Embed Size (px)
Citation preview

Rehabilitation After Hallux ValgusSurgery: Importance of PhysicalTherapy to Restore Weight Bearing ofthe First Ray During the Stance PhaseReinhard Schuh, Stefan G. Hofstaetter, Samuel B. Adams Jr, Florian Pichler,Karl-Heinz Kristen, Hans-Joerg Trnka
Background. Operative treatment of people with hallux valgus can yield favor-able clinical and radiographic results. However, plantar pressure analysis has dem-onstrated that physiologic gait patterns are not restored after hallux valgus surgery.
Objective. The purpose of this study was to illustrate the changes of plantarpressure distribution during the stance phase of gait in patients who underwenthallux valgus surgery and received a multimodal rehabilitation program.
Design. This was a prospective descriptive study.
Methods. Thirty patients who underwent Austin (n�20) and scarf (n�10) os-teotomy for correction of mild to moderate hallux valgus deformity were included inthis study. Four weeks postoperatively they received a multimodal rehabilitationprogram once per week for 4 to 6 weeks. Plantar pressure analysis was performedpreoperatively and 4 weeks, 8 weeks, and 6 months postoperatively. In addition,range of motion of the first metatarsophalangeal joint was measured, and the Amer-ican Orthopaedic Foot and Ankle Society (AOFAS) forefoot questionnaire was ad-ministered preoperatively and at 6 months after surgery.
Results. The mean AOFAS score significantly increased from 60.7 points (SD�11.9) preoperatively to 94.5 points (SD�4.5) 6 months after surgery. First metatar-sophalangeal joint range of motion increased at 6 months postoperatively, with asignificant increase in isolated dorsiflexion. In the first metatarsal head region,maximum force increased from 117.8 N to 126.4 N and the force-time integralincreased from 37.9 N�s to 55.6 N�s between the preoperative and 6-month assess-ments. In the great toe region, maximum force increased from 66.1 N to 87.2 N andthe force-time integral increased from 18.7 N�s to 24.2 N�s between the preoperativeand 6-month assessments.
Limitations. A limitation of the study was the absence of a control group due tothe descriptive nature of the study.
Conclusions. The results suggest that postoperative physical therapy and gaittraining may lead to improved function and weight bearing of the first ray after halluxvalgus surgery.
R. Schuh, CM, is Research Fellow,Gait Analysis Laboratory, Foot andAnkle Center Vienna, Alserstrasse43/8D, 1080 Vienna, Austria. Ad-dress all correspondence to MrSchuh at: [email protected].
S.G. Hofstaetter, MD, is SeniorResident, Department of Ortho-paedic Surgery, Klinikum Wels-Grieskirchen, Grieskirchnerstrasse43, Wels, Austria.
S.B. Adams Jr, MD, is Senior Resi-dent, Division of Orthopaedic Sur-gery, Duke University MedicalCenter, Durham, North Carolina.
F. Pichler, PT, is affiliated with Footand Ankle Center Vienna.
K.-H. Kristen, MD, is Senior Sur-geon, Foot and Ankle CenterVienna.
H.-J. Trnka, MD, PhD, is AssociateProfessor of Orthopaedic Surgery,Foot and Ankle Center Vienna.
[Schuh R, Hofstaetter SG, AdamsSB Jr, et al. Rehabilitation after hal-lux valgus surgery: importance ofphysical therapy to restore weightbearing of the first ray during thestance phase. Phys Ther. 2009;89:934–945.]
© 2009 American Physical TherapyAssociation
Research Report
Post a Rapid Response orfind The Bottom Line:www.ptjournal.org
934 f Physical Therapy Volume 89 Number 9 September 2009

Hallux valgus deformity remainsone of the most common anddisabling pathologies of the
foot. A myriad of potential thera-peutic interventions have been de-scribed for treating people withsymptomatic hallux valgus, includ-ing bracing, soft-tissue procedures,and a number of different osteoto-mies.1–3 The purpose of operativecorrection of the deformity by anosteotomy of the first metatarsal is toreduce the malalignment of the firstray, thereby restoring its function inweight bearing and ambulation.4 Op-erative correction has yielded goodto excellent results.5–12
However, recent plantar pressuredistribution analyses indicate that,despite improvement of clinical andradiographic parameters, restorationof function of the first ray and greattoe does not occur.8,13–17 Kernozekand Sterikker17 found decreased1-year peak pressures and force-timeintegrals (impulse) in the great toeregion compared with the preopera-tive values. They concluded thatphysical therapy may help to restoregreat toe function after the Austinprocedure. In a prospective pressuredistribution study, Bryant et al13
found decreased load beneath thehallux 1 year after the Austin proce-dure compared with preoperativelevels. They did not find any changes
of plantar pressure parameters onthe second, third, and fourth meta-tarsals after surgery. Guesgen et al18
reported that, at a mean of 3 yearsafter chevron osteotomy, 56% ofthe patients did not use their greattoe for push-off. Jones et al8 founddecreased peak pressures 20 monthsafter scarf osteotomy in the region ofthe first metatarsal head comparedwith the preoperative values. Dhuka-ram et al15 found decreased loadunder the hallux after scarf andMitchell osteotomies compared withindividuals with absence of any footpathology.
Because the first ray is the mostheavily loaded structure of the footduring gait, proper weight bearing isessential for physiologic gait pat-terns.19,20 Lateral deviation of the greattoe and subluxation of the sesamoidsrepresent pathomorphologic charac-teristics of hallux valgus deformity.21
These changes alter kinematics ofthe first metatarsophalangeal (MTP)joint, leading to reduced strength(force-generating capacity) of theplantar flexors.22 Plantar pressurestudies revealed that the great toeassumes a diminishing role in weightbearing of the forefoot. In additionto the lateral transfer of forces, thecenter of pressure shifts lat-erally.23–25 Therefore, several au-thors26–28 have mentioned decreasedweight bearing of the great toe dur-ing gait as the reason for lesser toemetatarsalgia. The results of plantarpressure distribution assessments per-formed after hallux valgus surgerysuggest that structural correction ofthe pathobiomechanics alone is notsufficient to restore forefootfunction.8,13,15,16–18
Postoperative physical therapy is awell-established method to restorefunction after surgical interventionfor disorders of the musculoskeletalsystem. The benefits of postoperativephysical therapy have been reportedfor nearly all orthopedic surgery
subspecialties.29–33 More applicableto this report, it has been shownthat postoperative physical therapyfor hindfoot surgical proceduresimproves postoperative function.34
However, there is a paucity of liter-ature describing the effect of physi-cal therapy on the functional out-come of forefoot surgery. Shamus etal35 reported good functional im-provement in patients with halluxlimitus when they underwent a spe-cial physical therapy program includ-ing sesamoid mobilization, flexorhallucis muscle strengthening, andgait training. These results indicatethat physical therapy and gait train-ing help to restore physiologic kine-matics in the affected first MTP joint.Therefore, we hypothesized thatphysical therapy would improvefunction following surgical correc-tion of symptomatic hallux valgus.
The purpose of this prospective de-scriptive study was to illustrate thechanges of plantar pressure distribu-tion during the stance phase of gaitin patients who underwent halluxvalgus surgery and received a multi-modal rehabilitation program.
MethodParticipantsProspective participants were re-ferred to the study by a fellowship-trained foot and ankle surgeon onthe basis of mild to moderate halluxvalgus deformity without radio-graphic signs of osteoarthritis of thefirst MTP joint. Between October2006 and December 2007, 30 pa-tients were included in this study. Allpatients complained of pain in theregion of the first MTP joint. Demo-graphics of the participants areshown in Table 1. None of the par-ticipants had evidence of lower-extremity malalignment (eg, genuvalgum, genu varum) or any otherpathologic conditions on the muscu-loskeletal system that might influ-ence gait patterns (eg, low backpain; disk herniations; spondyloar-
Available WithThis Article atwww.ptjournal.org
• eAppendix: RehabilitationProgram After Hallux ValgusSurgery
• The Bottom Line clinicalsummary
• The Bottom Line Podcast
• Audio Abstracts Podcast
This article was published ahead ofprint on July 16, 2009, atwww.ptjournal.org.
Rehabilitation After Hallux Valgus Surgery
September 2009 Volume 89 Number 9 Physical Therapy f 935

thritis or osteoarthritis of the hip,knee, ankle, subtalar, transverse tar-sal, or Lisfranc joints).
The operations were performed by asingle surgeon (H.J.T.), as previouslydescribed by Kristen et al9 and Trnkaet al,12 in an ambulatory surgery cen-ter setting. Briefly, the Austin osteot-omy is a distal V-shaped osteotomyof the first metatarsal combined witha release of the contractile aspects ofthe lateral joint capsule of the MTPjoint.36 The operative area is ex-plored through a median skin inci-
sion at the medial aspect of the firstMTP joint, as well as a dorsal skinincision at the first web space. TheV-shaped osteotomy is performedwith a sagittal oscillating saw, andafterward the distal fragment isshifted laterally to realign the firstmetatarsal. In the present study, fix-ation was performed by inserting anoblique compression screw (Char-lotte Multi Use Compression Screw*)from dorsomedial to plantarlateral.
The scarf osteotomy is a diaphysealZ-shaped osteotomy of the firstmetatarsal shaft.7–9,37,38 The opera-tive area is explored through thesame incisions as described for theAustin osteotomy. The osteotomyis performed using the oscillatingsaw. Correction of the deformity isprovided by pushing the distal frag-ment laterally. Fixation was per-formed with the same screw used forthe Austin osteotomy. This screwwas inserted in a dorsal to plantardirection.
Participants underwent the scarfosteotomy when their intermeta-tarsal angle was more than 16 de-grees and underwent the Austinosteotomy when it was less than 16degrees. The intermetatarsal angleis measured on weight-bearinganterior-posterior radiographs of thefoot. The intermetatarsal angle wasdetermined from the longitudinalaxes of the first and second metatar-sals. This angle is the main indicatorof the degree of the deformity.3,21,39
To avoid the specific influence of asingle surgical method, patients withboth operations were included inthis study.
MeasurementsPrior to collecting data, all partici-pants signed an informed consentform approved by the Foot and An-kle Center Vienna Institutional Re-
view Board. The rights of the partic-ipants were protected all the times.
All measurements were taken byan independent observer who wasneither the operating surgeon nora physical therapist. The measure-ments included pedobarographicanalysis and functional assessmentusing the metatarsophalangeal-interphalangeal score of the Ameri-can Orthopaedic Foot and AnkleSociety (AOFAS), as well as measure-ments of range of motion (ROM)of the first MTP joint according tothe criteria of the AOFAS.39,40 TheAOFAS score and ROM of the firstMTP joint were evaluated preopera-tively and 6 months after surgery.Plantar pressure analyses were per-formed preoperatively and 4 weeks,8 weeks, and 6 months after surgery.
Plantar Pressure AnalysisThe plantar loading parameters wereassessed using a capacitive pressuremeasurement platform (emed-at plat-form†). The platform has a total areaof 610 � 323 mm enclosing a 240- �380-mm sensor area. It includes atotal of 1,760 sensors, providing aresolution of 2 sensors per squarecentimeter. The sampling rate ofthe platform was fixed at 60 Hz andautomatically triggered upon firstcontact. The pressure threshold is10 kPa, with plantar pressures rang-ing up to 1,270 kPa. The platformhas a maximum measurable force of67,000 N, with a hysteresis of �3%.Because of the 18-mm depth of theplatform, the test arrangement en-closed the whole platform in thecenter of a polyethylene ramp with alength of 7 m. Participants were ableto cross the platform in both direc-tions. The validity, reliability, and re-peatability of the EMED system† havebeen investigated previously.41–43
According to Hughes et al,41 the co-efficients of reliability (Pearson r)
* Wright Medical Technology Inc, 5677 Air-line Rd, Arlington, TN 38002.
† Novel GmbH, Ismaniger Strasse 51, 81675Munich, Germany.
Table 1.Demographic Characteristics of theParticipants (N�30)
Characteristic Measurement
Sex
Male 2
Female 28
Type of osteotomy
Austin 20
Scarf 10
Age (y)
X 58.4
SD 13.8
Range 22–79
Height (cm)
X 166.3
SD 0.1
Range 152.0–178
Weight (kg)
X 64.8
SD 8.9
Range 49–88
Body mass indexa
X 23.4
SD 2.9
Range 17.8–31.6
Foot size (French)
X 38.5
SD 1.3
Range 36–42
a Body mass index calculated as weight inkilograms divided by the square of the height inmeters.
Rehabilitation After Hallux Valgus Surgery
936 f Physical Therapy Volume 89 Number 9 September 2009

range from .914 to .988 for the pa-rameters that were evaluated in thepresent study if 5 steps are recorded.In order to provide valid and reliableresults, the mid-gait method waschosen for this study. This methodrequires the individual to walkacross a walkway while pressuredata are collected from a single footcontact over the sensor platform.This method allows recording ofmeasurements during free move-ment and thus ensures that the effectof acceleration and deceleration atthe start and end of each walk isminimized.
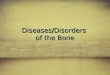
Putti et al42 investigated the repeat-ability of measurements of the EMEDsystem by having patients walk atnormal speed on 2 separate occa-sions, approximately 12 days apart.In the present study, the participantswere told to walk at normal speedand to keep their speed constant.Data were collected and stored foranalysis. Analysis of the records wasperformed with the emed/D soft-ware.†,44 An average of the 5 datasets was calculated by the software,and the foot was divided into geo-metric regions of interest accordingto the anatomical areas of the greattoe, second toe, first metatarsal head,and second metatarsal head, as wellas the total foot (Fig. 1). The follow-ing variables for each region weregenerated by the software: peakpressure (in kilopascals), maximumforce (in newtons), contact area (insquare centimeters), contact time (inmilliseconds), and force-time inte-gral (in newtons per second).
Measurements of plantar pressureprovide an indication of foot and an-kle function during gait. Data ob-tained from plantar pressure assess-ment can be used for the evaluationand treatment of patients with footdisorders. In the present study, plan-tar pressure measurements were per-formed to investigate changes in gaitbefore and in the postoperative pe-
Figure 1.Plantar pressure image with regions of interest: total foot, first metatarsal head (MH1),second metatarsal head (MH2), big toe, and second toe.
Rehabilitation After Hallux Valgus Surgery
September 2009 Volume 89 Number 9 Physical Therapy f 937

riod after hallux valgus surgery withrespect to the functional restorationof the operated area.45
Pressure (measured in pascals) is de-fined as force (measured in newtons)/area (measured in square meters).46
Peak pressure in the assessment ofdynamic plantar pressure distribu-tion is defined as the greatest pres-sure that is applied to the groundduring the stance phase of gait. Max-imum force is defined as the greatestvertical force that acts on a certainarea and indicates its load.46 In thepresent study, maximum force wasmeasured to determine the loadchanges of certain regions ofinterest.
The force-time integral (impulse) isthe area under the curve of a force(ie, time curve).45 These parametersare appropriate for describing theoverall loading effects of the footduring the stance phase of gait. Con-tact time reveals the time of groundcontact of either the total foot orcertain regions of interest during thestance phase. Contact area is thearea of contact of the foot to thesupporting surface during the stancephase. The data were not normalizedto foot size and weight. The standarddeviation reflects between-subjectvariations.
Rehabilitation ProgramAn Aircast cryo-cuff‡ was applied for8 hours starting immediately aftersurgery on the day of the operationand on the first postoperative day.This intervention was conducted asan inpatient treatment. Postopera-tively, participants were placed inthe Rathgeber postoperative shoe§
for 4 weeks. This shoe allows weightbearing of the operated limp whilereducing stress in the forefoot re-
gion. Participants also received aspecial sock (Gilofamed�) that re-duces swelling and the need fordressing changes. The first session ofthe physical therapy program started4 weeks after surgery, with one ses-sion per week. Physical therapytreatment was performed by 3 li-censed physical therapists followingthe same treatment protocol.
In the first session, elevation of theleg, lymphatic drainage, activation ofthe muscle pump, and cryotherapy(cool packs) were used to reduce theswelling. Participants were told toperform these actions at home oncea day for 20 minutes.
During gait training, physiologic gaitpatterns were achieved. The stancephase was trained by performing aheel-strike in its physiological posi-tion at the lateral aspect of the
heel,47 followed by weight bearingof the first metatarsal during mid-stance and terminal stance, withtraining of active push-off by thegreat toe flexors, the flexor digito-rum longus and brevis muscles, andthe lumbrical muscles.
Selective strengthening of the pero-neus longus muscle also was per-formed. The function of this muscleis to pronate the midfoot.20,48,49 Pro-nation is essential for ground contactof the first ray, the most heavilyloaded structure of the foot duringgait.19 If the peroneus longus muscleis too weak, people compensate bypushing the knee into a valgus posi-tion to achieve midfoot pronation. Inaddition, fascial release techniquesfor the peroneal muscles as well asto decrease of the tone (velocity-dependent resistance to stretch) ofthe tibialis anterior muscle were per-formed to improve the interaction ofthose antagonists.
‡ DonJoy Orthopaedics, ORMED GmbH, Merz-hauser Strasse, 112D-79100 Freiburg,Germany.§ OFA Bamberg GmbH, Laubanger 20, Bam-berg 96052, Germany.
� OFA Austria, Franz-Ofner Strasse, 6620 Salz-burg, Austria.
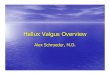
Figure 2.Manual therapeutic intervention at the first metarsophalangeal joint.
Rehabilitation After Hallux Valgus Surgery
938 f Physical Therapy Volume 89 Number 9 September 2009

Manual therapeutic interventionswere performed for all MTP joints.These manipulations focused on animprovement of flexion and in-cluded caudal sliding of the proximalphalanx to improve flexion and dor-sal sliding of the proximal phalanx toimprove extension (Fig. 2). In addi-tion, oscillating traction was per-formed to activate the mechanore-ceptors that inhibit the afferent painsensors.
The treatment protocol also in-cluded mobilization of the firstMTP, Lisfranc, transverse tarsal, sub-talar, and ankle joints. Concentricstrengthening exercises of the greattoe flexors and extensors were per-formed as well.
The participants received a mean of4.4 treatment sessions (range�3–6)based on their individual findings.The sessions took place once a weekfor 3 to 6 weeks. The duration of thesessions ranged from 35 to 45 min-utes. The participants also were in-structed to do a marble pick-up ex-ercise, apply cold packs, and dostrengthening exercises and gaittraining at home. A more-detailed de-scription of the rehabilitation pro-gram is included in the eAppendix(available at www.ptjournal.org).
Data AnalysisStudent t tests were used to deter-mine whether there was a significantdifference between the preoperativeand postoperative AOFAS scores andMTP ROM measurements. Repeated-measures analyses of variance andTukey post hoc analyses were usedto investigate the changes in plantarpressure parameters at the differenttime points. Statistical analysis wasperformed using SPSS version 11.3#
as well as Excel for Macintosh.** Thelevel of significance was defined as��.05.
ResultsTwenty-eight patients were availablefor a complete follow-up. One pa-tient was excluded from the 6-monthfollow-up examination because of arecent myocardial infarction. An-other patient was not able to partic-ipate in the 6-month follow-up exam-ination because of a work-relatedchange of his living area.
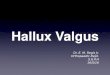
AOFAS ScoreThe mean AOFAS score increasedfrom 60.7 (SD�11.9) preoperativelyto 94.5 (SD�4.5) 6 months after sur-gery (P�.001) (Fig. 3).
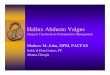
Pedobarographic AnalysisThe results of the plantar pressureassessment are summarized in Table2 and are illustrated in Figure 4.
Total FootThe total foot area maximum force,contact time, and force-time integraldid not show significant changes be-tween the different examinations.Mean peak pressure decreased from714.8 kPa (SD�195.8) preopera-tively to 622.4 kPa (SD�228.0) 4weeks postoperatively (P�.003). Sixmonths postoperatively, it reached687.8 kPa (SD�218.7), which wasnot statistically different from thepreoperative value (P�.896). Thecontact area decreased from a preop-erative mean value of 118.1 cm2
(SD�13.3) to 107.7 cm2 (SD�19.5)4 weeks postoperatively (P�.023).Likewise, the contact area demon-strated a statistically significant in-crease to 118.0 cm2 (SD�14.8) 8weeks after surgery (P�.048). By 6months after surgery, the mean totalfoot contact area of 119.0 cm2
(SD�12.8) was not significantly dif-ferent from the preoperative value(P�.960).
First Metatarsal HeadContact time did not show any sig-nificant changes for the first metatar-sal head. Mean maximum force de-creased from 117.8 N (SD�48.0)preoperatively to 77.3 N (SD�41.9)4 weeks postoperatively (P�.001)and increased to 123.7 N (SD�40.6)8 weeks after surgery (P�.001).Mean peak pressure decreased in thesame period from 288.9 kPa(SD�181.7) to 146.6 kPa (SD�73.5)(P�.001). Between the preopera-tive investigation and the assessment6 months postoperatively, therewas no statistically significant differ-ence either for maximum force orfor peak pressure (P�1.0). Meancontact area decreased between thepreoperative assessment and theevaluation 4 weeks after surgeryfrom 11.4 cm2 (SD�1.8) to 10.04
# SPSS Inc, 233 S Wacker Dr, Chicago, IL60606.** Microsoft Corp, One Microsoft Way, Red-mond, WA 98052-6399.
Figure 3.Preoperative and postoperative means of the American Orthopaedic Foot and AnkleSociety (AOFAS) score. The error bars indicate the standard deviation.
Rehabilitation After Hallux Valgus Surgery
September 2009 Volume 89 Number 9 Physical Therapy f 939

cm2 (SD�3.43) (P�.08) and in-creased to 12.1 cm2 8 weeks aftersurgery (P�.06). The force-time in-tegral increased from a mean of31.8 N�s 4 weeks postoperatively to47.5 N�s 8 weeks postoperatively(P�.026). It increased from 37.9 N�spreoperatively to 55.6 N�s 6 monthsafter surgery (P�.062). However,
this increase was not statisticallysignificant.
Second Metatarsal HeadMaximum force, peak pressure, andforce-time integral showed statisti-cally significant decreases betweenthe preoperative evaluation and theassessment 4 weeks after surgery
(P�.001, P�.001, P�.047, respec-tively) and significant increases be-tween the evaluation 4 weeks aftersurgery and the assessment 8 weeksafter surgery (P�.001, P�.021,P�.003, respectively).
Table 2.Resultsa of Plantar Pressure Assessments for Maximum Force (MF), Peak Pressure (PP), Contact Time (CT), Contact Area (CA),and Force-Time Integral (FTI)
Parameter Preoperative 4 Weeks Postoperative 8 Weeks Postoperative 6 Months Postoperative
Total foot
MF (N) 722.1�101.5 (690.3–766.1) 710.5�94.1 (670.7–750.2) 728.3�99.6 (694.1–767.5) 719.0�87.0 (686.0–753.7)
PP (kPa) 714.8�195.8b (649.9–805.7) 622.4�228.0 (429.7–600.0) 630.9�230.6 (534.0–710.8) 687.8�218.7 (603.0–772.5)
CT (ms) 818.4�181.7 (768.0–905.3) 934.1�132.5 (878.1–990.1) 894.7�131.0 (847.5–943.7) 891.1�137.7 (837.9–944.5)
CA (cm2) 118.1�13.3b (114.7–124.8) 107.7�19.5 (99.4–115.9) 118.00�14.77 (113.2–123.9) 119.0�12.8 (116.7–126.8)
FTI (N�s) 430.6�93.1 (404.6–480.8) 439.8�81.3 (405.5–474.1) 439.5�73.2 (415.2–473.8) 431.2�82.6 (408.5–480.3)
First metatarsal head
MF (N) 117.8�48.0b (105.6–142.2) 77.3�41.9c (59.6–95.0) 123.7�40.6 (110.8–142.0) 126.4�40.2 (131.2–162.0)
PP (kPa) 288.9�181.7b (220.2–350.9) 146.6�73.5 (115.6–177.7) 207.2�60.8 (189.9–242.8) 287.4�153.0 (228.0–346.7)
CT (ms) 613.5�134.2 (574.6–675.4) 661.2�188.0 (581.8–740.6) 661.3�133.2 (612.5–709.9) 661.6�135.6 (609.1–714.2)
CA (cm2) 11.4�1.8 (10.9–12.2) 10.04�3.43c (8.6–11.5) 12.1�2.2 (11.4–13.0) 12.1�1.6 (11.4–12.7)
FTI (N�s) 37.9�17.5 (34.2–49.5) 31.8�21.0c (22.9–40.6) 47.5�19.5 (40.8–55.1) 55.6�22.3 (46.9–64.3)
Second metatarsal head
MF (N) 169.4�37.1b,d (157.4–188.9) 118.1�51.0c (96.5–139.6) 173.1�54.0 (154.3–193.7) 185.8�41.9 (169.6–202.1)
PP (kPa) 614.2�217.1b (536.3–719.3) 325.8�212.7c (236.0–415.6) 519.0�255.2 (423.9–614.7) 584.4�246.2 (488.9–679.7)
CT (ms) 685.0�150.1 (638.6–751.6) 736.8�135.3 (670.7–793.9) 689.4�119.2 (647.0–736.0) 661.6�135.6 (578.1–1,019.1)
CA (cm2) 9.6�1.3 (9.3–10.2) 8.6�2.4 (7.6–9.7) 9.9�1.7 (9.3–10.5) 10.3�1.4 (9.8–10.7)
FTI (N�s) 62.4�16.7 (58.0–73.5) 50.3�21.1c (41.4–59.2) 71.1�22.8 (62.2–79.7) 74.7�21.1 (66.5–82.9)
Big toe
MF (N) 66.1�33.2b (57.0–83.2) 28.4�31.5 (15.1–51.7) 51.7�47.3e (33.2–67.6) 87.2�37.3 (72.8–101.7)
PP (kPa) 357.9�198.7b (301.4–451.2) 114.9�131.0 (59.6–170.2) 190.0�200.1 (117.9–265.4) 322.4�200.6 (244.6–400.0)
CT (ms) 548.8�138.3b (516.0–633.4) 363.7�262.3 (253.0–474.5) 437.7�201.0 (346.7–504.3) 533.6�161.8 (470.8–596.3)
CA (cm2) 7.3�2.1b,d (6.7–8.3) 5.09�3.1c (3.8–6.4) 7.4�2.4e (6.5–8.2) 9.2�1.5 (8.6–9.7)
FTI (N�s) 18.7�10.7b (16.0–25.6) 7.4�10.6 (2.9–11.9) 16.6�11.3e (6.7–17.0) 24.2�13.7 (18.9–29.5)
Second toe
MF (N) 23.6�15.4b (18.3–31.1) 10.4�11.2 (5.7–15.2) 15.5�12.1 (11.4–22.3) 20.8�16.6 (14.4–27.2)
PP (kPa) 150.6�83.2b (122.8–188.2) 68.9�56.8 (44.6–92.8) 103.5�66.5 (80.1–136.0) 135.7�90.0 (101.0–170.4)
CT (ms) 445.9�131.4 (417.4–522.9) 396.9�241.8 (294.9–499.0) 398.0�138.1 (361.2–466.0) 408.0�160.5 (345.8–470.3)
CA (cm2) 3.4�1.4b (3.0–4.0) 2.3�1.3 (1.7–2.8) 2.8�1.2 (2.4–3.3) 3.1�1.1 (2.7–3.5)
FTI (N�s) 5.8�3.9 (4.6–7.7) 2.5�3.7c (1.1–5.3) 3.9�3.9 (2.7–5.7) 5.3�5.5 (3.0–7.3)
a Results are expressed as mean�SD, with confidence interval (CI) in parentheses.b Statistically significant change at P�.05, preoperative assessment to 4-week postoperative assessment.c Statistically significant change at P�.05, 4-week assessment to 8-week postoperative assessment.d Statistically significant change at P�.05, preoperative assessment to 6-month postoperative assessment.e Statistically significant change at P�.05, 8-week assessment to 6-month postoperative assessment.
Rehabilitation After Hallux Valgus Surgery
940 f Physical Therapy Volume 89 Number 9 September 2009

Great ToeIn the great toe, maximum force,peak pressure, contact area, andforce-time integral decreased signifi-cantly between the preoperativeevaluation and the assessment at 4weeks following surgery (P�.001).The mean contact area showed a sta-tistically significant increase from5.09 cm2 (SD�3.1) 4 weeks after sur-gery (P�.001) to 7.4 cm2 (SD�2.4)8 weeks after surgery (P�.003) and9.2 cm2 (SD�1.5) 6 months after sur-gery (P�.017). The difference be-
tween the preoperative examinationand the assessment 6 months aftersurgery was statistically significant(P�.034).
Mean values for maximum forcewere 66.1 N (SD�33.2) preopera-tively and 87.2 N (SD�37.3) 6months after surgery (P�.320).Average force-time integral was 18.7N�s (SD�10.7) before surgery andreached 24.2 N�s (SD�13.7)(P�.752) 6 months postoperatively.
Contact time did not show any sta-tistically significant changes.
Second ToeIn the second toe, the maximumforce, peak pressure, and contactarea decreased significantly betweenthe preoperative evaluation and theassessment 4 weeks after surgery(P�.005, P�.001, P�.003, respec-tively). There were no statisticallysignificant changes for force-time in-tegral or contact time.
First MTP Joint ROMMean total ROM of the first MTP jointincreased from 68.9 degrees (SD�11.9, range�40–90) preoperativelyto 73.3 degrees (SD�21.4, range�30–150) 6 months after surgery.This improvement was not statisti-cally significant (P�.31). However,mean dorsiflexion significantly in-creased from 40.4 degrees (SD�9.0,range�25–60) preoperatively to45.9 degrees (SD�14.0, range�20–80) 6 months after surgery(P�.05). Mean plantar flexion was28.5 degrees (SD�6.9, range�15–40) preoperatively and 27.4 degrees(SD�11.5, range�5–45) 6 monthsafter surgery. This difference wasnot statistically significant (P�.44)(Fig. 5).
DiscussionIn our study, plantar pressure distri-bution was assessed in patients whounderwent hallux valgus surgery andreceived postoperative physical ther-apy and gait training. In general,loading parameters in the great toeregion and the region of the firstmetatarsal head did not decrease be-tween the preoperative examinationand the assessment at 6 months aftersurgery. Several authors8,13–17 havestudied changes in plantar pressuredistribution after hallux valgus sur-gery and found decreased loadingparameters in the hallux and thefirst metatarsal head region after sur-gery. To the best of our knowledge,the postoperative regimens in those
Figure 4.Regional force changes in the treated feet: preoperative (gray), 4 weeks postoperative(green), 8 weeks postoperative (blue), and 6 months postoperative (orange).
Figure 5.Range of motion (ROM) assessment: changes (in degrees) in plantar flexion, dorsiflex-ion, and overall ROM of the first metarsophalangeal joint.
Rehabilitation After Hallux Valgus Surgery
September 2009 Volume 89 Number 9 Physical Therapy f 941

studies did not include physical ther-apy and gait training, although Ker-nozek and Sterriker17 concluded thatthe inclusion of physical therapyand gait training would improve thefunctional outcome.
Plantar pressure distribution mea-surements are a proper method toassess the functional outcome ofhallux valgus surgery. This methodwas first recommended in 1956 byBarnett.50 Henry et al, in 1975, werethe first authors to report the re-sults of plantar pressure distribu-tion analysis.26 They studied 170 feetretrospectively and found that 50%underwent resection arthroplastyaccording to Keller or arthrodesisof the first MTP joint for treatmentof hallux valgus deformity. Theyshowed that patients who under-went resection arthroplasty did notuse their great toe for push-off. Inaddition, metatarsalgia showed a sig-nificantly higher incidence in the re-sectional arthroplasty group. Henryet al concluded that the higher inci-dence was attributable to the higherpressure distribution on the lateralaspects of the forefoot due to loadshift. Even though both methodsthat were investigated in that studyare joint-sacrificing methods ratherthan joint-preserving methods, whichare able to restore physiological jointbiomechanics as well as joint kine-matics, the results indicate that theuse of the great toe for push-off andweight bearing of the first ray is im-portant to avoid metatarsalgia dueto load shift after hallux valgus sur-gery. Therefore, a great deal of atten-tion should be drawn to the restora-tion of physiologic gait patterns aftersuch operations.
In agreement with Henry and col-leagues’ results,26 Stokes et al27
found no increase of plantar pres-sure patterns beneath the great toeregion in 40 feet of patients whounderwent a resectional arthroplastyor Wilson osteotomy. In addition,
they investigated the plantar pres-sure distribution of 64 individuals(128 feet) with absence of any footpathology and compared the resultswith the results of the hallux valgusgroup. On the lateral aspects of thefoot, the hallux valgus group showedhigher load before as well as aftersurgery compared to the controlgroup. Stokes et al also concludedthat this load shift may cause meta-tarsalgia. This was the first study thatrevealed pathologic plantar pressuredistribution after hallux valgus sur-gery with a joint-preserving method.
Feet affected with hallux valgus de-formity show a load shift to the lat-eral aspects of the foot and de-creased weight bearing of the greattoe.22,24,26–28 In a kinematic study,Mitternacht and Lampe22 found that,due to the lateral shift of the tendonsof the extrinsic muscles of the greattoe, a decrease in plantar-flexionmoment of the great toe can be iden-tified. Recently, Putti et al42 per-formed a plantar pressure distribu-tion assessment in 53 subjects whowere healthy and used the force-timeintegral to describe the overall load-ing effect. The force-time integral isappropriate for describing the over-all loading effect because it takesinto account the amplitude and du-ration of load application.45 Thestudy by Putti et al revealed meanforce-time integrals of 26 N�s for thehallux region and 52 N�s for the firstmetatarsal head region. In our study,we found mean preoperative force-time integrals of 37.9 N�s for the firstmetatarsal head region and 18.7 N�sfor the first metatarsal head region.These measurements indicate a de-creased load of the first ray in pa-tients with hallux valgus deformity.Six months after surgery, the meanvalues for these regions reached25.2 N�s for the big toe region and55.6 N�s for the first metatarsal headregion. These findings indicate in-creased weight bearing of the firstray and an almost physiological
plantar pressure distribution. In ad-dition, there were significantly de-creased plantar pressure parametersin the region of the first and secondmetatarsal heads 4 weeks after sur-gery compared with the preoperativeassessment. Considering the totalfoot region, no statistically signifi-cant changes for maximum force andforce-time integral were observed.These results indicate the possibilityof a load shift from the medial as-pect of the forefoot to the lateralaspects of the forefoot.
Our patients were placed in a post-operative shoe for 4 weeks after sur-gery. To ensure bone healing, thepostoperative shoe should decreasethe load in the traumatized region.2,3
The first ray is the most heavilyloaded structure of the foot duringgait.19 Therefore, the shoe is de-signed to shift the load from the me-dial aspect to the lateral aspect of theforefoot during propulsion. We be-lieve that one reason for the de-creased load in the great toe regionand the region of the medial forefoot4 weeks after surgery is the patho-logic gait pattern that is necessary inthe early postoperative period. How-ever, a multimodal rehabilitationprogram seems to be important forthe patient to eliminate these patho-logic gait patterns and to restore thefunction of the operated structures.
Recent plantar pressure distributionanalysis with an intermediate-termfollow-up revealed a decreased loadin the region of the first MTP joint aswell as in the great toe area afterhallux valgus surgery. Kernozek andSterricker17 found decreased peakpressure and force-time integral inthe great toe region 1 year after sur-gery compared with the preopera-tive examination in a prospectivestudy of 25 patients who underwentthe Austin procedure for correctionof hallux valgus deformity. They con-cluded that physical therapy may
Rehabilitation After Hallux Valgus Surgery
942 f Physical Therapy Volume 89 Number 9 September 2009

help to improve the functional out-come of this procedure.
Bryant et al13 investigated 31 sub-jects (44 feet) before and after anAustin osteotomy. They also assessedthe plantar pressure distribution in36 control subjects. They found adecreased load beneath the hallux 1year after the Austin procedure com-pared with preoperative levels.
In a retrospective analysis, Guesgenet al18 measured plantar pressure dis-tribution in 60 patients (66 feet) whounderwent a chevron osteotomy,with a mean follow-up of 3 years.Thirty-four percent of the patientswith a postoperative hallux valgusangle smaller than 20 degrees and56% of the patients with a postoper-ative hallux valgus angle greater than20 degrees did not use their great toeduring propulsion. These results sug-gest that a total of 45% of the patientshad pathologic gait patterns aftersurgery. Jones et al8 investigated 24patients (35 feet) who underwent ascarf osteotomy prospectively. Theyfound a decrease in the peak pres-sure of the first metatarsal after amean follow-up of 20 months.Dhukaram et al15 investigated 28patients who underwent a Mitchellor scarf osteotomy, with a meanfollow-up of 3 years. They also mea-sured plantar pressure distribution in15 individuals who were healthy.They found deficient load bearing ofthe hallux for both groups.
In this study, plantar pressure pat-terns in the great toe region de-creased significantly 4 weeks aftersurgery compared with the preoper-ative assessment. Maximum force,peak pressure, contact area, andforce-time integral showed statisti-cally significant increases betweenthe fourth and the eighth weekspostoperatively. For the great toe re-gion and the region of the first meta-tarsal head, maximum force andforce-time integral showed increases
compared with the preoperative val-ues. This tendency was statisticallynonsignificant. The changes con-cerning the plantar pressure distribu-tion indicate that there is improvedweight bearing of the first ray andthe great toe. This finding indicatesthat there is a functional improve-ment after hallux valgus surgery,which does not correspond to thepedobarographic results reported byother authors.8,13–15,17,18 Based onthose results, we believe that thisfunctional improvement is based onthe physical therapy interventions.
In agreement with other authors, theAOFAS score improved significantlyand reached 94.5 points at 6 monthsafter surgery. Cancilleri et al51 inves-tigated 30 patients after an Austinosteotomy and found a mean AOFASscore of 81.9 points at a mean of 37months after surgery. Trnka et al,11
in 2- and 5-year follow-up assess-ments of 66 patients after a modifiedchevron (Austin) osteotomy, found amean AOFAS score of 91 points.Aminian et al52 studied the clinicalresults of the scarf osteotomy in 27patients and found that the meanAOFAS score increased from 54.5points preoperatively to 86.5 pointsat an average follow-up of 16.1months. Kristen et al,9 in 89 patients(111 feet) who underwent a scarfosteotomy, reported that the meanAOFAS score increased from 50.1points preoperatively to 91 pointspostoperatively at a mean follow-upof 34 months. Perugia et al10 investi-gated 33 patients (45 feet) after ascarf osteotomy and reported a meanincrease in AOFAS score from 35.7points preoperatively to 89.8 pointspostoperatively. Jones et al,8 in 24patients (35 feet) who underwent ascarf osteotomy, found the meanAOFAS score increased from 52points preoperatively to 89 points ata mean of 22 months after surgery.Buchner et al,6 in 29 patients whounderwent a scarf osteotomy, foundan increase in mean AOFAS score
from 45 points preoperatively to 75points at an average follow-up of 6months. Crevoisier et al53 found in84 feet an increase in mean AOFASscore from 43 points preoperativelyto 82 points at a mean follow-up of22 months. In the present study, pa-tients had a relatively high AOFASscore in comparison with theseother investigations, even thoughsurgery was just 6 months prior.
The total ROM improved from 68.8degrees preoperatively to 73.3 de-grees by 6 months after surgery. Thisimprovement did not show statisti-cal significance, but isolated dorsi-flexion significantly improved from40.4 to 45.9 degrees. It is difficult tocompare the results of ROM mea-surements in our study with those ofother studies because of the differentmethods used for the assessment offirst MTP joint ROM. However, dur-ing propulsion, the first MTP jointhas been reported to dorsiflex be-tween 40 and 60 degrees during typ-ical gait.54 Plantar flexion of only afew degrees is necessary to allowphysiologic gait. The improvementof dorsiflexion also may help to re-store physiological gait patterns.
Weaknesses of this study include,due to its descriptive nature, the ab-sence of a control group that did notreceive physical therapy after halluxvalgus surgery. A randomized con-trolled design would improve thelevel of evidence. Further research isnecessary to determine whetherthere is a beneficial effect of a mul-timodal rehabilitation program onthe restoration of physiological plan-tar pressure patterns. Further re-search should focus on performing arandomized controlled trial address-ing this question. Gait speed seemsto affect plantar pressure distribu-tion.55 In the present study, plantarpressure assessment was performedusing the mid-gait method because itis the most favorable way to repre-sent normal gait patterns.42,45 Partic-
Rehabilitation After Hallux Valgus Surgery
September 2009 Volume 89 Number 9 Physical Therapy f 943

ipants were instructed to walk at anormal speed and to keep theirspeed constant. Putti et al42 showedthat this method produces repeat-able results. However, gait speedwas not recorded. Therefore, it isimpossible to analyze the influenceof gait speed on the plantar pressuredistribution in the patients in thisstudy.
The strengths of this study includeits prospective nature and a system-atic plantar pressure assessment. Inaddition, to the best of our knowl-edge, this is the first study determin-ing plantar pressure changes afterhallux valgus surgery and postopera-tive physical therapy.
ConclusionNumerous authors13,15–18,22,24,26–28
have reported pathologic gait pat-terns after hallux valgus surgery. Wefound that there was an increase inplantar pressure parameters in theregion of the great toe and the firstray after hallux valgus surgery in pa-tients who received physical therapyas well as gait training in the postop-erative period. Therefore, we believethat postoperative physical therapyhelps to restore function in weightbearing and ambulation after halluxvalgus surgery.
Mr Schuh and Dr Trnka provided concept/idea/research design. Mr Schuh and Dr Ad-ams provided writing. Mr Schuh and Dr Hof-staetter provided data collection. Mr Schuhprovided data analysis. Dr Hofstaetter andMr Pichler provided project management.Mr Pichler and Dr Kristen provided partici-pants. Dr Kristen and Dr Trnka provided fa-cilities/equipment. Dr Hofstaetter, Dr Ad-ams, Mr Pichler, and Dr Kristen providedconsultation (including review of manuscriptbefore submission). The authors acknowl-edge the help of Wolfgang Schuh, MSc, inpreparation of the manuscript.
This study was approved by the Foot andAnkle Center Vienna Institutional ReviewBoard.
This article was received November 24, 2008,and was accepted May 28, 2009.
DOI: 10.2522/ptj.20080375
References1 Easley ME, Trnka HJ. Current concept re-
view: hallux valgus, part II: operative treat-ment. Foot Ankle Int. 2007;29:748–758.
2 Robinson AH, Limbers JP. Modern con-cepts in the treatment of hallux valgus.J Bone Joint Surg Br. 2005;87:1038–1045.
3 Coughlin MJ. Instructional course lec-tures, the American Academy of Orthopae-dic Surgeons: hallux valgus. J Bone JointSurg Am. 1996;78:932–966.
4 Sammarco VAJ. Stability and fixation tech-niques in first metatarsal osteotomies.Foot Ankle Clin. 2001;6:409–432.
5 Barouk LS. Scarf osteotomy of the firstmetatarsal in the treatment of hallux val-gus. Foot Disease. 1995;2:35–48.
6 Buchner M, Schulze A, Zeitang F, Sabo D.Pressure distribution after scarf osteotomyfor hallux valgus surgery [in German]. ZOrthop Ihre Grenzgeb. 2005;143:233–239.
7 Dereymaeker G. Scarf osteotomy for cor-rection of hallux valgus: surgical tech-nique and results as compared to distalchevron osteotomy. Foot Ankle Clin.2000;5:513–524.
8 Jones S, Al Hussainy HA, Ali F, et al. Scarfosteotomy for hallux valgus: a prospec-tive clinical and pedobarographic study.J Bone Joint Surg Br. 2004;86:830–836.
9 Kristen KH, Berger C, Stelzig S, et al. TheSCARF osteotomy for the correction of hal-lux valgus deformities. Foot Ankle Int.2002;23:221–219.
10 Perugia D, Basile A, Gensini A, et al. Thescarf osteotomy for severe hallux valgus.Int Orthop. 2003;27:103–106.
11 Trnka HJ, Zembsch A, Easley ME, et al. Thechevron osteotomy for correction of hal-lux valgus: comparison of findings aftertwo and five years of follow-up. J BoneJoint Surg Am. 2000;82:1373–1378.
12 Trnka HJ, Zembsch A, Wiesauer H, et al.Modified Austin procedure for correctionof hallux valgus. Foot Ankle Int. 1997;18:119–127.
13 Bryant AR, Tinley P, Cole JH. Plantar pres-sure and radiographic changes to the fore-foot after the Austin bunionectomy. J AmPodiatr Med Assoc. 2005;95:357–365.
14 Dhanendran M, Pollard JP, Hutton WC.Mechanics of the hallux valgus foot andthe effect of Keller’s operation. Acta Or-thop Scand. 1980;51:1007–1012.
15 Dhukaram V, Hullin MG, Senthil Kumar C.The Mitchell and Scarf osteotomies for hal-lux valgus correction: a retrospective, com-parative analysis using plantar pressures.J Foot Ankle Surg. 2006;45:400–409.
16 Kernozek TW, Roehrs T, McGarvey S.Analysis of plantar loading parameters preand post surgical intervention for halluxvargus. Clin Biomech (Bristol, Avon).1997;12:S18–S19.
17 Kernozek TW, Sterriker SA. Chevron (Aus-tin) distal metatarsal osteotomy for halluxvalgus: comparison of pre- and post-surgical characteristics. Foot Ankle Int.2002;23:503–508.
18 Gusgen C, Walther M, Wolfel R, Vispo-Seara JL. The distal chevron osteotomy forhallux valgus: a medium-term retrospec-tive clinical, radiographic and pedo-barographic analysis [in German].Fu�Sprung. 2005;3:164–171.
19 Jacob HAC. Forces acting in the forefootduring normal gait: an estimate. Clin Bio-mech (Bristol, Avon). 2001;16:783–792.
20 Rodgers MM. Dynamic biomechanics of thenormal foot and ankle during walking andrunning. Phys Ther. 1988;68:1822–1830.
21 Myerson MS. The etiology and pathogen-esis of hallux valgus. Foot Ankle Clin.1997;2:583–598.
22 Mitternacht J, Lampe R. Calculation offunctional kinetic parameters from theplantar pressure distribution measure-ment [in German]. Z Orthop Ihre Grenz-geb. 2006;144:410–418.
23 Grieve DW, Rashdi T. Pressures under nor-mal feet in standing and walking as mea-sured by foil pedobarography. Ann RheumDis. 1984;43:816–818.
24 Hutton WC, Dhanendran M. The mechan-ics of normal and hallux valgus feet: aquantitative study. Clin Orthop Relat Res.1981;(157):7–13.
25 Sanders M. Conservative treatment andshoewear options for hallux valgus. FootAnkle Clin. 1997;4:639–649.
26 Henry AP, Waugh W, Wood H. The use offootprints in assessing the results of oper-ations for hallux valgus: a comparison ofKeller’s operation and arthrodesis. J BoneJoint Surg Br. 1975;57:478–481.
27 Stokes IA, Hutton WC, Stott JR, Lowe LW.Forces under the hallux valgus foot beforeand after surgery. Clin Orthop Relat Res.1979;(142):64–72.
28 Waldecker U. Metatarsalgia in hallux val-gus deformity: a pedographic analysis.J Foot Ankle Surg. 2002;41:300–308.
29 Malone TB, Blackburn TA, Wallace LA.Knee rehabilitation. Phys Ther. 1980;60:1602–1610.
30 Beynnon BD, Johnson RJ, Fleming BC. Thescience of anterior cruciate ligament reha-bilitation. Clin Orthop Relat Res. 2002;(402):9–20.
31 Chen B, Zimmerman JR, Soulen L, DeLisaJA. Continuous passive motion after totalknee arthroplasty: a prospective study.Am J Phys Med Rehabil. 2000;79:421–426.
32 Hodgson S. Proximal humerus fracture re-habilitation. Clin Orthop Relat Res. 2006;442:131–138.
33 Theiler R, Schmid C, Risler R, Moser L.Postoperative physiotherapy in acute care:when, what and how much [in German]?Orthopade. 2007;36:552, 554–559.
34 Shaffer MA, Okereke E, Esterhai JL Jr, et al.Effects of immobilization on plantar-flexion torque, fatigue resistance, andfunctional ability following an ankle frac-ture. Phys Ther. 2000;80:769–780.
Rehabilitation After Hallux Valgus Surgery
944 f Physical Therapy Volume 89 Number 9 September 2009

35 Shamus J, Shamus E, Gugel RN, et al. Theeffects of sesamoid mobilization, flexorhallucis strengthening, and gait training onreducing pain and restoring function inindividuals with hallux limitus: a clinicaltrial. J Orthop Sports Phys Ther. 2004;80:769–780.
36 Austin DW, Leventen EO. A new osteot-omy for hallux valgus: a horizontally di-rected “V” displacement osteotomy of themetatarsal head for hallux valgus and pri-mus varus. Clin Orthop Relat Res. 1981;(157):25–30.
37 Barouk LS. Scarf osteotomy for hallux val-gus correction: local anatomy, surgicaltechnique, and combination with otherforefoot procedures. Foot Ankle Clin.2000;5:525–558.
38 Jarde O, Trinquier-Lautard JL, Gabrion A,et al. Hallux valgus treated by Scarf osteot-omy of the first metatarsus and the firstphalanx associated with an adductor plasty:apropos of 50 cases with a 2-year follow up[in French]. Rev Chir Orthop ReparatriceAppar Mot. 1999;85:374–380.
39 Smith RW, Reynolds JC, Stewart MJ. Hal-lux valgus assessment: report of researchcommittee of American Orthopaedic Footand Ankle Society. Foot Ankle. 1984;5:92–103.
40 Kitaoka HB, Alexander IJ, Adelaar RS, et al.Clinical rating systems for the ankle-hindfoot, midfoot, hallux, and lesser toes.Foot Ankle Int. 1994;15:349–353.
41 Hughes J, Pratt L, Linge K, et al. Reliabilityof pressure measurements: the EMED Fsystem. Clin Biomech (Bristol, Avon).1991;6:14–18.
42 Putti AB, Arnold GP, Cochrane LA, Ab-boud RJ. Normal pressure values and re-peatability of the Emed ST4 system. GaitPosture. 2008;27:501–505.
43 van der Leeden M, Dekker JH, SiemonsmaPC, et al. Reproducibility of plantar pres-sure measurements in patients withchronic arthritis: a comparison of one-step, two-step, and three-step protocolsand an estimate of the number of measure-ments required. Foot Ankle Int. 2004;25:739–744.
44 Metaxiotis D, Accles W, Pappas A, Doede-rlein L. Dynamic pedobarography (DPB)in operative management of cavovarusfoot deformity. Foot Ankle Int. 2000;21:935–947.
45 Orlin MN, McPoil TG. Plantar pressure as-sessment. Phys Ther. 2000;80:399–409.
46 Barnes SZ, Berme N. Measurement of ki-netic parameters technology. In: Craik RL,Oatis CA, eds. Gait Analysis: Theory andApplication. St Louis, MO: Mosby-YearBook Inc; 1995:239–251.
47 Cheung RTN, Gabriel YF. Influence of dif-ferent footwear on force of landing duringrunning. Phys Ther. 2008;88:620–628.
48 Perry J. Gait Analysis: Normal and Patho-logic Function. Thorofare, NJ: Slack Inc;1992.
49 Riegger CL. Anatomy of the ankle and foot.Phys Ther. 1988;68:1802–1814.
50 Barnett CH. Phases of human gait. Lancet.1956;22:617–621.
51 Cancilleri F, Marinozzi A, Martinelli N,et al. Comparison of plantar pressure, clin-ical, and radiological changes of the fore-foot after biplanar Austin osteotomy andtriplanar Boc osteotomy in patients withmild hallux valgus. Foot Ankle Int. 2008;29:817–824.
52 Aminian A, Kelikian A, Moen T. Scarf os-teotomy for hallux valgus deformity: anintermediate follow-up of clinical and ra-diographic outcomes. Foot Ankle Int.2006;27:883–886.
53 Crevoisier X, Mouhsine E, Ortolano V,et al. The scarf osteotomy for the treat-ment of hallux valgus deformity: a re-view of 84 cases. Foot Ankle Int. 2001;22:970–976.
54 Hetherington VJ, Johnson RE, Albritton JS.Necessary dorsiflexion of the first metatar-sophalangeal joint during gait. J Foot Surg.1990;29:218–222.
55 Rosenbaum D, Hautmann S, Gold M, ClaesL. Effects of walking speed on pressuredistribution patterns and hindfoot angularmotion. Gait Posture. 1994;2:191–197.
Rehabilitation After Hallux Valgus Surgery
September 2009 Volume 89 Number 9 Physical Therapy f 945