Embed Size (px)
DESCRIPTION
Residential Mobility and Children’s Well-Being. David Murphey, Ph.D. Kristin A. Moore, Ph.D. Tawana Bandy. Presented to the International Society for Child Indicators, Biannual Meeting York, England July 27-29, 2011. - PowerPoint PPT Presentation
Citation preview

Residential Mobility and Children’s Well-Being
David Murphey, Ph.D.Kristin A. Moore, Ph.D.
Tawana Bandy
www.childtrends.org Twitter/childtrends www.facebook.com/childtrends:
Presented to the International Society for Child Indicators, Biannual MeetingYork, England
July 27-29, 2011

2Residential MobilityMurphey et al.
Goals:
• Examine the prevalence and frequency of residential moves among U.S. children
• Analyze the association of frequent moves with several measures of child well-being, controlling for other demographic variables

3Residential MobilityMurphey et al.
Residential moves are common among U.S. households with children
• The recent housing crisis has increased rates of residential discontinuity, prompting concerns about children’s welfare
• In 2010, nearly 10 million children (about 1 in 7, ages 1-17) changed residence; nearly three-quarters of these were moves within the same county
• However, we know less about children’s experience of multiple moves

4Residential MobilityMurphey et al.
Residential Mobility: A Negative or Positive Influence on Well-Being?
• Moving represents a source of (negative) turbulence in a child’s life, disrupting multiple contexts for development, as well as contributing to parental stress
• A move can also represent a positive change, if it is associated with improved opportunity or access to more resources, or with leaving a harmful environment

5Residential MobilityMurphey et al.
Moving is confounded with many family-level characteristics
• Younger families move more often• Poorer families move more often• Adult-couple instability may prompt moves• The older the child, the greater the likelihood he/she has
“ever” moved
• Thus, researchers must control for these and other “endogenous” variables

6Residential MobilityMurphey et al.
Younger children may be particularly vulnerable to frequent residential disruption
• Rapid development in multiple domains (social, emotional, cognitive)
• Dependence of their well-being on parents’ own coping abilities

7Residential MobilityMurphey et al.
However, older children may also be at risk, particularly when moves involve changing schools
• Social networks are an important part of adolescent well-being
• These extend beyond school, but school is a primary setting, not only socially, but for academic achievement

8Residential MobilityMurphey et al.
The present study
• Uses data from the 2007 National Survey of Children’s Health, a telephone survey designed to yield samples representative of the U.S. and each of the states.– Primary focus is health, but includes measures of a
number of child well-being constructs, and developmental contexts
– Parent is reporter on a single focal child– National sample size is approximately 90,000– Administered in 2003, 2007, and 2011

9Residential MobilityMurphey et al.
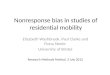
Descriptive Findings: Many children experience multiple moves
• Among 0- to 5-year-olds, although more than half have had no moves, more than one in four have moved 3 or more times, and nearly one in ten have moved 5 or more times.
• By the time they are 12 to 17 years old, a majority (61 percent) of children have moved 5 or more times.

10Residential MobilityMurphey et al.
Frequency of Moves, by Age Group Total Weighted Sample
No moves 1 or 2 moves 3 or 4 moves 5 or more moves
52%
30%
18%
9%
26%
36% 38%
29%
22%
34%
45%
62%
Ages 0-5Ages 6-11Ages 12-17

11Residential MobilityMurphey et al.
Multivariate analysis:
• Stratify sample by age group: 0-5, 6-11, and 12-17 • Within each group, statistically control for:– Family income (poor, near-poor, not poor)– Mother’s level of education (high school only, some
college, 4-year college degree or higher)– Race/ethnicity (white, African-American, Hispanic, other)– Family structure (2 biological or adoptive parents vs.
other)

12Residential MobilityMurphey et al.
Analysis (continued)
• Within each age group, and using single year of age as a covariate, use statistical regression to examine the independent contribution of frequent mobility (defined as 5+ moves) to:– Global health rating (“excellent” or “very good”)– Has received treatment/counseling from a mental health professional,
past 12 months– Problems with school, past 12 months (ages 6-11 and 12-17 only)
– “Externalizing” behavior problems composite (ages 6-11 and 12-17 only)
– “Internalizing” behavior problems composite (ages 6-11 and 12-17 only)
– School engagement composite (ages 6-11 and 12-17 only)
– Participation in after-school activities (ages 12-17 only)

13Residential MobilityMurphey et al.
Multivariate results: Ages 0-5
• No child outcomes significantly associated with frequent moves

14Residential MobilityMurphey et al.
Multivariate results: Ages 6-11
• Children who have moved frequently are more likely than others to have received mental health treatment/counseling
• Frequent movers more likely to have “externalizing” behavior problems (diagnosed conduct problems, and/or diagnosed attention deficit hyperactivity disorder)
• No significant associations with global health, “internalizing” behavior problems, school problems, or school engagement

15Residential MobilityMurphey et al.
Children Ages 6-11
7.7% 7.7%
12.5% 12.9%
Full SampleFrequent Movers

16Residential MobilityMurphey et al.
Multivariate results: Ages 12-17
• Frequent movers are more likely than others to have received mental health treatment/counseling
• Frequent movers are more likely than others to have “externalizing” behavior problems (diagnosed conduct problems, and/or diagnosed attention deficit hyperactivity disorder)
• Frequent movers are more likely than others to have had the school contact the family to report problems
• No significant associations with global health, “internalizing” behavior problems, school engagement, out-of-school activities

17Residential MobilityMurphey et al.
Children Ages 12-17
Receive
d Mental
Health Treatm
ent
Externali
zing B
ehaviors
School P
roblems
15.1% 15.1% 14.9%
24.0% 24.0% 23.9%
Full SampleFrequent Movers

18Residential MobilityMurphey et al.
Conclusions
• Frequent moving had no significant positive associations with well-being
• Negative findings were limited to school-age children• Negative findings were in the psycho-social domain, not in
physical health• There is some evidence to link frequent moving to reported
problems with school, but not to school engagement

19Residential MobilityMurphey et al.
Limitations of the present study
• Cannot make causal attributions• No measure of the distance of moves• No measure of what motivated moves• Single point in time; no measures of child’s adjustment over
time• Future work could examine:– Possible differences by child-gender – Possible mediator/moderator role for how parents cope
with moves• A good indicator?

Twitter/childtrends www.facebook.com/childtrends
www.childtrends.org
www.childtrends.org/WhatWorks

Contact information: NAMES, email, phone
Relevant paper(s) and link on Child Trends site if applicable.
www.childtrends.org Twitter/childtrends
www.facebook.com/childtrends