Embed Size (px)
Citation preview

Restrictive & Liberal Red Cell Transfusion Strategies in Adult Patients
Reconciling Clinical Data with Best Practice
Austrian Red CrossVienna - November 2015
Marek Mirski MD, PhDThomas & Dorothy Tung Professor – Anesthesiology &
Critical Care MedicineChief Neuroanesthesiology [1999-2015]Director – Neurosciences Critical Care Units [1999-2015]Professor – Anesthesiology, Neurology, NeurosurgeryJohns Hopkins Medicine

Disclosures -
� No Industry Conflicts
� My wife & I love visiting Vienna
� I am very happy to be here with my International Clinical & Scientific Colleagues

� There is general agreement that RBC transfusion is typically not indicated for hemoglobin (Hb) levels of > 10 g/dL and that transfusion of RBCs should be considered when Hb is < 7 to 8 g/dL depending on patient characteristics. The decision to transfuse RBCs should be based on a clinical assessment of the patient that weighs the risks associated with transfusion against the anticipated benefit.
American Association of Blood Banks (AABB)
Restrictive Transfusion Guideline

� There is general agreement that RBC transfusion is typically not indicated for hemoglobin (Hb) levels of > 10 g/dL and that transfusion of RBCs should be considered when Hb is < 7 to 8 g/dL depending on patient characteristics. The decision to transfuse RBCs should be based on a clinical assessment of the patient that weighs the risks associated with transfusion against the anticipated benefit.
American Association of Blood Banks (AABB)
Restrictive Transfusion Guideline

� Neuro – Physiological Benefits ?- Cerebral & spinal cord O2 delivery- Diminished ischemia- Improved neurological outcomes
� Transfusion Risks ?- Multiple organ dysfunction/failure (MOD/F)- Increased infection risk- Increased mortality
Blood Transfusion Issues -More Than Simply Hgb
� Cardiac Benefits ?- Coronary O2 delivery- Diminished ischemia
� Define Stable Patient?- Small hemorrhage?- Coagulopathy?- Stable post-op?
� Neuro-functional Outcome?- Post-op geriatric- Acute rehabilitation

Gombotz H, Rehak PH, Shander A, Hofmann A. Transfusion 2014;54,2646-57.
-The 2nd Austrian Benchmark Study: Blood Use in Elective Surgery -Results and Practice Change Since 2007
Discussion: “ Larger lost RBC volume, lower preoperative and postoperative nadir Hb levels, and female sex were the main independent predictors of transfusion. The multivariate models generally had high predictive values, accounting for more than 70% of the variation in transfusion rates. Likewise, independent significant predictors of the higher relative volume of transfused RBCs included higher relative lost RBC volume, lower preoperative and postoperative nadir Hb, and female sex when all procedures were considered.”
Nadir Hb in patients who receivedtransfusions (denoted by “TX”) and thosewho did not (denoted by “non TX”). In THRand TKR, the second study showed highernadir Hb in patients who receivedtransfusions and lower values in patients whodid not receive transfusions. In CABG, allpatients presented with lower nadir Hb in thesecond study. (■) First study; (□) secondstudy.

-RBC Transfusion -Results and Practice Change
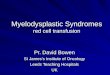
Murphy et. al. Crit Care Med2013;41,2344-55.

- EVIDENCE BASED MEDICINE –Era of Databases & Correlations
Be Careful What&
How You ReadThe Literature !
Since 2012 - > 550 PubMed articles on “Restrictive Transfusion”

� Left-shifting the Hb disassociation curve may theoretically impair tissue delivery of oxygen
� Ample clinical data - correction of anemia in both stable and critically ill patients provides an acute increase in oxygen delivery and functional organ tissue benefit following RBC transfusion2,3
� This effect also appears independent of the storage duration of the transfused red cells2-4.
� It has been demonstrated that Hb oxygen affinity is affected also by temperature, pH, and base excess, and it is the local in vivo environment with respect to these variables that may reduce the impact of the decreased 2,3-DPG2.
Important RBC storage lesion -depletion of 2,3 diphosphoglycerate(DPG) –Level is inversely proportional to theaffinity of hemoglobin for oxygen1
- Efficacy of Transfused RBC -
1. Chaplin H Jr, et. al. Current status of red-cell preservation and availability in relation to the developing national blood policy. N Engl J Med. 1974;291(2):68-74.2. Weiskopf RB, et. al. Fresh blood and aged stored blood are equally efficacious in immediately reversing anemia-induced brain oxygenation deficits in humans. Anesthesiology 2006;104(5):911-20.3 Walsh T, et. al. Does the storage time of transfused red blood cells influence regional or global indexes of tissue oxygenation in anemic critically ill patients? Crit Care Med 2004; 32(2):364–71.4. Roberson RS, et. al. Impact of transfusion of autologous 7- versus 42-day-old AS-3 red blood cells on tissue oxygenation and the microcirculation in healthy volunteers. Trans 2012;52(11):2459-64.

Between-Group Differences in 7-Day Change in MODS.
Steiner ME et al. Effects of Red-Cell Storage Duration on Patients Undergoing Cardiac Surgery. N Eng J Med2015;372:1419-1429.
- Efficacy of Transfused RBC –Recent (<10 days) vs. “Old” Blood (>21 days)

- Efficacy of Transfused RBC -
Steiner ME et al. Effects of Red-Cell Storage Duration on Patients Undergoing Cardiac SurgeryN Engl J Med 2015;372:1419-1429.
Primary and Secondary Outcomes.
Conclusions
The duration of red-cellstorage was not associatedwith significant differencesin the change in MODS.Wedid not find that thetransfusion of red cellsstored for 10 days or less wassuperior to the transfusion ofred cells stored for 21 days ormore among patients 12years of age or older whowere undergoing complexcardiac surgery

Yet - Current Strong Emphasis that �Restrictive Transfusion Practice is Beneficial
�Liberal Transfusion is Thereby Harmful
To the OR & ICU patient at the bedside – different
clinical settings:
i. Stable ICUii. Post-operativeiii. Recent hemorrhageiv. Under-resuscitatedv. Ongoing hemorrhagevi. Patient with severe organ
dysfunctionvii. Patient with ischemia

� Patients who died in ICU: lower hemoglobin
� Patients w/ anemia, APACHE II score > 20, and a cardiac diagnosis -significantly lower mortality rate following 1-6 PRBC
55% - no transfusions32-35% - 1 to 6 units
� Increasing Hgb in anemic cardiac patients - improved survival (OR = 0.80 for each 10 g/L increase, p = 0.012)
Retrospective: 4,470 critically ill patients
Hébert PC, et. al. Does transfusion practice affect mortality in critically ill patients? Transfusion Requirements in Critical Care (TRICC) Investigators and the Canadian Critical Care Trials Group. Am J Respir Crit Care Med. 1997 May;155(5):1618-23.
Conclusion: “anemia increases the risk of death incritically ill patients with cardiac disease. Bloodtransfusions appear to decrease this risk”
- Transfusion in Critical Care–Anemia & Cardiac Disease

� 30-day mortality was no different� Hospital mortality less (p=0.05)� 60-day mortality: no difference� ICU mortality: no difference� Restrictive group – lower
mortality only if –< 55 yrs, APACHE < 20 & no cardiac disease
TRICC Trial - 838 critically ill patientsRestrictive group: transfusion for Hgb <7Liberal group: transfusion for Hgb <10Primary Outcome: 30-day mortality
Hébert PC, et. al. Multicenter, randomized, controlled clinical trial of transfusion requirements in critical care. Transfusion Requirements in Critical Care Investigators, Canadian Critical Care Trials Group. N Engl J Med. 1999 Feb 11;340(6):409-17
- Liberal vs Restrictive Transfusion in Surgery -Anemia in Critical Illness vs Perioperative Period
Conclusion: “A restrictive strategy of red-cell transfusion is at least as effective as and possibly superior to a liberal transfusion strategy in critically ill patients, with the possible exception of patients with acute myocardial infarction and unstable angina.”
Alternative Conclusion: No difference amongst treatment groups.

Clinical
Trial
Patient
Population
Restrictive
Strategy
(Hb Trigger
- Target)
Liberal
Strategy
(Hb Trigger
- Target)
Reduction
in Blood
Utilization
Primary Outcome
EventRestrictive(Incidence)
Liberal(Incidence)
P
Hebert, et al, 19991
(n=838)Critically ill (adults)
7 to 8.5 g/dL 10 to 10.7 g/dL54% less RBC units transfused
30-day mortality 18.7% 23.3% 0.11
Hajjar, et al, 20103
(n=502)
Cardiac surgery (Adults)
8 to 9.1 g/dL10 to 10.5 g/dL
58% less RBC units transfused
Composite endpoint
•30-day mortality •Cardiogenic
Shock •ARDS •Acute renal injury
requiring dialysis
11%
6%9%2%4%
10%
5%6%1%5%
0.85
0.930.420.990.99
Carson, et al. 20115
(n=2,016)
Femur fracture(Elderly adults)
8.0 to 9.5 g/dL10.0 to 11.0 g/dL
65% less RBC units transfused
Composite endpoint
•60-day mortality •60-day Inability to
walk
34.7%
28.1%6.6%
35.2%
27.6%7.6%
NS
NSNS
Villanueva, et al, 20136
(n=921)
Gastrointestinal bleeding(Adults)
7 to 9.2 g/dL9 to 10.1 g/dL
59% less RBC units transfused
45-day all-cause mortality
5% 9%0.02
Table 1. Large Prospective Randomized Clinical Trials on Transfusion Triggers
Mirski MA, Frank SM, Kor DJ, Holmes DR Jr. The Spectrum of Restrictive and Liberal Red Cell Transfusion Strategies in Adult Patients – Reconciling Clinical Data with Best Practice . Critical Care 2015;19:202-12.
� Important !
� Trials on restrictive transfusion - documented the relative tolerance of lower hemoglobin levels in discrete patient cohorts
� Very same studies have largely failed to show actual physiological benefit over more liberal RBC transfusion practices.

- Correlation Between Transfusion & Adverse Effects -
� Data emanate - observational datasets
� Linked RBC transfusion with the risk for
� suppressive immunomodulation
� nosocomial infections
� ischemic complications
� acute kidney injury amongst others
� Aggregate of observational data do raise concern regarding these potential associations
� Pervasive risk for uncontrolled or unmeasured bias and confounding errors of analysis
� Observations may drive clinical impressions and protocols,but “research by association”must be interpreted with great caution
� In many cases, transfusion as a specific intervention merelyserves as a marker for increaseddisease complexity.

� Review of 203 trauma patients in TRICC Trial:� Primary endpoint: 30-day mortality
- Transfusion in Critical Care -Anemia & Trauma Patients
� No Difference Liberal vs Restrictive
Also No -– Increase MOD– Change ICU or hospital LOS– 30 or 60-day mortality – No difference in infection rates

Highest Level Clinical Studies
Adverse Effect Showing
Correlating Effect
Ref
Multi-System Organ Dysfunction Observational Studies 10,11
Nosocomial Infection Observational &Retrospective Studies
10, 12
Allergic or Immuno-modulation, Tumor Promotion
Observational &Retrospective Studies
13-15
Pulmonary Edema Level I RCT 1, 6
Pulmonary [Non-Edema] incl. ARDSObservational Studies 10, 16
Acute Kidney Injury Observational & Retrospective Studies
17, 18
Myocardial Ischemia Prospective Cohort 19, 20
Cerebral Ischemia Observational &Retrospective Studies
9, 19, 21
Shock Observational Study 10
Cardiac Arrest Prospective Cohorts 19, 20
Bleeding/Coagulopathy Observational Study 10
Table 2. Strength of Association Between Red Cell Transfusion and Purported Clinical Adverse Effects
Highest Level Study Reflects the rank order of scientific merit typically afforded to studies based on trial design. Highest to lowest: Prospective,randomized, clinical trial (RCT), Prospective subset analyses of randomized studies, Non-randomized Controlled Trials, Observational Case Series–
including prospective and retrospective cohort analysis, and consecutive and non-consecutive case series. ARDS– acute respiratory distress syndrome.
Mirski MA, Frank SM, Kor DJ, Holmes DR Jr. The Spectrum of Restrictive and Liberal Red Cell Transfusion Strategies in Adult Patients – Reconciling Clinical Data with Best Practice . Crit Care 2015;19:202-12.

Highest Level Clinical Studies
Adverse Effect Showing
Correlating Effect
Ref Showing No Correlation Ref
Multi-System Organ Dysfunction Observational Studies 10,11 Level I RCT 1
Nosocomial Infection Observational &Retrospective Studies
10, 12Level I RCT (2), RCT (1), RCT
Meta-Analysis2, 3, 6, 8
Allergic or Immuno-modulation, Tumor Promotion
Observational &Retrospective Studies
13-15 Level I RCT (2) 6
Pulmonary Edema Level I RCT 1, 6 Level I RCT (3), RCT Meta-Analysis 3, 5, 6, 8
Pulmonary [Non-Edema] incl. ARDSObservational Studies 10, 16 Level I RCT (3), RCT (1) 2, 3, 5, 6
Acute Kidney Injury Observational & Retrospective Studies
17, 18 Level I RCT (2), RCT (1) 2, 3, 6
Myocardial Ischemia Prospective Cohort 19, 20 Level I RCT (4), RCT (1) 1-3, 5, 6
Cerebral Ischemia Observational &Retrospective Studies
9, 19, 21Level I RCT (3), RCT (1), RCT
Meta-Analysis2, 3, 5, 6, 8
Shock Observational Study 10 Level I RCT 1, 3
Cardiac Arrest Prospective Cohorts 19, 20 Level I RCT 1, 3, 5
Bleeding/Coagulopathy Observational Study 10 Level I RCT 3
Table 2. Strength of Association Between Red Cell Transfusion and Purported Clinical Adverse Effects
Highest Level Study Reflects the rank order of scientific merit typically afforded to studies based on trial design. Highest to lowest: Prospective,randomized, clinical trial (RCT), Prospective subset analyses of randomized studies, Non-randomized Controlled Trials, Observational Case Series–
including prospective and retrospective cohort analysis, and consecutive and non-consecutive case series. ARDS– acute respiratory distress syndrome.
Mirski MA, Frank SM, Kor DJ, Holmes DR Jr. The Spectrum of Restrictive and Liberal Red Cell Transfusion Strategies in Adult Patients – Reconciling Clinical Data with Best Practice Crit Care 2015;19:202-12.

FINDINGS:2016 patients were enrolled and randomly assigned to the two treatment groups: 1007 to the liberal transfusion strategy and 1009 to the restrictive transfusion strategy.
“The median duration of follow-up was 3·1 years (IQR 2·4-4·1 years), during which 841 (42%) patients died. Long-term mortality did not differ significantly between the liberal transfusion strategy (432 deaths) and the restrictive transfusion strategy(409 deaths) (hazard ratio 1·09 [95% CI 0·95-1·25]; p=0·21).”
INTERPRETATION:“Liberal blood transfusion did not affect mortality compared with a restrictive transfusion strategy in a high-risk group of elderly patients with underlying cardiovascular disease or risk factors. The underlying causes of death did not differ between the trial groups. These findings do not support hypotheses that blood transfusion leads to long-term immunosuppression that is severe enough to affect long-term mortality rate by more than 20-25% or cause of death.”
- Long Term Adverse Effects of Transfusion?-Immunosuppression

From: Red Blood Cell Transfusion: A Clinical Practice Guideline From the AABB*Ann Intern Med. 2012;157(1):49-58. doi:10.7326/0003-4819-157-1-201206190-00429
Adverse effects of RBC transfusion contrasted with other risks. Risk is depicted on a logarithmic scale. Shaded bars represent the risk per RBC unit transfused, and unshaded bars represent the risk for fatality per person per year for various life events.

� Cardiac Disease
�Neurological Injury
�Peri-Operative Resuscitation
�Post-Operative Rehabilitation & Recovery
Anemia & Consequence in:
- RBC Transfusion -Peri-operative & Critical Care

- RBC Transfusion -Cardiac Disease


- RBC Transfusion -Cardiac Disease
� Hemoglobin as Fixed Variable – Not Transfusion
� Corresponding Ischemia Rates: 39.1% - 22.0% - 15.6% - 11.9%

- Transfusion & TBI -
� 76 Patients in TRICC Trial� Restrictive (Hgb 7-9) vs Liberal (10-12)
Results -– 30-day all-cause mortality rates:
Restrictive group - 17%Liberal group - 13%
– No change MOF– Same ICU & hospital LOS
McIntyre LA, Fergusson DA, Hutchison JS, Pagliarello G, Marshall JC, Yetisir E, Hare GM, Hébert PC. Effect of a liberal versus restrictive transfusion strategy on mortality in patients with moderate to severe head injury. Neurocrit Care. 2006;5(1):4-9.
Conclusion: “We were unable to detect significant improvements in mortalitywith a liberal as compared to restrictive transfusion strategy in critically illtrauma victims with moderate to severe head injury.”

- Transfusion & TBI -
� 200 patients� Restrictive (Hgb > 7) vs Liberal
(>10)� With or without EPO
Results -– 6- month neuro outcome
scores:No difference between all 4 groups
– Range Hgb 9-12 both groups.– Increase thrombotic risk in
Hbg >10 Group

- Transfusion & TBI -

� Lower PbtO2 [19.9 vs 27.2] (p=0.02)
� Increased LPR: 36 vs 29 (p=0.16)
� Increased brain hypoxia: 52% vs 21% (p<0.01)
- Hemoglobin & SAH –Cerebral Metabolism
20 SAH patients retrospective studyMonitoring – ICP, PbtO 2, microdialysisHgb < 9g/dL correlated with:
Oddo M, et. al. Hemoglobin Concentration and Cerebral Metabolism in Patients With Aneurysmal Subarachnoid Hemorrhage. Stroke 2009;40:1275 -1281.
Conclusion: “A Hgb concentration <9 g/dL is associated with an increased incidence of brain hypoxia and cell energy dysfunction in patients with poor-grade subarachnoid hemorrhage. ”

� Improved overall outcome (MRS) at 14d & 3 mo
� Reduced angiographic vasospasm
� Reduced risk of vasospasm induced infarction
- Transfusion Following SAH –
103 SAH patients; logistic regressionHigher Hgb correlated with -
Naidech AM, et. al. Higher hemoglobin is associated with less cerebral infarction, poor outcome, and death after subarachnoid hemorrhage. Neurosurgery. 2006 Oct;59(4):775-9.Naidech AM, et. al. Higher hemoglobin is associated with improved outcome after subarachnoid hemorrhage. Crit Care Med. 2007 Oct;35(10):2383-9.
Conclusion: “We found that SAH patients with higher initial andmean Hgb values had improved outcomes. Higher Hgb in SAHpatients may be beneficial….and may warrant further study”

� Anemia - 144 of 546 patients (26%) on admission
� PRBC transfusion - 100 patients (18%) during 1st 5 day
� Univariate 30-day mortality [anemia, age, glucose,
anticoagulation, GCS, hematoma volume, hematoma location,
IVH, and DNR] : transfusion improved survival at 30 days (odds
ratio: 2.76; 95%, 1.45-5.26; P = .002)
- Transfusion Following ICH -
Five hundred forty-six consecutive subjects were identified from an ongoingsingle-center, prospective cohort study of non-traumatic ICH over a 6-year period.
Conclusion: “PRBC transfusion was associated with improved outcome inthese patients.”

Villanueva C et al. N Engl J Med 2013;368:11-21.
“Death was due to unsuccessfully controlled bleeding in 3 patients (0.7%) in the restrictive-strategy group and in 14 patients (3.1%) in the liberal-strategy group (P=0.01).
RBC Transfusion During
Active Hemorrhage

Effects of Intravenous Fluid Restriction
on Postoperative Complications
• Brandstrup B, et. al., Danish Study Group on Perioperative Fluid Therapy.
OBJECTIVE: To investigate the effect of a restricted intravenous fluid regimen versus a standard regimen on complications after colorectal resection.
• SUMMARY BACKGROUND DATA: Associations between postoperative weight gain and poor survival as well as fluid overload and complications have been shown.
• METHODS: We did a randomized observer-blinded multicenter trial. After informed consent was obtained, 172 patients were allocated to either a restricted or a standard intraoperative and postoperative intravenous fluid regimen. The restricted regimen aimed at maintaining preoperative body weight; the standard regimen resembled everyday practice. The primary outcome measures were complications; the secondary measures were death and adverse effects.
• RESULTS: The restricted intravenous fluid regimen significantly reduced postoperative complications both by intention-to-treat (33% versus 51%, P = 0.013) and per-protocol (30% versus 56%, P = 0.003) analyses.The numbers of both cardiopulmonary (7% versus 24%, P = 0.007) and tissue-healing complications (16% versus 31%, P = 0.04) were significantly reduced. No patients died in the restricted group compared with 4 deaths in the standard group (0% versus 4.7%, P = 0.12). No harmful adverse effects were observed. CONCLUSION: The restricted perioperative intravenous fluid regimen aiming at unchanged body weight reduces complications after elective colorectal resection

Transfusion Requirements in Surgical Oncology Patients: A Prospective, Randomized Controlled Trial Anesthesiology. 2015;122(1):29-38.
Transfusion Requirements in Surgical Oncology Patients: A Prospective, Randomized Controlled Trial Anesthesiology. 2015;122(1):29-38.
Characteristics Related to the Underlying Malignancies of Patients and Types of Surgical Procedure
- Transfusion in Peri-Operative Critical Care–
2015

Transfusion Requirements in Surgical Oncology Patients: A Prospective, Randomized Controlled Trial Anesthesiology. 2015;122(1):29-38.
Transfusion Requirements in Surgical Oncology Patients: A Prospective, Randomized Controlled Trial Anesthesiology. 2015;122(1):29-38.
Outcome MeasuresHemoglobin Concentrations and Erythrocyte Transfusions

Transfusion Requirements in Surgical Oncology Patients: A Prospective, Randomized Controlled Trial Anesthesiology. 2015;122(1):29-38.
Transfusion Requirements in Surgical Oncology Patients: A Prospective, Randomized Controlled Trial Anesthesiology. 2015;122(1):29-38.
Kaplan–Meier curves showing the probability of 30-day survival in patients randomized to a restrictive strategy of erythrocyte transfusion (transfusion when hemoglobin concentration <7 g/dl) and those randomized to a liberal strategy (transfusion when hemoglobin concentration <9 g/dl). The P value of <0.005 was calculated with the use of the log-rank test.

Figure 2. Subgroup Analyses.The gray vertical lines represent the overall treatment estimate (solid line) andthe 95% confidence interval (dashed lines) for the primary outcome ascalculated for the entire analysis cohort. The sizes of the circles designating thepoint estimates reflect the sizes of the subgroups.
The restrictive transfusion threshold for hemoglobin was less than 7.5 g perdeciliter, and the liberal transfusion threshold was less than 9 g per deciliter.CABG denotes coronary-artery bypass grafting, COPD chronic obstructivepulmonary disease, GFR glomerular filtration rate, and LV left ventricular.
- Transfusion in Critical Care–Cardiac Surgery Trial - 2015

� Independent risk factor – poor outcome
� increased mortality, functional dependence, impaired cognition, re-admission to the hospital, and falls1-3
� Prospective study 2004 (1,156 patients >65 yr-old) -evaluated in 6 basic and 8 instrumental activities of daily living (IADLs):
Anemia (Hb<12.0 g/dL) - poorer performance and strength 4.
� Following orthopedic surgery - functional rehabilitation & recovery are impaired and the duration of rehabilitation prolonged in patients with anemia (Hb < 10 g/dL)5
� Functional Outcomes in Cardiovascular Patients Undergoing Surgical Hip Fracture Repair (FOCUS) trial - liberal transfusion strategy offered no benefit in terms of reducing mortality or the ability to ambulate (10 feet or across the room) without assistance6.
Primary functional outcome of walking (using the investigators’ criteria) may not, however, be a robust test of endurance.
- Anemia in the Elderly -
1. Balducci L. Anemia, fatigue and aging. Transfus Clin Biol 2010;17(5-6):375-81.2. Terekeci HM, et. al. Relationship between anaemia and cognitive functions in elderly people. Eur J Intern Med 2010;21(2):87-90.3. Chaves PH, et al. What constitutes normal hemoglobin concentration in community dwelling disabled older women?J Am Ger Soc 2004;52(11):1811–6.4. Penninx BW, et. al. Anemia is associated with disability and decreased physical performance and muscle strength in the elderly. J Am Geriatr Soc 2004;52(6):719-24.5. Foss NB, et. alAnaemia impedes functional mobility after hip fracture surgery. Age Ageing 2008;37(2):173-8.6. Carson JL,et. al; FOCUS Investigators. Liberal or restrictive transfusion in high-risk patients after hip surgery. N Engl J Med 2011;365(26):2453-62. .

Causes of death: 30-90 postoperative days in 284 elderly hip fracture patients Cause of Deaths -Restrictive strategy (Hg transfusion trigger <9.7 g/dL, n = 40) vs. Liberal strategy (Hg <11.3, n = 30)
Overall 30-days - p-value 0.03Nursing Home Residents 30 & 90 days – p<0.01Sheltered residents 30 or 90-days - NS
Postoperative Blood Transfusion Strategy in Frail, Anemic Elderly Patients with Hip Fracture - The TRIFE Randomized Controlled Trial
Gregersen M, Borri LCs, Damsgaard EM. Acta Orthopaedica 2015;86:363-72

J Am Med Dir Assoc.2015 Apr 28.Blood Transfusion and Overall Quality of Life After Hip Fracture in Frail Elderly Patients-The Transfusion Requirements in Frail Elderly Randomized Controlled Trial.Gregersen M Borris LC Damsgaard EM
BACKGROUND: We examined possible associations between different red blood cell (RBC) transfusion strategies, overall quality of life (OQoL), and recovery of activities of daily living (ADL) in operated frail elderly hip fracture patients, and the possibility that OQoL was related to ADL recovery.
METHODS: A prospective, assessor-blinded, randomized controlled trial was carried out among 157 elderly residents (≥65 years) from nursing homes and sheltered housing facilities with Mini-Mental State Examination scores ≥5 points. Patients were assigned to either a restrictive RBC transfusion strategy [hemoglobin (Hb) < 9.7 g/dL, 6 mmol/L] or a liberal strategy (Hb < 11.3 g/dL, 7 mmol/L) during the first 30 days after surgery. An interview-based questionnaire, the depression list (DL) assessing OQoL, and the modified Barthel Index (MBI) assessing ADL performance, were conducted on day 30 and 1 year after hip fracture surgery. Sum-scores of DL, MBI, and their changes from day 30 until 1 year (expressing recovery) were compared between RBC transfusion groups. Possible associations between changes of DL and MBI sum-scores were tested for across total patient population.
RESULTS: There was no association between OQoL and RBC transfusion strategies on day 30 or at 1 year. The DL sum-score changes were similar for both groups, (ie, 1.06 points) [95% confidence interval (CI) -0.62, 2.76)] P = .21. The MBI sum-scores increased at 1 year following the liberal transfusion strategy (ie, by 6.86 points) (95% CI 0.41, 13.3) P = .03. Recoveries of OQoL and ADL were associated: β = -0.06 (95% CI -0.11, -0.01) P = .02.
CONCLUSIONS: According to our Hb threshold criteria, OQoL and RBC transfusion strategies for frail elderly hip fracture patients are not associated. However, for survivors with less severe dementia, ADL recovery after 1 year is greater following a liberal transfusion strategy than a restrictive strategy. OQoL progress and ADL recovery were associated.

OBJECTIVES:It is still under debate that red blood cell (RBC) transfusions might increase the risk of healthcare-associatedinfections after hip fracture surgery. Previously, we found that a liberal RBC transfusion strategy improved survivalin nursing home residents. Our aim, therefore, wasto investigate whether a more liberal RBC transfusion strategywas associated with a higher infection risk in frail elderly hip fracture patients.
DESIGN:Prospective, assessor-blinded, randomized and controlled trial. 284 consecutively hospital-admitted elderly with hipfracture from nursing homes or sheltered housing facilities were included. A restrictive RBC transfusion strategy(hemoglobin <9.7 g/dL; 6 mmol/L) compared with a liberal strategy (hemoglobin <11.3 g/dL; 7 mmol/L)administered within 30 days after surgery. Leukocytes and C-reactive protein (CRP) in repeated blood sampleswithin 30 days, and number of all infections (pneumonia, urinary tract infection, and other infections) within10 days.
RESULTS:88 % of the patients received a RBC transfusion. A median of 1 RBC unit (interquartile range (IQR): 1-2) wastransfused for the restrictive strategy group versus 3 RBC units (IQR: 2-5) for the liberal group. Leukocytes andCRP measurements were similar for both groups. Rates of infection were 72 % for the restrictive group comparedto 66 % for the liberal group (risk ratio 1.08; 95 % confidence interval 0.93-1.27, p value 0.29).
CONCLUSIONS:A more liberal RBC transfusion strategy was not associated with higher risk of infection among residents fromnursing homes or sheltered housing undergoing hip fracture surgery.
Blood transfusion and risk of infection in frail elderly after hip fracture surgery: the TRIFE randomized controlled trial.
Gregersen M, Damsgaard EM, Borris LC. Eur J Orthop Surg Traumatol. 2015 Feb 18.

At an academic level, a multidisciplinary “think tank” from the US National Heart,Lung, and Blood Institute (NHLBI) convened in 2011 and agreed to 10 transfusion-related concepts deemed most important to examine in the near term and includedamong them were multiple trials evaluating RBC transfusion trigger strategies toimprove overall outcome. Specific recommendations included the need for threeadult trials designed to validate the following primary hypotheses:
� Higher Hb levels resulting from a liberal transfusion strategy during cardiopulmonarybypass surgery will lead to lower incidence of 30-day all-cause mortality;
� In patients with acute coronary syndrome or coronary artery disease undergoing cardiaccatheterization, a liberal transfusion strategy will be associated with a lower incidence ofcomposite outcome of all-cause mortality at 30 days;
� In hemodynamically stable patients in the ICU, with a history of ischemicheart disease,multiple organ dysfunction scores will be improved by maintaining the hemoglobingreater than 10 g/dL.
- Research Initiatives -

- 2012 AABB Clinical Guideline -
� Restrictive transfusion strategy (7-8 g/dL) in hospitalized, stable patients.
� No recommendation - for or against a liberal or restrictive transfusion strategy for hospitalized patients with acute coronary syndrome or neurological patients.
� No recommendation – during active hemorrhage
� No recommendation – during peri-operative period

Summary
� Restrictive therapy - tolerated in low complexity ICU or non-hemorrhagic surgical patients
� Liberal therapy – not worse than restrictive by trial evidence
� Optimal homeostasis
� Suggest Hgb higher (≥ 9.5-10) when risk ischemia for Cardiac & Neuro
� Balance between blood product & crystalloid
� Maintenance of adequate BP (perfusion) is equally vital

Questions?




� Transfusion at each level increased Pbto2
� No change in L/R ration or brain pH
- Transfusion Following TBI –Cerebral Oxygenation
Zygun DA, Nortje J, Hutchinson PJ, Timofeev I, Menon DK, Gupta AK. The effect of red blood cell transfusion on cerebral oxygenation and metabolism after severe traumatic brain injury. Crit Care Med. 2009 Mar;37(3):1074-8.
Conclusion: “Transfusion of packed red blood cells acutely results inimproved brain tissue oxygen without appreciable effect on cerebralmetabolism”
30 TBI patients; randomization to Hgb 8, 9, or 10 –Each group transfused if Hgb < thresholdMonitored brain pH, Pbto2, L/P ratio

� 15% rise in Hgb� 18% rise in DO2� Global CBF unchanged� Reduced O2 extraction
- Transfusion Following SAH –Increase in Brain Oxygen
8 SAH patients w/ O15 PET, Tx 1 u PRBCTransfusion correlated with -
Dhar R, Zazulia AR, Videen TO, Zipfel GJ, Derdeyn CP, Diringer MN. Red blood cell transfusion increases cerebral oxygen delivery in anemic patients with subarachnoid hemorrhage. Stroke. 2009 Sep;40(9):3039-44. Epub 2009 Jul 23.
Conclusion: “Transfusion of red blood cells to anemic patients withsubarachnoid hemorrhage resulted in a significant rise in cerebral DO2without lowering global CBF.”

� Medical complications –46% in patients receiving PRBC30% in non-PRBC transfused patients
� Infections rate higher – CNS & systemic� Mechanical ventilation� Reduced O2 extraction� But not mortality or outcome
- Transfusion Following SAH –
421 SAH patients; logistic regressionTransfusion correlated with -
Levine J, Kofke A, Cen L, Chen Z, Faerber J, Elliott JP, Winn HR, Le Roux P. Red blood cell transfusion is associated with infection and extracerebral complications after subarachnoid hemorrhage. Neurosurgery. 2010 Feb;66(2):312-8.
Alternative Conclusion: PRBC - a marker for more complex patients.
Conclusion: “These data suggest that RBCTs are associated with medicalcomplications after SAH. However, the data do not infer causation...”