Embed Size (px)
Citation preview

RESEARCH STUDY ON NECK INJURY LESSENING WITH ACTIVE HEAD RESTRAINT USING HUMAN BODY FE MODEL
Yuichi Kitagawa*, Tsuyoshi Yasuki*, Junji Hasegawa*
*Toyota Motor Corporation, Japan
ABSTRACT According to the traffic accident data in Japan, the number of rear impacts is the largest among the
various car crash scenarios on the road. Neck injury due to low speed rear impacts continues to be a significant issue in terms of social cost. Although the precise injury mechanism is still not determined clearly, it is commonly recognized that a relative motion between the head and torso could be one of the factors causing the injury. NIC and some other indicators have been developed to assess injury risk and some are used in laboratory tests. Recent studies focus on the joint capsules as a potential site of neck pain. Experiments were conducted to evaluate Joint Capsule Strain under simulated loading conditions. Various seat systems have been developed aiming to help reduce the injury risk. There have been two approaches used in reducing the relative motion between the head and torso. One is to allow the occupant torso to sink into the seatback, and the other is to support the head as early as possible. The second approach has led to the development of active head restraint systems. The active head restraint system is designed to move the head restraint forward (closer to the occupant’s head) when activated in rear impacts. The effectiveness of such systems is verified evaluating the dummy readings (indicator values) and sometimes investigating the field data. The authors previously conducted a study using a human body finite element (FE) model to estimate the effectiveness of a fixed head restraint system in terms of both NIC and Joint Capsule Strain. The results confirmed that seat design factors such as the forward location of the head restraint could help lower the indicator values. This study investigates the effectiveness of the active head restraint system in reducing both NIC and Joint Capsule Strain. A human FE model is used to simulate the occupant head and neck motion with the different head restraint systems. The study also analyzes the cervical vertebral motions to investigate the function of the active head restraint system in correlation with the strain growth in the joint capsules Keywords: Rear impacts, Neck injury, Seats, Active Head Restraint
JAPANESE TRAFFIC ACCIDENT DATA shows an increasing trend of rear impacts and that the number of rear impacts is the highest among the various car crash scenarios in Japan followed by collisions at intersections. Most of them are relatively low speed impacts and injury outcome is generally less severe, in terms of AIS coding. However, the insurance companies report that the claims of neck pain such as whiplash injury are the majority of total automotive insurance costs. Despite the frequency of neck injury in the field, its mechanism is not clearly determined yet. A common understanding is that a relative motion between the head and the torso could contribute to the cause of injury. Hypotheses were made focusing on hyperextension of the neck, stretch of the cervical muscles and the pressure gradient in the spinal canal. Recent studies assume that the cervical facet joint is a potential site of neck pain. Deng et al. (2000) analyzed the kinematics of the cervical vertebrae of a Post Mortem Human Subject (PMHS) using a high speed X-ray camera, while Ono et al. (1997) conducted a cineradiographic analysis on living human subjects (volunteers) in simulated rear impacts. They hypothesized that impingement in the facet joint could be a possible cause of pain in rear impacts. Yang et al. (1996) noted that shear motion in the cervical joint could attribute the pain to the joint capsules. Yoganandan et al. (2001) also supported the facet joint impingement mechanism as a possible mechanism of neck injuries. Winkelstein et al. (1999) examined the deformation of the joint capsules related to the relative motion between adjacent vertebrae. They observed an increase of the principal strain in the capsules when pretorque was applied, while
IRCOBI Conference – Bern (Switzerland) – September 2008 381

bending itself did not raise the strain up to a harmful level. There are some other studies that analyzed the facet joint motion (Sundararajan et al., 2004, Lee et al., 2004). The authors of this paper have conducted a study using a human body FE model to simulate head and neck kinematics of an occupant during a rear impact and to estimate tissue strain in the cervical joint capsules (Kitagawa et al., 2006). The study showed that the relative acceleration and displacement are generated after the impact and the joint capsule strain more correlated to the relative displacement. Another study on seat design factors found that the stiffness of the reclining joint, the location of the head restraint and the head restraint supporting stiffness are relatively important to help lower NIC and Joint Capsule Strain (Kitagawa et al., 2007).
On the other hand, research efforts have been made in developing criteria to assess neck injury risk. Boström et al. (1996) proposed a criterion called NIC based on their assumption that the pressure gradient in the spinal fluid could be a cause of injury. The indicator evaluates the amplitude of relative acceleration and velocity between the head and torso in its formula, and it has become a popular indicator in laboratory tests and assessment tests. There are some other indicators proposed for injury assessment, neck shear/tension force, moment, Nkm LNL, Rebound Velocity, Head Restraint Contact Time and T1 acceleration (Muser, 2000, Schmitt, 2001, Heitplatz, 2003). Because the injury mechanism is not clearly determined yet, multiple indicators are evaluated in assessment tests. Product seat systems have been developed aiming to help lower the neck injury risk in terms of the proposed criteria. A common approach is to locate the head restraint forward, expecting a shorter Head Restraint Contact Time, in order to reduce the relative motion between the head and torso. Other challenges are, for example, to soften the upper part of the seatback allowing the torso to sink (Sekizuka, 1998), and to design the reclining joint to yield absorbing energy (Jakobsson, 2004). An advanced technology in this area is the active head restraint system, where the head restraint is moved forward (closer to the head) when a rear impact occurs. Various systems have been developed by car makers. A popular approach is to activate the head restraint with mechanical linkages. Such product seat systems are often called “anti-whiplash” systems. Kullgren et al (2007) conducted a study investigating the effectiveness of such systems based on the Swedish accident data. The results showed that the cars fitted with the advanced anti-whiplash systems had 50% lower risk of neck injuries leading to long-term symptoms.
This study examined the effectiveness of the active head restraint system using a human body FE model. Considering the recent studies on the neck pain mechanism, Joint Capsule Strain was evaluated as well as NIC. The strain growth was attributed to the vertebral displacement, and the magnitude of the displacement was correlated with the interaction between the head and the head restraint. The study also focused on the alignment of the head restraint motion with respect to the facet joint surface, assuming its contribution to the strain growth.
METHOD HUMAN BODY FE MODEL: The study uses a human body FE model named the Total Human
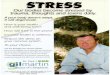
Model for Safety (THUMS), which was jointly developed by Toyota Motor Corporation and Toyota Central Research and Development Laboratory. THUMS represents an average-sized adult male person (175 cm and 77 kg) aiming to simulate body kinematics and responses during car crashes. The model includes all the bony parts and major ligaments so that the model can simulate a real human subject. Joint modeling is important for simulating body kinematics during crashes. The ligaments were modeled connecting bones to bones and contacts were defined between them. This modeling method simulates realistic joint motions and calculates force transmission through the joint. Each body part also imitates the human tissue material in terms of mechanical response against external loading. Such material properties are defined based on the literature data (Yamada, 1970, Yoganandan et al., 1998), while the geometry of the body parts refers to human body databases. The model also includes skin, fat, muscle, brain and internal organs, and most of them are simplified as solid parts in THUMS. The neck muscles are modeled with 1D discrete elements to simulate their passive responses against stretch. The cervical facet joint capsules are newly introduced into the model for this study in order to calculate Joint Capsule Strain. The model includes approximately 60,000 nodes and 80,000 elements, and it runs on a commercial finite element code LS-DYNATM. Figure 1 is a close-up view of the neck part with the joint capsules added. The
382 IRCOBI Conference – Bern (Switzerland) – September 2008

major ligaments included are: the anterior longitudinal ligament (ALL), the posterior longitudinal ligament (PLL), the ligamentum flavum (LF), the interspinous ligament (ITL), the supraspinous ligaments (SSL), and the intertransverse ligament (ISL). Relative motion between adjacent vertebrae generally occurs around the facet joints located on the right and left sides of the neural arch. The joints are covered with the joint capsules, and the capsule tissues were modeled with membrane elements. The model also includes the synovial fluid (represented with solid elements) which may affect the magnitude of joint capsule strain due to its uncompressive property. Internal contacts in the cervical region such as vertebra-to-vertebra or vertebra-to-ligament are also defined as treated in other joints. The surface-to-surface and/or node-to-surface algorisms in LS-DYNATM are adopted to handle such contacts.
MODEL VALIDATION: The model has been validated against human impact responses reported in
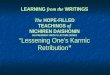
the literature (Iwamoto et al., 2002). The mechanical responses of the model against external loading were verified part by part such as impacts to the head, thorax, abdomen, pelvis and lower extremity. The responses were compared to those of Post Mortem Human Subject (PMHS) in the literatures. The model responses were found to be within the PMHS corridors. For rear impact simulations, the authors previously validated the model in its whole body motion and at the neck component level (Kitagawa et al., 2006). Head and neck kinematics in a whole body motion were verified comparing to the literature data with human volunteer subjects (Ono et al., 1997). An inclined sled system was used to generate low velocity rear impact, and head and neck kinematics were captured with a high speed X-ray (Figure 2). A numerical simulation was conducted using the THUMS model duplicating the test condition. Comparisons of rotations of the vertebral bodies found that the model well simulated the human head and neck responses, although it did not represent muscular effects working to reduce the head-neck motion after 100 ms (Figure 3). The calculated time history curve of the head rotation was shifted earlier compared to that of the test. This is possibly because of a difference in their initial head orientations. Another validation examined the validity of the cervical joint model in predicting Joint Capsule Strain (Kitagawa et al., 2008). Siegmund et al. (2000) conducted quasi-static loading tests where C3-C4 components segmented out from PMHS were subjected to shear and compressive loadings (Figure 4). The anterior-posterior displacement and the sagittal rotation of C3 with respect to C4 were monitored. Joint Capsule Strain was estimated from relative displacement among photo markers posted to the capsule tissue. A corresponding part was extracted from the THUMS neck, and then equivalent boundary conditions were applied to the model. The anterior-posterior displacement and sagittal rotation were calculated from nodal displacement in the model and Joint Capsule Strain was directly output from elements representing the capsule tissue. Figure 5 compares the test data and the simulation results, where the test data were plotted as corridors and the simulation results were plotted as curves. A comparison confirmed that the calculated Joint Capsule Strain (curves) were within the test corridors. These validation results indicate that the model can simulate vertebral motion and estimate joint capsule strain.
Figure 1. THUMS Occupant Model and Joint Capsule Modeling.
Cervical Vertebrae
Joint CapsuleHead
Neck
Figure 1. THUMS Occupant Model and Joint Capsule Modeling.
Cervical Vertebrae
Joint CapsuleHead
NeckCervical Vertebrae
Joint CapsuleHead
Neck
IRCOBI Conference – Bern (Switzerland) – September 2008 383

Figure 2. Inclined Sled Test System (Ono et al., 1997).
Energy Absorber
Sled
Inclined Rails
Subject
Figure 2. Inclined Sled Test System (Ono et al., 1997).
Energy Absorber
Sled
Inclined Rails
Subject
Figure 3. Comparison of Head and Vertebral Rotations between THUMS and Volunteer.
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[HEAD]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[T1]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C3]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C4]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C5]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C6]
VolunteerTHUMS
Figure 3. Comparison of Head and Vertebral Rotations between THUMS and Volunteer.
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[HEAD]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[HEAD]
VolunteerTHUMS
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[T1]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[T1]
VolunteerTHUMS
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C3]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
00.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C3]
VolunteerTHUMS
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C4]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C4]
VolunteerTHUMS
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C5]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C5]
VolunteerTHUMS
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C6]
VolunteerTHUMS
0.0 0.1 0.2
60
50
40
30
20
10
0
Rotation Angle (deg)
Time (sec)
[C6]
VolunteerTHUMS
VolunteerTHUMS
384 IRCOBI Conference – Bern (Switzerland) – September 2008

H
L
PosteriorShear Force
Measuring Points
Rotation
Displacement
C3
Compressive Force
Joint Capsule
C4
Figure 4. Loading Test on C3-C4 Component.(Siegmund et al., 2000)
H
L
H
L
PosteriorShear Force
Measuring Points
Rotation
Displacement
C3
Compressive Force
Joint Capsule
C4C4
Figure 4. Loading Test on C3-C4 Component.(Siegmund et al., 2000)
-2
-1
0
1
2
3
4
0 25 50 75 100 125 150
-1
0
1
2
3
4
5
0 25 50 75 100 125 150
0
10
20
30
40
0 25 50 75 100 125 150
Posterior Shear Force (N)
A-P
Disp
lace
men
t [m
m]
Sagi
ttal
-Rot
atio
n [d
eg]
Posterior Shear Force (N)
Join
t Cap
sule
Str
ain
Posterior Shear Force (N)
Figure 5. Comparison of A-P Displacement, Sagittal Rotation and Joint Capsule Strain between PMHS and THUMS.
PMHS THUMS
-2
-1
0
1
2
3
4
0 25 50 75 100 125 150
-2
-1
0
1
2
3
4
0 25 50 75 100 125 150
-1
0
1
2
3
4
5
0 25 50 75 100 125 150
-1
0
1
2
3
4
5
0 25 50 75 100 125 150
0
10
20
30
40
0 25 50 75 100 125 150
0
10
20
30
40
0 25 50 75 100 125 150
Posterior Shear Force (N)
A-P
Disp
lace
men
t [m
m]
Sagi
ttal
-Rot
atio
n [d
eg]
Posterior Shear Force (N)
Join
t Cap
sule
Str
ain
Posterior Shear Force (N)
Figure 5. Comparison of A-P Displacement, Sagittal Rotation and Joint Capsule Strain between PMHS and THUMS.
PMHS THUMS
IRCOBI Conference – Bern (Switzerland) – September 2008 385

SEAT MODEL: Two seat models were prepared for rear impact simulations. The first one is a prototype seat model with a fixed head restraint. Its design concept is called “WIL” introduced by Sekizuka et al. (1998), which reduces the relative motion between the head and torso allowing the torso to sink into the seatback. The effectiveness of this concept was previously examined in laboratory tests and with FE simulations (Sawada et al., 2005). The other one is a prototype seat equipped with an active head restraint system. The design concept is based on the WIL but is enhanced introducing an activation system explained later. In both models, the geometrical features of the seat structure were incorporated, including the construction of components and their mechanical properties. The material properties of the seat frames and cushion foams were also incorporated. Contacts between the parts were handled by the algorism implemented in the LS-DYNATM. Figure 6 shows overall views of the seat models. Each model was validated in advance so that its mechanical response against external loading simulated that in a physical experiment. A typical external load in rear impacts is a rearward force from the occupant torso to the seatback. Rotational stiffness of the reclining joint is thought to be one of the major factors. The joint stiffness property in the seat model was carefully adjusted to simulate actual seatback response. The active head restraint system in this study works to move the head restraint forward and upward. Such a motion is generated along guiding tubes where the head restraint supporting poles are inserted. The system is activated when the occupant pelvis loads the lower unit implemented in the seatback during a rear impact. The displacement of the lower unit is transmitted to the upper unit by attached cables, and the upper unit lifts the supporting poles (Figure 7). The model precisely simulates the linkage mechanism, and its reaction against loading was carefully verified.
Figure 6. Prototype Seat Models.
[Seat Model with Fixed Head Restraint] [Seat Model with Active Head Restraint]
Figure 6. Prototype Seat Models.
[Seat Model with Fixed Head Restraint] [Seat Model with Active Head Restraint]
Figure 7. Active Head Restraint System.
Head Restraint
Upper Unit
Cable
Lower Unit
Figure 7. Active Head Restraint System.
Head Restraint
Upper Unit
Cable
Lower Unit
386 IRCOBI Conference – Bern (Switzerland) – September 2008

REAR IMPACT SIMULATION: Rear impact simulations were conducted using the THUMS occupant model and the seat models. Figure 8 shows the simulation model. The posture of THUMS was adjusted so that it takes a natural sitting posture on the seat model, basically following the seating procedure in neck assessment tests. The adjustment was performed applying gravity in the downward and rearward direction, taking into account contacts between the THUMS body parts and the seat cushion surface. A small gap was allowed between the head and the head restraint, which was basically equal to the amount resulting with the 3D mannequin or the BioRID dummy. After the posture was adjusted, rear impact simulations were conducted. Each seat model was mounted on a rigid floor plate and the floor plate was accelerated assuming a rear impact. According to the research on rear collision data by the Ministry of Land, Infrastructure and Transport of Japan (2002), the average delta-V for rear impacts was around 16 km/h, which is more severe than roughly 60 percent of all rear collisions. A delta-V of 25 km/h covers approximately 90 percent of all rear collisions. This study focuses on the higher delta-V condition as a challenge to examine the benefit of the latest head restraint systems, although the authors have conducted simulation studies at delta-V’s of both 16 and 25 km/h. In the following rear impact simulations, a triangular acceleration pulse representing an impact at a delta-V of 25 km/h was applied to the model (Figure 9). In the FE input data, the impact condition was defined as a velocity boundary condition applied to the floor plate, converting the acceleration pulse to the velocity time history. An explicit integration scheme was used for the rear impact simulations, with an integration time-step determined from the material density and the stiffness (without mass scaling), and was terminated 200 ms after impact.
Figure 8. Model for Rear Impact Simulation (Fixed Head Restraint).
THUMS
Floor
Seat
Rear ImpactAcceleration
Figure 8. Model for Rear Impact Simulation (Fixed Head Restraint).
THUMS
Floor
Seat
Rear ImpactAcceleration
180
120
60
0
160
100
140
80
4020
120600 100804020
Figure 9. Triangle Acceleration Pulse for Input (delta-V = 25 kmh).
Acceleration (m/s2)
Time (ms)
180
120
60
0
160
100
140
80
4020
120600 100804020
Figure 9. Triangle Acceleration Pulse for Input (delta-V = 25 kmh).
Acceleration (m/s2)
Time (ms)
IRCOBI Conference – Bern (Switzerland) – September 2008 387

Contacts between the occupant body and the seat were again handled with the algorism in the LS-DYNATM. The contact search area was divided into four regions for the analysis. One was between the head and the head restraint, the second one was between the upper torso and the seatback surface, the third one was between the pelvis and the seatback surface, and the last one was between the lower extremities (buttock, thighs and calves) and the seat cushion surface. A set of nodes and elements was defined in advance, where time history responses such as displacement, velocity, acceleration and strain were output for analysis. The surface-to-surface algorism in the LS-DYNATM was used for contact calculations between the occupant body and the seat surface. The algorism automatically outputs the contact force as an integrated amount for each defined region. The calculated data were output to ASCII files at a time interval of 0.1 ms, and then processed with Post-Processing Software for plotting. The authors previously conducted a parametric study varying seat design factors to investigate the correlation among neck injury indicators (Kitagawa et al., 2007). The result showed that NIC represented the amplitude of relative acceleration between the head and the torso, while Joint Capsule Strain grew with the magnitude of neck extension. This study uses these two indicators in estimating neck injury risk. NIC is calculated using the following equation: where AHead and AT1 are the accelerations measured at the head (center of gravity) and T1 respectively, and VHead and VT1 are the velocities at the head and T1. In general, the maximum indicator values are taken for evaluation in injury assessment. Joint Capsule Strain is directly output from the element forming the capsule tissues. The maximum peaks in time history curves from all the capsule elements are compared and the largest strain value is used for evaluation.
RESULTS HEAD AND NECK KINEMATICS: The head and neck kinematics of the THUMS occupant model
were analyzed in the case of the seat equipped with a fixed head restraint. Figure 10 shows the entire motion of the occupant model in frames at 0, 50, 100 and 130 ms after the initiation of impact. Although the simulation was conducted applying a forward acceleration pulse reproducing the actual rear impact scene, the paper describes the occupant motion in the vehicle coordinate system (on the rigid floor) for a better understanding. There is a gap between the head and the head restraint at the initial state (0 ms), while the lower torso (buttock) contacts the seatback in the initial seating position. At the beginning of impact, the torso and the head start moving rearward, but the torso is immediately supported by the seatback, while the head moves free until it contacts the head restraint. In this simulation case, the head to head restraint contact occurred around 70 ms. The seatback frame deforms rearward as the occupant body loads into it. The magnitude of deformation reaches its maximum peak around 100 ms. The torso of the model moves in the forward direction at this point, which is called a ‘rebound’ motion. The head still moves back for a while as the head restraint deformation reaches its maximum peak at around 130 ms.
NIC=0.2*(AT1-AHead)+(VT1-VHead)2
Figure 10. Occupant (THUMS) Motion in Rear Impact with Fixed Head Restraint.
[0 ms] [50 ms] [100 ms] [130 ms]
Figure 10. Occupant (THUMS) Motion in Rear Impact with Fixed Head Restraint.
[0 ms] [50 ms] [100 ms] [130 ms]
388 IRCOBI Conference – Bern (Switzerland) – September 2008

Then the head turns to move forward. Contact forces between the occupant body and the seat were examined. Figure 11 plots the contact forces calculated at the pelvis, torso and head portions of the model. The contact force at the pelvis rises first, followed by the torso and the head rises last. The magnitude of each peak force may be related to the mass of the corresponding body part and the contact area. The contact force at the pelvis is generated by the inertia of the lower body and the posterior side of the buttock contacts the lower part of the seatback. The torso also has a large contact area but the upper torso does not contact the seatback at the initial state (0 ms), resulting in a delay in the latter rise after 50 ms. The magnitude of the peak is relatively lower than that at the pelvis because of relatively smaller mass of the torso. The contact force at the head is much smaller due to its lighter mass. The peak for the head appears around 130 ms, corresponding to the timing of the maximum deformation of the head restraint, which is later than the other peaks. Figure 12 shows the horizontal accelerations calculated at the pelvis, T1 and head. The pelvis is accelerated first, as also observed in the contact force, because the lower torso contacts the seatback from beginning. The T1 acceleration rises almost at the same timing, but its increasing trend is not continuous, possibly due to a gap behind the upper torso and penetration into the seatback. Note that T1 is located at the upper end of the torso. The head is accelerated last. There is a small rise from 30 to 70 ms possibly due to a transmitted motion through the cervical spine. The acceleration rise is more prominent after 70 ms where the head contacts the head restraint surface. The T1 acceleration rises again after the head to head restraint contact. The timings of the acceleration peaks at the head and T1 are close to those of the contact forces, while the timing of the head acceleration peak appears around 100 ms which is earlier than that of the contact force around 130 ms. The amplitudes of the acceleration peaks are much closer to each other compared to the maximum magnitudes in the contact
0
2000
4000
6000
8000
0 50 100 150 200Time (ms)
Figure 11. Contact Forces at Pelvis, Torso and Head with Fixed Head Restraint.
Force (N)
PelvisTorsoHead
Contact0
2000
4000
6000
8000
0 50 100 150 200Time (ms)
Figure 11. Contact Forces at Pelvis, Torso and Head with Fixed Head Restraint.
Force (N)
PelvisTorsoHead
PelvisTorsoHead
Contact
0
50
100
150
200
250
300
0 50 100 150 200
Head
T1
Pelvis
Time (ms)
Figure 12. Accelerations at Pelvis, T1 and Head with Fixed Head Restraint.
Acceleration (m/s2)
0
50
100
150
200
250
300
0 50 100 150 200
Head
T1
Pelvis
Time (ms)
Figure 12. Accelerations at Pelvis, T1 and Head with Fixed Head Restraint.
Acceleration (m/s2)
IRCOBI Conference – Bern (Switzerland) – September 2008 389

forces. Figure 13 plots the time history curves of NIC and Joint Capsule Strain calculated from the simulation. The strain was calculated at all the cervical joints from OC-C1 to C7-T1. The maximum strain value was always found at the C6-C7 joint under the impact condition assumed in this study. A comparison of the time history curves indicates the difference in timing of their peaks. NIC reaches its maximum peak around 70 ms when the head contacts the head restraint. Joint Capsule Strain has its maximum peak around 140 ms, which is slightly later than the timing of the maximum deformation of the head restraint.
ACTIVE HEAD RESTRAINT: A rear impact simulation was also conducted using the seat model
equipped with the active head restraint system. Figure 14 shows a close-up view of the head and neck with the motion of the active head restraint during the rear impact. The frames were selected from the initial state (0 ms), 60 ms and 100 ms. There is a gap between the head and the head restraint at the initial state, as observed in the previous case. The seatback deforms as the occupant leans on it, and the head restraint tends to move away as a result. As the deformation mostly grows around the reclining joint located at the bottom of the seatback, the head restraint moves backward and downward. The active system moves the head restraint forward and upward. It contacts the occupant head around 60 ms cancelling the frame deformation in moving away. The system keeps supporting the head after the contact. The relative motion between the head and torso is not significant at 100 ms compared to that at 60 ms. The horizontal accelerations calculated at the pelvis, T1 and head were plotted in Figure 15. Similar to the previous case, the pelvis acceleration rises first, followed by the torso and the head. Note that the seat configuration and the mechanical property of the seatback structure are different from the model with the fixed head restraint. Likewise, the acceleration responses are different from the previous case. The prominent difference is that the amplitude of the head acceleration is relatively higher than the other two curves, because the active head restraint more greatly supported the occupant’s head. There is a small rise in the head acceleration right after 50 ms, which is possibly due to the T1 acceleration rise as similarly observed in the previous case. The T1 acceleration rises earlier but has a small stop and a decrease, then it increases again synchronizing with the head acceleration. A similar trend was observed in the previous case although the amplitude and timing were different. Figure 16 and 17 compare NIC and Joint Capsule Strain respectively between the two cases. There are two peaks in the NIC curve with the active head restraint system while the other case has only one. The maximum value is lower in the case with the active system. The difference in Joint Capsule Strain is relatively larger. The maximum peak appears around 100 ms and there is another but smaller peak around 140 ms, while only one peak was observed in the previous case.
0
5
10
15
20
25
30
0 50 100 150 200
0.00
0.05
0.10
0.15
0.20
0.25
0.30
NIC
JCS
Time (ms)Figure 13. Time History Curves of NIC and Joint Capsule Strain (C6-C7) with Fixed Head Restraint.
NIC (m2/s2) Joint Capsule Strain
0
5
10
15
20
25
30
0 50 100 150 200
0.00
0.05
0.10
0.15
0.20
0.25
0.30
NIC
JCS
Time (ms)Figure 13. Time History Curves of NIC and Joint Capsule Strain (C6-C7) with Fixed Head Restraint.
NIC (m2/s2) Joint Capsule Strain
390 IRCOBI Conference – Bern (Switzerland) – September 2008

Figure 14. Close-Up View of Head and Neck Motion with Active Head Restraint.
0 ms 60 ms 100 ms
Figure 14. Close-Up View of Head and Neck Motion with Active Head Restraint.
0 ms 60 ms 100 ms
0
50
100
150
200
250
300
0 50 100 150 200
Head
T1
Pelvis
Time (ms)
Figure 15. Accelerations at Pelvis, T1 and Head with Active Head Restraint.
Acceleration (m/s2)
0
50
100
150
200
250
300
0 50 100 150 200
Head
T1
Pelvis
Time (ms)
Figure 15. Accelerations at Pelvis, T1 and Head with Active Head Restraint.
Acceleration (m/s2)
0
5
10
15
20
25
0 50 100 150 200
Fixed
Active
Time (ms)Figure 16. Comparison of NIC between Fixed and Active Head Restraints.
NIC (m2/s2)
0
5
10
15
20
25
0 50 100 150 200
Fixed
Active
Time (ms)Figure 16. Comparison of NIC between Fixed and Active Head Restraints.
NIC (m2/s2)
IRCOBI Conference – Bern (Switzerland) – September 2008 391

DISCUSSION The relative acceleration term in the NIC formulation greatly affects its maximum value. Assuming
that the T1 acceleration has an increasing trend, the NIC value becomes lower as the contact timing is earlier. This is why the maximum (first) NIC value was lower in the case with the active head restraint system. The second NIC peak observed in that case possibly came from the head acceleration rise which was relatively milder than that in the other case with the fixed head restraint. The head restraint support structure of the active system could be relatively less stiff when compared to that in the fixed structure. The milder rise of the head acceleration resulted in another peak in the NIC curve. However, the amplitude of both peaks are lower than that of the single peak in the first case.
The mechanism of strain growth in the joint capsule was examined focusing on the vertebral motion. The study selected the C6-C7 unit as it showed the maximum strain value among the cervical joints from C1 to C7. The C6 motion was analyzed with respect to C7, converting the global X and Z-displacements to a local coordinate system defined along the facet joint surface. Figure 18 illustrates the C6-C7 unit showing the local coordinate system used for analysis. Z-displacement means a stretch in the joint while X-displacement corresponds to a shear motion in the defined coordinate system. While the contribution from these displacement components to the neck pain is not known, the study monitored them to better understand the vertebral motion. The calculated local X and Z-displacements with the fixed head restraint are shown in Figure 19 as time history curves, superimposed with the Joint Capsule Strain. The left axis indicates the magnitude of displacement while the right one means the magnitude of strain. The timing of the maximum peak of Joint Capsule Strain was close to that of X-displacement, while the first rise of strain synchronized with Z-displacement. Figure 20 shows the calculated displacements in the second case with the active head restraint system. The magnitudes of both displacements are smaller in this case compared to that in the previous case. A similar correlation was found between the peaks of strain and displacements, but the maximum strain peak appeared when Z-displacement reached its maximum peak. There is another strain peak synchronizing with that of X-displacement, but the magnitude is much smaller. It suggests that the magnitude of Joint Capsule Strain in the second case was lower mostly because of small X-displacement. Note that the facet joint surface is inclined around 45 degrees against the spinal column. The shear deformation (X-displacement) in the joint causes a posterior-inferior motion of C6 with respect to C7. The forward and upward motion of the active head restraint aligns with the direction of the shear deformation. The magnitude of Joint Capsule Strain can be reduced by supporting the head from the posterior-inferior side, that is, moving the head restraint forward and upward. The active
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0 50 100 150 200
Fixed
Active
Time (ms)
Figure 17. Comparison of Joint Capsule Strain (C6-C7) between Fixed and Active Head Restraints.
Joint Capsule Strain
0.00
0.05
0.10
0.15
0.20
0.25
0.30
0 50 100 150 200
Fixed
Active
Time (ms)
Figure 17. Comparison of Joint Capsule Strain (C6-C7) between Fixed and Active Head Restraints.
Joint Capsule Strain
392 IRCOBI Conference – Bern (Switzerland) – September 2008

X
Facet Joint Surface
C7
C6
Z
C6-C7 Unit
Spinal Column
Figure 18. Local Coordinate System for Vertebral Motion Analysis.
X
Facet Joint Surface
C7
C6
Z
C6-C7 Unit
Spinal Column
Figure 18. Local Coordinate System for Vertebral Motion Analysis.
0.0
0.2
0.4
0.6
0.8
1.0
0 50 100 150 200
0.00
0.05
0.10
0.15
0.20
0.25
0.30X-displ
Z-displ
JCS
Time (ms)
Figure 19. Local X and Z Displacements and Joint Capsule Strain (C6-C7) with Fixed Head Restraint.
Displacement(mm) Joint Capsule Strain
0.0
0.2
0.4
0.6
0.8
1.0
0 50 100 150 200
0.00
0.05
0.10
0.15
0.20
0.25
0.30X-displ
Z-displ
JCS
Time (ms)
Figure 19. Local X and Z Displacements and Joint Capsule Strain (C6-C7) with Fixed Head Restraint.
Displacement(mm) Joint Capsule Strain
0.0
0.2
0.4
0.6
0.8
1.0
0 50 100 150 200
0.00
0.05
0.10
0.15
0.20
0.25
0.30X-displ
Z-displ
JCS
Time (ms)
Figure 20. Local X and Z Displacements and Joint Capsule Strain (C6-C7) with Active Head Restraint.
Displacement(mm) Joint Capsule Strain
0.0
0.2
0.4
0.6
0.8
1.0
0 50 100 150 200
0.00
0.05
0.10
0.15
0.20
0.25
0.30X-displ
Z-displ
JCS
Time (ms)
Figure 20. Local X and Z Displacements and Joint Capsule Strain (C6-C7) with Active Head Restraint.
Displacement(mm) Joint Capsule Strain
IRCOBI Conference – Bern (Switzerland) – September 2008 393

head restraint system begins to activate when the pelvis pushes against the loading unit. The early rise and the relatively larger magnitude of contact force at the pelvis indicate that the pelvis force could be an improved trigger mechanism to activate the system. The timing of the head to head restraint contact became shorter; around 60 ms with the active system while 70 ms with the fixed head restraint. The head restraint keeps supporting the occupant head as long as the lower unit is loaded by the pelvis. Although the strain can grow past 100 ms in some circumstances, the active head restraint system presented in this study could support the head for a sufficient period of time.
Toyota had developed a seat design concept “WIL” to help reduce loading to the occupant neck during a rear impact. This technology has been applied to product seat designs since 1997, employing energy absorbing design features and head restraint located relatively forward compared to the seatback. The effectiveness of the seat system was examined through dummy tests and THUMS simulations, confirming that both NIC and Joint Capsule Strain indicated lower values (Sawada et al., 2005). According to the field study conducted by Kllugren et al. (2007), investigating actual rear collision database in Sweden, the WIL seats showed lower risk of neck injury compared to those without an anti-whiplash system. The active head restraint system presented in this study is an extension of the WIL Concept seat. The results of this study indicated that the active head restraint system could further help reduce the neck injury risk in low speed rear impacts.
LIMITATIONS The study has limitations, as in many studies with human body FE models. Although the head and
neck kinematics of the THUMS model were validated against the literature data, the number of data samples and loading conditions were limited. The study assumes that the model could simulate the human head and neck response even when loading conditions and seat models are changed. The lack of active muscle function brings another limitation in simulating living human responses. The model cannot mimic muscular contraction due to spinal reflex, which could resist against a sudden stretch of the muscle. The model possibly overestimates the magnitude of body movement in the later phase of impact. The mechanism of neck pain in the form of Joint Capsule Strain needs further studies from a neurophysiology point of view. It should be also studied how vertebral displacements in X and Z directions contribute to the neck pain. Based on all such limitations, the calculated Joint Capsule Strain as well as the NIC value should be treated comparatively rather than absolutely. The results and findings were mostly discussed in terms of the difference (increase or decrease) among the study cases. Future study will focus on more advanced modeling including active muscular responses and also incorporating the latest research findings.
CONCLUSIONS Rear impact simulations were conducted using a human body FE model, THUMS, representing an
average size male occupant. The cervical system including the facet joint capsules was incorporated to the model. The validity of the model was examined comparing its mechanical responses to those in the literature such as the whole body motion of the volunteer subject and the vertebral motion in the PMHS tests. Rear impact simulations were conducted using the validated THUMS model and two prototype seat models, one had a fixed head restraint and the other one was equipped with an active head restraint system. The active head restraint system works moving the head restraint forward and upward when the lower unit is loaded by the pelvis. The head and neck kinematics and responses were analyzed from the simulation results. The force and acceleration rose at the pelvis first, followed by T1 and the head. The early timing of force rise and its magnitude indicated that the pelvis force was a good trigger for the active head restraint system. The results showed that the head was supported earlier in a case with the active head restraint system, and both NIC and Joint Capsule Strain were lowered. The study also analyzed the mechanism of strain growth in the joint capsules. Relatively greater strain was observed in the direction of the facet joint surface, which was around 45 deg inclined to the spinal column. The forward and upward motion of the active head restraint was aligned with the direction of the joint deformation, and contributed to lower strain in the joint capsules. The results indicated that the active head restraint could help reduce
394 IRCOBI Conference – Bern (Switzerland) – September 2008

the neck injury risk, not only by supporting the head at an early timing but also through its trajectory stopping the joint deformation.
ACKNOWLEDGMENTS THUMS has been developed in collaboration with the Toyota Central Research and Development
Laboratory. The authors would like to thank Toyota Technical Development Corporation for its assistance with the modeling and simulation work.
REFERENCES Boström, O., M. Svensson, B. Aldman, H. Hansson, Y. Haland, P. Lovsund, T. Seeman, A. Suneson, A. Saljo and T. Ortengen. 1996. “A New Neck Injury Criterion Candidate Based on Injury Findings in the Cervical Spinala Ganglia after Experimental Neck Extension Trauma.” Proc. International Conference on the Biomechanics of Impacts. 123-136. Deng, B., P. Begeman, K. Yang, S. Tashman and A. King. 2000. “Kinematics of Human Cadaver Cervical Spine During Low Speed Rear-End Impacts.” Stapp Car Crash Journal 44: 171-188. Hasegawa, J. 2004. “A Study of Neck Soft Tissue Injury Mechanisms During Whiplash Using Human FE Model.” Proc. International Conference on the Biomechanics of Impacts. 321-322. Iwamoto, M., Y. Kisanuki, I. Watanabe, K. Furusu, K. Miki and J. Hasegawa. 2002. “Development of a Finite Element Model of the Total Human Model for Safety (THUMS) and Application to Injury Reconstruction.” Proc. International Conference on the Biomechanics of Impacts. 31-42. Jakobsson L. 2004. “Field analysis of AIS1 neck injuries in rear end car impacts- injury reducing effect of WHIPS.” Thesis Chalmers University of Technology, Göteborg, Sweden. Japanese National Police Agency. 2004. “Traffic Green Paper 2003” (in Japanese). 1-23. Kitagawa, Y., T. Yasuki and J. Hasegawa. 2006. “A Study of Cervical Spine Kinematics and Joint Capsule Strain in Rear Impacts Using a Human FE Model.” Stapp Car Crash Journal 50: 545-566. Kitagawa, Y., T. Yasuki and J. Hasegawa. 2007. “Consideration of Possible Indicators for Whiplash Injury Assessment and Examination of Seat Design Parameters using Human FE Model.” 07-0093. 20th ESV Conference. Kitagawa, Y., T. Yasuki and J. Hasegawa. 2008. “A Study of Head and Neck Kinematics in Rear Impact and Whiplash Injury Predictors using Human FE Model.” World Congress on Neck Pain. Kraft, R., A. Kullugren, A. Ydenius, O. Bostrom, Y. Haland and C. Tingvall. “Rear Impact Neck Protection by Reducing Occupant Forward Acceleration – A Study of Cars on Swedish Roads Equipped with Crash Recorders and a New Anti-Whiplash Device.” Proc. International Conference on the Biomechanics of Impacts. 221-231. Lee, K., Davis, M., Mejilla, R. and Winkelstein, B. 2004. “In Vivo Cervical Facet Capsule Distraction: Mechanical Implications for Whiplash and Neck Pain.” Stapp Car Crash Journal 48: 373-395. Lu, Y., C. Chen, S. Kallakuri, A. Patwardhan and J. Cavanaugh. 2005. “Neural Response of Cervical Facet Joint Capsule to Stretch: A Study of Whiplash Pain Mechanism.” Stapp Car Crash Journal 49: 49-66. Ministry of Land, Infrastructure and Transport. 2002. The 3rd Car Safety Symposium. Kullgren, A., Krafft, M., Lie, A. Tingvall, C. 2007. “The Effect of Whiplash Protection Systems in real-Life Crashes and Their Correlation to Consumer Crash Test Programmes.” 07-0468. 20th ESV Conference.
IRCOBI Conference – Bern (Switzerland) – September 2008 395

Ono, K. and K. Kaneoka. 1997. “Motion Analysis of Human Cervical Vertebrae During Low Speed Rear Impacts by the Simulated Sled.” Proc. International Conference on the Biomechanics of Impacts. 223-237. Sawada, M., Hasegawa, J. 2005. “Development of New Whiplash Prevention Seat.” 05-0288 19th ESV Conference. Sekizuka, M. 1998.” Seat Designs for Whiplash Injury Lessening. “ 98-S7-O-06 16th ESV Conference. Siegmund, G. P., B. S. Myers, M. B. Davis, H. F. Bohnet and B. A. Winkelstein. 2000. “Human Cervical Motion Segment Flexibility and Facet Capsular Ligament Strain under Combined Posterior Shear, Extension and Axial Compression.” Stapp Car Crash Journal 44: 159-170. Svensson, Y., B. Aldman, P. Lövsund et al. 1993. “Pressure Effects in the Spinal Canal During Whiplash Extension Motion: A Possible Cause of Injury to the Cervical Spinal Ganglia.” Proc. International Conference on the Biomechanics of Impacts. 189-200. Yamada, H. 1970. “Strength of Biological Materials.” Evans, F. G. (Ed). Williams & Wilkins Company, Baltimore. Yoganandan, N., A. Pintar, S. Kumaresan and A. Elhagediab. 1998. “Biomechanical Assessment of Human Cervical Spine Ligaments.” 42nd Stapp Car Crash Conference. Winkelstein, B., R. Nightingale, W. Richardson and B. Myers. 1999. “Cervical Facet Joint Mechanics: Its Application to Whiplash Injury.” Proc. 43rd Stapp Car Crash Conference. 243-265.
396 IRCOBI Conference – Bern (Switzerland) – September 2008