Embed Size (px)
Citation preview

Residential Exposure to PesticideDuring Childhood and ChildhoodCancers: A Meta-AnalysisMei Chen, PhD, MS, Chi-Hsuan Chang, MSc, Lin Tao, PhD, Chensheng Lu, PhD, MS
abstractCONTEXT: There is an increasing concern about chronic low-level pesticide exposure duringchildhood and its influence on childhood cancers.
OBJECTIVE: In this meta-analysis, we aimed to examine associations between residentialchildhood pesticide exposures and childhood cancers.
DATA SOURCES:We searched all observational studies published in PubMed before February 2014and reviewed reference sections of articles derived from searches.
STUDY SELECTION: The literature search yielded 277 studies that met inclusion criteria.
DATA EXTRACTION: Sixteen studies were included in the meta-analysis. We calculated effect sizes and95% confidence intervals (CIs) by using a random effect model with inverse variance weights.
RESULTS: We found that childhood exposure to indoor but not outdoor residential insecticideswas associated with a significant increase in risk of childhood leukemia (odds ratio [OR] =1.47; 95% CI, 1.26–1.72; I2 = 30%) and childhood lymphomas (OR = 1.43; 95% CI, 1.15–1.78;I2 = 0%). A significant increase in risk of leukemia was also associated with herbicide exposure(OR = 1.26; 95% CI, 1.10–1.44; I2 = 0%). Also observed was a positive but not statisticallysignificant association between childhood home pesticide or herbicide exposure and childhoodbrain tumors.
LIMITATIONS: The small number of studies included in the analysis represents a major limitationof the current analysis.
CONCLUSIONS: Results from this meta-analysis indicated that children exposed to indoorinsecticides would have a higher risk of childhood hematopoietic cancers. Additional researchis needed to confirm the association between residential indoor pesticide exposures andchildhood cancers. Meanwhile, preventive measures should be considered to reduce children’sexposure to pesticides at home.
Department of Environmental Health, Harvard T.H. Chan School of Public Health, Boston, Massachusetts
Dr Chen participated in the study conception, design, identification of studies, data collection, study selection, data extraction, data analysis and interpretation, anddrafting and revision of the article; Ms Chang participated in data collection, study selection, data analysis, and revision of the article; Dr Tao participated in datacollection, study selection, and data analysis; Dr Lu participated in the study conception, design, identification of studies, data collection, study selection, dataextraction, analysis, and interpretation, and critical revision of the article; and all authors approved the final manuscript as submitted.
www.pediatrics.org/cgi/doi/10.1542/peds.2015-0006
DOI: 10.1542/peds.2015-0006
Accepted for publication Jul 7, 2015
Address correspondence to Chensheng Lu, PhD, MS, Department of Environmental Health, Harvard T.H. Chan School of Public Health, Landmark Center West 404G,401 Park Dr, Boston, MA 02215. E-mail: [email protected]
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2015 by the American Academy of Pediatrics
PEDIATRICS Volume 136, number 4, October 2015 REVIEW ARTICLE by guest on June 4, 2020www.aappublications.org/newsDownloaded from

Although pesticides are essential foreradication of pests in agriculture andfor public health, they are toxicchemicals and can affect children’shealth in a variety of settings, such asat home, in parks and gardens, and onschool grounds. Children greatlyincrease their chances of pesticideexposure when they play onpesticide-treated surfaces such asa floor or lawn and then put theirhands into their mouths. It is knownthat households with childrencommonly use and store pesticideproducts.1–3 The use of pesticides atchild care facilities,4 on athleticfields,5 and on school grounds6 couldall present potential exposures andhealth hazards to children.
Because children’s immune systemsare still developing, they may provideless protection than adult immunesystems. To be specific, theirenzymatic and metabolic systemsmay be less able to detoxify andexcrete pesticides than those ofadults. Therefore, they are morevulnerable to pesticides.Epidemiologic studies also supportthe idea that pesticide exposure canhave greater impact on children’shealth than on adults’ health.7,8
Children exposed to pesticides athome or at school have experiencedacute toxic effects on theirrespiratory, gastrointestinal, nervous,and endocrine systems, as well asother serious medical outcomes.6,9,10
Concern about the health effects oflow-level exposure to pesticides inchildren has been increasing in recentyears, generating a substantialnumber of epidemiologic studiesdemonstrating associations betweenpesticide exposures and childhoodcancers.11–16 However, most ofthese studies focused on parentaloccupational exposure or agriculturalexposure, not exposure in the home.We found a few systematic reviewsexamining the association betweenresidential pesticide exposure andchildhood cancers. But theassociation was not elucidated inthese reviews, because authors
included parental occupationalexposure data or studies investigatingmultiple risk factors that increasechance findings through multiplestatistical testing.12–14
The aim of our study was to performa systematic review of the currentlyavailable epidemiologic evidence toestimate the relationship betweenresidential (or nonoccupational andnonagricultural) childhood pesticideexposure and childhood cancers. Wesought to provide scientific evidencefor preventive actions and for makinglegislative decisions.
METHODS
Data Source and Study Selection
We conducted a literature searchin PubMed for articles publishedbefore February 2014. We usedcombinations of the followingkeywords to identify relevant articles:[residential, urban, indoor, house,home, household, domestic or school]AND [pesticide, insecticide, herbicide,fungicide, organochlorine ororganophosphorus] AND [children,childhood, youth, teenager,adolescent, toddler, infant, neonate,prenatal or postnatal] AND [cancer,tumor, malignancy, neoplasm,neuroblastoma, lymphoma, leukemia,sarcoma, astrocytoma, glioma,craniopharyngioma, ependymoma,rhabdomyosarcoma or retinoblastoma].The search was limited to humanstudies and written in English. Allabstracts were screened to determinetheir suitability for review.
We included original epidemiologicstudies reporting on nonoccupationalpesticide exposure and children’shealth. We used the following criteriato exclude articles from the meta-analysis. We excluded those notreporting original results (eg, reviewarticles, ecologic studies, or casereports); toxicological studies; studiesconducted in occupational settings,on hazardous waste sites, on farms,or in proximity to agriculturalpesticides; studies involving only
adults or children with Downsyndrome or without reportingchildren’s health outcomes; studieswith only pesticides in general (nospecific pesticide groups) or studieswith a list of chemicals includingpesticides; studies without specificwindows of exposure; or duplicatestudies that included subjects alreadyincluded in a more complete or morerecent study examining a greaternumber of subjects.
Two authors of this article (M.C. andC.L.) independently retrieved andscreened all the titles and abstractsof studies according to thepredetermined selection criteria. Wealso manually screened references inthe selected articles for additionalrelevant studies. The full texts of thestudies with potential eligibility wereobtained and assessed independentlyby the 2 authors (M.C. and C.L.) forfinal inclusion. Any discrepancieswere resolved by consensus.
Data Extraction
From each eligible study, 2 authors(M.C. and C.C.) extracted informationabout the study design, location,study period, study population andcontrol characteristics, exposureassessment method, outcomes, andkey findings. The same 2 authorsindependently extracted andtabulated the most relevantestimators, namely odds ratios (ORs)and 95% confidence intervals (CIs).ORs and CIs are 2 commonly usedestimators in most meta-analysesdealing with health risks associatedwith environmental chemicalexposures.12,13,15,17–21 The resultswere compared and consensus wasobtained before the meta-analysis.
After classification of the studies, thedata were subgrouped and calculatedby pesticide categories, exposurelocations, and type of cancer in thefollowing stratified meta-analyses:
• Pesticide category and exposurelocations:• Indoor pesticide exposure• Indoor insecticide exposure
720 CHEN et al by guest on June 4, 2020www.aappublications.org/newsDownloaded from

• Outdoor pesticide exposure• Herbicide exposure
• Outdoor insecticide exposure
• Cancer types: acute leukemia,leukemia, lymphoma, hematopoieticcancers (leukemia and lymphoma),childhood brain tumor, and allchildhood cancers (includingneuroblastoma, Wilms tumor, andsoft tissue sarcoma)
We analyzed data from professionalhome treatment (ie, the work done bylicensed pest control professionals)by performing a meta-analysis ondata with professional hometreatment together with parentalhome treatment or by using data forprofessional home treatments alone(if number of studies was $2). Wecalculated dose effect by performinga separate meta-analysis on data ofthe highest frequency of pesticideuses.
Data Analysis
We performed the meta-analysis byusing the Comprehensive MetaAnalysis version 2 (Biostat, Inc,Englewood, NJ) in accordance withMeta-analysis of ObservationalStudies in Epidemiology (MOOSE)guidelines.22 The random effectsmodel was used in this analysis. Therandom effects summary of ORs and95% CIs was estimated to provide anindicator of the overall strength ofassociation between childhoodpesticide exposure and childhoodcancers. These associations areillustrated in the forest plots. In theplots, the CI for each study isrepresented by a horizontal line andthe estimate of summary OR by a boxsquare. The box area is proportionalto the weight, which is the inverse ofthe variance of the effect estimatefrom each individual study in themeta-analysis. The diamond andbroken vertical line for type of cancerrepresent the subtotal summaryestimate, with CI indicated by itswidth. The null hypothesis is 1 and isrepresented by the central verticaldashed line from top to bottom of the
plot. All statistical tests were 2 sided,and a P value of ,.05 was consideredstatistically significant.
Assessment of Heterogeneity
Because the current review includesa limited number of studies, and theconventional statistical approach toevaluating heterogeneity usinga x2 test (Cochran’s Q) has low powerwhen there are few studies,23 weused the I2 statistic to quantify theamount of variation in results acrossstudies that is due to heterogeneity.I2 can be interpreted as a measure ofthe percentage of the total variationthat cannot be explained by chance.23
An I2 value of 25%, 50%, or 75% canbe taken to mean low, moderate, orhigh degrees of heterogeneity.23 Avalue of 0% indicates no observedheterogeneity, and estimations fromeither the fixed effects model orrandom effects model would be thesame. The P values for heterogeneityare based on the Q statistic.
Publication Bias
Publication bias was tested withfunnel plots and Egger’s test.24 Thefunnel plot was made by the naturallogarithm of the estimate of ORsversus the SE from all includedindividual studies in a meta-analysis.We tested funnel plot asymmetry,which can result from unpublishedsmall studies without statisticallysignificant effects, by using the linearregression method.24
Sensitivity Analysis
To measure the robustness anddetermine whether some of thefactors (or possible biases) havea major effect on the results of thismeta-analysis, we conducted severalsensitivity analyses by
• Removing the study with highestweight
• Removing the studies reportingextreme ORs (the highest and thelowest)
• Removing hospital-based studies(or performing a meta-analysis
including only population-basedstudies)
• Removing extended exposure win-dows or ill-defined pesticidecategories
RESULTS
Study Identification andCharacteristics
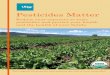
Figure 1 describes this study’sidentification, screening, andselection process. From the initial 277articles identified from PubMedsearch, 239 were excluded based ontheir titles or abstracts, and 17 wereexcluded based on the full text. Weexcluded 3 other studies from theanalysis. One had a duplicatedpopulation, another had a studypopulation located in a region withhigh agricultural pesticide use, anda third had insufficient data to permitthe calculation.25–27 No additionalarticles were identified from thereferences cited in the includedarticles. A total of 16 articles met thefull inclusion criteria and wereeventually included in the meta-analysis.28–43
The characteristics of the studies usedin the meta-analysis are shown inTable 1. All 16 studies are case-controlled studies published between1993 and 2012. The participation ratesfor most studies ranged between 65%and 96% for case groups and between61% and 99% for control groups.The sample sizes ranged from 4532 to1184 cases,38 and the upper age limitsof case groups were between 9 and19 years. Among these studies, 10focused on hematopoietic malignancies,5 on childhood brain tumor (CBT), and2 on Wilms tumor and neuroblastoma.Four other studies reported data on.1 malignancy.36–38,41
The current meta-analysis was runseparately for the 2 windows ofexposure: before and after birth todiagnosis, and after birth to diagnosis.Because the outcomes from eitherwindow of exposure were similar (asshown in Supplemental Table 3), the
PEDIATRICS Volume 136, number 4, October 2015 721 by guest on June 4, 2020www.aappublications.org/newsDownloaded from

following results and discussion focuson the window from prenatal andafter birth until diagnosis.
Publication Bias
We examined the main findings fromall studies and included them in aninverse funnel plot of log-transformedodds ratio versus SE. Although wewere limited by the small numberof studies included, we saw noclear trend of publication bias (orasymmetry) from visual inspection ofthe plot, with Egger’s test P valuesat .92, .10, and .14 for indoorpesticides, herbicides, and outdoorpesticide exposures, respectively.
Study Synthesis
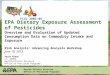
Table 2 summarizes the results of thesubgroup meta-analyses and theassessment of heterogeneity. Theresults of 13 studies on home
pesticide exposure, grouped by typesof childhood cancer and listed byyears of publication, are shown inFig 2. Exposure to indoor insecticidesduring childhood was associated witha significant increase in risk ofchildhood leukemia (OR = 1.47; 95%CI, 1.26–1.72; I2 = 30%) andchildhood lymphomas (OR = 1.43;95% CI, 1.15–1.78; I2 = 0%).
Additional subgroup analysiscombining studies on acute leukemia(AL) yielded elevated risks forexposure to both home pesticides(OR = 1.55; 95% CI, 1.38–1.75) andindoor insecticides (OR = 1.59; 95%CI, 1.39–1.81) with significantly lowerheterogeneities (I2 of 0%). When wecombined studies on leukemia andlymphoma, we observed a statisticallysignificant association betweenchildhood hematopoieticmalignancies and home pesticide
exposure during childhood (11 outof 12 data were from indoorinsecticides). There was lowheterogeneity (OR = 1.46; 95% CI,1.32–1.60; I2 # 5%). A positive butnot statistically significant associationbetween home pesticide exposureduring childhood and CBT wasobserved (OR = 1.22; 95% CI,0.83–1.81; I2 = 23%) and thisassociation decreased after data werecombined with those for professionalhome treatment (OR = 1.11; 95%CI, 0.87–1.42; I2 = 5%).
We conducted sensitivity analysis onthe results to test whether theseresults were influenced by 1 or 2studies (Supplemental Table 3).Sensitivity analysis conducted byremoving highest weights, excludingextreme ORs, or deleting hospital andfriends controls did not change theassociations between home pesticide(or indoor insecticide) exposure andchildhood AL, leukemia, lymphoma,and childhood hematopoieticmalignancies (shown in SupplementalTable 3), and statistical significanceremained. Heterogeneities weresignificantly lower (most I2 were 0%)after extreme ORs were removed inthe sensitivity analyses. When wereplaced the indoor pesticide data ofMa et al37 with insecticide data in thererun meta-analysis, the result wasvery similar. This finding wasconsistent with the statement bythose authors that “there wasa considerable overlap between thedefinition as well as the resultsbetween indoor pesticides andinsecticides.”
Subgroup analysis on dose andmultiple-agent effect yieldeda statistically significant higher riskfor childhood leukemia (OR = 1.92;95% CI, 1.27–2.89) andhematopoietic malignancies (OR =2.04; 95% CI, 1.40–2.97). However,when the studies on professionalhome treatment were groupedtogether, the seemingly significantincrease in risk for childhood leukemiabecame not statistically significant.
FIGURE 1PRISMA 2009 Flow Diagram. (Reprinted with permission from Moher D, Liberati A, Tetzlaff J, AltmanDG; The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: ThePRISMA Statement. PLoS Med. 2009;6(6):e1000097)
722 CHEN et al by guest on June 4, 2020www.aappublications.org/newsDownloaded from

TABLE1
Overview
oftheCase-ControlledStudiesIncluded
intheMeta-Analysis
Study
SampleSize
(case/control)
Age(y)
StudyPopulation,Location,andPeriod
Exposure
Assessment
Cases
Controls
Daviset
al(1993),U
SA45/85
#10
Patientsin
Missouri,diagnosed
1985–1989
Maternalphoneinterview
CBT
Noncancerfriendsor
other
cancer
matched
with
age
andgender
Leisset
al(1995),U
SA252/222
,15
Patientsin
Denver,1976–1983
Parental
interview
CBT,Leu,Lym,STS
Noncancerpopulationmatched
bygender,age,region
Pogoda
etal
(1997),U
SA224/218
#19
Patientsfrom
WestCoast,1984–1991
Maternalphoneinterview
CBT
Noncancerpopulationmatched
bygender,age,region
Infante-Rivard
etal
(1999),C
anada
491/491
#9
Patientsfrom
metropolitan
Montreal,
diagnosed1980–1993
Parental
phoneinterview
ALL
Noncancerpopulationmatched
byage,gender,region
Meinetet
al(2000),G
ermany
1184,234,940/2588
#15
Patientsfrom
WestGerm
any,
diagnosed1992–1994
Mailandparental
phone
interview
Leu,NH
LNoncancerpopulationmatched
bygender,age,region
Buckleyet
al(2000),U
SA268/268
#20
Patientsin
US,1986–1990
Maternalphoneinterview
NHL
Noncancerpopulationmatched
byage,gender,and
race
Daniel
etal
(2001),U
SA390/296
,19
Hospitalpatientsin
USand
Canada,1992–1994
Parental
phoneinterview
Neuroblastom
aNoncancerpopulationmatched
byage,region
Maet
al(2002),U
SA162/162
#14
Hospitalpatientsin
northern
California,1995–1999
Maternalin-hom
epersonal
interview
ALL,Leu
Noncancerpopulationmatched
bygender,age,m
other’s
race,region
Menegauxet
al(2006),France
280/288
,15
Hospitalpatientsin
France,
diagnosed1995–1999
Maternalpersonal
interview
ALHospitalnoncancerchildren
matched
byage,gender,
hospital,race
Rudant
etal
(2007),France
1060/1681
,15
Patientsin
France,d
iagnosed
2003–2004
Maternalphoneinterview
AL,H
L,NH
LNoncancerpopulationmatched
byage,gender
Urayam
aet
al(2007),U
SA294/369
,15
Patientsfrom
northern
andcentral
California,diagnosedsince1995
In-hom
einterviewswith
caretaker
ALL
Noncancerchildrenmatched
byage,gender,H
ispanic
status,m
aternalrace,region
Cooney
etal
(2007),U
SA523/517
,16
Patientsin
USandCanada,1999–2002
Maternalphoneinterview
Wilm
stumor
Noncancerchildrenmatched
byageandregion
Nielsenet
al(2010),U
SA201/285
#10
Patientsin
USwestcoast,1984–1991
Maternalin-personinterview
CBT
Noncancerchildrenmatched
byageandgender
Baileyet
al(2011),Australia
388/870
,15
Patientsin
Australia,2003–2007
Parental
questionnairesand
phoneinterviews
ALL
Noncancerpopulationmatched
bygender,age,region
Ding
etal
(2012),China
176/180
#14
Hospitalpatientsin
Shanghais
China,2010–2011
Maternalin-personinterview
andchildren’surine
collections
ALL
Noncancerhospitalchildren
matched
bygender
andage
Greenopet
al(2013),Australia
288/917
#14
Patientsin
Australia,2005–2010
Maternalin-personinterview
CBT
Noncancerpopulationmatched
bygender,age,and
region
ALL,acutelymphoblasticleukem
ia;H
L,Hodgkinlymphom
a;Leu,
leukem
ia;Lym
,lym
phom
a;NH
L,non-Hodgkinlymphom
a;STS,softtissuesarcom
a.
PEDIATRICS Volume 136, number 4, October 2015 723 by guest on June 4, 2020www.aappublications.org/newsDownloaded from

Part of the reason could be the smallnumber of studies included.
Combining all studies reportingchildhood cancers (includingneuroblastoma31 and Wilms tumor30)with childhood home pesticideexposure yielded a meta-rate
summary OR of 1.40 (95% CI,1.28–1.52) with a low degree ofheterogeneity (I2 of 5%). Therefore,the results show that there isa statistically significant risk ofchildhood cancers associated withexposures to home pesticides,
especially indoor insecticides, duringchildhood.
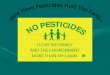
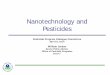
Outdoor pesticides include outdoorinsecticides, herbicides, andfungicides. Table 2 and Fig 3 show thecancer risks from exposure toresidential herbicides duringchildhood. A statistically significantassociation between childhoodleukemia and exposure to herbicides(OR = 1.26; 95% CI, 1.10–1.44, I2 =0%) was observed, and the sensitivityanalysis confirmed the robustness ofthis association. The greatest riskestimates were observed in theassociation between childhoodexposure to herbicides and the risk ofleukemia. The observed associationwith increase in risk of childhoodlymphoma became not statisticallysignificant during the sensitivityanalyses. No association appearedbetween herbicide exposure and CBT.When studies on all types ofchildhood cancers were combined,including neuroblastoma31 andWilms tumor,30 a statisticallysignificant association withresidential herbicide exposure wasobserved (OR = 1.35; 95% CI,1.16–1.55; I2 = 23%). We did not findany statistically significantassociation between exposure tooutdoor pesticides or outdoorinsecticides and any types ofchildhood cancers (Fig 4). Becauseonly a few studies were available onexposure to residential fungicides andchildhood cancers, we did not includeexposure to fungicides in the currentanalysis.
DISCUSSION
In this meta-analysis, we examined 16epidemiologic studies on the possibleassociation between residentialpesticide exposure during childhoodand childhood cancers. Overall, theresults suggest that cancer risks arerelated to the type of pesticide andwhere it was used. Exposure toresidential indoor insecticides but notoutdoor insecticides during childhoodwas significantly associated with an
TABLE 2 Meta-Analysis Using Random Effects Model for the Relationship Between ChildhoodCancer and Exposure to Residential Pesticides During Childhood
Subgroup Study N Summary Heterogeneity
OR 95% CI P I2
Indoor pesticidesa,b
(A) AL 6 1.59 1.40–1.80 .839 0Add professional home treatment 7 1.55 1.38–1.75 .794 0Indoor insecticides 5 1.59 1.39–1.81 .725 0
(B) Leukemia 8 1.48 1.29–1.70 .267 20Add professional home treatment 9 1.46 1.29–1.65 .327 13Dose and multiple agents effectsc 3 1.92 1.27–2.89 .959 0Professional treatment only 3 2.04* 1.05–3.95 .061 64Indoor insecticides 7 1.47 1.26–1.72 .197 30
(C) Lymphoma 4 1.43 1.15–1.78 .578 0Indoor insecticides 4 1.43 1.15–1.78 .578 0
(D) Hematopoietic cancers 12 1.47 1.33–1.62 .457 0Add professional home treatment 13 1.46 1.32–1.60 .513 0Indoor insecticides 11 1.46 1.31–1.63 .388 5Dose and multiple agents effectc 4 2.04 1.40–2.97 .894 0
(E) CBTsd,e,f 4 1.22 0.83–1.81 .275 23Add professional home treatment 5 1.11 0.87–1.42 .380 5
(F) All cancersf,g 20 1.40 1.28–1.52 .390 5Outdoor pesticidea,b
(A) Leukemia 6 1.15 0.95–1.38 .190 33Herbicide 5 1.26 1.10–1.44 .762 0Yard insecticidesh 3 1.11 0.60–2.05 .002 84
(B) Lymphoma 4 0.86 0.62–1.19 .131 47Herbicide 3 1.52* 1.02–2.27 .090 58Yard insecticidesi 2 1.12 0.78–1.59 .314 2
(C) Hematopoietic cancers 10 1.04 0.88–1.23 .086 41Herbicide 8 1.33 1.16–1.52 .350 10Yard insecticides 5 1.09 0.75–1.58 .007 71
(D) CBTs 3 0.95 0.47–1.89 .012 77Herbicide 2 1.98 0.94–4.14 .409 0Yard insecticidesj 2 1.29 0.86–1.92 .548 0
(E) All cancersg 16 1.10 0.93–1.32 .001 62Herbicide 12 1.35 1.16–1.55 .221 23Yard insecticidesk 8 1.14 0.89–1.45 .028 55
*The summary ORs became not statistically significant in the sensitivity analysis when we removed ill-defined herbicide orhighest weight or extreme ORs. Study N: number of studies included. Hematopoietic cancers include leukemia andlymphoma. All cancers include neuroblastoma and Wilms tumor and soft tissue sarcomas in outdoor pesticides. Studyresults with case numbers ,3 are not included in the summary.a In the study35 where insecticides against different types of nuisance were reported, data with the highest OR were used.b In the studies where results of different exposure windows in the same study were reported, the windows away frombirth were used.c The data of .10 per year were used in the study,38 and the data of .5 per year were used in the study.37d When both cancer-free controls and cancer controls were reported, cancer-free controls were used.e The crude OR and 95% CI were calculated based on the data in the article.42f Where .1 home pesticide usage was reported, home pesticides for nuisance pests were used.g In the study30 where the results were essentially the same during pregnancy and during childhood, the data reportedfrom pregnancy through childhood were treated as during childhood.h Includes studies35,39,41 and ORs associated with yard pesticides were replaced by yard insecticides in studies.35,39i Includes 2 data from the study.41j Includes 2 studies.32,40k In addition to all yard insecticides in each subgroup, an additional study30 was included and ORs associated with yardpesticides were replaced by yard insecticides.
724 CHEN et al by guest on June 4, 2020www.aappublications.org/newsDownloaded from

increasing risk of childhood cancersincluding leukemia, AL, andlymphoma but not CBT. Among the5 studies reporting CBT outcomes inthe analyses, 4 studies did notprovide specific exposure locations,although the applications wereprobably indoors. This ambiguityabout where pesticides were usedcould dilute the true effects ofresidential pesticides and thereforeresult in the association toward thenull. Similarly, the fact that addingprofessional home treatment inhematopoietic cancers and CBTlowers the summary ORs could alsoresult from the ambiguity of exposurelocation. The greatest risk estimateswere observed in the associationbetween childhood exposure toindoor insecticides and the risk of AL.The risk of childhood hematopoieticmalignancies increased with thefrequency of use. These observations
provide additional support to thepositive exposure–responserelationship between indoorinsecticide use and the increased riskof childhood hematopoieticmalignancies.
We did not observe any significantchildhood cancer risk associated withexposure to outdoor pesticides.However, when we looked into thedifferent categories of outdoorpesticides, we found that exposure toherbicides was associated witha slightly higher risk of childhoodcancers in general, which includeleukemia, lymphoma, and CBT,although statistical significanceappeared only in association withleukemia. No significant associationbetween outdoor insecticides andchildhood cancers was observed. Thisresult emphasizes how important it isto specify the type and location of thepesticide when analyzing pesticide
exposure and childhood cancer.Because of the small number ofstudies included in the current meta-analysis, more studies are needed toconfirm these associations.
Results from the current analysis arein agreement with the main findingsof 2 previously published studies onresidential pesticide exposure andchildhood leukemia.13,14 Bothobserved significant associationsbetween insecticide exposure andchildhood leukemia. Although theseresults were based on a small numberof studies, the consistency of the mainfindings suggests that there probablyis a higher risk of childhood leukemiawith indoor insecticide exposureduring childhood. We have observeda slightly elevated risk of childhoodleukemia associated with exposure toherbicides, with no evidence ofheterogeneity. This finding is alsoconsistent with that reported by VanMaele-Fabry et al14 but not by Turneret al,13 and both reported a highdegree of heterogeneity (I2 of 61%and 72%, respectively). Neither ourstudy nor the study of Turner et al13
observed any association betweenchildhood leukemia and exposure tooutdoor insecticides duringchildhood. Like Van Maele-Fabryet al,14 we also did not observe anyassociation between childhoodleukemia and outdoor pesticideexposure.
We also found a positive associationbetween childhood lymphoma andindoor insecticide exposure.Furthermore, the overall childhoodcancer risk is elevated with childhoodhome pesticide exposure. There wasa third study reporting that pesticideuse at home or in the garden wasstatistically associated with theelevated risk of lymphoma, leukemia,and CBT.20 However, Vinson et al20
did not provide information onspecific categories of pesticides orlocations of use in their analysis; mostof their study results were related tooccupational exposure. Therefore, we
FIGURE 2Meta-analysis of the association between childhood cancers and exposure to home pesticidesduring childhood. *Professional home treatments.
PEDIATRICS Volume 136, number 4, October 2015 725 by guest on June 4, 2020www.aappublications.org/newsDownloaded from

could not directly compare our resultswith those reported by Vinson et al.20
Although most of our findings areconsistent with those of the earliermeta-analyses, there are somedifferences. One main difference isthat several studies included in theprevious 2 meta-analyses wereexcluded from the current analysis.These were studies that either wereconducted in occupational settings,involved only adults, reported onlypesticides in general (not specifyingpesticide groups), or included otherchemicals with pesticides. Therefore,we eliminate the effects from thesestudies in the summary ORs.
Although previous meta-analysestook into account exposure locationsand pesticide categories whenperforming stratification analysis,Van Maele-Fabry et al14 reportedindoor and outdoor exposures but
gave no information about pesticidecategory. Stratification analysesbased on categories of pesticideexposure were run in the study byVan Maele-Fabry et al,14 but noanalysis was done on the exposurelocation for each category ofpesticide; therefore, the true riskfactors could be diluted. Therewere also no results fromsensitivity analyses provided byVan Maele-Fabry et al.14
Unlike Van Maele-Fabry et al’s14
report and our observation, Turneret al13 reported a statisticallysignificant positive associationbetween childhood leukemia andexposure to residential outdoorpesticides but not outdoorinsecticides nor herbicides. However,these results were inconsistent witheach other because outdoorpesticides were most likely to beoutdoor insecticides or herbicides.
In the current meta-analysis, wedivided studies into 3 subgroupsbased on the pesticide use pattern,such as indoor pesticides andinsecticides, outdoor pesticides andherbicides, and outdoor pesticidesand insecticides. We used a randomeffects model to estimate thesummary ORs for each subgroup. Inthe home pesticide (mostly indoorinsecticides) category, although somesubgroup analyses were conductedon only a limited number of studies(,5), the observed heterogeneitywas low (I2 # 13%) in theseanalyses. We also pooled studies toincrease the accuracy of estimatedsummary ORs for hematopoieticmalignancy and all cancers, and weobserved zero or low levels ofheterogeneity. Similarly, there wasno observed heterogeneity in theherbicide category, includingestimated summary ORs forhematopoietic malignancy and allcancers. These results of zero orlow heterogeneity for indoorpesticides and herbicide exposureindicated the consistency ofstudies included and suggest thatcombining data is appropriate.However, the heterogeneity foroutdoor pesticide or outdoorinsecticide exposure was high.Because these studies included in thecurrent meta-analysis differed instudy design, study population,and the exposure and timing ofexposure, the heterogeneity of theassociations should be interpretedwith caution.
Overall, our study has shown thatchildhood cancer risks are related tothe type of pesticide use and itsapplication locations duringchildhood. Childhood exposure toresidential indoor insecticides wasassociated with an increasing risk ofchildhood cancers but not outdoorinsecticides.
Although meta-analysis is a usefultool to assess causal relationships bycombining results from differentstudies, outcomes can be constrained
FIGURE 3Meta-analysis of the association between childhood cancers and exposure to residential herbicidesduring childhood.
726 CHEN et al by guest on June 4, 2020www.aappublications.org/newsDownloaded from

by the limitations of the originalstudies. In the current analysis, thesmall number of studies is a majorlimitation. Very few studies haveassessed pesticide exposures andchildhood cancers. In addition, otherlimitations such as selection bias,recall bias, misclassification, andpublication bias might limit theapplicability of the findings to thegeneral population. To deal withthe potential selection biasassociated with hospital or friendcontrols, we performed a sensitivityanalysis by excluding Davis et al32
and Menegaux et al39 from eachpesticide category to reinforce theassociations.
To reduce recall bias andmisclassification, the studies weincluded used several strategies toreduce confounding factors andbiases, such as restriction of entry tostudy of subjects with confounding
factors, matching controls to haveequal distribution of confounders,using standardized questionnaires,identical interviewing proceduresfor both cases and controls, andadjustment of the results.Publication bias refers to the factthat studies with less significantfindings may be less publishablethan those with positive outcomes;therefore, they would be unavailablefor meta-analyses. For example,one of the studies from the currentanalysis stated that “neitherresidential use of insecticides noruse of pesticides in the garden wasfound to be significantly morefrequent in any group of cases withsolid tumors compared withcontrols, therefore no quantitativedata were provided.”38 Althoughthe results from the currentmeta-analysis do not seem to besignificantly influenced by
publication bias, this bias cannotbe completely excluded. Note thatwhen Van Maele-Fabry et al14
assessed the impact of exclusion ofnonpublished data and studies inlanguages other than English, theyfound that rerunning the meta-analysis and including nonpublishedand non–English-language studiesdid not substantially modify theresults.
A positive exposure–responserelationship between residentialindoor insecticide use andoccurrence of childhood cancers wasobserved in the current study. Somestudies have also shown thatmaternal pesticide exposure duringpregnancy was associated withchildhood cancers.35,37,39 Althoughcurrent data do not establish themost critical exposure period for theoccurrence of childhood cancers,their development is probablymultifactorial and probablyincludes gene–environmentinteractions.11,44–46 Some studiesassert a possible associationbetween pesticide exposure withgenetic predisposition anddefined subtypes of childhoodcancers.26,42,43 Additional studiesare needed to examine the potentialmechanisms by which childhoodexposure to pesticides could lead tothe development of childhoodcancers.
CONCLUSIONS
The current meta-analysis hasrevealed positive associationsbetween exposure to home pesticidesand childhood cancers, with thestrongest association observedbetween indoor insecticide exposureand acute childhood leukemia.Although epidemiologic research islimited in identifying the associationbetween the adverse health outcomesin young children and pesticideuses in residential areas, the findingsfrom the present meta-analysis andthose previously published haveconsistently demonstrated
FIGURE 4Meta-analysis of the association between childhood cancers and exposure to residential outdoorpesticides during childhood.
PEDIATRICS Volume 136, number 4, October 2015 727 by guest on June 4, 2020www.aappublications.org/newsDownloaded from

associations between pesticideexposure and childhood cancers.While the research community isworking toward a betterunderstanding of the causality ofpesticides in various childhooddiseases, more and more pesticidesare being used in farming, inlandscape maintenance, and in thehome. Therefore, public healthpolicies should be developed tominimize childhood exposure to
pesticides in the home. States andlocal authorities can establishprograms, such as integrated pestmanagement, to minimizeresidential pesticide uses, especiallyindoor uses.47,48 In the meantime,parents, school and daycareteachers, and health care providerscan learn about common pesticidetypes and labeling information andcan stay aware of the short- andlong-term effects of these
chemicals.49,50 Every effort shouldbe made to limit children’s exposureto pesticides.
ABBREVIATIONS
AL: acute leukemiaCBT: childhood brain tumorCI: confidence intervalOR: odds ratio
FINANCIAL DISCLOSURE: The authors have indicated they have no financial relationships relevant to this article to disclose.
FUNDING: Supported by the Department of Energy and Environmental Protection, State of Connecticut (contract 042103580).
POTENTIAL CONFLICT OF INTEREST: The authors have indicated they have no potential conflicts of interest to disclose.
REFERENCES
1. Adgate JL, Kukowski A, Stroebel C, et al.Pesticide storage and use patterns inMinnesota households with children. JExpo Anal Environ Epidemiol. 2000;10(2):159–167
2. Bass JK, Ortega L, Rosales C, PetersenNJ, Philen RM. What’s being used athome: a household pesticide survey. RevPanam Salud Publica. 2001;9(3):138–144
3. Guha N, Ward MH, Gunier R, et al.Characterization of residential pesticideuse and chemical formulations throughself-report and household inventory: theNorthern California Childhood Leukemiastudy. Environ Health Perspect. 2013;121(2):276–282
4. Kim HH, Lim YW, Yang JY, et al. Health riskassessment of exposure to chlorpyrifosand dichlorvos in children at childcarefacilities. Sci Total Environ. 2013;444:441–450
5. Gilden R, Friedmann E, Sattler B, Squibb K,McPhaul K. Potential health effects relatedto pesticide use on athletic fields. PublicHealth Nurs. 2012;29(3):198–207
6. Alarcon WA, Calvert GM, Blondell JM,et al. Acute illnesses associated withpesticide exposure at schools. JAMA.2005;294(4):455–465
7. Faustman EM, Silbernagel SM, FenskeRA, Burbacher TM, Ponce RA.Mechanisms underlying children’ssusceptibility to environmental toxicants.Environ Health Perspect. 2000;108(suppl1):13–21
8. Sheets LP. A consideration of age-dependent differences in susceptibilityto organophosphorus and pyrethroidinsecticides. Neurotoxicology. 2000;21(1–2):57–63
9. Landrigan PJ, Claudio L, Markowitz SB,et al. Pesticides and inner-city children:exposures, risks, and prevention. EnvironHealth Perspect. 1999;107(suppl 3):431–437
10. Spann MF, Blondell JM, Hunting KL. Acutehazards to young children fromresidential pesticide exposures. Am JPublic Health. 2000;90(6):971–973
11. Infante-Rivard C, Weichenthal S.Pesticides and childhood cancer: anupdate of Zahm and Ward’s 1998 review.J Toxicol Environ Health B Crit Rev. 2007;10(1–2):81–99
12. Metayer C, Buffler PA. Residentialexposures to pesticides and childhoodleukaemia. Radiat Prot Dosimetry. 2008;132(2):212–219
13. Turner MC, Wigle DT, Krewski D.Residential pesticides and childhoodleukemia: a systematic review and meta-analysis. Environ Health Perspect. 2010;118(1):33–41
14. Van Maele-Fabry G, Lantin AC, Hoet P,Lison D. Residential exposure topesticides and childhood leukaemia:a systematic review and meta-analysis.Environ Int. 2011;37(1):280–291
15. Wigle DT, Turner MC, Krewski D. Asystematic review and meta-analysis of
childhood leukemia and parentaloccupational pesticide exposure. EnvironHealth Perspect. 2009;117(10):1505–1513
16. Zahm SH, Ward MH. Pesticides andchildhood cancer. Environ HealthPerspect. 1998;106(suppl 3):893–908
17. López-Cervantes M, Torres-Sánchez L,Tobías A, López-Carrillo L.Dichlorodiphenyldichloroethane burdenand breast cancer risk: a meta-analysisof the epidemiologic evidence. EnvironHealth Perspect. 2004;112(2):207–214
18. Merhi M, Raynal H, Cahuzac E, Vinson F,Cravedi JP, Gamet-Payrastre L.Occupational exposure to pesticides andrisk of hematopoietic cancers: meta-analysis of case–control studies. CancerCauses Control. 2007;18(10):1209–1226
19. Van Maele-Fabry G, Duhayon S, Lison D. Asystematic review of myeloid leukemiasand occupational pesticide exposure.Cancer Causes Control. 2007;18(5):457–478
20. Vinson F, Merhi M, Baldi I, Raynal H,Gamet-Payrastre L. Exposure topesticides and risk of childhood cancer:a meta-analysis of recentepidemiological studies. Occup EnvironMed. 2011;68(9):694–702
21. Meinert R, Kaatsch P, Kaletsch U,Krummenauer F, Miesner A, Michaelis J.Childhood leukaemia and exposure topesticides: results of a case–controlstudy in northern Germany. Eur JCancer. 1996;32A(11):1943–1948
728 CHEN et al by guest on June 4, 2020www.aappublications.org/newsDownloaded from

22. Stroup DF, Berlin JA, Morton SC, et al.Meta-analysis of observational studies inepidemiology: a proposal for reporting.Meta-analysis of Observational Studies inEpidemiology (MOOSE) group. JAMA.2000;283(15):2008–2012
23. Higgins JP, Thompson SG, Deeks JJ,Altman DG. Measuring inconsistency inmeta-analyses. BMJ. 2003;327(7414):557–560
24. Egger M, Davey Smith G, Schneider M,Minder C. Bias in meta-analysis detectedby a simple, graphical test. BMJ. 1997;315(7109):629–634
25. Metayer C, Colt JS, Buffler PA, et al.Exposure to herbicides in house dustand risk of childhood acutelymphoblastic leukemia. J Expo SciEnviron Epidemiol. 2013;23(4):363–370
26. Searles Nielsen S, Mueller BA, De RoosAJ, Viernes HM, Farin FM, Checkoway H.Risk of brain tumors in children andsusceptibility to organophosphorusinsecticides: the potential role ofparaoxonase (PON1). Environ HealthPerspect. 2005;113(7):909–913
27. Soldin OP, Nsouli-Maktabi H, GenkingerJM, et al. Pediatric acute lymphoblasticleukemia and exposure to pesticides[published correction appears in TherDrug Monit. 2009;31(5):668] Ther DrugMonit. 2009;31(4):495–501
28. Bailey HD, Armstrong BK, de Klerk NH,et al; Aus-ALL Consortium. Exposure toprofessional pest control treatments andthe risk of childhood acutelymphoblastic leukemia. Int J Cancer.2011;129(7):1678–1688
29. Buckley JD, Meadows AT, Kadin ME, LeBeau MM, Siegel S, Robison LL. Pesticideexposures in children with non-Hodgkinlymphoma. Cancer. 2000;89(11):2315–2321
30. Cooney MA, Daniels JL, Ross JA, BreslowNE, Pollock BH, Olshan AF. Householdpesticides and the risk of Wilms tumor.Environ Health Perspect. 2007;115(1):134–137
31. Daniels JL, Olshan AF, Teschke K, et al.Residential pesticide exposure andneuroblastoma. Epidemiology. 2001;12(1):20–27
32. Davis JR, Brownson RC, Garcia R, BentzBJ, Turner A. Family pesticide use andchildhood brain cancer. Arch EnvironContam Toxicol. 1993;24(1):87–92
33. Ding G, Shi R, Gao Y, et al. Pyrethroidpesticide exposure and risk of childhoodacute lymphocytic leukemia in Shanghai.Environ Sci Technol. 2012;46(24):13480–13487
34. Greenop KR, Peters S, Bailey HD, et al.Exposure to pesticides and the risk ofchildhood brain tumors. Cancer CausesControl. 2013;24(7):1269–1278
35. Infante-Rivard C, Labuda D, Krajinovic M,Sinnett D. Risk of childhood leukemiaassociated with exposure to pesticidesand with gene polymorphisms.Epidemiology. 1999;10(5):481–487
36. Leiss JK, Savitz DA. Home pesticide useand childhood cancer: a case–controlstudy. Am J Public Health. 1995;85(2):249–252
37. Ma X, Buffler PA, Gunier RB, et al. Criticalwindows of exposure to householdpesticides and risk of childhoodleukemia. Environ Health Perspect. 2002;110(9):955–960
38. Meinert R, Schüz J, Kaletsch U, Kaatsch P,Michaelis J. Leukemia and non-Hodgkin’slymphoma in childhood and exposure topesticides: results of a register-basedcase–control study in Germany. Am JEpidemiol. 2000;151(7):639–646,discussion 647–650
39. Menegaux F, Baruchel A, Bertrand Y, et al.Household exposure to pesticides andrisk of childhood acute leukaemia. OccupEnviron Med. 2006;63(2):131–134
40. Pogoda JM, Preston-Martin S. Householdpesticides and risk of pediatric braintumors. Environ Health Perspect. 1997;105(11):1214–1220
41. Rudant J, Menegaux F, Leverger G, et al.Household exposure to pesticides and
risk of childhood hematopoieticmalignancies: The ESCALE study (SFCE).Environ Health Perspect. 2007;115(12):1787–1793
42. Searles Nielsen S, McKean-Cowdin R,Farin FM, Holly EA, Preston-Martin S,Mueller BA. Childhood brain tumors,residential insecticide exposure, andpesticide metabolism genes. EnvironHealth Perspect. 2010;118(1):144–149
43. Urayama KY, Wiencke JK, Buffler PA,Chokkalingam AP, Metayer C, Wiemels JL.MDR1 gene variants, indoor insecticideexposure, and the risk of childhoodacute lymphoblastic leukemia. CancerEpidemiol Biomarkers Prev. 2007;16(6):1172–1177
44. Eden T. Aetiology of childhood leukaemia.Cancer Treat Rev. 2010;36(4):286–297
45. Kim AS, Eastmond DA, Preston RJ.Childhood acute lymphocytic leukemiaand perspectives on risk assessment ofearly-life stage exposures. Mutat Res.2006;613(2–3):138–160
46. Rossig C, Juergens H. Aetiology ofchildhood acute leukaemias: currentstatus of knowledge. Radiat ProtDosimetry. 2008;132(2):114–118
47. US Environmental Protection Agency.Integrated pest management (IPM) inschools. Available at: www.epa.gov/pesticides/ipm/. Accessed December 16,2014
48. US Centers for Disease Control andPrevention. Integrated pest management(IPM). Available at: www.cdc.gov/nceh/ehs/elearn/ipm.htm. Accessed March 6,2013
49. US Environmental Protection Agency.Pesticides: topical & chemical factsheets. Read the label first. Available at:www.epa.gov/pesticides/label/. AccessedMay 9, 2012
50. US Environmental Protection Agency.Citizen’s guide to pest control andpesticide safety. Read the label first. EPA735-K-04-002, March 2005. Available at:www.epa.gov/oppfead1/Publications/Cit_Guide/. Accessed, March 13, 2015
PEDIATRICS Volume 136, number 4, October 2015 729 by guest on June 4, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-0006 originally published online September 14, 2015; 2015;136;719Pediatrics
Mei Chen, Chi-Hsuan Chang, Lin Tao and Chensheng LuMeta-Analysis
Residential Exposure to Pesticide During Childhood and Childhood Cancers: A
ServicesUpdated Information &
http://pediatrics.aappublications.org/content/136/4/719including high resolution figures, can be found at:
Referenceshttp://pediatrics.aappublications.org/content/136/4/719#BIBLThis article cites 46 articles, 5 of which you can access for free at:
Subspecialty Collections
_subhttp://www.aappublications.org/cgi/collection/environmental_healthEnvironmental Healthfollowing collection(s): This article, along with others on similar topics, appears in the
Permissions & Licensing
http://www.aappublications.org/site/misc/Permissions.xhtmlin its entirety can be found online at: Information about reproducing this article in parts (figures, tables) or
Reprintshttp://www.aappublications.org/site/misc/reprints.xhtmlInformation about ordering reprints can be found online:
by guest on June 4, 2020www.aappublications.org/newsDownloaded from

DOI: 10.1542/peds.2015-0006 originally published online September 14, 2015; 2015;136;719Pediatrics
Mei Chen, Chi-Hsuan Chang, Lin Tao and Chensheng LuMeta-Analysis
Residential Exposure to Pesticide During Childhood and Childhood Cancers: A
http://pediatrics.aappublications.org/content/136/4/719located on the World Wide Web at:
The online version of this article, along with updated information and services, is
http://pediatrics.aappublications.org/content/suppl/2015/09/08/peds.2015-0006.DCSupplementalData Supplement at:
ISSN: 1073-0397. 60007. Copyright © 2015 by the American Academy of Pediatrics. All rights reserved. Print the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elk Grove Village, Illinois,has been published continuously since 1948. Pediatrics is owned, published, and trademarked by Pediatrics is the official journal of the American Academy of Pediatrics. A monthly publication, it
by guest on June 4, 2020www.aappublications.org/newsDownloaded from