Embed Size (px)
Citation preview

Respiratory insufficiency in bariatric patients
Special considerations or just
more of the same? Weaning and rehabilation conference 6th November 2015

Definition of obesity
Underweight BMI< 18
Normal weight BMI 18-25
Overweight BMI > 25
Obesity BMI > 30
Morbid obesity BMI > 40 or comorbidities

Perspective
Globally 1,9 billion are overweight (BMI>25)
600 mio are obese (BMI>30)
Compared to 800 mio starving
20-30% of ICU patients have a BMI > 30
WHO 2015
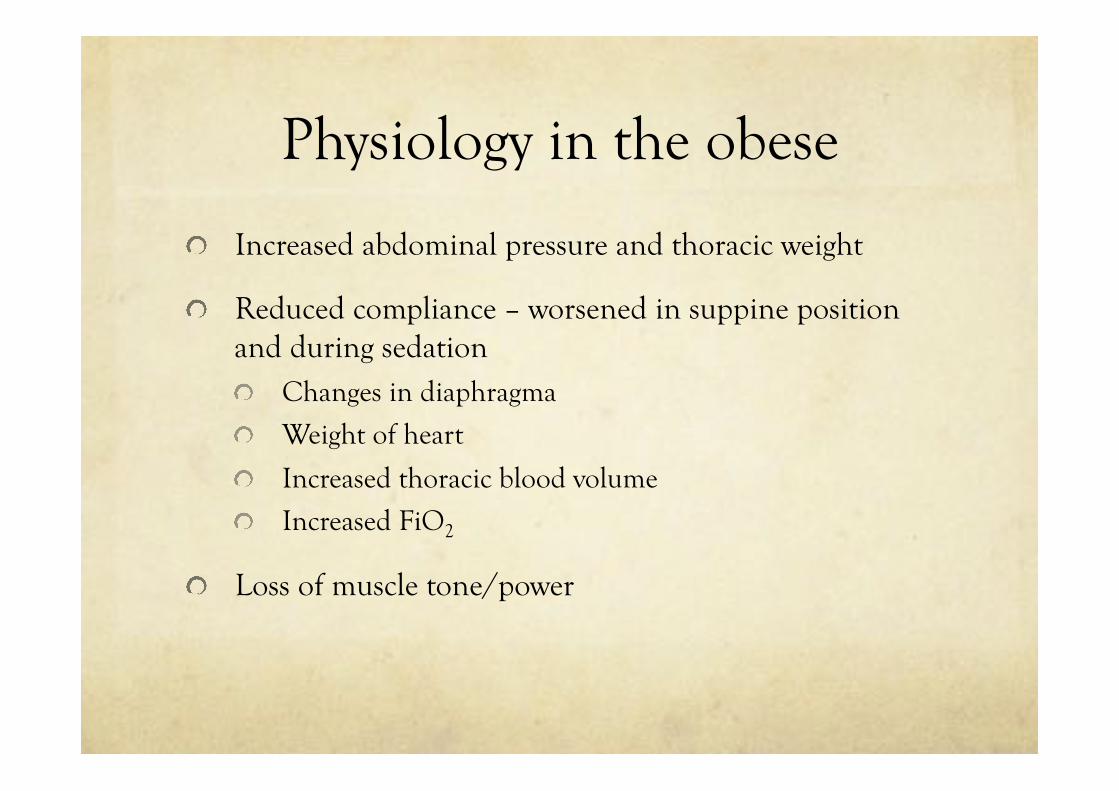
Physiology in the obese
Increased abdominal pressure and thoracic weight
Reduced compliance – worsened in suppine position and during sedation Changes in diaphragma
Weight of heart
Increased thoracic blood volume
Increased FiO2
Loss of muscle tone/power


Physiology in the obese
Reduction in end expiratory lung volumes
Reduction in functional residual volume – FRC: – 2 liters at BMI 25; 1 liter at BMI 35
Reduction of EELV below closing capacity causes collapse of bronchioli
Atelectasis – impaired gas exchange, ie shunt and hypoxemia
Compliance reduced: - 75 cmH2O at BMI 25; 50 at BMI 35

Complications to mechanical ventilation
Expiratory flow limitation: airway collapse (PEEPi)
Prolonged expiration
Increased incidence of asthma and bronchospasm
VILI – ventilator induced lung injury caused by repetetive opening and closing of og collapsed alveoli

Complications to anesthesia – not ICU
Postoperative complications 5 % in Morbidly obese are not increased (except 1 study)
When Intubation is needed postoperatively, increased risk of ARDS (not mortality)

Ventilator strategy
No evidence for particular ventilator mode
KEEP THE LUNG OPEN
Lowest FiO2 to mantain physiologic oxygenation
PEEP (10-15) after RM (up to 55-60 cmH2O 6-8 secs)
Sighs
Vt? IBW 6-8 ml/kg The lung does not grow with increased Body Mass

Date of download: 10/25/2015 Copyright © 2015 American Society of Anesthesiologists. All rights reserved.
Fig. 3. Representative computerized tomography (CT). A CT scan 1 cm above the diaphragm in the three different groups at all four time points. Note the sustained effect of RM + PEEP and the transient effect of RM + ZEEP. PEEP = positive end-expiratory pressure; RM = recruitment maneuver; ZEEP = zero end-expiratory pressure.
Figure Legend:
From: Prevention of Atelectasis in Morbidly Obese Patients during General Anesthesia and Paralysis:A Computerized Tomography Study Anesthesiology. 2009;111(5):979-987. doi:10.1097/ALN.0b013e3181b87edb

To PEEP or not to PEEP

Beware of hyperinflation
Zimbabwe 2008

Co morbidities
Obesity is correlated to a wide range of other diseases
Anxiety – depression
Ischemic heart disease, hypertension
COPD
Diabetes mellitus
Chronic inflammatory state
Increased risk of acute kidney injury – oedema
Special considerations
Obesity hypoventilation Syndrome – OHS PaCO2> 5,9 kPa (45
mmHg) + BMI > 30
Exclusion of other reasons for hypercapnia
Malignant OHS • When BMI > 40
Obesity supine death syndrome


Prepare for extubation
Minimal sedation
Protocolized sedation and weaning
Prevent neuromuscular weakness because of prolonged ventilation
Treat prolonged expiration to avoid increased WOB and fatigue
Optimize fluid status

Positioning
Position in sitting or half-sitting
Obesity supine death syndrome
McKenzie Anesth Analg 1980 Jan;59(1):81

Postextubation
NIV could reduce respiratory insufficiency in terms of reduced LOS in ICU and hospital. Mortality reduction in patients with hypercapnia
El Sohl; Eur Respir J 2006; 28.588-595
Common reintubation – what rate is acceptable
Outcomes
Overweight is not related to increased mortality but
Longer length of stay (LOS) 1,5 day and
Ventilator 1 day
Low BMI increases mortality!
Moderately overweight (BMI 30-40) might have a lower mortality RR 0,86 (CI 0,81-0,91; p < 0,001)
Akkinusi et al CCM 2008. Metaanalysis


Special considerations
Prevent or treat overt pain and anxiety
A priori higher PEEP. Allow for longer expiration
Prepare before mobilization and exercise Optimize blood pressure and cardiac output. Increase oxygen supply and ventilation if needed. Treat bronchospasm as needed.
Evaluate thoroughly before weaning and extubation
Consider NIV for postextubation profylaxis Especially with hypercapnia or for exercise

Key Points
Generally same challenges in obese patients as those with normal weight.
The obese patient with respiratory insufficiency has an increased risk of a more difficult weaning from the ventilator and thus longer time on mechanical ventilation
We need to take precautions in order to avoid further complications. These are the same measures as in any other patient with difficult weaning
Though a longer stay in the ICU the bariatric patient does not have an excess mortality (overweight might even be protective).

Thank you