Embed Size (px)
Citation preview

Respecting Diversity: Religious and Spiritual
Beliefs of the Older Person
Vicki Murdock, MSW, PhDUniversity of Wyoming

This module was developed for and peer reviewed by the South Carolina Geriatric Education Center.

Module Learning Objectives
1. Define religion and spirituality from a diversity perspective.
2. Identify theory, research, and policy that supports addressing client/patient spirituality.
3. Recognize particular spiritual issues of late life.
4. Recognize the importance of worker self-awareness and the challenges of addressing client/patient spirituality.
5. Describe various methods that can help address the older client/patient’s spirituality.

“The great error of our day is that physicians separate the soul and body, when they treat the body.”
Plato (427-347 BCE)

Spirituality
Spirituality “relates to the person’s search for meaning and morally fulfilling relationships between oneself, other people, the encompassing universe, and the ground of existence, whether a person understands this in terms that are theistic, atheistic, non-theistic, or any combination of these”1

Religion
Religion “involves the patterning of spiritual beliefs and practices into social institutions, with community support and traditions maintained over time”1

One Model of the Whole Person, Suggesting the Importance of
Body, Mind, and SoulOutside Environment
Biological Psychological
Spiritual
2
Inner Person

Theories of Aging that Include Spirituality3
• Continuity theory
• Social constructionism and phenomenology
• Symbolic interactionism

Theories of Aging that Include Spirituality3
• Erikson’s generativity stage
• Crisis/grief/loss theories
• Social exchange theory

Theories of Moral and Faith Development that Include Aging3
• Erikson’s stage/developmental theory
• Fowler’s stages of faith
• Kohlberg’s moral development theory
• Maslow’s hierarchy

Theories of Moral and Faith Development that Include Aging3
• Krill, Jung, and Assagioli’s work
• Wilber’s transpersonal theory
• Gilligan’s women’s moral development
• Tornstam’s gerotranscendence4

Spirituality/Religiosity and Physical and Mental Health
Over 750 empirical studies validate the benefits of spirituality/religion on health and
mental health outcomes.5

Spirituality/Religiosity and Physical and Mental Health
Client spirituality correlates with:• Reductions in mortality, anxiety,
depression, suicidal ideation, substance abuse, hypertension
• Increases in life satisfaction, well-being, immune function

Cultural Competence Continuum Applied to Spirituality6
6.Spiritual proficiency: builds community diversity awareness
5.Spiritual competence: acceptance and respect for spiritual diversity
4.Spiritual pre-competence: aware of problem
3.Spiritual blindness: all people are the same
2.Spiritual incapacity: unintentional sense of superiority of dominant group
1.Spiritual destructiveness: intentional destruction

Professional Organizations that Mandate Respect for Religious Diversity
• American Medical Association
• American Psychiatric Association
• American Psychological Association
• American Nursing Association
• JCAHO
• National Association of Social Workers
• American Counseling Association
• American Association of Pastoral Counselors
• American Association of Professional Chaplains
• COA, NAADAC

All Major Healthcare/Helping Professions in the U.S. Mandate Respect for the
Religious/Spiritual Diversity of our Patients/Clients.

Respectful Practice Behaviors
• To ask about client/patient spiritual beliefs and practices
• To make a referral to their religious group of choice• To listen to their beliefs in order to provide “best care”
to the client/patient• To honor your own beliefs, but without any need to
share/convert/convince others• For staff to receive training on this topic in order to be
respectful toward clients/patients

Behaviors that are Not Respectful
• To ignore, neglect, or fail to ask about the religious or spiritual beliefs of your patients/clients
• To fail to connect them to the social support of their religious/spiritual group and leaders
• For written or unwritten agency policy to prevent trained staff from addressing client/patient spirituality
• To share your beliefs with clients/patients from any conversion motives

Research Findings on Addressing Spirituality with Clients/Patients
• Clients want professionals to ask them about their beliefs.7
• Clients/patients “respond best” to inquiries by the healthcare professional.8
• 83% of 921 patients in outpatient settings reported that they wanted their healthcare professional to ask them about their spiritual beliefs.9
• 91% of these 921 patients reported that they had never been asked by their healthcare professional about their spiritual beliefs.9

Research Findings on Spirituality and Older Adults
• 76% of persons 65+ regard religion as highly important in their lives.10
• Of 4,000 older persons, the “religiously active” were half as likely to be depressed, regardless of age, gender, race, social support or disability.11
• Coping through faith predicted positive outcomes in a study of 586 persons.12
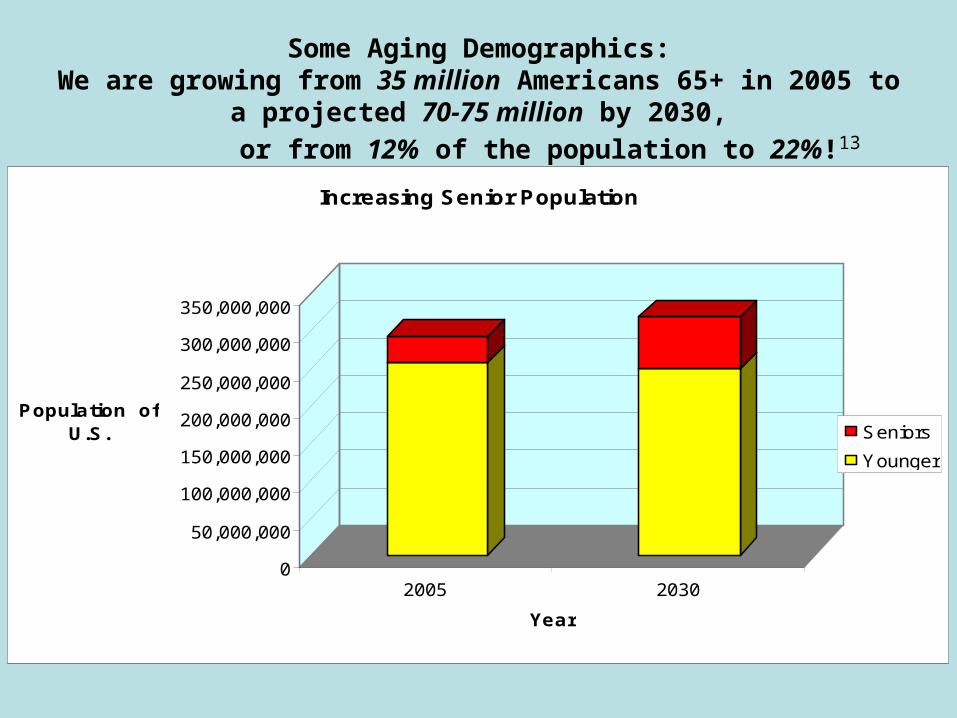
Some Aging Demographics:We are growing from 35 million Americans 65+ in 2005 to
a projected 70-75 million by 2030,
or from 12% of the population to 22%!13
0
50,000,000
100,000,000
150,000,000
200,000,000
250,000,000
300,000,000
350,000,000
Population of U.S.
2005 2030
Year
Increasing Senior Population
Seniors
Younger

American Generational Differences
We can expect some cross-generational issues in our work…
Current old cohort grew up in the early 20th century
Baby boomers grew up in the 1945-1965 era
Gen X and Y grew up in 1970-1990
What different worlds these generations
have experienced!

Spirituality and the Lifespan
• Some studies find religiosity a constant across the individual lifespan.14
• Some studies indicate people may become more religious with age.14,15
• As outward signs of religiosity decline, non-organizational religious activities may increase (private prayer, meditation).16

The Uniqueness of Being Old• Ability to look back across a life span
and integrate parts into a whole
• Ability to engage in inner or integrative activity that crosses the life span, despite limitations
• Ability learned over a lifetime to face loss and change

Imminent Psycho-Spiritual Needs
of Older Persons• Need for a sense of the wholeness of life (integration)
• Need for a sense of purpose in “being,” especially when “doing” is more difficult
• Need to acknowledge positive and negative life and spiritual events
• Need to confront, accept, and plan

Why Discuss Spiritual Beliefs with an Older Person?
• Explores a person’s journey, similar to a life review
• Explores often neglected spiritual aspects of life
• Explores late life and end-of-life issues

Why discuss…?
• Ensures a more thorough, holistic assessment
• Responds to emerging professional mandates on spirituality
• Clients/patients want professionals to ask them about their beliefs7,9

…more reasons to discuss
• Affirms the person’s past, present, and future
• Identifies person’s beliefs and values
• May open a dialogue on topics never addressed before
• Creates a “spiritual baseline” for interventions

And more reasons…
• Gives context to losses
• Emphasizes an aspect of life over which personal control is possible
• May point to individual, group, and community programming of private and shared faith activity

Barriers
Two major areas that hold us back from spiritually competent care are:
Worker Competence
and
Societal Taboos about Spirituality

Worker Competence Issues in Addressing Patient/Client Spirituality
• Self awareness
• Cultural/spiritual competence
• Professional and personal boundaries
• Little training in school or post-graduate

Worker Self Awareness
Three activities to help you think about aging and spirituality in your own life:
•Worker Self Awareness -Longevity Quiz
•Loss Awareness
•Spiritual Groups Awareness

Cultural/Spiritual Competence• Willingness to learn about other beliefs
• Willingness to promote organizational and community respect for diverse beliefs
• Willingness to learn from our clients, rather than think of ourselves as the “expert”
• Willingness to suspend our own personal beliefs in order to hear the client's story
• Willingness to recognize diversity and not ignore it

Professional and Personal Boundaries
Professionally:We are mandated to be respectful of religious or spiritual diversity.
We follow an ethical code or professional mission that respects human rights.
Personally:We may believe that we follow the “one true way.”
We may hold biases against people who represent, or behave in ways that we believe are “evil.”

Educational Preparation on Spiritual Issues
• Many disciplines have surveyed their workers to find that little or no time during their schooling was spent on issues that involved religion or spirituality.8,17,18
• Workers in many healthcare disciplines report continuing uncertainty about whether they should discuss spiritual issues with their clients.8,17, 18

Societal Taboos about Addressing Patient/Client
Spirituality
• Antithetical to “science”
• Too personal
• Measurability concerns
• Misunderstood legal concept of “separation of church and state”

Antithetical to Science• Spirituality is “designed to be imprecise.”19
• Spirituality addresses the mysterious or “holy;” science studies objects, behaviors, measurements.
• Religion and science have been placed on opposing sides in debates across the centuries (e.g., placement of the earth, evolution).
• Science depends on objective observation; spirituality is a subjective experience of the human mind/body/soul.

Too Personal to Discuss
• Like sex and politics, American society has proclaimed that we do not discuss religion.
• Spirituality and religion can only be measured by self-report and observable behaviors.
• Many people, including professionals, are uncomfortable with ideas that are unfamiliar, or that challenge what they believe.

Measurability Concerns
• Outward behaviors that can be counted may not provide an accurate measure of beliefs.
• Self-report may be limited by subjectivity or bias because of a desire to please the researcher.
• Language used to describe spiritual beliefs may be misunderstood, even with definitions, due to abstractness of concepts.
• Results are seldom generalizable due to the diversity of spiritual beliefs.
• Researcher bias, scale bias, methodological bias distort the results.20

Clarifying the Commonly Used Phrase “Separation of Church and
State”The 1st Amendment states, in its entirety: “Congress shall make no law respecting an establishment of religion or prohibiting the free exercise thereof.”21
Which means only that:
•There will be no “official” religion of the U.S.
•Each individual is free to worship as they choose.

Church and State…•Constitutional scholars continue to debate the intent of the First Amendment.
•Respectful treatment of a client/patient’s spirituality is not hindered by the First Amendment. 21
•Simply, respectfully, ask the client/patient to tell us their story.

Challenges in Addressing Spirituality in Late Life
• Increasing cultural diversity, including religious and spiritual diversity in the United States13
• Helping professions offer little preparation in spiritual care8,17,18
• Ethical issues of autonomy, rights, and privacy

More challenges…
• Being able to hear client/patient stories of negative experiences with religion or spirituality
• Agencies serving the aging population acknowledge offering little spiritual intervention to patients
• Continuing societal fears about mortality, beliefs about after-life, the dying process, facing painful past memories

Methods for Exploring Spirituality with Older Adults
Begin with questions about their childhood, rather than current beliefs (less personal and abstract; practices in childhood were not a choice).
Consider the cognitive functioning level of the adult(s) when planning an activity.
Think big: big paper, big diagrams, big markers
Use sensory-based spiritual activity to reach people with cognitive impairments.

Tools for Exploring Spirituality with an Older Adult
Develop diagrams with a group or individual, such as:
• timelines
• ecomaps
• genograms
• symbolic shapes that have meaning for the person

More Tools…
Use an interview format with an individual or with a group:
• Suggest oral or written responses
• Ask semi-structured or open-ended questions
• Ask a group just one question for that session, or move through many
questions
More Tools…
Use prepared scales/tools with an individual or a group:•Written instruments
•closed- or open-ended questions;
•Questions that call for scaled response (e.g., agree/disagree);
•Autobiographical narrative written on their own or with guidance

Another Tool: Ethical Wills22
• Ethical wills are a written account of a person’s:– Values– Beliefs – Life lessons– Hopes for the future– Understanding of Love– Understanding of Forgiveness

Sensory-based Spiritual Interventions for Persons with Dementia
• Recognize that sensory interventions may or may not be welcomed by the patient.
• Use audio and video recordings of songs and services that are part of the client/patient’s spiritual tradition.
• Invite the appropriate spiritual leader to offer prayers, burn incense, wear traditional robes, sing traditional songs, offer symbolic foods.
Sensory-based Spiritual Interventions for Persons with Dementia
• Encourage family or friends to bring traditional foods tied to spiritual traditions.
• In a group environment, explain activity to other patients so they may choose to stay or leave the area.

BirthEnd of Life
Significant Life orSpiritual Events
Timeline of a Spiritual Journey 23
After Life

Father’s Spiritual Tradition
Mother’s Spiritual Tradition
Faith Community
Individual or Family
God orTranscendence
Spiritual Ecomap24
Rituals
Supernatural Beings
SpiritualLeader

Adjectives describing the spiritual life
Things that anchor you in your beliefs
Visible responses to the spiritual life
+Goals
-Barriers
The Cherry Tree: A Personal Model of Spiritual Growth25

A Unifying Community Model of Meaning-Making26
Diverse Spiritual Behaviors-both positive and negative
Universal search for meaning of life
Hidden biases
Religions, individual beliefs, philosophies, cultures, myths, evolving groups

ConclusionHealthcare professionals are now mandated to
address the patient’s spiritual beliefs, regardless of the worker’s personal views or fears. Our patients want us to ask them about this dimension of their life. Failing to ask about this dimension is not respectful care.
It is incumbent upon each of us to work toward cultural proficiency by encouraging our workplace and our community to embrace the growing pluralism of the United States, and to work for dialogue about spiritual diversity.

References1. Canda E.R. (1997) Spirituality. In Encyclopedia of social work (19th ed.), 1997
supplement. Washington, D.C.: NASW Press.
2. Hutchison E.D. (1999). Dimensions of human behavior: Person and environment. Thousand Oaks, CA: Pine Forge Press.
3. Robbins, S. P., Chatterjee, P., Canda, E. R. (1998). Contemporary human behavior theory: A critical perspective for social work. Boston: Allyn & Bacon.
4. Tornstam, L. (1999). Gerotranscendence and the functions of reminiscence. Journal of Aging and Identity, 4(3), 155-166.
5. King, D.E. (2000). Faith, spirituality, and medicine: Toward the making of the healing practitioner. New York: Haworth Press, Inc.
6. Cross, T. L., Bazron, B. J., Dennis, K. W., Isaacs, M. R. (1989). Toward a culturally competent system of care. Washington, D.C.: Georgetown University Child Development Center.
7. Oyama, O., & Koenig, H.G. (1998). Religious beliefs and practices in family medicine. Archives of Family Medicine, 7, 431-435.
8. Maugans, T. A. & Wadland, W. C. (1991). Religion and family medicine: A survey of physicians and patients. The Journal of Family Practice, 32(2), 210-213.
References (Continued)9. McCord, G., Gilchrist, V.J., Grossman, S.D., King, B.D., McCormick, K.F., Oprandi,
A.M., Schrop, S.L., Selius, B.A., Smucker, W.D., Weldy, D.L., Amorn, M., Carter, M., Deak, A.J., Hefzy, H., & Srivastava, M. (2004). Discussing spirituality with patients: A rational and ethical approach. Annals of Family Medicine, 2, 356-361.
10. Princeton Religious Research Center. (1994). Importance of religion. PRRC Emerging Trends, 16(4).
11. Koenig, H. G. (1997). Is religion good for your health? The effects of religion on physical and mental health. Binghamton, NY: The Haworth Press.
12. Pargament, K. I., Ensing, D. S., Falgout, K., Olsen, H., Reilly, B., Van Haitsma, K., & Warren, R. (1990). God help me: Religious coping efforts as predictors of the outcomes of significant negative life events. American Journal of Community Psychology, 18, 793-824.
13. United States Bureau of the Census (2004). Retrieved from www.agingstats.gov
14. Futterman, A. & Koenig, H. (1996). Measuring religiosity in later life: What can gerontology learn from the psychology and sociology of religion? In Methodological approaches to the study of religion, health, and aging. Washington, D.C.: Department of Health and Human Services, Public Health Service, National Institutes of Health, National Institute on Aging

References (Continued)15. Schultz-Hipp, P.L. (2001). Do spirituality and religiosity increase with age? In D.O.
Moberg, Aging and spirituality: Spiritual dimensions of aging theory, research, practice, and policy (pp. 85-98).
• Koenig, H. G. (2001). Handbook of religion and health. New York: Oxford University Press.
• Shafranske, E. P. & Malony, H. N. (1990). Clinical psychologists’ religious and spiritual orientations and their practice of psychotherapy. Psychotherapy, 27(1), 72-78.
• Sheridan, M. J., Bullis, R. K., Adcock, C. R., Berlin, S. D., & Miller, P. C. (1992). Practitioners’ personal and professional attitudes and behaviors toward religion and spirituality: Issues for education and practice. Journal of Social Work Education, 28(2), 190-203.
• Marty, M. (1980). Social service: Godly and godless. Social Service Review, 54(4), 463-481.
• Moberg, D. O. (2001). Aging and spirituality: Spiritual dimensions of aging theory, research, practice, and policy. New York: Haworth Press.

References (Continued)21. Findlaw.com (2005). The First Amendment. Retrieved August 6, 2005 from
http://caselaw.lp.findlaw.com/data/constitution/amendment01/
22. Baines, B. K. (2002). Ethical wills: Putting your values down on paper. Cambridge, MA: Perseus Publishing.
23. Bullis, R. K. (1996). Spirituality in social work practice. Washington, D.C.: Taylor & Francis Publishing.
• Hodge, D. R. (2000). Spiritual ecomaps: A new diagrammatic tool for assessing marital and family spirituality. Journal of Marital and Family Therapy, 26(2), 217-228.
• Cherry (1996). The Cherry tree. In R. K. Bullis, Spirituality in social work practice. Washington, D.C.: Taylor & Francis Publishing.
• Murdock, V., Leedy, G., & Grubbs, L. (2005). A unifying model of meaning making. Paper presented at the Annual Program Meeting of the Council on Social Work Education, New York City, NY, 2005.
• Barker, R. L. (1999). The Social Work Dictionary (4th ed.). Washington, D.C.: National Association of Social Workers Press.
• Lum, D. (Ed.). (2003). Culturally competent practice: A framework for understanding diverse groups and justice issues (2nd ed.). Pacific Grove, CA: Thomson/Brooks/Cole.

BIOGRAPHY
Vicki Murdock is an Assistant Professor of Social Work at the University of Wyoming. Vicki’s research interests include gerontology, spirituality, and social work field education. Currently, research involves the aging of “Boomers,” loss issues for adult siblings whose family lost an infant at birth, and educational/curricular progress on aging.