. Early intervention and total surgical uncovering of the crown are advocated in cases of impacted teeth.
(Received ]or publication 2 Februaryj accepted 10 May 1976)
An impacted, malposed cuspid or bicuspid is always a difficult clinical problem. In various population studies the frequency of non-erupt ion of maxillary cuspids after the completion of occlusal development has been indicated at 0.92 % - 1.8 %~,~,21,~,a2. Patients with cuspid impactions constitute a relatively large proportion of the oral surgery and orthodontic patients gathering at orthodontic and oral surgery treatment
units. It is a frequent drawback in ortho- dontic practice that the patients present for treatment when they have completed their somatic and dental maturation and the eruptive movement of the surgically ex- posed tooth is slow or nonexistent. More- over, unfavorable secondary changes, due to the missing tooth, may be present in the dental arches. According to clinical ex- perience treatment is quicker, easier and

SURGICAL EXPOSURE OF TEETH 181
less compl i ca t ed in cases w h e r e t h e cuspid
i m p a c t i o n has b e e n r ecogn ized soon af ter
t he n o r m a l e r u p t i o n t i m e of t h e canine.
I n t h e p re sen t s t udy the e rup t i on of sur-
g ica l ly exposed i m p a c t e d t ee th is cor re la ted
to t h e pa t ien ts ' s o m a t i c and d e n t a l m a t u r a -
t ion.
Material and methods Forty-four patients had undergone a surgical exposure and subsequent or thodontic treat- men t for an impacted cuspid or bicuspid in the period f rom 1970-1974. Fifty'-two teeth had been exposed. Twelve of these patients were over 25 years old. Complete annual he ight and weight records were obtained from the school heal th records of 19 of the re- main ing 32 patients. The series thus consists of 22 adult and 19 adolescent patients. In the group of adults 14 malposed maxillary cuspids, four of which were labially real- posed, were uncovered. In the group of ado- lescents, 20 teeth were uncovered; one man- d ibular canine, one mand ibu la r first bicuspid, and two labially and 16 palatal ly malposed maxi l lary canines.
Surgical exposure was carried out as fol- lows. An or thopan tomogram and a stereo- scopic X-ray picture were taken in each case. Determinat ion of t he exact posit ion of the impacted cuspid and the choice of incision site were made on the basis of the stereo- scopic picture.
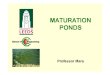
The operatio.n technique for maxillary cus- pids is shown in Figs. 1 and 2. Principally, the incision on the buccal side was made sim- ilarly to that on the palatal side. The deeper the crown was embedded in the buccal bone, the more marginally, measured f rom the cusp, was the arched incision made. T he palatal
incision through the interdental papillae was made from the second premolar to the mesial of the central incisor on the same side, and then, preserving the nasopalatine neurovaseu- lar bundle, toward the palate.
After reflection of the flap, the major pala- tal artery was ligated at the level of the second premolar. Using mallet and chisel the crown was exposed as f a r as the eementoenamel junction and on bo th sides of the crown as widely as was possible without damaging the roots of the adjacent teeth. The tooth was then luxated slightly with instruments. The flap was cleft, thinned and modified so as to cover well the wound surface in the bone around the exposed crown, and sutured if necessary. The operated area was covered with Nobetec| paste, which was removed after 14 days.
The crown was left exposed for a period of 4 months, during which the eruption was inspected by the orthodontist. At the end of this period the degree of eruption assessed
of the primary stereoscopic radio- clinical inspection, was recorded
on the basis graphs and as follOWs:
not erupted less t h a n half of the crown erupted
2> M = over ha l f of the crown erupted 1 = whole crown erupted 2 = whole crown erupted and tooth
moved into a more favorable posi- tion.
Dental age and growth velocity were used as individual matura t ion variables. The dental age of each patient was estimated from ortho~ pantomograms on the basis of tooth formation, using the age medians given by t t~Vlrd(o 11 for Finnish children. Third molars were not used in dental age estimation. If the apices of all teeth mesial to them were registered as closed, dental development was considered
i",,, / , 4',
C ---x_.__a_._..x.~ -
Fig. 1. Exposure method for buccally located unerupted cuspid. A. Incision for exposure. B. Two flaps bent to sides and crown freed from bone. C. Flaps are modeled and adapted around crown.

182 ALTONEN AND MYLL&RNIEMI
A B C Fig. 2. Exposure method for palatally located unerupted cuspid. A. Incision for exposure of one cuspid does not exceed the midline. B. Flap bent before ligation of major palatal artery, after which crown is uncovered. C. Flap is thinned and modeled around crown with scissors, and adapted to bone surface.
completed. The phase of root development of the impacted tooth was recorded from the orthopantomograph.
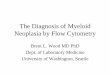
Conventional growth velocity curves (Fig. 3) were drawn in those cases where height measurements were available for a period of at least 3 years before and 1 year after the operation and the measurements had been annually performed in the same month. The time of surgical exposure was marked on each graph.
Results Only one labially malposed maxillary ca- nine in a 30-year-old male showed no erup- tive movement after operation. Table 1 shows the relationship between growth ve- locity and the postoperative eruption of the surgically exposed teeth in the present patier~ts. Complete eruption of the crown within 4 months occurred in the two groups with rapid growth and a :relatively good eruptive response was also obtained in those patients who approached the cessation of height gain. The slowest eruption was re- corded in the group of adult patients.
Using individual dental age as a variable (Table 2) the results also indicated a quick eruption in patients whose dentitions were still in formation. Root formation was ob- served in only three of the treated teeth. These belonged to the youngest patients, all of whom belonged to the group with rapid growth (Fig. 3).
Discussion The methods of exposure described in the literature are essentially similar, but indi- vidual variations in performing the opera- tion occur. To some extent the method depends on the location of the tooth in the bone 30. In order to prevent infection, the exposed crown has been covered again by suturing the flap to its site12, ~0. All authors have made an opening in the flap for the crown to extend through. A rather wide exposure of the crown is recom- mendedl4,~7,1s. The formation of scar tissue on the crown, which inhibits eruption, is best prevented by careful and exact mod- eling of the thinned mucous membrane around the crown.
An additional device, such as a pontostift or stainless steel wire~0, le, 27,'.,a, a crown form of plasticS, 0-2 or of stainless steel 2 has been fastened to the crown in order to guide the eruption and to bring the tooth into its proper position in the arch. Different packing materials have also been used in order to force the tooth in the desired direction. The present authors con- sider slight luxation of the exposed tooth a useful means of stimulating its eruption, especially in cases where the cuspid is di- rected toward the roots of incisors a,14
After wound-healing regular folIow-up is still necessary. If this is undertaken by

SURGICAL EXPOSURE OF TEETH 183
12 11 lC
9
6 .E 5
3 t b
n- 2
I .H. 1~ 12.0
i
8 lb 1? 111 1; 1; 6 Age
the orthodontist, the treatment possibly re- quired can be introduced immediately. A follow-up time of 4-6 months seems ap- propriate.
The regulation and mechanism of tooth eruption are not completely understood. Attention has been drawn to the effect of local factors on the eruptive movement. In this connection root development, changes
Fig. 3. Orthopantomogram and growth velocity curve of the youngest girl in the series. Upper left cuspid impacted palatally; apex of the tooth is closed. Surgical uncovering performed at 12.0 years when patient's dental age was 11.4 years and she was in a phase of rap~d growth. Crown of canine completely erupted in 4 months.
in the pulpal tissue and changes in the periodontal ligament and the tissues cov- ering the tooth have been discussed~. MASSLER :& SCHOUR 20 bave presented a "vascular theory", based on the presence of abundant blood vessels in the pulpal and periapical tissue of erupting teeth.
With regard to the systemic regulation of dental development and tooth eruption it is generally accepted that an association between dental and skeletal development exists, although not a very close one. I t appears that the factors determining bone age are not identical with those controlling dental development~,0, t6,26,~8. Dental devel- opment, especially tooth eruption, is dis- turbed in thyroid and pituitary disorders as weI1 as in hyperfunction of the adrenal

184 ALTONEN AND MYLLARNIEMI
Table 1. Degree of eruption 4 months postoperatively in various growth velociW levels
Degree of eruption Annual height gain at the time of operation Total no. of
2> 4 cm 2--4 cm O-Z cm 0 cm patients
0 - - - 1 1 < ~ / i - 1 2 8 11 >~A - 2 2 3 7
1 6 6 2 - 14 2 I - - - 1
Total no. of patients 7 9 6 12 34
cortex4,S, el. There are racial differences ha tooth eruption timing1% 9-7 and a genetic in- fluence has been demonstrated%
The emergence of the permanent teeth belonging to the second eruption period into the oral cavity occurs during the pe- riod of accelerated puberal growth, or is closely related to iP. In a study dealing with the years around puberty SIERSBAEK- NmLSEN -~* observed an increased rate of eruption of incisor teeth during the time of max imum puberal growth in height. HELM ,& SErDLER la pointed out that there is a tendency towards grouped emergence of teeth, the teeth within one group emer- ging more or less simultaneously. During its normal development the canine tooth in the maxilla undergoes alveolar eruption when two thirds of the root has developed and erupts into the oral cavity when the
root has reached its whole length but the apical part is still open n , simultaneously with the second premolarla. The various factors leading to impaction of canines have been discussed by DEWEL 7, SALMAN 23 THILANDER ,c~r JACOBSON 29 and SCHULZE 24.
On the basis of the obtained results the present authors venture to make the fol- lowing clinical recommendations:
The impacted tooth should be sufficient- ly uncovered. In order to avoid disturbance of the formation of periodontal ligaments, the uncovering should not exceed the ce- mentoenamel junction. Covering of the ex- posed bone surface with a thinned mu- cous flap is recommended to prevent gran- ulation tissue from forming around the c r o w n .
The uncovering of impacted teeth should be timed as closely as possible to the phys-
Table 2. Degree of eruption 4 months postoperatively in various dental age groups
Degree of eruption Dental age at the time
of operation Dental develop- Total no. of < 12 12-15 ment completed patients
0 - - 1 1 < ~ - - ~1 11 > ~ - 4 3 7
1 3 8 3 14 2 1 - - 1
Total no. of patients 4 12 18 34

SURGICAL EXPOSURE OF TEETH 185
iological eruption time of the tooth in question in order to use the patients ' growth and maturation to advantage and to prevent unfavorable secondary changes in the oc- clusion.
To make this possible a routine screening for maxillary canine impactions is sug- gested. This can easily be carried out in countries with systematic dental care. The most suitable time for radiographic inspec- tion in suspicious cases is after the eruption of the maxillary second premolars.
In cases of tooth impaction the phase of the patient's somatic and dental devel- opment should be evaluated, as this has an effect on the prognosis for the treatment. Rapid postoperative eruption can be ex- pected if the patient is still growing.
References 1. BJORK, A. ,& HELM, S.: Prediction of the
age of maximum puberal growth in body height. Angle Orthod. 1967: 37: 134-143.
2. BLr.rM, B. & LEWN, S.: A modified tech- nique for surgical exposure of impacted maxillary cuspids. N . Y . State Dent. J. 1967: 33: 83-86.
3. CLARK, D. C.: The management of im- pacted canines: free physiologic eruption. J. Am. Dent. Assoc. 1971: 82: 836-840.
4. CoREr, r, M. ,& WAON~R, K.: Dental devel- opment in pituitary dwarfism. J. Dent. Res. 1948: 27: 445-458.
5. Cm~MER, H. C.: Dental survey of one thousand adult males: A statistical study correlated with physical and laboratory findings. J. Am. Dent. Assoc. 1929: 16: 122.
6. DACnI, S. F. & HOWELL, F. V.: A survey of 3,874 routine fullmouth radiographs. II. A study of impacted teeth. Oral Surg. 1961: 14: 1165.
7. DEW, L, B. F.: Clinical diagnosis and treat- ment of palatally impacted cuspids. Dent. Digest 1945: 51: 492.
8. GARN, S., LEWIS, A. & BLIZZARD, R.: En- docrine factors in dental development. J. Dent. Res. 1965: 44: 243-257.
9. GAltN, S., LEwis, A. & KEREWSKY, R.: Genetic, nutritional and maturational cor-
relates of dental development. J. Dent. Res. 1965: ,14: 228-242.
10. Gwn'q~m, C. D.: Exposure of unerupted upper cuspids for orthodontic purpose. J. Am. Dent. Assoc. 1945: 32: 265-270.
11. HAAVIKKO, K.: The /ormation and the alveolar and clinical eruption oJ the per- manent teeth. Thesis, Helsinki, 1970.
12. HAOERS'~at6M, L. & BJ~SRr.rN, G.: Surgical- orthodontic treatment of impacted canines in the upper jaw. Sven. Tandlaek. Tidskr. 1967: 60: 129-133.
13. HELM, S. ,& SE~r~r.ER, B.: Timing of per- manent tooth emergence in Danish chil- dren. Commlmity Dent. Oral Epidemiol. 1974: 2: 122---129.
14. HELMORE, F. E. ~; NORTON, R. Y.: The unerupted cuspid. Co-operation between orthodontist and oral surgeon. Aust. Dent. J. 1954: 58: 370-378.
15. HURME, V. O.: Ranges of Imrmalcy in the eruption of permanent teeth. J. Dent. Child. 1949: 16: 11.
16. LACP.Y, K., PARKrN, J. & S'r~EL, G.: Re- lationship between bone age and dental development. Lancet 1973: ii: 736-737.
17. L~ow, C. S.: The oral surgeons' role in management of erupted teeth. Am. J. Or- thod. 1952: 38: 521-529.
18. I_aPmN, M. M.: Practical management of the impacted maxillary cuspid. Am. 1. Or- thod. 1951: 37: 769--778.
19. MAONUSSON, B.: Tissue changes during molar tooth eruption. Thesis, Vmes 1968.
20. MASSLER, M. ,& ScI-rOrJR, I.: The devel- opment of the human dentition. J. Am. Dent. Assoc. 1941: 28: 1153-1160.
21. MoNrELrUS, G. A.: Impacted teeth. A comparative study of Chinese and Cau- casian dentitions. J. Dent. Res. 1932: 12: 931.
22. REISER, R. E.: A technique for surgical- orthodontic management of impacted teeth. J. Pract. Orthod. 1969: 3: 410-417.
23. SALMAN, L.: The surgical exposure of the impacted and unerupted tooth as an aid to orthodontics. N. Y. State Dent. J. 1961: 27: 273-283.
24. ScrltrI.ZE, C.: DevelopmentM abnormalities of the teeth and jaws. In: G o ~ , R. & GOLDMAN, H. (ed.). The C. V. Mosby Company, St. Louis 1970, pp. 151-153.
25. S~RSDAE~-NmLsEN, S.: Rate of eruption of central incisors at puberty: an implant study on eight boys. Tandlaegebladet 1971: 75: 1288-1295.

186 ALTONEN AND MYLLXRNIEMI
26. STaEL, G. Iq.: The relation between dental maturation and physiological maturity. Dent. Pract. 1965: 16: 23-34.
27. STaGGEe, DA, M. ,& HzLL, T. J.: Eruption time of teeth among Whites, Negroes and Indians. Am. J. Orthod. Oral Surg. 1942: 28: 361-370.
28. T , ~ R , J. M.: Growth at adolescence. Blackwell Scientific Publications, Oxford 1962.
29. Tmr.~a'qDER, B. & JAKOBSSON, S. O.: Local factors in impaction of maxillary canines. Acta Odont. Scand. 1968: 26: 145-168.
30. THILANDER) H., THILANDER, B. ,(~ PERSSON, G.: Treatment of impacted teeth by sur- gical exposure. A survey study. Swed. Dent. J. 1973: 66: 519-525.
31. WAC~t,a~R, K., COHEN, M. & HUNT, E.: Dental development in idiopathic sexual precocity, congenital adrenocortical hyper- plasia and adrenogenic virilism. J. Pediat. 1963: 63: 560-576.
32. VON KONOW, L.: Condition of the denti- tlon and ]awbones of a Finnish working age population. Thesis, Helsinki 1971.
Address:
M. Altonen Fabianinkatu 24 00100 HeIsinki 10 Finland