Embed Size (px)
Citation preview

2021Making Education Easy
1
www.researchreview.com.au a RESEARCH REVIEW publication
facebook .com/researchrev iewau /Like us on Facebook
Claim CPD/CME points Click here for more info.
About the speakers
1999 2001 2002 2005 2006 2008 2009 2010 2012 2013 2014 2015 2016 2017
This publication summarises presentations given by renowned rheumatologists at a Sandoz-sponsored scientific education event in Australia in February 2021 (Scientific Education Events in Rheumatology by Sandoz, SEERS). Professor Gerd Burmester provided an overview of the history of the biologics with a focus on rheumatology, and Professor Ranjeny Thomas talked of disease interception and the potential for preventing rheumatoid arthritis in the future.
Biologics in 2020: history and perspectivesProfessor Gerd BurmesterHistorically, the goal of treatment in rheumatoid arthritis has been to partially reduce disease activity. In the 1993 Primer on Rheumatic Diseases textbook, the foundation of the therapeutic pyramid for rheumatoid arthritis included rest, combined with basic anti-inflammatory therapy with salicylates or other nonsteroidal anti-inflammatories (NSAIDs), with disease-modifying antirheumatic drug (DMARD) therapy added if needed.1 In the almost 30 years since this was published, there has been tremendous progress in the field of rheumatology, particularly with the development of the biologics.
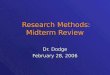
Revolution in the treatment of rheumatic diseasesImportant early milestones in the revolution of rheumatic disease treatment include the discovery of glucocorticoids in the 1950s, and then methotrexate, approved in 1988, and more recently, the biologics, small molecules and biosimilars (Figure 1).2
The first indication for the biologics was rheumatoid arthritis, and then ankylosing spondylitis and subsequently psoriatic arthritis were added as indications. The list of approved indications for biologic therapy now also includes psoriasis, juvenile idiopathic arthritis, Crohn’s disease, ulcerative colitis, cryopyrin-associated periodic syndrome, systemic lupus erythematosus, granulomatosis with polyangiitis and gout.
Figure 1. Treatments for rheumatic diseases – from 1999 (infliximab) onwards.2
The first antibody treatment was developed by Emil von Behring in 1890, against diphtheria, which at the time, in Germany, was the number one killer of children. Subsequent milestones in the pathway towards the biologics include Paul Ehrlich’s idea of antibody treatment – ‘Seitenketten’ (side chain) Therapie, in 1896 – with Ehrlich proposing use of antibodies as Magic Bullets (‘Zauberkugeln’) to cure diseases in 1906. By 1929 Ehrlich had lost hope, stating that nothing successful can be hoped regarding this direction of therapy. But luckily, he was entirely wrong because the biologics are a tremendous success.
Infliximab Rituximab
Abatacept
Certolizumab
Tocilizumab
Sarilumab
BaricitinibApremilast
Tofacitinib
Anakinra
Golimumab
Tocilizumab
Canakinumab
Ustekinumab
Biosimilars of several biologics DMARDs
EMA/FDA aproved:Upadacitinib
EMA aproved:Filgotinib
Appproved in Japan:Peficitinib
Biologics DMARDs ts DMARDs
Seckinumab
Adalimumab
Biologics
Biosimilars
Small Molecules
ContactResearch ReviewTM
Email [email protected]
Phone 1300 132 322
Ranjeny Thomas is a Professor of Rheumatology at the University of Queensland, Translational Research Institute, a consultant rheumatologist at Princess Alexandra Hospital, and a fellow of the Australian Academy of Health and Medical Sciences. She contributed to the founding of the Uniquest spin-off company Dendright, and in the 2020 Queen’s Birthday Honours, she was awarded Member of the Order of Australia. Her research is focused on understanding autoimmune disease and restoration of immune tolerance.
Professor Ranjeny Thomas
Gerd Burmester is a Professor of Medicine in the department of Rheumatology and Clinical Immunology at the Charité University Hospital, Free University of Berlin, and Humboldt University of Berlin, Germany. Professor Burmester is the recipient of numerous awards, including the Jan van Breemen Medal of the Dutch Society of Rheumatology and the Carol-Nachman Prize for Rheumatology. He is the author of more than 800 original and review articles, with research interests that include rheumatoid arthritis, Lyme borreliosis, immunotherapy, cellular activation mechanisms in inflammatory joint diseases, and tissue engineering.
Professor Gerd Burmester
RESEARCH REVIEW TM Australia's Leader in Specialist Publications
Research Review TM
SPEAKER SERIESScientific Education Events in Rheumatology

www.researchreview.com.au a RESEARCH REVIEW publication
2
In addition to TNF-alpha, interleukin 6 (IL-6), a very pleiotropic cytokine, was thought to be important in rheumatoid arthritis pathogenesis, and it was on this basis that tocilizumab, directed against the IL-6 receptor, was developed. Subsequently, there have also been some developments into tackling the ligand, IL-6 itself, but only olokizumab has survived, with very good effects, and there is also a second anti-receptor antibody called sarilumab.
Other biologics of importanceOther important milestones in biologics development and use include:
• Infliximab in ankylosing spondylitis and psoriasis
• IL-17 agents (such as secukinumab) in ankylosing spondylitis and psoriasis
• Abatacept in rheumatoid arthritis
• Rituximab for rheumatoid arthritis
BiosimilarsBiosimilars are now very important, they are game changers, making it possible to treat more patients with biologics, particularly in countries that have fewer resources. Biosimilars have been developed for many of the biologics, including infliximab, adalimumab, etanercept and rituximab, and these are widely accepted in many countries. There are many examples showing that it does not really matter if you take the original compound or if you switch to the biosimilar, the clinical efficacy, pharmacokinetics and the side effect profile are the same.8, 9 The EMEA said the biosimilars are a good way to save money, while maintaining good therapeutic success.10
Biologics and safetyNow we have 20 years of experience, we know that the most serious reported adverse events are serious infections, such as tuberculosis, and that opportunistic infections are rare events. Malignancy rates are similar to expected rates in the general population, with the possible exception of skin cancer, lymphoma rates are consistent with the expected rate in the background of rheumatoid arthritis, and we do not see increased risk of cardiovascular disease with anti-TNF agents, they might even be protective here. Standard mortality rates are at least comparable to expected rates in the general population and there might in fact be a survival advantage compared with the general population.11
Biologics are here to stayDespite the development of new small molecules, the biologics are here to stay. They are very specific, as well as being selective, they have no off-target effects regarding cytochrome inhibition, and have a very good safety profile. Their long half-life leads to long action, they can be modified – they can be bispecific, can have the addition of molecules (such as radioactive molecules) – and with modern technology, their rapid generation can mean it is possible to quickly address newly emerging needs such as SARS-CoV2. In many parts of the world, biosimilars can lead to significant cost savings, and in many indications there are no alternatives with small molecules.
Preventing rheumatoid arthritis: within reach
Professor Ranjeny ThomasDisease interception means implementation of drugs at an earlier time in the disease process, to slow or prevent the disease from progressing. This involves treatment when a patient has no, or early (pre-diagnosis), symptoms. Intervention would involve prognostic and/or stage-specific risk biomarkers, with treatment implemented to prevent disease symptoms using the risk biomarker. An example of disease interception is the statins, with the risk biomarker being cholesterol, where they are used to prevent future myocardial infarction or stroke.
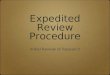
Disease interception for rheumatoid arthritis?Seventy percent of patients with rheumatoid arthritis are autoantibody seropositive: anti-citrullinated peptide antibody (ACPA), and rheumatoid factor (IgG)+, with antibodies developing up to 15 years before disease onset. Notably, ACPA+ disease is associated with particular HLA-DR (shared epitope alleles) and with smoking.
There are some other important risk factors for rheumatoid arthritis, particularly in seropositive disease, including family history/genetic risk, female sex, smoking, and high body mass index (BMI). The population attributable risk of known behavioural factors for rheumatoid arthritis is 40%, which means that up to 40% of rheumatoid arthritis is preventable with lifestyle intervention (Figure 3).
The breakthrough – monoclonal antibodiesThe true breakthrough in the revolution in rheumatology was the development of monoclonal antibodies. These were first developed by researchers investigating immunoglobulin genetics, who needed to increase the amount of material available to study, and hence cloned antibodies to produce monoclonal antibodies. In 1974, the first monoclonal antibodies were developed, and were first used in humans in 1986. In 1991, we published our first paper using an anti CD4 monoclonal antibody to treat very severe cases of rheumatoid arthritis, and it was quite effective at that time.3 However, another study by a different group of researchers using a different anti CD4 monoclonal antibody in rheumatoid arthritis, although initially promising, didn’t perform any better than placebo in a subsequent controlled trial.4 The anti CD4 approach at this time didn’t really work, but it was not known then that we have CD4 effector cells and CD4 regulatory cells, and that it depends which you hit as to whether your therapy will be effective or not.
Table 1. Many biologics used in rheumatology were initially planned for use in other indications
Biologic Initial planned primary indication
Infliximab Sepsis
Etanercept Sepsis
Adalimumab Graft-versus-host disease
Rituximab Non-Hodgkin lymphoma
Abatacept Transplantation/psoriasis
Tocilizumab Multiple myeloma
Although the anti CD4 approach was initially considered ineffective in rheumatoid arthritis, study in this area did resume at a later date. Many of the biological agents currently in use in rheumatology were initially planned for use in various different indications, and largely through serendipity were found to be effective in rheumatology (Table 1). For example, anti-TNF treatment did not work in sepsis, but then it was discovered that TNF alpha might be a very interesting target in rheumatoid arthritis (Figure 2).
Pathogenesis of Arthritisand Targets of Therapy
Cartilage
Antigen(s)(so far unknown)
Synovial fibroblastsOsteoclasts
Proteases
Joint destructionT cells
IL-15, IL-17
B cells
Macrophages
TNF-aa,, IL-6, GM-CSF, IL-1, IL-18© GR Burmester, 2020
Figure 2. Pathogenesis of arthritis and targets of therapy.Compiled by G. R. Burmester based on information from company members.
It was a lucky coincidence that researchers looking at TNF-alpha in rheumatoid arthritis were given leftover TNF-alpha (infliximab), tried it in a pivotal trial, and were able to show that this agent performed very well.
Subsequently, etanercept was developed, with two early published studies showing very positive results,5, 6 and etanercept was approved for use in juvenile rheumatoid arthritis on the basis of fewer than 200 individuals;7 etanercept has been a game changer in paediatric rheumatoid arthritis. Moreover, adalimumab, one of the most best-selling drugs of all times, was initially developed for the treatment of graft-versus-host disease, and there were no early publications in the big journals, just one review type paper showing preliminary results. Golimumab should also be mentioned here, as another fully human monoclonal anti-TNF antibody
Research ReviewTM
SPEAKER SERIES
Scientific Education Events in Rheumatology

At-risk investigation cohort (A3BC): symptomatic ACPA+, FDR
Early arthritis clinic
Induction ... maintain remission
www.researchreview.com.au a RESEARCH REVIEW publication
Figure 4. Preventing rheumatoid arthritis – lifestyle intervention, disease interception and control.12
CSA/UA = Clinically suspect arthralgia/Unclassified arthritis.
Our vision is for wearable precision monitoring that would include things like symptoms on the day, and a risk score (lifestyle, genetic factors and antibodies and inflammatory markers) that before disease onset might vary depending on lifestyle and interventions. When risk score goes up, a patient could monitor more frequently to see when therapy might need to be repeated or instituted.
References1. Schumacher HR, Klippel JH, Koopman WJ, editors. Primer on the Rheumatic Diseases. 10th ed.
Atlanta, Georgia, US: Arthritis Foundataion; 1993.
2. Burmester GR, Bijlsma JWJ, Cutolo M, et al. Managing rheumatic and musculoskeletal diseases - past, present and future. Nat Rev Rheumatol. 2017;13(7):443-8.
3. Horneff G, Burmester GR, Emmrich F, et al. Treatment of rheumatoid arthritis with an anti-CD4 monoclonal antibody. Arthritis Rheum. 1991;34(2):129-40.
4. van der Lubbe PA, Reiter C, Breedveld FC, et al. Chimeric CD4 monoclonal antibody cM-T412 as a therapeutic approach to rheumatoid arthritis. Arthritis Rheum. 1993;36(10):1375-9.
5. Moreland LW, Baumgartner SW, Schiff MH, et al. Treatment of rheumatoid arthritis with a recombinant human tumor necrosis factor receptor (p75)-Fc fusion protein. N Engl J Med. 1997;337(3):141-7.
3
There remain several important challenges in the development of antigen-specific immunotherapy in rheumatoid arthritis. For this reason, it is likely that the clinical efficacy of antigen-specific immunotherapy may first be demonstrated in a disease like coeliac disease or type 1 diabetes.
There are challenges around developing robust assays of antigen-specific T cells, which has been a major stumbling block in the field. The development of peptide-specific T-cell tetramer assays may help to address this particular challenge.15
A major challenge in rheumatoid arthritis is around identifying the important antigens that are actually involved, what antigens are in the synovial tissue that are stimulating the T cells that enter that space? In working to discover what these T cells recognise, we found that the most expanded T cell clonotypes that are shared between peripheral blood and synovial tissue are cytotoxic CD8 T cells, and this brings home the importance of controlling the bystander CD8 inflammatory drive when treating rheumatoid arthritis.
How do we prevent rheumatoid arthritis?Currently, DMARDs and biologics are available as treatment, but to prevent rheumatoid arthritis we would potentially commence these treatments back in the pre-rheumatoid arthritis period. While not expecting to cure anyone at this point with this approach, potentially by adding tolerising immunotherapy guided by biomarkers, this might become a reality for high-risk individuals. In earlier pre-rheumatoid arthritis phases, while we would not be able to justify giving DMARDs, there is a big opportunity for all of us to undertake lifestyle intervention, and to get people onto regular exercise, particularly high-intensity exercise, and to improve their diet (the Mediterranean diet for example). There may also be a place for oral therapies such as probiotics to influence the mucosal barrier function at this stage, but we need trial evidence (Figure 4). We currently have an Australia-wide at-risk cohort; we are recruiting through A3BC, symptomatic individuals who are APCA+ but who do not yet have rheumatoid arthritis, aiming to develop personalised risk scoring and biomarkers of progression.
Figure 3. Natural history of rheumatoid arthritis.12
CSA/UA = Clinically Suspect Arthralgia/Unclassified Arthritis.
Can rheumatoid arthritis be intercepted by earlier DMARDs?If DMARDs are given before onset of rheumatoid arthritis, we will reduce the severity of rheumatoid arthritis and improve the outcome. Rheumatoid arthritis onset is delayed rather than prevented, because these drugs suppress inflammation rather than inducing tolerance. But what about immunotherapy?
Evidence from type 1 diabetesType 1 diabetes has very similar disease pathogenesis to rheumatoid arthritis:
• Some of the same HLA subtypes
• Immunoregulatory genes contribute to genetic risk
• Imbalance in regulatory and effector cells
• Autoantibody development
• Epitope spreading
• Disease activity manifested as loss of glycaemic control
• Diagnosis with full-blown disease.
There are no conventional disease-modifying agents available for the treatment of type 1 diabetes, and thus there has been a focus on developing tolerising strategies to increase immune regulation. Teplizumab was the agent that provided the most hope, but it failed to meet the primary endpoint in recent-onset disease.13 However, a landmark trial in 2019 demonstrated that when given in high-risk individuals in a short course, teplizumab was able to halve progression to diabetes compared with placebo within 2 years of getting teplizumab.14 To achieve disease interception in type 1 diabetes using this approach, screening for at-risk patients would need to be performed across the population, we would need at-risk investigation and management clinics, and we would need a national screening programme (which is currently being rolled out in various countries, and is at early stages in Australia). We would also need to monitor treated children to determine the need for further treatment.
Back to rheumatoid arthritisWe are asking a similar question in rheumatoid arthritis, because the at-risk period is similar, but rheumatoid arthritis has the advantage that many at-risk people develop mild or intermittent symptoms whereas diabetes is silent. Antigen-specific immunotherapy is a future approach for safe interception to induce immune tolerance in people at risk of rheumatoid arthritis. One current approach is a subcutaneously administered dose of liposomes carrying a joint-specific peptide, collagen II peptide antigen plus the NF k B inhibitor calcitriol (vitamin D3). In this approach, uptake into the antigen-presenting cell enables antigen presentation to collagen-specific T cells, with antigen-specific regulation through functional effects on dendritic cells and on antigen-specific T cells. Autoantigen specificity avoids generalized immune suppression and has low toxicity. In preclinical models, this resets the effector cells to a regulatory function, with increasing regulatory capacity in the joint where the peptide is presented. Multiple mechanisms are thought to be involved. Key points are that inflammation supports tolerance, so where the dendritic cells express the checkpoint molecule PDL1 and take up the liposomes, they suppress the effector T cells, and thus increase regulation. Secondly, tolerogenic therapy with a single peptide supports bystander tolerance, suppressing other joint-reactive T cells.
AGE (YEARS) CLINICAL ONSETBIRTH
DISEASE STAGE SYMPTOMS
Systemic autoimmunity
AutobodiesACPA, RF
Abnormal T and B cells
Enviromental risk factors
Intermittant inflammation
Chronic inflammation
CRP
Genetic risk factors
RACSA/UA
SY
MP
TO
MS
, TIS
SU
E D
AM
AG
E
DISEASE STAGE SYMPTOMS
Systemic autoimmunity
AutobodiesACPA, RF
Abnormal T and B cells
Enviromental risk factors
Intermittant inflammation
Chronic inflammation
CRP
Genetic risk factors
RACSA/UA
SY
MP
TO
MS
, TIS
SU
E D
AM
AG
E
AGE (YEARS) CLINICAL ONSETBIRTH
Research ReviewTM
SPEAKER SERIES
Scientific Education Events in Rheumatology
Lifestyle behavioural intervention Exercise, diet
Oral therapies to influence mucosal barrier function: probiotics, others
DMARDs, Biologics
Tolerising immunotherapy guided by biomarkers

4© 2021 RESEARCH REVIEW
www.researchreview.com.au a RESEARCH REVIEW publication
Speaker Series are prepared with an independent commentary from relevant specialists. To become a reviewer please email [email protected] Review Australia Pty Ltd is an independent Australian publisher. Research Review receives funding from a variety of sources including Government depts., health product companies, insurers and other organisations with an interest in health. Journal content is created independently of sponsor companies with assistance from leading local specialists. Privacy Policy: Research Review will record your email details on a secure database and will not release them to anyone without your prior approval. Research Review and you have the right to inspect, update or delete your details at any time. Disclaimer: This publication is not intended as a replacement for regular medical education but to assist in the process. The reviews are a summarised interpretation of the published study and reflect the opinion of the writer rather than those of the research group or scientific journal. It is suggested readers review the full trial data before forming a final conclusion on its merits. Research Review publications are intended for Australian health professionals.
Australian Research Review subscribers can claim CPD/CME points for time spent reading our reviews from a wide range of local medical and nursing colleges. Find out more on our CPD page.
Research ReviewTM STUDY REVIEWReview titl placeholder text
11. Burmester GR, Gordon KB, Rosenbaum JT, et al. Long-Term Safety of Adalimumab in 29,967 Adult Patients From Global Clinical Trials Across Multiple Indications: An Updated Analysis. Adv Ther. 2020;37(1):364-80.
12. Thomas, R and Cope, AP. (2013) Pathogenesis of rheumatoid arthritis. In Watts, RA, et al. (Ed). Oxford textbook of rheumatology (4th ed). Oxford University Press.
13. Vudattu NK, Herold KC. Treatment of new onset type 1 diabetes with teplizumab: successes and pitfalls in development. Expert opinion on biological therapy. 2014;14(3):377-85.
14. Herold KC, Bundy BN, Long SA, et al. An Anti-CD3 Antibody, Teplizumab, in Relatives at Risk for Type 1 Diabetes. N Engl J Med. 2019;381(7):603-13.
15. Jansen DTSL, Ramnoruth N, Loh KL, et al. Flow Cytometric Clinical Immunomonitoring Using Peptide–MHC Class II Tetramers: Optimization of Methods and Protocol Development. Frontiers in Immunology. 2018;9(8).
6. Weinblatt ME, Kremer JM, Bankhurst AD, et al. A trial of etanercept, a recombinant tumor necrosis factor receptor:Fc fusion protein, in patients with rheumatoid arthritis receiving methotrexate. N Engl J Med. 1999;340(4):253-9.
7. Lovell DJ, Giannini EH, Reiff A, et al. Etanercept in children with polyarticular juvenile rheumatoid arthritis. Pediatric Rheumatology Collaborative Study Group. N Engl J Med. 2000;342(11):763-9.
8. Jaworski J, Matucci-Cerinic M, Schulze-Koops H, et al. Switch from reference etanercept to SDZ ETN, an etanercept biosimilar, does not impact efficacy, safety, and immunogenicity of etanercept in patients with moderate-to-severe rheumatoid arthritis: 48-week results from the phase III, randomized, double-blind EQUIRA study. Arthritis Res Ther. 2019;21(1):130.
9. Park MC, Matsuno H, Kim J, et al. Long-term efficacy, safety and immunogenicity in patients with rheumatoid arthritis continuing on an etanercept biosimilar (LBEC0101) or switching from reference etanercept to LBEC0101: an open-label extension of a phase III multicentre, randomised, double-blind, parallel-group study. Arthritis Res Ther. 2019;21(1):122.
10. OECD, Union E. Health at a Glance: Europe 20182018.
facebook.com/researchreviewau/
Keep up to date with all the latest research on our Research Review Australia Facebook page
Research ReviewTM
SPEAKER SERIES
Scientific Education Events in Rheumatology
Company Commissioned ArticleThis publication has been commissioned by Sandoz. The content is entirely independent and based on published studies and the authors’ opinions. It may not reflect the views of Sandoz. Please consult the full Product Information for any product mentioned in this review via the TGA website https://www.ebs.tga.gov.au before prescribing. Treatment decisions based on these data are the full responsibility of the prescribing physician.