Embed Size (px)
Citation preview

Results From Panitumumab Regimen Evaluation in Colorectal
Cancer to Estimate Primary Response to Treatment (PRECEPT):
Second-Line Treatment With Panitumumab and FOLFIRI by
Tumor KRAS StatusAllen L. Cohn,1 David A. Smith,2 Marcus A. Neubauer,3
Gerry Ann Houston,4 Pankaj Khandelwal,5 R. Glen Wiggans,6 Kathy Zhang,7 Mohamed Yassine8
1Rocky Mountain Cancer Centers, Denver, CO, USA; 2Northwest Cancer Specialists, PC, Vancouver, WA, USA; 3Kansas City Cancer Center, Overland Park, KS, USA; 4Jackson Oncology Associates PLLC, Jackson, MS, USA; 5West Texas Cancer Center, Odessa, TX, USA; 6Northeast Georgia Cancer Care,
LLC, Athens, GA, USA; 7Amgen Inc., South San Francisco, CA, USA; 8Amgen Inc., Mississauga, Ontario, Canada

Introduction• Panitumumab, a fully human antibody to the
epidermal growth factor receptor (EGFR), is approved in the US as monotherapy in patients with metastatic colorectal cancer (mCRC) after disease progression on standard chemotherapy and in the EU, Canada, and Australia as monotherapy in patients with wild-type tumor KRAS status1,2
• The status of the KRAS gene in tumors (wild-type or mutant) is a predictive biomarker of response to anti-EGFR antibody monotherapy in patients with mCRC3-5
• PRECEPT is the first study to prospectively estimate the efficacy of panitumumab plus folinic acid/ 5-fluorouracil/irinotecan (FOLFIRI) treatment according to tumor KRAS status in patients receiving second-line treatment for mCRC

Study Objectives• To estimate the effect of tumor KRAS
mutation status on efficacy endpoints in patients receiving panitumumab plus FOLFIRI treatment as second-line therapy in patients with mCRC
• To evaluate the safety profile of second-line panitumumab with FOLFIRI

MethodsStudy Design
• Phase 2, multicenter, open-label, single-arm, clinical trial conducted in the U.S.
• Patients received panitumumab (6 mg/kg) plus FOLFIRI until disease progression, panitumumab intolerability, death, or withdrawal from study
• Tumor tissue (paraffin block or slides) for KRAS testing was collected at screening
• Tumor response was assessed by the investigators using modified Response Evaluation Criteria in Solid Tumors (RECIST) at week 8 and every 8 weeks thereafter

MethodsStudy Design (continued)
• Tumor response was assessed approximately every 12 weeks in patients who discontinued second-line treatment prior to disease progression
• Adverse events were described using MedDRA version 11.1 terms and graded based on the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI CTCAE) version 3.0
• Patients who discontinued the study underwent a follow-up safety visit 4 weeks ± 7 days after the last dose of second-line treatment

Methods (continued) Study Schema
aPatients who discontinued second-line treatment prior to disease progression had repeat radiographic tumor assessments once every 12 weeks for up to 52 weeks after the final patient was enrolled FOLFIRI, folinic acid/5-fluorouracil/irinotecan; Q2W, Every 2 weeks; CR, Complete response; PR, Partial response; SD, Stable disease
SCREENING
DAY
1
OF
CYCLE
1
FOLFIRI plusPanitumumab 6 mg/kg
Q2W
TUMOR
RESPONSE
EVALUATION
CR, PR,or SD
TumorResponseEvaluation
Every 8Weeks
PROGRESSION
OR
TOXICITY
SAFETY
VISIT
POST-TREATMENT
FOLLOW-UPa
Within28 Days
OfStudyDay 1
StudyDay 1
Week 8
-

Study Endpoints• Efficacy Endpoints (Investigator
assessment)– Objective response rates – Best overall response rates– Progression-free survival– Time to disease progression– Time to treatment failure– Overall survival
• Safety Endpoints– Incidence and severity of adverse events– Changes in selected laboratory values

Key Eligibility Criteria• ≥ 18 years of age• Metastatic adenocarcinoma• Prior treatment failures:
– Disease progression following fluoropyrimidine and oxaliplatin-based chemotherapy with bevacizumab for mCRC (≥ 4 therapeutic doses of bevacizumab and oxaliplatin)
– Toxicity from fluoropyrimidine, oxaliplatin, and/or bevacizumab
• Measurable disease per modified RECIST• Eastern Cooperative Oncology Group (ECOG)
performance status of 0 or 1• Adequate hematologic, renal, hepatic, and metabolic
functions• No prior irinotecan therapy • No prior anti-EGFR therapy

KRAS Determinations• DNA was isolated from fixed tumor samples• Mutant KRAS was detected using a KRAS mutation
kit (DxS Ltd, Manchester, UK) that used allele-specific, real-time polymerase chain reaction (PCR)– The kit can detect approximately 1% of mutant DNA in a
background of wild-type genomic DNA– The test identifies 7 somatic mutations in codons 12 and
13:• Gly 12 Asp• Gly 12 Ala• Gly 12 Val• Gly 12 Ser• Gly 12 Arg• Gly 12 Cys• Gly 13 Asp

Statistical Analyses• Analysis sets:
– Primary Analysis Set – all patients receiving ≥ 1 dose of panitumumab with valid baseline KRAS status available (N = 109)
– Safety Analysis Set – all patients receiving ≥ 1 dose of panitumumab (N = 115)
• Efficacy data were stratified by KRAS mutation status
• Hazard ratios for progression-free survival, overall survival, and time to treatment failure were estimated from a Cox Proportional Hazards regression model with only KRAS effect (wild-type vs mutant)

ResultsPatient Disposition
• 109 patients have been enrolled, received ≥ 1 dose of panitumumab, and had known KRAS status– 64 patients (59%) had wild-type KRAS– 45 patients (41%) had mutant KRAS
• At the time of data cut-off (02 January 2009), 106 patients (97%) had discontinued second-line treatment– The most common reason was disease progression – 67
patients (61%)• 35 patients (55%) had wild-type KRAS• 32 patients (71%) had mutant KRAS
• 81 patients (74%) had ended the study– The most common reason was death – 70 patients (64%)
• 34 patients (53%) had wild-type KRAS• 36 patients (80%) had mutant KRAS

ResultsBaseline Patient Demographics and Disease Characteristics (Primary Analysis Set)
aTime from diagnosis to date of enrollmentECOG, Eastern Cooperative Oncology Group
Wild-Type KRAS Mutant KRAS All Patients(N = 64) (N = 45) (N = 109)
Male sex – n (%) 47 (73) 26 (58) 73 (67)
White/Caucasian race – n (%) 52 (81) 35 (78) 87 (80)
Age – mean years (minimum, maximum) 61 (33, 85) 59 (29, 80) 60 (29, 85)
ECOG performance status – n (%)0 30 (47) 27 (60) 57 (52)1 34 (53) 17 (38) 51 (47)2 0 1 (2) 1 (1)
Primary tumor diagnosis – n (%)Colon 45 (70) 27 (60) 72 (66)Rectum 19 (30) 18 (40) 37 (34)
Time since primary cancer diagnosisa –median months (minimum, maximum) 16.0 (5.8, 108.6) 14.9 (2.2, 225.7) 15.8 (2.2, 225.7)
Time since metastatic disease diagnosisa –median months (minimum, maximum) 12.6 (1.0, 50.2) 13.0 (0.8, 31.2) 12.8 (0.8, 50.2)
Reason for ending first-line treatment – n (%)Disease progression 52 (81) 38 (84) 90 (83)Toxicity 12 (19) 7 (16)

ResultsBest Objective Response (Primary Analysis Set)
CL, Confidence limit
Wild-Type KRAS Mutant KRAS All Patients(N = 64) (N = 43) (N = 107)
Objective tumor response – n (%)
Complete response 2 (3) 1 (2) 3 (3)
Partial response 13 (20) 6 (14) 19 (18)
Stable disease 26 (41) 18 (42) 44 (41)
Disease progression 13 (20) 11 (26) 24 (22)
Unable to evaluate/Not done 10 (16) 7 (17) 17 (16)
Objective response rate
Patients with complete or partial response - n 15 7 22
Crude rate - % (95% CL) 23 (13, 34) 16 (5, 27) 21 (13, 28)
• The odds ratio of the best objective response rate for wild-type vs mutant KRAS status was 1.57 (95% CL: 0.58, 4.26) in favor of wild-type KRAS status

ResultsProgression-Free Survival (Primary Analysis Set)
Events Median Weeksn/N (%) (95% CL)
Wild-type KRAS 54/64 (84) 26 (19, 33)Mutant KRAS 43/45 (96) 19 (12, 25)
Hazard ratio = 0.8 (95% CL: 0.5, 1.1)
Patients at risk:Wild-type KRAS 64 38 19 6 1 0Censored 0 3 3 0 3 1Mutant KRAS 45 24 9 3 1 0Censored 0 1 0 0 1 0
0 17 34 51 68 85
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
Prop
ortio
nof
Patie
nts
With
Prog
ress
ion-
Free
Surv
ival

ResultsOverall Survival (Primary Analysis Set)
Events Median Weeksn/N (%) (95% CL)
Wild-type KRAS 34/64 (53) 50 (39, 76)Mutant KRAS 36/45 (80) 31 (23, 47)
Hazard ratio = 0.6 (95% CL: 0.4, 0.9)
Patients at risk:Wild-type KRAS 64 51 35 18 6 0Censored 0 5 2 8 9 6Mutant KRAS 45 36 20 12 4 0Censored 0 1 1 0 5 2
Weeks0 19 38 57 76 95
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
Prop
ortio
nof
Patie
nts
Surv

ResultsTime to Treatment Failure (Primary Analysis Set)
Events Median Weeksn/N (%) (95% CL)
Wild-type KRAS 60/64 (94) 19 (14, 25)Mutant KRAS 44/45 (98) 15 (8, 19)
Hazard ratio = 0.7 (95% CL: 0.5, 1.1)
Patients at risk:Wild-type KRAS 64 34 7 4 0 0 0Censored 0 0 0 1 1 0 0Mutant KRAS 45 17 5 2 1 0 0Censored 0 0 0 0 0 1 1
Weeks
0 18 36 54 72 90 108
1.0
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
0.1
0
Prop
ortio
nof
Patie
nts
With
out

• The median estimated time to disease progression was:– 26 weeks (95% CL: 16, 34) in patients
with wild-type KRAS – 17 weeks (95% CL: 15, 25) in patients
with mutant KRAS
ResultsOther Efficacy Endpoints

ResultsTreatment Exposure (Safety Analysis Set)
Wild-Type KRAS Mutant KRAS All Patientsa
(N = 64) (N = 45) (N = 115)
Panitumumab
Median doses per patient (min, max) 7.5 (1, 30) 6.0 (1, 27) 7.0 (1, 30)
Median weeks of dosing per patient (min, max) 16.9 (2.0, 76.9) 14.0 (2.0, 55.1) 16.0 (2.0, 76.9)
Average RDI – median % (min, max) 88.2 (48.8, 104.7) 90.2 (53.3, 107.4) 89.3 (40.3, 107.4)
Irinotecan
Median doses per patient (min, max) 8.0 (1, 31) 5.0 (1, 27) 7.0 (1, 31)
Median weeks of dosing per patient
(min, max) 17.6 (2.0, 69.3) 12.0 (2.0, 55.1) 17.0 (2.0, 69.3)
Average RDI – median % (min, max) 86.9 (40.1, 197.9) 88.9 (38.4, 105.5) 87.4 (38.4, 197.9)
Infusional 5-FU
Average RDI – median % (min, max) 80.9 (40.2, 121.2) 78.3 (33.5, 122.3) 80.0 (33.5, 122.3)
Bolus 5-FU
Average RDI – median % (min, max) 88.3 (26.1, 104.4) 90.7 (0, 196.5)
aIncluded 6 patients without known KRAS statusRDI, Relative dose intensity

ResultsSummary of Adverse Events (Safety Analysis Set)
aIncluded 6 patients without known KRAS statusAE, Adverse event; SD, Standard deviation
Wild-Type KRAS Mutant KRAS All Patientsa
(N = 64) (N = 45) (N = 115)
Any AE – n (%) 64 (100) 45 (100) 115 (100)
Grade 3 40 (63) 29 (64) 72 (63)
Grade 4 9 (14) 4 (9) 14 (12)
Grade 5 4 (6) 3 (7) 8 (7)
Any panitumumab-related AE – n (%) 61 (95) 41 (91) 107 (93)
Worst grade ≥ 3 35 (55) 19 (42) 56 (49)
Any serious AE – n (%) 23 (36) 20 (44) 46 (40)
Any serious panitumumab-related AE – n (%) 9 (14) 6 (13) 15 (13)
Any AE leading to discontinuation – n (%) 11 (17) 6 (13) 18 (16)
Patients who died on study – n (%) 34 (53) 36 (80)
• Premedication is not required for panitumumab treatment– 2 patients had an investigator-reported infusion-related reaction;
subsequent doses and administrations were not altered

ResultsComparison of Safety Between KRAS Strata
• More patients with tumors with mutant KRAS– experienced serious adverse events
(44%) vs those with wild-type KRAS (36%)
– died during the study (80%) vs those with wild-type KRAS (53%)
– died within 60 days of the first dose (7%) vs those with wild-type KRAS (2%)

ResultsGrade 5 Events
• 8 grade 5 events were reported on study– In patients with tumors with wild-type KRAS,
events included: sepsis (n = 2; 1 death was deemed to be related to panitumumab by the investigator); metastatic colon cancer (n = 1); and respiratory failure (n = 1)
– In patients with tumors with mutant KRAS, events included: cardiac arrest (n = 1); colon cancer (n = 1); and rectal cancer (n = 1)
– In patients with tumors with unknown KRAS, 1 patient died of metastatic colon cancer

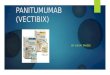
ResultsAdverse Events of Interesta (Safety Analysis Set)
aRelated and unrelated to panitumumab; MedDRA v11.1 preferred terms; grading based on NCI CTCAE v3.0 (with modification for panitumumab-related skin toxicities)bIncluded 6 patients without known KRAS status
Wild-Type KRAS Mutant KRAS All Patientsb
(N = 64) (N = 45) (N = 115)Any Grade Grade Any Grade Grade Any Grade Grade
Grade 3 4 Grade 3 4 Grade 3 4
Skin-related toxicity 56 (88) 18 (28) 0 38 (84) 10 (22) 0 99 (86) 30 (26) 0
Diarrhea 52 (81) 8 (13) 1 (2) 28 (62) 3 (7) 1 (2) 85 (74) 12 (10) 2 (2)
Nausea 34 (53) 3 (5) 0 26 (58) 5 (11) 0 64 (56) 8 (7) 0
Infections 31 (48) 7 (11) 1 (2) 18 (40) 5 (11) 0 54 (47) 14 (12) 1 (1)
Vomiting 20 (31) 2 (3) 0 12 (27) 4 (9) 0 36 (31) 6 (5) 0
Neutropenia 17 (27) 10 (16) 5 (8) 15 (33) 10 (22) 1 (2) 33 (29) 20 (17) 7 (6)
Hypomagnesemia 15 (23) 3 (5) 2 (3) 8 (18) 0 0 23 (20) 3 (3) 2 (2)
Dehydration 15 (23) 6 (9) 0 12 (27) 4 (9) 0 30 (26) 12 (10) 0
Deep vein thrombosis 6 (9) 6 (9) 0 2 (4) 1 (2) 0 8 (7) 7 (6) 0
Pulmonary embolism 5 (8) 2 (3) 3 (5) 2 (4) 0 2 (4) 7 (6) 2 (2) 5 (4)

Conclusions• Panitumumab plus FOLFIRI as second-line
treatment appeared to be well tolerated and had antitumor activity in patients with mCRC
• Numerical differences in favor of patients with wild-type KRAS were observed in efficacy endpoints in PRECEPT, consistent with results from previous panitumumab monotherapy studies4,5
– The observed response rates, progression-free survival, and overall survival are encouraging in patients with tumors expressing wild-type KRAS
• Panitumumab had a safety profile consistent with other FOLFIRI panitumumab trials

References1. Vectibix® Prescribing Information, Amgen Inc. Thousand Oaks, CA;
2008.2. Van Cutsem E, Peeters M, Siena S, et al. Open-label phase III trial
of panitumumab plus best supportive care compared with best supportive care alone in patients with chemotherapy refractory metastatic colorectal cancer. J Clin Oncol. 2007;25:1658-1664.
3. Benvenuti S, Sartore-Bianchi A, Di Nicolantonio F, et al. Oncogenic activation of the RAS/RAF signaling pathway impairs the response of metastatic colorectal cancers to anti-epidermal growth factor receptor antibody therapies. Cancer Res. 2007;67:2643-2648.
4. Amado RG, Wolf M, Peeters M, et al. Wild-type KRAS is required for panitumumab efficacy in patients with metastatic colorectal cancer. J Clin Oncol. 2008;26:1626-1634.
5. Freeman DJ, Juan T, Reiner M, et al. Association of KRAS, BRAF, and PI3K mutational status and clinical outcomes in patients with metastatic colorectal cancer receiving panitumumab monotherapy. Clinical Colorectal Cancer. 2008;7:184-190.