Embed Size (px)
Citation preview

European Journal of Orthodontics 4 (1982) 11-19© 1982 European Orthodontic Society
0141-5387/82/00070011S02.00
Residual extraction sites after orthodontictreatmentPart 1. At debanding
Bjorn Oftedal and Johan WisthDepartment of Orthodontics, University of Bergen, Norway.
Summary. The extraction sites of 90 patients with Angle's Class I, Angle's Class II, Div. 1 orAngle's Class II, Div. 2 malocclusions treated with fully banded appliances were examined atthe time of debanding. The frequency of incomplete closure of extraction spaces was relativelyhigh in all types of malocclusion but was highest in the maxilla in Class II, Div. 1 cases where83% showed spaces greater than 0.5 mm.
A multiple regression analysis including age at the start of treatment, type of malocclusion,space conditions in the buccal segments, treatment duration and alveolar atrophy accountedfor 33% of the variation in the spaces in the maxilla. In the mandible, 46% of the variation couldbe explained by changes in the overbite, space conditions in the labial and buccal segments,treatment duration and the axial inclination of th-3 teeth adjacent to the extraction site.
The aim of orthodontic treatment is not onlyto correct malocclusion and create optimaltooth position but also to ensure the treat-ment results remain stable (Andrews, 1972).Relapses are partly dependent on the mor-phology of the different malocclusions (Berg,1979) and relapses of overjet, overbite,crowding, rotation and opening of extractionsites are the commonest occurrences. Per-sistence or re-opening of spaces at extractionsites may be a side effect of orthodontictreatment that has included extraction ofpermanent teeth and this can result in acondition which was not part of the originalmalocclusion.
The factors responsible for incompletespace closure or re-opening of extractionspaces, and the frequency of occurrence, havebeen studied at the time of debanding, at theend of retention and several months out ofretention. This paper deals with the conditionsfound at the time of debanding.
Material and methods
The material consisted of 90 patients (51 boysand 39 girls) with a mean age at the start oftreatment of 12 years 5 months (range 9 years1 month-17 years 4 months). All of thesubjects had been treated by the Bergentechnique (Hasund, 1972) and their treatmentincluded extractions of the first maxillarypremolars, or all four first premolars, or themaxillary first premolars and the mandibularsecond premolars.
The patients were divided into threegroups based on the malocclusion at the startof treatment, namely Angle's Class I, Angle'sClass II, Div. 1 or Angle's Class II, Division 2.
The data were obtained from casts andintra-oral radiographs taken before treatmentand at debanding. Not all of the patients hadmodels and radiographs at debanding so thenumbers in the different comparisons varybut the actual numbers are given in each table.
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018

12 RESIDUAL EXTRACTION SITES
Overjet, overbite and the space conditionin the dental arches were measured on thecasts (Figs 1 and 2). Residual extraction
Figure 1 Overjet (a). The distance from the labialincisor edge of the right upper central to the labialsurface of the right lower central incisor measuredalong the upper occlusal plane.Overbite (b). The distance from the incisor edge of thelower right central incisor to the upper occlusal plane.Overlapping gives positive values, open bite negativevalues.
Figure 2 Measurement of the space conditions. Theupper and lower dentition was divided into threesegments on each side; incisor segment (i), caninesegment (c) and premolar segment (p). The sum ofeach segment was compared with the mesio-distaldiameter of the teeth in that segment. Excess of spacegave a positive value, lack of space a negative value.During the handling of the data the number ofsegments was reduced to three in each jaw, two lateralsegments (premolars and canines) and one frontsegment (the two incisor segments).
spaces were measured with steel wires ofknown diameter up to 1.2 mm; larger spaceswere measured with a sliding calliper to anaccuracy of 0.1 mm. The degree of atrophy ofthe alveolar processes at the extraction siteswas recorded (Fig 3). All the measurementswere made on two occasions with an intervalof three weeks and the method error, calcu-lated from the double recordings, was withinacceptable limits.
The inclination of the teeth mesial anddistal to the extraction sites was measured onstandardized intra-oral radiographs (Fig 4).The presence or absence of the third molarswas noted.
Figure 3 The atrophy of the alveolar process wasgiven three scores: 1. No atrophy (A), 2. Moderateatrophy (B), 3. Definite atrophy (C).
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018

RESIDUAL EXTRACTION SITES 13
Figure 4 Inclination of the teeth mesial and distal tothe extraction sites. The long axis of the first molar,defined as the perpendicular to a tangent to themesio-buccal and disto-buccal cusp, was used as thedistal reference. The long axis of premolar or caninewas defined as a line through the coronal pulpchamber and 3/4 of the root canal. The angle betweenthe tooth axes is positive when converging apically andnegative when diverging apically.
The amount of distal movement of themaxillary canines was measured from thepre- and post-treatment models and the caseswere divided into those in which the canineshad been moved distally by more than halfthe width of the premolar and those in whichthe distal movement was less than half thewidth of a premolar. These measurementswere made on two occasions for each casewith a four week interval and the measure-ments coincided in 76% of the cases. Theremaining 24% were measured again afteranother four weeks and the two evaluationsthat coincided were used.
The duration of the treatment wasrecorded in years and months.
Tables 1-4 summarise this data. The datawere evaluated by a computer using standardstatistical procedures.
Table 1 Extractions, presence or absence of third molars and treatment time
Number ofextractions
Presence or absence ofthird molars
Treatment duration(years and months)
18-28 38-48Angle Cl
1II, div. 1II, div. 2
Table 2
Angle Cl
I11, div. 1II, div. 2
Table 3
Angle Cl
I11, div. 1II, div. 2
14-24 34-44
43 2136 811 - 1
Overjet and overbite
35-45
1881
+39298
—
473
at the start of treatment
X
3.497.883.50
Space conditions in the maxilla
Overjet (mm)
s*
1.731.901.10
min
1.05.02.5
+423210
max
8.012.05.5
at the start of treatment
Lateral segments (mm)
X
-2.400.09
-2.23
Sx
2.282.062.54
min
-8.5-4.5-6.5
max
3.03.751.5
—
141
X
3.354.225.00
X
-0.400.53
-0.68
X
1-71-101-8
sx
0-50-80-8
Overbite (mm)
Sx
1.591.471.07
min
-1.0-1 .0
4.0
Front (mm)
Sx
2.072.541.33
min
-7 .0-2.5-3 .0
min
0-60-90-7
max
6.56.07.0
max
4.03.51.0
max
2-83-53-4
n
433611
n
433611
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018

14
Table 4 Space conditions in the mandible at the start of treatment
RESIDUAL EXTRACTION SITES
Angle
III, divII, div
Cl.
. 1
. 2
Lateral segments (mm)
X
-2.58-1.03
0.27
Sx
2.012.051.51
min
-8.5-6.5-3.0
max
1.501.752.75
X
-1.000.10
-0.64
Sx
1.321.081.29
Front (mm)
min
-6 .0-2 .0-1 .0
max
0.02.01.0
n
433611
Results
The results are summarised in Tables 5-8.
Table 5
Angle Cl
III, div. 1II, div. 2
Table 6
Angle Cl
I
H, div. 1
II, div. 2
Table 7
Angle Cl
I
II, div. 1
11, div. 2
Changes in overjet and overbite <
d
-1.63-6.08-1.50
during treatmen
Overjet
Sd min
1.68 -2.01.85 3.01.27 -0.5
t
max
6.010.53.5
d
1.101.702.05
Overbite
Sd
1.791.651.21
Inclination of the teeth mesial and distal to the extraction sites at debanding
•
max.mand.
max.mand.
max.mand.
X
9.65-8.46
10.225.19
9.75-0.25
Atrophy of the alveolar process ;
max.mand.
max.mand.
max.mand.
No
4931
4012
140
Sx
6.567.19
6.096.12
7.445.79
it the extraction
Inclination (degrees)
min
-4.5-15.0
-2 .0-10.5
-5.5-8 .0
sites at
i Moderate
2129
1814
84
max
24.516.0
24.018.0
24.56.0
debanding
Atrophy
Marked
410
20
00
n
5652
5421
164
min
-3.5-3.5
0.5
max
4.04.53.5
Pos.
X
1.391.70
1.371.54
1.362.00
5223
5319
142
n
343010
Neg.
429
n
7470
6026
224
12
22
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018

RESIDUAL EXTRACTION SITES 15
Table 8 Spaces at the extraction sites at debanding
Angle Cl.
I1
II, div. 1
II, div. 2
max.
mand.
max.
mand.
max.
mand.
Spaces
«0.5>0.5Total
«0.5>0.5Total
<0.5>0.5Total
^0.5>0.5Total
«0.5>0.5Total
>0.5Total
X
0.270.940.64
0.261.040.66
0.321.151.01
0.310.880.57
0.340.940.80
0.880.88
Sx
0.170.430.47
0.210.330.48
0.200.520.58
0.180.190.34
0.100.330.40
0.150.15
min
0.00.60.0
0.00.60.0
0.00.60.0
0.00.60.0
0.00.60.0
0.70.7
max
0.52.42.4
0.51.71.7
0.52.72.7
0.51.11.1
0.51.61.6
1.01.0
n
344074
343670
104959
141226
51722
44
0/
/o45.954.1
100.0
48.651.4
100.0
16.983.1
100.0
53.846.2
100.0
22.777.3
100.0
100.0100.0
Angle's Class I
Fifty-one canines were moved distally by lessthan half a premolar width and 37 by morethan half a premolar width.
There was no statistical differencebetween the maxilla and the mandible(Table 9).
Angle's Class II, Div. 1
Sixty canines were moved distally by less thanhalf the width of a premolar and 54 by morethan half the width.
The t-test revealed significantly greaterspaces in the maxilla (Table 9).
Angle's Class II, Div. 2
Fourteen canines were moved distally by lessthan half a premolar width and 8 by morethan half a premolar width.
Table9 Comparison of the maxillary and mandibularspaces in the same and in the different malocclusions
Gaps in
MaxillaMandible
MaxillaMandible
MaxillaMaxilla
MaxillaMaxilla
MaxillaMaxilla
MandibleMandible
Angle Cl.
II
II, div. 1II, div. 1
III, div. 1
III, div. 2
II, div. 111, div. 2
III, div. 1
X
0.640.66
1.010.57
0.641.01
0.640.80
1.010.80
0.640.57
n
7470
5926
7459
7422
5922
7426
1*1
0.26
3.60**
3.84"
1.45
1.56
0.70
*p<0.01
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018

16 RESIDUAL EXTRACTION SITES
The Whole Material
A comparison between the size of the spacesin the same jaw of the different groups showeda significant difference only between Angle'sClass I and Angle's Class II, Div. 1 in themaxilla, with larger spaces in the Class IIgroup (Table 9).
When all the groups were combined,the maxilla showed 15 small spaces and105 larger spaces (mean 0.29 mm and1.03 mm respectively). In the mandible,48 small spaces and 52 larger spaces wereobserved (mean 0.27 mm and 0.99 mmrespectively).
The t-test showed no significantdifferences between the total size of the spacesin the maxilla and the mandible.
Regression Analysis
Regression analysis was used to determine thefactors influencing the size of the spaces. Inthe maxilla, the important parameters were,the age at the start of treatment, type ofmalocclusion, change of overjet and overbite,space conditions in the anterior and buccalsegments at the start of treatment, thepresence of third molars, the duration oftreatment, atrophy of the alveolar processesand the angle between the teeth adjacent tothe extraction sites.
The analysis including these variablesgave a regression coefficient of RL = 0.62which means that 38% of the variation of thespaces can be accounted for by these variables.Changes in overjet and overbite, spaceconditions in the anterior segment, presenceof third molars and the angle between thefirst molar and the canine had little influenceon the regression coefficient.
An analysis including age at the start oftreatment (Xx), type of malocclusion (X2),space condition in the lateral segments (X3),treatment duration (X4) and alveolar atrophy(X5) resulted in a coefficient R2 = 0.57 whichaccounts for 33% of the variation of theresidual extraction spaces.
The magnitude of the spaces in the right
and left upper first premolar region (Y) willbe:—Y = -O.OlXi + 0.14*X2 + 0.09**X3 -0.02** Y4 + 0.34**X6 + 1.47
*p<0.05 **p<0.01
Measurements of the spaces after extrac-tion of both mandibular first premolars orboth mandibular second premolars werecombined. Using the same variables as in themaxilla, the mandibular analysis resulted in aregression coefficient R, = 0.73, accountingfor 53 % of the variation of the spaces.
The variables which most influenced thesize of the spaces were, changes in the overbite(Xx), space conditions in the anterior segment(X2), and the buccal segments (X3), durationof treatment (X4) and the angle between thelong axis of the teeth mesial and distal to theextraction site (X5).
An analysis including these four variablesresulted in a coefficient R2 = 0.68 accountingfor 46 % of the variation of the spaces. Themagnitude of the spaces in the mandibularfirst or second premolar region being thedependent variable (Y) can be expressed asfollows:—Y = 0.04Xi - 0.06X2 + 0.10**X3 - 0.01X4
+ 0.01X5+ 1.15
**p<0.01
Discussion
All clinicians are aware that the excellentpost-retention cases frequently demonstratedin case presentations are not achievedroutinely (Myrberg and Thilander, 1973).
This work is part of a study of changes inextraction spaces from the end of activetreatment to several months out of retention.
If orthodontic bands are used duringtreatment there will always be slight spacingbetween teeth at the time of debandingalthough this can be minimised by sectionaldebanding or by using direct bonded brackets.The optimal closure of spaces at extractionsites at debanding probably varies between0.0 mm and 0.3 mm.
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018
RESIDUAL EXTRACTION SITES 17
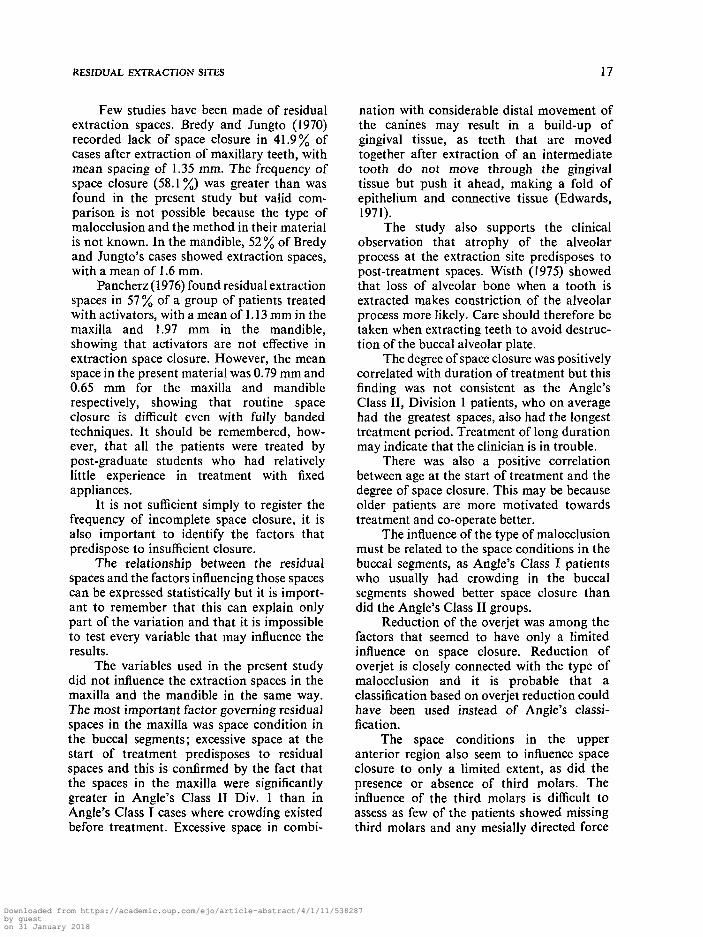
Few studies have been made of residualextraction spaces. Bredy and Jungto (1970)recorded lack of space closure in 41.9% ofcases after extraction of maxillary teeth, withmean spacing of 1.35 mm. The frequency ofspace closure (58.1%) was greater than wasfound in the present study but valid com-parison is not possible because the type ofmalocclusion and the method in their materialis not known. In the mandible, 52 % of Bredyand Jungto's cases showed extraction spaces,with a mean of 1.6 mm.
Pancherz (1976) found residual extractionspaces in 57 % of a group of patients treatedwith activators, with a mean of 1.13 mm in themaxilla and 1.97 mm in the mandible,showing that activators are not effective inextraction space closure. However, the meanspace in the present material was 0.79 mm and0.65 mm for the maxilla and mandiblerespectively, showing that routine spaceclosure is difficult even with fully bandedtechniques. It should be remembered, how-ever, that all the patients were treated bypost-graduate students who had relativelylittle experience in treatment with fixedappliances.
It is not sufficient simply to register thefrequency of incomplete space closure, it isalso important to identify the factors thatpredispose to insufficient closure.
The relationship between the residualspaces and the factors influencing those spacescan be expressed statistically but it is import-ant to remember that this can explain onlypart of the variation and that it is impossibleto test every variable that may influence theresults.
The variables used in the present studydid not influence the extraction spaces in themaxilla and the mandible in the same way.The most important factor governing residualspaces in the maxilla was space condition inthe buccal segments; excessive space at thestart of treatment predisposes to residualspaces and this is confirmed by the fact thatthe spaces in the maxilla were significantlygreater in Angle's Class II Div. 1 than inAngle's Class I cases where crowding existedbefore treatment. Excessive space in combi-
nation with considerable distal movement ofthe canines may result in a build-up ofgingival tissue, as teeth that are movedtogether after extraction of an intermediatetooth do not move through the gingivaltissue but push it ahead, making a fold ofepithelium and connective tissue (Edwards,1971).
The study also supports the clinicalobservation that atrophy of the alveolarprocess at the extraction site predisposes topost-treatment spaces. Wisth (1975) showedthat loss of alveolar bone when a tooth isextracted makes constriction of the alveolarprocess more likely. Care should therefore betaken when extracting teeth to avoid destruc-tion of the buccal alveolar plate.
The degree of space closure was positivelycorrelated with duration of treatment but thisfinding was not consistent as the Angle'sClass II, Division 1 patients, who on averagehad the greatest spaces, also had the longesttreatment period. Treatment of long durationmay indicate that the clinician is in trouble.
There was also a positive correlationbetween age at the start of treatment and thedegree of space closure. This may be becauseolder patients are more motivated towardstreatment and co-operate better.
The influence of the type of malocclusionmust be related to the space conditions in thebuccal segments, as Angle's Class I patientswho usually had crowding in the buccalsegments showed better space closure thandid the Angle's Class II groups.
Reduction of the overjet was among thefactors that seemed to have only a limitedinfluence on space closure. Reduction ofoverjet is closely connected with the type ofmalocclusion and it is probable that aclassification based on overjet reduction couldhave been used instead of Angle's classi-fication.
The space conditions in the upperanterior region also seem to influence spaceclosure to only a limited extent, as did thepresence or absence of third molars. Theinfluence of the third molars is difficult toassess as few of the patients showed missingthird molars and any mesially directed force
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018

18 RESIDUAL EXTRACTION SITES
from the erupting molars would be negligiblein view of the low age of the patients.
The angulation of the teeth adjacent tothe extraction site did not influence the degreeof space closure, in contrast to what wasobserved in the mandible. It is probable,however, that the effect would be greaterduring the retention and post-retentionperiods. The factors influencing space closurein the mandible were different from those inthe maxilla. Pre-treatment spaces in thebuccal segments resulted in residual spaces atthe end of treatment. Better space closure wasobserved after treatment of long duration.There was a definite correlation betweeninadequate space closure and lack of paral-lelism of the roots of the teeth adjacent to theextraction sites. It seems that tipping of theteeth results in incomplete space closure,probably because the teeth tend to uprightand the spaces open. This is in accordancewith the findings of Hatasaka (1976) andBerg (1979).
Marked changes in the overbite alsoresulted in smaller residual spaces, probablyas a result of the levelling of the curve of Speewhich, in itself, will tend to reduce theextraction spaces and produce mesial migra-tion of the buccal teeth (Hasund, 1972).
Age at the start of treatment did notinfluence the residual spaces nor did the typeof malocclusion affect the magnitude of thespaces, possibly because the problems oftreatment in the mandible are similar inAngle's Class I and Angle's Class IImalocclusions.
Surprisingly, the degree of atrophy of thealveolar process did not affect space closurein the mandible, possibly due to the fact thatclosure of mandibular spaces involved moretipping of the adjacent teeth which might berelatively unaffected by the atrophy. Thepresence or absence of third molars was notsignificant, possibly due to the relativelyinfrequent absence of the third molars and thelow age of the patients. Other investigatorshave observed that the third molars haverelatively little influence on the mesialmigration of the buccal teeth (Norderval,Wisth and Boe, 1975).
The five variables included in theregression analysis could account for only33% of the variation in the maxilla and 46%in the mandible. Thus, factors not included inthis study must have been involved. Othervariables that might be investigated in a studyof differences in space closure includeindividual variation in root length and bonedensity, magnitude of forces during treatment,patient co-operation and oral hygiene.
Address for correspondence
Per John Wisth,Department of Orthodontics,School of Dentistry,University of Bergen,Arstadveien 17N-5000 BergenNorway.
References
Andrews, L. F. (1972). Six keys to normalocclusion. American Journal of Orthodon-tics, 62: 296-309.
Berg, R. (1979). Post-retention analysis oftreatment problems and failures in 264consecutively treated cases. EuropeanJournal of Orthodontics, 1: 55-68.
Bredy, E. and Jungto, H. (1970). Spa'tergeb-nisse nach kieferorthopadischer Extrak-tionstherapie. Fortschritte der Kiefer-orthopadie, 31: 367-379.
Edwards, J. G. (1971). The prevention ofrelapse in extraction cases. AmericanJournal of Orthodontics, 60: 128-141.
Hasund, A. (1972). The Bergen technique. Aclinical manual for a light-wire edgewisetechnique. University of Bergen, Bergen,Norway.
Hatasaka, H. (1976). A radiographic study ofroots in extraction sites. Angle Orthodon-tist, 46: 64-68.
Myrberg, L. and Thilander, B. (1973). Anevaluation of the duration and the resultsof orthodontic treatment. ScandinavianJournal of Dental Research, 81: 85-91.
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018

RESIDUAL EXTRACTION SITES 19
Norderval, K., Wisth, P. J. and B6e O. E. activator (Andresen appliance) treatment.(1975). Mandibular anterior crowding in Odontologisk Revy, 27: Suppl. 35.relation to tooth size and cranio-facial Wisth, P. J. (1975). Periodontal status ofmorphology. Scandinavian Journal of neighbouring teeth after orthodonticDental Research, 83: 267-273. closure of mandibular extraction sites.
Scandinavian Journal of Dental Research,Pancherz, H. (1976). Long-term effects of 83:307-313.
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018
Downloaded from https://academic.oup.com/ejo/article-abstract/4/1/11/538287by gueston 31 January 2018