Embed Size (px)
Citation preview

RESECTION OF PAPILLARY TRANSITIONAL CELL CARCINOMA USING ENDOSCOPIC SNARE
SIMON CHUNG, M.D. ARNOLD M. KWART, M.D.
From the Department of Urology, The George Washington University Medical Center, Washington, D.C.
ABSTRACT-We describe a method to remove papillary transitional cell carcinoma of the bladder using an adapted colonoscopic snare for transurethral electroresection. This method permits safe and accurate resection of papillary bladder tumors without the com- plications associated with the use of the resectoscope.
Papillary transitional cell carcinoma of the blad- der particularly when large can present a thera- peutic challenge to the endoscopist. Bleeding, bladder perforation, injury to the ureteral orifices, and induction of the obturator reflex are recog- nized complications associated with transurethral resection of bladder tumors. We present our ini- tial experience with a transurethral endoscopic snare which facilitates tumor resection, may re- duce surgical morbidity, and may allow more con- cise pathologic staging. Although the actual inci- dence of complications in a modern series is not known, we encountered no complications in our patients.
MATERIAL AND METHODS
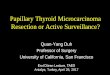
We modified an existing colonoscopy snare for cystoscopic use (Cook Urological) (Fig. 1). Our endoscopic snare consists of a conductive hexago- nal metal wire, 0.015 inch in diameter, encased in a sliding semirigid nonconductive Teflon sheath. The snare could be opened to a 5cm diameter and retracted by a hand-held slide mechanism which is connected to an electrosurgical unit. The tip of the snare is capped by a bulbous tip to allow quick and convenient point fulguration. The 7-F prototype snare is designed to pass easily through the working port of a cystoscope.
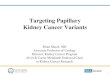
Under direct endoscopic vision with the bladder partially filled, the tumor is localized and its stalk identified. The snare is opened and manipulated with the cystoscope to encompass the bulk of the tumor (Fig. 2). The snare is then closed and
Submitted: April 2, 1993, accepted (with revisions):June 7, 1993
FIGURE 1. Adaptation of colonoscopy snare for cys- toscopic use,
secured tightly around the tumor at its junction with the bladder wall. Thirty-five watts of power can be delivered as a coagulating or cutting cur- rent through the snare. This is similar to the power levels used in colonoscopic polypectomy. A brief interval of coagulative current is applied fol- lowed by cutting current with gentle retraction of the snare loop into the sheath (Fig. 3). If bleeding followed, spot coagulation could be applied through the bulbous tip. Irrigation removed the relatively intact intraluminal component of the tumor. The tumor base is easily identified for deep biopsy by cold cup or resection.
RESULTS
Utilizing the endoscopic snare, 5 patients un- derwent tumor resection for a total of eight tu- mors ranging from 1 to 5 cm in diameter located
440 UROLOGY / OCTOBER 1993 / VOLUME 42, NUMBER 4

FIGURE 2. Drawing showing open snare encompass- ing bulk of tumor in bladder.
on the lateral, posterior, trigonal, and bladder neck surfaces of the bladder. Each tumor was suc- cessfully treated in a remarkably clear operative field by the described method followed by cold cup biopsy of the residual bases. We did not en- counter bleeding, bladder perforation, or obtura- tor reflex contractions. Tumors near the ureteral orifices were removed without ureteral trauma. Snare bladder tumor removal with deep bladder wall biopsy removed all tumors completely. Elec- trical artifact was minimal and did not interfere with pathologic interpretation and staging.
Two tumors deserve particular note. A 5cm tumor on the right ureteric ridge prevented identi- fication of the right ureteral orifice. Resection with the endoscopic snare at the tumor stalk re- sulted in a hemostatic 3-mm base with several residual papillary fronds, but the orifice was left undistorted. The residual tumor and base easily underwent biopsy without endangering the in- tegrity of the ureteral orifice. The tumor was re- moved in one piece with an Elik bulb evacuator. In another patient, a 2-cm tumor situated on the right lateral wall overlying the area of the obtura- tor nerve was resected with slight obturator nerve stimulation during application of electrocautery and the residual base was easily visualized and biopsy was done by cold cup.
FIGURE 3. Drawing shows retraction of snare loop into sheath.
COMMENT
Complications of transurethral resection of bladder tumors include bleeding, perforation, and damage to the ureteral orifices. Bleeding is com- monly encountered with electroresection particu- larly with larger tumors when the base is not eas- ily visualized. Bleeding obscures visualization (even at slow rates of bleeding) and if not con- trolled can result in prolonged resection time, per- foration, and hemorrhage requiring transfusion. Perforation can occur from poor visualization, in- accurate assessment of bladder thickness, and unanticipated obturator nerve stimulation. Unin- tentional resection of a ureteral orifice results
UROLOGY / OCTOBER 1993 / VOLUME 42, NUMBER 4 441

from poor visualization or inaccurate resection and may produce ureteral obstruction or a reflux- ing vesicoureteral junction which is not ideal in patients with transitional cell carcinoma of the bladder.
The endoscopic snare reduces the risk of com- plications by allowing quick simple resection di- rectly at the tumor stalk. The tumor stalk is cut flush with the surrounding urothelial surface making perforation unlikely even when per- formed adjacent to the obturator nerve. Initial re- section at the tumor stalk is seldom technically feasible with the resectoscope. Because minimal cutting is performed and electrocautery is used, bleeding is minimized and visualization opti- mized. The resection is precise and produces a less fragmented specimen. The residual tumor
442
base is usually well-preserved and biopsy can be done easily. Less burn artifact facilitates more ac- curate assessment of tumor invasion.
Our experience indicates that the endoscopic snare is quick and simple to use. It may reduce the risk of major complications of transurethral resection of bladder tumors. It is a technique well known to other surgeons and endoscopists which is adapted easily to removal of papillary tumors of the bladder. The technique of snare removal is adaptable to upper urinary tract resection of urothelial tumors. Resection by endoscopic snare is a viable alternative for papillary tumor removal.
Arnold M. Kwart, M.D. 2021 K St., N.W, #408
Washington, D.C. 20006
UROLOGY / OCTOBER 1993 / VOLUME 42, NUMBER 4