Embed Size (px)
Citation preview

Results From a EuropeanMulticenter Randomized Trial ofPhysical Activity and/or HealthyEating to Reduce the Risk ofGestational Diabetes Mellitus: TheDALI Lifestyle PilotDiabetes Care 2015;38:1650–1656 | DOI: 10.2337/dc15-0360
OBJECTIVE
Ways to prevent gestational diabetes mellitus (GDM) remain unproven. We com-pared the impact of three lifestyle interventions (healthy eating [HE], physicalactivity [PA], and both HE and PA [HE+PA]) on GDM risk in a pilot multicenterrandomized trial.
RESEARCH DESIGN AND METHODS
Pregnant women at risk for GDM (BMI ‡29 kg/m2) from nine European countrieswere invited to undertake a 75-g oral glucose tolerance test before 20 weeks’gestation. Those without GDM were randomized to HE, PA, or HE+PA. Womenreceived five face-to-face and four optional telephone coaching sessions, basedon the principles of motivational interviewing. A gestational weight gain (GWG)<5 kg was targeted. Coaches received standardized training and an interventiontoolkit. Primary outcome measures were GWG, fasting glucose, and insulin sen-sitivity (HOMA) at 35–37 weeks.
RESULTS
Among the 150 trial participants, 32% developed GDM by 35–37 weeks and 20%achieved GWG <5 kg. HE women had less GWG (22.6 kg [95% CI24.9,20.2]; P =0.03) and lower fasting glucose (20.3mmol/L [20.4,20.1]; P = 0.01) than those inthe PA group at 24–28 weeks. HOMA was comparable. No significant differencesbetween HE+PA and the other groups were observed.
CONCLUSIONS
An antenatal HE intervention is associated with less GWG and lower fasting glu-cose comparedwith PA alone. These findings require a larger trial for confirmationbut support the use of early HE interventions in obese pregnant women.
Gestational diabetes mellitus (GDM) is associated with increased risk of adverseperinatal outcomes, with a continuous relationship between glycemia on oral glu-cose tolerance test (OGTT) and pregnancy outcome (1). Obesity in pregnancy andexcess gestational weight gain (GWG) are associated with similar adverse pregnancyoutcomes, which are additional to any harm from antenatal hyperglycemia (2).
1Institute of Metabolic Science, AddenbrookesHospital, Cambridge, U.K.2University of Western Sydney, Campbelltown,NSW, Australia3Department of Public and Occupational Health,EMGO+ Institute for Health and Care Research, VUUniversityMedicalCenter,Amsterdam, theNetherlands4KU Leuven Department of Development andRegeneration: Pregnancy, Fetus and Neonate,Gynaecology and Obstetrics, University Hospi-tals Leuven, Leuven, Belgium5Institut de Recerca de l�Hospital de la Santa Creui Sant Pau, Barcelona, Spain6CIBERBioengineering,BiomaterialsandNanotech-nology, Instituto de Salud Carlos III, Madrid, Spain7National University of Ireland, Galway, Ireland8Department of Obstetrics and Gynecology,Medizinische Universitaet Graz, Graz, Austria9Gender Medicine Unit, Division of EndocrinologyandMetabolism, Department of Internal MedicineIII, Medical University of Vienna, Vienna, Austria10Center for Pregnant Women with Diabetes,Rigshospitalet, University of Copenhagen, Co-penhagen, Denmark11Odense University Hospital, Odense, Denmark12Universita Degli Studi di Padova, Padua, Italy13AziendaOspedaliero-UniversitariaPisana,Pisa, Italy14Department of Obstetrics and Women’s Diseases,PoznanUniversityofMedical Sciences,Poznan,Poland15Recherche en Sante Lawson SA, Bronschhofen,Switzerland16BAPHealthOutcomesResearch SL, Oviedo, Spain17Department ofMedical Psychology, VUUniver-sity Medical Center and Academic Medical Cen-ter, Amsterdam, the Netherlands
Corresponding author: David Simmons,[email protected].
Received 18 February 2015 and accepted 12May2015.
Clinical trial reg.no. ISRCTN70595832,www.isrctn.org.
This article contains Supplementary Data onlineat http://care.diabetesjournals.org/lookup/suppl/doi:10.2337/dc15-0360/-/DC1.
Aslide set summarizing thisarticle is availableonline.
© 2015 by the American Diabetes Association.Readers may use this article as long as the workis properly cited, the use is educational and notfor profit, and the work is not altered.
David Simmons,1,2 Judith G.M. Jelsma,3
Sander Galjaard,4 Roland Devlieger,4
Andre van Assche,4 Goele Jans,4
Rosa Corcoy,5,6 Juan M. Adelantado,5
Fidelma Dunne,7 Gernot Desoye,8
JurgenHarreiter,9 Alexandra Kautzky-Willer,9
Peter Damm,10 Elisabeth R. Mathiesen,10
Dorte M. Jensen,11 Lise Lotte Andersen,11
Annunziata Lapolla,12 Maria Dalfra,12
Alessandra Bertolotto,13
Ewa Wender-Ozegowska,14
Agnieszka Zawiejska,14 David Hill,15
Pablo Rebollo,16 Frank J. Snoek,17 and
Mireille N.M. van Poppel3
1650 Diabetes Care Volume 38, September 2015
CLINCARE/ED
UCATION/N
UTR
ITION/PSY
CHOSO
CIAL

Although obesity in pregnancy, ex-cess GWG, and GDM are associatedwith adverse outcomes, the evidencethat interventions to reduce theseharms are beneficial is mixed (3). In ameta-analysis, combined lifestyle inter-vention (physical activity [PA] withhealthy eating [HE]) was associatedwith reduced GWG (overall and insome studies), but not with improve-ment in perinatal outcomes (macroso-mia or cesarean delivery) or significantreduction in GDM rates (3). More recentlarge randomized controlled trials(RCTs) have shown no reduction in theincidence of GDM with lifestyle inter-vention, with limited differences inGWG between intervention and controlwomen (4–6), but potential reductionsin birth weight (5). Although preventionof excessive GWG and macrosomia arekey goals in such interventions, therehas been concern that too little mater-nal weight gain could be associated withan increased incidence of small-for-gestational-age babies and reduced off-spring fat-free mass (7). With thesecautions, it is clear that further trialsare needed to investigate efficacious ap-proaches that will reduce GWG and pro-gression to GDM, particularly in obesewomen.We now report on the findings from
the lifestyle pilot for DALI (Vitamin DAnd Lifestyle Intervention for GDM pre-vention) (8), undertaken to test the pro-cedures, methodology, and lifestyleinterventions for the forthcoming fullRCT within a European multicenter RCTof three different lifestyle approachesfor the prevention of GDM. The pilotreports on risk of GDM rather thanGDM itself and does not include the vi-tamin D intervention.
RESEARCH DESIGN AND METHODS
Overall Study DesignThe pilot study for DALI is a multicenterRCT of three different lifestyle ap-proaches that could prevent GDM. Thepilot was undertaken across 10 Euro-pean centers in nine countries, eachwith its own nutrition and PA culturalnorms. This diversity in backgroundpopulations was included to ensurethat the intervention was applicable indifferent settings and populations. Thestudy was approved by the relevantethics committees. The pilot was regis-tered as an RCT (ISRCTN70595832). The
primary outcomes were maternalweight gain (defined as the weightchange from baseline measurement tothe last measurement at 35–37 weeksof gestation), fasting glucose, and insulinsensitivity as derived from the HOMA at35–37 weeks (9). The pilot study was de-vised to recruit four women for each ofthe three interventions in each center(total n = 120).
ParticipantsPregnant women aged $18 years, be-fore 20 weeks of gestation with a pre-pregnancy BMI $29 kg/m2 (based onfeasibility following a review of Euro-pean obesity prevalence), were eligiblefor inclusion. Women were excludedfrom the study if they were diagnosedwith GDM by OGTT before randomiza-tion, using World Health Organization(WHO) 2013 criteria (fasting venousplasma glucose $5.1 mmol/L and/or1-h glucose $10 mmol/L and/or 2-hglucose$8.5 mmol/L) (10). Other exclu-sion criteria were pre-existing diabetes,inability to walk$100m safely, multiplepregnancy, requiring a complex diet, asignificant chronic medical condition orpsychiatric disease, and inability tospeak the major language of the countryof recruitment fluently or to conversewith the lifestyle coach in another lan-guage for which translated materialsexisted.
RecruitmentThe 10 centers were Cambridge (coordi-nating center), Galway, Amsterdam,Leuven, Poznan, Pisa/Padova (as onecenter), Barcelona, Vienna, Odense, andCopenhagen. A common informationsheet, in the local language, was givento eligible participants for considerationand the trial explained by the researchmidwife/nurse. Written consent was ob-tained for participation. The pilot studystarted in January 2012, and the last par-ticipant gave birth in August 2013.
ProceduresAfter signed consent, assessments weremade by the research midwife/nursebefore 20 weeks (screening/baseline),24–28 weeks, and 35–37 weeks of ges-tation and after delivery. The lifestyleintervention was delivered by a lifestylecoach. Where GDM developed afterbaseline, womenweremanaged accord-ing to local practice. Supplementary Fig. 1
provides a diagrammatic overview ofassessments and intervention.
RandomizationEligible women were randomly allo-cated to one of the three interventions(HE, PA, or both [HE+PA]) following anallocation schedule prestratified for in-tervention center, using a computerizedrandom number generator. Sealed opa-que envelopes (containing the interven-tion arm to which each participant wasallocated with a randomization number)were sent to each site by the DALI trialcoordinator (D.S.). After assurance of el-igibility, the personal details of the par-ticipant were provided to the lifestylecoach who opened the next randomiza-tion envelope. Those involved withmeasurements were kept blinded tothe intervention through noninvolve-ment and explicit training. Separationbetween coach and measurementsteam was assessed during site monitor-ing visits.
Lifestyle InterventionsAfter randomization, five face-to-faceand four optional telephone coachingsessions were scheduled for each partic-ipant, as shown in Supplementary Fig. 1.As previously described (8), coaching in-volved discussion of seven HE and/orfive PA “messages” based upon previouswork (11), as shown in Table 1. Mes-sages were supported by a “toolkit” forthe participant, including participanthandbook, educational materials (e.g.,adapted F.I.T.T. model [frequency, in-tensity, time, type]) based on AmericanCollege of Obstetricians and Gynecolo-gists (ACOG) guidelines (12), pedome-ters (Yamax Digiwalker SW-200, Tokyo,Japan), and flexible elastic dynabands(Thera-Band, Akron, OH). The messagedelivery was built upon behavioral the-ory principles (13), including patient em-powerment and cognitive behavioraltechniques inspired by motivational in-terviewing (14). At least four face-to-face coaching sessions were expectedto take place before the second mea-surement session, and the interventionwas completed by 35 weeks of gesta-tion. Standardization of the interventionwas achieved through a training pro-gram concluding with an observed ses-sion with an actor, provision of a deskfile with all materials and methods, anduse of a personal digital assistant (PDA;
care.diabetesjournals.org Simmons and Associates 1651

HTC HD7 Windows phone), with be-spoke software to provide a frameworkfor the session. A “paper” PDA includingall fields was available for when therewere any problems with the PDA.A key component was for women to
strive to achieve a maximum GWG of5 kg, as this is the lower limit of theweightgain recommended by the Institute ofMedicine (IOM) for those with a BMI$30 (15) and following the observationof better outcomes among Danish obesewomen with this degree of weight gain(16). If GWG was already beyond this be-fore the start of the intervention or GWGexceeded 5 kg, women were supportedto minimize their GWG thereafter. Thecoaches had scales available to assistwomen with their weight managementwhen scaleswerenot available in thehome.
AssessmentsAt the three OGTT sessions (Supplemen-tary Fig. 1), after a 10-h fast, womencompleted questionnaires (including,e.g., demographics, prepregnancy weight,lifestyle, past/current medical andobstetric history, and medication use)and anthropometric measurements be-tween blood tests. Local laboratorieswere used to rapidly obtain results ofthe OGTT to assess eligibility for thestudy. Blood samples were centrifuged,and separated serum and plasma ali-quots (1,000 or 250 mL) were placed inmicrorack tubes and stored at 2208C or2808C until further analysis in the cen-tral trial laboratory in Graz, Austria, cer-tified according to ISO 9001 standards.Glucose was measured using the
hexokinase method (DiaSys Diagnostic
Systems, Holzheim, Germany) with alower limit of sensitivity of 0.1 mmol/L.Insulin was quantified by a sandwich im-munoassay (ADVIA Centaur; SiemensHealthcare Diagnostics Inc., Vienna,Austria) with an analytical sensitivity of0.5 mU/L, intra-assay coefficients of var-iation (CVs) of 3.3–4.6%, and interassayCVs of 2.6–5.9%. Leptin was measuredusing a sandwich ELISA (DRG Instru-ments, Marburg, Germany). The assayhad an analytical sensitivity of 1.0 ng/mL,intra-assay CVs of 6.0–7.0%, and interas-say CVs of 8.7–11.6%. All assayswere per-formed according to the instructions ofthe manufacturer. HOMA was calculatedas [glucose z insulin]/22.5 (9).
Height was measured at baselinewith a stadiometer (SECA 206; SECA,Birmingham, U.K.; Leicester Height Mea-sure), and the average value of twomeasurements was used. Women wereweighed on calibrated electronic scales(SECA 888 and SECA 877) wearing noshoes and light clothes, to the nearest0.1 kg; the average value of two mea-surements was used. Weight gain wasdefined as the change in objectivelymeasured weight and was calculatedfor three periods: baseline to 24–28weeks, baseline to 35–37 weeks, and24–28 to 35–37 weeks. Data from themedical records were obtained regard-ing comorbidities, obstetric and perina-tal outcomes, and birth weight.
OutcomesAs primary outcomes, GWG, fasting glu-cose, and insulin sensitivity (HOMA) at35–37 weeks were used as they will bein the main trial. Secondary outcomes
were the number of women who devel-oped GDM, birth weight, insulin concen-tration, and leptin concentration.
StatisticsTrial data were entered into a bespokeweb-based electronic database using theMicrosoft.NET development environ-ment. For the assessment at 35–37weeks, fasting glucose and insulin and in-sulin sensitivity were carried forwardfrom24–28weeks if GDMwas diagnosed.WomendiagnosedwithGDMat 24weeks(n=44)wereexcluded fromthe35–37-weekGWG analyses. Insulin and HOMA datawere log transformed because ofskewness. As a pilot, no power calcula-tions were performed to decide on sam-ple size, and it was arbitrarily agreed thatfour women would be recruited per in-tervention per site to test local proce-dures while minimizing pilot size.
Data were analyzed according to theintention-to-treat principle. Analyses wereperformed blind to the intervention groupallocation. Analyses for the RCT were per-formed according to an a priori statisticalanalysis plan, and hence no adjustmentwas made to significance levels for multi-ple comparisons. Differences between to-tal study sample and number of subjectsdropping out of the study were assessedusing Student t test (normally distributedcontinuous variables), Mann-Whitney Utest (skewed continuous variables), orx2 test (categorical variables). To assess dif-ferences between intervention groups,multilevel analyses were performed, withtwo levels (coach and individual). Thistakes into account possible clustering ef-fects, since the success of treatment canbe dependent on the skills of the provideras well as specific characteristics of atreatment center. Analyseswere adjustedfor baseline values of the outcome or forBMI at baseline for the analyses withGWG outcomes. In the regression anal-yses, all three intervention groups wereentered simultaneously to calculatediffer-ences between groups. In the multilevelmodels, log-transformed data for insulinand HOMA were used. For dichoto-mous variables, logistic regressionmodels were used to assess differen-ces between intervention groups. A bi-lateral P, 0.05 was taken as significant.
RESULTS
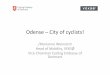
Figure 1 shows the flow of the partici-pants throughout the study. A large
Table 1—Lifestyle messages used
PA intervention1) “Be active every day”: Incorporate light and moderate PA as much as possible into daily
life (e.g., by parking further away from destination or undertaking special activities forpregnant women).
2) “Sit less”: Reduce sedentary time.3) “Build your strength”: Incorporate upper and/or lower limb resistance exercise as PA.4) “Take more steps”: Increase the number of steps taken per day.5) “Be more active at weekends”: Be more active during the weekends.
HE intervention1) “Replace sugary drinks”: Reduce intake of sugary drinks (e.g., replace with water).2) “Eat more nonstarchy vegetables”: Eat more nonstarchy vegetables.3) “Increase fiber consumption”: Choose high-fiber over low-fiber products ($5 g fiber/100 g).4) “Watch portion size”: Be conscious about the amount of food eaten each meal.5) “Eat protein”: Increase intake of proteins (e.g., meat, fish, beans).6) “Reduce fat intake”: Reduce fat intake (e.g., snack, fast food, fried foods).7) “Eat less carbohydrates”: Reduce intake of carbohydrates (e.g., potatoes, pasta, rice,
snacks, candy).
1652 DALI Lifestyle Pilot Diabetes Care Volume 38, September 2015

proportion (22%) had GDM on the initialOGTT and hence were not included inthe RCT. The numbers in each groupand their baseline characteristics weresimilar (Table 2). Women dropping out(35; 23%) before the final OGTT hadhigher post-OGTT load glucose and insu-lin concentrations and BMI at baseline(Table 2). Numbers per site rangedfrom 3 in Odense to 26 in Belgium. Sevenof the 150 women showed a weight gainof 5 kg or more between reported pre-pregnancy weight and baseline mea-surements, but many women wereeither unaware of or likely approximatedtheir prepregnancy weight.On average, women gained 8.6 kg (SD
4.6) from baseline to 35–37 weeks ofgestation, and only 20% of womenachieved the ,5 kg GWG target frombaseline across the three interventiongroups. HE alone was associated withless weight gain by 24–28 weeks and35–37 weeks than PA (–2.6 kg [95% CI24.9, 20.2] and 21.6 kg [23.0, 20.2],respectively) (Table 3). No differenceswere observed between HE+PA andthe other two groups.There were no significant differences
in glucose, insulin, or leptinmeasurementsacross groups at baseline or by 24–28weeks’ gestation (Table 3). However, by35–37 weeks’ gestation, HE had signifi-cantly lower fasting glucose and 2-h insulinconcentrationswith nonsignificantly lower
GDM incidence than PA. No significant dif-ferences between HE+PA and the othertwo groups were observed. There wereno significant differences in HOMA or lep-tin (Table 3). At 24–28 weeks, 24 of 130women (19%) had developed GDM, andby 35–37 weeks, this increased to 36 of112 women (32%), of whom 3 receivedinsulin treatment.
CONCLUSIONS
Procedures generally worked well (8),although recruitment overshot (to 150women) due to the lag between base-line data collection, receiving OGTTresults/confirming eligibility, and in-forming all sites that recruitment wascompleted. There was no expectationthat the study would be large enoughto show a difference in the primary out-comes comparing different interven-tions. The significant differences inGWG, fasting glucose, and 2-h insulinlevels (albeit trivial) between HE andPA were therefore surprising, althougheven with the DALI interventions, 32%of women developed GDM. The datasuggest that the HE intervention wasmore efficacious than the PA interven-tion in reducing GDM risk, although thehigher GWG in PA may reflect an in-crease in muscle mass, not necessarilyin adiposity.
Previous RCTs initiated before 20weeks’ gestation have largely shown no
impact on GDM prevalence, fasting glu-cose (3–6,17), or insulin concentrations.Exceptions are the BAMBINO PA inter-vention pilot, which saw a reduction infasting glucose by 28 weeks’ gestation,but with GWG unreported (18), and theLifestyle in Pregnancy (LiP) study, whichshowed lower insulin concentrations at28–30 weeks with the intervention, butno significant reduction in fasting glu-cose (19).
The LiP study showed a GWG differ-ence of only 1.4 kg between interven-tion and control women despite a veryambitious intervention program, in-cluding repeat visits to a dietitian,a weekly fitness class, and fitness cen-ter membership. Thus, a time-consumingprogram might be less effective than asimple one. One of the key issues withlifestyle interventions in general hasbeen their limited impact on GWGwhen compared with control subjects.Several of the RCTs did have lowerGWG in the intervention group (4–6),but control subjects had a lower GWGthan anticipated, resulting in a lesserdifference between the groups. A meta-analysis showed that differences be-tween intervention and control groupsacross 10 RCTs achieved a mean differ-ence in GWG of 22.21 kg (3). In spiteof this, few reported a significant re-duction in glycemia or GDM. The studyby Quinlivan et al. (20) (n = 124) wasthe only trial in the meta-analysisthat achieved a significant reductionin GDM (odds ratio [OR] 0.18) andachieved a 6.80-kg GWG difference.The study by Thornton et al. (21)(n = 232) also achieved a substantiallylower GWG (29.07 kg) but with anonsignificant reduction in GDM(OR 0.53).
Our findings of more/better effectsof diet alone are in line with a previousreview, finding larger effects of dietaryintervention alone on GWG, comparedwith PA or a combined approach (22).We speculate that a combined inter-vention might dilute the message orrequire too much change and then bedemotivating. Another interpretationwould be that a combined interventiondoes not mean “complete” but “partial”HE and PA; PA intervention being lesseffective, HE+PA ranks intermediatebetween HE and PA. The lack of effectof the PA interventions does not im-ply no effect of PA on pregnancy
Figure 1—Consolidated Standards of Reporting Trials (CONSORT) diagram of recruitment, ran-domization, and dropout.
care.diabetesjournals.org Simmons and Associates 1653

and offspring outcomes per se, as thispilot had no control subjects. Interven-tions to increase PA in pregnancy arewell known to be difficult (23), especiallyin the third trimester. Although we arebeing as careful as possible to avoid thekinds of GWG convergence seen in someother major RCTs, it might be difficult toprevent a low GWG in the control groupamong women motivated to come into alifestyle trial. Including multiple Europeancultures might generate a range of life-style responses in control subjects aswell as intervention participants. Suchdifferences between sites, with theirvery different underlying cultural land-scapes (and climates) and associated dif-ferences in nutrition and PA habits, willbe of interest in the main trial. At thispoint, it would appear that our genericapproach to the lifestyle change mes-sages (Table 1) has been successful.These were originally based on an inter-vention among New Zealand Maori (11)and hence expected to be cross cultural
to some extent. We found the motiva-tional interviewing approach to be wellsuited to the intervention. Even so, only29% of participants achieved the ,5 kgGWG goal even in the HE group of thepilot, a proportion comparable to thosein other RCTs (4).
One other difference in the DALI ap-proach from other RCTs is the exclusionof women with GDM by WHO 2013 cri-teria (22%) prior to recruitment. It maybe that in the other trials, it was neverpossible to reverse pre-existing GDM inthese women. However, there is debateover the validity of the new criteria inearly pregnancy (10), which were builtaround data at 24–28 weeks’ gestation(1). Data from China suggest that a sig-nificant proportion of womenwith GDMon the fasting glucose in early pregnancyhave no GDM using the new criteria at24–28 weeks (24).
The studyhas a number ofweaknesses.It was established as a pilot to a full RCT of440 women, and hence there were no
power calculations performed to decideon the number of participants requiredand there was no untreated controlgroup. As a pilot, the expertise of the in-tervention coaches would have improvedover time, in preparation for the main tri-al. Numberswere still too small to look foradherence to lifestyle change or adversepregnancy outcomes. The main trial willreport on accelerometer and food diarydata. We have not adjusted the signifi-cance level for multiple comparisons;however, the comparisons followedour a priori statistical analysis plan, andthe difference in GWG is in linewith otherRCTs, which speaks against the role ofchance.
In conclusion, an HE interventionamong obese European women led tolower GWG, fasting glucose, and 2-h in-sulin concentrations by 35–37 weeks’gestation than a PA intervention or acombination of the two. Although a largertrial is still clearly needed, these pilot find-ings are promising and support the use of
Table 2—Baseline characteristics of all women included in the DALI lifestyle pilot per intervention group and those whodropped out at 35–37 weeks’ gestation
HE, n = 50 HE+PA, n = 50 PA, n = 50 Total, n = 150
Drop out35–37 weeks,n = 35 (23.3%)
P drop out vs.continuing
Age (years) 31.1 6 6.0 30.5 6 5.0 33.1 6 5.2 31.6 6 5.5 32.3 6 5.8 0.37
Multiparous (%) 41.7% 46.0% 46.0% 44.6% 48.6% 0.70
European descent (%) 84.0% 88.0% 90.0% 87.3% 88.6% 1.00
Lives with partner (%) 90.0% 98.0% 87.8% 91.9% 80.0% 0.007
Higher education (%) 44.0% 64.0% 52.0% 53.3% 37.1% 0.03
Maternal smoking (%) 12.0% 22.0% 14.0% 16.0% 22.9% 0.29
Paternal smoking (%) 32.0% 38.0% 38.0% 36.0% 34.3% 0.84
History of GDM (%) 3.2% 3.4% 10.3% 5.6% 9.1% 0.59
First-degree family historyof diabetes (%) 28.0% 26.0% 24.0% 26.0% 28.6% 0.83
Chronic hypertension (%) 14.3% 10.0% 14.0% 12.8% 14.3% 0.78
Gestation on entry (weeks) 14.2 6 1.7 14.2 6 2.0 14.7 6 2.3 14.4 6 2.0 13.9 6 2.2 0.15
Prepregnancy weight (kg) 95.3 6 17.1 93.2 6 15.2 94.1 6 14.6 94.2 6 15.6 94.5 6 17.0 0.89
Weight at entry (kg) 96.4 6 17.0 93.9 6 14.8 96.6 6 14.9 95.7 6 15.5 96.0 6 16.9 0.87
Height (cm) 166.5 6 6.4 165.8 6 6.8 167.2 6 7.5 166.5 6 6.9 163.0 6 6.2 <0.001
BMI pp (kg/m2) 34.3 6 5.6 33.9 6 4.6 33.6 6 4.4 33.9 6 4.9 35.5 6 5.3 0.03
BMI at entry (kg/m2) 34.8 6 5.9 34.1 6 4.7 34.5 6 4.5 34.5 6 5.0 36.0 6 5.2 0.04
Fasting glucose (mmol/L) 4.4 6 0.4 4.6 6 0.6 4.5 6 0.4 4.5 6 0.5 4.6 6 0.3 0.11
1-h glucose (mmol/L) 6.3 6 1.7 6.5 6 1.3 6.5 6 1.5 6.4 6 1.5 7.1 6 1.2 0.01
2-h glucose (mmol/L) 5.5 6 1.2 5.7 6 1.3 5.5 6 1.1 5.6 6 1.2 6.2 6 1.3 0.001
Fasting insulin (mU/L) 14.1 (10.5, 18.2) 12.2 (8.1, 17.9) 14.0 (10.3, 16.6) 13.5 (9.2, 17.8) 12.7 (8.9, 21.6) 0.76
1-h insulin (mU/L) 85.9 (57.8, 156.3) 100.0 (73.3, 154.3) 66.6 (55.7, 120.0) 82.6 (61.5, 150.4) 108.9 (80.9, 174.6) 0.003
2-h insulin (mU/L) 60.3 (36.0, 121.1) 61.0 (40.5, 129.7) 49.3 (32.8, 83.7) 59.5 (36.7, 107.1) 125.8 (60.6, 174.8) <0.001
HOMA 2.76 (1.81, 3.66) 2.26 (1.56, 3.72) 2.75 (1.87, 3.50) 2.65 (1.76, 3.60) 2.49 (1.79, 4.40) 0.58
Leptin (ng/mL) 42.4 6 18.5 42.8 6 17.7 38.9 6 18.1 41.5 6 18.0 46.4 6 18.0 0.11
Data are mean6 SD or median (interquartile range) unless otherwise indicated. No baseline differences were found between intervention groups.The boldface data indicate statistically significant differences. Differences tested with Mann-Whitney U test.
1654 DALI Lifestyle Pilot Diabetes Care Volume 38, September 2015

Table
3—Matern
aloutco
mesin
theDALIlife
style
pilo
tthreeinterve
ntio
ngro
ups
nHE
nHE+PA
nPA
Adjusted
differen
ceorOR(95%
CI)
HEvs.
HE+PA
P
Adjusted
differen
ceorOR(95%
CI)
HEvs.
PAP
Adjusted
differen
ceorOR(95%
CI)
HE+PA
vs.PA
P
Glucose
metab
olism
24–28
weeks
Fastingglu
cose
(mmol/L)
404.3
60.3
424.4
60.4
414.5
60.4
20.001
(201,0.1)
0.9920.1
(20.2,0.1)
0.2020.1
(20.3,0.03)
0.131-h
glucose
(mmol/L)
377.2
61.6
397.2
61.4
397.6
61.7
0.2(2
0.4,0.9)0.43
20.1
(20.8,0.5)
0.6920.5
(21.1,0.2)
0.172-h
glucose
(mmol/L)
365.6
61.3
396.1
61.5
406.1
61.3
20.3
(20.9,0.3)
0.3720.5
(21.0,0.1)
0.1020.2
(20.7,0.4)
0.53Fastin
ginsulin
(mU/L)
4017.9
(12.0,20.6)42
13.1(10.9,20.2)
4315.4
(11.9,19.7)0.05
(20.1,0.2)
0.600.004
(20.2,0.2)
0.9720.04
(20.2,0.1)
0.661-h
insulin
(mU/L)
36157.6
(97.2,194.7)40
139.0(74.7,185.8)
41117.4
(79.7,183.2)0.1
(20.2,0.4)
0.390.1
(20.2,0.3)
0.4720.1
(20.3,0.2)
0.532-h
insulin
(mU/L)
3566.0
(49.1,132.6)40
91.0(44.7,144.6)
4292.2
(51.1,136.8)20.1
(20.4,0.3)
0.7020.2
(20.6,0.1)
0.1720.2
(20.5,0.2)
0.32HOMA
403.30
(2.25,4.08)42
2.63(2.18,3.65)
412.98
(2.11,4.28)20.01
(20.9,0.9)
0.9820.4
(21.4,0.5)
0.3620.4
(21.4,0.5)
0.38Lep
tin(ng/m
L)40
42.76
20.442
39.76
17.941
41.56
17.31.5
(24.8,7.9)
0.6321.6
(27.8,4.7)
0.6223.2
(29.4,3.1)
0.32
Glucose
metab
olism
35–37
weeks
Fastingglu
cose*
(mmol/L)
374.3
60.4
394.4
60.5
424.6
60.4
20.2
(20.3,0.03)
0.0920.3
(20.4,2
0.1)0.01
20.2
(20.3,0.05)
0.161-h
glucose*
(mmol/L)
337.9
61.4
377.8
61.5
388.1
61.6
0.4(2
0.3,1.0)0.28
0.1(2
0.6,0.8)0.79
20.3
(21.0,0.4)
0.412-h
glucose*
(mmol/L)
316.3
61.5
366.7
61.3
386.7
61.0
20.3
(21.0,0.4)
0.3520.6
(21.2,0.01)
0.0620.3
(20.9,0.3)
0.39Fastin
ginsulin*(m
U/L)
3821.8
(14.8,28.4)37
17.9(14.5,27.4)
4018.1
(14.7,24.2)0.1
(20.2,0.4)
0.470.01
(20.3,0.3)
0.9520.1
(20.4,0.2)
0.471-h
insulin*(m
U/L)
33177.6
(115.3,269.1)37
192.5(136.3,220.9)
39175.4
(119.9,230.0)0.1
(20.3,0.4)
0.710.1
(20.2,0.5)
0.470.03
(20.3,0.4)
0.872-h
insulin*(m
U/L)
31115.2
(56.5,187.7)36
152.3(99.6,207.2)
39156.4
(100.0,206.6)20.2
(20.7,0.2)
0.3320.4
(20.8,
20.02)
0.0420.2
(20.5,0.2)
0.37HOMA*
363.90
(2.73,5.54)37
3.44(2.80,5.57)
403.60
(2.29,5.25)20.7
(23.0,1.7)
0.6022.3
(25.6,1.0)
0.1721.8
(25.1,1.5)
0.29Lep
tin(ng/m
L)36
43.76
22.337
42.36
15.040
43.56
17.22.0
(26.6,10.7)
0.6422.6
(210.3,5.2)
0.5124.5
(212.4,3.4)
0.26GDM
at35
–37weeks
(%)
3610
(28%)
3511
(31%)
4115
(42%)
0.84(0.30,2.33)
0.740.67
(0.25,1.75)0.41
0.79(0.31,2.07)
0.64
Weigh
tgain
Weigh
tgain
T1–T2**
(kg)42
3.56
3.942
4.36
3.546
5.26
3.120.8
(22.4,0.7)
0.2922.6
(24.9,2
0.2)0.03
20.7
(23.0,1.6)
0.55Weigh
tgain
T1–T3**,§
(kg)31
7.66
5.330
8.56
4.234
9.66
4.321.0
(23.4,1.4)
0.3921.6
(23.0, 2
0.2)0.02
20.8
(22.3,0.6)
0.24Weigh
tgain
T2–T3**,§
(kg)31
3.96
2.730
3.96
2.034
4.56
2.820.1
(21.4,1.1)
0.8520.5
(21.7,0.87)
0.4320.2
(21.5,1.0)
0.72Weigh
tgain
,5kg**,§
(%)
319(29%
)30
4(13%
)34
6(18%
)2.98
(0.87,10.20)0.08
1.86(0.63,5.52)
0.260.59
(0.17,2.03)0.40
Data
aremean
6SD
ormed
ian(in
terquartile
range)
unless
otherw
iseindicated
.Forcontin
uousoutco
mevariab
les:adjusted
differen
cesfro
mmixed
models,w
ithtw
olevels
(coach
andindivid
ual),ad
justed
for
baselin
evalu
esoftheoutco
me.Fo
rdich
otomousoutco
mevariab
les:logistic
regressionmodels,ad
justed
forbaselin
evalu
esoftheoutco
me.N
aturallo
g-transfo
rmed
values
ofinsulin
were
used
inthemixed
models.N
umbers
ineach
columnvary
with
completen
essofd
ata.Theboldface
data
indicate
statisticallysign
ifican
tdifferen
ces.*Valu
eof24
–28weeks
carriedforw
ardto
35–37
weeks
forwomen
whohad
GDM
at24
–28weeks.**A
djusted
forBMIat
baselin
eandnumber
ofw
eeksbetw
eenmeasu
remen
ts:T1–T2
isweigh
tgain
betw
eenbaselin
eand24
–28weeks;T1
–T3isweigh
tgain
betw
eenbaselin
eand35
–37weeks;
T2–T3
isweigh
tgain
betw
een24
–28weeks
and35
–37weeks.
§Women
with
GDM
at24
–28weeks
excluded
from
analyses.
care.diabetesjournals.org Simmons and Associates 1655

early HE interventions in obese pregnantwomen.
Acknowledgments. The authors thank thecoaches, research midwives and nurses, women,and health professionals collaborating in therecruitment for this study.Funding. This project has received fundingfrom the European Community’s 7th Frame-work Programme (FP7/2007-2013) under grantagreement 242187. In the Netherlands, addi-tional funding was provided by the NetherlandsOrganisation for Health Research and Develop-ment (ZonMw) (grant 200310013). In the U.K.,the DALI team acknowledges the support re-ceived from the NIHR Clinical Research Net-work: Eastern, especially the local diabetesclinical and research teams based in Cambridge.In Spain, additional funding was provided byCAIBER 1527-B-226.
The funders had no role in any aspect of thestudy beyond funding.Duality of Interest.D.M.J. is part of an advisoryboard for research meetings arranged by NovoNordisk. No other potential conflicts of interestrelevant to this article were reported.Author Contributions. D.S. contributed to theconception and design of the trial, wrote theinitial draft of the paper, read and correcteddraft versions of the manuscript, and approvedthe final manuscript. J.G.M.J. performed theanalyses, read and corrected draft versions ofthe manuscript, and approved the final manu-script. S.G., G.J., and J.H. read and correcteddraft versions of the manuscript and approvedthe final manuscript. R.D., A.v.A., R.C., J.M.A.,F.D., G.D., A.K.-W., P.D., E.R.M., D.M.J., L.L.A.,A.L., M.D., A.B., E.W.-O., A.Z., D.H., P.R., and F.J.S.contributed to the conception and design ofthe trial, read and corrected draft versions of themanuscript, and approved the final manuscript.M.N.M.v.P. contributed to the conception anddesign of the trial, performed the analyses, readand corrected draft versions of the manuscript,and approved the final manuscript. D.S. is theguarantor of this work and, as such, had fullaccess to all the data in the study and takesresponsibility for the integrity of the data andthe accuracy of the data analysis.Prior Presentation. Parts of this study werepresented in abstract form at the 75th ScientificSessions of the American Diabetes Association,Boston, MA, 5–9 June 2015.
References1. Metzger BE, Lowe LP, Dyer AR, et al.; HAPOStudy Cooperative Research Group. Hyperglyce-mia and adverse pregnancy outcomes. N Engl JMed 2008;358:1991–2002
2. Simmons D. Diabetes and obesity in preg-nancy. Best Pract Res Clin Obstet Gynaecol2011;25:25–363. Oteng-Ntim E, Varma R, Croker H, Poston L,Doyle P. Lifestyle interventions for overweightand obese pregnant women to improve preg-nancy outcome: systematic review and meta-analysis. BMC Med 2012;10:474. Vinter CA, Jensen DM, Ovesen P, Beck-Nielsen H, Jørgensen JS. The LiP (Lifestyle inPregnancy) study: a randomized controlledtrial of lifestyle intervention in 360 obesepregnant women. Diabetes Care 2011;34:2502–25075. Luoto R, Kinnunen TI, Aittasalo M, et al. Pri-mary prevention of gestational diabetes melli-tus and large-for-gestational-age newborns bylifestyle counseling: a cluster-randomized con-trolled trial. PLoS Med 2011;8:e10010366. Renault KM, Nørgaard K, Nilas L, et al. TheTreatment of Obese Pregnant Women (TOP)study: a randomized controlled trial of the ef-fect of physical activity intervention assessed bypedometer with or without dietary interventionin obese pregnant women. Am J Obstet Gynecol2014;210:134.e1–134.e97. Catalano PM, Mele L, Landon MB, et al.; Eu-nice Kennedy Shriver National Institute of ChildHealth and Human Development Maternal-Fetal Medicine Units Network. Inadequateweight gain in overweight and obese pregnantwomen: what is the effect on fetal growth? AmJ Obstet Gynecol 2014;211:137.e1–137.e78. Jelsma JGM, van PoppelMNM, Galjaard S, et al.DALI: Vitamin D and lifestyle intervention for ges-tational diabetes mellitus (GDM) prevention: anEuropean multicentre, randomised trial - studyprotocol. BMC Pregnancy Childbirth 2013;13:1429. Matthews DR, Hosker JP, Rudenski AS,Naylor BA, Treacher DF, Turner RC. Homeostasismodel assessment: insulin resistance and beta-cell function from fasting plasma glucose andinsulin concentrations in man. Diabetologia1985;28:412–41910. World Health Organization. Diagnostic cri-teria and classification of hyperglycaemia firstdetected in pregnancy, WHO/NMH/MND/13.2.Geneva, World Health Org., 2013. Availablefrom http://apps.who.int/iris/bitstream/10665/85975/1/WHO_NMH_MND_13.2_eng.pdf. Ac-cessed 1 April 201411. Simmons D, Rush E, Crook N; TeWai o Rona:Diabetes Prevention Strategy Team. Developmentand piloting of a community health worker-basedintervention for the prevention of diabetes amongNew Zealand Maori in Te Wai o Rona: DiabetesPrevention Strategy. Public Health Nutr 2008;11:1318–132512. Artal R, O’Toole M. Guidelines of the Amer-ican College of Obstetricians and Gynecologistsfor exerciseduring pregnancy and the postpartum
period. Br J Sports Med 2003;37:6–12; discus-sion 1213. Miller WR, Rollnick S.Motivational Interview-ing, Preparing People to Change Addictive Behavior.New York, The Guildford Press, 199114. Moyers TB, Martin T, Manuel JK, Miller WR,Ernst D. RevisedGlobal Scales:Motivational Inter-viewing Treatment Integrity 3.1.1 (MITI3.1.1),2010. Available from casaa.unm.edu/download/MITI3_1.pdf. Accessed 2 January 201515. Institute of Medicine (US) and National Re-search Council (US); Committee to Re-examineIOM PregnancyWeight Guidelines. Weight GainDuring Pregnancy: Reexamining the Guidelines.Rasmussen KM and Yaktine AL, Eds. Washing-ton, DC, The National Academies Press, 200916. Jensen DM, Ovesen P, Beck-Nielsen H, et al.Gestational weight gain and pregnancy out-comes in 481 obese glucose-tolerant women.Diabetes Care 2005;28:2118–212217. Oostdam N, van Poppel MN, Wouters MG,van Mechelen W. Interventions for preventinggestational diabetes mellitus: a systematic re-view and meta-analysis. J Womens Health(Larchmt) 2011;20:1551–156318. Callaway LK, Colditz PB, Byrne NM, et al.;BAMBINO Group. Prevention of gestational di-abetes: feasibility issues for an exercise inter-vention in obese pregnant women. DiabetesCare 2010;33:1457–145919. Vinter CA, Jørgensen JS, Ovesen P, Beck-Nielsen H, Skytthe A, Jensen DM. Metabolic ef-fects of lifestyle intervention in obese pregnantwomen. Results from the randomized con-trolled trial ‘Lifestyle in Pregnancy’ (LiP). DiabetMed 2014;31:1323–133020. Quinlivan JA, Lam LT, Fisher J. A randomisedtrial of a four-step multidisciplinary approach tothe antenatal care of obese pregnant women.Aust N Z J Obstet Gynaecol 2011;51:141–14621. Thornton YS, Smarkola C, Kopacz SM, IshoofSB. Perinatal outcomes in nutritionally monitoredobese pregnant women: a randomized clinical tri-al. J Natl Med Assoc 2009;101:569–57722. Thangaratinam S, Rogozinska E, Jolly K, et al.Effects of interventions in pregnancy onmaternalweight and obstetric outcomes: meta-analysis ofrandomised evidence. BMJ 2012;344:e208823. Oostdam N, van Poppel MN, Wouters MG,et al. No effect of the FitFor2 exercise pro-gramme on blood glucose, insulin sensitivity,and birthweight in pregnant women who wereoverweight and at risk for gestational diabetes:results of a randomised controlled trial. BJOG2012;119:1098–1107
24. ZhuWW, Yang HX, Wei YM, et al. Evaluationof the value of fasting plasma glucose in the firstprenatal visit to diagnose gestational diabetesmellitus in China. Diabetes Care 2013;36:586–590
1656 DALI Lifestyle Pilot Diabetes Care Volume 38, September 2015