Embed Size (px)
Citation preview
7/29/13
1
Title by Presenter Name
Sandra Smith, PhD, APRN, NNP-‐BC Autonomic Nervous System Function and the Effect of Massage Therapy on Enhancing Parasympathetic Activity in
Preterm Infants Sandra L. Smith, PhD, APRN, NNP-BC
Associate Professor University of Louisville, School of Nursing
OVERVIEW OF AUTONOMIC
NERVOUS SYSTEM
DEVELOPMENT IN THE FETUS
AND INFANT
Three Subsystems (Circuits) of the Autonomic Nervous System (ANS)
1) Social communication—highest levels of communication
1) Partially available at term gestation
2) Mobilization—tantrums, behavioral acting-out
3) Immobilization--oldest circuit associated with survival—possum feigning death, physiologic shutdown
(Porges & Furman, 2011)
ANS: Focus on the Vagus Nerve • Mammalian ANS developed beyond the reptilian
survival function
– Rapidly adapted to accommodate fight-flight events and social interactions
• High vagal tone via myelinated vagal pathways to the heart
– Acts as a brake, slowing the heart, calming the person
– Low vagal tone: no inhibition on the heart (Porges, Doussard-‐Roosevelt, et al., 1996)
Vagal Pathways in Infants
• Partially myelinated at birth – Myelination is necessary for effective nerve signal
transmission
• Myelinated fibers increase from 24 weeks gestation through adolescence
• Greatest increase occurs between 32 and 34 weeks gestation to ~ 6 months of age – Vagal tone through myelinated fibers increases with
gestational age
7/29/13
2
Vagal Pathways in Infants
• Thus infants born prior to 30 weeks gestation lack the high vagal efferent and vagal brake activity on the heart
– Myelination is not complete
– Reactivity to stressors is exaggerated and recovery impaired
• Long term effects are unknown but may affect social and behavioral development
Preterm Infant ANS Function • Preterm infants demonstrate a prolonged
ANS dysfunction
– Yiallourou et al. (2013): preterm infants have a persistent depressed parasympathetic activity at 5-6 months of age
– Patural (2008): Preterm infants have depressed ANS activity at 1 year of age
Given the interrupMon of ANS development and the prolonged ANS dysfuncMon experienced by
preterm infants, what treatments may enhance ANS development in this vulnerable
group?
Effect of Massage Therapy on Preterm Infants
• Improved weight gain • Increased IGF-1 expression (enhanced growth) • Decreased length of hospital stay (~5 days) • Increased gastric motility • Improved bone mineral deposition • Alterations in brain waves (sleep) • No difference between massage and controls (Arora et al., 2005; Diego et al., 2003, 2007; Field et al., 2006, Guzzetta, 2011)
Methodological Concerns • Massage treatment given 2 x/day for 5-10 days • Variability in who delivered the massage
– Mothers – Others (OT, PT) – LMTs
• Underpowered due to small sample sizes • Lack of blinding by the researchers
Autonomic Nervous System Function and the Effect of Massage Therapy on Enhancing Parasympathetic Activity in
Preterm Infants
Longitudinal, randomized controlled trial of 44 medically stable preterm infants born
between 29 and 32 weeks gestation.
7/29/13
3
Environmental Sources of Neonatal Stress
u Painful procedures
u Noise and lighting
u Maternal separation
u Temperature fluctuation
u Hypoxia and hyperoxia
u Glucocorticoids
u Oxygen consumption
u Energy expenditure
u Temperature fluctuations
u Hypoxemia
Consequences of Neonatal Stress
The stress response is meant to be limited and of short duration
Massage may improve vagal activity, sleep, and growth (Arora et al., 2005; Diego et al., 2003, 2007; Field et al., 2006)
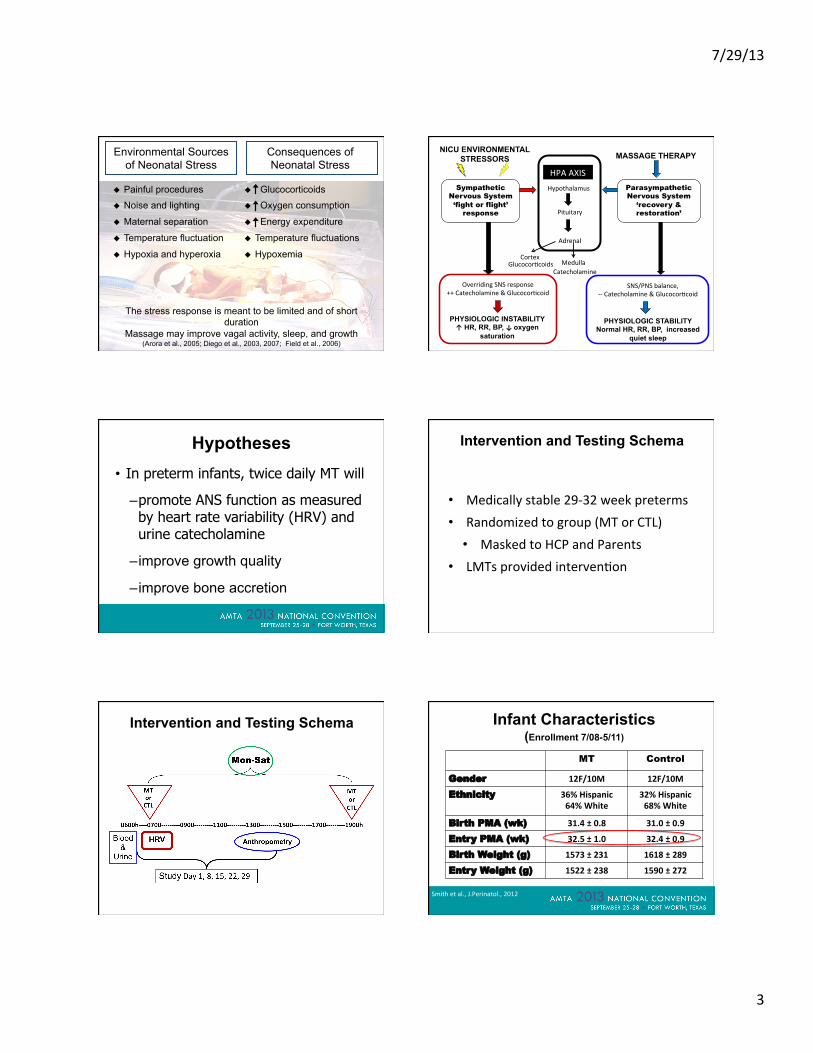
NICU ENVIRONMENTAL STRESSORS
Hypothalamus
Pituitary
Adrenal
Medulla Cortex
Catecholamine GlucocorMcoids
Sympathetic Nervous System ‘fight or flight’
response
Parasympathetic Nervous System
‘recovery & restoration’
Overriding SNS response ++ Catecholamine & GlucocorMcoid
SNS/PNS balance, -‐-‐ Catecholamine & GlucocorMcoid
PHYSIOLOGIC INSTABILITY ↑ HR, RR, BP, oxygen
saturation
PHYSIOLOGIC STABILITY Normal HR, RR, BP, increased
quiet sleep
HPA AXIS
↑
MASSAGE THERAPY
Hypotheses • In preterm infants, twice daily MT will
– promote ANS function as measured by heart rate variability (HRV) and urine catecholamine
– improve growth quality
– improve bone accretion
Intervention and Testing Schema
• Medically stable 29-‐32 week preterms • Randomized to group (MT or CTL)
• Masked to HCP and Parents • LMTs provided intervenMon
Intervention and Testing Schema Infant Characteristics (Enrollment 7/08-5/11)
MT Control
Gender 12F/10M 12F/10M
Ethnicity 36% Hispanic 64% White
32% Hispanic 68% White
Birth PMA (wk) 31.4 ± 0.8 31.0 ± 0.9
Entry PMA (wk) 32.5 ± 1.0 32.4 ± 0.9
Birth Weight (g) 1573 ± 231 1618 ± 289
Entry Weight (g) 1522 ± 238 1590 ± 272
Smith et al., J.Perinatol., 2012
7/29/13
4
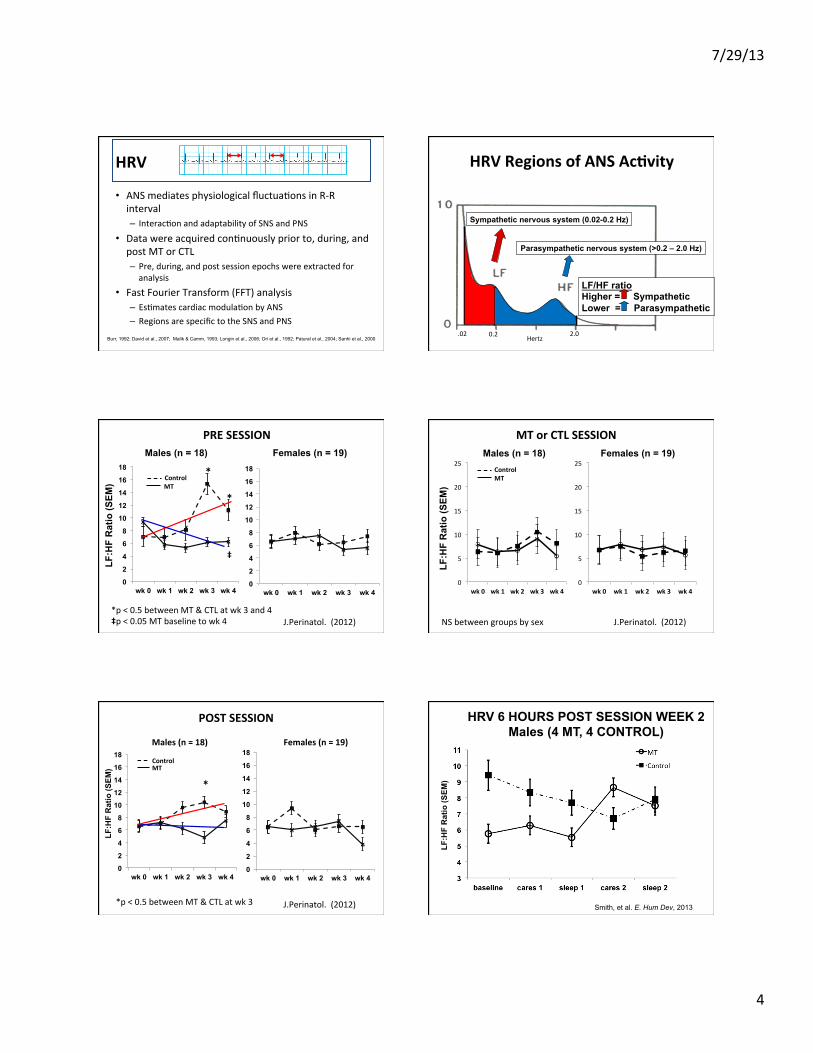
HRV
• ANS mediates physiological fluctuaMons in R-‐R interval – InteracMon and adaptability of SNS and PNS
• Data were acquired conMnuously prior to, during, and post MT or CTL – Pre, during, and post session epochs were extracted for analysis
• Fast Fourier Transform (FFT) analysis – EsMmates cardiac modulaMon by ANS – Regions are specific to the SNS and PNS
Burr, 1992; David et al., 2007; Malik & Camm, 1993; Longin et al., 2006; Ori et al., 1992; Patural et al., 2004; Sanhi et al., 2000
Sympathetic nervous system (0.02-0.2 Hz)
Parasympathetic nervous system (>0.2 – 2.0 Hz)
LF/HF ratio Higher = Sympathetic Lower = Parasympathetic
0.2 .02 2.0 Hertz
HRV Regions of ANS AcFvity
0
2
4
6
8
10
12
14
16
18
wk 0 wk 1 wk 2 wk 3 wk 4
MT Control
LF:H
F R
atio
(SEM
)
0
2
4
6
8
10
12
14
16
18
wk 0 wk 1 wk 2 wk 3 wk 4
*
‡
*
Males (n = 18) Females (n = 19)
*p < 0.5 between MT & CTL at wk 3 and 4 ‡p < 0.05 MT baseline to wk 4 J.Perinatol. (2012)
PRE SESSION
0
5
10
15
20
25
wk 0 wk 1 wk 2 wk 3 wk 4
LF:H
F R
atio
(SEM
)
0
5
10
15
20
25
wk 0 wk 1 wk 2 wk 3 wk 4
MT Control
Males (n = 18) Females (n = 19)
J.Perinatol. (2012) NS between groups by sex
MT or CTL SESSION
0
2
4
6
8
10
12
14
16
18
wk 0 wk 1 wk 2 wk 3 wk 4 0
2
4
6
8
10
12
14
16
18
wk 0 wk 1 wk 2 wk 3 wk 4
LF:H
F R
atio
(SEM
) MT Control
Males (n = 18) Females (n = 19)
*
*p < 0.5 between MT & CTL at wk 3 J.Perinatol. (2012)
POST SESSION HRV 6 HOURS POST SESSION WEEK 2 Males (4 MT, 4 CONTROL)
LF:H
F R
atio
(SEM
)
Smith, et al. E. Hum Dev, 2013
7/29/13
5
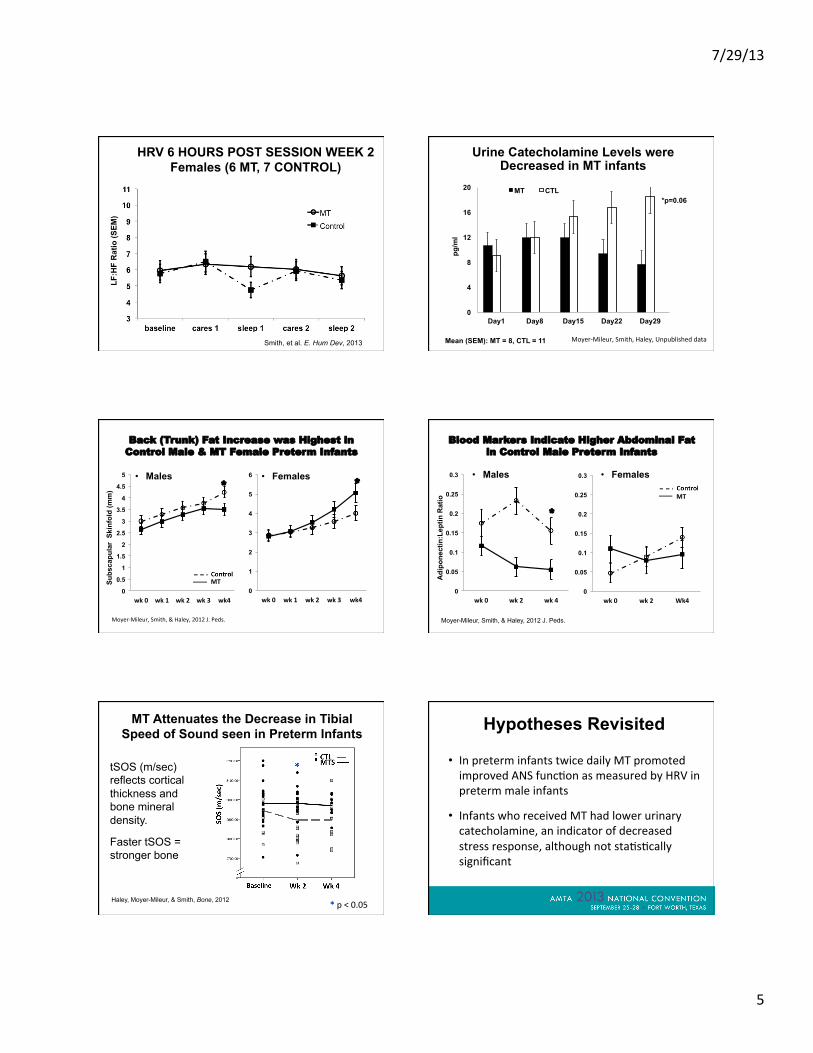
HRV 6 HOURS POST SESSION WEEK 2 Females (6 MT, 7 CONTROL)
Smith, et al. E. Hum Dev, 2013
LF:H
F R
atio
(SEM
)
Urine Catecholamine Levels were Decreased in MT infants
0
4
8
12
16
20
Day1 Day8 Day15 Day22 Day29
MT CTL *p=0.06
Mean (SEM): MT = 8, CTL = 11
pg/m
l
Moyer-‐Mileur, Smith, Haley, Unpublished data
Back (Trunk) Fat Increase was Highest in Control Male & MT Female Preterm Infants
0
0.5
1
1.5
2
2.5
3
3.5
4
4.5
5
wk 0 wk 1 wk 2 wk 3 wk4 0
1
2
3
4
5
6
wk 0 wk 1 wk 2 wk 3 wk4
• Males • Females
Moyer-‐Mileur, Smith, & Haley, 2012 J. Peds.
Subs
capu
lar
Skin
fold
(mm
)
* *
MT
Blood Markers Indicate Higher Abdominal Fat in Control Male Preterm Infants
0
0.05
0.1
0.15
0.2
0.25
0.3
wk 0 wk 2 wk 4 0
0.05
0.1
0.15
0.2
0.25
0.3
wk 0 wk 2 Wk4
• Males • Females
Moyer-Mileur, Smith, & Haley, 2012 J. Peds.
Adi
pone
ctin
:Lep
tin R
atio
*
MT
MT Attenuates the Decrease in Tibial Speed of Sound seen in Preterm Infants
tSOS (m/sec) reflects cortical thickness and bone mineral density.
Faster tSOS = stronger bone
Haley, Moyer-Mileur, & Smith, Bone, 2012 * p < 0.05
Hypotheses Revisited
• In preterm infants twice daily MT promoted improved ANS funcMon as measured by HRV in preterm male infants
• Infants who received MT had lower urinary catecholamine, an indicator of decreased stress response, although not staMsMcally significant
7/29/13
6
Hypotheses Revisited
• Although males had increased adiponecMn/lepMn raMo suggesMve of increased abdominal fat, we have insufficient data to support improved growth quality
• Twice daily MT improved bone strength in male and female preterm infants
Future Research
• Long term benefits of massage on ANS funcMon in preterm infants – Is there a carry over effect aier discharge? – What are the effects on neurobehavioral development?
• What are the mechanisms of massage in promoMng ANS funcMon in preterm infants
• Laurie Moyer-‐Mileur, PhD (PI) • Shannon Haley, PhD, LMT & LMT Team • Hillarie Slater, BS • Robert Lux, PhD • Nancy Allen • Funding
– NIH NCCAM R 21 – University of Utah Interdisciplinary Research, College of Nursing, and Division of Neonatology Grants
Presenter Name: