Embed Size (px)
Citation preview

Postgrad Med J (1990) 66, 1 - 15 © The Fellowship of Postgraduate Medicine, 1990
Reviews in Medicine
Respiratory diseases
D. Geraint James' and O.M. Sharma2
'Medical Unit, Royal Free Hospital, London NW3 2QG, UK and 2Pulmonary Disease Unit, University ofSouthern California, Los Angeles, California, USA.
Introduction
We have chosen to review prominent papers of1989 which influenced chest physicians' thinkingand practical management. We have drawn atten-tion to some manuscripts which will carry even a1990 reference and provide stop press information.We review, in this order, techniques, metabolicfunctions, Wegener's granulomatosis, adult res-piratory distress syndrome, asthma, interstitialpulmonary disease, lung cancer, transplantation,occupational lung disease, infections and thera-peutics.The garden is full ofthe most enchanting flowers.
We have plucked and offer for you, dear readers,our very personal choice. We have made up abunch of other men's flowers; we have only pro-vided the string that ties them together. Now goforth, sew your own seeds or gather a fresh crop inthe inviting field of respiratory medicine andsurgery.
Techniques
The study of respiratory disease has become morescientific and sophisticated with new techniques orrevitalized old ones. We are nearer the heart of thematter because of fibreoptic bronchoscopy, bron-choalveolar lavage (BAL), computed tomographic(CT) scanning, fine needle biopsy and physiologicaltests of lung function.
Bronchoscopy
Bronchoscopy is usually combined with BAL andbronchial biopsy to obtain the maximum inform-ation in the differential diagnosis of interstitial lungdisease for the clinician, histopathologist andimmunologist. BAL is already well recognized tobe helpful in providing some additional inform-ation in differentiating sarcoidosis from extrinsicallergic alveolitis (hypersensitivity pneumonitis)and fibrosing alveolitis. Attention is being increas-ingly focused on this technique worldwide in thedetection of subclinical infection of humanimmunodeficiency virus (HIV). Higher percentagesof neutrophils and lymphocytes have been noted inBAL fluid of patients with acquired immuno-deficiency syndrome (AIDS) and pulmonary infec-tion' contrasting with the decrease in the number oflymphocytes in blood, suggesting early or subc-linical infection in the pulmonary parenchyma.This is often due to Pneumocystis carinii but notalways so, as revealed by a recent study 2 in whicheight symptom-free HIV-positive patients under-went bronchoscopy, BAL and bronchial biopsy. P.carinii was absent from lavage fluid, biopsy orbrush material.BAL has also shed light on primary biliary
cirrhosis (PBC) in which an intense lymphocyticalveolitis indentical to that observed in sarcoidosismay be found. This brings closer together twoentirely different granulomatous disorders,formerly separated by the diaphragm, but nowreflecting a close lung-liver interface'. Let us hopethat this will lead towards a better understanding ofthe aetiology of these two idiopathic granulo-matoses.
Fine needle biopsy
When bronchoscopy and sputum examination arenegative, percutaneous core needle biopsy usingthe Hausser needle is commonly done in theUniversity of Saarland, Federal German Repub-lic.4 About two-thirds of the lesions in this study
Correspondence: D. Geraint James M.A., M.D.,F.R.C.P.This article is the first in a series of critical reviews ofmajor developments within the previous year which willbe a regular feature of the Journal. The remaining topicscovered in 1990 will be Oncology (February), ClinicalPharmacology (March), Cardiology (April), GeneralSurgery (May), Nephrology (June), Gastroenterology(July), Psychiatry (August), Haematology (September),Dermatology (October), Endocrinology (November) andInfectious Diseases (December).The Reviews in Medicine series has been made possible
by funds of the Fellowship of Postgraduate Medicine.Reprints will not be available from the authors.
Editor - Postgraduate Medical Journal
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

2 D.G. JAMES & O. SHARMA
were peripheral and 40% were 2 to 4cm indiameter. The biopsy needle was inserted underbiplanar fluoroscopic control; breath holding waslimited to the time the needle was crossing thepleura and thereafter shallow breathing wasallowed. The specimen, about 10 to 20 cm in lengthwas removed, trapped between the blades. Therewas a high diagnostic yield of about 90% and acomparatively low rate of complications of 15%.Interestingly, the diagnostic yield was high inundifferentiated large cell carcinoma, squamousand adenocarcinoma, but was low in carcinoid,alveolar cell and metastatic carcinoma, cylindromaand small cell anaplastic cancer. Benign lesionsincluded tuberculosis, aspergillus, histoplasma,haematoma, organizing pneumonia and non-specific granulomas. Complications were minorand should be weighed against an alternativeexploratory thoracotomy; they included pneumo-thorax, haemoptysis, haemothorax and intrapul-monary haematoma.
Drainage
In 1938, Monaldi5 of Naples introduced the tech-nique of intracavitary intubation and drainage forthe treatment of tuberculosis. This technique hasbeen modified for the treatment of severe bullousemphysema.6 Twenty two operations were carriedout on 20 patients with bullous lung disease, all ofwhom had severe debilitating dyspnoea. Therewere 12 males and 8 females; the median age was 56(range 43-71) years. All patients had respiratoryfunction tests, arterial blood gas measurement andposteroanterior and lateral chest radiography. Afew patients had computed tomography in order toobtain three-dimensional measurement of the bul-lae, both before and after surgery. Open intubationdrainage via a limited thoracotomy (10 cm) wasperformed. Dyspnoea improved in 16 patients. Itwas accompanied by objective improvement inlung function with a 22% median improvement inforced expiratory volume in one second (FEVI) anda 26% median reduction in residual volume. Onepatient remained unchanged. Three patients diedafter surgery: two due to progressive respiratoryfailure and the third because of staphylococcalsepticaemia. The surgical treatment of bullous lungdisease carries a high mortality. The BromptonHospital technique requires a limited surgical app-roach and avoids resection of the functioning lungtissue, which is important for patients with limitedlung reserve. The results are encouraging andprovide a ray of hope to some respiratory cripples.
Drainage procedures may also be helpful inpatients with carcinomatous pleural effusions.Thirty eight patients underwent thoracentesis witha finebore silastic catheter introduced under ultra-sound guidance.7 Pleurodesis using Corynebacter-
ium parvum, tetracycline, thiotepa or bleomycinwas achieved in 27 patients. The other 11 patientshad their effusions drained for the relief of symp-toms but did not have pleurodesis because of theterminal nature of their illness. All patients toler-ated the procedure well. The mean interval frompleurodesis to death in 17 patients was 225 days(range 80 days - 28 months); none had a recurrenceofeffusion before death. This is a simple technique,comfortable for the patient and preferable to thecommonly used wide bore chest tube.
LungfunctionThe long term effects on lung function of treatmentof idiopathic spontaneous pneumothorax by talcpoudrage or simple chest tube drainage wasassessed in 114 consecutive patients treated at thechest clinics at Oresundshospitalet and BispebjergHospital, Copenhagen.8 Ninety nine patients weremen. At the time of the first pneumothorax 99(87%) of the subjects were under 41 years of age.Eighty patients were treated with talc pleurodesisand 34 with simple pleural drainage. Seventeen ofthe 114 patients died from causes unrelated to theinitial complaint, so finally 75 subjects participatedin the study. A mild restrictive impairment of lungfunction was noted in those who were treated withtalc insufflation compared with those who receivedsimple drainage via an intercostal tube. One patienttreated with talc poudrage had extensive pleuralcalcification and mild pulmonary fibrosis. None ofthe patients developed a mesothelioma despite along observation extending up to 35 years. It can beconcluded that the long term prognosis with regardto lung function in idiopathic spontaneouspneumothorax is quite good regardless of thetherapeutic technique employed.Lung function and exercise performance have
also been assessed in hyperthyroidism before andafter treatment since many hyperthyroid patientsare breathless. In order to investigate the mech-anism of dyspnoea a Bristol team has performedextensive lung function tests including spirometry,lung volumes, transfer factor (diffusing capacity)for carbon monoxide, methacholine challenge,arterial blood gases and exercise in 16 patients withuntreated hyperthyroidism.9 Methacholine chall-enge tests showed mild increased hyperactivity inonly three of 14 patients. Functional residualcapacity and maximal inspiratory and expiratorypressures were reduced in some patients. Diffusingmembrane capacity for carbon monoxide wasreduced in two patients. Exercise ventilation,respiratory rate, and respiratory exchange ratiowere abnormally high; 14 of 16 patients discon-tinued exercise tests because of dyspnoea. Themaximum oxygen uptake achieved by the groupwas 53% of predicted maximum oxygen consump-
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

RESPIRATORY DISEASES 3
tion.Nine patients were studied after being rendered
euthyroid by treatment; they showed improvedexercise performance. Respiratory muscle functionis weak in hyperthyroid patients and this improvedfollowing treatment. It has been suggested thatthere is a link between thyroid disease and asthmabut it was not evident in this series. The occurrenceofincreased airways hyperreactivity was no greaterthan could be expected in healthy controls.
Respiratory muscle fatigue has also beencorrelated with lung function in systemic lupuserythematosus (SLE). Extensive lung function testsand electromyography were performed in 23 conse-cutive patients with SLE and 17 healthy controls inDusseldorf.'° Lung function included total lungcapacity (TLC), vital capacity (VC), residualvolume (RV), airway resistance (body plethysmo-graphy), the single breath transfer factor, and lungcompliance. Maximum inspiratory and expiratorymouth pressures, PImax and PEmax, were measur-ed at forced residual capacity (FRC). Fatigue ofrespiratory muscles (diaphragm, external inter-costal muscles), and of leg muscles was assessed byelectromyography. VC and TLC were significantlylower in SLE patients than in the controls.However, no significant difference between SLEpatients and controls was found for RV, FEVI,FEV/VC and airway resistance. Lung compliancewas slightly reduced in SLE patients. The patientswith SLE showed significantly (P<0.05) lowervalues of PImax and PEmax than the controls.Fatigue of all muscles occurred in a significantly(P<0.01) higher percentage at lower external loadsin SLE patients. The reduction in VC and TLC wasmost pronounced in SLE patients with signs ofrespiratory muscle fatigue while the patients with-out signs of fatigue showed normal or slightlyreduced (< 10%) lung volumes. This study noted asignificant correlation between duration of symp-toms and respiratory muscle dysfunction but thismuscle fatigue did not correlate with activity ofSLE. The degree of dyspnoea often correlates withinspiratory muscle dysfunction.
Diaphragmatic fatigue may sometimes contri-bute but this is controversial. Laroche et al." havereported an elegant study ofdiaphragm strength inthe shrinking lung syndrome of SLE from theBrompton and Hammersmith Hospitals and ano-ther authoritative review of respiratory muscleweakness and fatigue from the Brompton andKing's College Hospitals.12 They conclude that theshrinking lung syndrome of SLE is not explainedby a primary abnormality of the diaphragm. Thereis unlikely to be one single index of fatigue, butrather a whole sequence of closely inter-relatedchanges that occur in response to loading. Theirelegant techniques will undoubtedly lead to animproved understanding of the role of respiratory
muscle dysfunction in ventilatory failure. Thoseparticularly interested in the clinical and patho-logical features of lung involvement in SLE shouldread a recent review'3 and are also reminded that itis the silver anniversary of a pioneer article onunexplained dyspnoea and shrinking lungs in SLEby the editor of the Postgraduate Medical Journal(Hoffbrand and Beck, 1965).'4Positron emission tomography (PET)
PET is a powerful, quantitative, nuclear medicineimaging technique, useful for studying many prob-lems in lung physiology and biochemistry.15 Itallows measurements oflung density, extravascularlung water, blood volume, pulmonary blood flow,ventilation- perfusion relationships, vascularpermeability, glucose metabolism, amine clear-ance, hypoxic tissue markers and tumour imaging.Compounds are labelled with positron-emittingisotopes which include labelled oxygen, carbon,gallium, nitrogen, fluorine and neon, and may beadministered intravenously or by inhalation. Thetissue activity concentration of the isotope isdetermined with an imaging device similar inappearance to an X-ray CT scanner. Its applica-tions for the investigation of pulmonary problemsin health and disease are numerous, but PETresearch has its drawbacks. It represents a majorcollaborative effort in which the lung physiologistmust work with radiation chemists, physicists,computer programmers and mathematicians. Thecosts in personnel and equipment are high, butSchuster'5 outlines attractive lines of study for lungphysiologists of the future.
Metabolic functions
The lung has important metabolic functions, andmuch of our pulmonary pharmacology is directedat blocking the effects of lung mediators on bron-chi, parenchymal cells or lung vasculature. Themodern chest physician must be able to do morethan interpret a chest radiograph correctly and beconversant with endoscopy and lung function tests.Nowadays he must also understand the role ofsurfactant, serotonin, eicosanoids, platelet-activ-ating factor, oxygen free radicals and the applica-tion of molecular biology to pulmonary disease.This information is all brought together in a specialissue of Clinics in Chest Medicine.4 This is publishedquarterly and useful back numbers have includedRespiratory Muscles (June 1988), PulmonaryEffects of AIDS (September 1988) andInflammatory Disorders ofthe Airways (December1988). The present issue consists of elevenauthoritative chapters on metabolic functions ofthe lung. It is impossible to find such a scholarly
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

4 D.G. JAMES & O. SHARMA
and stimulating update on the physiology andbiochemistry of the lung elsewhere so it is wellrecommended.
Serotonin, also known as 5-hydroxytryptamine(5-HT) is one of the many substances processed bythe pulmonary vascular endothelium, whichremoves it from the circulation and metabolizes itintracellularly. When lung injury causes endo-thelial cell damage, ability to remove 5-HT isimpaired resulting in increased concentrations ofcirculating 5-HT. This increase affects airways andvascular muscle tone, and also leucocyte andplatelet function. Because 5-HT is a potent platelet-aggregatory agent and activator, increased 5-HTconcentrations cause platelets to adhere todamaged vascular endothelium. Likewise, leuco-cytes adhere to vascular endothelium by the samemechanism. Refined techniques for the measure-ment of 5-HT will in the future provide earlyevidence of lung injury in such emergencies as theadult respiratory distress syndrome and in latentpulmonary embolism, and hopefully provide asignal for early treatment.17
Surfactant acts by lowering surface forces at theair-liquid tissue interface. It is well-recognized thatpremature newborns are unable to produce ade-quate amounts of functional surfactant so surfaceforces collapse the lung at resting transpulmonarypressures, resulting in atelectasis and impaired gasexchange. The metabolism of alveolar surfactantprotein and surfactant lipid turnover are dis-cussed,18 particularly since surfactant replacementtherapy is being introduced in a variety of clinicalconditions.
Eicosanoids are metabolites of the essential fattyacid, arachidonic acid which is an integral part ofall cell membranes. Fast and sensitive enzymeimmunoassay techniques aided by high per-formance liquid chromatography separation ofextracts and of mass spectrometry have facilitatedthe identification and quantification of prosta-glandins, leukotrienes and platelet-activatingfactor in bronchoalveolar lavage and lung tissue.The authors of this scholarly review'9 then proceedto discuss the treatment of human lung diseasebased on manipulations of the eicosanoid system.They consider two diametrically opposed treat-ment strategies, namely by inhibiting eicosanoidsynthesis or by the use of eicosanoids.
The reader will also be interested in other quarterlyissues which include Pulmonary Function Testing(June 1989), Mycobacterial Diseases (September1989) and Pulmonary Manifestations of SystemicDisease (December 1989).
Wegener's granulomatosis (WG)
Friedrich Wegener lives in happy retirement inLubeck, Germany.20 Now aged 82 years, he haslived to witness two important advances in know-ledge of a disorder he first described in the Germanliterature in 1937, and reprinted in English to markthe 50th anniversary of a classic paper.2' The twoimportant advances concern diagnosis and treat-ment. Serum autoantibodies against cytoplasmiccomponents of neutrophils (ANCA for antineu-trophil cytoplasmic antibodies or ACPA for anti-cytoplasmic antibodies) show a high specificity forWG and microscopic polyarteritis and as a monitorof activity of the disease. A Dutch-Danish teammade a decisive step forward with the demonstra-tion of fine granular centrally accentuatedimmunofluorescence staining pattern, due to IgGautoantibodies, in the cytoplasm of neutrophils.22Fluorescence is additionally seen in monocytes butnot in lymphocytes. There has been a recentsplendid review by another German pioneer,23 andan Edinburgh group has laid down strict criteriafor patterns of immunofluorescence, which distin-guish the bright coarsely granular pattern which isspecific for WG from other non-specific patterns.The technique is simple, inexpensive, rapid andreproducible.24 Associated with this article is anadmirable balanced editorial.25 A new ELISA-test,based on purified antigen derived from normalhuman neutrophils, has yielded results equivalentto those obtained by indirect immunofluorescencein a joint study by Kiel University and the MayoClinic.26 This multicentre study is based on 277patients with WG and 1657 control patients. Bothtests are highly specific and are helpful in diagnosisand as markers of disease activity.The second advance which Wegener has lived to
enjoy is treatment, which has significantly changedthe morbidity and mortality. His twelve patientsdied and the mortality in that era was 100%; butwith corticosteroid therapy and cyclophosphamideit has fallen to about 5%. IfWG progresses despitethis oral combination of drugs, then cyclophos-phamide should be given as monthly intravenousbolus treatment in a dose of 0.5 to 1 g/sq metretogether with high dose steroid therapy.27 Cyclos-porin has also been shown to cause dramaticimprovement in fulminant disease resistant tocyclophosphamide and in a patient with renalfailure.28
Adult respiratory distress syndrome (ARDS)This is a state of shock lung which has also beentermed adult hyaline membrane disease or the stifflung syndrome. Pulmonary oedema is associatedwith normal rather than raised pulmonary vascular
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

RESPIRATORY DISEASES 5
pressure. There are numerous precipitating causes- septic shock, burns, pancreatitis, drug abuseamongst them - to be followed within 24 hours bydyspnoea, tachypnoea, a low arterial oxygen ten-sion (PaO2< 50 mmHg) despite high inspiredoxygen concentrations, and diffuse fluffy patchyinfiltrates in the chest radiograph. It has beendescribed as refractory hypoxaemic respiratoryfailure with radiographic evidence of pulmonaryoedema occurring in the setting of an appropriaterisk factor.9 The oedema fluid is protein-richbecause of increased pulmonary vascular perme-ability to plasma proteins. This protein leak hasbeen assessed by a double-isotope method for thedetection of transferrin accumulation in the lungsof patients with widespread pulmonary infiltrates.'In 22 patients with ARDS the mean transferrinaccumulation rate was threefold greater than acontrol group. However, there was some overlapbetween ARDS and controls so it cannot beregarded as a diagnostic test. However, it is a
relatively simple method for serial bedside deter-mination of pulmonary microvascular perme-ability to transferrin.
Prematurity
Premature low birth-weight children with im-mature lungs suffer severe bronchopulmonarydysplasia; it is a major medical problem in neonatalintensive care nurseries. It has been the subject of arecent important editorial based on two articles inthe same issue of the New England Journal ofMedicine. The editorial3 describes the dedicationof neonatal physicians and nurses and the grief ofparents who watch helplessly as their infantsstruggle to survive with assisted ventilation,oxygen, correction of poor nutrition, antibioticsand surfactant.Dexamethasone therapy for 42 days improves
pulmonary and neurodevelopmental outcome inthese circumstances,31 but this is on the principle ofbuying time for the very existence of the infant andthe cost in longterm complications may be infec-tion, hypertension or hyperglycaemia. An alter-native procedure is prophylactic surgical closure ofthe open ductus arteriosus for recurrent pulmonaryoedema is associated with large left-to-rightshunts;32 but this has proved disappointing. Stahl-man's editorial30 is an illuminating background ofthe wretched contributing social problems whichstill exist; it is compulsive reading.
Asthma
PregnancyThere have been detailed studies of asthma duringpregnancy in Helsinki and in Bristol. The Finnish
authors33 monitored 198 pregnancies lasting 24weeks or more in 181 women with asthma. Allpatients received optimum treatment includinginhaled adrenergic drugs, beclomethasone, sodiumcromoglycate, oral theophylline, and systemiccorticosteroids. Clinical case records and labourhistories of the 198 non-asthmatic women, match-ed for age and parity were reviewed. Duringpregnancy 18% needed less and 42% more medi-cation. Pre-eclampsia occurred more often inasthmatic than in control subjects, particularly inthose with severe asthma. Hypoglycaemia occurredmore often in infants of mothers with severeasthma. Theophylline did not influence eitherlabour or delivery. Twenty eight per cent of babiesamong the asthma subjects were delivered byCaesarean section compared with 17% in thecontrol group. There was no difference betweenasthma patients and control subjects with regard tolength of gestation, birth weight, incidence ofperinatal deaths, low Apgar scores, neonatalrespiratory difficulties, hyperbilirubinaemia orcongenital malformations. The authors concludedthat severe asthma or systemic corticosteroidtherapy or both during pregnancy seems to inc-rease the incidence of mild pre-eclampsia in themother and hypoglycaemia in the infant. Theoutcome of pregnancy is not significantly alteredby asthma. Although breast feeding was encour-aged, antiasthma drugs did not affect the infant.The Bristol team34 followed 31 asthmatic women
during pregnancy and for 6 weeks of the puer-perium. Subjectively 22 (69%) women consideredtheir asthma to have improved, two were worse andin seven (22%) there was no change. The resultssuggest that in patients with mild or moderateasthma an improvement is likely to occur duringpregnancy, particularly in the last trimester, butthat in over one-third there may be a post-nataldeterioration.
Nocturnal asthma
It is well-known that gastro-oesophageal (GO)reflux can cause aspiration and a constellation ofrespiratory disorders including recurrent pneu-monia, asthma, atelectasis and fibrosis. A highincidence of GO-reflux has been observed inasthma patients. It has been suggested that noctur-nal asthma is triggered by GO-reflux.
Thirty seven adults with nocturnal asthma formore than 100 days a year and a history ofGO-reflux have been under close medical super-vision in Sweden.35 Determination of 24-hour pHmonitoring of the oesophagus and hourly measure-ment ofpeak expiratory flow (PEF) rate were madeduring waking hours. Half of the patients hadsevere nocturnal GO-reflux, the other half had nosuch symptoms. Respiratory symptoms and the use
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

6 D.G. JAMES & O. SHARMA
of 1-2-agonists during the night were recorded andPEF was measured in the morning. There was asignificant relationship between the presence ofGO-reflux at night and the degree of broncho-spasm in the early morning, but there was nocorrelation between the night time reflux andnocturnal respiratory symptoms. It appears thatGO-reflux in most of the asthmatics does notimmediately precipitate asthma and produceclinical symptoms although it does seem toinfluence vagal bronchomotor tone as was demon-strated by a low morning PEF value.
Patients with asthma and gastro-oesophagealreflux should be given a trial of conservativetreatment including elevation ofthe head ofthe bedand smaller and solid meals in the evening. One ortwo doses of antacids after meals and at bedtimemay produce marked relief, or alternatively an H2receptor antagonist may be given. A careful reviewof medications is important because anti-cholinergic drugs, calcium-blocking agents, andtheophylline may exacerbate gastro-oesophagealreflux.There has also been an excellent review of the
many other factors which contribute to nocturnalasthma, including body temperature and cold,snoring, autonomic nerve activity, and circadianrhythm.36 The severity of nocturnal asthma cor-relates with the degree of bronchial reactivity; themore exaggerated the hyper-responsiveness tovarious stimuli, the more marked is the nocturnalbronchoconstriction. Long-acting inhaled bron-chodilators should simplify the management ofnocturnal asthma.36
Mechanics
A Vancouver group has studied the histology oftheairways in post-mortem specimens of lung obtain-ed from 18 asthma fatalities.37 The results werecompared to similar airways from 23 patientswithout asthma. Seventeen of 18 patients hadsevere steroid dependent asthma; one patient hadmild disease. Each airway was projected onto adigitizing board of a microcomputer to trace theinternal and external perimeter of the airway and tocalculate the submucosal and mucosal thicknesses.The relaxed length of the airway smooth muscleand the shortening required to occlude the airwaylumen were calculated. The wall area in themembranous and cartilagenous airways of asth-matic patients was greater (P <0.001) than non-asthmatic airways. This increase in wall area wasdue to increased areas of epithelium, muscle andsubmucosa. The airways smooth muscle shorten-ing required to occlude the lumen was less inasthmatic than non-asthmatic airways (P< 0.001).
Chronic inflammation causes thickening of thewalls of the airways, a fact which has been
emphasized in Southampton by elegant techniqueswhich display subepithelial fibrosis in the bronchiof asthmatics.38 This study highlights the extensivedeposition of collagen beneath the bronchialepithelium of young patients with mild atopicasthma. Endobronchial biopsy specimens wereexamined by immunochemistry and electronmicroscopy. They suggest a pathogenic role for twoof the classic cellular protagonists of asthma - themast cell and the eosinophil leucocyte - as stim-ulants of fibrogenesis. They recommend furtherstudies to determine the cellular basis of thisexcessive deposition of collagen and its role in thenatural history of bronchial asthma, particularlywith respect to the pathogenesis of chronic irre-versible airways obstruction.38
Interstitial pulmonary disease
There was a recent internal medicine conference atSouthwestern Medical Center, Dallas, based onidiopathic pulmonary fibrosis. By way of an intro-duction, Weissler's Table 1 (which runs into 2pages) presents the differential diagnosis of in-terstitial pulmonary diseases.39 It has 10 mainheadings, each of which is followed by about 5subheadings and each subheading by between 6and 16 topics representing about 150 differentinterstitial pulmonary diseases. This encyclopaedictable would form an admirable list of contents foran exhaustive textbook. Weissler's 130 referencesalso make it a comprehensive review of the topic.The pages between Table 1 and the referencesencompass collagen homeostasis, the cytology ofbronchoalveolar lavage fluid, injury by lymph-ocytes, fibroblast participation in idiopathic pul-monary fibrosis (IPF), the role of growth factorsand cytokines. It ends with a summary of newertherapies for IPF, including colchicine, gamma-interferon and lung transplantation. It is hopedthat readers will derive as much information andlearning as Dr Weissler must have done in compos-ing and compiling this splendid review.
Langerhans' cell granulomatosis (LCG)
The alternative name is histiocytosis X. It encom-passes a group of disorders of unknown aetiologycharacterized by granulomatous infiltration oflungs, bones, skin, lymph nodes and brain. It issometimes mistakenly diagnosed as sarcoidosis.Consider it in young adult heavy-smoking maleswith interstitial lung disease, presenting with recur-rent pneumothoraces or diabetes insipidus. Thegroup with the most experience of this disorderhave recently published an exhaustive review oftheir experience in Paris.40 Lung biopsy reveals amixed cellular exudate, foam cells, eosinophils and
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

RESPIRATORY DISEASES 7
characteristic X bodies in macrophages. X orLangerhans' bodies are an ultrastructural featurein 90% of patients. They are identical to thegranules in Langerhans' epidermal cells, and con-sist of intracytoplasmic rod-, plate-, or cup-likepentalaminar structures, which are diagnostic ofthis disorder.
Paul Langerhans (1847-1888) was born andstudied medicine in Berlin and became professor ofpathology in Freiburg. His special interest in skinpathology led to his description in 1873 of thegranular cells in the exterior portion of theMalpighian layer of the epidermis, the stratumgranulosum or Langerhans' layer. He is alsoremembered by the islets of Langerhans, and nowhas been provided with yet another eponymousdisorder, one hundred years after his death fromtuberculosis in Madeira.
Talcosis
Another interstitial lung disease has recently beenbrought into focus in Montreal by longtermfollow-up of six drug abusers who injected intra-venously talc-containing drugs intended for oraluse.4' Although these patients had discontinued theaddiction, in the course of 10 years or more theydeveloped severe granulomatous inflammation andfibrosis surrounding the talc particles. Talc (hyd-rated magnesium silicate), starch and cellulose areinsoluble fillers commonly used in the preparationof oral medicines; they keep the medicinal com-ponents together and act as lubricants preventingthe tablets from sticking to punches and dyesduring manufacture. When talc-containing drugsare injected intravenously the talc is trapped inpulmonary arterioles and capillaries causinginflammation, thrombosis, granuloma formationand fibrosis. At necropsy, the lungs show severepanacinar emphysema with focal bulla formationand dense perihilar tissue. Chest X-rays revealdiffuse micronodular interstitial infiltrates progres-sing into conglomerate shadows in the upper lungfields. Lung function studies reveal both restrictiveand obstructive patterns early in the course buteventually become markedly obstructive. Death isdue to severe respiratory failure which occurstragically many years after drug abusers haveovercome and discontinued this particular addic-tion.
Chronic eosinophilic pneumoniaThere has been a comprehensive review of 119 casesof chronic eosinophilic pneumonia (CEP).42 Theauthors personally evaluated 19 patients with CEPover an 11-year period and reviewed an additional100 cases from the literature. The majority ofpatients with chronic eosinophilic pneumonia are
middle-aged women. Pre-existing atopic disease ispresent in half of the cases. Despite the atopichistory, most patients are well before the onset ofCEP. Peripheral blood eosinophilia of greater than6% is present in 98% and the erythrocyte sediment-ation rate is more than 20 mm/h in 94% of thepatients. Pulmonary infiltrates are peripherallydistributed; pathological findings include an intra-alveolar and interstitial infiltrate comprisingeosinophils, histiocytes and other inflammatorycells. Bronchiolitis obliterans occurs in about onequarter of patients, and rarely there are eosin-ophilic micro-abscesses.
This is an elegant review42 based on soundclinical judgement. The authors emphasize that theclinical diagnosis ofCEP in most cases can be madewith reasonable certainty without lung biopsy.These patients are exquisitely sensitive to cortico-steroids and an initial therapeutic trial withouttissue diagnosis is worthwhile in most instances.
MediastinalfibrosisMost infections with Histoplasma capsulatum areasymptomatic or produce minimal symptoms.Mediastinal granuloma and fibrosis are infrequent,but serious, complications with a mortality rate of30%. A Tennessee survey43 describes the clinicaland radiographic features of 71 patients withmediastinal fibrosis. This group of 71 patientsincluded 65 selected from the medical literature and6 previously unreported cases. All patients hadclinical evidence of occlusion of major centralairways (trachea or mainstem bronchus) or majorvessels (pulmonary arteries or veins) and theabsence of any other disease which might causesuch obstruction. The majority of patients werebetween ages 20 and 40 at the time of diagnosis.Dyspnoea, cough and haemoptysis were commonsymptoms. A loud pulmonary second sound wasthe most frequent clinical sign followed by wheezes,rales and rhonchi. A systolic murmur was heard in26% of patients. Radiographic abnormalitiesincluded mass lesions and infiltrates or loss ofvolume. In many patients chest X-ray films werenormal, even in the presence of a major centralairway or vascular occlusion. In some cases com-puted tomography revealed large subcarinalmasses with pulmonary vascular invasion when thechest X-ray was normal; CT scans are helpful indelineating the location and extent of mediastinalabnormalities. Surgery was of limited therapeuticvalue and there is no evidence that antifungaltherapy modifies the course of the disease sincegranuloma and fibrosis are late consequences ofmediastinal adenitis.
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

8 D.G. JAMES & O. SHARMA
Cysticfibrosis (CF)
The Cystic Fibrosis Research Unit has just cele-brated its twenty-fifth anniversary by launching a£5 million fund-raising campaign. When the Trustwas set up in 1964 about 90% of those born withthe disease died in early childhood, but now there isa 75% chance of survival into adulthood. CF arisesfrom a single gene defect on the long arm ofchromosome 7. The defect probably involves aregular protein responsible for control of ion andwater movement across epithelial cell membranes.This causes high levels of sodium and chloride insweat and is the basis of the helpful diagnosticsweat test. Chorionic villus sampling of fetal DNApermits prenatal diagnosis in one day. The combin-ation of genetic screening, the development ofheart-lung transplantation, new antibiotics, im-proved nutrition, and the development of specialcentres have all contributed to a new healthy air ofoptimism for the future of CF sufferers.44 Theestablishment of a network of regional units is alsorecommended.45
Lung cancer
CT scanning
Is CT scanning essential in the pre-operative assess-ment of lung cancer? This is the increasinglycommon question Pearson poses and answersauthoritatively.46 CT scanners are expensive, bothto buy and run, and alternative imaging methodsshould be employed whenever possible. Abdom-inal ultrasound is valuable in demonstratinghepatic and para-aortic metastatic disease. Themost valuable role of CT is its ability to demon-strate mediastinal lymph nodes. Whilst 95% ofnodes greater than 2 cm in size are infiltrated withmalignant cells only half of those between 1 and1.5 cm are neoplastic; a node greater than 1 cm insize is pathologically enlarged. If the patient isalready in the scanning room, the brain can beexamined in approximately 10 minutes. This mayuncover latent distant metastases which renderthoracotomy inappropriate.46Lymphangitic carcinomatosis
Transbronchial lung biopsy is the diagnostic proce-dure of choice for histology of pulmonary carcino-matosis. If this is refused or considered hazardous,then a worthwhile alternative is pulmonary micro-vascular cytology. Blood is drawn through awedged pulmonary artery catheter. Malignant cellswere found in seven ofeight patients with lymphan-gitic spread of carcinoma from prostate, breast,oesophagus and lung.47 Cytology was normal in 16
of 17 patients with cancer but without pulmonarymetastases and in 22 of 23 patients with non-malignant pulmonary disorders. In a patient withcancer with tumour embolism to the lungs, thefindings were positive because of extensive intra-vascular tumour in large hepatic veins. One falsepositive occurred in a patient with extensive pul-monary infarction. Megakaryocytes, present inlarge numbers in the pulmonary capillary bed, arethe hallmark of a satisfactory pulmonary vascularblood sample for pulmonary microvascular cyto-logical study.
Malignant mainstem bronchial obstruction
If a patient with known or suspected lung cancerhas a significant reduction in forced vital capacityand a normal slope to the expiratory limb of flowvolume, then consider mainstem bronchial ob-struction. The flow volume (FV) loops of 11patients with unilateral, mainstem bronchial ob-struction before and after Nd-YAG laser orsurgical treatment were studied.48 There were 6males and 5 females ranging from 21 to 78 years inage (59 + 18). Each patient had photoendoscopicevidence of malignant tumour causing either com-plete occlusion or severe unilateral mainstem bron-chial narrowing. Maximal expiratory flow volume(MEFV) curves in the three patients with underly-ing emphysema showed a diffuse intrathoracicobstructive pattern before and after treatment; inthe other patients, MEFV curves were consistentwith a restrictive abnormality. After treatment, allpatients showed an increase of forced vital capacitywith a roughly parallel shift of the MEFV curveand little change in the slope ofthe descending limbof the MEFV curve. These results indicate that inthe absence of underlying emphysema, severeunilateral bronchial obstruction produces a restric-tive ventilatory pattern. In the presence ofemphysema, however, the mainstem bronchial obs-truction may remain physiologically masked. Inselected patients, laser therapy offers palliativerelief.
Solitary pulmonary nodule
Geddes and Elliott49 have reviewed succinctly thecontinuing problem of management of thesymptom-free patient found to have a solitarypulmonary nodule; is it benign or malignant?Should the chest physician do nothing, recommendthoracotomy or undertake invasive investigations?A diagnosis may be made by transbronchial lung
biopsy in a quarter ofcases in which the nodules aresmaller than 2 cm and in about two-thirds of casesin which they are larger. Percutaneous needlebiopsy is simpler but may be contraindicated. Theauthors reproduce a pretty diagram relating nodule
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

RESPIRATORY DISEASES 9
diameter to age and to various management stra-tegies. There is, however, little to choose betweenthe various strategies and since there is little in it,perhaps the patient's choice should also berespected.Radiation pneumonitisRadiation pneumonitis occurs within 3 monthsafter thoracic irradiation, and it is generallyregarded to be direct radiation-induced lung injury.Investigators in Sydney regard this as an unlikelyexplanation and show that it is more likely to be ahypersensitivity pneumonitis by an immunologic-ally-mediated mechanism.5 Four patients whodeveloped pneumonitis after unilateral thoracicirradiation for carcinoma ofthe breast were studiedwith bronchoalveolar lavage, gallium scan of thelung, and respiratory function tests. On the irrad-iated side of the chest, all four patients showed anincrease in total cells recovered and a markedlymphocytosis in both relative and absolute terms.However, surprisingly, a similar prominent lym-phocytosis was noted in the lavage fluid obtainedfrom the non-irradiated lung. Likewise, galliumscans showed increased uptake in both irradiatedand non-irradiated lungs, providing further evid-ence that the changes extended well outside theirradiated area. Could these changes be due tohypersensitivity pneumonitis, resembling chronicberyllium disease, sarcoidosis or extrinsic allergicalveolitis. Further studies will undoubtedly beperformed to characterize the T cell subsets, ma-crophages and cytokines involved in this process.
TransplantationSix patients, four females and two males withchronic obstructive pulmonary disease underwenta double lung transplant procedure in Toronto.5The obstructive lung disease was emphysemasecondary to alpha 1-antitrypsin deficiency in 3patients, familial emphysema in one, post-viralbronchiolitis obliterans in one and eosinophilicgranuloma in another. All patients had progres-sive, disabling disease with a life expectancy of 12 to18 months and right ventricular ejection fractionsgreater than 20%. They were all well 5 to 15 monthsafter surgery. It appears that double lung trans-plants are effective for patients with advancedchronic obstructive lung disease. It is an instanttechnological triumph: ethical, social and politicalviewpoints will follow in Toronto and elsewhere.Bone marrow transplants may be followed by
pulmonary complications. Approximately two-thirds of the deaths following allogeneic bonemarrow transplantation (BMT) are due to graft-versus-host disease (GVHD) and non-bacterial,
non-fungal pneumonitis known as interstitialpneumonitis (IP). IP is defined as a clinical syn-drome characterized by hypoxaemia, a diffusepulmonary infiltrate in the absence of heart failureand without any fungal or bacterial cause of thepneumonitis. During a 9-year period 166 (43%) of386 patients with BMT developed interstitialpneumonitis at the Johns Hopkins Hospital.52Tissue examination was helpful in defining 113episodes of IP. Forty percent were caused bycytomegalovirus (CMV) alone or by CMV plusanother pathogen; Pneumocystis carinii or a viruswas responsible for 10% risk but 50% had norecognizable cause. Risk factors for IP overall wereacute graft-versus-host disease, leukaemia, andGVHD prophylaxis with drugs other than cyclos-porin. Risk factors for CMV IP were pre-transplant CMV seropositivity, CMV excretion,age more than 10 years, GVHD prophylaxis withdrugs other than cyclosporin and a remote trans-plant date.The chest physician should also be aware of the
pulmonary complications of liver transplantationwhich are clearly set out in a review ofthe liver lunginterface.53 The lungs and liver may be involvedsimultaneously or in tandem in many pathologicalprocesses. Chronic liver failure (cirrhosis) is mark-ed by pulmonary circulatory changes related topulmonary vasodilatation, arterio-venous shunt-ing and ventilation-perfusion inequality. Pulmon-ary oedema may complicate fulminant liver failure.Pleural effusion in cirrhotic patients is largely dueto defects in the diaphragm. Sclerotherapy foroesophageal varices has been associated with chestpain, pleural effusion and aspiration pneumonitis.The liver transplant patient develops lung pro-blems due to the surgical procedure, intensiveantibiotic therapy, poor cellular immunity andimmunosuppressive drug therapy.
Papworth Hospital, CambridgeThis hospital deserves a heading of its own becauseof the exciting transplant programme undertakenby its superb team. They have already recountedtheir early experience oflung transplantation in theJournal,54 but their continuing experience withheart-lung transplantation is even more impres-sive. The patients receiving heart-lung transplantssuffered from cystic fibrosis, bronchiectasis,sarcoidosis, histiocytosis X, fibrosing alveolitis,emphysema, Eisenmenger's syndrome and primarypulmonary hypertension (PPH). One patient withboth PPH and primary biliary cirrhosis underwenta triple organ transplant of heart, lungs and liver.Three main complications occur in longterm sur-vivors: opportunistic infections, acute pulmonaryrejection and chronic rejection causing disablingobliterative bronchiolitis.55 Transbronchial biopsy
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

10 D.G. JAMES & O. SHARMA
(TBB) has eliminated the need for endomyocardialbiopsy (EMB) in heart-lung recipients.56 AlthoughEMB is a safe procedure it is invasive and causesunnecessary discomfort. A switch from EMB toTBB has also resulted in significant economicsavings. TBB provides an early warning of rejec-tion so that intensive specific treatment may begiven early in the clinical course and decrease theincidence of obliterative bronchiolitis.57 At leastfour biopsies are recommended using a largeralligator forceps to obtain bigger samples of tissue.Following heart-lung transplantation, cytome-galovirus infection is the cause of considerablemortality and morbidity. It is recommended thatCMV antibody-negative recipients should receiveorgans only from antibody-negative donors. If adonor-recipient mismatch occurs, hyperimmuneglobulin and ganiclovir may improve survival.5
Occupational lung disease
Asbestos-related diseases
Asbestos is a family of crystalline hydrated silicateswith a fibrous geometry (defined as a ratio of lengthto diameter, or aspect ratio, of more than 3:1).Disorders associated with it are the subject of arecent exhaustive and authoritative review ofmesothelioma, lung cancer, cancer of the larynxand gastrointestinal tract, interstitial pulmonaryfibrosis, pleural fibrosis and plaques.59 The averagelatency period between the first exposure to as-bestos and the clinical diagnosis of malignantmesothelioma is 35 to 40 years, with most deathsoccurring in patients over 60 years of age.Advances in histochemistry, immunocytochemis-try and electron microscopy contribute to earlierand more accurate diagnosis if sufficient biopsymaterial is available. This means open thora-cotomy rather than cytological smears or needle-biopsy specimens. Bronchoalveolar lavage mayconfirm asbestos exposure. Asbestos appears to bea complete carcinogen, initiating interaction withcellular DNA to produce heritable changes in thegenetic material and also promoting the prolifera-tion and expansion of the initiated cells in a mannerthat encourages the development of malignancy.59Ear lobe oximetry discloses significant oxygendesaturation on exercise in asbestos patients.60Cobalt
For 40 years cases of interstitial pneumonia andbronchial asthma have been described in hardmetal workers, that is alloys of tungsten carbideand cobalt. A Belgian team has now recognizedand defined fibrosing alveolitis or hypersensitivitypneumonia due to cobalt in diamond cutters.61
Exposure is due to diamond cobalt discs used forpolishing diamonds. About 1% of those exposedpresent with bronchopulmonary lesions includingbronchial asthma and/or alveolitis. The diagnosisis established by lung biopsy or bronchoalveolarlavage, which reveals characteristic multinucleatedgiant cells. There are significant changes by specificinhalation provocation tests to cobalt or by lungfunction measurements at the place of work.Tungsten carbide does not produce pulmonarylesions but its association with cobalt intensifies theeffects of the latter.
Farmers' lungA Lancet editorial62 reviews respiratory symptomsin farmers in its broadest sense, including graindust, animal danders, unventilated pig house airand bacterial endotoxin. Atopy is a risk factor innovice seasonal workers. In terms of prevention,the main thrust is towards reducing dust exposureby ventilation and respirators.
Beryllium
Laser microprobe mass spectrometry (LAMMS)detects elements in low concentration and hasproved invaluable in identifying, amongst others,beryllium in organic tissue, and its recognition ingranulomas. There are few, if any rival techniques.Conventional histology sections, 5 im thick, areobtained with simple aniline dyes, preferablytoluidine blue, and viewed through a standardoptical microscope which enables the laser beam tobe directed to specific features. Fifty or more areasare examined in each section, yielding qualitativebut not quantitative results. In an extensive andelegant study,63 beryllium was detected in thegranulomas of patients with chronic berylliumdisease (CBD) but not in those with sarcoidosis orother granulomatous disorders. This exhaustivestudy also delineated the central birefringent cry-stals of Schaumann bodies and proved that thesecrystals are calcite and confirmed the presence ofcalcium and iron in the conchoidal bodies.Schaumann bodies persist in scarred lungs andtheir presence indicates previous granulomatousdisease.CBD is a hypersensitivity disease in which
beryllium is the specific class II-restricted antigen,stimulating local proliferation and accumulation inthe lung of beryllium-specific CD4 positive helper-inducer T cells. This study64 was made on T cellsobtained from peripheral blood and by broncho-alveolar lavage in 8 patients with CBD and 5healthy controls. The wider implications of thisstudy embrace comparison of the pathogenesis ofseveral granulomatous diseases including sarcoi-dosis and tuberculoid leprosy, in which antigen-
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

RESPIRATORY DISEASES 11
specific T cells at the site ofdisease have the CD4 +phenotype and are selectively granulomagenic. Inthe case of CBD, the CD4 + lung T cells areprimed to recognize beryllium specifically and toproliferate through the interleukin-2-interleukin-2receptor pathway onwards to granuloma forma-tion and to granulomatous interstitial fibrosis.Since CBD only develops in a fraction of workersexposed to beryllium, the terrain or soil ofthe CBDsufferer is surely all important in the developmentof this hypersensitivity disease.
Infections
Nosocomial infectionsIt is important to draw attention to a special articlefrom the Centers for Disease Control (CDC), whohave developed a new set of definitions for surveil-lance of nosocomial infections. Since it appears inthe American Journal of Infections Control65 itmight be missed and we might also have over-looked it but for this special annual research for theJournal. The definitions are based on severalimportant principles; the clinical findings andresults of laboratory tests, supported by X-raystudies, ultrasound examination, CT scan, endos-copy, biopsy, needle aspiration and magneticresonance. To be defined as nosocomial, the infec-tion is acquired in hospital even if it becomesevident after hospital discharge. It also includesnewborn infection as a result of passage throughthe birth canal. This report sets out authoritativelythe 23 criteria for nosocomial pneumonia, includ-ing symptoms and signs, chest X-ray abnormality,microbiology, histology and immunology. Thereare also criteria for lower respiratory tract infec-tion, excluding pneumonia, and the chest physicianwould also like to know the CDC criteria forcardiovascular system and throat infection. Thiswill become a widely quoted document on stan-dards and criteria.65
Human retroviruses
Semenzato and Agostini of Padua66 have clarifiedour understanding of human retroviruses and lunginvolvement. Bronchoalveolar lavage (BAL) hasopened a fresh window on the respiratory tractproviding information on host-lung defences fol-lowing invasion by members of the Retroviridaefamily of viruses. Retroviruses are schematicallycomposed of a characteristic dense icosahedralviral core containing two single strands of RNA,which, in turn, is surrounded by an envelopederived from the membrane of previous host cells.The viruses infect susceptible cells by means of aspecific interaction between viral envelope proteins
and normal cellular protein. Once inside the cell,viral particles containing RNA chains are used as atemplate for conversion to a double-stranded DNAby a reverse transcriptase. This backwards systemmakes retroviruses different from all other viruses;and hence the term Retroviridae. The DNAintermediate enters the nucleus and covalentlyintegrates into a chromosome of the host cell. Thisintegrated DNA sequence is termed provirus; itmay remain in this form throughout the life of thecell or it may pass on to daughter cells.
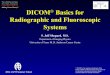
Alternatively, transcription of the integratedprovirus may result in synthesis of new RNAparticles in cytoplasm and thereafter exit from hostcells. This is the basic life cycle of this family ofhuman T leukaemic viruses (HTLV), which arenow prominently associated with various pulmon-ary disorders (Table I). The lungs are preferentialtargets for HIV infection. There is a selectivedepletion ofpulmonary CD4 subsets expressing T4epitopes with high affinity for HIV. This permitsPneumocystis carinii pneumonia, which is the com-monest cause of death in patients with AIDS. BALis now a good window for recognizing lymphocyticalveolitis in patients and carriers ofHTLV- 1, whichalso seems to have a special tropism for the lung.Semenzato's66 review is academic, thoughtful, bal-anced and a powerful stimulus for chest physiciansto collaborate closely with virologists, molecularbiologists and other basic research workers to solvemany of our present pulmonary problems.Pulmonary infection in AIDS is also comprehen-
sively covered in a report from Denver.67 It isanticipated that by 1991 the total number of casesof AIDS will increase to 270,000 with 179,000deaths, mainly as a result of pulmonary complica-tions. Cytomegalovirus is a major cause of mor-bidity almost always associated with reactivationrather than primary infection since the majorpopulation at risk of AIDS - homosexuals anddrug abusers - are nearly all virus carriers.6Examination ofinduced sputum is an easy, inexpen-sive and non-invasive technique for the diagnosis ofPneumocystis carinii pneumonia in patients withAIDS.9 In 40 consecutive patients with knownor suspected HIV infection sputum was producedby deep coughing induced by 3% saline via a jetnebulizer. The specimen was liquefied withdithiothreitol and cells were sedimented andstained. A total of28 patients were found to have P.carinii, which was detected in concentrated sputumin 21 of 38 patients, and by bronchoscopy in 25 of37 patients. Sensitivity of concentrated sputumcompared with bronchoscopy was 78% with anegative predictive value of 71%. Values forunconcentrated sputum were 43% and 48%respectively. Liquefaction of adequately inducedsputum facilitates processing and interpretationand increases yield for P. carinii, eliminating the
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

12 D.G. JAMES & O. SHARMA
Table I Human retroviruses and lung involvement
Retrovirus Alternative name Disorder
HTLV- I ATTLL (adult T Cutaneous T cell leukaemialeukaemia/ Tropical spastic paraparesislymphoma) Lung leukaemia
Progressive pulmonary fibrosis? Multiple sclerosis? Red cell aplasia? Malignant hypereosinophilic syndrome
HTLV- II ? Leukaemia
HTLV- III HIV 1 AIDSLAV Lymphoid interstitial pneumonitis
HTLV- IV MycosisHTLV- V FungoidesHIV-2 Immunodeficiency
? AIDS
need for invasive procedures in most patients. Thisstudy shows that sputum adequate for the diag-nosis of P. carinii can be obtained in most HIV-infected patients by using this simple technique.The process may in the future replace bronchos-copy and bronchoalveolar lavage as further studiesvalidate the test.70
Hydatid cyst
Hydatid cyst due to Echinococcus granulosus isparticularly common in rural Turkey with anincidence of 20 per million. This has providedconsiderable experience and an authoritativereport from Ankara of the surgical management of1055 cases of pulmonary hydatidosis.7' The prefer-red technique was aspiration of the cystic material,opening of the cyst with cautery (cystotomy),suction, removal of the germinative membrane,irrigation of the residual cavity, and then oblitera-tion of the space with pursestring sutures (capiton-nage). This conservative technique, preferred tomore radical measures was followed by a complica-tion rate of 3.8%, and an overall mortality of 1%.Chemotherapy with mebendazole was disappoint-ing, and is now only given to patients who areinoperable. If there are liver cysts, the thoracictranspleural approach is used to remove both lungand liver cysts. The Casoni skin test and bloodeosinophil count have been abandoned because oftheir low diagnostic yield and false negative results.Abdominal ultrasonography is routinely perform-ed to disclose liver cysts.
Therapeutics
Alpha-l-antitrypsin deficiencyThe hepatocyte synthesizes plasma proteins, in-cluding alpha-1-antitrypsin (al AT) which are dis-charged into the plasma. Falls in concentrationusually reflect decreased hepatic synthesis, and adefect ofa AT causes a well-recognized pattern ofemphysema and hepatic cirrhosis. It is an inhibitorof trypsin and other proteases so its deficiencycauses a tissue imbalance of protease-antiproteaseand severe pulmonary disease.
Its genetic control is by a single autosomaldominant gene responsible for 30 different alleleslabelled alphabetically, B to Z. The clinical pictureof emphysema clearly seen with the homozygousdeficiency ZZ is that of increasing dyspnoea andbasal emphysema in young smokers under 40 yearsof age. Death and severe ill-health is now beingbrought under control by weekly intravenousinfusions of human xal AT prepared from pooledplasma. The pioneering hard work done at theNational Institutes of Health, Bethesda, is now tobe matched by well designed trials conducted underthe auspices of European and North AmericanThoracic Societies.7 The present cost of weeklytreatment is about 20,000 US dollars annually(R. Crystal, personal communication).
Protriptyline
Protriptyline is a tricyclic antidepressant whichmay benefit patients with chronic obstructive lung
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

RESPIRATORY DISEASES 13
disease by influencing sleep architecture, reducingthe sleep-induced falls in arterial oxygen saturationand improving diurnal arterial oxygen tension.Controlled trials are necessary to confirm theseQuebec observations." Care should be exercised inits use in men because it causes dysuria and mayprecipitate urinary obstruction; and it causes drymouth in both sexes.
Protriptyline is also helpful in the managementof sleep apnoea, which has been well reviewed.74Sleep apnoea is a serious medical problem which isbeing diagnosed more frequently. The authors givea clear and concise definition of sleep apnoeafollowed by a description of obstructive sleepapnoea and a classification of the population atrisk. Investigations, including a full assessment byan otolaryngologist, measurement of overnightarterial oxygen desaturation and polysom-nography, are discussed. While evaluating theavailable medical and surgical management, theauthors emphasize that little attention had beenpaid to the psychological and psychiatric distur-bances resulting from the condition. Consider it inthe overweight heavy-drinking smoker becausethese factors demand immediate correction.Protriptyline is given in doses varying from 5 to30 mg daily. Much attention is now being given tothis problem as a cause of traffic accidents insleeping drivers, particularly weary long distancelorry drivers. Adrian Williams (personal com-munication) says that there is only one animalmodel for this disorder, namely the English bull-dog, a syndrome well-recognized by veterinarians.
Muscarinic receptor subtypes
Barnes" has contributed an elegant editorial on theimplications of muscarinic receptor subtypes forlung disease and a masterly classification andhelpful line drawings. Nobel Laureate Henry Daleshowed that acetylcholine produced two types ofresponse, which were mimicked by nicotine and bymuscarine, and that the muscarinic action wasblocked by atropine. Barnes has now brought usup-to-date with his classification of muscarinereceptors. M1 receptors may be found in para-sympathetic ganglia, M2 receptors on cholinergicnerves (autoreceptors) and M3 receptors on airwaysmooth muscle and mucus-secreting glands. Adefect in M2 receptor function may help to explain
why asthma may be induced by beta blockingdrugs. Ifyou have read this far then, read in full theoriginal editorial.
Conclusion
Bronchoalveolar lavage (BAL) is an exciting tech-nique which provides a new window on respiratorydisease. Through this window we have observedfresh phenomena which will influence our currentand future management of disease. Let us heed DrSemenzato ofPadua (page 11) who urges the chestphysician to hold hands with the virologist,molecular biologist and other basic researchworkers in a joint endeavour using such techniquesto solve many of our present pulmonary problems.It may help solve problems in transplantation as DrHiginbottom (Papworth) (page 12) indicates and asthe Center for Disease Control (Atlanta) finds(page 11) in reassessing nosocomial infections.BAL has proved helpful in the management ofAIDS, hypersensitivity pneumonitis, asbestosisand sarcoidosis.Wegener (page 4) has lived to see two major
advances since he first described this malignantgranulomatosis 53 years ago. A highly sensitive,specific and easily performed autoantibody test isdiagnostic, and will allow the disorder to berecognized at a much earlier stage. Secondly,treatment with steroids and cyclophosphamidehave reduced the mortality from 100% to 5%.
There has been a similar fundamental revolutionin the prognosis of cystic fibrosis (page 8). Whenthe Cystic Fibrosis Research Unit was launched 25years ago, about 90% of those born with thedisease died in early childhood, but now there is a75% chance of survival into adulthood. Thisimproved outlook is due to improved nutrition,new antibiotics, the development of specialmanagement centres and transplantation. There isfuture optimism based on genetic screening,chorionic villus sampling of fetal DNA permittingprenatal diagnosis in one day, and the establish-ment of a network of special regional units.Dr Schuster (page 3) argues persuasively that
positron emission tomography promises to be anattractive research technique for lung physiologistsof the future - and that is surely the way we shouldbe looking.
ReferencesTechniques
1. Plaza, V., Jimenez, P., Xaubet, A., Picado, C., Torres, A.,Agusti, C. & Agusti-Vidal, A. Bronchoalveolar lavage cellanalysis in patients with human immunodeficiency virusrelated diseases. Thorax 1989, 44: 289-291.
2. Lundgren, J.D., Orholm, M., Nielson, T.L., Iverson, J.,Hertz, J. & Nielson, J.O. Bronchoscopy of symptom-freepatients with human immunodeficiency virus for detection ofpneumocystis. Thorax 1989, 44: 68-69.
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

14 D.G. JAMES & 0. SHARMA
3. Spiteri, M.A. & Clarke, S.W. The nature of latent pul-monary involvement in primary biliary cirrhosis. Sar-coidosis 1989, 6: 107-110.
4. Morgenroth, A., Pfenffer, H.P., Austgen, M., Viereck, H.J.& Frendelenburg, F. Six years' experience with perthoraciccore needle biopsy in pulmonary lesions. Thorax 1989, 44:177-183.
5. Monaldi, V. Endocavitary aspiration: Its practical applica-tion. Tubercle 1946, 28: 223-228.
6. Ven, G.E., Williams, P.R. & Goldstraw, P. Intracavitarydrainage for bullous emphysematous lung disease:experience with the Brompton technique. Thorax 1988, 43:i 998-1002.
7. Shand, J., McCreath, G.T. & Monie, R.D.H. The use offine bore silastic catheters to drain carcinomatous pleuraleffusions. Br J Dis Chest 1988, 82: 394-397.
8. Lange, P., Mortensen, J. & Groth, S. Lung function 22 to35 years after treatment of idiopathic spontaneouspneumothorax with talc poudrage or simple drainage.Thorax 1988, 43: 559-561.
9. Kendrick, A.H., Oreilly, J.F. & Laszlo, G. Lung functionand exercise performance in hyperthyroidism before andafter treatment. Q J Med 1988, 68: 615-627.
10. Worth, H., Grahn, S., Lahomek, H.J., Bremer, G. &Goekenjan, G. Lung function disturbances versus res-piratory muscle fatigue in patients with systemic lupuserythematosus. Respiration 1988, 53: 81-90.
11. Laroche, C.M., Mulvey, D.A., Hawkins, P.N. et al. Diaph-ragm strength in the shrinking lung syndrome of systemiclupus erythematosus. Q J Med 1989, 265: 429-439.
12. Laroche, C.M., Moxham, J. & Green, M. Respiratorymuscle weakness and fatigue. Q J Med 1989, 265:373-397.
13. Quismorio, F. Clinical and pathological features of lunginvolvement in systemic lupus erythematosus. Semin RespirMed 1988, 9: 297-304.
14. Hoffbrand, B.I. & Beck, E.R. Unexplained dyspnoea andshrinking lungs in systemic lupus erythematosus. Br Med J1965, 1: 1273-1277.
15. Schuster, D.P. Positron emission tomography: therapy andits application to the study of lung disease. Am Rev RespirDis 1989, 139: 818-840.
Metabolic functions
16. Jenkinson S.G. (Guest Editor) Metabolic functions of thelung. Clin Chest Med 1989, 10: 1-128.
17. Hart, C.M. & Block, E.R. Lung serotonin metabolism.Clin Chest Med 1989, 10: 59-70.
18. Wright, J.R. & Hawgood, S. Pulmonary surfactantmetabolism. Clin Chest Med 1989, 10: 83-93.
19. Voelkel, N.F., Stenmark, K.R., Westcott, J.Y. & Chang,S.W. Lung eicosanoid metabolism. Clin Chest Med 1989,10: 93-105.
Wegener's granulomatosus
20. Socias, R. & Pozniak, A. In honour of Dr FriedrichWegener's eightieth birthday. Sarcoidosis 1988, 5:153- 154.
21. Wegener, F. On generalised septic vessel disease. Thorax1987, 42: 918-919.
22. Van der Woude, F.J., Rasmussen, N., Lobatto, S. et al.Autoantibodies against neutrophils and monocytes: toolfor diagposis and marker of disease activity in Wegener'sgranulomatosis. Lancet 1985, i: 425-429.
23. Gross, W.L. Wegener's granulomatosis. New aspects of thedisease course, immunodiagnostic procedures, and stage-adapted treatment. Sarcoidosis 1989, 6: 15-29.
24. Harrison, D.J., Simpson, R., Kharbanda, R., Abernethy,V.E. & Nimmo, G. Antibodies to neutrophil cytoplasmicantigens in Wegener's granulomatosis and other condi-tions. Thorax 1989, 44: 373-377.
25. Specks, U. & DeRemee, R.A. Significance of antibodies tocytoplasmic components of neutrophils. Thorax 1989, 44:369-370.
26. Nolle, B., Specks, U., Ludemann, J., Rohrbach, M.S.,DeRemee, R.A. & Gross, W.L. Anticytoplasmic autoanti-bodies: their immunodiagnostic value. Ann Intern Med1989, 111: 28-40.
27. Steppat, D. & Gross, W.L. Stage-adapted treatment ofWegener's granulomatosis. First results of a prospectivestudy. Klin Wochenschr 1989, 67: 666-671.
28. Gremmel, F., Druml, W., Schmidt, P. & Graninger, W.Cyclosporin in Wegener's granulomatosis. Ann Intern Med1988, 106: 491.
Adult respiratory distre sydrome
29. Rocker, G.M., Pearson, D., Stephens, M. & Shale, D.J.An assessment of a double-isotope method for the detec-tion of transferrin accumulation in the lungs of patientswith widespread pulmonary infiltrates. Clin Sci 1988, 75:47-52.
30. Stahlman, M.T. Medical problems in premature infants. NEngl J Med 1989, 320: 1551-1553.
31. Cummings, J.J., D'Eugenio, D.B. & Gross, S.J. A cont-rolled trial of dexamethasone in preterm infants at highrisk for bronchopulmonary dysplasia. N Engl J Med 1989,320: 1505-1510.
32. Cassady, G., Crouse, D.T., Kirklin, J.W. et al. A ran-domised, controlled trial of very early prophylactic ligationof the ductus arteriosus in babies who weighed 1000 G orless at birth. N Engl J Med 1989, 320: 1511-1516.
Asthma
33. Stenius-Aarniale, Piirila, P. & Teramo, K. Asthma andpregnancy: a prospective study of 198 pregnancies. Thorax1988, 43: 12-18.
34. White, R.J., Coutts, L.L., Gibbs, C.J. & Maclntyre, C. Aprospective study of asthma during pregnancy and thepuerperium. Respiratory Medicine 1989, 83: 103-106.
35. Ekstrom, K. & Tibbling, L. Gastro-oesophageal reflux andnocturnal asthma. Eur Respir J 1988, 1: 636-638.
36. Douglas, N.J. Nocturnal asthma. Q J Med 1989, 264:279-289.
37. James, A.L., Pare, P.D. & Hogg, J.C. The mechanics ofairway narrowing in asthma. Am Rev Resp Dis 1989, 139:242-246.
38. Roche, W.R., Beasley, R., Williams, J.H. & Holgate, S.T.Subepithelial fibrosis in the bronchi of asthmatics. Lancet1989, i: 520-523.
Interstitial pulmonary disease
39. Weissler, J.C. Southwestern Internal Medicine Conference.Idiopathic pulmonary fibrosis: cellular and molecularpathogenesis. Am J Med Sci 1989, 297: 91-104.
40. Hance, A.J., Cadranel, J., Solar, P. & Basset, F. Pul-monary and extrapulmonary Langerhans' cell granulo-matosis (Histiocytosis X). Semin Respir Med 1988, 9:349-368.
41. Pare, J.P., Cote, G. & Fraser, R.S. Longterm follow-up ofdrug abusers with intravenous talcosis. Am Rev Respir Dis1989, 139: 233-241.
42. Jederlinic, P.J., Sicilian, L. & Gaensler, E. Chroniceosinophilic pneumonia: a report of 19 cases and a reviewof the literature. Medicine 1988, 67: 154-162.
43. Loyd, J.E., Tillman, B.F., Atkinson, J.B. & Desprez, R.M.Mediastinal fibrosis complicating histoplasmosis. Medicine1988, 67: 295-310.
44. Hodson, M.E. Managing adults with cystic fibrosis. BrMed J 1989, 296: 471-472.
45. Geddes, D.M. Cystic fibrosis: future trends in care. Thorax1988, 43: 869-871.
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from

RESPIRATORY DISEASES 15
Lung cancer
46. Pearson, M. Is CT scanning essential in the pre-operativeassessment of lung cancer? Respir Med 1989, 83: 93-94.
47. Masson, R.G., Krikorian, J., Lukl, P., Evans, G.L. &McGrath, J. Pulmonary microvascular cytology in thediagnosis of lymphangitic carcinomatosis. N Engl J Med1989, 321: 71-76.
48. Gelb, A.F., Tashkin, D.P., Epstein, J.D., Szeftel, A. &Fairshter, A. Physiologic characteristics of malignantunilateral mainstem bronchial obstruction. Diagnosis andNd-YAG laser treatment. Am Rev Respir Dis 1988, 138:1382-1385.
49. Geddes, D.M. & Elliott, M. The solitary pulmonarynodule. Br Med J 1989, 298, 67-68.
50. Gibson, P.G., Bryant, D.H., Morgan, G.W. et al.Radiation-induced lung injury: a hypersensitivity pneu-monitis. Ann Intern Med 1988, 109: 288-291.
Transplantation
51. Cooper, J.D., Patterson, G.A., Grossman, R. & Maurer, J.Double lung transplant for advanced chronic obstructivelung disease. Am Rev Resp Dis 1989, 139: 303-307.
52. Wingard, J.R., Mellits, E.D., Sostrin, M.B. et al. Inter-stitial pneumonitis after allogeneic bone marrow transplan-tation: nine years' experience at a single institution.Medicine 1988, 67: 175-186.
53. Sherlock, S. The liver-lung interface. Semin Respir Med1988, 9: 247-253.
54. Higenbottam, T. & Wallwork, J. Transplantation of lungs.Postgrad Med J 1988, 64 (Suppl 4), 120-124.
55. Penketh, A.R.L., Higenbottam, T., Hutter, J., Coutts, C.,Stewart, S. & Wallwork, J. Clinical experience in the man-agement of pulmonary opportunist infection and rejectionin recipients of heart-lung transplants. Thorax 1988, 43:762-769.
56. Higenbottam, T., Hutter, J.A., Stewart, S. & Wallwork, J.Transbronchial biopsy has eliminated the need for endo-myocardial biopsy in heart-lung recipients. J Heart Trans-plantation 1988, 7: 435-439.
57. Hutter, J.A., Stewart, S., Higenbottam, T., Scott, J.P. &Wallwork, J. Histologic changes in heart-lung transplantrecipients during rejection episodes and at routine biopsy.J Heart Transplantation 1988, 7: 440-444.
58. Hutter, J.A., Scott, J., Wreghitt, T., Higenbottam, T. &Wallwork, J. The importance of cytomegalovirus in heart-lung transplant recipients. Chest 1989, 95: 627-631.
Occupational lung disease
59. Mossman, B.T. & Gee, J.B.L. Asbestos-related diseases. NEngi J Med 1989, 320: 1721-1730.
60. Britton, M.G., Apps, M.C.P., Maxwell, D.L., Hughes,D.T.D. & Hanson, A. The value of ear lobe oximetry inthe assessment of disability in asbestos-related disease.Respir Med 1989, 83: 43-49.
61. Eeckhout, A., Van Den, Verbeken, E. & Demedts, M. Lapathologie pulmonaire due au cobalt et aux metaux durs.Rev Mal Resp 1988, 5: 201-207.
62. Editorial. Respiratory symptoms in farmers. Lancet 1989,i: 1054-1055.
63. Jones Williams, W. & Wallach, E.R. Laser MicroprobeMass Spectrometry (LAMMS) analysis of beryllium, sar-coidosis and other granulomatous diseases. Sarcoidosis1989, 6: 111-117.
64. Saltini, C., Winestock, K., Kirby, M., Pinkston, P. &Crystal, R.G. Maintenance of alveolitis in patients withchronic beryllium disease by beryllium-specific helper Tcells. N Engl J Med 1989, 320: 1103-1109.
Infections
65. Carner, J.S., Jarvis, W.R., Emori, T.G., Horan, T.C. &Hughes, J.M. CDC definitions for nosocomial infections1988. Am J Infect Control 1988, 16: 128-140.
66. Semenzato, G. & Agostini, C. Human retroviruses and lunginvolvement. Am Rev Resp Dis 1989, 6: 1317-1322.
67. Cohn, D.L. Pulmonary infections in the acquired immunedeficiency syndrome. Semin Respir Med 1989, 10: 1-11.
68. Sissons, J.G.P. & Borysiewicz, L.K. Human cytomegalovirusinfection. Thorax 1989, 44: 241-246.
69. Zaman, M.K., Wooten, O.J., Subrahmanya, B. et al. Rapidnoninvasive diagnosis of Pneumocystis carinii from inducedliquefied sputum. Ann Intern Med 1988, 109: 7-10.
70. Leigh, T.R., Parsons, P., Hume, C., Husain, O.A.N., Gaz-zard, B. & Collins, J.V. Sputum induction for diagnosis ofPneumocystis carinii pneumonia. Lancet 1989, u: 205-206.
71. Dogan, R., Yuksel, M., Cetin, G. et al. Surgical treatment ofhydatid cysts of the lung; report on 1055 patients. Thorax1989, 44: 192-199.
Therapeutics
72. Editorial. Augmentation therapy in alpha-l-antitrypsindeficiency. Lancet 1988, i: II 19- 1120.
73. Series, F., Cormier, Y. & La Forge, J. Changes in day andnight time oxygenation with protriptyline in patients withchronic obstructive lung disease. Thorax 1989, 44: 275-279.
74. Prowse, K. & Allen, M.B. Sleep apnoea. Br J Dis Chest 1988,82: 329-340.
75. Barnes, P.J. Muscarinic receptor subtypes: implications forlung disease. Thorax 1989, 44: 161-167.
copyright. on January 25, 2020 by guest. P
rotected byhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.66.771.1 on 1 January 1990. Dow
nloaded from