Embed Size (px)
Citation preview

568
RESECTION WITH RESTORATION OFCONTINUITY IN THE TREATMENT OFCARCINOMA OF THE RECTUM AND
RECTOSIGMOIDJ. C. GOLIGHER, Ch.M., F.R.C.S.
Assistant Surgeon St. Mary's Hospital and St. Mark's Hospitalfor Diseases of the Rectum and Colon
The results of excision of the rectum for carci-noma by the modem abdomino-perineal operationare among the most gratifying in cancer surgery.In experienced hands the immediate operativemortality is certainly no greater than io per cent.even when the range of operability has beenbroadened to include fully 80 per cent. or more ofall the cases presenting for treatment, and of theoperation survivors approximately one-half arealive and well five years later. Yet the excellenceof these achievements is to some extent marredby the fact that all these patients are left with a
permanent colostomy. True, the average patientsoon learns to adapt himself to this disability andseldom suffers serious inconvenience or economichardship on account of it, but it is an exceptionalpatient who would not give a good deal to be ridof this unnatural and objectional state of affairs.Under the circumstances, though the surgeonmight wish to avoid a colostomy in these cases, itwould certainly not be justifiable to accept a
lowering of the prospect of complete eradicationof the disease in order to do so, and it would bemost deplorable if preservation of natural con-tinence were to be allowed to deflect the surgeonfrom his main objective of curing the patient.The problem, therefore, is whether retention
of the anal sphincter apparatus can ever be prac-tised without prejudicing the chances of radicalremoval of a rectal carcinoma. Obviously inmany cases this is absolutely impossible. Wherethe growth actually invades the sphincters or liesclose to them complete excision without sacrificeof the sphincter apparatus is quite out of thequestion. Likewise if the growth is situated inthe lower one-third or half of the rectum where itis supported laterally and posteriorly by thelevator muscles so that direct spread into these'structures may readily occur, it is undoubtedly
preferable that these muscles should be excisedtogether with the rectum by a formal combinedabdomino-perineal excision rather than conservedas in a sphincter-saving resection. But even if allthe carcinomata arising in the extraperitoneal partof the rectum (i.e. below the peritoneal reflection)are regarded as unsuitable for sphincter preserva-tion, this still leaves for consideration the intra-peritoneal growths, and, if to these are addedcarcinomata of the rectosigmoid, the number con-cerned is quite large. Thus in a recent analysis ofthe site of the growth in a consecutive series ofI,500 combined excision specimens at St. Mark'sHospital the writer found that in 713, or 47.5 percent., it lay entirely above the peritoneal reflectionin the intraperitoneal part of the rectum or in therectosigmoid (see Table i). Is it really necessaryto sacrifice the sphincter apparatus in dealingradically with these growths ?Some surgeons such as Rankin (1947), Allen
(1946) and Gabriel (1948) reply most emphaticallythat it is, and, as their authority for this state-ment, quote the classical researches of Miles(1910). It may be recalled that Miles (1910), onthe basis of a most careful examination of opera-tion specimens of rectal carcinoma, of recurrencesafter limited operations for this disease and ofpatients dying in the late stages of untreatedrectal cancer, came to the conclusion that with acarcinoma anywhere in the rectum, even whenquite early, lymphatic spread could take place inseveral different directions. These includedspread downwards to the pararectal glands on theback of the rectum below the growth, lateralwardsthrough glands on the levator muscles eventuallyto the internal iliac glands on the side wall of thepelvis, and upwards, not only along the maininferior haemorrhoidal and inferior mesentericvessels but also to the paracolic glands lying in the
by copyright. on July 27, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.27.313.568 on 1 Novem
ber 1951. Dow
nloaded from

November I95I GOLIGHER: The Treatment of Carcinoma of the Rectum 569
TABLE I
SITUATION OF GROWTH IN I,500 CONSECUTIVE COMBINED ExcISIoI4 SPECIMENS OF CARCINOMAOF THE RECTUM AND RECTOSIGMOID EXAMINED AT ST. MARK'S HOSPITAL, 1933-47.
D.istance of lower eklgeof growth from anus on Number of growths Percentage of growths Percentage of intra and
sigmoidoscopy at each level at each level extra peritoneal growths
Inchesi6 2
'5 --
14 2
13 512 7II 27 I.8o10 33 2.229 70 4.67 47-53 per cent.8 8I 5.40 intra-peritoneal7 I20 8.oo6 i6o I0.675 206 I3.67
InchesAverage site 4 205 I 3.67peritoneal 3 I98 13.20 52.47 per cent.reflection 2 i88 12.53 extra-peritoneal
- I 196 13J07N.B.-Up to 1947 it was customary at St. Mark's Hospital to perform a Paul-Mikulicz resection
and not a combined excision for growths situated more than I I in. from the anus hencethe small numbers found at higher levels ifi this series of combined excision specimens.
.
mesocolon on the marginal artery close to thesigmoid colon. To cope with all these possibleextensions obviously nothing short of the wideremoval of rectum and related structures providedfor in the now classical abdomino-perineal ex-cision devised by him would suffice, and his worktherefore left no place for sphincter preservationin the radical treatment of rectal cancer.
Subsequent workers, however, and notablyCuthbert Dukes (1930, 1940) and HeinrichWesthues (1930, I934) who have reinvestigatedthe mode of spread of rectal cancer as revealedby dissection of many hundreds of operativespecimens removed by perineal or combined ex-cision, paint a rather different picture. Theyagree with Miles in showing that the main avenueof lymphatic extension is upwards along thesuperior haemorrhoidal and inferior mesentericvessels, but find that the paracolic glands in thesigmoid mesocolon are seldom implicated. Asfor downward spread in the extramural lymphaticsbelow the level of the primary growth, this intheir experience is very rare except when theglands of the upgoing lymphatics are chokedwith carcinoma cells and the case is virtuallyincurable anyway. Lateral lymphatic spreadalong the levator muscles could not be verifiedas a rule because, contrary to the illustrations ofMiles (I926), excision specimens seldom contain
any glands in this region. Finally spread in therectal wall itself either by direct extension or inthe submucous lymphatic plexus is, except inhighly anaplastic growths, a very limited processseldom reaching more than 1.5 to 2 cm. beyondthe palpable edge of the primary carcinomatousulcer.
Their work then would suggest that in excisinggrowths of the upper half of the rectum-and evenmore so those of the rectosigmoid-it should notbe necessary to remove more than iI in. or so ofrectal wall and perirectal fat and lymphatics distalto the lower edge of the growth, nor to sacrificethe sigmoid colon and mesocolon extensively asrecommended by Miles. It may be considered tojustify, nay demand, a retrial of splhincter-savingoperations for these higher rectal and rectosigmoidgrowths. On the strength of these investigationsmany surgeons, including Pannett (I935), Bab-cock (I932, I940), Bacon (1945), Dixon (I939,I944) and Wangensteen (I943, 1945), have turnedtheir attention to this type of operation, and agroup of us at St. Mark's Hospital have also con-ceived it as our duty to test these operations inactual practice especially since the advent of sulphadrugs and antibiotics to minimize the risks ofsepsis. W have now treated some I46 cases bythese procedures and this paper is an account ofour experiences in their management.
by copyright. on July 27, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.27.313.568 on 1 Novem
ber 1951. Dow
nloaded from

POSTGRADUATE MEDICAL JOURNAL
Selection of Cases for Sphincter-SavingResectionsThe site of the growth has been the main
criterion in deciding on the suitability of a case fora sphincter-preserving excision. As already men-tioned, we consider that extraperitoneal growthsof the rectum call for a combined excision andshould not be treated by resection. We have,therefore, reserved resection for growths situatedat or above the level of the peritoneal reflectionoff the front of the rectum. Actually this reflec-tion is a rather variable landmark, but usually itlies about 8-io cm. on sigmoidoscopy or roughly asfar as the finger can feel on digital examinationof the rectum. We have, therefore, taken it as arule that growths lying at a lower level than this,which can easily be felt with the examining finger,are too low for resection.Not every growth above this level encountered
by the three or four surgeons contributing to thisseries of cases was in fact treated by resection. Allthe rectosigmoid growths and most of the intra-peritoneal rectal growths were, but the nearer thelesion lay to the peritoneal reflection the greaterwere the technical difficulties and sometimes thesemade it impossible to carry out a, resection. Thusirb a few cases a combination of a narrow pelvisand a bulky fat-laden sigmoid colon and meso-colon, rendering intrapelvic suturing difficult,decided us against a sphincter-preserving opera-tion. In some others the presence of a doublegrowth or marked diverticulosis necessitatingsacrifice of an unusually large amount of colonhas put resection with anastomosis out of court,and a combined excision has had to be performedinstead. With increasing experience of the tech-nique, however, we have less frequently beenbaulked by difficulties of this sort.
It should be emphasized that, at any rate forthe greater part of this series, no attempt has beenmade to follow the recommendation of GreyTurner (1935) and select for resection only thosecases adjudged clinically and at operation to havespecially early growths. We have rejected thispolicy for two reasons: firstly, because we areconvinced that it is impossible to decide, prior topathological examination of the excised specimen,how extensively any growth has spread, bitterexperience having shown us on many occasionsthat carcinomata which we thought were in avery early stage of development were in factassociated with extensive lymphatic metastases,and, secondly, because it implies that resectionoperations are procedures of less radical scopethan a formal combined excision. As we under-stand it, on theoretical grounds a resection shouldsecure as thorough an eradication of growthsof the upper rectum and rectosigmoid as an
abdomino-perineal excision, but if in practice itis demonstrated that it does not do so, then itshould be discarded entirely as a radical procedure.
Finally, special mention should be made of thecases with hepatic metastases. It has been ourpractice when operating on carcinomata of therectum and other parts of the gastro-intestinaltract to carry out palliative excision of the primarygrowth even when liver secondaries are present,provided that not more than a half of the liversubstance has been replaced by tumour tissue,because these patients often survive for twelvemonths or two years subsequently and theirsymptomatic condition in that remaining periodof life is enormously improved if the primarylesion has been removed. Obviously the pallia-tive value of excision in cases of this kind withrectal growths is greatly enhanced if it can becarried out as a resection without sacrifice of thesphincters. When we find, therefore, that hepaticdeposits are present in a case of carcinoma of therectum we make every effort to perform a resectionrather than an ordinary excision, stretching theindications to include rather lower growths thanwe would normally be prepared to accept forresection with a view to cure, and in consequenceshouldering much greater technical difficulties.
Choice of OperationSacral Resection. A very large number of resec-
tions of this type have been performed in Ger-many and Austria where owing to the advocacyof Kraske (I885), Hochenegg (i888, I889), Kiittner(1910, 1916) and Mandl (I932, 1945), this was formany years the most popular form of resectionfor rectal carcinoma in some of the leading sur-gical clinics, and Hochenegg and Kiittner alonewere responsible for nearly a thousand of theseoperations. We have not employed this methodbecause it has seemed to us an insufficientlyradical procedure in that, through a purely sacralwound, it is impossible to carry out a really highligation of the superior haemorrhoidal-inferiormesenteric vascular pedicle. It was for thisreason that the perineal excision of Lockhart-Mummery was quite properly abandoned at St.Mark's Hospital in favour of the combinedabdomino-perineal or perineo-abdominal opera-tion. In turning to resection operations, there-fore, it was logical that we should try to developmethods incorporating an abdominal phase topermit of adequate clearance of the upward-training lymphatic channels.
Abdomino-sacral Resection. This operation hasbeen extensively practised by Finsterer (I941),Goetze (x944), and d'Allaines (I950) and was thefirst method recommended by Pannett (1935).We have used it on only three occasions and
November 1 95570
by copyright. on July 27, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.27.313.568 on 1 Novem
ber 1951. Dow
nloaded from

GOLIGHER : The Treatment of Carcinoma of the Rectum
found that in all the patients the sacral woundbroke down to some extent, in two of themresulting in the formation of a fistula between thebowel and the skin, despite the fact that a pre-liminary transverse colostomy had invariably beenestablished to defunction the rectum. Finsterer(1941) and d'Allaines (1950) do not seem to havehad this trouble, but Goetze (i944) recognizes itas one of the main problems of this operation,and it is significant that Pannett (I95i) has nowgiven up this technique and gone over to a purelyabdominal resection.
Abdomino-anal Resection. The most popularoperation of this type is the .' pull through'operation of Babcock (I947) and Bacon (I945).In this procedure as usually practised the analmucosa is excised and the sphincter musclesdivided and resutured round the sigmoid colon,which has been drawn through the anus afterresection of the rectum. These manoeuvres,however, have the effect of damaging or com-pletely destroying the sensory and motor com-ponents of the delicate sphincter apparatus andas a consequence continence is grossly impaired.An examination of four patients operated on byother surgeons with this technique left us in nodoubt that after this operation patients are notusually properly continent but have really analcolostomies, and we did not feel that these func-tional results justified the use of this particulartechnique.An alternative method of performing abdomino-
anal excision which we have used in 26 cases isthat associated with the names of Maunsell (I892)and Weir (1901). Here after an abdominal dis-section the rectum is resected leaving a long colonstump and short ano-rectal stump. The latter isthen turned inside out through the anus so thatits cut upper margin becomes the projectinglower edge, and the colon stump is drawn downthrough it so that the free edges of both stumpslie opposite one another and can be suturedtogether outside the anus. Finally the anasto-mosis is returned through the anus. The surgeonis thus enabled to perform a very low resectionand anastomosis without a perineal or sacralwound, and without dividing the sphincters ordamaging the mucosa of the anal canal or lower,rectum. The functional results are accordinglyvery much better than after the Bacon-Babcockoperation, and, though a few of the patients havehad some difficulty in controlling flatus and liquidfaeces at first, the majority are fully continent.Our main criticism of this operation is that itrequires a particularly long piece of colon tostretch to the anal region and we have not-alwaysbeen able to manufacture a well vascularized colonatump of sufficient length, Also the colo-rectI!
anastomoses in these cases seem specially liableto break down in part, probably due to post-operative thrombosis in the vessels supplying thelong piece of colon.Abdominal or Anterior Resection. This is the
technique which we have chiefly ,employed, andfollowing the important papers of Wangensteen(1943, 1945) we have used it almost to the completeexclusion of other methods of resection. Accept-ing as we do only intra-peritoneal rectal and recto-sigmoid growths for resection, we find that we candeal with these growths perfectly satisfactorily byanterior resection without having to resort to anabdomino-sacral or -anal technique to completethe anastomosis. It is undoubtedly an advantageto be able to avoid these latter methods becauseafter the purely abdominal resection healing of theanastomosis is much more certain, and, due to thelarger rectal remnant left, the functional result 'isalways perfect. It is only very occasionally nowwhen doing a palliative resection for a ratherlower growth than usual that we find it necessaryto use the abdomino-anal technique. Altogether wehave treated I20 cases by anterior resection em-ploying the following technique with slightmodifications according to the individual surgeon.Technique of Anterior Resection
Pre-operative Care. The preparation of patientsfor anterior resection does not differ essentiallyfrom that employed for an ordinary combinedexcision. Loqally it is designed to clear thebowel of faeces retained above the growth, and tosterilize the gut contents by intestinal antiseptics.The former aim is secured as far as possible byadministration of aperients such as Milpar tosoften the faeces and assist in their expulsionthrough the carcinomatous stricture, and by twicedaily enemata or washes-out. It must be ad-mitted, however, that if the growth is completelyannular and tightly constricting, this mechanicalcleansing is often very ineffective even if prolongedover a period of a fortnight or three weeks insteadof the usual seven to ten days set aside for pre-paration of these cases. The intestinal antisepticused in most of our cases was sulphasuccidine(20 gm. daily in divided doses every four hours) orsulphathaladine (io gm. daily in divided doses) forfive to seven days, but more recently this has beensupplemented by streptomycin, i gm. orally b.i.d.for the last two or three days. Terramycin or aureo-mycin are perhaps even more effective- thanstreptomycin but they have not been readilyavailable to us. We have recently started usingchloromycetin and it may prove to be the bestdrug of all for this purpose.
In addition to this local preparation the patients'general condition is carefully assessed, and anaemia
November 195 I 57Iby copyright.
on July 27, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.313.568 on 1 N
ovember 1951. D
ownloaded from

POSTGRADUATE MEDICAL JOURNAL
and hypoproteinaemia are rectified by pre-operative blood transfusion and by high proteindiet supplemented by protein concentrates suchas Casilan. All patients are given vitamin Band C preparations as a routine to correct anyvitamin deficiency.
Operative Technique. We like to have the patientin the lithotomy-Trendelenburg position for thisoperation because, if the growth should be shownat laparotomy to be unsuitable for an anteriorresection, it is an easy matter with the patient sopositioned to change the operative procedure toan abdomino-anal resection or a synchronouscombined excision as required. Also in thisposition it is possible for the rectum to be washedout per anum during the course of the operationjust before it is divided below the growth, whichgreatly reduces the risks of soiling and dissemina-tion of loose carcinoma cells in the pelvis.The operation is perfQrmed through a long left
paramedian incision extending from the pubis toi4 in. above the umbilicus. The steps of thedissection follow those of the abdominal phase ofthe abdomino-perineal excision the rectum beingmobilized posteriorly, anteriorly and then laterallyas far almost as the anorectal ring. If, however,the growth is situated high in the rectosigmoid itis not necessary to separate the extraperitonealpart of the rectum from the sacral concavity or todivide the lateral ligaments. The inferior mesen-teric vessels are then tied and divided; it is usuallypossible to apply this ligature just below or abovethe origin of the first sigmoid artery. The sig-moid mesocolon is then divided obliquely fromthis point to the colon which is severed betweencrushing clamps, leaving proximally a stump ofsigmoid colon and mesocolon nourished by thefirst sigmoid or the descending branch of the leftcolic artery (Goligher, 1949). Attention is nowdirected to dividing the rectum i in. to 2 in.below the growth. As a preliminary the meso-rectum is separated from the back of the rectumat this level by blunt dissection and dividedbetween clamps. The bowel is thus bared allround for a segment of an inch or so. A curvedParker-Kerr crushing clamp is next applied to theupper limit of the bared zone, and about 4i in.below the growth, and an assistant then passes aproctoscope per anum, irrigates the closed-offlower compartment of the rectum with 1/500perchloride of mercury for five minutes and finallyswabs it dry. The operation is then continuedby applying another Parker-Kerr clamp just belowthe first one and dividing between them; thiscompletes the resection of the carcinomatoussegment of bowel.The clamps holding the colon and rectal stumps
are now approximated and a posterior row of
Lembert sutures of fine interrupted Deknatelinserted. The clamps are. then removed, thecrushed edges of rectum and colon trimmed off,and a continuous through and through stitch offine No. 2/0 chromic catgut, mounted on a smallhalf circle atraumatic needle on a needle holder,inserted between the colon and rectum, the pos-terior half being introduced as a simple over andover stitch, the anterior as a Connell stitch tosecure good inversion of the mucosa. Theanastomosis is completed by an anterior row ofLembert sutures of fine Deknatel. Finally thepelvic peritoneum is stitched to the colon 2 or 3 in.above the bowel suture line, which has the effectof placing the entire anastomosis below the peri-toneum. The extraperitoneal pelvic space isdrained extraperitoneally by a strip of corrugatedrubber taken out below the reflection of pelvicperitoneum at the side of the bladder and throughthe lower end of the main paramedian wound.Penicillin sulphonamide powder is dusted locallyaround the anastomosis. The abdomen is closedin layers usually with nylon or stainless steel wire.
In our earlier cases a preliminary transversecolostomy was created two or three weeks beforethe main resection and irrigations and sulpha-succidine suppositories given into the distal limbdaily to cleanse and sterilize the left half of thecolon and rectum. Then for a time we made itour practice to establish the colostomy just at theend of the main resection operation to protect theanastomosis from undue strain, but more recentlyand for quite the majority of our cases, a colos-tomy has been avoided entirely with apparentlyno greater incidence of serious complications. Atthe present time we reserve transverse colostomyfor the few cases where the anastomosis hasproved exceptionally difficult or the colon hasbeen unduly loaded. Also in three cases, wherea simultaneous Wertheim's hysterectomy wasperformed with anterior resection of the rectum,a transverse colostomy was established to lessenthe risk of a rectovaginal fistula developing if thebowel suture line should break down. In thecases not having colostomy we used to pass arectal tube from the anus into the sigmoid colon,the point of the tube being guided through theanastomosis by the operator before the abdomenwas shut. This was retained for four or five days.Alternatively the anal sphincters were vigorouslystretched to paralyse them and prevent the accu-mulation of flatus in the rectum under tension.But in most cases now these steps are all omitted.With suitably long retractors, scissors, needle-
holders and other instruments and experience ofthe technique this is not a difficult operation, butit does usually take a little longer to completethan the average synchronous combined excision.
Novuember I951572by copyright.
on July 27, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.313.568 on 1 N
ovember 1951. D
ownloaded from

GOLIGHER : The Treatment of Carcinoma of the Rectum
Our anaesthetists and registrars, however, areunanimous in their opinion that the condition ofthe patients at the end of these operations is dis-tinctly better than after a formal combinedexcision, presumably because of the avoidance ofthe haemorrhage and shock associated with theperineal phase of the latter procedure.
Post-operative Care and Complications. Blood isadministered during and after operation asrequired, and an intravenous infusion of saline ordextrose water is usually continued for two orthree days, till flatus is passed or peristalticsounds return to normal. As mouth feeds aregradually built up and light diet is resumed thebowels usually act spontaneously about the fourthor fifth day. A routine in all these cases is, ofcourse, chemotherapy with oral or intramuscularsulphamezathine i gm. four-hourly, penicillin500,000 units b.d., and intramuscular strepto-mycin 0.5 gm. b.i.d. In addition, when thecolon is sectioned at operation a sample of thefaeces is cultured for any organism surviving thepre-operative intestinal antisepsis and the sensi-tivity of such organisms to various antibiotics isdetermined as a guide to further treatment ifrequired.The suprapubic drain is left in situ for at least
five days. There is often a good deal of dis-charge of blood-stained fluid along it for the firstday or so, later this dries up or may becomeslightly purulent or, in about one case in twelve,frankly faecal, indicating that the suture line inthe bowel has broken down. However, even if afaecal fistula should occur this nearly alwayscloses spontaneously in io to 14 days and onlyrarely has it been necessary to establish a tem-porary transverse colostomy to get it to close.
If the suture line in the bowel is gently pal-pated or inspected sigmoidoscopically at the endof a week, it is found in about one case in six tohave broken down at some point on its circum-ference, usually the posterior third, and the rectallumen then communicates with an extrarectalpresacral cavity. Only in about a half of thesecases does faeces escape suprapubically, and inany event the defect rapidly closes so that at theend of two-and-a-half or three weeks it is repre-sented only by a slight dimple on the suture line.
If a transverse colostomy has been made anenterotome is applied to the colostomy spur at theend of io to I4 days, provided that the tempera-ture has returned to normal and there is noevidence of gross pelvic sepsis. When the spurhas been completely obliterated the colostomyopening is finally closed extraperitoneally.One of the striking and unexpected features
about the convalescence from these operations hasbeen the relative freedom from serious sepsis,
which is presumably due in part to the use ofantibiotics. In four cases, however, pelvic ab-scesses did develop; these discharged into thelumen of the rectum through the bowel sutureline or suprapubically, and one burst into thevagina as well giving the patient a temporaryrecto-vaginal fistula which fortunately closedspontaneously.
Another impressive thing about these cases hasbeen the fact that, though there is often consider-able narrowing at the suture line at the conclusionof the operation, this never results in a permanentorganic stenosis. Actually, if the patients arere-examined at the end of three months, thoughthe lumen has opened up considerably, the sutureline is still evident as a slight fibrous constriction,but on further examination after another six ortwelve months no narrowing usually remains andit may indeed be difficult to identify the colo-rectal junction with confidence. Therefore, nospecial operative technique or post-operativedilatation is required to guard against stenosis;the patients' own faeces are a sufficient dilator.As already mentioned, after anterior resection
even when this is carried as low as is technicallyfeasible, the patients invariably enjoy perfectcontrol of flatus and faeces, but owing to theloss of part of the sigmoid colon in which faecesare normally accommodated, more frequentmotions are required, usually two or three a dayat least.
Operative MortalityEleven of the I20 cases subjected to anterior
resection died and also one of the 26 patientstreated by abdomino-anal excision, giving anoverall majority of I2 or 8.2 per cent. in a total of146 sphincter-saving resections. This com-pares satisfactorily with the current immediatemortality rate for combined excision in St. Mark'sHospital of approximately 7 per cent. The causesof death are shown in Table 2. It should beespecially noted that only two cases died of sepsis.
TABLE 2
CAUSES OF OPERATION DEATHS AFTER ANTERIOR ORABDOMINO-ANAL RESECTION
Shock .. .. ..
Coronary occlusion ..Paralytic ileus and cardiac failurePerforated gastric or duodenal ulcer ..
Pulmonary embolus .. .Peritonitis ..Intestinal obstruction and bronchitis ..
Pelvic abscess .. ..Post-operative jaundice
.. 2 cases
.. I case
.. I ,I
.. 2 cases
.. I case
.. I ,,
.. I ,,
. . I ,,
.. 2 cases
12 cases
D1
November 1951by copyright.
on July 27, 2020 by guest. Protected
http://pmj.bm
j.com/
Postgrad M
ed J: first published as 10.1136/pgmj.27.313.568 on 1 N
ovember 1951. D
ownloaded from

574 POSTGRADUATE MEDICAL JOURNAL November 1951
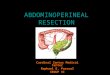
ORIGINAL RESECTION SPECIMEN
4,
FIG. I.
0>
/
t.
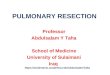
\l)FIG. 2.-Recurrence (?) fresh primary growthdeveloping three years and nine monthsafter anterior resection for carcinomarecti. The second growth arose in theampulla of the rectal stump posteriorlyjust below the colo-rectal suture line.
FURTHERGROWTHREMOVEDBYCOMBINEDEXCISION31 YEARSLATER.
by copyright. on July 27, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.27.313.568 on 1 Novem
ber 1951. Dow
nloaded from

November 1951 GOLIGHER : The Treatm.ent of Carcinoma of the Rectum 575
Late ResultsWhile the immediate results of these resection
operations have been most encouraging, it must beadmitted frankly that the remote results havecaused disappointment. Of the I34 cases treatedby anterior resection, already II have developedlocal recurrences, and as most of these operationswere performed in the last three or four yearsfurther recurrences may reasonably be expectedin the more recently treated cases. A detailedreport on these recurrences and others is beingmade by the writer in conjunction with CuthbertDukes and H. J. R. Bussey (195I). It suffices tosay here that usually the recurrence appeared in thebowel wall, most often at the site of the anastomosis,sometimes in the rectal stump as in Fig. 2. Theyhave appeared at any time from three or fourmonths to six or seven years after. It is quitepossible that some of them may be fresh primarygrowths, whilst others may be due to implantationon the suture' line of loose carcinoma cells mixedwith the faeces in the lumen of the rectum, hencethe precautions which we now take to cleanse therectum with perchloride of mercury beforedividing it. But presumably many of them areordinary recurrences due to inadequate removal.Before condemning the operation, however, it isimportant to realize that local recurrences are alsosometimes found after ordinary combined excision,and, owing to the greater difficulty of demon-strating them clinically in these cases are probablypresent more frequently than is generally imagined.
We do, of course, know the results of thecombined excision in terms of five-year survivalrate but similar figures cannot yet be worked outfor anterior resection, and three or four years willhave to elapse before this comparision can bemade. It will be seen, therefore, that sufficientdata are not yet available to enable one to deter-mine the precise value of these resection operationsin the treatment of carcinoma of the upper rectumand rectosigmoid. The most that one can say atthe moment is that they are excellent palliativeprocedures for patients with growths in eitherof these situations who are having an excisiondone in the presence of hepatic metastases(and who represent approximately io percent. of the cases having rectal excision done atSt. Mark's Hospital). It is highly likely thatresection will retain its place in the managementof these incurable cases because even if localrecurrences should develop subsequently thepatients will probably succumb from their liversecondaries before the local recurrence causesserious symptoms. But for other cases the claimsof this operation to be considered as a radicalprocedure on a par with the orthodox combinedexcision remain to be substantiated.The writer is greatly indebted to his colleagues
at St. Mark's Hospital for kindly permitting himto include their cases in this survey. He alsowishes to record his thanks to the British EmpireCancer Campaign a grant from which defrayedsome of the expenses involved in this work.
BIBLIOGRAPHY
ALLEN, A. W. (1946), Surg. Gynec. & Obstet., 82, 490.BABCOCK, W. W. (I932), Ibid., 55, 627.BABCOCK, W. W. (1940), in ' The Treatment of Cancer and Allied
Diseases,' by G. T. Pack and E. M. Livingstene, New York,P. Hoeber, 1513.
BABCOCK, W. W. (1947), Surg. Gynec. & Obstet., 85, i.BACON, H. (i945), Ibid., 8x, 113.D'ALLAINES (1950), Proc. Roy. Soc. Med., 43, 697.DIXON, C. F. (1939), Anter. J. Surg., 46, 12.DIXON, C. F. (I944), Surgery, 15, 367.DUKES, C. E. (1930), Brit. J. Surg., 17, 643.DUKES, C. E. (1940), J. Path., 50, 527.FINSTERER, H. (I941), Arch. f. klin Chir.. 202, 15.GABRIEL, W. B. (1948), 'The Principles and Practice of Rectal
Surgery,' 4th edition, H. & K. Lewis, London.GOETZE, O. (I944), Arch. f. k'n. Chir., 2o6, 293.GOLIGHER, J. C. (1949), Brit. J. Surg., 37, I57.GOLIGHER, J. C., DUKES, C. E., and BUSSEY, H. J. R. (x951).
Brit. J. Surg. (in the press).HOCHENEGG, J. (I888), WTien klin. Wschr., 1, 254, 272, 290, 309,
324, 348.HOCHENEGG, J. (1889), Ibid., i, 578.
KRASKE, P. (I885), Verlhndl. d. deutsch. Gesellsch. f. Chir., Bert.,14, P. 2, 464.
KUTTNER, H. (I9Io), Deutsch Med. Wschr., 36, 606.KUTTNER, H. (1916), Zbl. Chir., 43, 905.MANDL, F. (1932), Ibid., 394.MANDL, F. (1945), Surgery, I8, 318.MAUNSELL, H. W. (I892), Lancet, 2, 473.MILES, W. E. (I9IO), Brit. Med. Journal, 2, 940.MILES, W. E. (1926), 'Cancer of the Rectum,' Harrison & Sons,London.PANNETT, C. A. (I935), Lancet, 2, 423.PANNETT, C. A. (195I), personal communication.RANKIN, F. W. (1947), Ann. Surg., 126.TURNER, G. GREY (1935), Proc. Roy. Soc. Med., 28, 559.WANGANSTEEN, O. H. (I943), Surgery, 14, 403.WANGANSTEEN, 0. H. (I945), Surg. Gynec. & Obstet., 81, x.WEIR, R. F. (I9o0), J.A.M.A., 37, 8oi.WESTHUES, H. (1930), Arch. f. klin. Chir., x16, 582.WESTHUES, H. (1934), ' Die Pathologish-Anatomischen Grund-
lagen der Chirurgie des Rectumkarzinoms,' Georg ThiemeVerlag, L.'- zig.
D2
by copyright. on July 27, 2020 by guest. P
rotectedhttp://pm
j.bmj.com
/P
ostgrad Med J: first published as 10.1136/pgm
j.27.313.568 on 1 Novem
ber 1951. Dow
nloaded from