Embed Size (px)
Citation preview

Kim et al
Achieving an optimal esthetic result when replacing missing teeth with implant-supported restorations in the esthetic zone is a demanding surgical and restorative challenge. This clinical report describes the use of a cantilevered, ce-mented, implant-supported restoration with gingiva-colored ceramics and a circumferential pressure-ridge lap pontic to replace 2 incisors and the adjacent tissue. (J Prosthet Dent 2010;104:71-76)
Restoration using gingiva-colored ceramic and a ridge lap pontic with circumferential pressure: A clinical report
Tae Hyung Kim, DDS,a Domenico Cascione, CDT, BS,b Alena Knezevic, DDS, PhD,c and Hessam Nowzari, DDS, PhDd
University of Southern California, Herman Ostrow School of Dentistry of USC, Los Angeles, Calif; School of Dental Medicine, University of Zagreb, Zagreb, Croatia
aAssistant Professor, Division of Restorative Science, Chair of Removable Section, University of Southern California, Herman Os-trow School of Dentistry of USC.bAdjunct Faculty Clinical Assistant Professor, Division of Restorative Science, University of Southern California, Herman Ostrow School of Dentistry of USC.cResearch Associate, University of Southern California, Herman Ostrow School of Dentistry of USC; Assistant Professor, Depart-ment of Endodontics and Restorative Dentistry, School of Dental Medicine, University of Zagreb.dProfessor, Clinical Dentistry, and Director, Advanced Periodontics, University of Southern California, Herman Ostrow School of Dentistry of USC.
Missing anterior teeth, especially those adjacent to each other, pres-ent a difficult esthetic challenge, and multiple surgical and restorative pro-cedures may be required to achieve an acceptable esthetic outcome. For many years, using adjacent implants for the replacement of lost anterior teeth was a common procedure.1,2 However, while it is possible to place adjacent implants in central and later-al positions, or lateral and canine po-sitions, it can be difficult to maintain 3 mm of space between their plat-forms, as recommended in the litera-ture.1 This can pose a significant risk of loss of the interproximal crest of bone between the implants over time and a subsequent loss of papillary height.1 Furthermore, the discrepancy in papillae height is more noticeable if papillary height is lost between the central and lateral on one side, while natural teeth remain intact on the contralateral side. Different types of pontic designs and their relationship with the residual ridge have been de-
scribed in the literature.3-7A solution suggested by Spear,1,3 to use a cantile-ver pontic connected to a central inci-sor or a canine implant, is esthetically more predictable and functionally as acceptable as adjacent implants.
Deficiencies in the soft tissue anat-omy and residual ridge defects can compromise esthetics and oral hy-giene as well.8 Surgical modification of soft tissue areas and residual ridge defects often results in improved es-thetics and is frequently included in preprosthetic treatment.9,10 However, alternative treatment options must also be considered. Previously, auto-polymerizing acrylic resin and flexible silicone materials were occasionally used to mask soft tissue defects,9,11,12 but they have been replaced by gin-giva-colored ceramics that provide superior esthetics.13-17 The method of using gingiva-colored ceramics works well when there are missing anterior teeth and extreme residual ridge re-sorption. The soft tissue responds well to these ceramic restorations if
the patient cleanses as instructed.16 This clinical report describes the res-toration of lateral and central incisors and the adjacent gingiva using a can-tilevered, single implant, fixed partial denture (FPD) with gingiva-colored ceramic.
CLINICAL REPORT
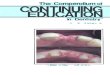
A 29-year-old woman who lost her maxillary right central and lateral incisor in a baseball-related accident when she was young presented to the Oral Health Center at the University of Southern California for treatment. She was referred by her dentist, and at the time of referral, she had a provi-sional restoration consisting of a 3.75 mm x 11.5-mm machined surface implant (Brånemark System, external connection; Nobel Biocare AB, Göte-borg, Sweden) placed in the maxillary right lateral incisor location, with a cantilevered crown on the maxillary right central incisor (Fig. 1). The im-plant was positioned buccally, which

72 Volume 104 Issue 2
The Journal of Prosthetic Dentistry Kim et al
resulted in further bone resorption in the labial aspect. The long axis of the implant and the screw access chan-nel were located on the buccal aspect of the desired tooth contour (Fig. 2). This increased the level of difficulty in achieving an esthetically appealing outcome.
The treatment options for this pa-tient were discussed during the first visit. Possible treatment alternatives included a fixed partial denture or re-movable partial denture. Since the pa-tient had an implant in the maxillary right lateral incisor position, another treatment option was to apply a bone graft, due to the bony defect in the position of the maxillary right central incisor, place an additional implant, and fabricate 2 single crowns. How-ever, the patient declined all of the ini-tially recommended options, refusing further tooth preparation and bone grafting as she had already under-gone bone grafting to reconstruct the defect. The most acceptable solution was restoration using gingiva-colored ceramic and a ridge lap pontic with circumferential pressure.
A completed diagnostic waxing (S-U-SHADE-SET Wax, no. 5 intensive white; Schuler-Dental, Ulm, Germany) of the teeth and gingiva determined how much tissue conditioning was needed at the pontic site to meet the esthetic needs (Fig. 3).14 The waxing was accom-plished after implant placement be-cause the residual ridge augmentation and implant surgery occurred prior
to the patient referral. To initiate the diagnostic waxing, an impression (Ex-trude Extra; Kerr Corp, Orange, Calif ) was made with an implant impres-sion coping in an open tray. The im-pression was poured in type IV white dental stone (GC Fujirock, ISO 6873; GC Europe NV, Leuven, Belgium). The impression of the opposing arch was made in reversible hydrocolloid (Identic Dust Free Alginate; Dux Den-tal, Oxnard, Calif ) and poured in type IV white dental stone (GC Fujirock; GC Europe NV). When the diagnos-tic waxing was completed, the cast was duplicated using a light-viscosity silicone (Elite Double 22; Zhermack, Inc, Eatontown, NJ). The silicone was placed into a plastic bowl (Wamix-3M; Wassermann Dental-Maschinen GmbH, Hamburg, Germany) in a 1:1 mixing ratio of base to catalyst. Then the bowl with silicone was placed in the vacuum mixer (Wamix-3M; Was-sermann Dental-Maschinen GmbH), and the silicone was mixed under vac-uum conditions for 48 seconds.
Following polymerization of the silicone, type IV white dental stone (GC Fujirock EP; GC Europe NV) was poured into the silicone and the mixture was placed in a pressure pot (Polymat; Reitel Feinwerktechnik GmbH, Bad Es-sen, Germany) at 60 psi to avoid any air inclusion. The type IV white dental stone was used to create a new cast inside the duplicated silicone. A sili-cone index (Platinum 85; Zhermack, Inc) was fabricated on this new dupli-
cated cast to allow the dental labora-tory technician to evaluate the space availability for the fixed partial denture design. A propelling pencil (Staedtler, Inc, Chatsworth, Calif ) with a graph-ite diameter of 0.4 mm was used to mark the outline of the waxing on the definitive cast (Fig. 3). After the wax was removed from the cast using hot water, the pontic site of the fixed par-tial denture was exposed on the cast. Then the cast was scored following the pencil markings by trimming the stone using a no. 8 round carbide ro-tary cutting instrument (H1, size 023; Brasseler USA, Savannah, Ga), and the entire circumference was cut to a 1-mm depth uniformly. The same rotary cutting instrument was used to smooth and blend other areas of the pontic site. A scalpel (Multi-pur-pose instrument; Renfert USA, St. Charles, Ill) was used as a finishing step to smooth the pontic area (Fig. 4).14 The shape of the pontic was de-signed to capture the anatomical and architectural contours of the tissue.
A provisional plastic abutment (Brånemark System Temporary Abut-ment, Plastic Engaging; Nobel Biocare AB) in acrylic resin (Enamel Plus Temp; Gruppo Micerium SpA, Avegno, Italy) was made, and a cementable crown from the same acrylic resin was used for the provisional restoration (Fig. 5).14 Since the incisal-gingival dimen-sion of the lateral incisor extended be-yond the natural clinical crown length of a lateral incisor (Fig. 6), a ceramic/
1 Condition of maxillary arch at time of referral. 2 Long axis of implant and facially oriented screw access channel.

73August 2010
Kim et al
acrylic resin gingival substitute (ENA HFO Tender Pink, Intro Kit; Gruppo Micerium SpA) was used to correct the tissue defect. During placement of the provisional restoration, pressure was applied on the pontic site (Fig. 7). The provisional restoration was slow-ly seated in place with finger pressure over a 15- to 20-minute period to al-low the tissue of pontic site to adjust to the pressure. Controlled pressure on the pontic site enhances the inter-dental papilla and creates the illusion of pontics emerging from the soft tis-sue, thus creating a natural-looking effect of the cantilevered restoration on the central incisor (Fig. 8).14 The rationale for using a 15- to 20-minute time period was to slowly contour the pontic receptor area where the 1-mm revision of the cast initially prevented the provisional fixed partial denture
from seating completely. Subjective tools, such as diagnos-
tic waxing and provisional restora-tions,4,14,18 were used to predict the out-come of the definitive restorations for this esthetically demanding patient. The definitive restoration simply replicated the approved provisional restoration. A zirconia abutment (Procera; Nobel Bio-care USA, Yorba Linda, Calif) was used for the definitive restoration. The sur-face of the zirconia abutment (Procera; Nobel Biocare USA) was prepared to receive the gingiva-colored ceramic (SNF PressCeram Zirconia; Swiss NF Metals, Inc, Toronto, Canada) (Fig. 9).14 The gingiva-colored ceramic was added to the abutment, in contrast to the provisional restoration for which pink acrylic resin (ENA HFO Tender Pink, Intro Kit; Gruppo Micerium SpA) was added onto the crown. In
this manner, the restoration margin was located supragingivally, which facilitated the removal of excess ce-ment19 (Fig. 10). A compressible ce-ramic fixed partial denture layered over a zirconia abutment (Procera; Nobel Biocare USA) was used to fabricate the definitive restoration, which was cemented with a restor-ative composite resin material (ENA HFO; Gruppo Micerium SpA). The laboratory procedures were previous-ly described.14 The gingival tissue at the pontic site was successfully con-toured by the provisional restoration (Fig. 10), which allowed the definitive restoration to fit precisely. Due to the use of gingiva-colored ceramic and a circumferential pressure-ridge lap pontic, the clinical outcome of the definitive restoration met the expec-tations of the patient (Fig. 11).14
5 Custom abutment pattern developed with acrylic resin.14 (Figure reproduced with permission from Spec-trum Dialogue.)
6 Cervical margin of lateral incisor positioned apically compared to contralateral side.
3 Marking pontic periphery of diagnostic waxing with pencil.14 (Figure reproduced with permission from Spec-trum Dialogue.)
4 Scored pontic area; pontic site designed to obtain anatomical gingival contour.14 (Figure reproduced with permission from Spectrum Dialogue.)

74 Volume 104 Issue 2
The Journal of Prosthetic Dentistry Kim et al
to achieve lasting, predictable results from the definitive restoration.
DISCUSSION
Among various techniques report-ed to improve soft tissue deficiency are the use of a gingiva-colored, acrylic
resin facade, flexible, silicone-based, tissue-colored material, or remov-able prostheses.9,12 The loss of periim-plant tissue can also be corrected by applying gingiva-colored ceramic on the cervical portion of implant-sup-ported metal ceramic restorations.9 However, achieving harmonious mu-
9 Gingiva-colored ceramic on zirconia abutment.14 (Figure reproduced with permission from Spectrum Dialogue.)
7 Pressure applied on pontic site during placement of provisional restoration.
10 Supragingival margin of custom abutment. Note pon-tic site conditioning.
11 Definitive prosthesis.14 (Figure reproduced with per-mission from Spectrum Dialogue.)
8 Natural appearance of central incisor pontic.14 (Figure reproduced with permission from Spectrum Dialogue.)
This restoration has been in place for 19 months, and no postinsertion complications have been noted. How-ever, due to the specific design of the restoration, it is important that prop-er oral hygiene be maintained and that the condition of the restoration and periimplant tissue be monitored

75August 2010
Kim et al
cogingival contours may be enhanced by the application of gingiva-colored ceramic to the cervical collars of cus-tomized ceramic implant abutments, as described in this clinical report. Another advantage of the described technique is the repositioning of the cement interface between the abut-ment and the restoration away from the tissues. The excess cement on the margins of a restoration may be dif-ficult to remove completely, which can result in an unfavorable effect on periimplant tissue.19 Therefore, the approach described facilitates easier, more complete cement removal.
When the gingiva-colored ceramic is applied to the crown, the cervical extension of porcelain toward gingival embrasure spaces may be limited by the path of insertion of the crown and adjacent teeth.15 In contrast, the ap-plication of gingiva-colored ceramic on a customized abutment allows a gingival embrasure space to be filled where interproximal papillae are miss-ing and allows for the creation of a natural appearance, as well as fewer limitations from the contours of the adjacent teeth. In the situation present-ed, the esthetics were also improved by using a pontic with controlled pressure on the pontic site to enhance the inter-dental papilla and create the illusion of a pontic emerging from the soft tissue. It is suggested in the literature that the intaglio surface of the pontic should be convex, smooth, and well polished, with no-pressure contact points to allow proper cleaning.8,10 For the patient pre-sented in this clinical report, a concave pontic gingival surface was formed. However, a concave pontic surface does not allow appropriate cleansing of the gingival surface of the pontic. Also, no flossing is possible under the pontic due to the amount of pressure applied. Nevertheless, the applied pressure seemed to create a seal that theoretically could prevent plaque ac-cumulation and plaque retention un-der the pontic.4
Plaque control was performed at each recall visit, and no visible signs of inflammation under or around the
pontic were observed for the 8-month period during which the patient wore the provisional restoration. A signifi-cant advantage of the method de-scribed is that pressure, rather than invasive tissue modification, is used to achieve the desired tissue readap-tation. The most favorable outcome is obtained when pressure is applied to thick tissue; therefore, tissue volume should be adequate to compress the tissue 1 mm without any surgical in-tervention. During placement of the restoration using pressure, the clini-cian may meet resistance from the soft tissue, followed by an ischemic blanching reaction, which is transi-tory in most situations.10 The pon-tic site should be observed until the blanching has disappeared, prior to discharging the patient, as a readjust-ment of the region to which pressure was applied may be needed. Pressure applied by provisional restorations enables controlled displacement of the soft tissue, allowing the desired soft tissue contour to be created.
Kim et al4 previously described a similar procedure for using a provi-sional restoration to change the tissue contour. In that situation, a screw-retained provisional restoration was used to alter the tissue contour. For the patient described in this report, a cementable provisional restoration was used to contour the tissue. Due to tissue resiliency, the cementable provisional restoration must be held continuously during insertion to re-tract the tissue. The provisional resto-ration should be held in position until the tissue is readapted. However, the screw-retained restoration does not need to be maintained in position during insertion in the procedure de-scribed by Kim et al.4
An additional advantage of the method described in this clinical re-port is the use of a single implant in-stead of 2 adjacent implants to avoid higher interdental bone resorption, which occurs when 2 adjacent im-plants are placed.3
SUMMARY
A technique involving use of a single implant with a circumferential pressure-ridge lap pontic to replace 2 missing anterior teeth, and a nonsur-gical approach for the management of soft tissue deficiencies in the im-plant site, was described. Controlled pressure was used on the pontic site to enhance the interdental papilla and create the illusion of pontics emerg-ing from the soft tissue, thus creating a natural-looking effect of the can-tilevered restoration on the central incisor. Gingiva-colored dental por-celain was added on the abutment to replace the missing gingival tissue, which further improves the esthetic outcome of the definitive restoration.
REFERENCES
1. Spear FM. The use of implants and ovate pontics in the esthetic zone. Compend Contin Educ Dent 2008;29:72-4, 76-80.
2. Grunder U. Stability of the mucosal topography around single-tooth implants and adjacent teeth: 1-year results. Int J Peri-odontics Restorative Dent 2000;20:11-7.
3. Spear F. Implants or pontics: decision mak-ing for anterior tooth replacement. J Am Dent Assoc 2009;140:1160-6.
4. Kim TH, Cascione D, Knezevic A. Simulated tissue using unique pontic design: a clinical report. J Prosthet Dent 2009;102:205-10.
5. Abrams L. Augmentation of the deformed residual edentulous ridge for fixed pros-thesis. Compend Contin Educ Gen Dent 1980;1:205-13.
6. Liu CL. Use of a modified ovate pontic in areas of ridge defects: a report of two cases. J Esthet Restor Dent 2004;16:273-83.
7. Stein RS. Pontic-residual ridge relation-ship: a research report. J Prosthet Dent 1966;16:251-85.
8. Tripodakis A, Constandtinides A. Tissue response under hyperpressure from convex pontics. Int J Perodontics Restorative Dent 1990;10:408-14.
9. Garcia LT, Verrett RG. Metal-ceramic restorations--custom characterization with pink porcelain. Compend Contin Educ Dent 2004;25:242, 244, 246.
10.Jacques LB, Coelho AB, Hollweg H, Conti PC. Tissue sculpturing: an alternative method for improving esthetics of anterior fixed prosthodontics. J Prosthet Dent 1999;81:630-3.
11.Cura C, Saraçogulu A, Cötert HS. Alter-native method for connecting a remov-able gingival extension and fixed partial denture: a clinical report. J Prosthet Dent 2002;88:1-3.

76 Volume 104 Issue 2
The Journal of Prosthetic Dentistry Kim et al
12.Greene PR. The flexible gingival mask: an aesthetic solution in periodontal practice. Br Dent J 1998;184:536-40.
13.Hannon SM, Colvin CH, Zurek DJ. Selec-tive use of gingival-toned ceramics: case reports. Quintessence Int 1994;25:233-8.
14.Cascione D, Nowzari H, Kim TH. Simulated tissue in modern implant dentistry. Spec-trum Dialogue 2008;7:64-76.
15.Kamalakidis S, Paniz G, Kang KH, Hi-rayama H. Nonsurgical management of soft tissue deficiencies for anterior single implant-supported restorations: a clinical report. J Prosthet Dent 2007;97:1-5.
16.Goldstein RE. Esthetics in dentistry: prin-ciples, communications, treatment meth-ods, vol. 1. 2nd ed. Hamilton: B.C. Decker Canada; 1998. p.133-86.
17.Rhoads JE, Rudd KD, Morrow RM. Dental laboratory procedures: fixed partial dentures, vol. 2. St. Louis: Mosby; 1985. p.122-39.
18.Reshad M, Cascione D, Magne P. Di-agnostic mock-ups as an objective tool for predictable outcomes with porcelain laminate veneers in esthetically demanding patients: a clinical report. J Prosthet Dent 2008;99:333-9.
19.Gapski R, Neugeboren N, Pomeranz AZ, Reissner MW. Endosseous implant failure influenced by crown cementation: a clinical case report. Int J Oral Maxillofac Implants 2008;23:943-6.
Corresponding author:Dr Tae Hyung KimUniversity of Southern CaliforniaHerman Ostrow School of Dentistry of USC925 W 34th StLos Angeles, CA 90089-0641Fax: 213-740-1524E-mail: [email protected]
AcknowledgementsThe authors thank Odena Chinchilla, CDT, for help in writing the lab procedures; Randy J. Phillips, BA, DDS, and Flavia Panduru, Herman Ostrow School of Dentistry of USC, University of Southern California, Los Angeles, for proofreading; and Gruppo Micerium SpA, Avegno, Italy, and Zhermack, Inc, Eatontown, NJ, for the donation of materials.
Copyright © 2010 by the Editorial Council for The Journal of Prosthetic Dentistry.
Noteworthy Abstracts of the Current Literature
Clinical outcome of three-unit lithium-disilicate glass-ceramic fixed dental prostheses: up to 8 years results
Wolfart S, Eschbach S, Scherrer S, Kern M.Dent Mater 2009;25:e63-71. Epub 2009 Jun 11.
Objectives. The purpose of this prospective study was to evaluate the clinical outcome of crown-retained fixed dental prostheses (FDPs) made from a lithium-disilicate glass-ceramic (IPS e.max Press, Ivoclar-Vivadent).
Methods. Thirty-six three-unit FDPs were placed in 28 patients. The FDPs replaced teeth in the anterior (16%) and posterior (84%) regions. All teeth were prepared following a standardized protocol. The size of the proximal connector of the FDPs was 12 mm2 (anterior) or 16 mm2 (posterior). FDPs were cemented either with glass-ionomer cement (n = 19) or composite resin (n = 17). The following parameters were evaluated at baseline, 6 months after cementation and then annually (at abutment and contralateral teeth): probing pocket depth, plaque index, bleeding on probing, and tooth vitality.
Results. Three FDPs were defined as drop-out. The mean observation period of the remaining 33 FDPs was 86 months (range: 67-98 months): two FDPs in two patients had to be replaced (6%) because of fractures. The 8-year survival rate according to Kaplan-Meier was 93%. In addition, chipping of the veneering material was found in two FDPs (6%). Two abutments (3%) of two restorations had to be treated endodontically; and two FDPs (6%) lost reten-tion and had to be recemented. These complications did not affect the function of the involved restorations clinically. There were no significant differences between the periodontal parameters of the test and control teeth.
Significance. Short-span crown-retained three-unit FDPs made from lithium-disilicate glass-ceramic can be used clini-cally irrespective of an adhesive or conventional cementation.
Reprinted with permission of the Academy of Dental Materials.