Embed Size (px)
Citation preview

COMMUNITY HEALTH STUDIES VOLUME IV, NUMBER 3, 1980
RESPONSE OF DEPUTISING SERVICES IN MELBOURNE TO ACUTE CEREBROVASCULAR EPISODES: AN EVALUATION
David Christie
Depurtment of Communiry HrulJt. University of Melhurnr, 243 Gruttun Strect. Curlton, Vic.
Abstrsct
Between R-mh 1978 and September 1979, a stroke incidence study was canied out in Melbourne. Of the 300 subjects who sought help from a general practitioner, in 68 the call was answered by a member of a ckputising service. Each of tbe latter subjects was matched for age, severity and time of onset with a patient whose call had been responded to by his own general practitioner. Re nse times, use of hospital resources, mortality Z s i d u a l disability in sur- vivors were compared. It was concluded that, in this condition at least. the deputising services provide fast, effective care meeting the needs of both general prac- titioners and patients in perceived emergency situa- tions.
IntrodueuoA
The use of dcputising or locum services to cover wt-of-hours primuy care is widespread in Australia', it.. it is in many countries. Yet then have been few studies of the quality of care d e l i v d by such services. ond none a p p u to have bcut carried out in Australia.
In thc present study, acute onset of stroke has been used as a tracer condition and the course of early care, a d its outcome. compad in those patients cared for by their own doctor with thou attended by tht deputising service. Stroke is a ruitabk tracer condition because it is common, a definite diagnosis can usurlly be made. and it is perceived by the patient plid his family as a crisis situation wherc help is needed urgently.
Because cases were identified from a poprlation-basad svdrc register, ntha than from a hospital series, an u a b i i view of the cervices received by a gmgmphhlly defined ccmmuniIy may be obtained.
mteri&.adMc(kdr
From March 1978 to September 1979. a
out in an urban area of Melbourne. The population at risk was approximately 16O.OOO. yielding 508 stroke
population-based strolrt incidence study was carried
patients; ascenainment was believed almost compkte. Of these patients, 426 w m living at home oc independently and of these 300 (70 per cent) cdkd for help to a general practitioner. This call was regarded as 'successful' by 279. pad of thtse. 68 of the visits were made by a mmberof the deputising service. The latter service wpll n a over-represented in the 21 'unsut;cessful' medid axwnters.
Eoch of the 68 subjects. who had been attended by a locum, was mplchod with the next consecutive patient who had been seen by their general prac- titioner. Tk matching required the pairs to be within the same ten-year agbpup. general severity (fully conscious as q p o d to not fully conrcious at time of maximal impairment) ud time of onset.
Non-parametric tests of statistical significance were employed throughout the analysis'; the Willcoxon matched pairs signed rank test wherc possible. and the sign test when the outcomc was dichotomous.
RgalQ Time P e r i d
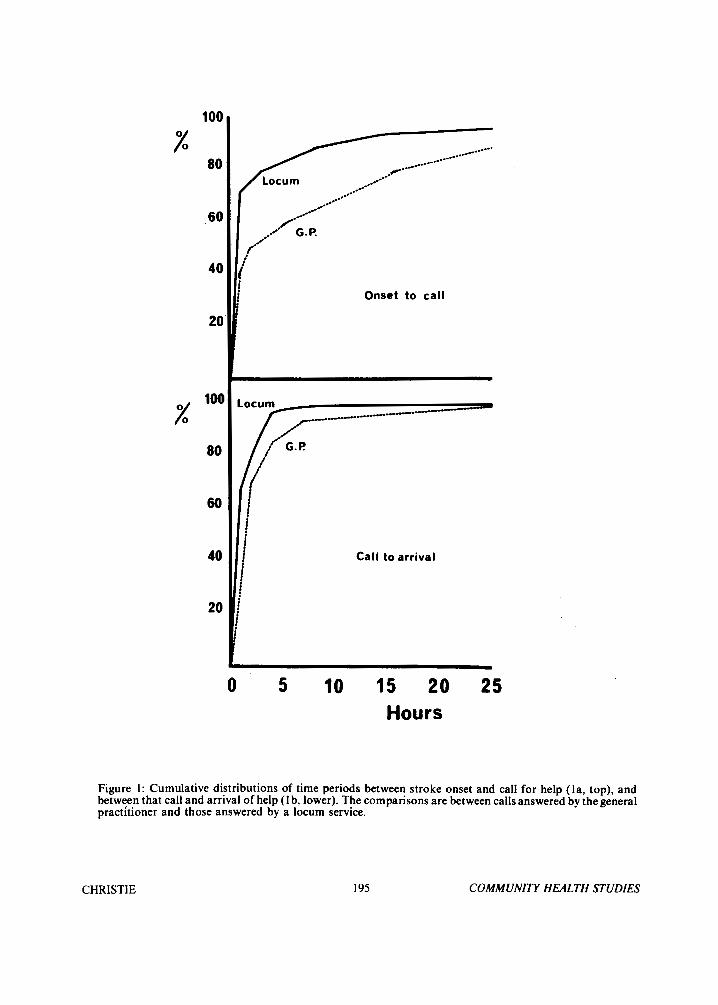
In comparing the time aspects of 'process', there arc two period0 of interrst. The first is the period between scrdre on- and the decision to call for help. the second is the period between calling and the arrival of that help.
Figure I@) is the cumulative distribution of the time pen& between onset and call. for both locumr and general itioncn. All 68 locum attended caws
g c m l practitioners. the misvidg cues being thvw in which n tinw of onvet could MU bc revwnvhly estllblirhed. Thew wm P longer &lay when the prac?itioner attcnded than thc deputising service; 72 per cent calktl the locum within an hour of nmct as c m to 41 pa cent in the c u e of thc.gencml practitkmr. This diffcmncc is highly xignificwrt (P<O.OOI) using a matched puirs. signed rank tea o n 64 puirs. Thc most likely cxplanation is that pecplc whosc doctors regularly use the locum service have M) kitation abwt cdlin at odd hours; those whose doctor docs his own calfs arc more likely to delay to a more rcrwnahle time.
werc availo r k for analysis a d 64 in the c w or
C H R 1 S TI E 194 COMMUNITY HEALTH STUDIES
100
80 %
60
40
20
% loo
80
60
40
20
Onset to call
Call to arrival
0 5 10 15 20 25 Hours
Figure 1: Cumulative distributions of time periods between stroke onset and call for help (la, top), and between that call and arrival of help (1 b, lower). The comparisons are between calls answered by the general practitioner and those answered by a locum service.
CHRISTIE 195 COMMUNITY HEALTH STUDIES

The second question, the time between call for help and arrival of that help, i s examined in Figure I(b). For locum visits there were 68 cases available, and 56 cases tor general practitioner visits. The missing cases in the lattcr group are those in whom rhc patient was tiihcn to the doctor's surgery. nnd thosx for whom the practitioner arranged matters by tclcphonc to the patient'> satisfaction. Once more. i t is appircnt that the ~(MXIIII'S response tinic i s shorter with h X pt cchl of ciills hcinp met witliiii tlic hour, ;IS oplwscil ro 41 per cent in the case of general practitioners. 'l ' l i is diffcrcnce is statistically significant (P<0.025).
kclion Tukiw by Doc~or In the case of an acute onset of stroke, the mo>i
immediate decision by the attending dcrtor i s whcthcr to have the patient admitted to a general hospital. Ot the patients seen by the deputising service. 57.4 per cent were admitted within 6 hours ot' onset ah compared with 38 per cent of those patients seen by ;I general practitioner (P<0.025). Yet when the days spent in an xu te general hospital. in the first month after onset, arc compared there is no significant difference (PCO. 10). although the trend is in favour 01 the general practitioner.
Outcome of' Cure Measures o f precess, including usage o f health
service resources, are important in evaluation, but the most important measures of all must relate to outcome. In the present study two measures of outcome have been chosen, survival to three months after onset, and mobility three weeks after onset.
The survival to three months o f those patients attended by the deputising service was 6 I per cent, the survival of those attended by their general practitioner was 66 per cent. A paired analysis, taking into account actual survival times, showed no statistically signific- ant 'difference. With regard to functional state, each survivor was assessed at three wceks.after onset for observed walkipg ability. The classification used was: walks entirely independently, walks with aid of mechanical device (including simple walking stick), walks only with the active suppofl of another person,
and, finally i s bedfast. When each o f these possible outcomes is scored from ' I' to walking independently to ' 5 ' for being dead at three weeks, a paired comparison i s possible. There was no statistically signiticant difference in outcomes betwecn t h o i subjects seen by a locum or a general practitioner.
Discussion
The task of the locum, or member o f a deputising service, i s to provide medical care where i t i s urgently needed, usuully in an 'out-of-hours' situation. There can be litt le question that a patient's own general practitioner i s able to deliver better all-round primary care, but the quality of the care delivered by the locum may only be evaluated in terms o f what he is required to do; provide emergency cover. Whether early intervention by a doctor, in the case of acute cerebrovaxular accident, makes a difference may be debatable; it is not so for the client and his family waiting for help in what they perceive as a crisis situation. Speed in attendance would thus seem important to the client, and for this reason stroke i s a reasonable tracer for investigating the effectiveness of emergency services.
The present study shows that, in the case of acute cerebrovascular accident, the deputising services respond rapidly 68 per cent o f calfs being attended within the hour. Speed of rcsponse i s related to the probable diagnosis, and, in Melbourne, the response time to stroke i s almost identical 10 that reported from the United Kingdom for acute myocardial infarction:'. With regard to outcome, patients attended by a locum do not appear to be at all disadvantaged in terms of survival or residual disability, a finding which is consistent with other work'. The locum i s more inclined to solve his problem by arranging immediate admission to a general hospital. but this does not significantly affect hospital bed usage over the longer term.
A reasonable conclusion i s that whilst lccum services appear to be necessary to primary care practice. thc quality of the care they dclivcr is appropriate ( ( I the joh they arc asked to do.
References
1. P. Elliott, The function and fate o f locum services. Med. J . Aust., 1976; 1:709. 4. B. T. Williams, R. A. Dixon, J . Knowelden,
2. S . Siegel, Non-parametric statistics. Tokyo: Emergency admission to hospital from a degutis- McGraw-Hill. Koyakusha Ltd., 1956. ing service; a controlled study o f duration of stay
3. R. A. Dixon, B. T. Williams, Twelve months of and outcome. Brit. J . Prev. SOC. Med. 1973; deputising : 100,OOO patient contacts with eighteen 27: 126.
services. Brit. Med. J . 1977; 1:560.
CHRISTIE 1% COMMUNITY HEALTH STUDIES