Embed Size (px)
Citation preview
1
The mechanisms that bring about normal pulmonary functionare complex. The clinician must fully comprehend the physio-logic processes associated with respiratory disease of the infant.Only through advanced knowledge can the clinician effi-ciently assess and evaluate the newborn’s respiratory status.Systematic use of these assessment skills allows the clinician,as part of the collaborative team, to positively affect patientoutcome.
EMBRYOLOGIC DEVELOPMENT OF THE LUNGPulmonary development of the embryo proceeds along a pre-determined sequence throughout gestation (Greenough &Milner, 2005). Pulmonary development begins with formationof an outpouching of the embryonic foregut during the fourthweek of gestation and continues on to form sufficient alveoli to maintain gas exchange in most infants by 32 to 36 weeks of gestational age. Additional alveoli continue to develop inthe newborn infant and well into childhood, perhaps as late as the seventh year of life (Table 1-1). Sequential branching ofthe lung bud, which appears at about 4 weeks and is completeby the sixth week, marks the embryonic phase of lung devel-opment. The following 10 weeks are marked by the formationof conducting airways by branching of the aforementionedlung buds. This phase, the pseudoglandular phase, continuesthrough week 16 and ends with completion of the conductingairways. The canalicular phase follows through week 28, whengas exchange units, known as acini, develop. Type II alveolarcells, the surfactant-producing cells, begin to form during thelatter part of this phase. Mature, vascularized gas-exchangesites form during the saccular phase, which spans the 29ththrough 35th weeks. During this phase, the interstitial spacebetween alveoli thins, so respiratory epithelial cells tightlycontact developing capillaries. The alveolar development phase,marked by expansion of gas-exchange surface area, begins at 36 weeks and extends into the postnatal period. The alveolarwall and interstitial spaces become very thin, and the singlecapillary network comes into close proximity to the alveolarmembrane. No firm boundaries separate these phases, and gasexchange, albeit inefficient, is possible relatively early in gesta-tion, even before mature, vascularized gas-exchange sites form.
Lung development is a continuum that is marked by rapidstructural changes. Interference at any time by premature birthor by disease introduces the possibility of inducing iatrogenicdisease through intervention.
NEWBORN PULMONARY PHYSIOLOGY ANDTHE ONSET OF BREATHINGThe fetal lung is fluid filled, underperfused, and dormant withregard to gas exchange. The fetal lung receives only approxi-mately 10% of the cardiac output. Because the placenta is thegas-exchange organ in fetal life, a high blood flow is directedtoward it rather than to the lungs. Consequently, most of theright ventricular output is shunted from the pulmonary arteryacross the ductus arteriosus into the aorta, bypassing thepulmonary circulation.
Within moments after the umbilical cord is clamped, thenewborn undergoes an amazing transformation from a fetusfloating in amniotic fluid to an air-breathing neonate. Whenthe normal onset of breathing occurs, the ensuing chain ofevents converts the fetal circulation to the circulation patternof an adult. The lung fluid is absorbed and replaced with air,thus establishing lung volume and allowing for normalneonatal pulmonary function. The process of fetal lung fluidabsorption begins before birth when the rate of alveolar fluid secretion declines. Reabsorption speeds up during labor.Animal data suggest that as much as two thirds of the totalclearance of lung fluid occurs during labor. This clearanceprobably results from the cessation of active chloride secretioninto the alveolar space. Oncotic pressure favors the move-ment of water from the air space back into the interstitium andinto the vascular space. With the onset of breathing and lung expansion, water moves rapidly from the air spaces intothe interstitium and is removed from the lung by lymphaticand pulmonary blood vessels. Because a large portion of theclearance of lung fluid occurs during labor, neonates bornwithout labor after cesarean section are at particularly high riskfor delayed absorption of fetal lung fluid and thus for transienttachypnea of the newborn.
With the onset of breathing, highly negative intrathoracicpressures are generated with inspiratory efforts, filling the
Respiratory System
Javier Cifuentes • Waldemar A. Carlo
C h a p t e r 1
U N I T I
Systems Assessment and Management of Disorders
Ch01-X2942.qxp 11/22/06 2:49 PM Page 1

2 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
alveoli with air. Replacing alveolar fluid with air causes aprecipitous decrease in hydrostatic pressure in the lung;therefore, pulmonary artery pressure decreases, which lowerspressure in the right atrium and increases pulmonary bloodflow. These changes result in an increase in alveolar oxygentension (PaO2), causing constriction of the ductus arteriosus,which normally shunts right ventricular blood away from thelungs. By clamping of the cord, the large, low-resistance,placental surface area is removed from the circulation. Thischange in resistance causes an abrupt increase in systemicarterial pressure, reflected all the way back to the left atrium.As left atrial pressure rises, its flap valve closes the openingbetween the atria, known as the foramen ovale. This closureprevents blood from bypassing the lungs by eliminating theshunt across the foramen ovale from the right atrium to the leftatrium. As a result of closure of fetal pathways and the decreasein pulmonary vascular resistance, systemic pressure becomesgreater than pulmonary artery pressure. The infant successfullyconverts from the pattern of fetal circulation to neonatalcirculation when blood coming from the right ventricle flowsin its new path of least resistance (lower pressure) to the lungs,instead of shunting across the foramen ovale to the left atriumor across the ductus arteriosus from the pulmonary artery to the aorta.
Understanding ventilation enables the clinician to assessthe infant in respiratory distress and devise strategies formanagement. The respiratory system is composed of the fol-lowing: (1) the pumping system (the chest-wall muscles,diaphragm, and accessory muscles of respiration), which movesfree gas into the lungs; (2) the bony rib cage, which providesstructural support for the respiratory muscles and limits lungdeflation; (3) the conducting airways, which connect gas-exchanging units with the outside but offer resistance to gasflow; (4) an elastic element, which offers some resistance to gas flow but provides pumping force for moving stale gas outof the system; (5) air-liquid interfaces, which generate surfacetension that opposes lung expansion on inspiration butsupports lung deflation on expiration; and (6) the abdominalmuscles, which aid exhalation by active contraction.
Limitations in the respiratory system predispose the new-born to respiratory difficulty. The circular, poorly ossified ribcage, with a flat instead of angular insertion of the diaphragm,is less efficient at generating negative intrathoracic pressure to
move air into the system. Small muscles and a relative paucityof type I muscle fibers hinder the strength and endurance ofrespiratory muscles. The newborn has a relatively low func-tional residual capacity (lung volume at the end of exhalation)because the comparatively floppy chest wall offers little resis-tance to collapse, even when a normal amount of functionalsurfactant is present.
An alveolar cell known as the type II pneumocyte producespulmonary surfactant. Surfactant coats the alveoli, preventingalveolar collapse and loss of lung volume during expiration—that is, as expiration ensues and the lung deflates, the alveolardiameter becomes smaller. Surfactant coating of the alveolusreduces surface tension so that collapse is prevented and lesspressure is required to re-inflate it with the next inspiration.Neonates with respiratory distress syndrome (RDS) have sur-factant deficiency. In the absence of surfactant, surface tensionis high, and the tendency is toward collapse of alveoli at endexpiration.
Surface tension is the force that arises from the interactionamong the molecules of a liquid. Molecules in the interior ofthe liquid bulk are attracted to each other, but molecules onthe surface of the liquid are attracted to other molecules in the interior of the liquid, which results in the movement of thesurface molecule toward the bulk of the liquid. This explainswhy a droplet of water over a surface tends to adopt a given size and not continuously expand. If we think of the alveolusas a soap bubble, the molecules of the wall of the bubble areattracted to each other, which tends to collapse the bubble.The pressures across the wall of the bubble act against thesurface tension and avoid the collapse of the bubble. The rela-tionship between the surface tension and the distending pres-sures and the pressure across the wall of the bubble aredescribed by Laplace’s law, as shown in the following equation:
P = 2 ST/r
P is pressure, ST is surface tension, and r is radius of thealveolus. It is difficult to inflate a small or collapsed alveolusbecause it has a very small diameter. As its volume increases,the pressure needed to continue inflation becomes progres-sively less—that is, compliance of the alveolus and thus com-pliance of the lung has improved. Coating the alveoli with anagent that decreases surface tension reduces the effort requiredto inflate the lungs from a low volume. Pulmonary surfactant isa surface tension–reducing mixture of phospholipids andproteins found in mature alveoli. Surfactant coats the alveoli.
Compliance is the elasticity, or distensibility, of the lung. Itis expressed as the change in volume caused by a change inpressure as follows:
CL = V/P
CL is compliance of the lung; V is volume; and P is pressure.The higher the compliance, the larger the volume delivered tothe alveoli per unit of applied inspiratory pressure. Surfacetension and compliance are particularly important in the pre-term infant with RDS. Surface tension is a force that opposeslung expansion. Surfactant deficiency leads to increased surfacetension in the alveoli. Lungs with higher surface tension aremore difficult to inflate. During expiration, some alveoli col-lapse. This results in a decreased lung volume at the end ofexpiration (low functional residual capacity). Clinically, the
Phase Timing Major Event
Embryonic Weeks 4 to 6 Formation of proximal airway
Pseudoglandular Weeks 7 to 16 Formation of conducting airways
Canalicular Weeks 17 to 28 Formation of aciniSaccular Weeks 29 to 35 Development of gas-
exchange sitesAlveolar Weeks 36 through Expansion of surface
postnatal life area
Stages of Normal Lung GrowthTABLE 1-1
Ch01-X2942.qxp 11/22/06 2:49 PM Page 2

presence of retractions and other signs of respiratory distressmanifest the effects of this increased surface tension.Respiratory muscles contract to inflate the lungs against thesurface tension that acts in the opposite direction. The nega-tive pleural pressure easily deforms the floppy thoracic wall of the preterm infant. When a preterm infant with RDS isintubated, a high peak inspiratory pressure (PIP) is required toexpand the thorax (i.e., tidal volume is obtained only with ahigh change in pressure). After surfactant is administered, chestexpansion increases with the same PIP. This effect (increasedcompliance) is due to a decrease in surface tension (i.e., asmaller force opposing lung distention). Thus the tidal volumeobtained with the same PIP is increased. Before surfactant isadministered, it is very difficult to inflate the lung becausecompliance is low. After surfactant is administered, surfacetension decreases, and it becomes easier to inflate the lung(i.e., compliance is improved).
Resistance is a term used to describe characteristics of gasflow through the airways and pulmonary tissues. Resistancecan be thought of as the capacity of the lung to resist airflow.The principal component of resistance is determined by thesmall airways. Pressure is required to force gas through the airways (airway resistance) and to overcome the forces of the lung and chest wall, which work to deflate therespiratory system (tissue resistance). At a specific flow rate,resistance is described by the following equation:
R = P1 – P2 / V.
P1 and P2 are pressures at opposite ends of the airway, and V.
is the flow rate of gas (volume per unit of time). Resistanceincreases as airway diameter decreases. Because the infant hasairways of relatively small radius, the resistance to gas flowthrough those airways is high. The time constant is the timenecessary for airway pressure to partially equilibrate through-out the respiratory system and equals the mathematic productof compliance and resistance. In other words, the time con-stant is a measure of how quickly the lungs can inhale orexhale. The time constant (Kt) is directly related to both com-pliance (C) and resistance (R). This relationship is describedby the following equation:
Kt = C × R
An infant with RDS has decreased compliance, so the timeconstant of the respiratory system is relatively short. In such an infant, little time is required for pressure to equilibrate be-tween the proximal airway and alveoli, so short inspiratory andexpiratory times may be appropriate during mechanical venti-lation. When compliance improves (increases), however, thetime constant becomes longer. If sufficient time is not allowedfor expiration, the alveoli may become overdistended, and anair leak may result.
Blood Gas Analysis and Acid-Base BalanceOxygen diffuses across the alveolar-capillary membrane,moved by the difference in oxygen pressure between thealveoli and the blood. In the blood, oxygen dissolves in theplasma and binds to hemoglobin. Thus arterial oxygen content(CaO2) is the sum of dissolved and hemoglobin-bound oxygen,as is shown by the following equation:
CaO2 = (1.37 × Hb × SaO2) (0.003 × PaO2)
CaO2 is arterial oxygen content (ml/100 ml of blood); 1.37is the milliliters of oxygen bound to 1 g of hemoglobin at 100%saturation; Hb is hemoglobin concentration per 100 ml ofblood (g/100 ml); SaO2 is the percentage of hemoglobin boundto oxygen (%); 0.003 is the solubility factor of oxygen inplasma (ml/mm Hg); and PaO2 is oxygen partial pressure in arterial blood (mm Hg).
In the equation for arterial oxygen content, the first term—(1.37 × Hb × SaO2)—is the amount of oxygen bound tohemoglobin. The second term—(0.003 × PaO2)—is the amountof oxygen dissolved in plasma. Most of the oxygen in the bloodis carried by hemoglobin. For example, if a premature infanthas a PaO2 of 60 mm Hg, an SaO2 of 92%, and a hemoglobinconcentration of 14 g/100 ml, then CaO2 is the sum of oxygenbound to hemoglobin (1.37 × 14 × 92/100) = 17.6 ml, plus theoxygen dissolved in plasma (0.003 × 60) = 0.1 ml. In thistypical example, only less than 1% of oxygen in blood isdissolved in plasma; more than 99% is carried by hemoglobin.If the infant has an intraventricular hemorrhage and thehemoglobin concentration decreases to 10.5 g/dl but PaO2 andSaO2 remain the same, then CaO2 (1.37 × 10.5 × 92/100) +(0.003 × 60) equals 13.4 ml/100 ml of blood. Thus, withoutany change in PaO2 or SaO2, a 25% decrease in hemoglobinconcentration (from 14 to 10.5 g/dl) reduces the amount ofoxygen in arterial blood by 24% (from 17.6 to 13.4 ml/100 mlof blood). This is an important concept for clinicians who carefor patients with respiratory disease. SaO2 and hemoglobinshould be monitored and, if low, corrected to keep an adequatelevel of tissue oxygenation. Besides SaO2 and hemoglobin,cardiac output is the other major determination of oxygendelivery to the tissues.
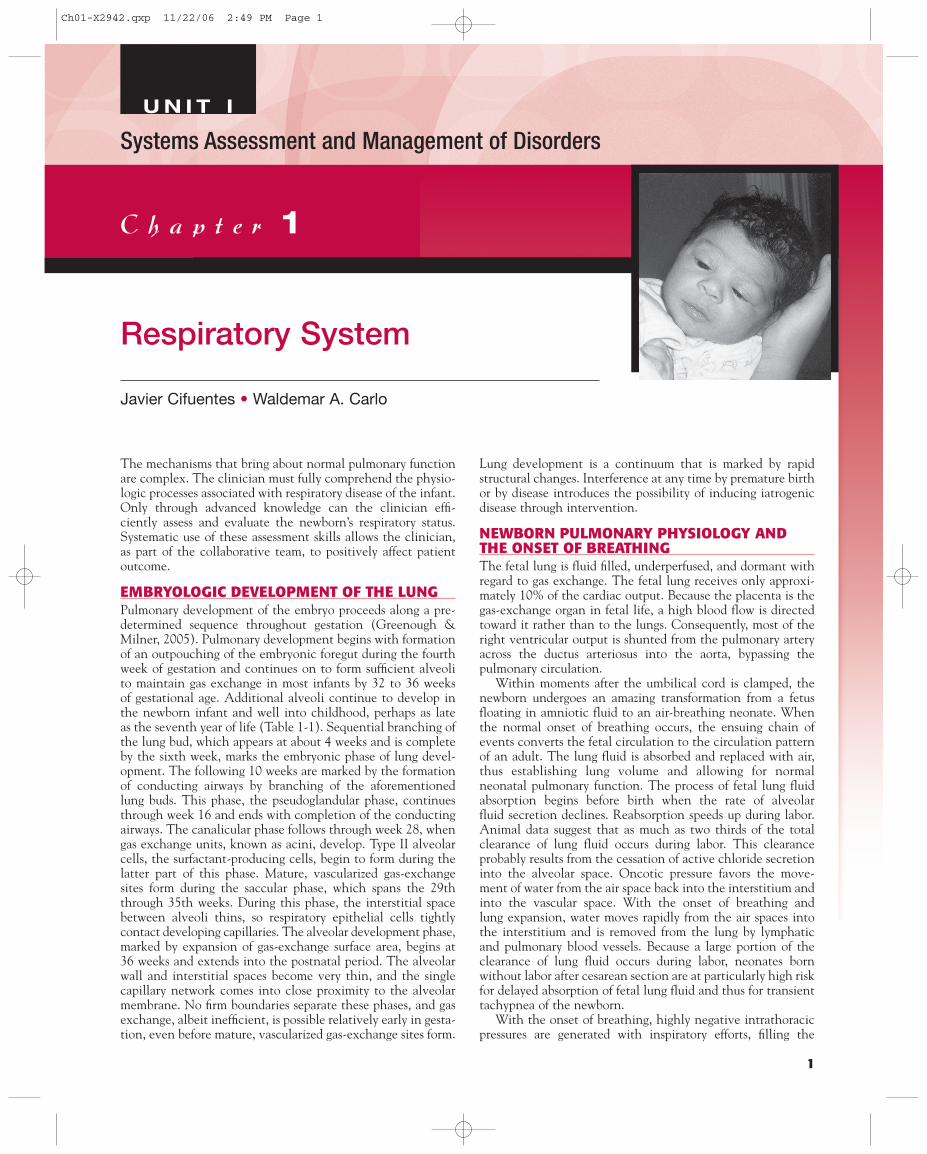
The force that loads hemoglobin with oxygen in the lungsand unloads it in the tissues is the difference in partial pressureof oxygen. In the lungs, alveolar oxygen partial pressure ishigher than capillary oxygen partial pressure so that oxygenmoves to the capillaries and binds to the hemoglobin. Tissuepartial pressure of oxygen is lower than that of the blood, sooxygen moves from hemoglobin to the tissues. The relation-ship between partial pressure of oxygen and hemoglobin isbetter understood with the oxyhemoglobin dissociation curve (Figure 1-1). Several factors can affect the affinity ofhemoglobin for oxygen. Alkalosis, hypothermia, hypocapnia,and decreased levels of 2,3-diphosphoglycerate (2,3-DPG)increase the affinity of hemoglobin for oxygen (as shown inFigure 1-1 by a left shift of the curve). Acidosis, hyperthermia,hypercapnia, and increased 2,3-DPG have the opposite effect,decreasing the affinity of hemoglobin for oxygen, so that thehemoglobin dissociation curve shifts to the right. This charac-teristic of hemoglobin facilitates oxygen loading in the lungand unloading in the tissue, where the pH is lower and alveolarcarbon dioxide tension (PaCO2) is higher. Fetal hemoglobin,which has a higher affinity for oxygen than adult hemoglobin,is more fully oxygen-saturated at lower PaO2 values. This isrepresented by a left shift on the curve of dissociation ofhemoglobin.
Once loaded with oxygen, the blood should reach the tissuesto transfer oxygen to the cells. Oxygen delivery to the tissuedepends on cardiac output (CO) and CaO2, as described in thefollowing equation:
Oxygen delivery = CO × CaO2
3CHAPTER 1 Respiratory System
Ch01-X2942.qxp 11/22/06 2:49 PM Page 3
In the case of the infant discussed previously, increased COcompensates for the decrease in CaO2 that results fromanemia. The key concept is that when a patient’s oxygenationis assessed, more information than just PaO2 and SaO2 shouldbe considered. PaO2 and SaO2 may be normal, but, if hemo-globin concentration is low or CO is decreased, oxygendelivery to the tissues is decreased. With this approach, theclinician should be able to better plan the interventionsneeded to improve oxygenation.
As in the adult, the acid-base balance in the neonate ismaintained within narrow limits by complex interactions be-tween the pulmonary system (which eliminates carbondioxide) and the kidneys (which conserve carbon dioxide andeliminate metabolic acids). Carbon dioxide elimination,which is more efficient than oxygenation across the alveolarcapillary membrane, is usually not as problematic asoxygenation. Carbon dioxide has a high solubility coefficient,so cellular diffusion is efficient and no measurable partialpressure gradient exists between venous blood and the tissues.Therefore elevated carbon dioxide tension (PCO2) values inarterial blood samples nearly always indicate ventilatorydysfunction. Dissolved carbon dioxide moves rapidly acrosscell membranes of peripheral chemoreceptors, thereby makingthem sensitive to changes in ventilation. Increased intra-cellular PCO2 elevates the cellular hydrogen ion concentra-tion as carbon dioxide combines with water to form carbonicacid. This stimulates neural impulses to the medulla, which inturn stimulates respiration. However, excessively high PCO2levels can depress ventilation. Acid-base balance is controlledby homeostatic mechanisms and is expressed by the followingequation:
pH = 6.1 + log HCO3–/0.03 × PCO2
It can be seen from this mathematical relationship thatacid-base balance depends on the interplay of bicarbonate ion(HCO3
–) and carbon dioxide (CO2). Serum pH is tightlyregulated in the normal range. Low pH (in other words,acidosis) can contribute to vasoconstriction and can result in
worsening hypoxemia caused by extrapulmonary shunt acrossthe ductus or foramen ovale. A pH of less than 7.0 is not welltolerated and is associated with a poor survival rate in thesepatients.
If PaCO2 rises above normal, as in hypoventilation, pHdeclines and the patient suffers from respiratory acidosis. The patient with a chronic respiratory acidosis may retainbicarbonate, thus self-inducing a compensatory metabolicalkalosis. A patient who is hyperventilated with a low PaCO2has respiratory alkalosis. Depressed bicarbonate ion con-centration (less than approximately 20 mmol/L in plasma) iscalled metabolic acidosis and can be associated with any causeof anaerobic metabolism, such as poor CO from congenitalheart disease—for example, hypoplastic left heart syndrome orsevere aortic coarctation—or from myocardial ischemia, myo-cardiopathy, myocarditis, hypoxia, or septic shock. Metabolicacidosis that results from renal bicarbonate wasting commonlydevelops in extremely immature infants. Less common causesfor prolonged and severe metabolic acidosis are the inbornerrors of metabolism, including urea-cycle defects andaminoacidopathies.
The clinician should become proficient at interpretingblood gas data. With knowledge of the accepted normal valuesand definitions of the simple blood gas disorders and theircompensatory mechanisms, the clinician can examine data in light of the disease process and interpret blood gas values ina fairly straightforward manner. Normally, the body does notovercompensate for a pH above or below the normal range.Therefore, when presented with an abnormal pH, the clinicianrapidly determines whether acidosis (Figure 1-2, A) or alkalosis(Figure 1-2, B) exists. An examination of PaCO2 and HCO3
–
determines whether the process is respiratory, metabolic, ormixed. The clinician should determine which derangementoccurred first. For example, an acidotic, acutely ill hypoxemicinfant with a high PaCO2 and depressed HCO3
– is usuallyhypoventilating and suffering metabolic acidosis secondary toanaerobic metabolism. The infant with a low PaCO2 is hyper-ventilating, either spontaneously or secondary to overzealousmechanical ventilation. A concomitantly low pH and lowPaCO2 indicate that the infant is compensating for metabolicacidosis with hyperventilation in an effort to normalize thepH. A pure metabolic alkalosis with high pH is nearly alwayscaused by bicarbonate administration. Infants with broncho-pulmonary dysplasia usually have a compensated respiratoryacidosis, with an elevated PaCO2 and concomitantly elevatedHCO3
–. The pH may be in the normal range or slightlyacidotic. A severely depressed pH usually indicates acutedecompensation.
ASSESSMENT OF THE NEONATE WITHRESPIRATORY DISTRESSThe assessment of a neonate with respiratory distress shouldalways begin with the compilation of a detailed perinatalhistory. In many cases, the history is difficult to obtain, espe-cially when the infant has been transferred from one center toanother, often with incomplete records. Even so, every effortshould be made to obtain as much pertinent information aspossible. The clinician is often able to gain important supple-mental information from the father or visiting relatives at thebedside. A review of the maternal-perinatal history and a com-plete physical examination, combined with a limited labora-tory and radiologic evaluation, leads to a timely diagnosis in
4 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
100
80
60
40
20
00 20 40 60 80 100 120 600
°CpH
Paco2
DPG
°CpHPaco2
DPGA
dult
Neo
nata
l
PO2 mm Hg
Hb
O2
Sat
ura
tio
n (
%)
FIGURE 1-1Oxyhemoglobin equilibrium curves of blood from term infants atbirth and from adults (at pH 7.40).
Ch01-X2942.qxp 11/22/06 2:49 PM Page 4

most circumstances. Many neonatal diseases, including manywith nonpulmonary origins, may manifest with signs of respi-ratory distress. Therefore a comprehensive differential diagnosismust be considered (Figure 1-3).
HistoryIn most situations, data from a patient’s history can direct theclinician to the correct diagnosis of neonatal respiratorydistress. The prenatal record should be reviewed carefully forpossible causes of the infant’s difficulties. The mother’s age,gravidity, parity, blood type, and Rh status should be recorded.The obstetrician’s best estimate of gestational age should bedocumented as determined by first-trimester ultrasound or lastmenstrual period. Ultrasonography often provides informationrelated to anomalies, which is useful in the anticipation ofrequired support at birth. Historical information such asprevious preterm birth is relevant as it is often associated withan increased risk of premature delivery in subsequentpregnancies. Because excessive maternal weight gain occurswith diabetes, multiple gestation, or polyhydramnios, pre-pregnancy weight and total gain should be noted. Theclinician is often alerted to the possibility of gestationaldiabetes with abnormal glucose tolerance screening results,which will be reflected in the prenatal record.
The duration of membrane rupture, the presence ofmaternal fever with or without accompanying amnionitis, andthe presence of meconium-stained amniotic fluid are impor-tant pieces of information that may help in the differentialdiagnosis of a newborn with respiratory distress. Additionally,antepartum and intrapartum administration of certain medica-tions may affect diagnosis and management of these infants.
Administration of steroids to the mother reduces the likeli-hood that RDS will develop in the infant; administration ofnarcotics to the mother close to delivery may result in poorrespiratory effort by an otherwise normal infant.
Physical Examination of the Respiratory SystemOne or more of the major signs of respiratory difficulty (e.g.,cyanosis, tachypnea, grunting, retractions, and nasal flaring)are usually present in neonates with both pulmonary and non-pulmonary causes of respiratory distress. Observation ofthe distressed infant with the unaided eye and ear is theclinician’s first step in the physical assessment. Cyanosis maybe central, as caused by pulmonary disease and cyanotic heartdisease, or peripheral, as occurs in conditions with impairedCO. Tachypnea typically manifests infants with decreased lungcompliance, such as RDS, whereas patients with high airwayresistance (e.g., airway obstruction) usually have deep but slowbreathing. Grunting is produced by an adduction of vocalcords during expiration. Grunting holds gas in the lungsthroughout expiration, which helps maintain lung volume andavoid alveolar collapse. At the end of expiration the gas isreleased and rapidly propelled, causing an audible grunt.Grunting is more typical of infants with decreased functionalresidual capacity, such as preterm infants with RDS. Chest wallretractions occur more often in very premature infants becauseof the highly compliant chest wall (Bates & Balistreri,2002).When the infant is intubated, observation of the chestgives important information. Careful observation of chest wallexcursions produced by the ventilator allows the clinician toadjust the magnitude of the ventilator pressure so that optimalgas exchange is achieved while risk of barotrauma is mini-
5CHAPTER 1 Respiratory System
AcidosisLow pH
Mixed
RespiratoryHigh Pco2
Normal Pco2Low Pco2 High HCO3Normal HCO3
MetabolicLow HCO3
No compensation No compensation CompensationCompensation
A
ACID-BASE BALANCEDIAGNOSTIC APPROACH
MixedRespiratoryHigh Pco2
Normal Pco2High Pco2 Low HCO3Normal HCO3
MetabolicLow HCO3
No compensation No compensation CompensationCompensation
B
AlkalosisHigh pH
FIGURE 1-2Acid-base balance: diagnostic approach. A, Low pH. B, High pH.
Ch01-X2942.qxp 11/22/06 2:49 PM Page 5

mized. The chest of an intubated infant should move the sameor only slightly less than that of a healthy spontaneouslybreathing infant. The clinician should assess the appropri-ateness of the magnitude of the chest expansion in ventilatedpatients. The nurse should assess for and report changes inchest rise in an intubated infant. Abrupt decreases in the chestrise may indicate atelectasis, a plugged endotracheal tube, apneumothorax, or ventilator failure. Slow decreases in thechest rise over the hours may indicate a deteriorating lungcompliance or gas trapping. An overinflated thorax, as deter-mined from radiographs, is a sign of gas trapping. In the intu-bated infant, this observation should prompt the clinician toadjust the positive end-expiratory pressure (PEEP) or expira-tory time so that gas trapping and air leakage are prevented.An anguished intubated infant with cyanosis and gaspingefforts may have endotracheal tube obstruction.
Careful attention should be given to the sounds that emanatefrom the respiratory tract, as variations in quality often aid inlocalization of the source of respiratory distress. Stridor iscommon in neonates with upper airway and laryngeal lesions.Inspiratory stridor occurs most often with upper airway andlaryngeal lesions, whereas expiratory stridor suggests lower airwayproblems. Hoarseness is a common sign of laryngeal disorders.Forced inspiratory efforts may indicate upper airway or laryngealinvolvement, whereas expiratory wheezes suggest a lower airwaydisease. Congenital airway disorders that may cause respiratorydistress in the neonate are included in Figure 1-3.
Auscultation of the chest further aids the examiner.Because infants with RDS have low lung volumes, breathsounds are faint, usually without rales. In comparison, theinfant with pneumonia may have rales indicative of alveolarfilling. Auscultation allows the clinician to detect the presenceof secretions in the airway and to evaluate the response tophysiotherapy and suctioning. Rhonchi may be heard inneonates with airway disease, such as meconium aspirationsyndrome (MAS). Unequal breath sounds may be due to a
pneumothorax or to one of the many causes of diminishedventilation to a lung lobe (e.g., atelectasis, main-stem bron-chial intubation, and pleural effusion). A shift of the apex ofthe heart can occur with a pneumothorax, diaphragmatichernia, unilateral pulmonary interstitial emphysema, pleuraleffusion, or atelectasis, which may be differentiated by transillumination of the chest. Dullness to percussion may bedue to a pleural effusion or solid mass. Muffled heart tonessuggest a pneumopericardium. Respiratory distress may occurin many chest wall disorders that restrict rib-cage movements.Increased oral secretions and choking with feedings are com-mon in neonates with a tracheoesophageal fistula. Becausenewborns are obligate nasal breathers, those with choanalatresia typically improve with crying and have worsening respi-ratory distress with rest and feeding. Characteristic Potterfacies and other compression deformities and contractures maybe present in neonates with hypoplastic lungs secondary tooligohydramnios.
Examination of the cardiovascular system and assessment ofperipheral perfusion yield many clues toward a diagnosis.Pallor and poor perfusion may indicate anemia, hypotension,or hypovolemia. Polycythemia with plethora may also causerespiratory distress. Cardiovascular signs of congestive failure(e.g., hyperactive precordium, tachycardia, and hepato-megaly), poor CO, pathologic murmurs, decreased femoralpulses, and nonsinus rhythm suggest a primary cardiac causefor the respiratory distress.
When hypotonia, muscle weakness, or areflexia accom-panies respiratory distress, a neuromuscular cause should beconsidered (Box 1-1). In such cases, an accompanying historyof less frequent fetal movement often is involved. Sometimes ahistory of muscular disease exists in the family. Brachial plexusinjury or fracture of a clavicle may accompany phrenic nerveinjury and diaphragm paralysis.
Abnormalities found on abdominal examination en-lighten the examiner to other causes of respiratory difficulty.
6 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Respiratory distress sydromeTransient tachypneaPneumoniaAspiration syndromesPneumothorax and other air leaksPulmonary edemaPleural effusionPulmonary hemorrhage
Diaphragmatic herniaTracheoesophageal fistulaCysts and tumorsCongenital lobar emphysemaPulmonary hypoplasiaAccessory or sequestered lobesPulmonary lymphangiectasiaPulmonary arteriovenous fistula
Common Uncommon
Yes NoAbnormallungs by chest
radiograph
Neonate with Acute Respiratory Distress
AnemiaPolycythemiaHypotensionHypovolemia
AsphyxiaIntracranial hemorrhageNeuromuscular disorders Drugs
Chest wall disordersDiaphragmatic disorders
Upper airwayLaryngealLower airway
Persistent fetal circulationCyanotic congenital heart diseaseCongestive heart failure
AscitesNecrotizing enterocolitisAbnormal massOmphaloceleGastroschisis
SepsisAcidosisHypothermia (cold stress)HyperthermiaHypoglycemiaMethemoglobinemia
Abnormalities in
OtherfindingsAirway
findings
PerfusionBP,HCT
CVSfindingsor echo
Abdominalfindings
Neuro-muscularfindings
Diaphragmor chest
wall
FIGURE 1-3Neonate with acute respiratory distress.
Ch01-X2942.qxp 11/22/06 2:49 PM Page 6

Abdominal distention that results from causes such as ascites, necrotizing enterocolitis, abdominal mass, ileus, ortracheoesophageal fistula can cause respiratory distress,whereas a scaphoid configuration of the abdomen suggests adiaphragmatic hernia.
Other nonpulmonary disorders such as sepsis, metabolicacidosis, hypothermia, hyperthermia, hypoglycemia, andmethemoglobinemia may also cause respiratory distress in theneonate.
Radiographic and Laboratory InvestigationRadiographic examination is often the most useful part of thelaboratory evaluation and may serve to narrow the differentialdiagnosis. An anteroposterior view is usually sufficient, but alateral chest radiograph may be useful when fluid, masses, orfree air is suspected. Other diagnostic imaging techniques(ultrasonography, fluoroscopy, computed tomography, or mag-netic resonance imaging) may be helpful in selected patients.Bronchoscopy allows direct visualization of the upper airway.This technique, albeit invasive and technically difficult, mayin selected cases be a great aid in the differential diagnosis andtreatment of patients with a suspected airway lesion.
Much can be learned from a relatively small battery oflaboratory tests. In the NICU setting, the clinician is oftenrequired to collect specimens for and interpret the results ofphysiologic testing. Considerable skill is required in samplingboth venous and arterial blood from small patients who are atsubstantial risk for iatrogenic anemia and vascular damage.Ideally, the hospital laboratory is equipped to do most routinetests on microliter quantities of blood. The clinician mustmonitor total quantities of blood sampled from the infant andbe alert to the development of iatrogenic anemia.
Analysis of arterial blood for pH and gas tensions is perhapsone of the most common tasks of the clinicians caring for theinfant with respiratory illness. Noninvasive methods to assessgas exchange, such as transcutaneous blood gas measurementsor oxygen saturation, are very useful. Because oxygen deliveryto the tissues so intimately depends on circulating red bloodcell volume, a hematocrit should be performed.
COMMON DISORDERS OF THE RESPIRATORYSYSTEMA large variety of disorders may afflict neonates. The mostcommon disorders are discussed here. Figure 1-3 lists both pul-monary and non-pulmonary disorders that cause respiratory
symptoms in the newborn infant. Several diseases may startlater in the neonatal period and extend into infancy (Box 1-2).The most common is bronchopulmonary dysplasia (BPD), achronic lung disease that affects newborns, mainly prematureinfants exposed to mechanical ventilation and oxygen for RDSor other respiratory problems.
Respiratory Distress Syndrome (RDS)RDS, or hyaline membrane disease (the term hyaline membranedisease originated from the histological observation of alveolarspace lined by an eosinophilic membrane formed by cellulardebris), is the most common cause of respiratory distress inpremature neonates (Bates & Balistreri, 2002). RDS occurs inabout 10% of all premature infants in the United States(American Lung Association [ALA], 2006). Fifty to sixtypercent of infants born before 29 weeks’ gestation have RDS(ALA, 2006; Lemons et al, 2001) and account for thousands ofpatient days in the NICUs and millions of dollars in healthcare expenditures. In rare cases, RDS develops in full-terminfants born to mothers with diabetes or in full-term infantswho have experienced asphyxia. RDS is progressively morecommon the lower the infant’s gestational age.
Antenatal SteroidsAcceleration of lung maturation with antenatal steroids is nowthe standard of care in women with preterm labor of up to 34 weeks. Antenatal corticosteroid therapy to the mothers ofpreterm fetuses of up to 34 weeks significantly reduces theincidence of RDS with odds ratios of around 0.5 and decreasesmortality, with odds ratios of around 0.6. Subgroup analysesconfirm that these benefits occur regardless of race and gender.No adverse effects have been reported with the usual singlecourse of antenatal steroids.
TreatmentThe lung is deficient in pulmonary surfactant, the surfacetension–reducing agent that prevents alveolar collapse at endexpiration and loss of lung volume. Treatment with surfactantis quite effective (see Chapter 2). Progressive atelectasis leadsto intrapulmonary shunting, owing to perfusion of unventi-lated lung, and subsequent hypoxemia. The radiograph displaysa characteristic ground glass, reticulogranular appearance withair bronchograms. When the lung inflation is poor, the arterialblood gas analysis usually reveals respiratory acidemia as well ashypoxemia.
7CHAPTER 1 Respiratory System
BOX 1-1
Neuromuscular Disorders That May CauseRespiratory Distress in the Neonate
MyopathiesMyasthenia gravisWerdnig-Hoffmann diseaseSpinal cord disorderPoliomyelitisOthers
Adapted from Battista MA, Carlo WA (1992). Differential diagnosisof acute respiratory distress in the neonate. Tufts University School ofMedicine and Floating Hospital for Children reports on neonatalrespiratory diseases 2(3):1-4, 9-11.
BOX 1-2
Causes of Late Respiratory Distress in theNeonate
Bronchopulmonary dysplasiaPneumonia (bacterial, viral, or fungal)Congestive heart failureRecurrent pneumonitis or aspirationUpper airway obstructionWilson-Mikity syndromeIdiopathic pulmonary fibrosis (Hamman-Rich syndrome)Pulmonary lymphangiectasiaCystic fibrosisImmature lungs
Ch01-X2942.qxp 11/22/06 2:49 PM Page 7

Therapy is directed toward improving oxygenation as wellas maintaining optimal lung volume. Continuous positive air-way pressure (CPAP) or positive end-expiratory pressure(PEEP) is applied to prevent volume loss during expiration. Insevere cases, mechanical ventilation via tracheal tube isrequired. Exogenous surfactants (artificial and natural), whichare available for intratracheal instillation, improve survivaland reduce some of the associated morbidity of RDS. Theearlier surfactant is administered, the better the effect on gasexchange. Clinical trials indicate that prophylactic surfactantadministration to extremely premature infants in the deliveryroom is more effective than waiting for the treatment afterdevelopment of RDS (Soll & Morley, 2001). Prophylactichigh-frequency ventilation for treatment of RDS has mixedresults, but these new modes of ventilation should be con-sidered as alternatives to conventional mechanical ventilationin specific circumstances, such as in infants with air leaks asinterstitial emphysema or bronchopleural fistula. Infantsgreater than 34 weeks who have RDS and respiratory failureunresponsive to ventilatory management have respondedfavorably to extracorporeal membrane oxygenation (ECMO)(Thome et al, 2005).
Nursing care for infants with RDS is demanding; the mostunstable infants often require a 1:1 nurse:patient ratio. Thenurse must monitor the quality of respirations and observe thedegree of difficulty that the infant is experiencing. Worseningretractions may signal progressive volume loss and impendingrespiratory failure. Arterial blood gas tensions and pH shouldbe measured frequently, and continuous noninvasive moni-toring of oxygenation may allow early identification of gasexchange problems. The risk of pneumothorax and right main-stem intubation is high, and the symmetry of breath soundsmust be verified regularly. A crying infant loses airway pressurewhen the mouth is open and therefore must be kept calm whenreceiving nasal CPAP. The intubated infant must be moni-tored for appropriate endotracheal tube position and patency.Suctioning of the airway should be done carefully. The suctioncatheter should be passed only as far as the end of the endo-tracheal tube because overzealous suctioning can denude thetracheal epithelium (Cordero et al, 2000). Lung volume can belost during prolonged disconnection from the ventilator. Rapidloss of lung volume can precipitate hypoxemia, so disconnec-tion time should be minimized. Any sudden decompensation
should alert the nurse to investigate for ventilator failure,pneumothorax, or tracheal tube plugging (Figure 1-4).
A common complication of RDS in the tiny prematureinfant is bronchopulmonary dysplasia. BPD generally refers toa chronic obstructive pulmonary disorder characterized by pul-monary fibrosis, bronchiolar metaplasia, emphysema, and inter-stitial edema. It is most commonly seen in survivors of extremeprematurity who were diagnosed with RDS, but extremely-low-birth-weight infants may develop BPD without history ofRDS. According to the National Institute of Child Health andHuman Development consensus, infants with mild BPD arethose who continue to require oxygen supplementation for atotal of at least 28 days, while those with moderate or severeBPD require oxygen supplementation and/or ventilatorysupport at 36 weeks of postmenstrual age and for more than 28 days (Jobe & Bancalari, 2001). The incidence of BPDincreases as gestational age decreases. Of the infants less thanor equal to 1,000 g at birth, 77% develop mild BPD, while 46% develop moderate BPD and 16% develop severe BPD(Ehrenkranz et al, 2005). Pulmonary morbidities and adverseneurodevelopmental outcomes at 18 to 22 months were moreprevalent with more severe BPD. Premature infants with birthweights less than 1500 g develop moderate to severe BPD.
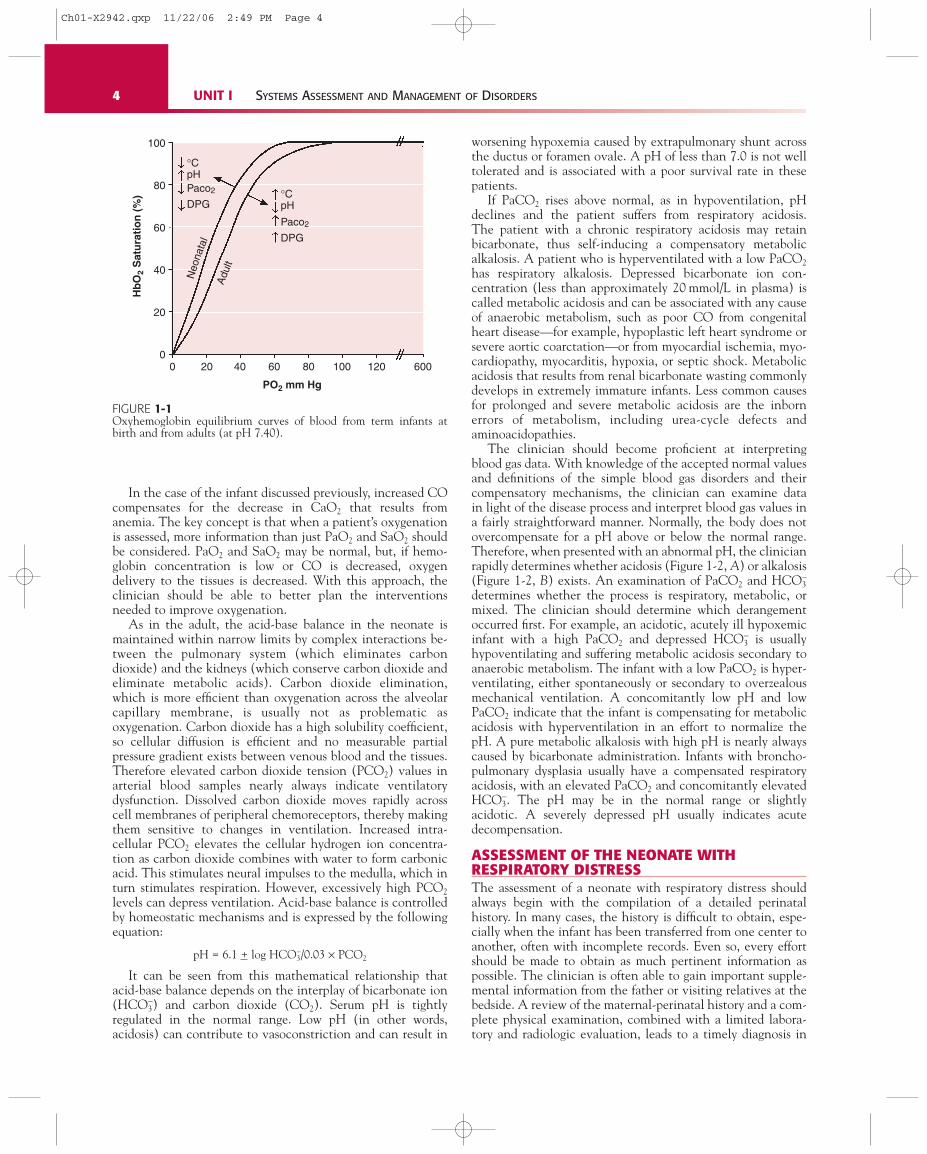
Air LeaksAir leaks frequently complicate RDS and other neonatal respi-ratory disorders. Air leaks are characterized by air in an ectopiclocation (Box 1-3). Many air-leak syndromes begin with atleast some degree of pulmonary interstitial emphysema, whichis the result of alveolar rupture from overdistention, usuallyconcomitant with mechanical ventilation or continuous dis-tending airway pressure. Pulmonary interstitial emphysemaoccurs most commonly in preterm infants but may be seen in infants of any gestational age. Lung compliance is non-uniform, and areas of poor aeration and alveolar collapse exist. Interspersed are alveoli of normal or near-normalcompliance, which become overdistended. The more normallung units (those with better compliance) become overdis-tended and eventually rupture. Air is forced from the alveolusinto the loose tissue of the interstitial space and dissects toward the hilum of the lung, where it may track into the mediastinum—causing a pneumomediastinum—or into thepericardium—causing a pneumopericardium. The astute clini-
8 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
FIGURE 1-4Acute deterioration in a ventilated patient.
Ventilator malfunction:Gas source and blenderVentilatorTubing
Inadvertent changes in settings
Ventilator
Accidental extubationPlugged tubeBronchial intubationDisconnection from ventilator
PneumothoraxAtelectasisFighting against ventilatorPulmonary hemorrhageExtrapulmonary causes (e.g., IVH, seizures)
Endotrachealtube
Patient
Acute Deterioration in a Ventilated Patient
Ch01-X2942.qxp 11/22/06 2:49 PM Page 8
cian may notice that an infant’s chest becomes barrel-shapedwith overdistention and that breath sounds become distant onthe affected side. In contrast, the infant who suffers a pneu-mothorax usually becomes unstable, with development ofcyanosis, oxygen desaturation, and carbon dioxide retention.The infant may become hypotensive and bradycardic becausethe high intrathoracic pressure impedes CO. A tensionpneumothorax, in which the free pleural air compresses thelung, is a medical emergency, and prompt relief bythoracentesis or tube thoracostomy is indicated.
Transient Tachypnea of the NewbornTransient tachypnea of the newborn occurs typically in infantsborn by cesarean section, particularly in the absence of labor.The cause of the disorder is thought to be transient pulmonaryedema that results from the infant’s “missed” chance duringlabor to absorb pulmonary alveolar fluid. The chest radiographmay show increased perihilar interstitial markings and smallpleural fluid collections, especially in the minor fissure. Incontrast to the infants with RDS, infants with transienttachypnea tend to have a normal or low PCO2. Oxygenationcan usually be maintained by supplementing oxygen with ahood, although some infants benefit from a short course ofpositive pressure support. The infant usually recovers in 24 to48 hours.
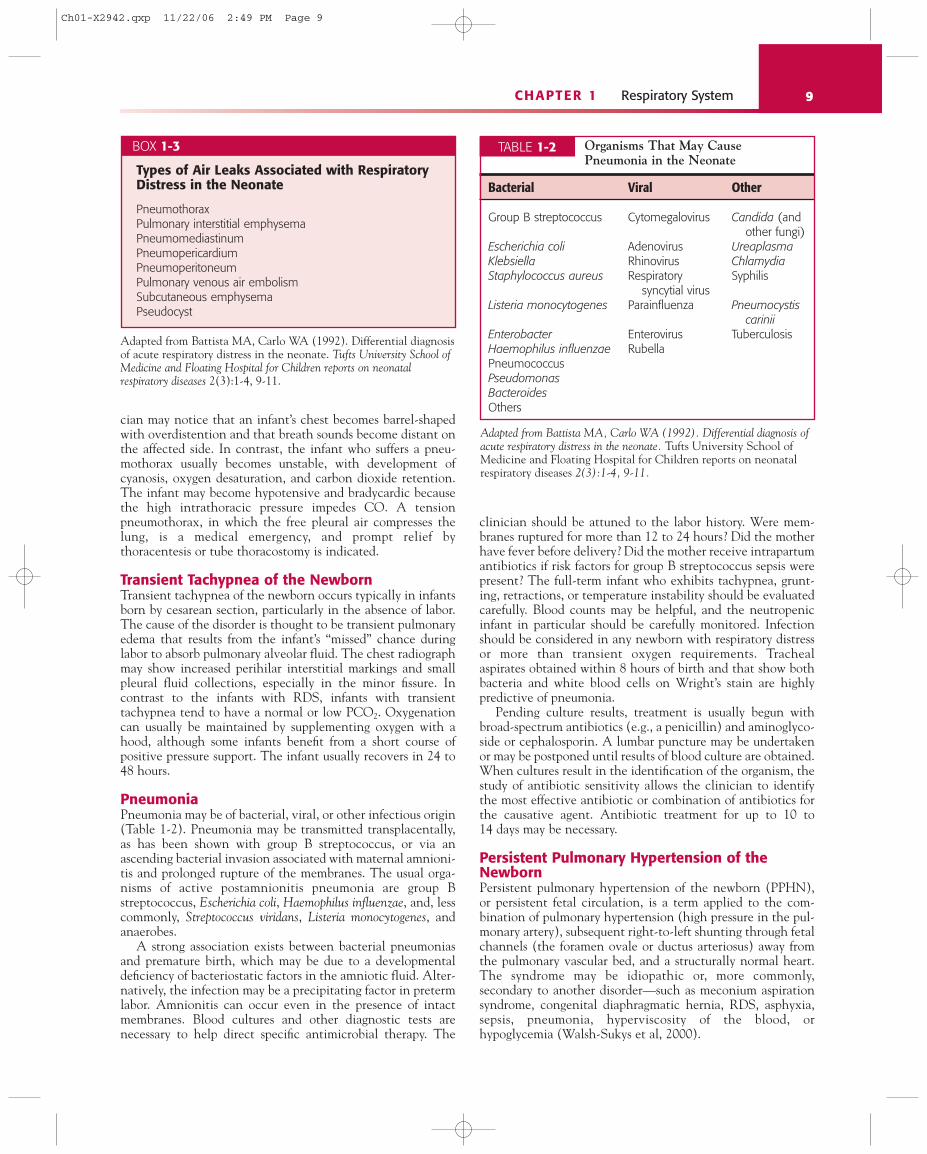
PneumoniaPneumonia may be of bacterial, viral, or other infectious origin(Table 1-2). Pneumonia may be transmitted transplacentally,as has been shown with group B streptococcus, or via anascending bacterial invasion associated with maternal amnioni-tis and prolonged rupture of the membranes. The usual orga-nisms of active postamnionitis pneumonia are group Bstreptococcus, Escherichia coli, Haemophilus influenzae, and, lesscommonly, Streptococcus viridans, Listeria monocytogenes, andanaerobes.
A strong association exists between bacterial pneumoniasand premature birth, which may be due to a developmentaldeficiency of bacteriostatic factors in the amniotic fluid. Alter-natively, the infection may be a precipitating factor in pretermlabor. Amnionitis can occur even in the presence of intactmembranes. Blood cultures and other diagnostic tests arenecessary to help direct specific antimicrobial therapy. The
clinician should be attuned to the labor history. Were mem-branes ruptured for more than 12 to 24 hours? Did the motherhave fever before delivery? Did the mother receive intrapartumantibiotics if risk factors for group B streptococcus sepsis werepresent? The full-term infant who exhibits tachypnea, grunt-ing, retractions, or temperature instability should be evaluatedcarefully. Blood counts may be helpful, and the neutropenicinfant in particular should be carefully monitored. Infectionshould be considered in any newborn with respiratory distressor more than transient oxygen requirements. Trachealaspirates obtained within 8 hours of birth and that show bothbacteria and white blood cells on Wright’s stain are highlypredictive of pneumonia.
Pending culture results, treatment is usually begun withbroad-spectrum antibiotics (e.g., a penicillin) and aminoglyco-side or cephalosporin. A lumbar puncture may be undertakenor may be postponed until results of blood culture are obtained.When cultures result in the identification of the organism, thestudy of antibiotic sensitivity allows the clinician to identifythe most effective antibiotic or combination of antibiotics forthe causative agent. Antibiotic treatment for up to 10 to 14 days may be necessary.
Persistent Pulmonary Hypertension of theNewbornPersistent pulmonary hypertension of the newborn (PPHN),or persistent fetal circulation, is a term applied to the com-bination of pulmonary hypertension (high pressure in the pul-monary artery), subsequent right-to-left shunting through fetalchannels (the foramen ovale or ductus arteriosus) away fromthe pulmonary vascular bed, and a structurally normal heart.The syndrome may be idiopathic or, more commonly,secondary to another disorder—such as meconium aspirationsyndrome, congenital diaphragmatic hernia, RDS, asphyxia,sepsis, pneumonia, hyperviscosity of the blood, orhypoglycemia (Walsh-Sukys et al, 2000).
9CHAPTER 1 Respiratory System
BOX 1-3
Types of Air Leaks Associated with RespiratoryDistress in the Neonate
PneumothoraxPulmonary interstitial emphysemaPneumomediastinumPneumopericardiumPneumoperitoneumPulmonary venous air embolismSubcutaneous emphysemaPseudocyst
Adapted from Battista MA, Carlo WA (1992). Differential diagnosisof acute respiratory distress in the neonate. Tufts University School ofMedicine and Floating Hospital for Children reports on neonatalrespiratory diseases 2(3):1-4, 9-11.
Bacterial Viral Other
Group B streptococcus Cytomegalovirus Candida (and other fungi)
Escherichia coli Adenovirus UreaplasmaKlebsiella Rhinovirus ChlamydiaStaphylococcus aureus Respiratory Syphilis
syncytial virusListeria monocytogenes Parainfluenza Pneumocystis
cariniiEnterobacter Enterovirus TuberculosisHaemophilus influenzae RubellaPneumococcusPseudomonasBacteroidesOthers
Adapted from Battista MA, Carlo WA (1992). Differential diagnosis ofacute respiratory distress in the neonate. Tufts University School ofMedicine and Floating Hospital for Children reports on neonatalrespiratory diseases 2(3):1-4, 9-11.
Organisms That May Cause Pneumonia in the Neonate
TABLE 1-2
Ch01-X2942.qxp 11/22/06 2:49 PM Page 9

The neonatal pulmonary vasculature is sensitive to changesin PaO2 and pH and, during stress, can become even hyper-reactive and constrict to cause increased pressure againstwhich the neonatal heart cannot force blood flow to the lungs.If the pulmonary artery pressure is higher than systemicpressure, blood flows through the path of least resistance, awayfrom the lungs through the foramen ovale and the ductusarteriosus. The infant becomes progressively hypoxemic andacidemic, and the cycle perpetuates.
Collaborative management of infants with PPHN demandsthe greatest diligence that the health care professional cansummon. Because the pulmonary vasculature is unstable, almostany event can precipitate severe hypoxemia, including routineprocedures such as endotracheal tube suctioning, weighing,positioning, and diaper changes. Under these circumstances,minimal stimulation is usually practiced.
Occasionally, sedation and even muscle paralysis arenecessary to prevent spontaneous episodes of hypoxemia ordeterioration associated with procedures (e.g., suctioning andposition changes). Alkalosis—either with bicarbonate infusionor by hyperventilation—often relaxes the pulmonary vascularbed and allows better pulmonary perfusion and thus oxygenation.The approach to therapy should be directed toward preventinghypoxemia and acidosis. The critical pH necessary for over-coming pulmonary vasoconstriction seems to be unique to theindividual. High applied ventilator pressures predispose thelung to air-leak syndromes, further increasing the risk of suddendestabilization. Vasopressor therapy with dopamine and dobu-tamine is often used in conjunction with hyperventilation, butcontrolled data are not available. Presumably, they act both to improve contractility of the stressed myocardium, whichimproves CO, and to raise systemic arterial pressure abovepulmonary artery pressure to reduce right-to-left shunting.
When conventional therapies fail, high-frequency ventila-tion may be attempted. Approximately 30% to 60% of patientswho fail conventional mechanical ventilation respond tohigh-frequency ventilation. However, the exact role of high-frequency ventilation on mortality or in preventing the needfor ECMO needs further evaluation. Since the early 1990s,inhalation of nitric oxide—alone and in association with high-frequency ventilation—has been shown to be an effectivetherapy for PPHN (The Neonatal Inhaled Nitric Oxide StudyGroup, 1997; Davidson et al, 1998).
When oxygenation cannot be accomplished despite the useof conventional mechanical ventilation, high-frequency venti-lation, or nitric oxide, ECMO has proven to be an effectivetherapy (UK Collaborative ECMO Trial Group, 1996).Neonatologists disagree about the exact indications forECMO, and some centers report impressive survival statisticswithout the use of ECMO (Mok et al, 1999). However, ECMOoften is the only treatment that improves the outcome of someinfants who fail less invasive therapies.
Meconium Aspiration Syndrome (MAS)MAS is the most common aspiration syndrome that causesrespiratory distress in neonates. The role of meconium in thepathophysiology of aspiration pneumonia has become contro-versial. It is unclear whether the material itself causes pneu-monitis severe enough to lead to hypoxemia, acidosis, andpulmonary hypertension or whether the presence of meconiumin the amniotic fluid is merely a marker for other events thatmay have predisposed the fetus to severe pulmonary disease.
The severely ill infant with MAS typically comes from astressed labor and has depressed cord pH from metabolicacidosis. These infants are often postmature and exhibit classicsigns of weight loss, skin peeling, and deep staining of the nailsand umbilical cord.
Pharyngeal suctioning at the time of birth does not reduceMAS (Vain et al, 2004). The depressed infant with meconium-stained fluid should receive endotracheal suction at birth. Ifthe infant has absent or depressed respirations, is hypotonic, orhas a heart rate of fewer than 100 beats/min, then rapidintubation under direct laryngoscopy to allow for suctioning ofthe airway is recommended (International Guidelines forNeonatal Resuscitation, 2000). Endotracheal suctioning atbirth is used to prevent MAS in the newly born withmeconium-stained fluid but is not necessary if the infant isvigorous at birth (Wiswell et al, 2000). The American Academyof Pediatrics Neonatal Resuscitation Program suggests that ifthe infant is not vigorous then the trachea should be suctionedas soon as possible after delivery (Clark & Clark, 2004).
Pulmonary disease arises from chemical pneumonitis,interstitial edema, and small-airway obstruction and fromconcomitant persistent pulmonary hypertension. The infantmay have uneven pulmonary ventilation with hyperinflationof some areas and atelectasis of others, leading to ventilation-perfusion mismatching and subsequent hypoxemia. The hy-poxemia may then exacerbate pulmonary vasoconstriction,leading to deeper hypoxemia and acidosis. Infants with MASmay have evidence of lung overinflation with a barrel-chestedappearance. Auscultation reveals rales and rhonchi. Theradiograph shows patchy or streaky areas of atelectasis andother areas of overinflation.
As with other cases of pulmonary hypertension, nursingcare of infants with MAS centers on maintenance of adequateoxygenation and acid-base balance and on the avoidance ofcold stress, which contributes to acidosis. A high incidence of air leaks exists in these infants, and positive pressure venti-lation is best avoided if the patient can be adequatelyoxygenated, even at very high-inspired oxygen concentrations.Antibiotics are often used, however, particularly in desperatelyill infants, at least until a bacterial infection is ruled out, butantibiotic therapy may not be necessary. The infant is oftenexquisitely sensitive to environmental stimuli and should betreated in as quiet an environment as possible. Interventionsshould be preplanned to maximize efficiency of handling the infant. Infants with very severe respiratory failure andMAS improve with the administration of exogenoussurfactant.
Although aspiration of meconium is most common, theneonate may become symptomatic as a result of the aspirationof blood, amniotic fluid, or gastrointestinal contents. Thehistory is important in the differential diagnosis becauseradiographs are non-diagnostic.
Pulmonary HemorrhagePulmonary hemorrhage is rarely an isolated condition andusually occurs in an otherwise sick infant. RDS, asphyxia,congenital heart disease, aspiration of gastric content ormaternal blood, and disseminated intravascular coagulationand other bleeding disorders may play a role in the cause ofpulmonary hemorrhage. The risk for pulmonary hemorrhage isincreased by approximately 5% in infants receiving eithernatural or artificial surfactant. Massive bleeding may also occur
10 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Ch01-X2942.qxp 11/22/06 2:49 PM Page 10

as a complication of airway suction secondary to direct traumaof the respiratory epithelium.
Pulmonary hemorrhage is manifested by the presence ofbloody fluid from the trachea. When massive, it may be herald-ed by a sudden deterioration with pallor, shock, cyanosis, orbradycardia. Attention must be given to maintenance of apatent airway because an obstructed endotracheal tuberequires emergency replacement. Suctioning must be donewith great care to avoid precipitation of further bleeding.Clotting factors can be consumed rapidly, and the nurse shouldbe alert to signs of generalized bleeding.
Pleural EffusionsPleural effusions may be caused by accumulation of fluidbetween the parietal pleura of the chest wall and the visceralpleura enveloping the lung. A pleural effusion may also be dueto chylothorax (lymphatic fluid) or hemothorax (blood).Lymphatics drain fluid that filters into the pleural space. Fluidaccumulates in the pleural space as a result of either increasedfiltration or decreased absorption. An increase in filtrationpressure, as seen with increased venous pressure in hydropsfetalis or congestive heart failure, leads to pleural effusion. Therate of filtration into the pleural space also increases if thepleural membrane becomes more permeable to water andprotein, as occurs with infection.
Pleural effusion with high glucose content in an infant whois receiving parenteral nutrition via a central venous cathetershould raise the suspicion of catheter perforation into thepleural space. If the infant is also receiving lipid infusion, thefluid may appear milky and be confused with chylothorax.
Chylothorax may be congenital or acquired and is asso-ciated with obstruction or perforation of the thoracic duct. Itmay also be a surgical complication of repair of diaphragmatichernia, tracheoesophageal fistula, or congenital heart defect.Congenital chylothorax may be suspected in the infant whocannot be ventilated in the delivery room. Breath sounds aredifficult to hear, and chest movement with ventilation isminimal. Bilateral thoracenteses may be lifesaving. The typicalpleural fluid in a chylothorax—opalescent and rich in fat—ispresent only if the infant has been fed.
Pleural effusions that impede respiratory function typicallyrequire drainage by thoracentesis or tube thoracostomy. It maybe necessary for chest tubes placed for chylothorax and tho-racic duct injury to remain in place for extended periods whilethe infant is given total parenteral nutrition, receiving nothingby mouth, thus minimizing thoracic duct flow.
ApneaApnea is the common end product of a myriad of neonatalphysiologic events. Hypoxemia, infection, anemia, thermalinstability, metabolic derangement, drugs, and intracranialdisease can cause apnea. These causes should be ruled outbefore idiopathic apnea of prematurity is diagnosed.
Apnea is observed in more than half of surviving prematureinfants who weigh less than 1.5 kg at birth. The respiratorycontrol mechanism and central responsiveness to carbondioxide is progressively less mature the lower the gestationalage. In contrast to adults, infants respond to hypoxemia withonly a brief hyperpneic response followed by hypoventilationor apnea. In any infant who has apnea, hypoxemia shouldalways be ruled out before the clinician embarks on any otherworkup or institutes therapy.
Care of the infant experiencing apneic episodes requiresclose observation. Obstructive apnea cannot be detected withthe impedance respiratory monitor because normal or pro-nounced respiratory excursions of the chest wall exist. Prompttactile stimulation for mild “spells” is often sufficient to abortthe episode of apnea, obviating the need for further therapy.Infants with apneic episodes accompanied by profound brady-cardia need prompt attention to their immediate needs as wellas more aggressive diagnostic and therapeutic intervention.
Sensory stimulation with waterbeds or other means cansometimes be used to manage these infants, particularly thosewith mild apnea. Many apneic neonates respond to nasalCPAP at low pressures because the apnea may be due to airwayobstruction or intermittent hypoxemia. Pressure support mayalso stimulate pulmonary stretch receptors, thus stimulatingrespiration. Nursing care that is directed toward promoting aneutral thermal environment, normoxia, optimal airway main-tenance, and prevention of aspiration is essential in the care ofneonates at risk for apnea.
Use of methylxanthines, such as caffeine and amino-phylline, has markedly simplified the treatment of apnea insome premature infants. Xanthines appear to exert a centralstimulatory effect on brainstem respiratory neurons and oftenmarkedly decrease the frequency and severity of apneicepisodes. The clinician must be attuned to the toxicities ofxanthines, including tachycardia, excessive diuresis, and vomit-ing, which may precede neurologic toxicity at inadvertentlyhigh blood drug levels. Caffeine may be associated with a lowerrisk of adverse effects (Schmidt et al, 2006).
CONGENITAL ANOMALIES THAT AFFECTRESPIRATORY FUNCTIONDiaphragmatic HerniaCongenital diaphragmatic hernia (CDH) occurs at a frequencyof 1 in 2500 live births and may be unsuspected until birth.Herniation of abdominal contents into the chest cavity earlyin gestation is accompanied by ipsilateral pulmonary hypo-plasia. By mechanisms that are not well understood, there isoften some degree of pulmonary hypoplasia on the contra-lateral side. Most infants are symptomatic at birth, with severerespiratory distress in the delivery room. The affected new-born’s abdomen is usually scaphoid, and breath sounds areabsent on the side of the defect (a left-sided defect occurs in90% of cases). Bowel sounds may be heard in the chest, andheart sounds may be heard on the right side because theherniated abdominal contents push the mediastinum to the right.
As soon as the diagnosis is suspected, bag and mask ventilation should be avoided because it fills the herniacontents with gas and can compress the lungs and worsenventilation. When CDH has been diagnosed prenatally, the infant should be intubated and mechanical ventilationshould be begun immediately after birth. An orogastric tubeshould be placed to aid in decompression of the herniatedabdominal viscera. Ventilation should be attempted with arapid rate and low inflation pressure and toleratinghypercapnia. Symptomatic neonates often have pulmonaryhypertension and progressive right-to-left shunting.Hypotension is common, and, when adequate intravascularvolume is established, dopamine infusion may be helpful.Pulmonary vasodilators have been advocated by someclinicians and have met with variable success, but they should
11CHAPTER 1 Respiratory System
Ch01-X2942.qxp 11/22/06 2:49 PM Page 11

not be used unless adequate systemic blood pressure can bemaintained. Although evidence of surfactant deficiency inthese newborns exists, surfactant administration does notappear to improve their clinical course or outcome (Colby etal, 2004).
Survival rate is poor in infants who are symptomatic atbirth, and ECMO commonly is required, often to no avail.Surgery to repair the defect is indicated. Controversy regardingthe urgency of the procedure exists among pediatric surgeons,and some prefer to stabilize the patient with mechanical ven-tilation, vasopressors, and correction of acidosis before under-taking surgical intervention; others perform surgical repairwhile the patient is maintained on ECMO (see Chapter 3).
Congenital Heart DiseaseCongenital heart disease commonly manifests with signs ofrespiratory distress. Neonates with congenital heart diseaseand who demonstrate right-to-left shunting and decreasedpulmonary blood flow (e.g., tetralogy of Fallot, pulmonaryvalve atresia, and tricuspid valve atresia or stenosis) usuallypresent with profound cyanosis unresponsive to oxygensupplementation. Neonates with congenital heart disease andwho demonstrate increased pulmonary blood flow or obstruc-tion to the left outflow tract (e.g., transposition of the greatvessels, total anomalous pulmonary venous return, atrioven-tricular canal, hypoplastic left heart syndrome, and criticalcoarctation of the aorta) may transiently improve with oxygensupplementation. Neonates with non-cyanotic lesions such aspatent ductus arteriosus and ventricular septal defect maypresent with signs of congestive heart failure (see Chapter 3).
Choanal AtresiaChoanal atresia causes upper airway obstruction in theneonate. The choanae, or nasal passages, are separated fromthe nasopharynx by a structure known as the bucconasalmembrane, which normally perforates during gestation. Failureof this developmental event results in an obstructed airway,occurring bilaterally in 50% of cases. Most affected infants arefemale and half of affected infants have associated anomalies asCHARGE (coloboma, heart defects, atresia of the choanae,retardation of growth and development, genital and urinaryabnormalities, and ear abnormalities and/or hearing loss) asso-ciation. Because newborns are obligate nasal breathers, theyhave chest retractions and severe cyanosis (particularly duringfeeding), and paradoxically turn pink when crying. Emergencytreatment consists of tracheal intubation or placement of an oral airway. Surgical correction is indicated (Park et al,2000).
Cystic HygromaA variety of space-occupying lesions can impose on the airwayof the newborn (Box 1-4). Most are derived from embryonictissues. Cystic hygroma, derived from lymphatic tissue, is themost common lateral neck mass in the newborn. It is multi-lobular, is multicystic, and, when large, obstructs the airway.Surgery is curative, although it is sometimes technicallydifficult. The clinician must always be mindful of the airwayand its patency. Many of these lesions are of great cosmeticconcern and cause great distress in the parents. A care planshould address these parental concerns. It is sometimes helpfulto facilitate contact with parents of other children with similarproblems who can share similar experiences.
Pierre Robin Syndrome or SequenceThe major feature of Pierre Robin syndrome or sequence ismicrognathia (a small mandible). The tongue is posteriorlydisplaced into the oropharynx, thus obstructing the airway.Sixty percent of affected patients also have a cleft palate.Obstructive respiratory distress and cyanosis are common andmay be severe. In an emergency, as with all airway obstructions(obstructive apnea), tracheal intubation should be under-taken. Infants with Pierre Robin syndrome or sequence arenursed in the prone position to prevent the tongue from fallingbackward. Nasogastric tube feedings are usually required in theneonatal period. With good care, the infant has a good prog-nosis for survival; the mandible usually grows; and the problemresolves by 6 to 12 months of age.
The newer term for this condition, in many cases, issequence, but syndrome can also be used because the clusters ofsymptoms can occur in many ways. Sequence refers to apattern that is a result of a single problem in morphogenesisthat leads to this variety of problems. Syndrome is usually usedwhen no one determinant can be identified. For example, itmay result from multifactorial inheritance, may be part ofother conditions, or may be genetic (whereby one or moregenes are responsible). Thus this condition is more than just an explainable, describable syndrome or a sequence of visibledefects (Tewfik et al, 2006; Van den Elsen et al, 2001).
COLLABORATIVE MANAGEMENT OF INFANTSWITH RESPIRATORY DISORDERSSupportive CareSupportive care of the infant in respiratory distress requiresattention to detail. The clinicians’ primary goals are to mini-mize oxygen consumption and carbon dioxide production.These goals are accomplished by maintaining a neutral
12 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
BOX 1-4
Thoracic Cysts and Tumors That May CauseRespiratory Distress in the Neonate
TeratomaCystic hygroma
• Neurogenic tumor• Neuroblastoma• Ganglioneuroma• Neurofibroma
Bronchial or bronchogenic cystIntrapulmonary cystGastrogenic cystHemangiomaAngiosarcomaMediastinal goiterThymomaMesenchymomaLipomaCystic adenomatous malformation
Adapted from Battista MA, Carlo WA (1992). Differential diagnosisof acute respiratory distress in the neonate. Tufts University School ofMedicine and Floating Hospital for Children reports on neonatalrespiratory diseases 2(3):1-4, 9-11.
Ch01-X2942.qxp 11/22/06 2:49 PM Page 12

thermal environment. The nurse must be skilled in physicalassessment to interpret signs and symptoms, such as cyanosis,gasping, tachypnea, grunting, nasal flaring, and retractions. Byunderstanding the pathophysiology of breathing, the nurseknows that the infant with retractions has decreased lungcompliance and that the cyanotic infant has poor tissueoxygenation.
Excellent communication is needed between the neonatalnurse and the rest of the neonatal team. Acutely ill neonateswith respiratory disease are often unstable and their conditioncan deteriorate rapidly, so astute observation skills are neces-sary. Assessment is a continuous process, and effective com-munication among nurses, respiratory therapists, physicians,and support staff is necessary for proper delivery of intensivecare. The nurse, who is the primary bedside caregiver, is thegatekeeper for all interactions between the patient and the environment. The nurse who is caring for an unstablepatient should be the patient’s advocate, whether such a roleinvolves regulating the timing of a physical examination bythe physician or venipuncture for laboratory investigation.
Technical competence is an important facet of the nurse’srepertoire. The nurse is responsible for maintaining intra-venous lines and tracheal tube patency, accurately measuringvolumes of intravenous intake as well as urinary output, andoperating advanced electronic machinery. Moreover, the nursemust also be adept at interpreting arterial blood gas andlaboratory data in order to communicate these to the rest ofthe care team and to develop a cogent management plan.Many functions are shared to some degree with respiratorytherapists. Whether nurses or respiratory therapists makeventilator changes, the nurse should become familiar with theeffects of ventilator setting changes on blood gases. PaCO2 isaffected by changes in ventilator rate and tidal volume. Tidalvolume depends on the difference between PIP and PEEP.Thus, to decrease PaCO2, either rate or inspiratory pressureshould be increased. PaO2 depends on the fraction of inspiredoxygen concentration (FiO2) and mean airway pressure(MAP). MAP depends on PIP, PEEP, inspiratory to expiratorytime ratio, and gas flow. To improve PaO2, the most effectivechanges are to increase MAP by increasing PIP or PEEP or toincrease FiO2. Table 1-3 shows the effect of ventilator settingchanges on blood gases. The nurse should also be familiar withventilator functioning so that malfunctions can be detectedpromptly. The nurse should always be prepared to bag-ventilate an intubated neonate in the event that decompen-sation occurs while the status of the ventilatory apparatus ischecked. Nurses and therapists often share such functions asairway suctioning, monitoring and recording of inspiredoxygen concentration, and delivery of chest physical therapy.
The delivery of oxygen therapy should always be carefullymonitored. Desired oxygenation parameters should be recordedin the nurse’s notes and followed up with measurement ofarterial blood gases or by noninvasive means. The acutely illinfant should have FiO2 measured continuously and recordedfrequently. The goal for oxygenation depends on the patient’sdiagnosis and condition. For example, in infants with PPHN,an apparently acceptable saturation may occur despite markedright-to-left shunting. In preterm infants oxygen saturationcan be kept in the high 80s and low 90s, thus avoiding the risksassociated with hyperoxia in preterm infants (The STOP-ROPMulticenter Study Group, 2000). Higher oxygen saturationsdo not improve growth or neurodevelopment (Askie et al,
2003) but increase the risk for retinopathy of prematurity.Procedures such as suctioning, chest physiotherapy, andhandling may lead to desaturations and may have to beminimized.
Airway suctioning is a procedure that may be associatedwith cardiopulmonary derangement, hypoxemia, bradycardia,and hypertension. Various techniques to perform airway suc-tioning exist—including preoxygenation (increase in FiO2before the procedure), normal saline instillation before thesuctioning to improve secretion aspiration, and the use of aclosed system to avoid disconnection from the ventilator. Thenurse should become familiar with the techniques used in theNICU and be aware of the associated complications.
The sudden decompensation of a ventilated infant shouldalert the nurse to assess disconnection of the ventilator,pulmonary air leak, ventilator failure, or obstructed trachealtube (see Figure 1-4). The very small infant who suddenlydecompensates may have experienced a severe intracranialhemorrhage.
Care of the infant who is receiving CPAP can be partic-ularly challenging. These infants should be kept calm andswaddled if necessary. Crying releases pressure through themouth; thus lung volume is lost. Nasal CPAP can be effective,but particular attention must be given to maintaining patencyof the nose, the nasal prongs, and the pharynx. The infant’snares and nasal septum should be guarded from pressure necro-sis from inappropriately applied prongs. The infant whorequires mechanical ventilation must be constantly assessed forairway patency. If the infant is unable to grunt against a closedglottis and maintain positive airway pressure, the conditionmay worsen if airway pressure is not maintained properly.Suctioning of the airway should be done only as often as nec-essary to remove pulmonary secretions that could occlude theairway. The suction catheter should be passed no further thanthe end of the tracheal tube because epithelium is easilydamaged. Vibration and percussion should be used judiciouslyin the infant with pulmonary secretions to loosen them andallow removal via suction. There is perhaps little need to vig-orously suction the intubated infant with RDS in the first daysafter birth because secretions are minimal and lung volume islost with every disconnection of the ventilator circuit.
13CHAPTER 1 Respiratory System
Ventilator Setting Changes PaCO2 PaO2
�PIP Ø ��PEEP � ��Frequency Ø ±��I:E ratio æ ��FiO2 æ ��Flow ±Ø ±�
�, Increase; Ø, decrease; ±, minimal effect; æ, no consistent effect;FiO2, fraction of O2 in dry inspired air; PEEP, positive end-expiratorypressure; PIP, peak inspiratory pressure.Modified from Carlo WA et al (1994). Advances in conventionalmechanical ventilation. In Boynton BR et al, editors. New therapies forneonatal respiratory failure, p 144. Cambridge University Press: New York.
Effects of Ventilator Setting Changes on Blood Gases
TABLE 1-3
Ch01-X2942.qxp 11/22/06 2:49 PM Page 13

ASSESSMENT AND MONITORINGThe most important aspect in monitoring patients withrespiratory disease is the close and continuous observation ofsigns and symptoms. The color of the patient gives importantclues. An infant with pink lips and oral mucosa has goodoxygenation and perfusion; a cyanotic patient has poor tissueoxygenation. If the hemoglobin concentration is too low, thepatient can be hypoxemic, but because the concentration ofdeoxyhemoglobin is low, there may be no cyanosis. An infantwith tachypnea and retraction usually has decreased lung com-pliance. A patient with a barrel-shaped thorax, taking deepbreaths, and with a normal or low respiratory rate probably hasan increased airway resistance and gas trapping. Observation ofthe intubated patient is especially important. An anguishedinfant, who is cyanotic and breathing deeply, may have anobstructed endotracheal tube. An infant with RDS andincreased chest expansion over time, despite no change inventilatory pressure, is experiencing improvement in lungcompliance. The same infant with later asymmetry in chestand sudden deterioration of oxygenation may have a pneu-mothorax. Cardiac beats, easily seen through the thoracic wall,may be caused by the presence of a symptomatic patent ductusarteriosus. A recently extubated infant, in whom increasedretractions and inspiratory stridor develop, probably has upperairway obstruction. Auscultation helps in the diagnosis ofincreased airway resistance or the presence of secretions. It alsoallows the clinician to assess the response to different treat-ment maneuvers, such as suctioning, chest physiotherapy, andbronchodilation. Asymmetries in auscultation suggest main-stream bronchial intubation, atelectasis, pneumothorax, orpleural effusion.
Great progress has been made in noninvasive monitoring ofblood gas tensions, but blood sampling is still necessary for pHdetermination and arterial samples are preferable. Capillaryspecimens are undependable, especially for PO2. If peripheralperfusion is adequate, capillary blood approximates arterialvalues of pH and PCO2. However, capillary blood PO2 valuesdo not reliably reflect arterial oxygenation.
Neonatal care has changed dramatically with the adventand widespread use of transcutaneous monitoring of PaO2,PaCO2, and SaO2. The neonatal intensive care team shouldbecome familiar with the devices used in noninvasive gasmonitoring. Knowing the basis for their functioning as well ashow to interpret the information they provide and being awareof clinical situations in which the information provided is notreliable or needs to be complemented before any managementdecisions are made is essential.
Transcutaneous PO2 (TcPO2) is measured with an electrodethat is applied over the skin and heated to 42º C to 44º C. Theelectrode measures skin PO2, not arterial PO2. Skin PO2 meas-urement depends on skin perfusion and on oxygen diffusionacross the epidermis. Warming the skin to 42º C to 44º Cunder the electrode increases skin perfusion so that TcPO2correlates better with arterial PO2. For initiation of TcPO2monitoring, 10 to 15 minutes are needed to obtain a stablereading. After that, TcPO2 reflects changes on FiO2 with a 10- to 20-second delay. After 4 to 6 hours, the methodbecomes unreliable because of changes in skin secondary tohyperthermia, so the electrode position should be changed. Inpremature infants with more labile skin, the electrode place-ment should be changed even more frequently to avoid skinburns. The nurse should be aware of situations that make
TcPO2 lose its reliability. Overestimation of oxygenationoccurs when an air bubble or leak between the electrode andthe skin occurs or when the calibration is improper. Under-estimation occurs with skin hypoperfusion, in older infants(increased thickness of the skin), with insufficient heating ofthe electrodes, or with improper calibration.
TcPO2 monitoring has been largely supplanted by continu-ous pulse oximetry. Arterial oxygen saturation is computedfrom absorption of emitted low-intensity red or infrared light.The probe is attached to a finger or toe in large infants or to ahand or foot in small premature infants. Pulse oximetry offersthe following advantages over transcutaneous oxygenmonitoring: (1) avoidance of heating the skin and the risk ofburns; (2) elimination of a delay period for transducerequilibration; (3) accurate measurement regardless of presenceof edema or patient age; (4) in vitro calibration not required;and (5) frequent position changes not required. However, thenurse should be aware that SaO2 higher than 97% may beassociated with PaO2 higher than 100 mm Hg. This isimportant in premature infants who are at risk for retinopathyof prematurity. SaO2 between 85% and 95% probably isassociated with a safe range of PaO2. With SaO2 over 95% to97%—and especially when it is 100%—the clinician cannotpredict a patient’s PaO2. When the saturation is 100%, thePaO2 can be approximately 100 mm Hg or much higher (seeFigure 1-1). This situation is particularly important in infantswith PPHN because the decision whether to wean ventilatorsettings depends on PaO2. In these patients, the simultaneoususe of TcPO2 and pulse oximetry is a useful alternative.
A common problem of pulse oximetry is the presence ofmotion artifact, an altered signal caused by movement of the part of the body where the sensor is applied. Because thepulse waveform is not detected, this movement is recognizedby the loss of correlation between the oximeter pulse rate andthe electrical monitor heart rate. With new technology themotion artifacts have been minimized (Malviya et al, 2000).Peripheral pulse oximetry may not detect pulse signals inpatients with hypotension and poor perfusion. TcPO2 may also give false readings in this situation. The clinician shouldbe aware that pressure of the probe over the skin can produceskin pressure necrosis. This consideration is particularlyimportant in the premature infant. Phototherapy may interferewith accuracy of SaO2 monitoring, but this problem can beavoided by covering the sensor with an opaque material (e.g.,a diaper).
TcPO2 monitoring and pulse oximetry are useful in severalclinical situations. They may be used in neonates with mildrespiratory distress, such as transient tachypnea, to assess theoxygen requirement and to allow weaning without placementof an arterial catheter. In infants receiving mechanical venti-lation, TcPO2 or pulse oximetry helps to assess the effects ofventilator setting changes, thus reducing the need for arterialblood sampling. Continuous oxygenation monitoring reducesthe risk of hyperoxemia or hypoxemia during interventionssuch as airway suctioning, position change, lumbar puncture,or venous cannulation. This monitoring is particularly helpfulin the care of infants who do not tolerate excessive stimu-lation, such as those with PPHN. TcPO2 and pulse-oximetrymonitoring are also useful in caring for patients with PPHNbecause simultaneous monitoring of preductal (head, rightarm, right upper chest) and postductal (left arm, abdomen,legs) TcPO2 or SaO2 allows assessment of the magnitude of
14 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Ch01-X2942.qxp 11/22/06 2:49 PM Page 14

ductal shunting or the response to therapies such as vasodila-tion or alkalinization.
Transcutaneously measured PCO2 is accomplished with aglass electrode that is pH-sensitive. Transcutaneous PCO2response is slower than that of TcPO2, and the value measuredmust be corrected for skin production of carbon dioxide. Thustranscutaneously measured values are approximately 1.3 to 1.4times higher than arterial PCO2 values. Most modern monitorsdisplay an electronically corrected value to TcPO2. Thismodality is especially useful for monitoring chronicallyventilated patients without indwelling catheters. Blood gasvalues during arterial puncture or vigorous crying during theprocedure are often affected by breath holding and shuntingand thus may be misleading.
ENVIRONMENTAL CONSIDERATIONSMaintenance of the therapeutic environment is an importantnursing function. Much attention has been given recently tothe effects of sensory stimulation on the infant with respiratorydistress. The sick newborn often has unstable pulmonaryvasculature and may be particularly prone to hypoxic vaso-constriction. This phenomenon may be triggered in someindividuals by excess stimulation, such as loud noise, handling,or venipuncture. It has been shown that the agitated neonatehas more difficulty with oxygenation and that a quiet, mini-mally stimulating environment allows for more stable oxygena-
tion (Als, 1998). The nurse should develop a care plan thatallows the baby long periods of undisturbed rest by clusteringinterventions into short periods whenever possible. Position-ing the infant in the flexed or fetal position or “nesting” mayhelp in calming some infants.
FAMILY CARENeonates with respiratory distress frequently require multipleinstrumentation. They may have endotracheal tubes, umbilicalcatheters, oximeter probes, chest leads, and other parapher-nalia attached or applied to the skin. All of these interventionscan give parents an unnatural feeling or increased separationfrom the infant. The nurse should explain the equipmentsurrounding the bedside as well as the function of invasivecatheters, monitoring leads, and tracheal tubes. Terminologyappropriate to the parents’ level of understanding should beused. Even the most astute parents may be bewildered, andrepetition is necessary. Staff should maintain consistent termi-nology so that the parents do not become confused between“respirators” and “ventilators.” Whenever possible, the use of frightening or inaccurate terms should be avoided. Imaginethe fear engendered by the phrase, “We paralyzed your babylast night.”
Parents should be involved in developing and implement-ing the plan of care as much as possible. The mother who plansto breastfeed can be assisted in pumping her breasts and
15CHAPTER 1 Respiratory System
Continued
Case StudyIDENTIFICATION OF THE PROBLEMA term infant was admitted to the NICU. The infant devel-oped respiratory distress soon after birth. Birth weight was4000 g. Since birth, the infant had an increasing oxygenrequirement and because of a recent desaturation episode,he is now receiving 100% oxygen on a ventilator. Theventilatory settings are peak inspiratory pressure of 25 cmH2O, positive end-expiratory pressure of 5 cm H2O,ventilator rate 60 per minute, and inspiratory time 0.4seconds.
ASSESSMENT: HISTORY AND PHYSICALEXAMINATIONThe infant was born by emergency C-section because of late desaturations and thick meconium-stained fluid. Nosigns of infection were observed. The infant was notvigorous at birth and was intubated and receivedendotracheal suction. No meconium was aspirated from theendotracheal tube. Blow-by oxygen was given and theinfant responded well, initially weaning to 40% oxygen.However, after transfer to the NICU, he had increasingoxygen requirements.
The physical examination is now pertinent for excellentchest rise, equal breath sounds, central cyanosis withoxygen saturations in the mid-80s, good color andperfusion, and normal tone and reflexes.
DIFFERENTIAL DIAGNOSISMany conditions may be considered the differentialdiagnosis in this patient.
1. Persistent pulmonary hypertension of theneonate. This is a likely possibility given the severityand persistence of the very abnormal alveolar toarterial oxygen gradient (AaDO2). Pulmonary hyper-tension may be associated with meconium aspirationsyndrome. It is important to consider that right-to- left shunting can occur associated with disorders such as myocardial dysfunction, sepsis, metabolicabnormalities, and others.
2. Meconium aspiration syndrome. Meconium aspi-ration syndrome with intrapulmonary (ventilation-perfusion mismatch) or extrapulmonary shunting (atrialor ductal shunting with pulmonary hypertension)may lead to desaturation despite high oxygensupplementation.
3. Pneumothorax. Infants with meconium aspirationsyndrome are at high risk for pneumothorax. A pneu-mothorax can cause severe desaturation.
4. Gas trapping. Because this infant has a large tidalvolume for the given pressure gradient (positive inspi-ratory pressure [PIP] minus positive end-expiratorypressure [PEEP]) and thus high compliance, a long-time constant of the respiratory system leading to gas
Ch01-X2942.qxp 11/22/06 2:49 PM Page 15

freezing the milk, even if enteral feedings are delayed for sometime. This pumping may be the only thing that she alone cando for her baby.
Often lost in the bustle of critical care is the need forprivacy. The perceptive nurse senses this need and backs awayfrom the bedside when appropriate, allowing the parent sometime with the infant.
SU M MARYMost infants admitted to the NICU present with breathingdifficulty. Nursing care of these infants requires a broad knowl-edge of newborn physiology and practical skills in the appli-cation of therapies that are directed toward solving the manyproblems that sick infants can have. The nurse often mustanticipate these problems. While managing the nursing carefor several patients, the neonatal nurse must also care for thesickest of infants. Parents and family of all infants in the NICUrequire special attention not only to achieve an understandingof the complex issues surrounding the infant’s illness but alsoto calm fears and guilt that are often experienced. The rewardsof being part of the accomplishments in the NICU may be overlooked as they are usually slowly achieved. But, whenthey are recognized, the victories surpass the greatest ofexpectations.
R E F E R E N C E SAls H (1998). Developmental care in the newborn intensive care unit.
Current opinion in pediatrics 10:138-142.American Lung Association (ALA) (2006). Lung disease data at a glance:
Respiratory distress syndrome (RDS). Available at: http://www.lungusa.org/site/pp.asp?c=dvLUK9O0E&b=327819. Accessed May 28, 2006.
Askie LM et al (2003). Oxygen-saturation targets and outcomes in extremelypreterm infants. New England journal of medicine 349:959-967.
Bates MD, Balistreri WF (2002). The neonatal gastrointestinal tract: partone: development of the human digestive system. In Fanaroff AA, MartinRJ, editors. Neonatal-perinatal medicine: diseases of the fetus and infant, ed 7.St Louis: Mosby.
Clark DA, Clark MB (2004). Meconium aspiration syndrome. eMedicinefrom WebMD. Available at: http://www.emedicine.com/PED/topic768.htm.Accessed May 27, 2006.
Colby CE et al (2004). Surfactant replacement therapy on ECMO does notimprove outcome in neonates with congenital diaphragmatic hernia.Journal of pediatric surgery 39:1632-1637.
Cordero L et al (2000). Comparison of a closed (trach care MAC) with anopen endotracheal suction system in small premature infants. Journal ofperinatology 20:151-156.
Davidson D et al (1998). Inhaled nitric oxide for the early treatment ofpersistent pulmonary hypertension of the term newborn: a randomized,double-masked, placebo-controlled, dose-response multicenter study.Pediatrics 101:325-334.
Ehrenkranz RA et al (2005). Validation of the National Institutes of Healthconsensus definition of bronchopulmonary dysplasia. Pediatrics116:1353-1360.
Greenough A, Miner AD (2005). Pulmonary disease of the newborn. InRennie JM, editor. Roberton’s textbook of neonatology, 4th ed. London,England: Churchill Livingstone.
International Guidelines for Neonatal Resuscitation (2000). An excerptfrom the Guidelines 2000 for Cardiopulmonary Resuscitation andEmergency Cardiovascular Care: International Consensus on Science.Pediatrics 106(3):E29. Available at: http://www.pediatrics.org/cgi/–content/–––full/106/3/e29.
Jobe AH, Bancalari E (2001). Bronchopulmonary dysplasia. American journalof respiratory critical care medicine 163:1723-1729.
Lemons JA et al (2001). Very low birth weight outcomes of the NationalInstitute of Child Health and Human Development Neonatal ResearchNetwork, January 1995 through December 1996. Pediatrics 107:E1.
Malviya S et al (2000). False alarms and sensitivity of conventional pulseoximetry versus the Masimo SET technology in the pediatricpostanesthesia care unit. Anesthesia & analgesia 90(6):1336-1340.
Mok Q et al (1999). Persistent pulmonary hypertension of the term neonate:a strategy for management. European journal of pediatrics 158:825-827.
Park AH et al (2000). Endoscopic versus traditional approaches to choanalatresia. Otolaryngology clinics of North America 33:77-90.
Schmidt B et al (2006). Caffeine therapy for apnea of prematurity. NewEngland journal of medicine 354(20):2179-2180.
Soll RF, Morley CJ (2001). Prophylactic versus selective use of surfactant forpreventing morbidity and mortality in preterm infants. Cochrane databaseof systematic reviews 2:CD000510.
The Neonatal Inhaled Nitric Oxide Study Group (1997). Inhaled nitricoxide in full-term and nearly full-term infants with hypoxic respiratoryfailure. New England journal of medicine 336(9):597-604.
The STOP-ROP Multicenter Study Group (2000). Supplementaltherapeutic oxygen for prethreshold retinopathy of prematurity (STOP-ROP): a randomized, controlled trial. I: Primary outcomes. Pediatrics105:295-310.
16 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Case Study—cont’dtrapping at a borderline high ventilator rate should be considered.
5. Other causes. There are other less frequent causesin the differential diagnosis.
DIAGNOSTIC TESTSThe chest radiograph was obtained, repeat blood gases werefollowed, and pre- and postductal pulse oximetry and trans-cutaneous measurements of gases were monitored conti-nuously. In addition, a CBC and blood culture wereobtained. Four extremity blood pressures and an echo-cardiogram were obtained.
WORKING DIAGNOSISThe chest radiograph showed bilateral gas trapping. TheCBC and the blood cultures were negative. The echocar-
diogram was consistent with persistent pulmonaryhypertension.
DEVELOPMENT OF MANAGEMENT PLANThe infant was given surfactant and initial improvementwas seen. However, during the next 24 hours there wereepisodes of repeated intracardiac and ductal shunting,which lead to the initiation of nitric oxide.
IMPLEMENTATION AND EVALUATION OFEFFECTIVENESSNitric oxide resulted in a marked reduction of the shuntingepisodes. The infant was gradually weaned off FiO2 andsubsequently weaned off nitric oxide before extubation. Hewas entirely weaned off the ventilator and FiO2 over thesubsequent 3 days.
Ch01-X2942.qxp 11/22/06 2:49 PM Page 16

Tewfik TL et al (2006). Pierre Robin syndrome. eMedicine from WebMD.Available at: http://www.emedicine.com/ent/topic150.htm. Accessed May 27, 2006.
Thome UH et al (2005). Ventilation strategies and outcome in randomisedtrials of high frequency ventilation. Archives of disease in childhood: fetaland neonatal edition 90:F466-473.
UK Collaborative ECMO Trial Group (1996). UK collaborative randomisedtrial of neonatal extracorporeal membrane oxygenation. Lancet348(9020):75-82.
Vain NE et al (2004). Oropharyngeal and nasopharyngeal suctioning ofmeconium-stained neonates before delivery of their shoulders:multicentre, randomised controlled trial. Lancet 364:597-602.
Van den Elsen AP et al (2001). Diagnosis and treatment of the Pierre Robinsequence: results of a retrospective clinical study and review of theliterature. European journal of pediatrics 160:47-53.
Walsh-Sukys MC et al (2000). Persistent pulmonary hypertension of thenewborn in the era before nitric oxide: practice variation and outcomes.Pediatrics 105:14-20.
Wiswell TE et al (2000). Delivery room management of the apparentlyvigorous meconium-stained neonate: results of the multicenter,international collaborative trial. Pediatrics 105:1-7.
17CHAPTER 1 Respiratory System
Ch01-X2942.qxp 11/22/06 2:49 PM Page 17

This chapter focuses on innovative technologies and newerstrategies for the management of intractable hypoxemia andrespiratory failure in the newborn. These include exogenoussurfactant administration, conventional and high-frequencyventilation, inhaled nitric oxide, extracorporeal membraneoxygenation, and liquid ventilation. Discussion of these tech-nologies and strategies requires understanding of the patho-physiology of neonatal hypoxemia as well as the standardtreatments for hypoxemia in the newborn. Neonatal cardio-respiratory physiology and the physiology of transition arediscussed in depth later in this book and will only briefly becovered in this chapter.
NEONATAL HYPOXEMIAIn the neonate, the transition from complete dependence onthe maternal-placental unit for oxygenation to complete respi-ratory self-reliance must occur rapidly and requires a cascade ofimmediate responses (Table 2-1). The central nervous systemresponds to changes in oxygen and carbon dioxide tensions bygenerating the necessary efferent signals to establish a regularrespiratory pattern. The chest wall and its respiratory musclesmust have sufficient stiffness and strength to respond to thesignals received from the central nervous system. The pul-monary blood flow must be adequate for the delivery of oxygenfrom the alveolus to the body, and shunting through the ductusarteriosus and foramen ovale must be minimal. Adequatecardiac output is needed to deliver oxygen to the tissues, andthe affinity of hemoglobin for oxygen must allow oxygenrelease to the tissues. All of the above responses need to occurwithin minutes of birth, and, unsurprisingly, a large proportionof the problems in the neonatal intensive care unit (NICU)relate to tissue oxygenation.
For numerous reasons outlined in the following sections,preterm newborns are at particular risk for hypoxemia duringextrauterine transition. The respiratory control center of thepreterm infant often lacks sufficient maturity to sustain regularrespiration, as manifested by the frequent occurrence ofperiodic breathing and apnea. The chest wall may be highlycompliant, which leads to inefficient breathing and causesinward or expiratory movement of the rib cage (retractions)during inspiration. The highly compliant chest wall is oftenconfronted with a stiff lung (low compliance) because of
surfactant deficiency. This problem causes increased work forthe respiratory muscles. The preterm ductus arteriosus also mayremain patent and shunt blood away from the systemic organs.Furthermore, the preterm newborn’s blood hemoglobin con-centration is lower than that of the full-term newborn, therebylimiting oxygen-carrying capacity. Finally, there are limits tohow much the preterm infant can increase cardiac output torespond to increased oxygen demand or other deficits inoxygen delivery.
Term newborns have different problems that may interferewith the ability to establish adequate tissue oxygenation at birth. Aspiration of meconium, infectious pneumonia,retained fetal lung fluid, and air-leak syndromes are someexamples of respiratory disorders that can cause intrapul-monary shunting, hypoxemia, and increase work of breathing.Hypoxemia, whether caused by a known respiratory disorder oridiopathic in nature, can result in pulmonary arterioles thatremain constricted rather than dilate normally. Constrictedpulmonary arterioles elevate pulmonary vascular resistanceand lead to a vicious cycle of right-to-left (pulmonary-to-systemic) shunting, maintenance of pulmonary vasoconstric-tion, and protracted neonatal hypoxemia. This condition iscalled persistent pulmonary hypertension of the newborn(PPHN).
Two additional threats to normal tissue oxygenation atbirth are anemia and polycythemia. A variety of events maylead to neonatal anemia—including abruptio placenta,placenta previa, fetal-maternal hemorrhage, trauma to thecord or fetal placental vessels, and timing of cord clamping.Anemia results in a diminished oxygen-carrying capacity andthus an increased risk for inadequate tissue oxygenation.Polycythemia may be caused by intrauterine events such aschronic hypoxia and twin-to-twin transfusion or extrauterineevents such as delayed cord clamping. Paradoxically, poly-cythemia increases blood oxygen-carrying capacity but maydecrease tissue oxygen delivery by causing poor tissue bloodflow from hyperviscosity.
CONVENTIONAL MANAGEMENT OF NEONATALHYPOXEMIAThe perinatal caregiver’s first line of defense for the preventionor treatment of hypoxemia is an increased inspired oxygen
C h a p t e r 2
Emerging Technologies for theManagement of Respiratory
Disorders
Waldemar A. Carlo
18
Ch02-X2942.qxp 11/22/06 3:22 PM Page 18

concentration. Although fetal hypoxemia does not responddramatically to an increase of maternal inspired oxygen con-centrations, providing oxygen by mask or nasal cannula tomothers whose fetuses show signs of hypoxia is an acceptedmode of therapy in most obstetrical units. Administration ofoxygen dramatically increases maternal arterial oxygen tension(PaO2) but increases fetal PaO2 by only a few millimeters ofmercury. However, because fetal PaO2 is on the steep portionof the oxygen-hemoglobin dissociation curve, small changes infetal PaO2 are associated with relatively large increases in fetalblood-oxygen content.
After birth, the response to an increased inspired oxygenconcentration in the hypoxic newborn depends on the cause ofthe hypoxemia. When hypoxemia is caused by hypoventila-tion, PaO2 increases in an approximately one-to-one relation-ship with alveolar oxygen tension. Thus the PaO2 increases byapproximately 60 mm Hg in the hypoventilating newborn whois placed in 30% oxygen. On the other hand, when hypoxemiais caused by an intrapulmonary or extrapulmonary right-to-leftshunt (pulmonary-to-systemic shunt), the neonatal PaO2increases minimally in response to an increased inspiredoxygen concentration. For example, a newborn with a 50%right-to-left shunt (i.e., 50% of right ventricular output doesnot pass through the lungs) has a PaO2 of approximately 50 to55 mm Hg in room air. Placing the newborn in a head hoodthat contains 100% oxygen may raise the PaO2 to only 60 to65 mm Hg. In infants with right-to-left shunts who are placedon oxygen, blood oxygen content may increase significantlybecause of the position and shape of the oxygen-hemoglobindissociation curve, although little is gained in terms of PaO2.Although increasing the inspired oxygen concentration in thehypoxemic newborn may be essential to prevent permanentcell injury or cell death, this benefit must be weighed againstthe risk for chronic lung disease due to the toxic effects ofpulmonary oxygen.
Another technique used in the newborn at risk for hypox-emia is the maintenance of an adequate oxygen-carrying capa-city by intermittent blood transfusion. Although few scientificstudies have been published, it is empirically accepted thatprevention and treatment of anemia in the newborn withcardiorespiratory disease are important aspects of management.For example, transfusion of infants with bronchopulmonarydysplasia results in decreased use of oxygen. Some studiessupport the administration of human erythropoietin combined
19CHAPTER 2 Emerging Technologies for the Management of Respiratory Disorders
with iron supplementation to reduce the risk of repeated bloodtransfusions. In one study using this treatment, patientsreceived significantly fewer transfusions (1.0 vs 2.9) than didcontrols (Carnielli et al, 1998). However, this treatment maynot be cost-effective because donor blood is usually split intoquad packs, and therefore a small but significant reduction innumber of transfusions would not reduce exposure to differentblood donors.
Decreasing oxygen demand and thus minimizing thenewborn’s metabolic rate can reduce the risk for cell injurysecondary to tissue hypoxia. Depending on the specific thermalenvironment, the neonatal energy (and oxygen) expenditurenecessary to keep warm may be great or small. Thisrelationship has been recognized for more than 40 years andhas led to studies designed to define the thermal environ-ment in which energy expended to keep warm is minimal(known as a neutral thermal environment). Attempts to createa near-neutral thermal environment have shown improvedsurvival of sick premature newborns, presumably by favorablyaffecting the balance between oxygen demand and oxygensupply.
Another critical factor that affects the delivery of oxygen tothe tissues is the adequacy of organ blood flow. Organ bloodflow may be globally decreased because of decreased cardiacoutput, thus increasing the risk for tissue hypoxia. Methodscommonly employed for maintenance of adequate cardiacoutput include volume expansion of the hypovolemic newbornand inotropic drugs to stimulate the poorly contractile myo-cardium. Clinical evaluation often is used to estimate cardiacoutput, including determination of the rate of capillary refill;determination of the presence or absence of acrocyanosis, skinmottling, or relative coolness of the extremities; and deter-mination of pulse strength and blood pressure. Laboratory aids,including serial hematocrit determinations to diagnose acuteblood loss and echocardiography to evaluate cardiac contrac-tility, are at times helpful. Bedside evaluation of neonatalcardiac output is difficult, remains an inexact science, and haslittle benefit over the long term. Therefore, it will not beaddressed in this text. Determination of the distribution oforgan blood flow is also almost impossible. Even when cardiacoutput is normal or nearly normal, some organs suffer hypoxicinsults because of low blood flow. If, for example, necrotizingenterocolitis results in part from decreased intestinal bloodflow and thus decreased intestinal oxygenation, it would beuseful to be able to estimate that flow. Similarly, decreasedurine output may indicate decreased renal blood flow;however, waiting for changes in blood and urine chemistries(e.g., elevated creatinine) may mean that an irreversible renalhypoxic injury already has occurred. Rapid determination ofthe distribution of neonatal organ blood flow awaits thedevelopment of new methods.
A discussion of strategies now available in NICUs for themanagement of hypoxemia would not be complete without atleast mentioning the widespread use of techniques for measur-ing or estimating blood-oxygen tension or blood-oxygen satu-ration. The direct measurement of PaO2 and oxygen saturationin small samples of blood (0.1 to 0.2 ml) has been available forseveral years. Although they are not in widespread use,indwelling vascular catheters for the continuous measure-ment of blood PaO2 or oxygen saturation are available.Perhaps the most significant technologic development foraiding the management of potentially hypoxic sick newborns
Components Functions
Central and peripheral nervous Control of breathingsystem
Chest wall (ribs and respiratory Pumpmuscles)
Pulmonary circulation Oxygen uptake from alveoli
Hemoglobin Oxygen transportSystemic cardiac output Oxygen deliveryMitochondria Oxygen-dependent energy
production
TABLE 2-1 The Neonatal Respiratory System
Ch02-X2942.qxp 11/22/06 3:22 PM Page 19

has been noninvasive methods of measuring transcutaneousPaO2 and transcutaneous oxygen saturation nearly continu-ously to provide fairly reliable estimations of blood-oxygenlevels.
TREATMENT OF NEONATAL LUNG DISEASEWITH EXOGENOUS SURFACTANTIt has generally been accepted for more than 30 years thatrespiratory distress syndrome (RDS), or hyaline membranedisease, is associated with an abnormal gas-liquid interface inthe lung. Normal airways contain a surface-active substance,now called surfactant that reduces airway and alveolar surfacetension and therefore increases lung compliance. In the late1950s, studies determined that the liquid found in the airwaysof premature infants and of infants whose mothers had diabetesand who died with RDS had a diminished ability to decreasesurface tension in vitro (Avery & Mead, 1959; Pattle, 1958).Thus the hypothesis that decreased lung compliance in infantswith RDS was due to lack of surfactant was developed.
RDS is characterized by diffuse pulmonary microatelectasis.Atelectasis causes tachypnea, low tidal-volume breathing, andincreased work of breathing. Clinically, infants with RDS haveretractions as a consequence of decreased lung compliance,expiratory grunting to prevent further atelectasis, and hypox-emia secondary to intrapulmonary shunting. RDS is thereforedefined as the immediate onset after birth of tachypnea,retractions, grunting, and cyanosis in a premature infant or inan infant of a mother with diabetes. The chest radiograph inthese patients usually confirms the presence of diffusemicroatelectasis with uniform increased opacity of the alveolarportions of the lung and widespread air bronchograms. Thearterial carbon dioxide tension (PaCO2) may be eitherincreased or normal, thus reflecting the infant’s ability tocompensate for decreased lung compliance. When the infantbreathes room air, the PaO2 is always decreased because ofintrapulmonary shunting. The arterial hydrogen ion concen-tration (pH) reflects the presence or absence of an elevatedPaCO2 and the adequacy of tissue oxygenation. Infants withRDS often have both a metabolic and a respiratory acidosis.
Surfactant Biochemistry and PhysiologySurfactant is generally defined as the noncellular liquid foundin the more distal airways and alveoli of normal lungs.Although surfactant contains a mixture of various phospho-lipids, proteins, and neutral lipids, the extent to which each ofthese components contributes to the surface tensiondecreasing properties of surfactant is not certain.
Surfactant is produced and secreted by cuboid type IIpneumocytes that line the distal airways. Phospholipids andsurfactant-specific proteins are packaged within intracellularlamellar bodies. These are secreted by exocytosis into theliquid lining layer of the airway. Within the hypophase of thisliquid interface between the pneumocytes and lung gas,surfactant forms a regular microscopic latticework calledtubular myelin. It is thought that surfactant exerts its surfacetension decreasing activity by the movement of certain surfac-tant components from the hypophase to the gas-liquid inter-face. Surface tension is decreased by molecular interactions asthe gas-liquid interface is compressed during expiration. Anintrapulmonary conservation of surfactant, in which “usedsurfactant” is reabsorbed by the type II pneumocyte, isrepackaged, and is resecreted, probably exists.
Surfactant TherapySurfactant therapy has been one of the major advances in thecare of preterm infants (Table 2-2). Prophylactic and rescueadministration of synthetic and natural surfactants havereduced important adverse outcomes, including mortality(Shah et al, 1999; Soll, 1998a, 1998b, 1999, 2000; Soll &Morley, 2001; Soll & Blanco, 2001; Yost & Soll, 1999).Specifically, neonatal mortality [relative risk (RR), confidenceinterval (CI), and number needed to treat (NNT)] is decreasedwith prophylactic (vs rescue) administration of both synthetic(23% to 17%; RR 0.70; CI 0.58, 0.85; NNT 15) and naturalsurfactant (12% to 7%; RR 0.61; CI 0.48, 0.77; NNT 24)(Shah et al, 1999; Soll, 1998a, 1998b). Prophylactic adminis-tration of surfactants decreases the risk for pneumothorax andpulmonary interstitial emphysema. The lack of reduction inbronchopulmonary dysplasia (BPD) rates following surfactantreplacement is probably due in part to the increased survival(Cifuentes, 1996).
Trials have been conducted to determine if early (vsdelayed) rescue therapy with surfactant improves importantoutcomes. Early (less than 2 hours) vs delayed rescue surfac-tant (Yost & Soll, 1999) resulted in decreased risk for neonatalmortality (22% to 20%; RR 0.87; 0.77, 0.99; NNT 36). Earlyrescue administration reduced both pneumothorax (14% to12%, RR 0.70; CI 0.59, 0.82; NNT 50) and pulmonaryinterstitial emphysema (15% to 10%; RR 0.63; CI 0.43, 0.93;NNT 19). An alternative to early administration in manyinfants is to treat infants with surfactant before ventilation isneeded. Temporary endotracheal intubation for surfactantadministration when infants are requiring only continuouspositive airway pressure (CPAP) reduces the subsequent needfor mechanical ventilation and may reduce mortality and/orBPD (Verder et al, 1994, 1999).
Trials of natural and synthetic surfactants report superiorityof the natural surfactants. Natural (vs synthetic) surfactants(Hudak et al, 1996; Soll & Blanco, 2001) resulted in decreasedrates of pneumothoraces (12% to 7%; RR 0.63; CI 0.53, 0.75;NNT 22) and mortality (18% to 16%; RR 0.86; CI 0.76, 0.98;NNT 37).
Initial protocols of surfactant administration used single-dose therapies. However, when compared to a strategy of singledose of surfactant, a policy of administration of multiple dosesof surfactant when indicated according to the protocol resultedin decreased pneumothorax risk (18% to 9%; RR 0.63; CI0.30, 0.88; NNT 11) and a trend for less mortality.
Thus, a review of all the current evidence supports the useof prophylactic or early use of natural surfactants as early aswhen infants are requiring CPAP. More than one dose ofsurfactant should be administered, if indicated, to optimize thebenefits of this therapy.
20 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Name Source
Calf lung surfactant extract BovineHuman Amniotic fluidCurosurf PorcineSurvanta BovineInfasurf BovineExosurf Artificial
TABLE 2-2 Exogenous Surfactants
Ch02-X2942.qxp 11/22/06 3:22 PM Page 20

Collaborative Care: Surfactant TherapyNurses in particular play an important role in caring for infantswho receive surfactant replacement therapy in the NICU. Thecare of the infants before, during, and after surfactantadministration is unique to this treatment modality. It isimportant for nurses to have a working knowledge of thespecific care needs of infants treated with surfactant.
Before administration of surfactant, several factors shouldbe considered. Accurate weights of the infants must be deter-mined to ensure the proper doses of surfactant to be given.Confirmation of proper placement of the infants’ endotrachealtubes by chest radiographs must be documented. These infantsshould have continuous cardiac and respiratory monitoring.Cardiac monitoring may include electrocardiograms as well asarterial catheters. Respiratory monitoring may include trans-cutaneous measurement of PO2 or PCO2 and pulse oximetry.Nurses or physicians may also suggest increases in ventilatorsettings before dosing for infants who do not tolerate handlingor who become hypoxic quickly. Endotracheal suctioning isanother essential part of the care prior to the administration ofsurfactant. These infants should be suctioned approximately15 minutes before surfactant dosing to rid the infants of secre-tions that may inhibit the administration of the surfactant.
The care of infants during surfactant dosing is also unique tothis treatment modality. Of utmost importance during dosing isthe ongoing assessment and monitoring of the infants. Becausedosing with surfactant may impair ventilation transiently, nursesand physicians must be alert for signs that indicate the need toslow or stop the dosing momentarily to allow the infants torecover. Some signs that ventilation may be impaired includebradycardia, duskiness, and decrease in transcutaneous PO2 oroxygen saturation. Optimal positioning of infants during sur-factant administration is another critical facet of care. Infantsreceive some surfactants, such as Survanta (Columbus, OH:Ross Labs), in four aliquots, each in a different body position.
The infants are positioned head down, head turned to theright; head down, head turned to the left; head up, head turnedto the right; and head up, head turned to the left. The infantsare held in each position for 30 seconds after the dose isadministered into the endotracheal tube. Administration ofExosurf requires only turning the head from midline to theright, then midline to the left.
Lastly, nurses have specific responsibilities after surfactant isadministered to infants. Immediately after dosing, the nurseshould assess the infant’s skin color, respirations, oxygen satu-ration, and transcutaneous monitoring. Arterial blood gasshould be sampled, and the ventilator should be weaned appro-priately. Surfactant produces changes in pulmonary com-pliance that generally requires rapid weaning of ventilatorsettings, but some infants may also experience respiratorydistress immediately after dosing. Endotracheal suctioning isdelayed after dosing of surfactant for at least 1 to 2 hours toprevent removal of the instilled surfactant. Other side effectsof this effective therapy are sudden changes in cerebral bloodflow, which makes intraventricular hemorrhage a realpossibility, and changes in retinal blood flow, which increaseschances for retinopathy of prematurity.
CONVENTIONAL VENTILATORY SUPPORT ANDRESPIRATORY CONSIDERATIONSThis chapter focuses on the ventilator technologies and strat-egies. Both continuous positive airway pressure (CPAP) and
conventional mechanical ventilation (CMV) continue to bethe mainstay of the care of infants with respiratory failure.
Continuous Positive Airway PressureContinuous positive airway pressure can be defined as the useof positive pressure continuously throughout the respiratorycycle. The use of CPAP requires that the infant be breathingspontaneously without the full support of a ventilator. Threedevices are commonly used to administer CPAP (nasal prongs,endotracheal tubes, and nasopharyngeal tubes), each with itsown advantages and disadvantages. Nasal prongs are nonin-vasive but may not always transmit optimal pressure to theairway because they are easily dislodged and may cause damageto the nasal septum with prolonged use. Endotracheal tubesgive optimal transmission of pressure and can be convertedeasily to mechanical ventilation but can cause pharyngealgrooves or subglottic stenosis with prolonged use. Nasopharyn-geal CPAP is more stable than prongs but can result innasopharyngeal irritation and plugging with secretions.
Physiologic effects of CPAP are increased transpulmonarypressure with a resultant increase in functional residual capa-city, stabilization of collapsed alveoli, and improvement inventilation-perfusion matching. These improvements lead tobetter oxygenation and ventilation. In preterm infants withrelatively floppy airways, CPAP can provide increased pressureto the posterior pharynx and prevent airway collapse duringinspiration and prevent obstructive apnea (Hansen, 1998).Although CPAP is relatively safe, some complications areassociated with its use. Excessive levels of CPAP can raiseintrathoracic pressure and compress the right atrium and venacava, thus compromising venous return. Excessive CPAP mayalso overdistend alveoli and result in air leaks.
Conventional Mechanical VentilationThe two types of conventional ventilators commonly used inneonatal intensive care units are pressure or volume ventila-tors. Pressure ventilators are used more frequently than volumeventilators. These ventilators are constant-flow, time-cycled,and pressure-limited devices. This means there is a constantflow of gas through the endotracheal tube, breaths are given atfixed intervals, and a preset peak inspiratory pressure (PIP) ismaintained through the duration of the inspiration. In apressure-limited ventilator an increase in ventilation (decreasein pO2) can be achieved by increasing ventilator rate orincreasing tidal volume. Oxygenation improvement is achievedby increasing the mean airway pressure (increasing PIP,increasing Ti, increasing PEEP, increasing flow, and increasingrate) or by increasing the FiO2. An increase in ventilation(decrease in pCO2) can be achieved by increasing ventilatorrate or increasing tidal volume. If compliance changes in acompression ventilator, no change in pressure is delivered. Thedisadvantages are decreases in tidal volume if the compliancedecreases or overdistention if compliance improves.
Volume ventilators deliver the same tidal volume with eachbreath, regardless of the pressure needed to achieve the presetvolume. In a volume-limited ventilator, an increase in venti-lation is achieved by increasing the ventilator rate or increas-ing delivered tidal volume. An increase in oxygenation willoccur if the FiO2, PEEP, or tidal volume is increased. Thedisadvantage to the volume ventilator is that a fixed volumewill be delivered regardless of changes in compliance and canlead to the use of very high PIPs.
21CHAPTER 2 Emerging Technologies for the Management of Respiratory Disorders
Ch02-X2942.qxp 11/22/06 3:22 PM Page 21

The newer conventional ventilators can use a variety ofdifferent operating modes. In this chapter, intermittentmandatory ventilation (IMV), synchronous IMV, and assistcontrol will be briefly discussed. IMV provides a continuousflow of oxygen/air mixture through the ventilatory circuit;however, the neonate can breathe spontaneously. The termmandatory refers to the number of mandatory breaths perminute that are set by the caregiver. The settings allow PIP,rates, inspiratory time, and flow to be adjusted to individualventilation. This very simply means giving intermittentbreaths at a fixed rate. If the infant is breathing faster than thepreset rate, then the ventilator does not support those breaths.The disadvantage with this mode is that infants may exhaleduring the ventilator’s inspiratory cycle and thus “fight” againstthe ventilator. SIMV is similar to IMV except that theventilator senses the infant’s spontaneous respirations andmechanically delivered breaths are synchronized to thoseefforts. If the infant is breathing faster than the set SIMV rate,those breaths are not supported, which is similar to the IMVmode. SIMV is more flexible than IMV and can be used forprimary ventilatory support and weaning. However, in somecases SIMV may fail as a weaning mode because at low set ratesthe infant must exert a considerable work of breathing.Assist/control ventilation (A/C) is also known as patient-triggered ventilation (PTV). This therapy uses the sponta-neous respiratory efforts of the infant to “trigger” a mechanicalbreath by the ventilator. In PTV a sensor is used to detect avariety of stimuli such as airflow, airway pressure, chest wallmovement, and esophageal pressure. When the machinedetects an inspiration, it delivers a breath with a preset PIP,inspiratory time, and airflow. PTV is therefore similar to SIMVand has the theoretical advantage of supporting all breaths bythe ventilator, even those above the set rate. A disadvantageof PTV is that very immature infants have weak respiratoryeffort that does not trigger this machine (Carlo &Ambalavanan, 1999). Backup respiratory rates may be used toreduce this problem.
There is emerging consensus that ventilator support, byitself, may inflict lung injury (Artigas et al, 1998; Clark et al,2001). A strategy to minimize ventilator-associated lung injuryis the use of CPAP instead of endotracheal intubation. Severalretrospective studies suggest that the decreased need forventilator support with the use of CPAP may allow lunginflation to be maintained but may prevent volutrauma due tooverdistention and/or atelectasis. However, preliminary sum-maries of three large multicenter randomized controlled trialsincluding a total of 495 preterm infants do not report benefitsof early CPAP (Finer et al, 2005; Sandri et al, 2004; Thomson,2002). Further research on the use of early CPAP is ongoing.Interestingly, nasal intermittent mandatory ventilation (vsnasal CPAP) reduces extubation failure in small trials (18% to7%; RR 0.39; CI 0.16, 0.97; NNT 9) and this could be analternative to prevent intubation (Greenough et al, 2000).
The strategy most evaluated with conventional mechanicalventilation is the use of high rates and presumably small tidalvolumes as PaCO2 levels were kept in comparable ranges.Meta-analyses of the randomized controlled trials of high (>60per min) vs low (usually 30 to 40 per min) rates (and presumedlow vs high tidal volumes, respectively) revealed that the high ventilatory rate strategy led to fewer air leaks (28% to19%; RR 0.69; CI 051, 093; NNT 11) and a trend for increasedsurvival.
If mechanical ventilation is needed, a ventilatory approachof small tidal volumes and permissive hypercapnia can beemployed (Carlo et al, 2002; Hargett, 1995; Mariani et al,1999). Permissive hypercapnia is a strategy for the manage-ment of patients receiving ventilatory support in whichpriority is given to the prevention or limitation of lung injurysecondary to the ventilator by tolerating relatively high levelsof PaCO2 rather than maintenance of normal blood gases(Acute Respiratory Distress Syndrome Network, 2000; Carloet al, 2002; Mariani et al, 1999). A multicenter trial of infants <1000 g reported that permissive hypercapnia (target PaCO2 >50 mm Hg) during the first 10 days led to atrend for reduced BPD or death at 36 weeks (68% vs 63%).Furthermore, the strategy of permissive hypercapnia reducedseverity of BPD as evidenced by a decreased need of ventilatorsupport at 36 weeks from 16% to 1% (P <0.005). In summary,a gentle ventilator strategy of small tidal volumes, higher rates,and permissive hypercapnia may reduce BPD in very preterminfants, but further research is needed.
Hyperoxia may also contribute to lung injury in preterminfants. Thus, permissive hypoxemia is another strategy thatmay reduce BPD. Trials to target different levels of oxygensaturations performed for treatment of retinopathy of pre-maturity (STOP-ROP Pediatrics, 2000) or BPD (Askie et al,2003) revealed that the groups with lower saturation targets(89% to 94% and 91% to 94%, respectively) had less need foroxygen supplementation and fewer BPD/BPD exacerbations.Further trials of permissive hyperoxemia are needed before thisstrategy can be recommended. Technological advances,including improvement in flow delivery systems, triggering ofinspiration, breath termination criteria, guaranteed tidalvolume delivery, stability of PEEP, air-leak compensation,prevention of pressure overshoot, and on-line pulmonaryfunction monitoring have resulted in better ventilators.Patient-initiated mechanical ventilation, patient-triggeredventilation, and synchronized intermittent mandatoryventilation are being used increasingly in neonates.
HIGH-FREQUENCY VENTILATIONIn contrast to high-frequency ventilation (HFV), CMV usesventilator rates and tidal volumes that correspond to the spon-taneous ventilation patterns of newborns. High mean and peakairway pressures may be required during CMV to adequatelyventilate noncompliant lungs. Exposure to high inflating pres-sures may lead to lung and airway injury, including pulmonaryinterstitial emphysema, pneumothoraces, bronchopleural fistulas,and bronchopulmonary dysplasia. HFV attempts to avoid thesecomplications by delivering low tidal volumes at high frequen-cies. HFV may be used as a “rescue” technique to prevent furtherdamage in infants who have developed complications secondaryto CMV. HFV allows severely ill infants to be adequatelyventilated at lower volumes than with CMV while improvinggas exchange. HFV may be used perioperatively and postopera-tively to reduce movement of the airway and thoracic cavity.HFV may be beneficial to infants who have preexistingpneumothoraces or bronchopleural fistulas. There is nogenerally accepted ventilator rate, which defines the term highfrequency. Accepted definitions generally include ventilatorrates at 2 to 4 times the natural breathing frequency andventilation with tidal volumes smaller than anatomic deadspace. Gas transport during high frequency cannot be explainedby conventional concepts of ventilation and lung mechanics.
22 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Ch02-X2942.qxp 11/22/06 3:22 PM Page 22

Three types of HFV are approved for use in the UnitedStates: the high-frequency oscillatory ventilator (HFOV), thehigh-frequency jet ventilator (HFJV), and the high-frequencyflow interrupter (HFFI) (Table 2-3). The HFOV has adiaphragm or piston that oscillates a flow of gas, thus creatingboth positive and negative pressure changes. Mean airwaypressure is generated by gas flow through a filter, which acts asa resistor. The respiratory therapist or clinician can adjust themean airway pressure, frequency, and amplitude. The meanairway pressure affects lung inflation and can be increased byincreasing MAP oxygenation. The piston amplitude affectsventilation, and increases in ventilation occur when amplitudeis increased. The HFOV is the only HFV in which inspirationand exhalation are active.
HFJV delivers tidal volumes that may be less than or greaterthan anatomic dead space at frequencies of 60 to 600 breathsper minute. HFJV operates similarly to constant-flow time-cycled ventilation with passive expiration. With an HFJV, ahigh-pressure gas source is connected to a small airway cannulawith use of a high-frequency flow interrupter valve. This valveopens and closes rapidly, thus propelling the pressurized gasinto the airway. HFJV requires a specific endotracheal tubewith a lumen for the jet gas flow and a lumen for the fresh gasflow. The fresh gas flow allows entrainment of gases andaddition of PEEP. There is a port, near the jet gas flow lumen,for the instillation of nebulized saline to prevent trachealerosion. A conventional ventilator may be used with a jetventilator to provide “background” ventilation or sighs at alow rate. Background ventilation may decrease the risk formicroatelectasis that may occur with long-term HFJV. Theoperator can adjust the PIP of the jet and the CMV as well asthe PEEP and frequency. To increase the pO2, the operatoradjusts PEEP and FiO2. Elimination of carbon dioxide isdependent mostly on the PIP-to-PEEP pressure difference.
The HFFIs have both conventional and high-frequencyoptions. A high-pressure source of gas is delivered into astandard ventilator circuit, and this flow of gas is interruptedby a valve mechanism that is operated by a microprocessor.The operator can adjust the PIP, PEEP, and frequency. Theconventional ventilator is often used to give intermittent“sigh” breaths. Oxygenation depends primarily on the PEEPthat is delivered by the conventional ventilator, whereasventilation depends primarily on the difference between thePIP and the PEEP.
HFOV and high-frequency flow interruption have beenevaluated in 12 randomized controlled trials including morethan 3000 stable preterm infants. Even though there is someheterogeneity in results between the trials, meta-analysisreveals no clear evidence that high-frequency oscillatory
ventilation is superior to conventional as the initial mode ofventilatory support (Thome et al, 2005). There are trends forreduction in mortality and BPD (Thome & Carlo, 2003;Henderson-Smart et al, 2003) despite a significant increase inair leaks with HFOV (OR 1.23; CI 1.04-1.46; NNT 30). Also,there are trends for an increase in grade 3 to 4 intraventricularhemorrhage and periventricular leukomalacia but the resultsare inconsistent (Thome & Carlo, 2003). Long-term outcomestudies do not show an advantage of high-frequency venti-lation over conventional ventilation. HFJV in stable preterminfants resulted in less BPD at 36 weeks’ (33% to 20%; RR0.59, 0.35, 0.99; NNT 8) but the data are limited (Bhuta &Henderson-Smart, 2002).
HFV has also been used as a rescue mode in severalrandomized controlled trials. A trial in infants with severeRDS observed a reduction in air leaks and development andprogression of air leaks in infants randomized to HFOV (HiFOStudy Group, 1993). However, there was no improvement inother major outcome measures. HFJV in preterm infants withpulmonary interstitial emphysema led to a more frequent andfaster resolution of emphysema but no reduction in mortalityor other adverse outcomes (Keszler et al, 1991).
Few data from large, multicenter, randomized trials thatexamine the use of HFV for lung diseases other than RDSexist. It is generally accepted that HFV is useful in themanagement of newborns with severe pulmonary interstitialemphysema because airway pressures may be significantlyreduced and thus theoretically decrease the risk for further airleak, other pressure-related airway injury, and decreasedcardiac output.
Complications Associated with High-Frequency VentilationHFV can provide adequate ventilation to infants, but its use isassociated with the possibility of complications. The gases thatare used during HFV need to be heated to avoid the delivery ofcold gas into the airway. Cold air can lead to hypothermia andnecrotizing tracheobronchitis (NTB). NTB is a lesion of theairway that is caused by epithelial erosion and loss of cells inthe airway; it is commonly found near the distal end of theendotracheal tube. It leads to formation of granulation tissuethat can cause impaired gas exchange, airway obstruction, oratelectasis. With high ventilatory frequencies, the inspiratoryand expiratory times are decreased, which may increase therisk for gas trapping in the lungs. Gas trapping occurs less oftenduring HFOV because it is the only form of HFV in whichexpiration is active. With some high-frequency ventilators,such as the jet-and-flow interrupter, expiration occurs bypassive recoil of the distended respiratory system (lung andchest).
Nursing Care—High-Frequency VentilationCaring for infants who receive HFV presents many challengesto NICU nurses. Nurses must adopt new skills and alter thoseused in caring for infants who are conventionally ventilated.Specific care needs unique to infants who receive HFV includephysical assessment, airway management, positioning, andcomfort (Tables 2-4 and 2-5).
One of the most challenging yet critical aspects of caring forthese infants is the physical assessment. Recognizing subtlechanges in the physical exam is critical because these changesmay signify changes in the infant’s condition. Of extreme
23CHAPTER 2 Emerging Technologies for the Management of Respiratory Disorders
Maximal Rate Type (breaths/min) Expiration
Pressure-limited, time-cycled 150 PassiveJet 250 to 300 PassiveOscillator 1800 Active
Classification of High-FrequencyNeonatal Ventilators
TABLE 2-3
Ch02-X2942.qxp 11/22/06 3:22 PM Page 23

importance is the assessment of chest wall vibration, which isan indicator of tidal volume. Even small changes in the vibra-tions may indicate a change in the neonate’s condition.Decreased chest vibration may indicate pneumothorax,endotracheal secretions, and mechanical malfunction. Thenoise of the ventilator and the constant vibration of theinfants make auscultation of breath sounds, heart tones, andbowel sounds difficult. If oscillating ventilators are used, thisevaluation is best done when the infants are momentarilyremoved from the ventilator (for routine circuit changes) orwhen the ventilator is in standby (interruption of oscillation
but not from ventilator mean airway pressure). Disconnectionfrom HFV is discouraged because of possible alveolar collapseand loss of lung volume. Therefore, when necessary, discon-nection from HFV should be limited to short periods. If theinfant is receiving HFOV, it is also important to auscultatebreath sounds to assess the symmetry of oscillatory intensitywhile he or she is being oscillated.
The second specific area of care unique to infants whoreceive HFV is airway management. Suctioning of theseinfants requires two people—one person to suction andanother to either manually ventilate or return the infants to
24 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Responsibility Intervention
Obtain and record baseline physiologic data Record temperature, heart rate, respiratory rate, systolic and diastolic blood pressures, transcutaneous PO2, and PCO2
Obtain and record baseline biochemical data Draw blood samples for arterial gasesMaintain current ventilation Record ventilator parameters: rate, PIP, PEEP, MAP, inspiratory:expiratory ratio, FiO2
Assemble and prepare equipment Ensure that infant is attached to monitoring devices for heart rate, intra-arterial blood pressure, transcutaneous oxygen and carbon dioxide
Check alarms on all monitorsAssist with arterial line insertion
From Inwood MS (1991). High-frequency oscillation. In Nugent J, editor. Acute respiratory care of the neonate. Petaluma, CA: NICU Ink.
Nursing Responsibilities and Interventions for Oscillated Infants Before High-Frequency VentilationTABLE 2-4
Responsibility Intervention
Monitor and document physiologic parameters Record hourly temperature, heart rate, spontaneous respirations, systolic and diastolic blood pressure
Measure and record accurate intake and output of fluids every 8 hoursMonitor and document biochemical parameters Draw arterial blood gas samples as orderedMaintain patent airway Monitor for continuous vibration of chest
Assess transcutaneous PO2 and PCO2 hourlyPerform endotracheal suctioning every 2 hours and prnRecord amount, color, and consistency of secretionsAssess bilateral air entry while hand bagging at sigh pressures, before and after
suctioningEnsure adequate humidification of gas flow
Prevent pneumothorax Maintain ordered MAPObserve for decreased vibrations of the chestAssess infant for signs of respiratory difficulty: increased spontaneous respirations,
increased chest retraction, diminished air entry, increased FiO2 requirements, increased transcutaneous PCO2 readings
Obtain chest radiograph as required and ensure that oscillator is stopped during filming
Provide pulmonary support Monitor and record MAP, amplitude, frequency, and FiO2 hourlyPerform a sustained inflation after endotracheal suctioning and disconnection at
ordered pressure and durationRecord infant’s response to sigh
Provide physical care Reposition infant from side to side or from prone to supine every 2 hoursProvide emotional support to family Provide accurate, consistent information
Promote bonding by encouraging nurse specialist or social worker for assistance with coping skills
Encourage parents to attend parents’ support group
From Inwood MS (1991). High-frequency oscillation. In Nugent J, editor. Acute respiratory care of the neonate. Petaluma, CA: NICU Ink.MAP, Mean airway pressure.
Nursing Responsibilities and Interventions for Oscillated Infants During OscillationTABLE 2-5
Ch02-X2942.qxp 11/22/06 3:22 PM Page 24

HFV. Remember that disconnection from HFV may lead toalveolar collapse, so the infants may need to be manuallyventilated or the mean airway pressure increased aftersuctioning. It is generally accepted practice to suction infantswhile they are disconnected from HFOV and HFJV. Position-ing and comfort of infants who are receiving HFV are alsoimportant facets of care. Because of the physical restraints ofthe delivery devices and the importance of disconnecting theinfant from the ventilator for only short durations, positioningand repositioning become challenging. Two caregivers shouldbe used for repositioning—one to turn the infant and stabilizethe endotracheal tube and another to reposition the circuitand ventilator. Although water mattresses are not recom-mended, sheepskins, lamb’s wool, and egg-crate mattresses maybe used to provide comfort and prevent skin breakdown.However, there is rising concern that infants may inhale fibersfrom sheepskin, so it may not be used in some units.
Sedatives, paralytics, and analgesics may be necessary tofacilitate comfort for infants while they are receiving HFV.Interventions such as bundling and soothing music maydecrease the need for pharmacologic agents. Whereas somebelieve that the noise and the constant vibration may bedisturbing to the infants, others believe them to have acalming effect.
INHALED NITRIC OXIDEIn the past 20 years, it has become apparent that vascularendothelium has an important role in the regulation of bloodvessel smooth muscle tone as well as in other importantphysiologic functions. Relaxation of vascular smooth muscle inresponse to acetylcholine requires an intact endothelium.Nitric oxide (NO) is thought to be the molecule released fromthe endothelium that is responsible for vascular smooth musclerelaxation. These findings were the catalyst for additionalinvestigations of the biologic effects of NO.
NO has an unpaired electron and therefore rapidlycombines with other free radicals. The biologic half-life of themolecule is estimated to be 110 to 130 msec. In vivo, biologicactivity of NO is limited because it is rapidly inactivatedwithin the vessel lumen. Inactivation occurs because NO hasa high affinity for hemoglobin and avidly binds to the iron ofheme proteins to form a biologically inactive compound,nitrosyl-hemoglobin. Nitrosyl-hemoglobin is then oxidized toform methemoglobin and nitrate.
The NO molecule is synthesized from the amino acid L-arginine in a reaction that is catalyzed by a group of enzymescalled the nitric oxide synthases (NOS). The by-product ofthis reaction is L-citrulline: L-arginine + molecular O2 → NO+ L-citrulline.
Three major types or isoforms of NOS exist. The first isoformis the endothelial or constitutive type, which is located invascular endothelial cell wall, endocardium, myocardium, andplatelets. Neuronal NOS is the isoform located in both theperipheral and central nervous systems. The third isoform, indu-cible NOS, is not present under normal physiologic conditionsbut is produced in response to various inflammatory stimuli.Excitation of the inducible NOS causes production of muchgreater quantities of NO than activation of other isoforms.Activation of inducible NOS during sepsis plays a major partin producing vasodilation and consequent hypotension.
The biologic actions of NO are mediated through theguanylate cyclase–cyclic guanosine monophosphate (cGMP)
system. After formation from L-arginine in the endothelialcell, NO readily diffuses into the cytosol of smooth musclebecause it is a small, lipophilic molecule. Once inside thesmooth muscle cell, NO binds soluble guanylate cyclase, whichin turn catalyzes the formation of cGMP from guanosinetriphosphate. Increases in cGMP lead to activation of cGMP-dependent protein kinase, which triggers a reduction in intra-cellular calcium concentration through extrusion andsequestration. The decreased calcium concentration causessmooth muscle relaxation.
NO is a biologic mediator of a variety of physiologicresponses in numerous systems in the body. In the healthystate, the arterial circulation is partially dilated by basalproduction of NO in the endothelium. At birth, production ofendogenous NO in response to rhythmic distention of thelung, shear stress, and acetylcholine release plays a major rolein mediating a decrease in pulmonary vascular resistance. Inaddition to being an important determinant of basal tone insmall arteries and arterioles, NO inhibits platelet aggregationand adherence and may alter vascular permeability. In thenervous system, NO may have a role in memory formation,pain perception, and electrocortical activation, but moreresearch is needed to support this hypothesis. In the gastro-intestinal and genitourinary tracts, NO participates in controlof signals that regulate smooth muscle relaxation. NO is pro-duced in large quantities in response to various immunologicstimuli. It may also have a role in nonspecific immunitybecause it is generated when macrophages are activated.
A particularly frustrating problem for caregivers in theNICU is the treatment of acute hypoxic respiratory failure dueto pulmonary arterial vasoconstriction. Successful adaptationfor extrauterine life depends on the ability of the fetus to makea transition from fetal to postnatal circulation. A variety offactors, probably related to adverse intrauterine events, mayalter the ability of the newborn to decrease pulmonary vascularresistance at birth and make this adaptation. When pulmonaryvascular resistance remains elevated postnatally, blood isshunted right to left across the ductus arteriosus and foramenovale and away from the lungs, thus causing hypoxemia. Thiscondition, PPHN, is seen either in isolation or in conjunctionwith various diseases such as meconium aspiration syndrome,severe birth asphyxia, sepsis, congenital diaphragmatic hernia,and RDS. In the past, pharmacologic interventions—such astolazoline, an alpha-adrenergic blocker with histamine-likeproperties—have been used to decrease pulmonary vascularresistance. However, the effects of these drugs are unpre-dictable and inconsistent, and because they are not selectivefor the pulmonary bed, nearly 50% of patients developsystemic hypotension. Sodium nitroprusside is another drugthat causes vasodilation through activation or release of NO,but it is not selective for the pulmonary arterial bed anddecreases systemic vascular resistance as well. Other intra-venous vasodilators, such as prostaglandin I2 and adenosinetriphosphate–magnesium chloride, may selectively decreasepulmonary vascular resistance. The ideal agent for thetreatment of pulmonary hypertension would be one that causespulmonary vasodilation without decreasing systemic vascularresistance.
The early 1990s saw the development of theories thatinhaled NO would diffuse from the alveolar space across theepithelium to directly mediate vascular smooth musclerelaxation. Ultimately, NO would diffuse into the lumen of the
25CHAPTER 2 Emerging Technologies for the Management of Respiratory Disorders
Ch02-X2942.qxp 11/22/06 3:22 PM Page 25

pulmonary blood vessels and be inactivated on binding hemo-globin, thus avoiding effects on the systemic circulation.Theoretically, inhaled NO could increase systemic oxygena-tion by two mechanisms: by global pulmonary arterialvasodilation with increased pulmonary blood flow and cardiacoutput or by improved matching of ventilation and perfusionin the lung.
Concern grew, however, with potential toxic effects thatmight be associated with the use of inhaled NO. One potentialproblem is the formation of excess amounts of methemoglobin,thus causing the clinical condition known as methemoglo-binemia. This serious condition is associated with hypoxemiabecause of the inability of methemoglobin to carry oxygen.The body’s defense mechanism against the formation of methe-moglobin is the enzyme methemoglobin reductase, which readilyconverts methemoglobin back to hemoglobin. If the rate ofaccumulation of methemoglobin is slow, this enzyme will limitincreases in methemoglobin. To date, significant methemo-globin levels have not been noted in trials in which lowconcentrations of inhaled NO have been used in neonates.
Another possible problem is the production of nitrogendioxide and higher oxides of nitrogen such as peroxynitritewhen NO is used with high concentrations of oxygen.Nitrogen dioxide and peroxynitrite in high concentrations candirectly damage the lung. Using low concentrations of NO andlimiting the time of mixing of NO and oxygen minimizes theformation of these toxic molecules.
Large multicenter, double-masked, randomized, placebo-controlled studies have determined that inhaled nitrous oxide(INO) can decrease the need for ECMO in infants withPPHN. The NINOS study enrolled 235 patients under the ageof 2 weeks with PPHN and compared responses to either 20ppm of INO or placebo gas, which was 100% oxygen. Theprimary hypothesis was that INO would result in a reductionin the risk of death or need for ECMO by 120 days from 50%in controls to 30% in infants who received INO (Finer, 2000).This study encouraged the use of all other aggressive modalitiesin the treatment of PPHN and was terminated early by anExternal Data Safety Monitoring Committee when treatedinfants were shown to have a statistically significant lower riskof death or need for ECMO. Another well-conductedmulticenter trial matched control and treatment infants fordiagnoses, blood gases, oxygen indices, and ventilator settings(Roberts et al, 1992). The trial was stopped early at interimanalysis when it demonstrated a significant increase insystemic oxygenation when INO-treated infants were com-pared to controls. A third multicenter randomized trialcompared high-frequency oscillatory ventilation (HFOV) toINO in term and near-term infants with hypoxic respiratoryfailure (Kinsella & Abman, 1995). This study showed anequivalent response to either modality. In this study, if infantsfailed to respond to either treatment used alone (n = 125), theywould then receive treatment with both. Thirty-two percent ofinfants who failed with a single modality improved with acombination of both treatments, which led the investigators tospeculate that INO works better with maximized lung recruit-ment. A recent, large randomized study had similar results tothe NINOS trial despite the use of lower doses of nitric oxide(Clark et al, 2000). A total of 248 infants with hypoxemicrespiratory failure were randomly assigned to be controls or toreceive treatment with 24 hours of INO at 20 ppm followed byanother 96 hours of INO at 5 ppm. The two groups were then
compared with regard to ECMO requirements. Sixty-fourpercent of controls vs 38% of treated infants (P = 0.001)required ECMO. Mortality was not different in the two groups,but treated infants showed a lower incidence of broncho-pulmonary dysplasia. INO significantly improves oxygenationand lowers the oxygenation index 30 to 60 minutes aftertreatment. A significant overall reduction in the combinedincidence of need for ECMO and death in infants treated withINO also occurs. Extensive data on long-term outcome ofinfants treated with INO are not yet available. Some existingdata on neurodevelopmental follow-up after the NINOS trialhave been gathered (Finer & Barrington, 2001). Of the 173infants seen at follow-up, no differences exist between controland INO-treated infants with respect to incidence of cerebralpalsy, mental or psychomotor development index scores, orhearing loss. The currently published trials of inhaled nitricoxide for preterm infants present heterogeneous results(Barrington & Finer, 2006; Field et al, 2005; Schreiber et al,2003; Van Meurs et al, 2005) and do not support the routineuse of inhaled nitric oxide in this subpopulation. Furtherclinical trials are ongoing.
NO gas is supplied in aluminum tanks that contain highconcentrations of gaseous NO in equilibrium with inertnitrogen. This gas is added to the inspiratory limb of theventilator circuit by flowmeters and blenders. Use of high flowrates limits NO mixing time with oxygen and decreases theformation of nitrogen dioxide. Scavenging equipment at theexpiratory limb of the ventilator eliminates potentially toxicexhaust gases. In-line monitoring of NO and a chemolumi-nescence analyzer performs nitrogen dioxide tests to determinelevels. Samples of gas in the ventilator circuit are aspirated,and the concentrations of these two molecules are determined.Blood is periodically monitored for methemoglobin levelswhen patients receive INO.
INO holds promise as a selective pulmonary vasodilatorthat may soon be added to the clinician’s armamentarium.Several small pilot studies suggest that INO may be effective indecreasing pulmonary vascular resistance and improvingoxygenation without reducing systemic blood pressure orcardiac output. Extreme care must be taken to monitor bloodlevels of methemoglobin and the formation of higher oxides of nitrogen when NO is used. Until larger controlled trials arecompleted, the benefit-to-risk ratio of INO as a possible treat-ment for neonatal pulmonary hypertension remains unknown.
Collaborative Care: Nitric OxideMulticenter trials have shown that INO decreases the chancethat some critically ill infants will need ECMO. Future studiesare currently underway to determine the most effective andsafe doses of INO in the management of term and preterminfants with respiratory dysfunction. Over the next severalyears the use of this treatment modality will slowly increase,and the nursing care of these infants as we know it today willchange. Like liquid ventilation, NO therapy will bring with itmany new challenges to NICU nurses and physicians.
TREATMENT OF NEONATAL HYPOXEMIA WITH EXTRACORPOREAL MEMBRANEOXYGENATION (ECMO)ECMO is a complex and expensive therapy for infants withsevere respiratory failure. Because this therapy has limitedapplicability to most NICU nurses, it will be discussed only
26 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Ch02-X2942.qxp 11/22/06 3:22 PM Page 26

briefly. The first heart-lung machines, designed to serve thefunction of cardiopulmonary bypass during pediatric cardiacsurgery, were developed in the 1950s. Blood was removed fromthe patient and pumped through an oxygenator before returnto the systemic circulation. At the end of the surgical proce-dure, the patient was disconnected from the machine, andpulmonary and systemic flows were restored with the patient’sown heart as the pump. In the mid-1970s, the first attempts atprolonged cardiopulmonary bypass in infants with potentiallyreversible hypoxemia were made. The differences betweenthese efforts and those employed during cardiac surgery werethat the duration of bypass was measured in days rather thanhours and that the underlying disease that led to hypoxemiawas potentially reversible lung disease rather than primarycardiac disease.
In the past 20 years, prolonged cardiopulmonary bypass,also known as extracorporeal membrane oxygenation(ECMO) or extracorporeal life support, has been used inthousands of newborn infants with hypoxemia that appears tobe intractable to aggressive nonsurgical management. A fewcontrolled clinical trials of ECMO have shown its effectiveness(UK Collaborative Trial Group, 1996). Despite its efficacy inimproving oxygen delivery in sick newborns and markedlyincreasing survival, there is concern for morbidity associatedwith its use.
ECMO is widely used in the United States as well as inseveral other industrialized nations. Neonatal ECMO is usedin the management of intractable hypoxemia in near-termnewborns with meconium aspiration syndrome, RDS, pneu-monia/sepsis, and congenital diaphragmatic hernia. Contra-indications to the use of ECMO exist. The most importantcontraindication is prematurity. Early reports of ECMO use inpremature infants revealed alarmingly high rates of intra-cranial hemorrhage. Whether intracranial hemorrhage inthese patients is related to the systemic anticoagulationrequired with ECMO or to the abnormal cerebrovascularpressures and flows associated with ECMO is unknown. Othercontraindications to ECMO include preexisting intracranialhemorrhage and hypoxemia that is not potentially reversible,such as that seen in patients with cyanotic congenital heartdisease.
The follow-up study of the 4-year-old children enrolled in a trial of ECMO revealed that ECMO resulted in a decrease in death/disability (37% vs 59%, RR 0.55; CI 0.47–0.86) with a number needed to treat of only 4 to 5 (Bennett et al,2001). This study provides strong evidence for the efficacy and safety of ECMO.
ECMO is an expensive and labor-intensive procedure. Twocaretakers are required 24 hours per day—one to provide nursingcare directly to the patient and one to monitor the functionalintegrity of the circuit and its various components because avariety of technical malfunctions can occur. During ECMO thecircuit must be heparinized, and the most frequently reportedECMO complication is hemorrhage secondary to this. Table 2-6lists other common complications of ECMO.
Although it is used widely, ECMO is likely to be replaced by less invasive and less risky preventive and therapeuticprocedures. However, at this time, referral to an ECMO centeris a logical approach when infants with severe hypoxicrespiratory failure do not respond to surfactants, convention-al or high-frequency ventilation, or inhaled nitric oxidetherapy.
LIQUID VENTILATIONThe skills, technologies, and resources for managing respira-tory compromise in neonates have continued to improve.Despite these advancements, prematurity and respiratorydistress are still associated with significant morbidity andmortality. Modern therapies can cause lung injury thateventually may lead to a chronic lung disease. To decrease lunginjury, efforts have concentrated on decreasing inspiredoxygen concentration and decreasing inspiratory pressure. Todecrease inspiratory pressure, surface tension in the alveolimust be uniformly decreased. This surface tension arisesbecause of the air-liquid interface at the lining of the alveolarmembrane. Surfactant therapy is used to decrease surfacetension but is not always successful in improving acute respi-ratory distress or preventing chronic lung disease. Liquidventilation has been studied as a therapy that could reducesurface tension in the alveoli. Because this therapy is stillconsidered experimental, it will only briefly be discussed.
As early as the 1920s, it was demonstrated that oxygenatedsaline could be used to inflate the lung and improveventilation. However, saline proved to be inadequate becauseof its low gas-carrying ability and its high viscosity. In 1966, itwas first demonstrated that perfluorochemical liquids couldsupport the respiration of animals. Perfluorochemical liquidsare inert, have high solubility for respiratory gases, andminimize surface tension. They appear to be absorbed onlyminimally through the mature epithelium. Limited clinicalexperience and extensive work in animals suggest that thesecompounds are relatively nontoxic, even when givenintravenously.
A liquid gel surfactant that acts to decrease surface tension,enhance alveolar stability, and protect the respiratory epithe-lium lines the alveolus. The surface-tension forces within thealveolus are the result of the air-fluid interface and are dramati-cally increased by the absence of surfactant. Surfactant produc-tion and function are usually deficient in preterm infants. Thisdeficiency results in noncompliant alveoli that tend to collapsespontaneously. Because surfactant deficiency tends to benonhomogeneous, alveolar surface tension varies from oneportion of the lung to another. Respiratory function in preterminfants is characterized by stiff lungs, increased work ofbreathing, uneven ventilation, and ventilation-perfusionmismatch. One way to decrease alveolar surface tension is toeliminate the air-liquid interface in the alveolus by filling itwith liquid. Elimination of the air-liquid interface can improvealveolar compliance, reverse ventilation-perfusion abnormali-ties, and—if the liquid contains oxygen—increase oxygenuptake (Shaffer et al, 1999).
Tidal Liquid VentilationEfforts were initially made to entirely replace gas breathingwith liquid respiration. In tidal liquid ventilation (TLV), aliquid is used to transport dissolved oxygen and carbondioxide; inhaled liquid brings dissolved oxygen to the lungs,and exhaled liquid carries off carbon dioxide. During TLV,both functional residual capacity and tidal volume are replacedby perfluorocarbon liquid. Technically, TLV is difficult.Clinically, provisions need to be made to mechanically deliverand withdraw liquid from the lung. Equipment is needed foreliminating carbon dioxide from the liquid and for equilibrat-ing it with oxygen. TLV requires new equipment and proce-dures. Moreover, the high viscosity of the perfluorocarbon
27CHAPTER 2 Emerging Technologies for the Management of Respiratory Disorders
Ch02-X2942.qxp 11/22/06 3:22 PM Page 27

28 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Complication Rationale and Treatment
PHYSIOLOGICElectrolyte/glucose/ Sodium requirements decrease to 1 to 2 mEq/kg/day; potassium requirements increase
fluid imbalance to 4 mEq/kg/day secondary to action of aldosteroneCalcium replacement may be required if citrate is a component of prime blood anticoagulantHyperglycemia may occur if citrate-phosphate-dextrose anticoagulated blood is used; reduce
dextrose concentration of maintenance and heparin infusionsMaintain total fluid intake of 100 to 150 ml/kg/dayFluid intake should balance output; furosemide may be required if positive fluid balance occurs
Central nervous system This significant complication of ECMO can be related to pre-ECMO hypoxia, acidosis, deterioration: hypercapnia, or vessel ligationcerebral edema, intracranial Drug of choice for seizures is phenobarbitalhemorrhage, seizures Serial electroencephalograms and cranial ultrasound examinations may be required
Generalized edema Extracellular space is enlarged by distribution of crystalloid solution from the prime fluid and action of aldosterone and antidiuretic hormone
Furosemide or hemofiltration may be indicated if edema causes brain or lung dysfunctionRenal failure Acute tubular necrosis results from pre-ECMO hypotension and hypoxia
Monitor output and indicators of renal failure: blood urea nitrogen, creatinineIncrease renal perfusion by increasing pump flow and use of dopamine (5 mcg/kg/min)Hemodialysis may be added to the circuit if necessary
Bleeding/thrombocytopenia Most frequent cause of deathLarge foreign surface of ECMO circuit lowers platelet function and countMost common in infants requiring surgery or chest tubesMinimize with good control of ACT (180 to 200 seconds) and judicious use of platelets
and frozen plasmaAll surgical procedures must be done with electrocautery
Decreased venous Infant must have adequate circulating volume to obtain adequate flow ratesreturn/hypovolemia Manifested by collapsing silicone bladder triggering bladder box alarm and decrease in
extracorporeal flow rate, arterial pressure, and arterial pulse amplitudeBlood sampling, wound drainage, or peripheral dilatation may account for hypovolemiaCheck for pneumothorax, partial venous catheter occlusion, or malposition, which may
decrease venous drainage and returnReplace volume with packed cells, fresh frozen plasmaTreat pneumothorax with chest tube placementRaise level of bed to enhance gravity drainage of venous blood
Hypervolemia Caused by overinfusion of blood products, which causes a larger percentage of blood to flow through malfunctioning lungs
Can also be caused by renal ischemia and excretion of renin/angiotensinManifested by widening pulse amplitude and decreasing systemic oxygenation at an
extracorporeal flow rateTreat overinfusion by removing blood from the circuit; renal hypertension may dictate use of
captopril or labetalolPatent ductus arteriosus Left-to-right shunting may occur, thus causing increased blood flow to the lungs and
necessitating high pump flows without expected increase in PaO2
Ligation may be indicated because weaning will not be successful
MECHANICALTubing rupture, air in oxygenator Increase ventilator to pre-ECMO parameters; take patient off bypass (repair circuit, aspirate
air, replace malfunctioning oxygenator); be prepared to resuscitate infantPower failure Always plug pump into hospital’s emergency power supply; hand crank until emergency power
is availableDecannulation Apply firm pressure; come off bypass; increase ventilator parameters; repair vessel; replace
blood volume; be prepared to resuscitate infant
From Askin DF, editor (1997). Acute respiratory care of the neonate, ed 2. Santa Rosa, CA: NICU Ink. Adapted from Nugent J (1986).Extracorporeal membrane oxygenation in the neonate. Neonatal network 4(5):33.ACT, Activated coagulation time; ECMO, extracorporeal membrane oxygenation.
Complications of Extracorporeal Membrane OxygenationTABLE 2-6
Ch02-X2942.qxp 11/22/06 3:22 PM Page 28

liquid limits the number of breaths that can be delivered perminute.
Partial Liquid Ventilation (PLV)PLV, also known as perfluorocarbon-associated gas exchange(PAGE), is a hybrid method that attempts to overcome someof the limitations of TLV while retaining the advantages ofliquid ventilation. During PLV, functional residual capacity isreplaced by liquid, but tidal ventilation is conventional, usingoxygen-enriched gas and standard ventilator equipment. Thelung is filled with perfluorocarbon liquid to a volume equiv-alent to the normal pulmonary functional residual capacity.This volume of liquid is left in the lung, and gas ventilation isresumed with use of conventional gas ventilators. On inspi-ration, oxygen is pushed down the airway into the liquid-filledalveoli, where it forms bubbles and where oxygen and carbondioxide are exchanged in the liquid from bubbles to thealveoli. This process oxygenates the alveolar perfluorocarbonreservoir and purges it of carbon dioxide. On exhalation, thegas is expelled from the lung. Breaths can be delivered at afrequency appropriate for the size and needs of the patientbecause the viscosity of the liquid does not limit respiratoryrate. PLV has been shown to be effective in surfactant-deficientpremature lambs. PLV improved oxygenation and carbondioxide elimination as well as lung compliance. It has alsobeen shown to work in two models of ARDS, oleic acid lunginjury, and saline lavage. A small, nonrandomized studytreated 13 preterm infants who failed conventional manage-ment of severe respiratory distress with PLV (Leach et al,1996). In this study when PaO2 and compliance improved, theoxygen index decreased significantly within 1 hour oftreatment. Six term infants with respiratory failure and noimprovement after ECMO were treated with PLV in anotherstudy (Greenspan et al, 1997). The study concluded that PLVappeared to be safe, improved lung function, and recruitedlung volume. However, this therapy remains experimental asrandomized trials have not been performed in neonates.
Collaborative Care: Liquid VentilationThe care of infants with respiratory compromise may be greatlyaffected if future advances prove liquid ventilation to be safeand effective. Because of the complexity of the deliverysystems, a specialized team, similar to an ECMO team, wouldbe required to care for these infants. These specialists will needto be trained in fluid pharmacologic mechanics and liquidbreathing techniques.
PHARMACOLOGIC THERAPIES FORVENTILATED INFANTSSeveral pharmacologic options are available to the clinicianfor the treatment of RDS and prevention of its complications.Selected treatments are reviewed in this section.
A large multicenter randomized controlled trial and othersmaller trials have shown benefits of vitamin A administrationin preterm infants. Vitamin A supplementation given largelyto infants less than 1 kg resulted in a decrease in death and/orBPD at 36 weeks (66% to 60%; RR 0.87; CI 0.83, 0.99; NNT17) and trends for less nosocomial sepsis and retinopathy ofprematurity (Tyson et al, 1999; Darlow & Graham, 2002).Nonetheless, vitamin A supplementation is only used in theminority of the infants less than 1 kg currently in the UnitedStates (Ambalavanan et al, 2003).
Systemic corticosteroids have been used to treat infants withRDS, to selectively treat infants who continue to require respi-ratory support, and to treat those who develop BPD. Mortalityand/or BPD at 36 weeks decreases (from 72% to 45%; RR 0.63;CI 0.51, 0.78; NNT 4) with moderately-early (7 to 14 days)administration of corticosteroids. Early (<96 hours) and delayed(>3 weeks) administration of systemic steroids has also beenassessed with meta-analyses and the results are qualitatively simi-lar. However, there are short-term adverse effects includinghyperglycemia, hypertension, gastrointestinal bleeding, gastro-intestinal perforation, hypertrophic obstructive cardiomy-opathy, poor weight gain, poor growth of the head, and a trendtoward a higher incidence of periventricular leukomalacia(American Academy of Pediatrics/Canadian PaediatricSociety, 2002). Furthermore, data including an increased inci-dence of neurodevelopmental delay and cerebral palsy ininfants randomized to systemic corticosteroids raise seriousconcerns about adverse long-term outcomes. Thus, routine useof systemic corticosteroids is not recommended for the preven-tion or treatment of BPD by the Consensus Group of theAmerican Academy of Pediatrics and the Canadian PaediatricSociety. Administration of inhaled steroids to ventilated pre-term infants during the first 2 weeks after birth reduced theneed for systemic steroids (45% to 35%; RR 0.78; CI 0.62, 0.99;NNT 10) and tended to decrease death and/or BPD at 36 weekswithout an increase in adverse effects (Shah et al, 1999).
Inhaled nitric oxide has been evaluated in preterm infantsfollowing the observation of its effectiveness in term and near-term infants with hypoxemic respiratory failure. Despiteoptimistic results from a large randomized controlled trial(Schreiber et al, 2003), trials in preterm infants report hetero-geneous effects on bronchopulmonary dysplasia, mortality, and other important outcomes (Barrington & Finer, 2001;Schreiber et al, 2003; Van Meurs et al, 2005). The mostcurrent data do not support the routine administration ofinhaled nitric oxide in preterm infants with hypoxemicrespiratory failure, but this is an area of much research.
Prevention of extubation failure has been attempted usingvarious pharmacologic approaches. Methylxanthines appear tohave a large effect on reducing extubation failure (51% to25%; RR 0.47; CI 0.32, 0.70; NNT 4). Similarly, systemicsteroids before extubation reduces need for reintubation (10%to 1%; RR 0.18; CI 0.04; 0.97; NNT 11). In contrast, racemicepinephrine post extubation does not improve pulmonaryfunction or extubation failure (Davies & Davis, 2001).
Other medications that have been evaluated includediuretics, bronchodilators, and antioxidants. Administrationof furosemide to ventilated preterm infants improved pul-monary function (various measures with heterogeneity ofresults) but did not result in important or long-term benefits(Brion et al, 2003). Bronchodilators have been used to treatpreterm infants with evolving or established BPD. Improve-ment in pulmonary mechanics (both resistance and com-pliance) has been reported without effect on long-term orimportant outcomes. Vitamin E or superoxide dismutasetherapy did not reduce BPD.
SU M MARYHypoxemia continues to contribute significantly to bothmorbidity and mortality in NICUs. As our understanding ofthe pathophysiology of neonatal hypoxemia improves, newapproaches to prevention and treatment are suggested. The
29CHAPTER 2 Emerging Technologies for the Management of Respiratory Disorders
Ch02-X2942.qxp 11/22/06 3:22 PM Page 29

development of new therapeutic techniques—such as surfac-tant replacement, ECMO, HFV, NO, and liquid ventilation—holds the promise of improved neonatal outcome. There is apaucity of data regarding long-term outcome with some ofthese newer therapies and whether they hold significantbenefits over older conventional methods. The evaluation anddiscovery of newer and safer methods to prevent and treatneonatal hypoxemia requires the collaborative efforts of basicscientific research and ongoing large, multicenter, randomizedclinical trials.
R E F E R E N C E SAcute Respiratory Distress Syndrome Network (2000). Ventilation with
lower tidal volumes as compared with traditional tidal volumes for acutelung injury and the acute respiratory distress syndrome. New Englandjournal of medicine 342:1301-1308.
Ambalavanan N et al (2003). Vitamin A supplementation in extremely lowbirth weight (ELBW) infants: prevalence and factors inhibiting itswidespread use. Pediatric research 371A:2108.
American Academy of Pediatrics/Canadian Paediatric Society (2002).Postnatal corticosteroids to treat or prevent chronic lung disease inpreterm infants. Pediatrics 109:330-340.
Anonymous (2000). Supplemental therapeutic oxygen for pre-thresholdretinopathy of prematurity (STOP-ROP), Randomized, Controlled Trial.I: Primary outcomes. Pediatrics 105:295-310.
Artigas A et al (1998). The American-European Consensus Conference onRDS, Part 2. Ventilation, pharmacologic, supportive therapy, study designstrategies, and issues related to recovery and remodeling. American journalof respiratory critical care medicine 157:1332-1347.
Askie LM et al (2003). Oxygen-saturation targets and outcomes in extremelypreterm infants. New England journal of medicine 349:959-967.
Avery ME, Mead J (1959). Surface properties in relation to atelectasis andhyaline membrane disease. American journal of diseases of children97:517-523.
Barrington KJ, Finer NN (2001). Inhaled nitric oxide for respiratory failurein preterm infants. Neonatal Collaborative Review Group. NICHDCochrane neonatal reviews. Available at: http://156.40.88.3/cochrane/barrington/barring1.htm.
Barrington KJ, Finer NN (2006). Inhaled nitric oxide for respiratory failure inpreterm infants. Cochrane database of systematic reviews, 2001(4):CD000509.
Bennett CC et al (2001). UK collaborative randomised trial of neonatalextracorporeal membrane oxygenation: follow-up to age 4 years. Lancet357(9262):1094-1096.
Bhuta T, Henderson-Smart DJ (2002). Elective high frequency jetventilation versus conventional ventilation for respiratory distresssyndrome in preterm infants. NICHD Cochrane neonatal reviews. Availableat: www.cochrane.org/reviews/en/ab000104.html.
30 UNIT I SYSTEMS ASSESSMENT AND MANAGEMENT OF DISORDERS
Case Study
IDENTIFICATION OF THE PROBLEMA female infant was born after an elective repeat cesareansection. The amniotic fluid was clear. The infant developedrespiratory distress in the first hours after birth while in thenewborn nursery. She was placed on a radiant warmer forobservation, and pulse oximetry revealed a saturation of90% while breathing room air.
ASSESSMENT: HISTORY AND PHYSICALEXAMINATIONThe infant was born after elective repeat cesarean section,but decreased beat-to-beat variability of the fetal heart ratehad been noted for the first time during routine monitoringjust before the cesarean section. The pregnancy had beenuncomplicated. Amniotic fluid was clear. Apgar scores were7 and 8 at 1 and 5 minutes, respectively. There was nohistory of infection or other complications during preg-nancy. At half an hour after birth, the infant was taken fromthe mother to the normal newborn nursery for routine care.During the subsequent hours she was noted to haveoccasional grunting and retractions.
DIFFERENTIAL DIAGNOSISThe differential diagnosis for a term infant with mildrespiratory distress in the first hours after birth by cesareansection include transient tachypnea of the newborn, hypo-thermia, hypoglycemia, and other less common conditions.
DIAGNOSTIC TESTSThe initial arterial blood gas values were as follows: pH7.35, PCO2 48, PO2 43, bicarbonate 27. The blood sugarwas 29 mg/dL. The infant was given 100% oxygen, andoxygen saturations remained around 90%. A chestradiograph, blood culture and CBC, and serial blood gases
were obtained. Because of persistent low saturations, theinfant was intubated.
WORKING DIAGNOSISThe preductal and postductal oxygen saturations persistedaround 90% despite 100% oxygen and endotrachealintubation. The chest radiograph showed clear lungs withdecreased perfusion. The blood pressures were normal. TheCBC and white blood cell count were normal.
DEVELOPMENT OF MANAGEMENT PLANNitric oxide was initiated because of a suspicion ofpulmonary hypertension. Because of persistent lowsaturations, congenital cyanotic heart disease was alsosuspected. An echocardiogram was obtained to assist in thediagnosis. A prostaglandin E drip was initiated while theechocardiogram was obtained. The echocardiogram con-firmed the diagnosis of interrupted aortic arch. No evidenceof pulmonary hypertension was seen, but moderate-to-severe obstruction to left cardiac output was observed. Thenitric oxide was discontinued. The infant was continued onprostaglandin E1 until surgical repair was performed. Theserum calcium level was 7.5 mg/dl.
IMPLEMENTATION AND EVALUATION OFEFFECTIVENESSThe infant was continued on a prostaglandin E1intravenous infusion. Because of the association ofinterrupted aortic arch and other outcome obstructionlesions with DiGeorge syndrome, the DiGeorge probe wasobtained, which confirmed this diagnosis. The infant hadintractable hypocalcemia treated with high doses ofcalcium. In addition, she had a decreased T cell count.Surgical repair of the interrupted aortic arch was successful.
Ch02-X2942.qxp 11/22/06 3:22 PM Page 30

Brion LP et al (2003). Diuretics acting on the distal renal tubule for preterminfants with (or developing) chronic lung disease. Neonatal CollaborativeReview Group. NICHD Cochrane neonatal reviews. http://156.40.88.3/cochrane/brion5/brion.htm.
Carlo WA, Ambalavanan N (1999). Conventional mechanical ventilation:traditional and new strategies. Pediatrics in review 20:e117-e126.
Carlo WA et al (2002). Minimal ventilation to prevent bronchopulmonarydysplasia in extremely-low birth-weight infants. Journal of pediatrics141:370-374.
Carnielli VP et al (1998). Iron supplementation enhances response to highdoses of recombinant human erythropoietin in preterm infants. Archives ofdisease in childhood: fetal and neonatal edition 79(1):F4448.
Cifuentes J (1996). Does surfactant administration reduce the incidence ofbronchopulmonary dysplasia (BPD)? Pediatric research 39:1192.
Clark RH et al (2000). Low-dose nitric oxide therapy for persistentpulmonary hypertension of the newborn. Clinical inhaled nitric oxideresearch group. New England journal of medicine 342(7):469-474.
Clark RH et al (2001). Lung injury in neonates: causes, strategies forprevention, and long-term consequences. Journal of pediatrics 139:478-486.
Darlow BA, Graham PJ (2002). Vitamin A supplementation for preventingmorbidity and mortality in very low birth weight infants. NeonatalCollaborative Review Group. NICHD Cochrane neonatal reviews.http://156.40.88.3/cochrane/Darlow/Darlow.htm.
Davies MW, Davis PG (2001). Nebulized racemic epinephrine for extubationof newborn infants. Neonatal Collaborative Review Group. NICHDCochrane neonatal reviews. Available at: http://156.40.88.3/cochrane/Davies/Davies.htm.
Field D et al (2005). Neonatal ventilation with inhaled nitric oxide versusventilatory support without inhaled nitric oxide for preterm infants withsevere respiratory failure: the INNOVO multicentre randomisedcontrolled trial (ISRCTN 17821339). Pediatrics 115(4):926-936.
Finer NN (2000). Inhaled nitric oxide in term and near-term infants:neurodevelopmental follow-up of the neonatal inhaled nitric oxide studygroup (NINOS). Journal of pediatrics 136(5):611-617.
Finer NN, Barrington KJ (2001). Nitric oxide for respiratory failure in infantsborn at or near term. Cochrane database of systematic reviews, Issue 2.
Finer et al (2005). NICHD Neonatal Network. Delivery room continuouspositive airway pressure/positive end-expiratory pressure in extremely lowbirth weight infants: a feasibility trial. Pediatrics 115:197-198.
Greenough A et al (2000). Synchronized mechanical ventilation forrespiratory support in newborn infants. Cochrane database of systematicreviews, Issue 4.
Greenspan JS et al (1997). Pulmonary sequelae in infants treated withextracorporeal membrane oxygenation. Pediatric pulmonology 23(1):31-38.
Hansen TN (1998). Contemporary diagnosis and management of neonatalrespiratory disease, ed 2. Newton, PA: Handbooks in Health Care.
Hargett KD (1995). Mechanical ventilation of the neonate. In Barnhart SL,Czervinske MP, editors. Perinatal and pediatric respiratory care. Philadelphia:Saunders.
Henderson-Smart DJ et al (2003). Elective high frequency oscillatoryventilation versus conventional ventilation for acute pulmonarydysfunction in premature infants. Cochrane database of systematic reviews2003(3):CD000104.
HiFO Study Group (1993). Randomized study of high-frequency oscillatoryventilation in infants with severe respiratory distress syndrome. Journal ofpediatrics 122:609-619.
Hudak ML et al (1996). A multicenter randomized, masked comparison trialof natural versus synthetic surfactant for the treatment of respiratorydistress syndrome. Journal of pediatrics 128(3):396-406.
Keszler M et al (1991). Multicenter controlled trial comparing high-frequencyjet ventilation and conventional mechanical ventilation in newborn infantswith pulmonary interstitial emphysema. Journal of pediatrics 119:85-93.
Kinsella JP, Abman SH (1995). Recent developments in the pathophysiologyand treatment of persistent pulmonary hypertension of the newborn.Journal of pediatrics 126(6):853-863.
Leach CL et al (1996). Partial liquid ventilation with perflubron inpremature infants with severe respiratory distress syndrome. The liquiventstudy group. New England journal of medicine 335(11):761-767.
Mariani G, Cifuentes J, Carlo WA (1999). Randomized trial of permissivehypercapnia in preterm infants. Pediatrics 104:1082-1088.
Pattle RE (1958). Properties, function and origin of alveolar lining layer.Proceedings of the Royal Society of London B148:217-240.
Roberts JD et al (1992). Inhaled nitric oxide in persistent pulmonaryhypertension of the newborn. Lancet 340(8823):818-819.
Sandri F et al (2004). Prophylactic nasal continuous positive airway pressure in newborns 28-31 weeks gestation: multicenter randomizedcontrolled trial. Archives of disease in childhood: fetal and neonatal edition89:F394-F398.
Schreiber MD et al (2003). Inhaled nitric oxide in preterm infants withrespiratory distress syndrome. New England journal of medicine349(22):2099-2107.
Shaffer TH et al (1999). Liquid ventilation: current status. Pediatrics in review20e:134-142.
Shah V et al (1999). Early administration of inhaled corticosteroids forpreventing chronic lung disease in ventilated very low birth weightpreterm neonates. Neonatal Collaborative Review Group. NICHDCochrane neonatal reviews. Available at: http://156.40.88.3/cochrane/shah2/shah.htm.
Soll RF (1998a). Synthetic surfactant treatment for preterm infants withrespiratory distress syndrome. Neonatal Collaborative Review Group.NICHD Cochrane neonatal reviews. Available at: http://156.40.88.3/cochrane/SOLL8/SOLL.htm.
Soll RF (1998b). Prophylactic synthetic surfactant in preterm infants.Neonatal Collaborative Review Group. NICHD Cochrane neonatal reviews.Available at: http://156.40.88.3/cochrane/SOLL5/SOLL.htm.
Soll RF (1999). Multiple versus single dose natural surfactant extract forsevere neonatal respiratory distress syndrome. Neonatal CollaborativeReview Group. NICHD Cochrane neonatal reviews. Available at:http://156.40.88.3/cochrane/SOLL/SOLL.htm.
Soll RF (2000). Natural surfactant extract versus synthetic surfactant forneonatal respiratory distress syndrome. Cochrane database of systematicreviews, Issue 4.
Soll RF, Blanco F (2001). Natural surfactant extract versus syntheticsurfactant for neonatal respiratory distress syndrome. NeonatalCollaborative Review Group. NICHD Cochrane neonatal reviews.Available at: http://156.40.88.3/cochrane/SOLL2/SOLL.htm.
Soll RF, Morley CJ (2001). Prophylactic versus selective use of surfactant inpreventing morbidity and mortality in preterm infants. NeonatalCollaborative Review Group. NICHD Cochrane neonatal reviews.Available at: http://156.40.88.3/cochrane/SOLL4/SOLL.htm.
The STOP-ROP Multicenter Study Group (2000). Supplementaltherapeutic oxygen for prethreshold retinopathy of prematurity (STOP-ROP): a randomized, controlled trial. I: Primary outcomes. Pediatrics105:295-310.
Thome UH, Carlo WA (2003). High-frequency ventilation: when is itbeneficial? Neonatal respiratory diseases 13:1-11.
Thome UH et al (2005). Ventilation strategies and outcome in randomizedtrials of high frequency ventilation. Archives of disease in childhood: fetaland neonatal edition 90(6):F466-F473.
Thomson MA on behalf of the IFDAS study group (2002). Early nasalcontinuous positive airways pressure (nCPAP) with prophylacticsurfactant for neonates at risk of RDS. The IFDAS multi-centrerandomized trial. Pediatric research 379A:2204.
Tyson JE et al (1999). Vitamin A supplementation for extremely-low-birth-weight infants. NICHD Neonatal Research Network. New England journalof medicine 340:1962-1968.
UK Collaborative Trial Group (1996). UK collaborative randomized trial ofneonatal extracorporeal membrane oxygenation. Lancet 348:75-82.
Van Meurs KP et al (2005). Inhaled nitric oxide for premature infants withsevere respiratory failure. New England journal of medicine 353(1):13-22.
Verder H et al (1994). Surfactant therapy and nasal continuous positiveairway pressure for newborns with respiratory distress syndrome. Danish-Swedish Multicenter Study Group. New England journal of medicine331:1051-1055.
Verder H et al (1999). Nasal continuous positive airway pressure and earlysurfactant therapy for respiratory distress syndrome in newborns of lessthan 30 weeks’ gestation. Pediatrics 103:E25.
Yost CC, Soll RF (1999). Early versus delayed selective surfactant treatmentfor neonatal respiratory distress syndrome. Neonatal Collaborative ReviewGroup. NICHD Cochrane neonatal reviews. Available at: http://156.40.88.3/cochrane/YOST/YOST.htm.
31CHAPTER 2 Emerging Technologies for the Management of Respiratory Disorders
Ch02-X2942.qxp 11/22/06 3:22 PM Page 31