Embed Size (px)
Citation preview

Research ArticleCalretinin as a Diagnostic Adjunct for Ameloblastoma
Chitra Anandani1 Rashmi Metgud1 and Karanprakash Singh2
1 Department of Oral and Maxillofacial Pathology Pacific Dental College and Hospital PAHER University UdaipurRajasthan 313024 India
2Department of Public Health Dentistry Genesis Institute of Dental Sciences and Research Ferozepur Punjab 152001 India
Correspondence should be addressed to Chitra Anandani drchitraanandanigmailcom
Received 19 January 2014 Revised 27 March 2014 Accepted 28 March 2014 Published 15 April 2014
Academic Editor Gary Tse
Copyright copy 2014 Chitra Anandani et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
Background Calretinin is a 29 kDa calcium-binding protein of the EF-hand family which is expressed in a variety of normal andtumorigenic tissues Its expression in odontogenic epithelium during odontogenesis and in neoplastic odontogenic tissues has beendemonstrated Unicystic ameloblastoma poses a diagnostic challenge as its histologic presentation can be sometimes mistakenfor keratocystic odontogenic tumor (KCOT) This study was performed to assess the usefulness of calretinin as a confirmatorymarker for ameloblastic tissue Methodology Total of 40 cases 16 unicystic ameloblastoma 4 multicystic ameloblastoma and 20KCOT were evaluated immunohistochemically for the presence localization distribution and intensity of calretinin expressionStatistical analysis was done using Chi-square test to intercompare the expression between ameloblastoma and KCOT ResultsSixteen cases of ameloblastoma (12 unicystic 4 multicystic) showed positive calretinin staining of ameloblastic epithelium and onlyone case of KCOTwas positive for calretinin with the positivity restricted to the stellate reticulum like epithelium Intercomparisonbetween two groups revealed statistically significant difference (119875 = 0000) Conclusion Calretinin appears to be a specificimmunohistochemicalmarker for neoplastic ameloblastic epithelium andmay be an important diagnostic adjunct in the differentialdiagnosis of ameloblastoma and KCOT
1 Introduction
Calcium ions (Ca2+) regulate a large number of biologicalprocesses such as metabolism contraction secretion celldivision cell growth and memory storagemdasheither directlyor indirectly Elevated cytoplasmic calcium levels found inseveral tumor cells might contribute to the increasedmotilityand hence invasiveness of these cells
The calcium signal is transmitted into the intracellularresponse in part via interactions with a wide variety ofintracellular calcium-binding proteins that are involved inthe regulation of many cellular activities One class of theseproteins shares a common calcium-binding motif the EF-hand [1]The EF-hand homologue family contains more than200 different calcium-binding proteins among them being29 kDa calretinin which was isolated initially from a cDNAclone from the chick retina and it is most homologous toanother important member of the EF-hand family that is28 kDa calbindin [2]
Calretinin is widely expressed in central and peripheralneural tissues particularly in the retina and in neurons ofsensory pathways Outside the central nervous system it isexpressed in normal and reactive mesothelial lining of allserosal membranes the pilar infundibulum eccrine glandsconvoluted tubules of the kidney leydig and sertoli cells of thetestis endometriumand ovarian stromal cells adrenal cortexepithelial cells of the thymus and adipocytes [2 3]
Studies in rats have demonstrated calretinin expression inneural elements of the tooth pulp periodontal ligament andviscerosensory nerve fibres of oral and pharyngeal tissues [4]as well as in epithelium-derived tissues during odontogenesisin rat molar tooth germs suggesting that this protein mayplay a part in enamel formation [2] The exact biologicalfunction of calretinin remains unknown but its possible rolesas a calcium buffer andor calcium sensor and regulator ofapoptosis have been postulated [5] Calretinin also seemsto share with calbindin certain features such as regulationof expression by growth factors and involvement in cell
Hindawi Publishing CorporationPathology Research InternationalVolume 2014 Article ID 308240 7 pageshttpdxdoiorg1011552014308240
2 Pathology Research International
proliferation differentiation and neoplastic transformation[6]
Apart from its expression in normal human tissuescalretinin has been shown to be expressed in a wide vari-ety of tumors [7] Calretinin has recently emerged as animmunohistochemical marker with great utility for delin-eating mesothelioma and adenocarcinomas of lung as itsdiagnostic sensitivity for mesothelioma is nearly 100 [8]
Odontogenic tumors comprise a group of heterogeneouslesions ranging from hamartomatous or nonneoplastic tissueproliferations to benign neoplasms to malignant tumors withmetastatic potential [9] The odontogenic cysts which maybe intimately associated with the development of certain ofthe odontogenic tumors also represent an aberration at somestage of odontogenesis [10] Keratocystic odontogenic tumor(KCOT) has been recently classified by World Health Orga-nization (WHO) in 2005 as a benign tumor of odontogenicepithelium to emphasize its neoplastic nature [9]
Unicystic ameloblastoma is considered at best an in situor superficially invasive form of ameloblastoma [11] Uni-cystic ameloblastomas arewell known to be lined by a variableepithelium ranging from one that has typical ameloblasticcharacteristics to one that is metaplastic and which appearscompletely nondescript consisting of several layers of nonker-atinizing squamous cells In such cases the differentiation ofodontogenic cysts from the unicystic ameloblastoma can beproblematic [12]
The histologic presentation of ameloblastoma especiallyunicystic type can be in some instances mistaken for ker-atocystic odontogenic tumor (KCOT) Overlapping clinicaland radiographic presentation further adds to this diagnosticdifficulty [3]
Hence the present study was carried out to evaluate andintercompare the expression of calretinin in ameloblastomaand keratocystic odontogenic tumor in order to assess itsusefulness as a confirmatory marker for ameloblastic tissuethat would aid in the differential diagnosis of such lesions
2 Materials and Methods
21 Case Selection Formalin-fixed paraffin-embedded tissueblocks of ameloblastoma (unicystic and multicystic variants)and KCOT (parakeratinized type) were retrieved from thearchives of Department of Oral and Maxillofacial PathologyPacific Dental College and Hospital Udaipur Re-evaluationof all cases was performed according to the World HealthOrganization histological typing of odontogenic tumors [9]by two oral pathologists on light microscopy using hema-toxylin and eosin sections The study protocol was reviewedby the Ethical Committee of Pacific Dental College andHospital and was granted ethical clearance
22 Immunohistochemistry Formalin-fixed paraffin-embed-ded tissue blocks were cut into 4 120583m thick sections andplaced on organosilane-pretreated slides Immunohisto-chemical staining was performed using the primary antibodyfor calretinin using supersensitive one-step polymer-HRPtechnique (Biogenex Life Sciences San Ramon CA USA)
The sections were deparaffinized and rehydrated throughxylene and descending grades of alcohol respectively Anti-gen retrieval was carried out using commercial microwaveantigen retrieval system where the sections were immersedin 10mM sodium citrate buffer (pH 60) at 800 420 and320∘F for three cycles of 10min each (EZ-Retriever SystemBiogenex Life Sciences) After rinsing in tris buffer (pH 72)the sections were incubated with 3 hydrogen peroxide inwater for 15min to block the endogenous peroxidase activityThis was followed by a power block for 10min at roomtemperature to block any nonspecific antigenic sites Thesectionswere then incubatedwith optimally prediluted rabbitpolyclonal antibody against calretinin protein (BiogenexCA USA) for 30min at room temperature in a moistchamber After washing with tris buffer (pH 72) for 5minthe sections were then incubated with super enhancer for20min at room temperature followed by secondary antibodyincubation with one-step polymer-HRP reagent for 30minat room temperature in a moist chamber Visualizationwas performed using freshly prepared 331015840-diaminobenzidinehydrochloride (DAB) substrate (Sigma) for 5min The slideswere counterstained with Mayerrsquos hematoxylin for 3minsubsequent to which sections were dehydrated cleared andmounted with dibutyl phthalate xylene (DPX) (RankemRFCL Ltd) For each batch of staining positive and negativecontrols were run simultaneously with the study specimensHuman mesothelioma which is known to have a high levelof calretinin expression served as the positive control whilethe primary antibodies were replaced by nonimmune mouseserum at the same dilutions for the negative controls
23 Evaluation of Slides The evaluation of the stained slideswas carried out using a binocular research microscope(Lawrence ampMayo) under 100x and 400x magnificationThesections stained with calretinin antibody were evaluated forthe presence localization distribution and intensity of theimmunoreactive cells [4] Presence was evaluated to estimatewhether the staining was positive or negative and if positivewhich epithelial layer was stained Localizationwas evaluatedto estimate whether the stainingwas nuclear (N) cytoplasmic(C) or both Distribution was evaluated as being either focal(involving lt50 of positive cells) or diffuse (involving gt50of positive cells) The intensity was graded based on thenumber of positive cells seen 0 = no staining 1 = weakstaining 2 = moderate staining 3 = intense staining
The Chi-square test was applied to intercompare thecalretinin expression between ameloblastoma andKCOT andfor the comparison between the variants of ameloblastoma(unicystic and multicystic) P values lt005 were consideredto be statistically significant
3 Results
A total of 40 cases (20 each) of ameloblastoma and KCOTwere studied Out of the 20 cases of ameloblastoma 16were of unicystic type and the remaining 4 were of solidmulticystic type [2 follicular 1 plexiform and 1 granular cellameloblastoma]
Pathology Research International 3
Table 1 Intercomparison of calretinin presence in ameloblastomaand KCOT
Presence Ameloblastoma (119899 = 20) KCOT (119899 = 20)Frequency Percent Frequency Percent
+ 12 30 1 25minus 8 20 19 475119875lowast value 0000lowast119875 value lt 005 statistically significant
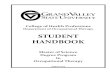
31 Unicystic Ameloblastoma Out of the 16 cases of uni-cystic ameloblastoma positive calretinin expression of theameloblastic epithelium was seen in 8 (50) cases In allthe immunopositive cases reactivity was observed in boththe nucleus and cytoplasm of the cells The distribution ofcalretinin was focal in 5 and diffuse in 3 cases and waslimited to the stellate reticulum like area The luminal layerof ameloblast-like cells did not stain except for the few singlebasal cells that were positive in 2 cases only Four casesshowed weak staining 3 showed moderate and 1 showedsevere staining of the ameloblastic epithelium (Figure 1)
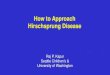
32 SolidMulticystic Ameloblastoma All the 4 cases showedweak positive staining of stellate reticulum like areas whereasonly one case showed focal positivity in the basal cell layeralso Immunoreactivity was observed in both the nucleus andcytoplasm of the cells Staining was focally distributed in 3cases while one case stained diffusely (Figure 2)
In addition all the cases of ameloblastoma also showedscattered positive cells within the stroma whichwere thoughtto be nonepithelial in type and could represent mast cells
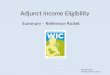
33 Keratocystic Odontogenic Tumor Nineteen (95) casesshowed negative staining of calretinin in the epithelial liningof the cyst except for some scattered darkly stained individ-ual cells in the fibrous connective tissue wall Only one casethat showed positivity to calretinin revealed a highly inflamedodontogenic keratocyst with one bit of tissue depictingstellate reticulum like epithelium overlying the palisadedbasal cell layer in the hematoxylin and eosin stained sectionsThe calretinin staining for the same bit showed uniformdiffuse immunopositivity of the nucleus and cytoplasm of thestellate reticulum like epithelium (Figure 3)
The intercomparison of calretinin positivity betweenameloblastoma and KCOT revealed a statistically significantdifference at 119875 = 0000 (Table 1)
4 Discussion
Odontogenic cysts and tumors are a group of lesions aris-ing from the tooth-producing apparatus or its remnantsThey may originate from odontogenic epithelium andorectomesenchyme with varying degrees of inductive tissueinteraction [13] They are rare and lack of familiarity withthese lesions and their variable appearance may lead todifficulties in diagnosis with occasional serious confusionwith more sinister lesions [14]
Different odontogenic cysts and tumors have variableclinical and biological behaviors Ameloblastoma is a benignlocally aggressive epithelial odontogenic tumor that hasthe potential to become malignant and produce metastasisto distant sites such as lungs and kidneys KCOT is anaggressive cyst with neoplastic behaviour while unicysticameloblastoma is a neoplasm with cyst like behaviour [1516] KCOT also arises from cell rests of the dental lam-ina same origin as ameloblastoma and there are clinicaland radiographic similarities between KCOT and unicysticameloblastoma as both present as ordinary cysts in thedentate areas [17] Histologically unicystic ameloblastomais lined in some areas but rarely entirely by odontogenicepithelium of ameloblastoma appearance and stratified squa-mous epithelium in the remaining areas [18] In fact suchsquamous metaplasia is a relatively frequent phenomenon inunicystic ameloblastoma and many of these lesions are linedby such nondescript epithelium which can create diagnosticconfusion with odontogenic cysts [12]
KCOT is characterized histologically by a palisaded basalcell layer of basophilic columnar cells and a surface of cor-rugated parakeratin sometimes with spongiosis resemblingclosely the stellate like reticulum and the acanthomatousdifferentiation of ameloblastoma If the tissue sample is smalland if the neoplastic epithelium displays reactive changesinduced by inflammation it can closely resemble unicysticameloblastoma histologically [3] Thus at times both lesionsbecome histologically indistinguishable
Many techniques have been used in an attempt to distin-guish odontogenic cysts (including KCOT) from ameloblas-tomas (especially unicystic type) which include demon-stration of cell surface carbohydrates with blood groupspecificity determination of alkaline phosphatase activityin the stroma distribution of lectins and involucrin in theepithelium characterization of cytokeratin profiles countingof AgNORs and quantification of cell proliferation markerssuch as PCNA and Ki67 While differences have been shownto occur between various cysts and ameloblastomas consid-erable overlap exists and none of the above techniques can beused to routinely distinguish these lesions from one another[5]
Also a number of studies have reported the immuno-histochemical expression of intermediate filaments growthfactors basement membrane components cell cycle regu-lating factors and apoptotic proteins in ameloblastomas butcalcium-binding proteins have not been investigated to agreater extent in these tumors [19]
The present study assessed the expression of calretinin in20 cases each of ameloblastoma and keratocystic odontogenictumor and the results demonstrated frequent expressionof calretinin in the epithelium of both unicystic and solidmulticystic ameloblastomas Positive staining was seen in50 (8 cases) of unicystic ameloblastoma and 100 (4 cases)of multicystic ameloblastoma whereas only 1 out of 20 casesof KCOT lining showed positive staining for calretinin Theintercomparison between both groups revealed a statisticallysignificant difference at 119875 = 0000 Also the immunopositiv-ity was seen exclusively in the stellate reticulum like epithe-lium in both the unicystic and multicystic ameloblastomas
4 Pathology Research International
(a) 100x (b) 400x
Figure 1 Photomicrograph showing calretinin staining in unicystic ameloblastoma in (a) 100x and (b) 400x
(a) 100x (b) 400x
Figure 2 Photomicrograph showing calretinin staining in solid multicystic ameloblastoma in (a) 100x and (b) 400x
(a) (b)
Figure 3 Photomicrograph showing (a) negative calretinin staining in keratocystic odontogenic tumor (100x) and (b) positive calretininstaining in keratocystic odontogenic tumor (100x)
Pathology Research International 5
and the ameloblast-like basal cells were positive in only 1 ofthe multicystic and 2 of the unicystic variants where singlecell expressing calretinin was observed
These findings were in accordance with earlier studieswhich also observed calretinin positive cells restricted to theneoplastic stellate reticulum like epithelium in ameloblas-toma only Altini et al [19] and Coleman et al [12] foundpositive staining in 815 cases of unicystic ameloblastomasand 935 cases of multicystic ameloblastoma while Dev-illiers et al [3] Sundaragiri et al [5] and DrsquoSilva et al[20] found positivity in all cases of ameloblastoma (100)In all these studies none of the odontogenic cystsrsquo liningshowed positivity except DrsquoSilva et al [20] who observedpositive staining of the cystic lining epithelium and keratinflakes in the cystic lumen of 40 cases of odontogenickeratocystThe authors attribute this finding to the aggressivebiologic behavior of odontogenic keratocyst similar to abenign neoplasm and its high mitotic activity as comparedto other nonneoplastic odontogenic cysts Also Piattelli et al[21] found positivity to calretinin in 8 of 12 parakeratinizedkeratocysts in the parabasal-intermediate layers of the cystepithelium This could point to the aggressive behavior ofKCOT and help to explain the differences in the clinical andpathologic behavior of odontogenic keratocysts in particularthe differences found between orthokeratinized keratocystsand parakeratinized keratocysts
Alaeddini et al [4] also found that calretinin immunore-activity was positive only for ameloblastoma when comparedto calcifying epithelial odontogenic tumour adenomatoidodontogenic tumour ameloblastic fibroma and odontogenicmyxoma stating that this protein may have a role in thetransition of the dental lamina remnants to ameloblastomaThey hypothesized that calretinin may be one of the factorsresponsible for the differences between this aggressive neo-plasm and other odontogenic tumors studied
Further in the present study the distribution pattern ofthe immunopositive cells was focal in 8 cases (40) anddiffuse in 4 cases (20) Also the staining was weak in mostof the cases (40) with 3 cases (15) showing moderate andonly 1 case (5) intense stainingThe staining was not equallydistributed throughout the sections with some areas showingintense staining but absolutely no staining in the immediatevicinity This was in contrast to the earlier studies wheremost of the cases showed intense staining of the ameloblasticepithelium [3ndash5 12 19 20]
Altini et al [19] stated that the better the differentiationof the epithelium was the lesser the expression of calretininoccurred in their study where they found little or noimmunostaining in those cases of unicystic ameloblastomasthat were lined by typical ameloblastic epithelium while theepithelium which completely lacked ameloblastic featuresfrequently expressed calretinin Hence they indicated thatcalretinin expression in some cells varied according to theirmetabolic activity andmay be lost when this activity changesLater Coleman et al [12] observed intense positive stainingin both areas of nondescript epithelial lining and areas withtypical ameloblastic features in unicystic ameloblastomawhich indicated that although the metaplastic cyst liningsmay have lost their typical ameloblastic features the cells have
retained their immunophenotypic characteristics resultingin the continued expression of calretinin Our study can becorrelated with the observation of Altini et al [19] as majorityof the unicystic ameloblastoma cases that we observed werelined by typical ameloblastic epithelium due to which theymay not have stained intensely with calretinin
In a study by Mistry et al [2] on developing rat molarscalretinin immunoreactivity was present in the inner enamelepithelium and presecretory ameloblasts from the late capstage onwards In the cap and late cap stages many ofthe specimens were immunopositive for calretinin in thestellate reticulum and this number increased to gt90 for theearly and late bell stages In the present study the patternof reactivity of the stellate reticulum observed appearedsimilar to the late bell stage of normal tooth developmentHowever in the peripheral layers of the ameloblastic islandscalretinin immunoreactivity was not observed as was the casein normal tooth germs As enamel organ has been proposedto be one of the possible origins of ameloblastoma [17] thispeculiar distribution of calretinin in ameloblastic epitheliumis noteworthy and it thus appears that there is no obviouscorrelation between the staining of normal odontogenictissues and their neoplastic counterparts [19]
A possible explanation for this dynamic spatial andtemporal distribution was that calretinin may be presentonly in cells that reside directly in the path of calciumin transition on its way to the enamel matrix acting as aldquocalcium ferryrdquo [2] However Hubbard et al [22] found thatcalretinin was primarily expressed during the differentiationstage of enamel formation and only a faint calretinin bandwas observed at secretion stage while no such band wasdetectable during maturation Based on these findings theauthors suggest retirement of the calcium ferry dogma fromenamel biologymdashin murine models at least
Gotzos et al [23 24] have shown increased expressionof calretinin in rapidly proliferating WiDr colon adenocar-cinomas cells Upon being induced to differentiate by treat-mentwith sodiumbutyrate and hexamethylene bisacetamidethey showed marked reductions in cell proliferation as wellas expression of full length calretinin When treated witholigonucleotides against calretinin synthesis these cells wereblocked in the G1 phase of the cell cycle and subsequentlyunderwent apoptosisThese authors suggested that calretininmay maintain an undifferentiated proliferative state charac-teristic of neoplastic transformation Also calretinin may actas an antiapoptotic factor [25]
The single case of KCOT in our study that showedpositivity to calretinin was of a 17-year-old male patienthaving radiolucency in 24 and 25 region with impacted 23The hematoxylin and eosin stained sections of the biopsyspecimen revealed a highly inflamed odontogenic keratocystwith one bit of tissue depicting stellate reticulummdashlikeepithelium overlying the palisaded basal cell layer Uponcalretinin staining uniform diffuse immunopositivity of thestellate reticulum like epitheliumwas observedThis suggeststhat the previous biopsy may have been misdiagnosed asKCOT on the basis of hematoxylin and eosin staining
This result can be compared with that of Devilliers et al[3] wherein they evaluated a tumor from their archives
6 Pathology Research International
originally diagnosed as KCOT which recurred 2 years laterHistologic sections from the tissue biopsied earlier (diag-nosed as KCOT) and from the tissue sample of the recurrence(diagnosed as ameloblastoma)were testedwith calretinin andboth showed positive staining of the neoplastic epitheliumconfined to the stellate reticulum
This finding helps us to understand the importance of cal-retinin as a differential diagnostic marker for ameloblastomaand how important it is for the pathologist to differentiateboth entities which carry different treatment protocols withpotentially serious functional and esthetic consequences forthe patient
Few nonepithelial cells that stained positive for calretininwere also observed in the connective tissue stroma of virtuallyall cases of ameloblastoma and KCOT in our study Altiniet al [19] and Coleman et al [12] also found such darklystained cells within the tumor or cyst epithelium and inthe fibrous connective tissue walls These were interpretedas being mast cells or Langerhans cells both of whichhave been documented as occurring in ameloblastomas andodontogenic cysts
5 Conclusion
The present study suggests that calretinin may be usedas a specific immunohistochemical marker for neoplasticameloblastic epithelium as calretinin positivity was observedexclusively in ameloblastomas Hence it can serve as animportant diagnostic adjunct in the differential diagnosisof ameloblastoma and keratocystic odontogenic tumor Theexpression of calretinin in these neoplastic lesions mightbe recapitulating dental ontogeny as its role during normaltooth development has also been speculated
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
Theauthors wish to thank all themembers in theDepartmentofOral andMaxillofacial Pathology for their general support
References
[1] C W Heizmann ldquoCalcium-binding proteins basic conceptsand clinical implicationsrdquo General Physiology and Biophysicsvol 11 no 5 pp 411ndash425 1992
[2] D Mistry M Altini H G Coleman H Ali and E MaioranoldquoThe spatial and temporal expression of calretinin in developingrat molars (Rattus norvegicus)rdquoArchives of Oral Biology vol 46no 10 pp 973ndash981 2001
[3] P Devilliers H Liu C Suggs et al ldquoCalretinin expression inthe differential diagnosis of human ameloblastoma and kera-tocystic odontogenic tumorrdquo The American Journal of SurgicalPathology vol 32 no 2 pp 256ndash260 2008
[4] M Alaeddini S Etemad-Moghadam and F Baghaii ldquoCompar-ative expression of calretinin in selected odontogenic tumours
a possible relationship to histogenesisrdquo Histopathology vol 52no 3 pp 299ndash304 2008
[5] S K Sundaragiri J Chawda S Gill S Odedra and G ParmarldquoCalretinin expression in unicystic ameloblastoma an aid indifferential diagnosisrdquo Journal of Oral Biosciences vol 52 no2 pp 164ndash169 2010
[6] G V Sherbet Calcium Signalling in Cancer Taylor amp FrancisBoca Raton Fla USA 2010
[7] A Lugli Y Forster P Haas et al ldquoCalretinin expression inhuman normal and neoplastic tissues a tissue microarrayanalysis on 5233 tissue samplesrdquo Human Pathology vol 34 no10 pp 994ndash1000 2003
[8] C Doglioni A P Dei Tos L Laurino et al ldquoCalretinin a novelimmunocytochemicalmarker formesotheliomardquoTheAmericanJournal of Surgical Pathology vol 20 no 9 pp 1037ndash1046 1996
[9] L Barnes J W Eveson P Reichart and D Sidransky EdsPathology amp Genetics Head and Neck Tumours IARC PressLyon France 2005
[10] R Rajendran and B Sivapathasundharam Shafers Oral Pathol-ogy Elsevier New York NY USA 2009
[11] D R Gnepp Diagnostic Surgical Pathology of the Head andNeck SaundersElsevier Philadelphia Pa USA 2009
[12] H Coleman M Altini H Ali C Doglioni G Favia and EMaiorano ldquoUse of calretinin in the differential diagnosis ofunicystic ameloblastomasrdquo Histopathology vol 38 no 4 pp312ndash317 2001
[13] A M Fernandes E C B Duarte F J G S Pimenta et alldquoOdontogenic tumors a study of 340 cases in a Brazilianpopulationrdquo Journal of Oral Pathology andMedicine vol 34 no10 pp 583ndash587 2005
[14] R C K Jordan and P M Speight ldquoCurrent concepts of odon-togenic tumoursrdquo Diagnostic Histopathology vol 15 no 6 pp303ndash310 2009
[15] P A Reichart P Reichart and H P Philipsen OdontogenicTumors and Allied Lesions Quintessence 2004
[16] M Shear and P Speight Cysts of the Oral and MaxillofacialRegions Wiley New York NY USA 2008
[17] B W Neville Oral and Maxillofacial Pathology WB SaundersPhiladelphia Pa USA 2002
[18] H P Philipsen and P A Reichart ldquoUnicystic ameloblastoma Areview of 193 cases from the literaturerdquo Oral Oncology vol 34no 5 pp 317ndash325 1998
[19] M Altini H Coleman C Doglioni G Favia and E MaioranoldquoCalretinin expression in ameloblastomasrdquoHistopathology vol37 no 1 pp 27ndash32 2000
[20] S DrsquoSilva M K Sumathi N Balaji et al ldquoEvaluation ofcalretinin expression in Ameloblastoma and non-neoplasticodontogenic cystsmdashan immunohistochemical studyrdquo Journal ofInternational Oral Health vol 5 no 6 pp 42ndash48 2013
[21] A Piattelli M Fioroni G Iezzi and C Rubini ldquoCalretininexpression in odontogenic cystsrdquo Journal of Endodontics vol 29no 6 pp 394ndash396 2003
[22] M J Hubbard N J McHugh and J E Mangum ldquoExclusionof all three calbindins from a calcium-ferry role in rat enamelcellsrdquo European Journal of Oral Sciences vol 119 no 1 pp 112ndash119 2011
[23] V Gotzos B Schwaller N HetzelM Bustos-Castillo andM RCelio ldquoExpression of the calcium binding protein calretinin inWiDr cells and its correlation to their cell cyclerdquo ExperimentalCell Research vol 202 no 2 pp 292ndash302 1992
Pathology Research International 7
[24] V Gotzos B Schwaller J-C Gander M Bustos-Castillo andM R Celio ldquoHeterogeneity of expression of the calcium-binding protein calretinin in human colonie cancer cell linesrdquoAnticancer Research vol 16 no 6B pp 3491ndash3498 1996
[25] J-C Gander V Gotzos B Fellay and B Schwaller ldquoInhibitionof the proliferative cycle and apoptotic events in WiDr cellsafter down-regulation of the calcium-binding protein calre-tinin using antisense oligodeoxynucleotidesrdquo Experimental CellResearch vol 225 no 2 pp 399ndash410 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 Pathology Research International
proliferation differentiation and neoplastic transformation[6]
Apart from its expression in normal human tissuescalretinin has been shown to be expressed in a wide vari-ety of tumors [7] Calretinin has recently emerged as animmunohistochemical marker with great utility for delin-eating mesothelioma and adenocarcinomas of lung as itsdiagnostic sensitivity for mesothelioma is nearly 100 [8]
Odontogenic tumors comprise a group of heterogeneouslesions ranging from hamartomatous or nonneoplastic tissueproliferations to benign neoplasms to malignant tumors withmetastatic potential [9] The odontogenic cysts which maybe intimately associated with the development of certain ofthe odontogenic tumors also represent an aberration at somestage of odontogenesis [10] Keratocystic odontogenic tumor(KCOT) has been recently classified by World Health Orga-nization (WHO) in 2005 as a benign tumor of odontogenicepithelium to emphasize its neoplastic nature [9]
Unicystic ameloblastoma is considered at best an in situor superficially invasive form of ameloblastoma [11] Uni-cystic ameloblastomas arewell known to be lined by a variableepithelium ranging from one that has typical ameloblasticcharacteristics to one that is metaplastic and which appearscompletely nondescript consisting of several layers of nonker-atinizing squamous cells In such cases the differentiation ofodontogenic cysts from the unicystic ameloblastoma can beproblematic [12]
The histologic presentation of ameloblastoma especiallyunicystic type can be in some instances mistaken for ker-atocystic odontogenic tumor (KCOT) Overlapping clinicaland radiographic presentation further adds to this diagnosticdifficulty [3]
Hence the present study was carried out to evaluate andintercompare the expression of calretinin in ameloblastomaand keratocystic odontogenic tumor in order to assess itsusefulness as a confirmatory marker for ameloblastic tissuethat would aid in the differential diagnosis of such lesions
2 Materials and Methods
21 Case Selection Formalin-fixed paraffin-embedded tissueblocks of ameloblastoma (unicystic and multicystic variants)and KCOT (parakeratinized type) were retrieved from thearchives of Department of Oral and Maxillofacial PathologyPacific Dental College and Hospital Udaipur Re-evaluationof all cases was performed according to the World HealthOrganization histological typing of odontogenic tumors [9]by two oral pathologists on light microscopy using hema-toxylin and eosin sections The study protocol was reviewedby the Ethical Committee of Pacific Dental College andHospital and was granted ethical clearance
22 Immunohistochemistry Formalin-fixed paraffin-embed-ded tissue blocks were cut into 4 120583m thick sections andplaced on organosilane-pretreated slides Immunohisto-chemical staining was performed using the primary antibodyfor calretinin using supersensitive one-step polymer-HRPtechnique (Biogenex Life Sciences San Ramon CA USA)
The sections were deparaffinized and rehydrated throughxylene and descending grades of alcohol respectively Anti-gen retrieval was carried out using commercial microwaveantigen retrieval system where the sections were immersedin 10mM sodium citrate buffer (pH 60) at 800 420 and320∘F for three cycles of 10min each (EZ-Retriever SystemBiogenex Life Sciences) After rinsing in tris buffer (pH 72)the sections were incubated with 3 hydrogen peroxide inwater for 15min to block the endogenous peroxidase activityThis was followed by a power block for 10min at roomtemperature to block any nonspecific antigenic sites Thesectionswere then incubatedwith optimally prediluted rabbitpolyclonal antibody against calretinin protein (BiogenexCA USA) for 30min at room temperature in a moistchamber After washing with tris buffer (pH 72) for 5minthe sections were then incubated with super enhancer for20min at room temperature followed by secondary antibodyincubation with one-step polymer-HRP reagent for 30minat room temperature in a moist chamber Visualizationwas performed using freshly prepared 331015840-diaminobenzidinehydrochloride (DAB) substrate (Sigma) for 5min The slideswere counterstained with Mayerrsquos hematoxylin for 3minsubsequent to which sections were dehydrated cleared andmounted with dibutyl phthalate xylene (DPX) (RankemRFCL Ltd) For each batch of staining positive and negativecontrols were run simultaneously with the study specimensHuman mesothelioma which is known to have a high levelof calretinin expression served as the positive control whilethe primary antibodies were replaced by nonimmune mouseserum at the same dilutions for the negative controls
23 Evaluation of Slides The evaluation of the stained slideswas carried out using a binocular research microscope(Lawrence ampMayo) under 100x and 400x magnificationThesections stained with calretinin antibody were evaluated forthe presence localization distribution and intensity of theimmunoreactive cells [4] Presence was evaluated to estimatewhether the staining was positive or negative and if positivewhich epithelial layer was stained Localizationwas evaluatedto estimate whether the stainingwas nuclear (N) cytoplasmic(C) or both Distribution was evaluated as being either focal(involving lt50 of positive cells) or diffuse (involving gt50of positive cells) The intensity was graded based on thenumber of positive cells seen 0 = no staining 1 = weakstaining 2 = moderate staining 3 = intense staining
The Chi-square test was applied to intercompare thecalretinin expression between ameloblastoma andKCOT andfor the comparison between the variants of ameloblastoma(unicystic and multicystic) P values lt005 were consideredto be statistically significant
3 Results
A total of 40 cases (20 each) of ameloblastoma and KCOTwere studied Out of the 20 cases of ameloblastoma 16were of unicystic type and the remaining 4 were of solidmulticystic type [2 follicular 1 plexiform and 1 granular cellameloblastoma]
Pathology Research International 3
Table 1 Intercomparison of calretinin presence in ameloblastomaand KCOT
Presence Ameloblastoma (119899 = 20) KCOT (119899 = 20)Frequency Percent Frequency Percent
+ 12 30 1 25minus 8 20 19 475119875lowast value 0000lowast119875 value lt 005 statistically significant
31 Unicystic Ameloblastoma Out of the 16 cases of uni-cystic ameloblastoma positive calretinin expression of theameloblastic epithelium was seen in 8 (50) cases In allthe immunopositive cases reactivity was observed in boththe nucleus and cytoplasm of the cells The distribution ofcalretinin was focal in 5 and diffuse in 3 cases and waslimited to the stellate reticulum like area The luminal layerof ameloblast-like cells did not stain except for the few singlebasal cells that were positive in 2 cases only Four casesshowed weak staining 3 showed moderate and 1 showedsevere staining of the ameloblastic epithelium (Figure 1)
32 SolidMulticystic Ameloblastoma All the 4 cases showedweak positive staining of stellate reticulum like areas whereasonly one case showed focal positivity in the basal cell layeralso Immunoreactivity was observed in both the nucleus andcytoplasm of the cells Staining was focally distributed in 3cases while one case stained diffusely (Figure 2)
In addition all the cases of ameloblastoma also showedscattered positive cells within the stroma whichwere thoughtto be nonepithelial in type and could represent mast cells
33 Keratocystic Odontogenic Tumor Nineteen (95) casesshowed negative staining of calretinin in the epithelial liningof the cyst except for some scattered darkly stained individ-ual cells in the fibrous connective tissue wall Only one casethat showed positivity to calretinin revealed a highly inflamedodontogenic keratocyst with one bit of tissue depictingstellate reticulum like epithelium overlying the palisadedbasal cell layer in the hematoxylin and eosin stained sectionsThe calretinin staining for the same bit showed uniformdiffuse immunopositivity of the nucleus and cytoplasm of thestellate reticulum like epithelium (Figure 3)
The intercomparison of calretinin positivity betweenameloblastoma and KCOT revealed a statistically significantdifference at 119875 = 0000 (Table 1)
4 Discussion
Odontogenic cysts and tumors are a group of lesions aris-ing from the tooth-producing apparatus or its remnantsThey may originate from odontogenic epithelium andorectomesenchyme with varying degrees of inductive tissueinteraction [13] They are rare and lack of familiarity withthese lesions and their variable appearance may lead todifficulties in diagnosis with occasional serious confusionwith more sinister lesions [14]
Different odontogenic cysts and tumors have variableclinical and biological behaviors Ameloblastoma is a benignlocally aggressive epithelial odontogenic tumor that hasthe potential to become malignant and produce metastasisto distant sites such as lungs and kidneys KCOT is anaggressive cyst with neoplastic behaviour while unicysticameloblastoma is a neoplasm with cyst like behaviour [1516] KCOT also arises from cell rests of the dental lam-ina same origin as ameloblastoma and there are clinicaland radiographic similarities between KCOT and unicysticameloblastoma as both present as ordinary cysts in thedentate areas [17] Histologically unicystic ameloblastomais lined in some areas but rarely entirely by odontogenicepithelium of ameloblastoma appearance and stratified squa-mous epithelium in the remaining areas [18] In fact suchsquamous metaplasia is a relatively frequent phenomenon inunicystic ameloblastoma and many of these lesions are linedby such nondescript epithelium which can create diagnosticconfusion with odontogenic cysts [12]
KCOT is characterized histologically by a palisaded basalcell layer of basophilic columnar cells and a surface of cor-rugated parakeratin sometimes with spongiosis resemblingclosely the stellate like reticulum and the acanthomatousdifferentiation of ameloblastoma If the tissue sample is smalland if the neoplastic epithelium displays reactive changesinduced by inflammation it can closely resemble unicysticameloblastoma histologically [3] Thus at times both lesionsbecome histologically indistinguishable
Many techniques have been used in an attempt to distin-guish odontogenic cysts (including KCOT) from ameloblas-tomas (especially unicystic type) which include demon-stration of cell surface carbohydrates with blood groupspecificity determination of alkaline phosphatase activityin the stroma distribution of lectins and involucrin in theepithelium characterization of cytokeratin profiles countingof AgNORs and quantification of cell proliferation markerssuch as PCNA and Ki67 While differences have been shownto occur between various cysts and ameloblastomas consid-erable overlap exists and none of the above techniques can beused to routinely distinguish these lesions from one another[5]
Also a number of studies have reported the immuno-histochemical expression of intermediate filaments growthfactors basement membrane components cell cycle regu-lating factors and apoptotic proteins in ameloblastomas butcalcium-binding proteins have not been investigated to agreater extent in these tumors [19]
The present study assessed the expression of calretinin in20 cases each of ameloblastoma and keratocystic odontogenictumor and the results demonstrated frequent expressionof calretinin in the epithelium of both unicystic and solidmulticystic ameloblastomas Positive staining was seen in50 (8 cases) of unicystic ameloblastoma and 100 (4 cases)of multicystic ameloblastoma whereas only 1 out of 20 casesof KCOT lining showed positive staining for calretinin Theintercomparison between both groups revealed a statisticallysignificant difference at 119875 = 0000 Also the immunopositiv-ity was seen exclusively in the stellate reticulum like epithe-lium in both the unicystic and multicystic ameloblastomas
4 Pathology Research International
(a) 100x (b) 400x
Figure 1 Photomicrograph showing calretinin staining in unicystic ameloblastoma in (a) 100x and (b) 400x
(a) 100x (b) 400x
Figure 2 Photomicrograph showing calretinin staining in solid multicystic ameloblastoma in (a) 100x and (b) 400x
(a) (b)
Figure 3 Photomicrograph showing (a) negative calretinin staining in keratocystic odontogenic tumor (100x) and (b) positive calretininstaining in keratocystic odontogenic tumor (100x)
Pathology Research International 5
and the ameloblast-like basal cells were positive in only 1 ofthe multicystic and 2 of the unicystic variants where singlecell expressing calretinin was observed
These findings were in accordance with earlier studieswhich also observed calretinin positive cells restricted to theneoplastic stellate reticulum like epithelium in ameloblas-toma only Altini et al [19] and Coleman et al [12] foundpositive staining in 815 cases of unicystic ameloblastomasand 935 cases of multicystic ameloblastoma while Dev-illiers et al [3] Sundaragiri et al [5] and DrsquoSilva et al[20] found positivity in all cases of ameloblastoma (100)In all these studies none of the odontogenic cystsrsquo liningshowed positivity except DrsquoSilva et al [20] who observedpositive staining of the cystic lining epithelium and keratinflakes in the cystic lumen of 40 cases of odontogenickeratocystThe authors attribute this finding to the aggressivebiologic behavior of odontogenic keratocyst similar to abenign neoplasm and its high mitotic activity as comparedto other nonneoplastic odontogenic cysts Also Piattelli et al[21] found positivity to calretinin in 8 of 12 parakeratinizedkeratocysts in the parabasal-intermediate layers of the cystepithelium This could point to the aggressive behavior ofKCOT and help to explain the differences in the clinical andpathologic behavior of odontogenic keratocysts in particularthe differences found between orthokeratinized keratocystsand parakeratinized keratocysts
Alaeddini et al [4] also found that calretinin immunore-activity was positive only for ameloblastoma when comparedto calcifying epithelial odontogenic tumour adenomatoidodontogenic tumour ameloblastic fibroma and odontogenicmyxoma stating that this protein may have a role in thetransition of the dental lamina remnants to ameloblastomaThey hypothesized that calretinin may be one of the factorsresponsible for the differences between this aggressive neo-plasm and other odontogenic tumors studied
Further in the present study the distribution pattern ofthe immunopositive cells was focal in 8 cases (40) anddiffuse in 4 cases (20) Also the staining was weak in mostof the cases (40) with 3 cases (15) showing moderate andonly 1 case (5) intense stainingThe staining was not equallydistributed throughout the sections with some areas showingintense staining but absolutely no staining in the immediatevicinity This was in contrast to the earlier studies wheremost of the cases showed intense staining of the ameloblasticepithelium [3ndash5 12 19 20]
Altini et al [19] stated that the better the differentiationof the epithelium was the lesser the expression of calretininoccurred in their study where they found little or noimmunostaining in those cases of unicystic ameloblastomasthat were lined by typical ameloblastic epithelium while theepithelium which completely lacked ameloblastic featuresfrequently expressed calretinin Hence they indicated thatcalretinin expression in some cells varied according to theirmetabolic activity andmay be lost when this activity changesLater Coleman et al [12] observed intense positive stainingin both areas of nondescript epithelial lining and areas withtypical ameloblastic features in unicystic ameloblastomawhich indicated that although the metaplastic cyst liningsmay have lost their typical ameloblastic features the cells have
retained their immunophenotypic characteristics resultingin the continued expression of calretinin Our study can becorrelated with the observation of Altini et al [19] as majorityof the unicystic ameloblastoma cases that we observed werelined by typical ameloblastic epithelium due to which theymay not have stained intensely with calretinin
In a study by Mistry et al [2] on developing rat molarscalretinin immunoreactivity was present in the inner enamelepithelium and presecretory ameloblasts from the late capstage onwards In the cap and late cap stages many ofthe specimens were immunopositive for calretinin in thestellate reticulum and this number increased to gt90 for theearly and late bell stages In the present study the patternof reactivity of the stellate reticulum observed appearedsimilar to the late bell stage of normal tooth developmentHowever in the peripheral layers of the ameloblastic islandscalretinin immunoreactivity was not observed as was the casein normal tooth germs As enamel organ has been proposedto be one of the possible origins of ameloblastoma [17] thispeculiar distribution of calretinin in ameloblastic epitheliumis noteworthy and it thus appears that there is no obviouscorrelation between the staining of normal odontogenictissues and their neoplastic counterparts [19]
A possible explanation for this dynamic spatial andtemporal distribution was that calretinin may be presentonly in cells that reside directly in the path of calciumin transition on its way to the enamel matrix acting as aldquocalcium ferryrdquo [2] However Hubbard et al [22] found thatcalretinin was primarily expressed during the differentiationstage of enamel formation and only a faint calretinin bandwas observed at secretion stage while no such band wasdetectable during maturation Based on these findings theauthors suggest retirement of the calcium ferry dogma fromenamel biologymdashin murine models at least
Gotzos et al [23 24] have shown increased expressionof calretinin in rapidly proliferating WiDr colon adenocar-cinomas cells Upon being induced to differentiate by treat-mentwith sodiumbutyrate and hexamethylene bisacetamidethey showed marked reductions in cell proliferation as wellas expression of full length calretinin When treated witholigonucleotides against calretinin synthesis these cells wereblocked in the G1 phase of the cell cycle and subsequentlyunderwent apoptosisThese authors suggested that calretininmay maintain an undifferentiated proliferative state charac-teristic of neoplastic transformation Also calretinin may actas an antiapoptotic factor [25]
The single case of KCOT in our study that showedpositivity to calretinin was of a 17-year-old male patienthaving radiolucency in 24 and 25 region with impacted 23The hematoxylin and eosin stained sections of the biopsyspecimen revealed a highly inflamed odontogenic keratocystwith one bit of tissue depicting stellate reticulummdashlikeepithelium overlying the palisaded basal cell layer Uponcalretinin staining uniform diffuse immunopositivity of thestellate reticulum like epitheliumwas observedThis suggeststhat the previous biopsy may have been misdiagnosed asKCOT on the basis of hematoxylin and eosin staining
This result can be compared with that of Devilliers et al[3] wherein they evaluated a tumor from their archives
6 Pathology Research International
originally diagnosed as KCOT which recurred 2 years laterHistologic sections from the tissue biopsied earlier (diag-nosed as KCOT) and from the tissue sample of the recurrence(diagnosed as ameloblastoma)were testedwith calretinin andboth showed positive staining of the neoplastic epitheliumconfined to the stellate reticulum
This finding helps us to understand the importance of cal-retinin as a differential diagnostic marker for ameloblastomaand how important it is for the pathologist to differentiateboth entities which carry different treatment protocols withpotentially serious functional and esthetic consequences forthe patient
Few nonepithelial cells that stained positive for calretininwere also observed in the connective tissue stroma of virtuallyall cases of ameloblastoma and KCOT in our study Altiniet al [19] and Coleman et al [12] also found such darklystained cells within the tumor or cyst epithelium and inthe fibrous connective tissue walls These were interpretedas being mast cells or Langerhans cells both of whichhave been documented as occurring in ameloblastomas andodontogenic cysts
5 Conclusion
The present study suggests that calretinin may be usedas a specific immunohistochemical marker for neoplasticameloblastic epithelium as calretinin positivity was observedexclusively in ameloblastomas Hence it can serve as animportant diagnostic adjunct in the differential diagnosisof ameloblastoma and keratocystic odontogenic tumor Theexpression of calretinin in these neoplastic lesions mightbe recapitulating dental ontogeny as its role during normaltooth development has also been speculated
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
Theauthors wish to thank all themembers in theDepartmentofOral andMaxillofacial Pathology for their general support
References
[1] C W Heizmann ldquoCalcium-binding proteins basic conceptsand clinical implicationsrdquo General Physiology and Biophysicsvol 11 no 5 pp 411ndash425 1992
[2] D Mistry M Altini H G Coleman H Ali and E MaioranoldquoThe spatial and temporal expression of calretinin in developingrat molars (Rattus norvegicus)rdquoArchives of Oral Biology vol 46no 10 pp 973ndash981 2001
[3] P Devilliers H Liu C Suggs et al ldquoCalretinin expression inthe differential diagnosis of human ameloblastoma and kera-tocystic odontogenic tumorrdquo The American Journal of SurgicalPathology vol 32 no 2 pp 256ndash260 2008
[4] M Alaeddini S Etemad-Moghadam and F Baghaii ldquoCompar-ative expression of calretinin in selected odontogenic tumours
a possible relationship to histogenesisrdquo Histopathology vol 52no 3 pp 299ndash304 2008
[5] S K Sundaragiri J Chawda S Gill S Odedra and G ParmarldquoCalretinin expression in unicystic ameloblastoma an aid indifferential diagnosisrdquo Journal of Oral Biosciences vol 52 no2 pp 164ndash169 2010
[6] G V Sherbet Calcium Signalling in Cancer Taylor amp FrancisBoca Raton Fla USA 2010
[7] A Lugli Y Forster P Haas et al ldquoCalretinin expression inhuman normal and neoplastic tissues a tissue microarrayanalysis on 5233 tissue samplesrdquo Human Pathology vol 34 no10 pp 994ndash1000 2003
[8] C Doglioni A P Dei Tos L Laurino et al ldquoCalretinin a novelimmunocytochemicalmarker formesotheliomardquoTheAmericanJournal of Surgical Pathology vol 20 no 9 pp 1037ndash1046 1996
[9] L Barnes J W Eveson P Reichart and D Sidransky EdsPathology amp Genetics Head and Neck Tumours IARC PressLyon France 2005
[10] R Rajendran and B Sivapathasundharam Shafers Oral Pathol-ogy Elsevier New York NY USA 2009
[11] D R Gnepp Diagnostic Surgical Pathology of the Head andNeck SaundersElsevier Philadelphia Pa USA 2009
[12] H Coleman M Altini H Ali C Doglioni G Favia and EMaiorano ldquoUse of calretinin in the differential diagnosis ofunicystic ameloblastomasrdquo Histopathology vol 38 no 4 pp312ndash317 2001
[13] A M Fernandes E C B Duarte F J G S Pimenta et alldquoOdontogenic tumors a study of 340 cases in a Brazilianpopulationrdquo Journal of Oral Pathology andMedicine vol 34 no10 pp 583ndash587 2005
[14] R C K Jordan and P M Speight ldquoCurrent concepts of odon-togenic tumoursrdquo Diagnostic Histopathology vol 15 no 6 pp303ndash310 2009
[15] P A Reichart P Reichart and H P Philipsen OdontogenicTumors and Allied Lesions Quintessence 2004
[16] M Shear and P Speight Cysts of the Oral and MaxillofacialRegions Wiley New York NY USA 2008
[17] B W Neville Oral and Maxillofacial Pathology WB SaundersPhiladelphia Pa USA 2002
[18] H P Philipsen and P A Reichart ldquoUnicystic ameloblastoma Areview of 193 cases from the literaturerdquo Oral Oncology vol 34no 5 pp 317ndash325 1998
[19] M Altini H Coleman C Doglioni G Favia and E MaioranoldquoCalretinin expression in ameloblastomasrdquoHistopathology vol37 no 1 pp 27ndash32 2000
[20] S DrsquoSilva M K Sumathi N Balaji et al ldquoEvaluation ofcalretinin expression in Ameloblastoma and non-neoplasticodontogenic cystsmdashan immunohistochemical studyrdquo Journal ofInternational Oral Health vol 5 no 6 pp 42ndash48 2013
[21] A Piattelli M Fioroni G Iezzi and C Rubini ldquoCalretininexpression in odontogenic cystsrdquo Journal of Endodontics vol 29no 6 pp 394ndash396 2003
[22] M J Hubbard N J McHugh and J E Mangum ldquoExclusionof all three calbindins from a calcium-ferry role in rat enamelcellsrdquo European Journal of Oral Sciences vol 119 no 1 pp 112ndash119 2011
[23] V Gotzos B Schwaller N HetzelM Bustos-Castillo andM RCelio ldquoExpression of the calcium binding protein calretinin inWiDr cells and its correlation to their cell cyclerdquo ExperimentalCell Research vol 202 no 2 pp 292ndash302 1992
Pathology Research International 7
[24] V Gotzos B Schwaller J-C Gander M Bustos-Castillo andM R Celio ldquoHeterogeneity of expression of the calcium-binding protein calretinin in human colonie cancer cell linesrdquoAnticancer Research vol 16 no 6B pp 3491ndash3498 1996
[25] J-C Gander V Gotzos B Fellay and B Schwaller ldquoInhibitionof the proliferative cycle and apoptotic events in WiDr cellsafter down-regulation of the calcium-binding protein calre-tinin using antisense oligodeoxynucleotidesrdquo Experimental CellResearch vol 225 no 2 pp 399ndash410 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Pathology Research International 3
Table 1 Intercomparison of calretinin presence in ameloblastomaand KCOT
Presence Ameloblastoma (119899 = 20) KCOT (119899 = 20)Frequency Percent Frequency Percent
+ 12 30 1 25minus 8 20 19 475119875lowast value 0000lowast119875 value lt 005 statistically significant
31 Unicystic Ameloblastoma Out of the 16 cases of uni-cystic ameloblastoma positive calretinin expression of theameloblastic epithelium was seen in 8 (50) cases In allthe immunopositive cases reactivity was observed in boththe nucleus and cytoplasm of the cells The distribution ofcalretinin was focal in 5 and diffuse in 3 cases and waslimited to the stellate reticulum like area The luminal layerof ameloblast-like cells did not stain except for the few singlebasal cells that were positive in 2 cases only Four casesshowed weak staining 3 showed moderate and 1 showedsevere staining of the ameloblastic epithelium (Figure 1)
32 SolidMulticystic Ameloblastoma All the 4 cases showedweak positive staining of stellate reticulum like areas whereasonly one case showed focal positivity in the basal cell layeralso Immunoreactivity was observed in both the nucleus andcytoplasm of the cells Staining was focally distributed in 3cases while one case stained diffusely (Figure 2)
In addition all the cases of ameloblastoma also showedscattered positive cells within the stroma whichwere thoughtto be nonepithelial in type and could represent mast cells
33 Keratocystic Odontogenic Tumor Nineteen (95) casesshowed negative staining of calretinin in the epithelial liningof the cyst except for some scattered darkly stained individ-ual cells in the fibrous connective tissue wall Only one casethat showed positivity to calretinin revealed a highly inflamedodontogenic keratocyst with one bit of tissue depictingstellate reticulum like epithelium overlying the palisadedbasal cell layer in the hematoxylin and eosin stained sectionsThe calretinin staining for the same bit showed uniformdiffuse immunopositivity of the nucleus and cytoplasm of thestellate reticulum like epithelium (Figure 3)
The intercomparison of calretinin positivity betweenameloblastoma and KCOT revealed a statistically significantdifference at 119875 = 0000 (Table 1)
4 Discussion
Odontogenic cysts and tumors are a group of lesions aris-ing from the tooth-producing apparatus or its remnantsThey may originate from odontogenic epithelium andorectomesenchyme with varying degrees of inductive tissueinteraction [13] They are rare and lack of familiarity withthese lesions and their variable appearance may lead todifficulties in diagnosis with occasional serious confusionwith more sinister lesions [14]
Different odontogenic cysts and tumors have variableclinical and biological behaviors Ameloblastoma is a benignlocally aggressive epithelial odontogenic tumor that hasthe potential to become malignant and produce metastasisto distant sites such as lungs and kidneys KCOT is anaggressive cyst with neoplastic behaviour while unicysticameloblastoma is a neoplasm with cyst like behaviour [1516] KCOT also arises from cell rests of the dental lam-ina same origin as ameloblastoma and there are clinicaland radiographic similarities between KCOT and unicysticameloblastoma as both present as ordinary cysts in thedentate areas [17] Histologically unicystic ameloblastomais lined in some areas but rarely entirely by odontogenicepithelium of ameloblastoma appearance and stratified squa-mous epithelium in the remaining areas [18] In fact suchsquamous metaplasia is a relatively frequent phenomenon inunicystic ameloblastoma and many of these lesions are linedby such nondescript epithelium which can create diagnosticconfusion with odontogenic cysts [12]
KCOT is characterized histologically by a palisaded basalcell layer of basophilic columnar cells and a surface of cor-rugated parakeratin sometimes with spongiosis resemblingclosely the stellate like reticulum and the acanthomatousdifferentiation of ameloblastoma If the tissue sample is smalland if the neoplastic epithelium displays reactive changesinduced by inflammation it can closely resemble unicysticameloblastoma histologically [3] Thus at times both lesionsbecome histologically indistinguishable
Many techniques have been used in an attempt to distin-guish odontogenic cysts (including KCOT) from ameloblas-tomas (especially unicystic type) which include demon-stration of cell surface carbohydrates with blood groupspecificity determination of alkaline phosphatase activityin the stroma distribution of lectins and involucrin in theepithelium characterization of cytokeratin profiles countingof AgNORs and quantification of cell proliferation markerssuch as PCNA and Ki67 While differences have been shownto occur between various cysts and ameloblastomas consid-erable overlap exists and none of the above techniques can beused to routinely distinguish these lesions from one another[5]
Also a number of studies have reported the immuno-histochemical expression of intermediate filaments growthfactors basement membrane components cell cycle regu-lating factors and apoptotic proteins in ameloblastomas butcalcium-binding proteins have not been investigated to agreater extent in these tumors [19]
The present study assessed the expression of calretinin in20 cases each of ameloblastoma and keratocystic odontogenictumor and the results demonstrated frequent expressionof calretinin in the epithelium of both unicystic and solidmulticystic ameloblastomas Positive staining was seen in50 (8 cases) of unicystic ameloblastoma and 100 (4 cases)of multicystic ameloblastoma whereas only 1 out of 20 casesof KCOT lining showed positive staining for calretinin Theintercomparison between both groups revealed a statisticallysignificant difference at 119875 = 0000 Also the immunopositiv-ity was seen exclusively in the stellate reticulum like epithe-lium in both the unicystic and multicystic ameloblastomas
4 Pathology Research International
(a) 100x (b) 400x
Figure 1 Photomicrograph showing calretinin staining in unicystic ameloblastoma in (a) 100x and (b) 400x
(a) 100x (b) 400x
Figure 2 Photomicrograph showing calretinin staining in solid multicystic ameloblastoma in (a) 100x and (b) 400x
(a) (b)
Figure 3 Photomicrograph showing (a) negative calretinin staining in keratocystic odontogenic tumor (100x) and (b) positive calretininstaining in keratocystic odontogenic tumor (100x)
Pathology Research International 5
and the ameloblast-like basal cells were positive in only 1 ofthe multicystic and 2 of the unicystic variants where singlecell expressing calretinin was observed
These findings were in accordance with earlier studieswhich also observed calretinin positive cells restricted to theneoplastic stellate reticulum like epithelium in ameloblas-toma only Altini et al [19] and Coleman et al [12] foundpositive staining in 815 cases of unicystic ameloblastomasand 935 cases of multicystic ameloblastoma while Dev-illiers et al [3] Sundaragiri et al [5] and DrsquoSilva et al[20] found positivity in all cases of ameloblastoma (100)In all these studies none of the odontogenic cystsrsquo liningshowed positivity except DrsquoSilva et al [20] who observedpositive staining of the cystic lining epithelium and keratinflakes in the cystic lumen of 40 cases of odontogenickeratocystThe authors attribute this finding to the aggressivebiologic behavior of odontogenic keratocyst similar to abenign neoplasm and its high mitotic activity as comparedto other nonneoplastic odontogenic cysts Also Piattelli et al[21] found positivity to calretinin in 8 of 12 parakeratinizedkeratocysts in the parabasal-intermediate layers of the cystepithelium This could point to the aggressive behavior ofKCOT and help to explain the differences in the clinical andpathologic behavior of odontogenic keratocysts in particularthe differences found between orthokeratinized keratocystsand parakeratinized keratocysts
Alaeddini et al [4] also found that calretinin immunore-activity was positive only for ameloblastoma when comparedto calcifying epithelial odontogenic tumour adenomatoidodontogenic tumour ameloblastic fibroma and odontogenicmyxoma stating that this protein may have a role in thetransition of the dental lamina remnants to ameloblastomaThey hypothesized that calretinin may be one of the factorsresponsible for the differences between this aggressive neo-plasm and other odontogenic tumors studied
Further in the present study the distribution pattern ofthe immunopositive cells was focal in 8 cases (40) anddiffuse in 4 cases (20) Also the staining was weak in mostof the cases (40) with 3 cases (15) showing moderate andonly 1 case (5) intense stainingThe staining was not equallydistributed throughout the sections with some areas showingintense staining but absolutely no staining in the immediatevicinity This was in contrast to the earlier studies wheremost of the cases showed intense staining of the ameloblasticepithelium [3ndash5 12 19 20]
Altini et al [19] stated that the better the differentiationof the epithelium was the lesser the expression of calretininoccurred in their study where they found little or noimmunostaining in those cases of unicystic ameloblastomasthat were lined by typical ameloblastic epithelium while theepithelium which completely lacked ameloblastic featuresfrequently expressed calretinin Hence they indicated thatcalretinin expression in some cells varied according to theirmetabolic activity andmay be lost when this activity changesLater Coleman et al [12] observed intense positive stainingin both areas of nondescript epithelial lining and areas withtypical ameloblastic features in unicystic ameloblastomawhich indicated that although the metaplastic cyst liningsmay have lost their typical ameloblastic features the cells have
retained their immunophenotypic characteristics resultingin the continued expression of calretinin Our study can becorrelated with the observation of Altini et al [19] as majorityof the unicystic ameloblastoma cases that we observed werelined by typical ameloblastic epithelium due to which theymay not have stained intensely with calretinin
In a study by Mistry et al [2] on developing rat molarscalretinin immunoreactivity was present in the inner enamelepithelium and presecretory ameloblasts from the late capstage onwards In the cap and late cap stages many ofthe specimens were immunopositive for calretinin in thestellate reticulum and this number increased to gt90 for theearly and late bell stages In the present study the patternof reactivity of the stellate reticulum observed appearedsimilar to the late bell stage of normal tooth developmentHowever in the peripheral layers of the ameloblastic islandscalretinin immunoreactivity was not observed as was the casein normal tooth germs As enamel organ has been proposedto be one of the possible origins of ameloblastoma [17] thispeculiar distribution of calretinin in ameloblastic epitheliumis noteworthy and it thus appears that there is no obviouscorrelation between the staining of normal odontogenictissues and their neoplastic counterparts [19]
A possible explanation for this dynamic spatial andtemporal distribution was that calretinin may be presentonly in cells that reside directly in the path of calciumin transition on its way to the enamel matrix acting as aldquocalcium ferryrdquo [2] However Hubbard et al [22] found thatcalretinin was primarily expressed during the differentiationstage of enamel formation and only a faint calretinin bandwas observed at secretion stage while no such band wasdetectable during maturation Based on these findings theauthors suggest retirement of the calcium ferry dogma fromenamel biologymdashin murine models at least
Gotzos et al [23 24] have shown increased expressionof calretinin in rapidly proliferating WiDr colon adenocar-cinomas cells Upon being induced to differentiate by treat-mentwith sodiumbutyrate and hexamethylene bisacetamidethey showed marked reductions in cell proliferation as wellas expression of full length calretinin When treated witholigonucleotides against calretinin synthesis these cells wereblocked in the G1 phase of the cell cycle and subsequentlyunderwent apoptosisThese authors suggested that calretininmay maintain an undifferentiated proliferative state charac-teristic of neoplastic transformation Also calretinin may actas an antiapoptotic factor [25]
The single case of KCOT in our study that showedpositivity to calretinin was of a 17-year-old male patienthaving radiolucency in 24 and 25 region with impacted 23The hematoxylin and eosin stained sections of the biopsyspecimen revealed a highly inflamed odontogenic keratocystwith one bit of tissue depicting stellate reticulummdashlikeepithelium overlying the palisaded basal cell layer Uponcalretinin staining uniform diffuse immunopositivity of thestellate reticulum like epitheliumwas observedThis suggeststhat the previous biopsy may have been misdiagnosed asKCOT on the basis of hematoxylin and eosin staining
This result can be compared with that of Devilliers et al[3] wherein they evaluated a tumor from their archives
6 Pathology Research International
originally diagnosed as KCOT which recurred 2 years laterHistologic sections from the tissue biopsied earlier (diag-nosed as KCOT) and from the tissue sample of the recurrence(diagnosed as ameloblastoma)were testedwith calretinin andboth showed positive staining of the neoplastic epitheliumconfined to the stellate reticulum
This finding helps us to understand the importance of cal-retinin as a differential diagnostic marker for ameloblastomaand how important it is for the pathologist to differentiateboth entities which carry different treatment protocols withpotentially serious functional and esthetic consequences forthe patient
Few nonepithelial cells that stained positive for calretininwere also observed in the connective tissue stroma of virtuallyall cases of ameloblastoma and KCOT in our study Altiniet al [19] and Coleman et al [12] also found such darklystained cells within the tumor or cyst epithelium and inthe fibrous connective tissue walls These were interpretedas being mast cells or Langerhans cells both of whichhave been documented as occurring in ameloblastomas andodontogenic cysts
5 Conclusion
The present study suggests that calretinin may be usedas a specific immunohistochemical marker for neoplasticameloblastic epithelium as calretinin positivity was observedexclusively in ameloblastomas Hence it can serve as animportant diagnostic adjunct in the differential diagnosisof ameloblastoma and keratocystic odontogenic tumor Theexpression of calretinin in these neoplastic lesions mightbe recapitulating dental ontogeny as its role during normaltooth development has also been speculated
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
Theauthors wish to thank all themembers in theDepartmentofOral andMaxillofacial Pathology for their general support
References
[1] C W Heizmann ldquoCalcium-binding proteins basic conceptsand clinical implicationsrdquo General Physiology and Biophysicsvol 11 no 5 pp 411ndash425 1992
[2] D Mistry M Altini H G Coleman H Ali and E MaioranoldquoThe spatial and temporal expression of calretinin in developingrat molars (Rattus norvegicus)rdquoArchives of Oral Biology vol 46no 10 pp 973ndash981 2001
[3] P Devilliers H Liu C Suggs et al ldquoCalretinin expression inthe differential diagnosis of human ameloblastoma and kera-tocystic odontogenic tumorrdquo The American Journal of SurgicalPathology vol 32 no 2 pp 256ndash260 2008
[4] M Alaeddini S Etemad-Moghadam and F Baghaii ldquoCompar-ative expression of calretinin in selected odontogenic tumours
a possible relationship to histogenesisrdquo Histopathology vol 52no 3 pp 299ndash304 2008
[5] S K Sundaragiri J Chawda S Gill S Odedra and G ParmarldquoCalretinin expression in unicystic ameloblastoma an aid indifferential diagnosisrdquo Journal of Oral Biosciences vol 52 no2 pp 164ndash169 2010
[6] G V Sherbet Calcium Signalling in Cancer Taylor amp FrancisBoca Raton Fla USA 2010
[7] A Lugli Y Forster P Haas et al ldquoCalretinin expression inhuman normal and neoplastic tissues a tissue microarrayanalysis on 5233 tissue samplesrdquo Human Pathology vol 34 no10 pp 994ndash1000 2003
[8] C Doglioni A P Dei Tos L Laurino et al ldquoCalretinin a novelimmunocytochemicalmarker formesotheliomardquoTheAmericanJournal of Surgical Pathology vol 20 no 9 pp 1037ndash1046 1996
[9] L Barnes J W Eveson P Reichart and D Sidransky EdsPathology amp Genetics Head and Neck Tumours IARC PressLyon France 2005
[10] R Rajendran and B Sivapathasundharam Shafers Oral Pathol-ogy Elsevier New York NY USA 2009
[11] D R Gnepp Diagnostic Surgical Pathology of the Head andNeck SaundersElsevier Philadelphia Pa USA 2009
[12] H Coleman M Altini H Ali C Doglioni G Favia and EMaiorano ldquoUse of calretinin in the differential diagnosis ofunicystic ameloblastomasrdquo Histopathology vol 38 no 4 pp312ndash317 2001
[13] A M Fernandes E C B Duarte F J G S Pimenta et alldquoOdontogenic tumors a study of 340 cases in a Brazilianpopulationrdquo Journal of Oral Pathology andMedicine vol 34 no10 pp 583ndash587 2005
[14] R C K Jordan and P M Speight ldquoCurrent concepts of odon-togenic tumoursrdquo Diagnostic Histopathology vol 15 no 6 pp303ndash310 2009
[15] P A Reichart P Reichart and H P Philipsen OdontogenicTumors and Allied Lesions Quintessence 2004
[16] M Shear and P Speight Cysts of the Oral and MaxillofacialRegions Wiley New York NY USA 2008
[17] B W Neville Oral and Maxillofacial Pathology WB SaundersPhiladelphia Pa USA 2002
[18] H P Philipsen and P A Reichart ldquoUnicystic ameloblastoma Areview of 193 cases from the literaturerdquo Oral Oncology vol 34no 5 pp 317ndash325 1998
[19] M Altini H Coleman C Doglioni G Favia and E MaioranoldquoCalretinin expression in ameloblastomasrdquoHistopathology vol37 no 1 pp 27ndash32 2000
[20] S DrsquoSilva M K Sumathi N Balaji et al ldquoEvaluation ofcalretinin expression in Ameloblastoma and non-neoplasticodontogenic cystsmdashan immunohistochemical studyrdquo Journal ofInternational Oral Health vol 5 no 6 pp 42ndash48 2013
[21] A Piattelli M Fioroni G Iezzi and C Rubini ldquoCalretininexpression in odontogenic cystsrdquo Journal of Endodontics vol 29no 6 pp 394ndash396 2003
[22] M J Hubbard N J McHugh and J E Mangum ldquoExclusionof all three calbindins from a calcium-ferry role in rat enamelcellsrdquo European Journal of Oral Sciences vol 119 no 1 pp 112ndash119 2011
[23] V Gotzos B Schwaller N HetzelM Bustos-Castillo andM RCelio ldquoExpression of the calcium binding protein calretinin inWiDr cells and its correlation to their cell cyclerdquo ExperimentalCell Research vol 202 no 2 pp 292ndash302 1992
Pathology Research International 7
[24] V Gotzos B Schwaller J-C Gander M Bustos-Castillo andM R Celio ldquoHeterogeneity of expression of the calcium-binding protein calretinin in human colonie cancer cell linesrdquoAnticancer Research vol 16 no 6B pp 3491ndash3498 1996
[25] J-C Gander V Gotzos B Fellay and B Schwaller ldquoInhibitionof the proliferative cycle and apoptotic events in WiDr cellsafter down-regulation of the calcium-binding protein calre-tinin using antisense oligodeoxynucleotidesrdquo Experimental CellResearch vol 225 no 2 pp 399ndash410 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 Pathology Research International
(a) 100x (b) 400x
Figure 1 Photomicrograph showing calretinin staining in unicystic ameloblastoma in (a) 100x and (b) 400x
(a) 100x (b) 400x
Figure 2 Photomicrograph showing calretinin staining in solid multicystic ameloblastoma in (a) 100x and (b) 400x
(a) (b)
Figure 3 Photomicrograph showing (a) negative calretinin staining in keratocystic odontogenic tumor (100x) and (b) positive calretininstaining in keratocystic odontogenic tumor (100x)
Pathology Research International 5
and the ameloblast-like basal cells were positive in only 1 ofthe multicystic and 2 of the unicystic variants where singlecell expressing calretinin was observed
These findings were in accordance with earlier studieswhich also observed calretinin positive cells restricted to theneoplastic stellate reticulum like epithelium in ameloblas-toma only Altini et al [19] and Coleman et al [12] foundpositive staining in 815 cases of unicystic ameloblastomasand 935 cases of multicystic ameloblastoma while Dev-illiers et al [3] Sundaragiri et al [5] and DrsquoSilva et al[20] found positivity in all cases of ameloblastoma (100)In all these studies none of the odontogenic cystsrsquo liningshowed positivity except DrsquoSilva et al [20] who observedpositive staining of the cystic lining epithelium and keratinflakes in the cystic lumen of 40 cases of odontogenickeratocystThe authors attribute this finding to the aggressivebiologic behavior of odontogenic keratocyst similar to abenign neoplasm and its high mitotic activity as comparedto other nonneoplastic odontogenic cysts Also Piattelli et al[21] found positivity to calretinin in 8 of 12 parakeratinizedkeratocysts in the parabasal-intermediate layers of the cystepithelium This could point to the aggressive behavior ofKCOT and help to explain the differences in the clinical andpathologic behavior of odontogenic keratocysts in particularthe differences found between orthokeratinized keratocystsand parakeratinized keratocysts
Alaeddini et al [4] also found that calretinin immunore-activity was positive only for ameloblastoma when comparedto calcifying epithelial odontogenic tumour adenomatoidodontogenic tumour ameloblastic fibroma and odontogenicmyxoma stating that this protein may have a role in thetransition of the dental lamina remnants to ameloblastomaThey hypothesized that calretinin may be one of the factorsresponsible for the differences between this aggressive neo-plasm and other odontogenic tumors studied
Further in the present study the distribution pattern ofthe immunopositive cells was focal in 8 cases (40) anddiffuse in 4 cases (20) Also the staining was weak in mostof the cases (40) with 3 cases (15) showing moderate andonly 1 case (5) intense stainingThe staining was not equallydistributed throughout the sections with some areas showingintense staining but absolutely no staining in the immediatevicinity This was in contrast to the earlier studies wheremost of the cases showed intense staining of the ameloblasticepithelium [3ndash5 12 19 20]
Altini et al [19] stated that the better the differentiationof the epithelium was the lesser the expression of calretininoccurred in their study where they found little or noimmunostaining in those cases of unicystic ameloblastomasthat were lined by typical ameloblastic epithelium while theepithelium which completely lacked ameloblastic featuresfrequently expressed calretinin Hence they indicated thatcalretinin expression in some cells varied according to theirmetabolic activity andmay be lost when this activity changesLater Coleman et al [12] observed intense positive stainingin both areas of nondescript epithelial lining and areas withtypical ameloblastic features in unicystic ameloblastomawhich indicated that although the metaplastic cyst liningsmay have lost their typical ameloblastic features the cells have
retained their immunophenotypic characteristics resultingin the continued expression of calretinin Our study can becorrelated with the observation of Altini et al [19] as majorityof the unicystic ameloblastoma cases that we observed werelined by typical ameloblastic epithelium due to which theymay not have stained intensely with calretinin
In a study by Mistry et al [2] on developing rat molarscalretinin immunoreactivity was present in the inner enamelepithelium and presecretory ameloblasts from the late capstage onwards In the cap and late cap stages many ofthe specimens were immunopositive for calretinin in thestellate reticulum and this number increased to gt90 for theearly and late bell stages In the present study the patternof reactivity of the stellate reticulum observed appearedsimilar to the late bell stage of normal tooth developmentHowever in the peripheral layers of the ameloblastic islandscalretinin immunoreactivity was not observed as was the casein normal tooth germs As enamel organ has been proposedto be one of the possible origins of ameloblastoma [17] thispeculiar distribution of calretinin in ameloblastic epitheliumis noteworthy and it thus appears that there is no obviouscorrelation between the staining of normal odontogenictissues and their neoplastic counterparts [19]
A possible explanation for this dynamic spatial andtemporal distribution was that calretinin may be presentonly in cells that reside directly in the path of calciumin transition on its way to the enamel matrix acting as aldquocalcium ferryrdquo [2] However Hubbard et al [22] found thatcalretinin was primarily expressed during the differentiationstage of enamel formation and only a faint calretinin bandwas observed at secretion stage while no such band wasdetectable during maturation Based on these findings theauthors suggest retirement of the calcium ferry dogma fromenamel biologymdashin murine models at least
Gotzos et al [23 24] have shown increased expressionof calretinin in rapidly proliferating WiDr colon adenocar-cinomas cells Upon being induced to differentiate by treat-mentwith sodiumbutyrate and hexamethylene bisacetamidethey showed marked reductions in cell proliferation as wellas expression of full length calretinin When treated witholigonucleotides against calretinin synthesis these cells wereblocked in the G1 phase of the cell cycle and subsequentlyunderwent apoptosisThese authors suggested that calretininmay maintain an undifferentiated proliferative state charac-teristic of neoplastic transformation Also calretinin may actas an antiapoptotic factor [25]
The single case of KCOT in our study that showedpositivity to calretinin was of a 17-year-old male patienthaving radiolucency in 24 and 25 region with impacted 23The hematoxylin and eosin stained sections of the biopsyspecimen revealed a highly inflamed odontogenic keratocystwith one bit of tissue depicting stellate reticulummdashlikeepithelium overlying the palisaded basal cell layer Uponcalretinin staining uniform diffuse immunopositivity of thestellate reticulum like epitheliumwas observedThis suggeststhat the previous biopsy may have been misdiagnosed asKCOT on the basis of hematoxylin and eosin staining
This result can be compared with that of Devilliers et al[3] wherein they evaluated a tumor from their archives
6 Pathology Research International
originally diagnosed as KCOT which recurred 2 years laterHistologic sections from the tissue biopsied earlier (diag-nosed as KCOT) and from the tissue sample of the recurrence(diagnosed as ameloblastoma)were testedwith calretinin andboth showed positive staining of the neoplastic epitheliumconfined to the stellate reticulum
This finding helps us to understand the importance of cal-retinin as a differential diagnostic marker for ameloblastomaand how important it is for the pathologist to differentiateboth entities which carry different treatment protocols withpotentially serious functional and esthetic consequences forthe patient
Few nonepithelial cells that stained positive for calretininwere also observed in the connective tissue stroma of virtuallyall cases of ameloblastoma and KCOT in our study Altiniet al [19] and Coleman et al [12] also found such darklystained cells within the tumor or cyst epithelium and inthe fibrous connective tissue walls These were interpretedas being mast cells or Langerhans cells both of whichhave been documented as occurring in ameloblastomas andodontogenic cysts
5 Conclusion
The present study suggests that calretinin may be usedas a specific immunohistochemical marker for neoplasticameloblastic epithelium as calretinin positivity was observedexclusively in ameloblastomas Hence it can serve as animportant diagnostic adjunct in the differential diagnosisof ameloblastoma and keratocystic odontogenic tumor Theexpression of calretinin in these neoplastic lesions mightbe recapitulating dental ontogeny as its role during normaltooth development has also been speculated
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
Theauthors wish to thank all themembers in theDepartmentofOral andMaxillofacial Pathology for their general support
References
[1] C W Heizmann ldquoCalcium-binding proteins basic conceptsand clinical implicationsrdquo General Physiology and Biophysicsvol 11 no 5 pp 411ndash425 1992
[2] D Mistry M Altini H G Coleman H Ali and E MaioranoldquoThe spatial and temporal expression of calretinin in developingrat molars (Rattus norvegicus)rdquoArchives of Oral Biology vol 46no 10 pp 973ndash981 2001
[3] P Devilliers H Liu C Suggs et al ldquoCalretinin expression inthe differential diagnosis of human ameloblastoma and kera-tocystic odontogenic tumorrdquo The American Journal of SurgicalPathology vol 32 no 2 pp 256ndash260 2008
[4] M Alaeddini S Etemad-Moghadam and F Baghaii ldquoCompar-ative expression of calretinin in selected odontogenic tumours
a possible relationship to histogenesisrdquo Histopathology vol 52no 3 pp 299ndash304 2008
[5] S K Sundaragiri J Chawda S Gill S Odedra and G ParmarldquoCalretinin expression in unicystic ameloblastoma an aid indifferential diagnosisrdquo Journal of Oral Biosciences vol 52 no2 pp 164ndash169 2010
[6] G V Sherbet Calcium Signalling in Cancer Taylor amp FrancisBoca Raton Fla USA 2010
[7] A Lugli Y Forster P Haas et al ldquoCalretinin expression inhuman normal and neoplastic tissues a tissue microarrayanalysis on 5233 tissue samplesrdquo Human Pathology vol 34 no10 pp 994ndash1000 2003
[8] C Doglioni A P Dei Tos L Laurino et al ldquoCalretinin a novelimmunocytochemicalmarker formesotheliomardquoTheAmericanJournal of Surgical Pathology vol 20 no 9 pp 1037ndash1046 1996
[9] L Barnes J W Eveson P Reichart and D Sidransky EdsPathology amp Genetics Head and Neck Tumours IARC PressLyon France 2005
[10] R Rajendran and B Sivapathasundharam Shafers Oral Pathol-ogy Elsevier New York NY USA 2009
[11] D R Gnepp Diagnostic Surgical Pathology of the Head andNeck SaundersElsevier Philadelphia Pa USA 2009
[12] H Coleman M Altini H Ali C Doglioni G Favia and EMaiorano ldquoUse of calretinin in the differential diagnosis ofunicystic ameloblastomasrdquo Histopathology vol 38 no 4 pp312ndash317 2001
[13] A M Fernandes E C B Duarte F J G S Pimenta et alldquoOdontogenic tumors a study of 340 cases in a Brazilianpopulationrdquo Journal of Oral Pathology andMedicine vol 34 no10 pp 583ndash587 2005
[14] R C K Jordan and P M Speight ldquoCurrent concepts of odon-togenic tumoursrdquo Diagnostic Histopathology vol 15 no 6 pp303ndash310 2009
[15] P A Reichart P Reichart and H P Philipsen OdontogenicTumors and Allied Lesions Quintessence 2004
[16] M Shear and P Speight Cysts of the Oral and MaxillofacialRegions Wiley New York NY USA 2008
[17] B W Neville Oral and Maxillofacial Pathology WB SaundersPhiladelphia Pa USA 2002
[18] H P Philipsen and P A Reichart ldquoUnicystic ameloblastoma Areview of 193 cases from the literaturerdquo Oral Oncology vol 34no 5 pp 317ndash325 1998
[19] M Altini H Coleman C Doglioni G Favia and E MaioranoldquoCalretinin expression in ameloblastomasrdquoHistopathology vol37 no 1 pp 27ndash32 2000
[20] S DrsquoSilva M K Sumathi N Balaji et al ldquoEvaluation ofcalretinin expression in Ameloblastoma and non-neoplasticodontogenic cystsmdashan immunohistochemical studyrdquo Journal ofInternational Oral Health vol 5 no 6 pp 42ndash48 2013
[21] A Piattelli M Fioroni G Iezzi and C Rubini ldquoCalretininexpression in odontogenic cystsrdquo Journal of Endodontics vol 29no 6 pp 394ndash396 2003
[22] M J Hubbard N J McHugh and J E Mangum ldquoExclusionof all three calbindins from a calcium-ferry role in rat enamelcellsrdquo European Journal of Oral Sciences vol 119 no 1 pp 112ndash119 2011
[23] V Gotzos B Schwaller N HetzelM Bustos-Castillo andM RCelio ldquoExpression of the calcium binding protein calretinin inWiDr cells and its correlation to their cell cyclerdquo ExperimentalCell Research vol 202 no 2 pp 292ndash302 1992
Pathology Research International 7
[24] V Gotzos B Schwaller J-C Gander M Bustos-Castillo andM R Celio ldquoHeterogeneity of expression of the calcium-binding protein calretinin in human colonie cancer cell linesrdquoAnticancer Research vol 16 no 6B pp 3491ndash3498 1996
[25] J-C Gander V Gotzos B Fellay and B Schwaller ldquoInhibitionof the proliferative cycle and apoptotic events in WiDr cellsafter down-regulation of the calcium-binding protein calre-tinin using antisense oligodeoxynucleotidesrdquo Experimental CellResearch vol 225 no 2 pp 399ndash410 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Pathology Research International 5
and the ameloblast-like basal cells were positive in only 1 ofthe multicystic and 2 of the unicystic variants where singlecell expressing calretinin was observed
These findings were in accordance with earlier studieswhich also observed calretinin positive cells restricted to theneoplastic stellate reticulum like epithelium in ameloblas-toma only Altini et al [19] and Coleman et al [12] foundpositive staining in 815 cases of unicystic ameloblastomasand 935 cases of multicystic ameloblastoma while Dev-illiers et al [3] Sundaragiri et al [5] and DrsquoSilva et al[20] found positivity in all cases of ameloblastoma (100)In all these studies none of the odontogenic cystsrsquo liningshowed positivity except DrsquoSilva et al [20] who observedpositive staining of the cystic lining epithelium and keratinflakes in the cystic lumen of 40 cases of odontogenickeratocystThe authors attribute this finding to the aggressivebiologic behavior of odontogenic keratocyst similar to abenign neoplasm and its high mitotic activity as comparedto other nonneoplastic odontogenic cysts Also Piattelli et al[21] found positivity to calretinin in 8 of 12 parakeratinizedkeratocysts in the parabasal-intermediate layers of the cystepithelium This could point to the aggressive behavior ofKCOT and help to explain the differences in the clinical andpathologic behavior of odontogenic keratocysts in particularthe differences found between orthokeratinized keratocystsand parakeratinized keratocysts
Alaeddini et al [4] also found that calretinin immunore-activity was positive only for ameloblastoma when comparedto calcifying epithelial odontogenic tumour adenomatoidodontogenic tumour ameloblastic fibroma and odontogenicmyxoma stating that this protein may have a role in thetransition of the dental lamina remnants to ameloblastomaThey hypothesized that calretinin may be one of the factorsresponsible for the differences between this aggressive neo-plasm and other odontogenic tumors studied
Further in the present study the distribution pattern ofthe immunopositive cells was focal in 8 cases (40) anddiffuse in 4 cases (20) Also the staining was weak in mostof the cases (40) with 3 cases (15) showing moderate andonly 1 case (5) intense stainingThe staining was not equallydistributed throughout the sections with some areas showingintense staining but absolutely no staining in the immediatevicinity This was in contrast to the earlier studies wheremost of the cases showed intense staining of the ameloblasticepithelium [3ndash5 12 19 20]
Altini et al [19] stated that the better the differentiationof the epithelium was the lesser the expression of calretininoccurred in their study where they found little or noimmunostaining in those cases of unicystic ameloblastomasthat were lined by typical ameloblastic epithelium while theepithelium which completely lacked ameloblastic featuresfrequently expressed calretinin Hence they indicated thatcalretinin expression in some cells varied according to theirmetabolic activity andmay be lost when this activity changesLater Coleman et al [12] observed intense positive stainingin both areas of nondescript epithelial lining and areas withtypical ameloblastic features in unicystic ameloblastomawhich indicated that although the metaplastic cyst liningsmay have lost their typical ameloblastic features the cells have
retained their immunophenotypic characteristics resultingin the continued expression of calretinin Our study can becorrelated with the observation of Altini et al [19] as majorityof the unicystic ameloblastoma cases that we observed werelined by typical ameloblastic epithelium due to which theymay not have stained intensely with calretinin
In a study by Mistry et al [2] on developing rat molarscalretinin immunoreactivity was present in the inner enamelepithelium and presecretory ameloblasts from the late capstage onwards In the cap and late cap stages many ofthe specimens were immunopositive for calretinin in thestellate reticulum and this number increased to gt90 for theearly and late bell stages In the present study the patternof reactivity of the stellate reticulum observed appearedsimilar to the late bell stage of normal tooth developmentHowever in the peripheral layers of the ameloblastic islandscalretinin immunoreactivity was not observed as was the casein normal tooth germs As enamel organ has been proposedto be one of the possible origins of ameloblastoma [17] thispeculiar distribution of calretinin in ameloblastic epitheliumis noteworthy and it thus appears that there is no obviouscorrelation between the staining of normal odontogenictissues and their neoplastic counterparts [19]
A possible explanation for this dynamic spatial andtemporal distribution was that calretinin may be presentonly in cells that reside directly in the path of calciumin transition on its way to the enamel matrix acting as aldquocalcium ferryrdquo [2] However Hubbard et al [22] found thatcalretinin was primarily expressed during the differentiationstage of enamel formation and only a faint calretinin bandwas observed at secretion stage while no such band wasdetectable during maturation Based on these findings theauthors suggest retirement of the calcium ferry dogma fromenamel biologymdashin murine models at least
Gotzos et al [23 24] have shown increased expressionof calretinin in rapidly proliferating WiDr colon adenocar-cinomas cells Upon being induced to differentiate by treat-mentwith sodiumbutyrate and hexamethylene bisacetamidethey showed marked reductions in cell proliferation as wellas expression of full length calretinin When treated witholigonucleotides against calretinin synthesis these cells wereblocked in the G1 phase of the cell cycle and subsequentlyunderwent apoptosisThese authors suggested that calretininmay maintain an undifferentiated proliferative state charac-teristic of neoplastic transformation Also calretinin may actas an antiapoptotic factor [25]
The single case of KCOT in our study that showedpositivity to calretinin was of a 17-year-old male patienthaving radiolucency in 24 and 25 region with impacted 23The hematoxylin and eosin stained sections of the biopsyspecimen revealed a highly inflamed odontogenic keratocystwith one bit of tissue depicting stellate reticulummdashlikeepithelium overlying the palisaded basal cell layer Uponcalretinin staining uniform diffuse immunopositivity of thestellate reticulum like epitheliumwas observedThis suggeststhat the previous biopsy may have been misdiagnosed asKCOT on the basis of hematoxylin and eosin staining
This result can be compared with that of Devilliers et al[3] wherein they evaluated a tumor from their archives
6 Pathology Research International
originally diagnosed as KCOT which recurred 2 years laterHistologic sections from the tissue biopsied earlier (diag-nosed as KCOT) and from the tissue sample of the recurrence(diagnosed as ameloblastoma)were testedwith calretinin andboth showed positive staining of the neoplastic epitheliumconfined to the stellate reticulum
This finding helps us to understand the importance of cal-retinin as a differential diagnostic marker for ameloblastomaand how important it is for the pathologist to differentiateboth entities which carry different treatment protocols withpotentially serious functional and esthetic consequences forthe patient
Few nonepithelial cells that stained positive for calretininwere also observed in the connective tissue stroma of virtuallyall cases of ameloblastoma and KCOT in our study Altiniet al [19] and Coleman et al [12] also found such darklystained cells within the tumor or cyst epithelium and inthe fibrous connective tissue walls These were interpretedas being mast cells or Langerhans cells both of whichhave been documented as occurring in ameloblastomas andodontogenic cysts
5 Conclusion
The present study suggests that calretinin may be usedas a specific immunohistochemical marker for neoplasticameloblastic epithelium as calretinin positivity was observedexclusively in ameloblastomas Hence it can serve as animportant diagnostic adjunct in the differential diagnosisof ameloblastoma and keratocystic odontogenic tumor Theexpression of calretinin in these neoplastic lesions mightbe recapitulating dental ontogeny as its role during normaltooth development has also been speculated
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
Theauthors wish to thank all themembers in theDepartmentofOral andMaxillofacial Pathology for their general support
References
[1] C W Heizmann ldquoCalcium-binding proteins basic conceptsand clinical implicationsrdquo General Physiology and Biophysicsvol 11 no 5 pp 411ndash425 1992
[2] D Mistry M Altini H G Coleman H Ali and E MaioranoldquoThe spatial and temporal expression of calretinin in developingrat molars (Rattus norvegicus)rdquoArchives of Oral Biology vol 46no 10 pp 973ndash981 2001
[3] P Devilliers H Liu C Suggs et al ldquoCalretinin expression inthe differential diagnosis of human ameloblastoma and kera-tocystic odontogenic tumorrdquo The American Journal of SurgicalPathology vol 32 no 2 pp 256ndash260 2008
[4] M Alaeddini S Etemad-Moghadam and F Baghaii ldquoCompar-ative expression of calretinin in selected odontogenic tumours
a possible relationship to histogenesisrdquo Histopathology vol 52no 3 pp 299ndash304 2008
[5] S K Sundaragiri J Chawda S Gill S Odedra and G ParmarldquoCalretinin expression in unicystic ameloblastoma an aid indifferential diagnosisrdquo Journal of Oral Biosciences vol 52 no2 pp 164ndash169 2010
[6] G V Sherbet Calcium Signalling in Cancer Taylor amp FrancisBoca Raton Fla USA 2010
[7] A Lugli Y Forster P Haas et al ldquoCalretinin expression inhuman normal and neoplastic tissues a tissue microarrayanalysis on 5233 tissue samplesrdquo Human Pathology vol 34 no10 pp 994ndash1000 2003
[8] C Doglioni A P Dei Tos L Laurino et al ldquoCalretinin a novelimmunocytochemicalmarker formesotheliomardquoTheAmericanJournal of Surgical Pathology vol 20 no 9 pp 1037ndash1046 1996
[9] L Barnes J W Eveson P Reichart and D Sidransky EdsPathology amp Genetics Head and Neck Tumours IARC PressLyon France 2005
[10] R Rajendran and B Sivapathasundharam Shafers Oral Pathol-ogy Elsevier New York NY USA 2009
[11] D R Gnepp Diagnostic Surgical Pathology of the Head andNeck SaundersElsevier Philadelphia Pa USA 2009
[12] H Coleman M Altini H Ali C Doglioni G Favia and EMaiorano ldquoUse of calretinin in the differential diagnosis ofunicystic ameloblastomasrdquo Histopathology vol 38 no 4 pp312ndash317 2001
[13] A M Fernandes E C B Duarte F J G S Pimenta et alldquoOdontogenic tumors a study of 340 cases in a Brazilianpopulationrdquo Journal of Oral Pathology andMedicine vol 34 no10 pp 583ndash587 2005
[14] R C K Jordan and P M Speight ldquoCurrent concepts of odon-togenic tumoursrdquo Diagnostic Histopathology vol 15 no 6 pp303ndash310 2009
[15] P A Reichart P Reichart and H P Philipsen OdontogenicTumors and Allied Lesions Quintessence 2004
[16] M Shear and P Speight Cysts of the Oral and MaxillofacialRegions Wiley New York NY USA 2008
[17] B W Neville Oral and Maxillofacial Pathology WB SaundersPhiladelphia Pa USA 2002
[18] H P Philipsen and P A Reichart ldquoUnicystic ameloblastoma Areview of 193 cases from the literaturerdquo Oral Oncology vol 34no 5 pp 317ndash325 1998
[19] M Altini H Coleman C Doglioni G Favia and E MaioranoldquoCalretinin expression in ameloblastomasrdquoHistopathology vol37 no 1 pp 27ndash32 2000
[20] S DrsquoSilva M K Sumathi N Balaji et al ldquoEvaluation ofcalretinin expression in Ameloblastoma and non-neoplasticodontogenic cystsmdashan immunohistochemical studyrdquo Journal ofInternational Oral Health vol 5 no 6 pp 42ndash48 2013
[21] A Piattelli M Fioroni G Iezzi and C Rubini ldquoCalretininexpression in odontogenic cystsrdquo Journal of Endodontics vol 29no 6 pp 394ndash396 2003
[22] M J Hubbard N J McHugh and J E Mangum ldquoExclusionof all three calbindins from a calcium-ferry role in rat enamelcellsrdquo European Journal of Oral Sciences vol 119 no 1 pp 112ndash119 2011
[23] V Gotzos B Schwaller N HetzelM Bustos-Castillo andM RCelio ldquoExpression of the calcium binding protein calretinin inWiDr cells and its correlation to their cell cyclerdquo ExperimentalCell Research vol 202 no 2 pp 292ndash302 1992
Pathology Research International 7
[24] V Gotzos B Schwaller J-C Gander M Bustos-Castillo andM R Celio ldquoHeterogeneity of expression of the calcium-binding protein calretinin in human colonie cancer cell linesrdquoAnticancer Research vol 16 no 6B pp 3491ndash3498 1996
[25] J-C Gander V Gotzos B Fellay and B Schwaller ldquoInhibitionof the proliferative cycle and apoptotic events in WiDr cellsafter down-regulation of the calcium-binding protein calre-tinin using antisense oligodeoxynucleotidesrdquo Experimental CellResearch vol 225 no 2 pp 399ndash410 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 Pathology Research International
originally diagnosed as KCOT which recurred 2 years laterHistologic sections from the tissue biopsied earlier (diag-nosed as KCOT) and from the tissue sample of the recurrence(diagnosed as ameloblastoma)were testedwith calretinin andboth showed positive staining of the neoplastic epitheliumconfined to the stellate reticulum
This finding helps us to understand the importance of cal-retinin as a differential diagnostic marker for ameloblastomaand how important it is for the pathologist to differentiateboth entities which carry different treatment protocols withpotentially serious functional and esthetic consequences forthe patient
Few nonepithelial cells that stained positive for calretininwere also observed in the connective tissue stroma of virtuallyall cases of ameloblastoma and KCOT in our study Altiniet al [19] and Coleman et al [12] also found such darklystained cells within the tumor or cyst epithelium and inthe fibrous connective tissue walls These were interpretedas being mast cells or Langerhans cells both of whichhave been documented as occurring in ameloblastomas andodontogenic cysts
5 Conclusion
The present study suggests that calretinin may be usedas a specific immunohistochemical marker for neoplasticameloblastic epithelium as calretinin positivity was observedexclusively in ameloblastomas Hence it can serve as animportant diagnostic adjunct in the differential diagnosisof ameloblastoma and keratocystic odontogenic tumor Theexpression of calretinin in these neoplastic lesions mightbe recapitulating dental ontogeny as its role during normaltooth development has also been speculated
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgment
Theauthors wish to thank all themembers in theDepartmentofOral andMaxillofacial Pathology for their general support
References
[1] C W Heizmann ldquoCalcium-binding proteins basic conceptsand clinical implicationsrdquo General Physiology and Biophysicsvol 11 no 5 pp 411ndash425 1992
[2] D Mistry M Altini H G Coleman H Ali and E MaioranoldquoThe spatial and temporal expression of calretinin in developingrat molars (Rattus norvegicus)rdquoArchives of Oral Biology vol 46no 10 pp 973ndash981 2001
[3] P Devilliers H Liu C Suggs et al ldquoCalretinin expression inthe differential diagnosis of human ameloblastoma and kera-tocystic odontogenic tumorrdquo The American Journal of SurgicalPathology vol 32 no 2 pp 256ndash260 2008
[4] M Alaeddini S Etemad-Moghadam and F Baghaii ldquoCompar-ative expression of calretinin in selected odontogenic tumours
a possible relationship to histogenesisrdquo Histopathology vol 52no 3 pp 299ndash304 2008
[5] S K Sundaragiri J Chawda S Gill S Odedra and G ParmarldquoCalretinin expression in unicystic ameloblastoma an aid indifferential diagnosisrdquo Journal of Oral Biosciences vol 52 no2 pp 164ndash169 2010
[6] G V Sherbet Calcium Signalling in Cancer Taylor amp FrancisBoca Raton Fla USA 2010
[7] A Lugli Y Forster P Haas et al ldquoCalretinin expression inhuman normal and neoplastic tissues a tissue microarrayanalysis on 5233 tissue samplesrdquo Human Pathology vol 34 no10 pp 994ndash1000 2003
[8] C Doglioni A P Dei Tos L Laurino et al ldquoCalretinin a novelimmunocytochemicalmarker formesotheliomardquoTheAmericanJournal of Surgical Pathology vol 20 no 9 pp 1037ndash1046 1996
[9] L Barnes J W Eveson P Reichart and D Sidransky EdsPathology amp Genetics Head and Neck Tumours IARC PressLyon France 2005
[10] R Rajendran and B Sivapathasundharam Shafers Oral Pathol-ogy Elsevier New York NY USA 2009
[11] D R Gnepp Diagnostic Surgical Pathology of the Head andNeck SaundersElsevier Philadelphia Pa USA 2009
[12] H Coleman M Altini H Ali C Doglioni G Favia and EMaiorano ldquoUse of calretinin in the differential diagnosis ofunicystic ameloblastomasrdquo Histopathology vol 38 no 4 pp312ndash317 2001
[13] A M Fernandes E C B Duarte F J G S Pimenta et alldquoOdontogenic tumors a study of 340 cases in a Brazilianpopulationrdquo Journal of Oral Pathology andMedicine vol 34 no10 pp 583ndash587 2005
[14] R C K Jordan and P M Speight ldquoCurrent concepts of odon-togenic tumoursrdquo Diagnostic Histopathology vol 15 no 6 pp303ndash310 2009
[15] P A Reichart P Reichart and H P Philipsen OdontogenicTumors and Allied Lesions Quintessence 2004
[16] M Shear and P Speight Cysts of the Oral and MaxillofacialRegions Wiley New York NY USA 2008
[17] B W Neville Oral and Maxillofacial Pathology WB SaundersPhiladelphia Pa USA 2002
[18] H P Philipsen and P A Reichart ldquoUnicystic ameloblastoma Areview of 193 cases from the literaturerdquo Oral Oncology vol 34no 5 pp 317ndash325 1998
[19] M Altini H Coleman C Doglioni G Favia and E MaioranoldquoCalretinin expression in ameloblastomasrdquoHistopathology vol37 no 1 pp 27ndash32 2000
[20] S DrsquoSilva M K Sumathi N Balaji et al ldquoEvaluation ofcalretinin expression in Ameloblastoma and non-neoplasticodontogenic cystsmdashan immunohistochemical studyrdquo Journal ofInternational Oral Health vol 5 no 6 pp 42ndash48 2013
[21] A Piattelli M Fioroni G Iezzi and C Rubini ldquoCalretininexpression in odontogenic cystsrdquo Journal of Endodontics vol 29no 6 pp 394ndash396 2003
[22] M J Hubbard N J McHugh and J E Mangum ldquoExclusionof all three calbindins from a calcium-ferry role in rat enamelcellsrdquo European Journal of Oral Sciences vol 119 no 1 pp 112ndash119 2011
[23] V Gotzos B Schwaller N HetzelM Bustos-Castillo andM RCelio ldquoExpression of the calcium binding protein calretinin inWiDr cells and its correlation to their cell cyclerdquo ExperimentalCell Research vol 202 no 2 pp 292ndash302 1992
Pathology Research International 7
[24] V Gotzos B Schwaller J-C Gander M Bustos-Castillo andM R Celio ldquoHeterogeneity of expression of the calcium-binding protein calretinin in human colonie cancer cell linesrdquoAnticancer Research vol 16 no 6B pp 3491ndash3498 1996
[25] J-C Gander V Gotzos B Fellay and B Schwaller ldquoInhibitionof the proliferative cycle and apoptotic events in WiDr cellsafter down-regulation of the calcium-binding protein calre-tinin using antisense oligodeoxynucleotidesrdquo Experimental CellResearch vol 225 no 2 pp 399ndash410 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Pathology Research International 7
[24] V Gotzos B Schwaller J-C Gander M Bustos-Castillo andM R Celio ldquoHeterogeneity of expression of the calcium-binding protein calretinin in human colonie cancer cell linesrdquoAnticancer Research vol 16 no 6B pp 3491ndash3498 1996
[25] J-C Gander V Gotzos B Fellay and B Schwaller ldquoInhibitionof the proliferative cycle and apoptotic events in WiDr cellsafter down-regulation of the calcium-binding protein calre-tinin using antisense oligodeoxynucleotidesrdquo Experimental CellResearch vol 225 no 2 pp 399ndash410 1996
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom