Embed Size (px)
Citation preview
1Researching a brighter future for stroke
Researching a brighter future for strokeThe European Stroke Network
2 The European Stroke Network
ContentsForeword 3
What is a stroke? 4
Improving treatments 6
Repairing the brain 8
Saving the barrier 10
Delivering drugs to the brain 12
European Stroke Network 14
Member organizations 15
Written by Lorna Layward
Produced in collaboration with the Stroke Alliance for Europe (SAFE). SAFE is a non-profit organization representing patient groups across Europe whose goal is for a world where there are fewer strokes and all those touched by stroke get the help they need. For more information, please visit www.safestroke.org
Some of the photographs used in this publication have been kindly provided by The Stroke Association in the UK, a member of SAFE.
3Researching a brighter future for stroke
ForewordA stroke can be devastating and life changing. In a single moment, someone can go from being fit and active to living with disability. Because a stroke causes brain damage, it can affect the ability to communicate, walk, move arms and hands, and how people think and feel. Most people know someone who has had a stroke, and know that it can also affect the lives of those around them, turning loved ones into carers.
Despite stroke being the third biggest killer in Europe, research into the prevention, understanding, care, and treatment of stroke has been underdeveloped. The European Stroke Network was created to bring together the best clinical and scientific stroke researchers in Europe to speed up the production of new treatments for stroke. The Network has been designed to bring in the right expertise that will make new treatments a reality, even recruiting people who have never worked in stroke research before. The inclusion of industry and patient organizations forms a unique collaboration.
We are grateful to the European Union for recognizing the importance of the Network and providing funding for our work.
We aim to develop new treatments for people who have had a stroke. We want to reduce brain damage and improve recovery so that people survive their stroke and live independent and fulfilled lives.
This publication describes work in progress and we hope that you enjoy reading about it. The research is far from finished. Only when stroke is either a condition of the past, or when everyone who has a stroke survives with minimal consequences will our work be complete.
Professor Stephen Meairs Professor Ulrich Dirnagl
Coordinators of the European Stroke Network
4 The European Stroke Network
A stroke happens when the blood supply to part of the brain is cut off and brain cells are damaged or die.
The longer the brain is starved of oxygen the more damage is done.
Strokes are more likely to occur as we age, with three quarters of strokes happening to people aged over 65. However, it can strike at any age, even in children.
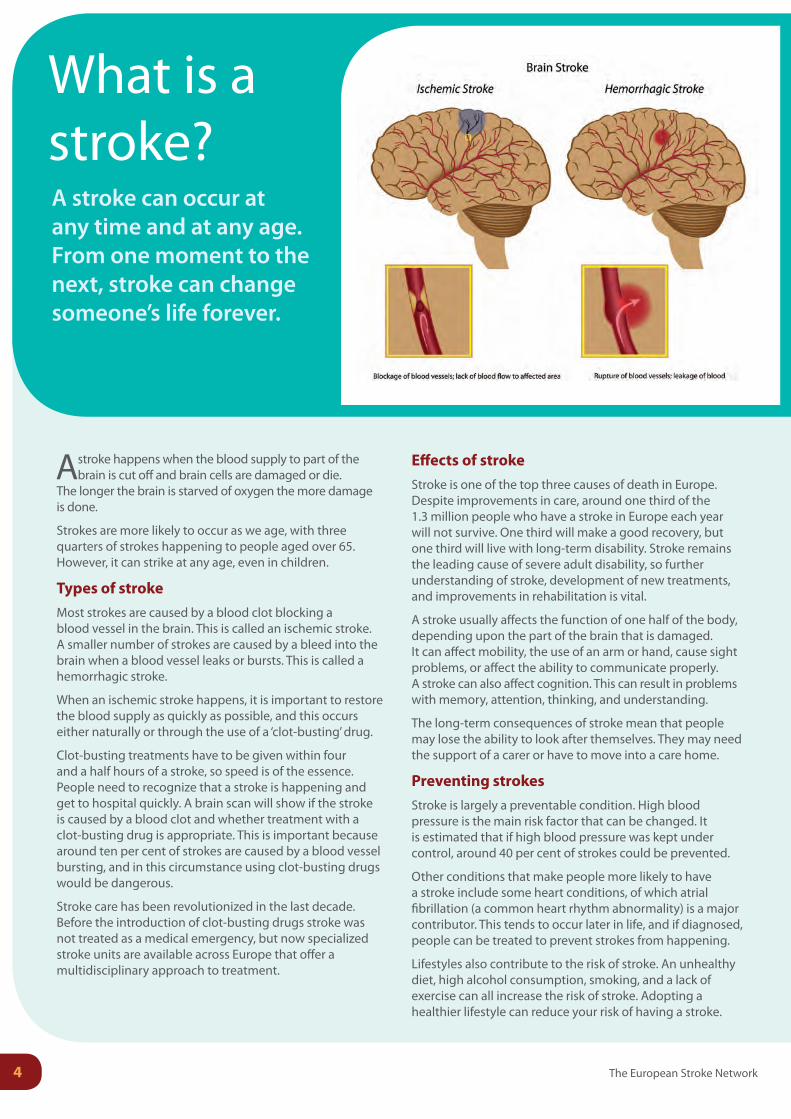
Types of strokeMost strokes are caused by a blood clot blocking a blood vessel in the brain. This is called an ischemic stroke. A smaller number of strokes are caused by a bleed into the brain when a blood vessel leaks or bursts. This is called a hemorrhagic stroke.
When an ischemic stroke happens, it is important to restore the blood supply as quickly as possible, and this occurs either naturally or through the use of a ‘clot-busting’ drug.
Clot-busting treatments have to be given within four and a half hours of a stroke, so speed is of the essence. People need to recognize that a stroke is happening and get to hospital quickly. A brain scan will show if the stroke is caused by a blood clot and whether treatment with a clot-busting drug is appropriate. This is important because around ten per cent of strokes are caused by a blood vessel bursting, and in this circumstance using clot-busting drugs would be dangerous.
Stroke care has been revolutionized in the last decade. Before the introduction of clot-busting drugs stroke was not treated as a medical emergency, but now specialized stroke units are available across Europe that offer a multidisciplinary approach to treatment.
Effects of strokeStroke is one of the top three causes of death in Europe. Despite improvements in care, around one third of the 1.3 million people who have a stroke in Europe each year will not survive. One third will make a good recovery, but one third will live with long-term disability. Stroke remains the leading cause of severe adult disability, so further understanding of stroke, development of new treatments, and improvements in rehabilitation is vital.
A stroke usually affects the function of one half of the body, depending upon the part of the brain that is damaged. It can affect mobility, the use of an arm or hand, cause sight problems, or affect the ability to communicate properly. A stroke can also affect cognition. This can result in problems with memory, attention, thinking, and understanding.
The long-term consequences of stroke mean that people may lose the ability to look after themselves. They may need the support of a carer or have to move into a care home.
Preventing strokesStroke is largely a preventable condition. High blood pressure is the main risk factor that can be changed. It is estimated that if high blood pressure was kept under control, around 40 per cent of strokes could be prevented.
Other conditions that make people more likely to have a stroke include some heart conditions, of which atrial fibrillation (a common heart rhythm abnormality) is a major contributor. This tends to occur later in life, and if diagnosed, people can be treated to prevent strokes from happening.
Lifestyles also contribute to the risk of stroke. An unhealthy diet, high alcohol consumption, smoking, and a lack of exercise can all increase the risk of stroke. Adopting a healthier lifestyle can reduce your risk of having a stroke.
What is a stroke?A stroke can occur at any time and at any age. From one moment to the next, stroke can change someone’s life forever.

Researching a brighter future for stroke 5
A personal account of having a stroke
‘My guinea pig rushed to the front of his hutch as I collected his water bottle. It is the first thing I do every day to ensure he has fresh water.
‘Suddenly things start to happen. Strange things. First of all, I drop the bottle, but still have the top tightly gripped in my left hand. I can’t see the bottle anywhere. I feel dizzy and look around bewildered. When I look down again, there is the bottle at my feet. Feeling rather stupid that I had missed it the first time, I pick it up and walk back into the kitchen to clean and refill it. My actions are almost robotic – I’m not feeling “right” but I don’t feel ill either. My right arm won’t work properly, it feels heavy, and I can’t grip the newspaper I’m trying to pick up. I go to sit down and pull myself together.
‘My husband is sitting in the lounge and looks up as I enter from the kitchen. He hurries towards me. Now I’m in the bathroom. There are two anxious faces looking at me – my husband and a paramedic. How come I’m in the bedroom now sitting on my bed? More people come in.
‘I’m in an ambulance with an oxygen mask on and a man is telling me not to be frightened by the siren noise as we speed towards the hospital…’
Mrs P.F.
Living with the effects of stroke
‘After my stroke three years ago, I received physiotherapy, occupational therapy, speech and language therapy and help from social services.
‘Initially I hated the speech and language therapy. I couldn’t recognize a single letter of the alphabet and it frightened me. It was like living in a foreign country. I quickly became very depressed, life was not worth living. My doctor prescribed me antidepressants and very slowly I began to improve.
‘Immediately after my stroke I was not able to stand, and I remember seeing a man walking with two sticks and I said to the physiotherapist: “I’ll never be able to do that.” She said: “Of course you will.” And she was right. I was able to walk out of hospital with a stick.
‘I still struggle with movement and still have speech and sight problems and suffer from depression and fatigue. I am learning to read again and have learnt to paint – something I’ve never done before.
‘Slowly my wife and I began to climb out of the terrible hole that we had plunged into. We now have a life that we have adapted to; we have made new friends and are able to enjoy life again.’
Mr M.B.
Stroke is an expensive condition, costing Europe over €64 billion a year. Following a stroke, people may spend considerable time in hospital and need long-term rehabilitation, such as physiotherapy, speech, and occupational therapy. Social services also have a major role to play in enabling stroke survivors to live their lives to the full.
The European Stroke Network
Improving treatments
Clot-busting drugs are the only early treatment presently approved by the authorities for stroke. Introduced around a decade ago, it has revolutionized stroke care and has led to improved recovery from stroke.
6 The European Stroke Network

Researching a brighter future for stroke
Most strokes are caused by a blood clot lodging in a blood vessel to the brain, blocking it and starving the
brain of oxygen. If the blood clot is not removed quickly, the part of the brain affected will die. It is this brain death that leads to the disabling long-term effects of stroke.
Clot-busting treatments are available, but are not suitable for everyone and must be given within four and a half hours of a stroke to be effective. People must be scanned before treatment to make sure that the stroke is caused by a clot rather than a bleed, which means that they must arrive at a specialist stroke center with plenty of time to spare.
With these restrictions, it is estimated that only 5% of people who have a stroke in Europe are treated with clot-busting drugs. In addition, the medication is effective in only some of those treated. This leaves the overwhelming majority of people who have a stroke without treatment.
Researchers in the European Stroke Network are working to change this. They are exploring ways to improve the effectiveness of clot-busting drugs and developing treatments to reduce the unwanted side effects, so that in future more people can benefit from treatment when they have a stroke.
As part of the European Stroke Network, Professor Denis Vivien, who works at Cyceron (INSERM) in France, is leading the research effort to improve the action of clot-busting drugs and remove the side effects.
The active ingredient in clot-busting drugs used in stroke is called tissue-type plasminogen activator or tPA for short. tPA is a protein normally found in the body that activates the major enzyme responsible for breaking down clots. It is found on the cells that line the blood vessels.
Like all drugs, tPA has side effects as well as benefits. It is reducing these unwanted side effects that Professor Vivien has been focusing his efforts.
‘In my laboratory we found that tPA is also produced by neurons and that it triggers these nerve cells to die when the brain is injured,’ Professor Vivien explains.
‘The last thing you want to happen after a stroke is for nerve cells to die. So we set about finding a way to prevent clot-busting drugs doing this. We developed an antibody that blocks this negative effect of tPA on nerve cells and showed that it works in experimental models of stroke.’
In collaboration with a pharmaceutical company, the antibody is in the process of being produced in sufficient quantities and purity to be used in humans. Professor Vivien hopes that the first clinical trials in people who have a stroke will start soon.
Since the brain itself produces some tPA during a stroke, this antibody could also be of benefit to people who are not eligible for clot-busting treatment. If natural tPA stimulates the death of brain cells after a stroke, then blocking its action could help protect the brain.
Professor Vivien envisages that if this treatment is proved safe and effective, everyone who has a stroke, even if the stroke is caused by a bleed into the brain, could benefit.
‘We have evidence that in hemorrhagic stroke – caused by bleeding in the brain – this antibody can have a positive effect on protecting nerve cells,’ he explains. ‘This means that it could be used as a first line of defense, given quickly after a stroke without the need for brain imaging and before arriving in a specialist stroke center.’
Professor Vivien’s team is also designing and producing new variations of the tPA molecule that still keeps its ability to break up blood clots, but eliminates the unwanted side effects. His laboratory has already produced and patented some new variations, and a spin-off company has been formed to develop them for patient use. If this goes well, clinical trials will follow, although this will be some time away.
There is no doubt that clot-busting drugs have already made a real difference, but we are only just at the beginning of developing treatments for stroke. Professor Vivien thinks that not so far in the future people who have a stroke will receive a range of different treatments that not only remove blood clots, but also protect brain cells, reduce inflammation, and encourage growth of new brain cells.
One of the major benefits of working in the European Stroke Network has been the sharing of experimental models so that groups in different countries are producing comparable results.
‘Researchers from other groups have come to work in my laboratory to learn different techniques, and we work closely together to get the science done more effectively,’ Professor Vivien says. ‘But it is the mix of laboratory science and clinical research that makes the real difference. It is only by this collaboration that discoveries get quickly from the laboratory to benefitting patients.’
The European Stroke Network promotes this collaborative approach and encourages researchers from different disciplines and different countries to talk to one another. Everyone within the Network gets together twice a year to discuss results and ideas. Better science often results from researchers meeting and creating new ideas and ways of working together.
7Researching a brighter future for stroke
Professor Vivien
8 The European Stroke Network
Not so long ago scientists thought that once brain cells were lost, they were gone forever and could not be
replaced, resulting in a lifetime of disability. This view has been changed by the discovery of stem cells.
‘When I first started as a neurologist, it was thought to be impossible to re-grow nerve cells in the brain,’ says Professor Olle Lindvall. ‘But over the last 20 years we have learnt much more, and even seen that it is possible to improve the lives of people with brain conditions using cell transplantation.’
Professor Lindvall, from Lund University in Sweden, pioneered the use of cell therapy in Parkinson’s disease. Even 15 years after transplanting fetal cells into the brain, the dramatic improvements in the function of some of his patients are still maintained.
‘This means that the principle that you can replace dead cells in the patient’s brain with new healthy nerve cells and improve function is working,’ he explains. ‘And now we are attempting to find out the best way to do this using stem cells in stroke.’
We now understand that the brain is a dynamic structure with new cells being formed all the time from the brain’s own neural stem cells. It seems the brain has the potential to repair itself. If we can harness this natural repair process, it would provide real hope that more people can recover after a stroke.
After a stroke or other brain injury in animal models, the brain does try to repair itself. A stroke triggers the production of a whole range of molecules that encourage the production
of stem cells to form new nerve cells and other support cells within the damaged brain.
Professor Lindvall and his team have been focusing their research on a newly discovered protein molecule called Meteorin.
‘We chose Meteorin because it is normally present in the brain, and is increased when the brain is damaged,’ explains Professor Lindvall. ‘We also found in the laboratory that it helps the survival, maturation and movement of neurons formed from neural stem cells – just the characteristics that we were looking for.’
‘In experimental models of stroke we also found that Meteorin increased the number of mature neurons in the brain,’ he adds. ‘This was encouraging news but we need to know much more about how it works in animals and how we can get the best functional improvement from Meteorin before we try it out in patients.’
Professor Lindvall’s team is also looking into the role of inflammation in brain repair.
‘Until recently, inflammation in the brain associated with stroke was thought to be harmful,’ he says. ‘But we now think that inflammation could be a major player in a positive way by promoting or even triggering regeneration including the formation of new neurons.’
The researchers are therefore teasing out the damaging aspects of inflammation from its regeneration potential and hope to be able to harness this potential to help brain repair.
Being part of the European Stroke Network has helped this area of work progress. Professor Lindvall’s team has benefited from the expertise of researchers from
Repairing the brainDisrupting the blood supply to the brain means that cells are starved of oxygen and die. Researchers are now looking into how to replace lost nerve cells.
Professor Lindvall
Researching a brighter future for stroke
Professor Nancy Rothwell’s laboratory in Manchester, United Kingdom.
‘We have a researcher from England who is an expert in inflammation now working in our lab, which has helped considerably to move on our work in this area,’ explains Professor Lindvall. ‘Being part of a large network means that I now know all the major researchers in stroke in Europe and we have built up trust, exchanged ideas, and developed collaborations.’
In the future, Professor Lindvall believes that we need to develop a range of strategies to rebuild the brain, including promoting the natural repair process with molecules such as Meteorin, alongside stem cell transplantation and modification of inflammation, to maximize brain repair.
Restoring nerve damage will not be the end of the story. Rehabilitation will have to take place at the same time, as the new brain tissue will have to learn the functions lost due to stroke. It is thought that intensive rehabilitation will be vital to regain function.
Interestingly, exercise and rehabilitation cause the release of the same molecules that are thought to be important for promoting brain repair, so rehabilitation may take on dual roles – both relearning function and repairing the brain.
Boosting brain repair in stroke could become a reality in the not too distant future. While it may not be the answer to the most severe of strokes, it provides hope that it can help many more stroke survivors enjoy more active, independent, and fulfilled lives.
STEM CELLS are found in all multicellular organisms. They divide and differentiate into all the cell types in the body and can self-renew to produce more stem cells. In mammals, there are two broad types of stem cells: embryonic stem cells and adult stem cells.
EMBRYONIC STEM CELLS are produced in the embryo and differentiate into all the specialized cells of the body including adult stem cells. These embryonic stem cells are called pluripotent cells because they have the potential to become many types of cells (from the world plural). There are currently no approved treatments using embryonic stem cells.
ADULT STEM CELLS replenish tissues, acting as a repair system for the body. They maintain the normal turnover of organs such as blood, skin, or intestinal tissue. Adult stem cells are also routinely used in medicine. They can be taken from a variety of sources, including umbilical cord blood, fat tissue, and bone marrow. Adult stem cell treatments have been successfully used for many years to treat leukemia and other blood cancers through bone marrow transplants.
Stem cells can now be artificially grown in culture and transformed into specialized cell types with characteristics of cells of various tissues such as muscles or nerves.
The use of adult stem cells is not as controversial as the use of embryonic stem cells, because the production of adult stem cells does not require the destruction of an embryo. Furthermore, in cases where adult stem cells are obtained from the intended recipient, the risk of rejection is essentially non-existent.
Many medical researchers believe that stem cell therapy has the potential to dramatically change the treatment of human diseases. However, there still exists a great deal of social and scientific uncertainty surrounding stem cell research that needs public debate, further research, and education.
9

The European Stroke Network
Saving the barrierThe brain is such an important organ that it has an ingenious barrier to protect it, but when a stroke occurs, the barrier is breeched.
10
The brain is essentially isolated from the circulating blood by a blood-brain barrier. The barrier is along all the small
blood vessels of the brain and consists of cells forming very tight junctions between themselves that do not let objects such as bacteria and even small molecules pass through, but allow free passage of oxygen and carbon dioxide.
Cells of the barrier actively transport the nutrients needed by the brain, such as glucose and some proteins, keeping the brain’s environment constant and safe.
Professor Britta Engelhardt from the University of Bern in Switzerland is an expert on the blood-brain barrier and how cells of the immune system manage to cross the barrier into the brain.
‘We want to know what happens to the blood vessel behind the blockage when someone has a stroke,’ she explains. ‘The blood vessel is starved of oxygen and glucose just as the brain is, and if the blood supply is not restored very quickly then the blood-brain barrier begins to break down.’
It is not just the lack of blood supply that causes damage to the blood-brain barrier. When the blood supply returns
after the removal of the blockage, this process causes further damage beyond that caused by lack of oxygen and glucose.
Little is known about what happens to the blood-brain barrier in stroke. If researchers are going to find ways to protect the barrier, they must first understand what causes its breakdown.
‘If you envisage a medieval castle surrounded by a two-walled moat,’ Professor Engelhardt explains, ‘you can imagine what the blood-brain barrier is like. The castle is the brain, which is protected first by the outer wall. If this wall is breeched then not too much damage might take place unless there is a trigger, such as an infective agent that then causes an influx of chemicals and cells. If a second step – lowering of the drawbridge across the moat – takes place, then the inner wall can be breeched leaving the brain open to assault.’
If the blood-brain barrier breaks down, the consequences can be serious, as cells and molecules normally kept away from the brain flood in. The brain needs a stable environment as nerve cells communicate by electrical activity. Blood-brain barrier breakdown can interfere with nerve activity and even cause them to die.
One of the cells thought to be important in breaking down the blood-brain barrier are white blood cells called neutrophils, the natural scavengers of the blood stream. They are important in other conditions of the brain, such as in multiple sclerosis, but clinical trials in stroke aimed at these cells did not improve outcome.
Professor Britta Engelhardt
Researching a brighter future for stroke
After a stroke, a person’s immune system may be suppressed. It is thought that the brain causes this immunosuppression because it wants to protect itself. The brain is normally relatively isolated from the immune system by the blood-brain barrier, but once it is broken, there is a danger that brain tissue will be viewed as being ‘foreign’ and therefore the target of attack. We do not know how this happens, but researchers within the European Stroke Network are working towards piecing this together.
Our immune systems primarily protect us from infections. With a suppressed immune system, the brain may be protected from attack, but it leaves people more exposed to infection.
11
‘In stroke these cells do not seem to cause damage in the brain as they seem to only get as far as the moat,’ says Professor Engelhardt. ‘We were therefore back to square one and needed to go back to the laboratory and determine what exactly these cells are doing.’
This is why the European Stroke Network is so important. It brings together a new mix of scientists, experts in their own field, who work together in collaboration.
‘With our colleagues we have developed new models of the blood-brain barrier in the laboratory,’ Professor Engelhardt explains. ‘And when we recreated the conditions that happen in stroke, we found that instead of the endothelial cells that line the barrier being damaged as previously thought happened, these cells were remarkably unharmed.’
But when the researchers added to their model the cells that line the blood brain barrier on the brain side, called astrocytes, then they found that the barrier was broken down.
‘It appears that astrocytes are key cells in breeching the barrier in stroke. They produce molecules that cause the barrier to break down,’ she continues. ‘If we can identify what these molecules are, we can start to develop ways to protect the barrier.’
‘We are at the beginning of the journey,’ she comments. ‘We would like to get to a point of developing new treatments for people who have a stroke, but we
first need to spend more time in the laboratory understanding the mechanisms that break the blood brain barrier in stroke.’
The blood-brain barrier makes delivering drugs into the brain difficult. But delivery of drugs to prevent the break-up of the barrier is much easier. Professor Engelhardt believes that once treatments have been identified, they can easily be delivered at the same time that the blood supply is restored.
Stroke research has been lagging behind other conditions of the brain, such as multiple sclerosis. One of the stumbling blocks in stroke research in the past has been the lack of involvement of researchers from a wide range of disciplines. The European Stroke Network has overcome this block, and Professor Engelhardt believes that this provides unique added value.
One of the barriers to understanding the biological mechanisms in stroke has been that researchers have been using different techniques and models of stroke. This means that the results from different laboratories are difficult to compare. The European Stroke Network is taking a coordinated approach with different laboratories using common approaches that should speed up the progress of research.
‘I was previously concentrating my research efforts in multiple sclerosis,’ says Professor Engelhardt. ‘And when I was approached to be a member of the European Stroke Network, I must admit that I needed some persuasion. But I am now inspired, and plan to remain in stroke research as I feel I can contribute by bringing a different perspective.’
The European Stroke Network
One of the major obstacles in stroke treatment is how to get drugs into the brain. The brain is protected by
the blood-brain barrier that lines the small blood vessels and prevents passage of many larger molecules. While it is very effective in keeping the brain safe and in a controlled environment, it does not allow over 95 per cent of all current medicines to pass through to the brain.
‘There are a very limited number of drugs that we can currently use to treat problems in the brain because of the blood-brain barrier,’ says Professor Stephen Meairs.
‘We need to find new ways to deliver drugs into the brain if we are going to protect nerve cells and repair the damage that stroke can do.’
It is to the relatively new science of nanotechnology that Professor Meairs and his team at the University Hospital Mannheim in Germany have turned for inspiration and support. The idea is to use extremely small particles to deliver drugs through the blood-brain barrier, but still leave the barrier intact.
‘We have developed very tiny bubbles of gas covered with a membrane that we can stick drugs or molecules such as growth factors to,’ says Professor Meairs. ‘But the most exciting thing about these micro-bubbles is that we can target them where we want to the blood-brain barrier.’
Using a focused low-level beam of ultrasound to the blood-brain barrier, the researchers can open it up to deliver the important payload of drugs on the microbubbles to the brain. The blood-brain barrier is not damaged in this process.
‘This means that we can target drugs to a particular part of the brain,’ Professor Meairs explains. ‘We can pinpoint exactly where we want to deliver the drug, get the right concentration of drug to where we want it, and reduce any unwanted side effects.’
Another approach being tested is to use tiny biodegradable nanoparticles with drugs attached to them. Also on the particle’s surface are receptors that attach, like a lock and key, onto the blood-brain barrier.
‘This is our Trojan horse approach,’ explains Professor Meairs. ‘We use the receptors on the surface of the particles to trick the blood-brain barrier into taking up these particles inside the barrier and delivering them intact to the other side.’
While this approach does not allow the targeting of the delivery of drugs to a specific area of the brain, it does effectively allow drugs to get into the brain.
Professor Meairs’ team are using this approach to deliver growth factors that can recruit brain stem cells and stimulate them into forming new nerve cells to repair the brain after a stroke.
‘Imagine the number of drugs that are already available for stroke but we cannot use at present because of the blood-brain barrier,’ he says. ‘And we are discovering new potential treatments all the time.
Delivering drugs to the brainAs we discover new treatments to protect and repair the brain after a stroke, researchers in the European Stroke Network are developing the best ways to target drugs into the brain.
12
13Researching a brighter future for stroke
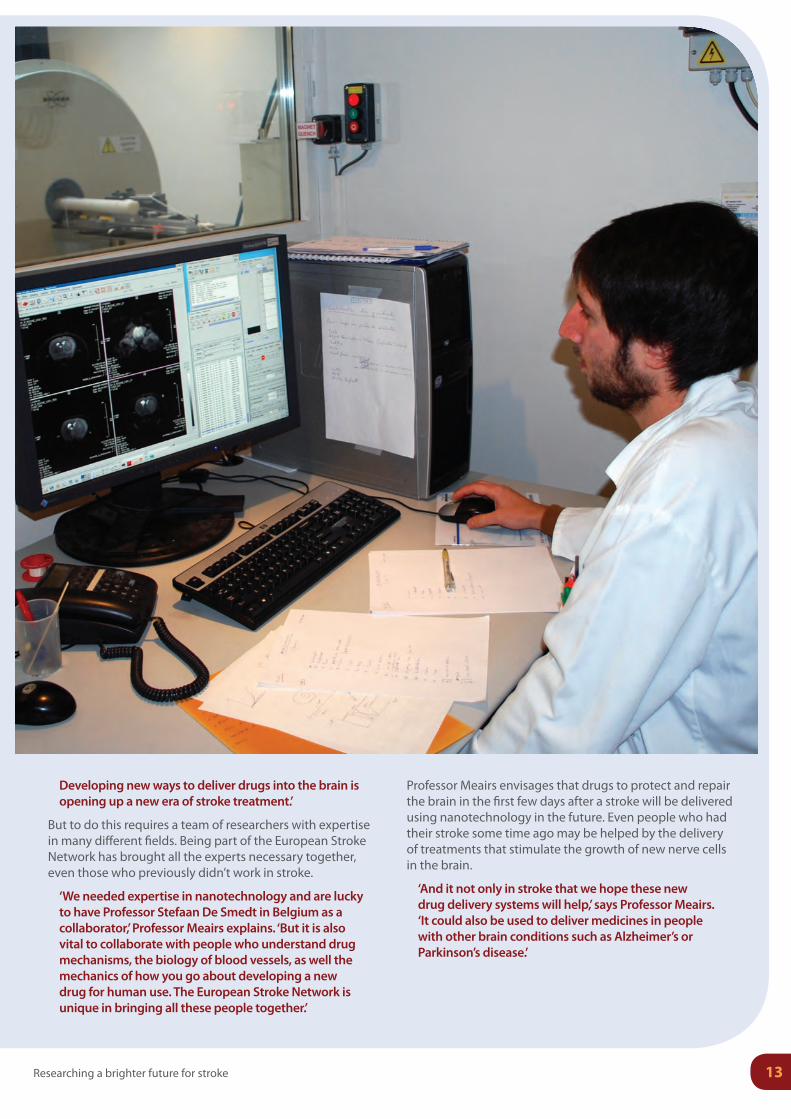
Developing new ways to deliver drugs into the brain is opening up a new era of stroke treatment.’
But to do this requires a team of researchers with expertise in many different fields. Being part of the European Stroke Network has brought all the experts necessary together, even those who previously didn’t work in stroke.
‘We needed expertise in nanotechnology and are lucky to have Professor Stefaan De Smedt in Belgium as a collaborator,’ Professor Meairs explains. ‘But it is also vital to collaborate with people who understand drug mechanisms, the biology of blood vessels, as well the mechanics of how you go about developing a new drug for human use. The European Stroke Network is unique in bringing all these people together.’
Professor Meairs envisages that drugs to protect and repair the brain in the first few days after a stroke will be delivered using nanotechnology in the future. Even people who had their stroke some time ago may be helped by the delivery of treatments that stimulate the growth of new nerve cells in the brain.
‘And it not only in stroke that we hope these new drug delivery systems will help,’ says Professor Meairs. ‘It could also be used to deliver medicines in people with other brain conditions such as Alzheimer’s or Parkinson’s disease.’
The European Stroke Network14
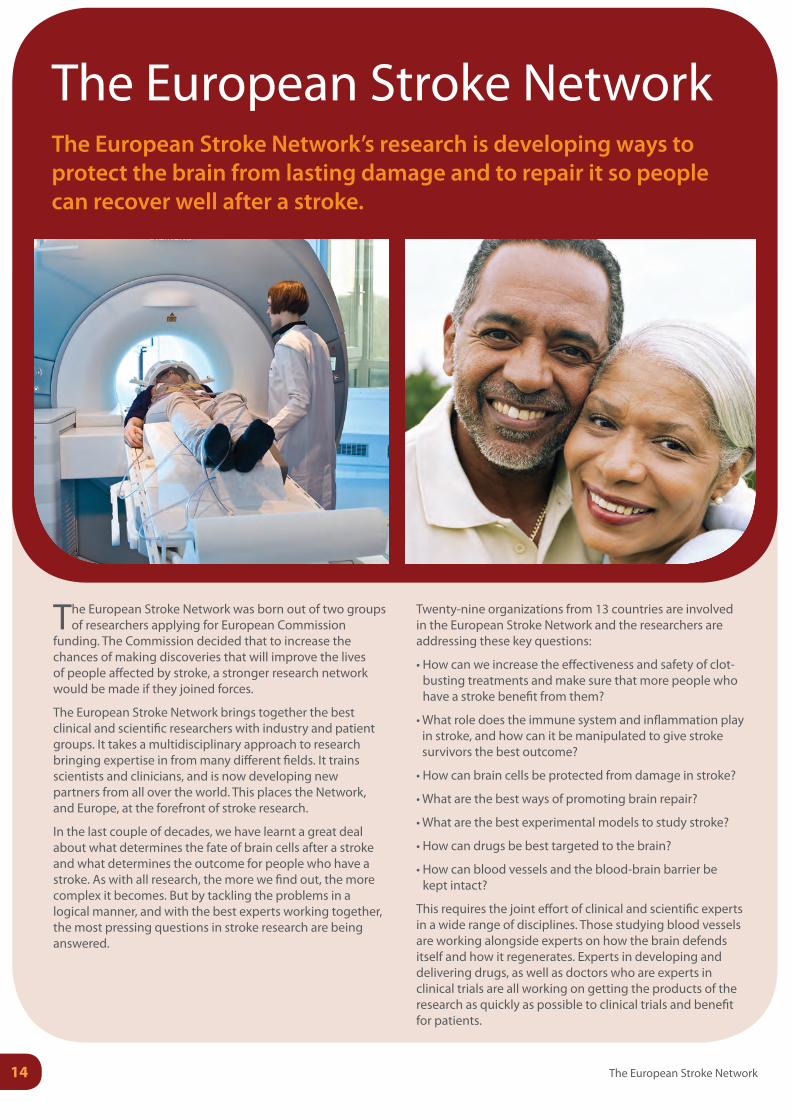
The European Stroke Network was born out of two groups of researchers applying for European Commission
funding. The Commission decided that to increase the chances of making discoveries that will improve the lives of people affected by stroke, a stronger research network would be made if they joined forces.
The European Stroke Network brings together the best clinical and scientific researchers with industry and patient groups. It takes a multidisciplinary approach to research bringing expertise in from many different fields. It trains scientists and clinicians, and is now developing new partners from all over the world. This places the Network, and Europe, at the forefront of stroke research.
In the last couple of decades, we have learnt a great deal about what determines the fate of brain cells after a stroke and what determines the outcome for people who have a stroke. As with all research, the more we find out, the more complex it becomes. But by tackling the problems in a logical manner, and with the best experts working together, the most pressing questions in stroke research are being answered.
Twenty-nine organizations from 13 countries are involved in the European Stroke Network and the researchers are addressing these key questions:
• How can we increase the effectiveness and safety of clot-busting treatments and make sure that more people who have a stroke benefit from them?
• What role does the immune system and inflammation play in stroke, and how can it be manipulated to give stroke survivors the best outcome?
• How can brain cells be protected from damage in stroke?
• What are the best ways of promoting brain repair?
• What are the best experimental models to study stroke?
• How can drugs be best targeted to the brain?
• How can blood vessels and the blood-brain barrier be kept intact?
This requires the joint effort of clinical and scientific experts in a wide range of disciplines. Those studying blood vessels are working alongside experts on how the brain defends itself and how it regenerates. Experts in developing and delivering drugs, as well as doctors who are experts in clinical trials are all working on getting the products of the research as quickly as possible to clinical trials and benefit for patients.
The European Stroke NetworkThe European Stroke Network’s research is developing ways to protect the brain from lasting damage and to repair it so people can recover well after a stroke.
15Researching a brighter future for stroke
Member organizations and project leaders of the European Stroke Network
August Pi i Sunyer Institute for Biomedical Research, Spain (Dr. Anna M. Planas)Boehringer Ingelheim, Germany (Prof. Wolfgang Eisert)Charité - University Medicine Berlin, Germany (Prof. Ulrich Dirnagl, Prof. Matthias Endres)Cochin Institute (INSERM), France (Dr. Pierre-Olivier Couraud)Cyceron (INSERM), France (Prof. Denis Vivien)FIRC Institute of Molecular Oncology Foundation, Italy (Prof. Elisabetta Dejana)GABO:mi, Germany (Birgit Fuchs)Ghent University, Belgium (Prof. Stefaan De Smedt)Hospital District of Helsinki and Uusimaa, Finland (Prof. Turgut Tatlisumak)Karolinska Institute, Sweden (Prof. Nils Wahlgren)Lund University, Sweden (Prof. Tadeusz Wieloch)Nencki Institute of Experimental Biology, Poland (Prof. Leszek Kaczmarek)NsGene, Denmark (Dr. Lars U. Wahlberg)PAION, Germany (Prof. Karl-Uwe Petersen)QuickCool AB, Sweden (Mr. Lennart Sjölund)SOLVO Biotechnology, Hungary (Dr. Péter Krajcsi)Stroke Alliance for Europe, Belgium (Dr. Markus Wagner)SYGNIS Bioscience, Germany (Dr. Armin Schneider)University Medical Center Utrecht, Netherlands (Dr. Rick M. Dijkhuizen)University of Artois, France (Prof. Roméo Cecchelli)University of Bern, Switzerland (Prof. Britta Engelhardt)University of Cambridge, UK (Prof. Jean-Claude Baron)University of Eastern Finland, Finland (Prof. Jari Koistinaho)University of Heidelberg, Germany (Prof. Stephen Meairs, Prof. Markus Schwaninger)University of Manchester, UK (Prof. Nancy Rothwell)University of Münster, Germany (Prof. Lydia Sorokin)University of Saarland, Germany (Prof. Ulrich Laufs)University of Zurich, Switzerland (Prof. Martin Schwab)Vall d’Hebron University Hospital, Spain (Dr. Joan Montaner)
16 The European Stroke Network
For further information on the European Stroke Network please visit the ESN website at
www.europeanstrokenetwork.eu
or contact Dr. Laszlo Szabo, scientific project manager, at