Embed Size (px)
Citation preview

Hindawi Publishing CorporationEvidence-Based Complementary and Alternative MedicineVolume 2013, Article ID 827915, 7 pageshttp://dx.doi.org/10.1155/2013/827915
Research ArticleAn n-of-1 Trial Service in Clinical Practice:Testing the Effectiveness of Liuwei Dihuang Decoction forKidney-Yin Deficiency Syndrome
Huang Yuhong,1 Liu Qian,2 Liu Yu,1 Zhao Yingqiang,1 Li Yanfen,1 Yu Shujing,2
Qin Shufang,1 Sun Lanjun,1 Zou Shuxuan,1 and Wang Baohe1
1 Second Affiliated Hospital, Tianjin University of Traditional Chinese Medicine, Tianjin, China2 Tianjin University of Traditional Chinese Medicine, Tianjin, China
Correspondence should be addressed to Huang Yuhong; [email protected]
Received 11 June 2013; Revised 31 July 2013; Accepted 7 August 2013
Academic Editor: Guillermo Schmeda-Hirschmann
Copyright © 2013 Huang Yuhong et al.This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Objective. To describe the clinical use of n-of-1 RCTs for kidney-Yin deficiency syndrome that is a traditional Chinese medicinesyndrome in publicly clinical practice inChina.Methods. Our study included patients with kidney-Yin deficiency syndrome, using awithin-patient, randomized, double-blind, crossover comparison of Liuwei Dihuang decoction versus placebo.OutcomeMeasures.Primary outcome measures included number of individual completion rates, response rate, and post-n-of-1 RCTs decisions.Secondarymeasureswere thewhole group score of individual Likert scale, SF-36 questionnaire.Results. Fifty patients were recruitedand 3 were not completed. Forty-seven patients completed 3 pairs of periods, 3 (6.38%) were responders, 28 (59.57%) werenonresponders, and 16 (34.05%) were possible responders. Doctors and patients used the trial results to making decision. Threeresponders stayed on the medication management, 28 nonresponders ceased the LDD, 7 patients of the 16 possible responderscould not give clear decision, and the others kept the same medication station. Among the whole group, neither the individualLikert score nor the SF-36 showed any statistical differences between LDD and placebo. Discussion. More attention should be paidto choose experienced TCM doctor as investigator and keep the simulant same with test medication in n-of-1 RCTs of TCM andsufficiently biological half-life period of Chinese medicine compound.
1. Introduction
Liuwei Dihuang decoction (LDD) was first recorded in theKnack of Prescription in Pediatrics (xiao’er yaozheng zhijue) inAD1114 of the BeisongDynasty. Its author is Qian Yi, whowasfamous pediatrician and prescribed the LDD to dysplasia inchildren. From the Chinese medicine perspective, dysplasiain children is thought to be associated with a decline inkidney Yin. Hereafter, the LDD had been practiced in manydiseases except the dysplasia in children. Until the QingDynasty (AD1644–1911), in the comprehension of medicine(yixue xinwu) that records the practical and concise expe-rience of the famous doctor Zhongling Cheng, the LDDhad been reported to be practiced in less than 20 diseases,such as stroke, headache, urinary incontinence, lumbago, andasthma. From Beisong Dynasty to Qing Dynasty, the LDD
had been practiced not only in pediatrics but also in immune,endocrine, digestive, respiratory, urinary, and circulatorysystem diseases [1].
The Liuwei Dihuang decoction, a classic Chinese medic-inal formula, is a compound prescription comprising six in-gredients—Rehmanniae Radix Praeparata, Dioscoreae Rhi-zoma, Corni Fructus, Poria,Moutan Cortex, andAlisma Rhi-zoma. It has been reported that it effectively inhibits thedevelopment of benign prostatic hyperplasia [2]; decreasesproteinuria, protects kidney function, and ameliorates his-topathology [3]; alleviates 𝛽-amyloid-induced toxicity [4];lowers body weight and improves insulin and leptin sensi-tivity [5]; and so on. Based on gene and phenotype infor-mation associated with both LWDH (Liuwei Dihuang) herbsand LWDH-treated disease, LWDH-treated diseases showhigh phenotype similarity and identified certain “comodules”

2 Evidence-Based Complementary and Alternative Medicine
enriched in cancer pathways and neuroendocrine-immunepathways, which may be responsible for the action of treatingdifferent diseases by the same LWDH formula [6].
At present, in clinical practice, LDD has been used toimprove or restore declined functions related to aging andgeriatric disease such as impaired mobility, vision, hearing,cognition andmemory [4]. Its indication is deficiency of Kid-ney Yin including many diseases, how to establish evidenceto guide doctor and patient to administer LDD rationally isconsidered. The n-of-1 trials maybe are a promising method.Nikles et al. had developed n-of-1 trials into clinical tests forseveral conditions, designing them to assist clinicians to iden-tify whether a specific patient responds to a particular drugfor chronic stable conditions in which individual response totreatment is variable [7]. We performed n-of-1 randomizedcontrolled trials (n-of-1 RCTs) of LDP whose indication isdeficiency of kidney-Yin in order to guide the clinicians andpatients whether to take it continually.
2. Methods
2.1. Medicine Choose. There are many forms of the LDD onsale in China, such as honey bolus, water pill, liquid, and softcapsule. In this study, we choose the LDD soft capsule that isbest tomake simulant than other forms because of the specialflavor and color of Chinese herbs.
2.2.The Clinical n-of-1 Service. The trial was conducted in thesecond hospital affiliated to the Tianjin University of TCMin China from September 2009 to September 2011. Wesupplied request and consent forms to interested doctors.Doctors could explain the process to interested patients andobtained informed consent.The Kanion Pharmaceutical Co.,Ltd, standing in middle-east of china Jiangsu Province thatwas approved to produce LDD (soft capsule) in November2000 by state food and drug administration of china (SFDA)prepared the study medication and randomized it accordingto a computer-generated randomization schedule. Kits con-taining the correct sequence of randomized medicine wereposted to our hospital. A research pharmacist at the hospitalreceived the study medicines labeled with treatment identi-fication and distributed them to eligible participants sequen-tially according to the randomization schedule.
2.3. Patients. The trial protocol was approved by the ethicscommittees of the Second Affiliated Hospital of TianjinUniversity of Traditional ChineseMedicine in February 2009.Informed written consent was given before the trial beganand the participants were free to withdraw at any time duringthe study.
Participantswere eligible if they had a clinical diagnosis ofdeficiency of kidney Yin (Table 1) according to the same diag-nosis of two senior TCM clinicians who assessed separately,were aged 25 to 65 years, and had uncertainty about treatmenteffectiveness of LDP. The exclusion criteria were (1) majorneuropsychiatric disorder (schizophrenia, epilepsy, alcoholabuse, anorexia, and so forth); (2) planning to have a baby;(3) cardiocerebral vascular diseases, insufficiently controlled
Table 1: Diagnosis criteria of deficiency of kidney-Yin.
(1) Dizziness(2) Tinnitus(3) Flaccid waist and knees(4) Hectic fever(5) Dry mouth and throat(6) Night sweat(7) Spermatorrhea(8) Thirst and drink(9) Red tongue and less fur(10) Thready and rapid pulsePatients who have not less than 3 items above can be diagnosed as deficiencyof kidney-Yin.
Placebo Placebo LDDLDDLDD Placebo
Participants with deficiency of kidney Yin
Eligible participants and informed consent
First Second ThirdWeeks 1–4 Weeks 5–8 Weeks 9–12 Weeks 13–16 Weeks 17–20 Weeks 21–24
Record symptoms using Likert scale and life quantity using SF-36
Diary analysis, report production and post-trial
Management follow-up at 6 months after the n-of-1 trial
Figure 1: Flowchart for the n-of-1 trial. In this example, “weeks 1–4”is a treatment period. Weeks 1–4 and weeks 5–8, combined, are thefirst pair of treatment periods. The whole n-of-1 trial consists of the3 pairs of treatment periods.
hypertension or hypotension, thromboembolic diseases, gas-trointestinal diseases affecting drug absorption, hematopoi-etic system diseases, or autoimmune system diseases; (4)abnormal liver function or abnormal renal function; (5) oth-ers that the investigator assessed not suitable to take part instudy. Participants came from the Second Affiliated Hospitalof Tianjin University of Traditional Chinese Medicine.
2.4. Randomization. The individual studies ran for 24 weeks.Patients undertook 3 pairs of 8-week treatment periods(each period consisting of 4-week LDD and 4-week placeboin random order). Each pair contained the LDD and theplacebo, two treatment periods (Figure 1). Both the patientsand doctors interacting with them and the research assistantwere all blind to when patients were taking the LDD or theplacebo.
2.5. Data Collection. Patients completed diaries containingten clinical kidney-Yin deficiency syndromes rated by theLikert scale (strongly agree 5, agree 4, neither agree, or dis-agree 3, disagree 2, strongly disagree 1) during and at the end

Evidence-Based Complementary and Alternative Medicine 3
of each treatment period, which was used to assess the degreeof kidney-Yin deficiency before and after treatment. Itemsof the Likert scale of Kidney-Yin deficiency syndrome wereselected from TCM teaching material issued by Chinesegovernment and were discussed by 5 senior TCM clinicaldoctors before validity and reliability tests. The validity andreliability of the Likert scale was tested in a small amount ofpeople (15 patients with kidney-Yin deficiency and 20 cases ofhealthy college students) before research. The survey resultsshow that it has good discriminant validity.
Patients also completed the SF-36 (the MOS item shortfrom health survey, SF-36) at the end of each treatmentperiod, which were used to measure perceived health andquality of life.
We collected information about medication history,demographic variables, and treatment decision immediatelyafter the n-of-1 trial.
2.6. Data Analysis. An n-of-1 RCT was considered “respon-der” if Likert scale score and SF-36 score were both morefavorable response to LDD treatment (in all 3 treatmentpairs), “possible responder” (in 2 of 3 treatment pairs), or“nonresponder.”
To address the effect of LDD on the entire group, weconducted repeated-measures analysis of variance, exam-ining the effects of treatment, pair, and the treatment-pair interaction. Besides, we pooled the standardized meandifferences from every patient who completed the trial byusing meta-analysis, comparing the effect of LDD with thatof placebo.
All statistical analyses, except for the meta-analysis, wereperformed using SPSS 13.0. The meta-analysis was calculatedusing RevMan5.0. All descriptive data are expressed asmeansand standard deviations. All estimates are expressed as meandifferences and 95% CI unless otherwise stated.
3. Results
3.1. Patients. Six doctors in the Second Affiliated Hospitalof the Tianjin University of Traditional Chinese Medicineparticipated in this study. Fifty patients who met trial entrycriteria were recruited, and 47 people completed the trial.The reasons for the three withdrawals were that 1 because ofright oophorectomy, 1 because of leg injury, and 1 because ofnoeffectiveness. Table 2 presents the characteristics of the 47patients who completed the study.
3.2. Individual n-of-1 RCTs. Three patientsmet the criteria fora responder, 16 patients met the criteria for a possible respon-der, 28 patients were non-responders, and no patients metcriteria for responder to placebo. Figure 2 presents details ofone clear responder.
The n-of-1 trial had a marked effect on management.Medication immediately after trial changed for 29 (65.91%)of 47 of those completing the trial: of 41 patients who hadtaken the LDD, 26 patients ceased it, 8 patients kept thesame medication station, and 7 patients could not give clear
Table 2: Patient characteristics.
CharacteristicsAge, yr 48.76 ± 2.01
Females/males, 𝑛 35/15Married/unmarried, 𝑛 49/1Taken the LDD previously, 𝑛 41Baseline individual Likert score 15.23 ± 3.91
Baseline SF-36 score 118.44 ± 13.58
Values are absolute numbers or mean ± SD.
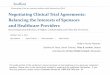
0
5
10
15
20
25
30
Month 1 Month 2 Month 3 Month 4 Month 5 Month 6
Likert score
(a)
0100200300400500600700800
SF-36
PL LDDPLPLMonth 1 Month 2 Month 3 Month 4 Month 5 Month 6
LDDLDD
(b)
Figure 2: Example of a responder to LDD. The responder’s Likertscore and SF-36 show clear differences between months 1, 3, and 5(placebo) and months 2, 4, and 6 (LDD). Higher scores of Likertscore indicate worse behavior. Higher scores of SF-36 indicate betterbehavior.
decision. Of 6 patients who had not taken the LDD, 3 patientsbegan to take it, 2 had no plan to take it, and 1 could not giveclear decision.
It is necessary to put the post-n-of-1 trial managementdecisions into context. Doctors and patients used the trialresults for making decision. Three responders stayed on themedication management, 28 non-responders ceased theLDD, 7 patients of the 16 possible responders could notgive clear decision, and the others kept the same medicationstation (Table 3).
3.3. Group n-of-1 RCTs. Results from repeated-measuresanalysis show individual Likert score improved over time, butno significant differences between LDD and placebo group

4 Evidence-Based Complementary and Alternative Medicine
Table 3: Management changes immediately post-n-of-1 trial.
Taking LDD No taking LDD Unclear decision TotalPatients had taken LDP or not, 𝑛 (%)
Yes 8 (19.51) 26 (63.42) 7 (17.07) 41 (100)No 3 (50.00) 2 (33.33) 1 (16.67) 6 (100)Total 11 (23.40) 28 (59.58) 8 (17.02) 47 (100)
The n-of-1 trials, 𝑛 (%)Responders 3 (100.00) 0 (0.00) 0 (0.00) 3 (100)Possible responders 9 (56.25) 0 (0.00) 7 (43.75) 16 (100)Nonresponders 0 (0.00) 28 (100.00) 0 (0.00) 28 (100)Total 12 (25.53) 28 (59.57) 7 (14.90) 47 (100)
Table 4: Repeated measure of individual Likert score.
Source Sum of squares df Mean square 𝐹 𝑃
Group 5.121 1 5.121 0.267 0.607Pair 329.199 2 164.599 30.478 0.000Group ∗ pair 2.433 2 1.216 0.225 0.789Error (group) 1766.681 92 19.203Error (pair) 993.702 184 5.401Test statistics of Mauchly’s test of sphericity:𝑊 = 0.954, 𝑃 = 0.117. Individual Likert score improved significantly in different pair. No significant differencesbetween LDD and placebo. No interaction between group and pair.
(Table 4). Although there was an improvement over time forevery SF-36 domain (𝑃 < 0.05), except for SF-36 physiologyand SF-36 emotion, these effects were unrelated to LDDbeingused, nor any interaction between treatment and pair for anyof the SF-36 domain (Table 5).
Patients show same level of individual Likert scorebetween LDD and placebo in meta-analysis. The standard-ized mean difference in the Likert score between LDD andplacebo was −0.09 (95% CI −0.36 to 0.17), using a weightedmean difference technique. Because of no heterogeneity inresults across the patients (test for heterogeneity, 𝑃 = 0.07),fixed model was used (Figure 3). Similarly, patients show nodifference of SF-36 total score between LDD and placebo.Overall, the standardized mean difference SF-36 total scorebetween LDD and placebo was 2.41 (95% CI −0.95 to5.76), using a weighted mean difference technique. Becauseof no heterogeneity in results across the patients (test forheterogeneity, 𝑃 = 0.76), fixed model was used (Figure 4).
Adverse effects were not found between LDD andplacebo.
4. Discussion
4.1. Research Background. Traditional Chinese medicine(TCM) whose basic principle of treatment is the syndromedifferentiation-based treatment emphasizes the individual-ized medicine.The n-of-1 trial may be a good means to guideclinical practitioner and patient to manage the TCM. LDD isone of the most classical formulas, which is OTC medicinein China, and is consumed numerously every year. Abuse ofLDD also may cause some side effects such as indigestionand loose stool [1]. The n-of-1 trial is an effective means todecrease the abuse of LDD. Our study is a good example.
4.2. Summary of Main Findings. The n-of-1 design is anattractive technique to define efficacy on an individual basis.In our study, the n-of-1 trial identified 3 patients for whomLDD was clearly beneficial, 16 who showed nonsignificantbenefit and 28 who showed no benefit. Despite its weakextrapolation, we compare the difference between LDD andplacebo. Group results showed no apparent effect of LDD onindividual Likert score or any of eight domains of the SF-36.
4.3. Strengths andWeaknesses of the Study. Then-of-1 clinicaltrial can leverage study design and statistical techniquesassociated with standard population-based clinical trials,including randomization, washout and crossover periods,and placebo controls.
Many Chinese are confident with the TCM and desired tochoose TCM for treatment of chronic diseases or health care,so in our study, the patient compliance is good. A limitationof the trial was washout period which has not been fullyconsidered. Because it is difficult to know biological half-lifeperiod of Chinese medicine compounds, we speculate that2 days of biological half-life period in our study may notbe enough, which resulted in residual effects of traditionalChinese medicine interfered the differences between LDDand placebo. It in part explains why LDD showed non-significant benefit compared with placebo in our study.
4.4. Relationship of Our Study to the Existing Literature.While not observed in our study, the documented adverseeffects of LDP are reported in other articles, such as diarrheaand inappetence [1]. Although to date, no serious adversereactions have been reported about LDD, it is still necessaryto pay attention to the abuse of LDD.

Evidence-Based Complementary and Alternative Medicine 5
Study or subgroup
NO1NO10NO12NO13NO15NO16NO17NO18NO19NO2NO20NO21NO22NO23NO24NO25NO26NO27NO28NO3NO30NO31NO32NO33NO34NO35NO36NO37NO38NO39NO4NO40NO41NO42NO43NO44NO45NO46NO47NO48NO49NO5NO50NO6NO7NO8NO9
Total (95% CI)
Mean
15.3325
21.3319.33
2221.33
023.67
24252519
23.6719.3324.33
025
22.6720.33
024.3320.3317.67
2122.6722.6725.33
1921.33
2321
23.3318.6718.67
240
2122
23.3323
19.331822
16.6716.6725.3320.67
SD
1.152.644.161.15
21.52
01.15
03.461.735.192.08
2.31.15
02.641.154.04
05.031.151.522.641.151.151.151.733.511.734.583.051.151.52
20
1.732
3.051.731.154.58
24.046.354.041.15
Total
33333333333333333333333333333333333333333333333
129
Mean
19.6722.6722.6720.6720.3321.6724.6724.67
2523.33
024.3324.6719.33
2423.3323.33
2422.33
023.6720.3317.3318.3323.3324.6724.6718.67
2122.6724.6723.3318.6720.33
2423.33
2122.6722.67
2321.33
1823.33
1520.3323.6719.33
SD
0.573.054.161.152.082.081.150.57
10.57
03.211.151.152.641.153.051.734.04
04.161.151.150.57
2.32.3
1.151.15
3.61.15
5.53.051.15
2.32
3.051.73
2.33.05
3.62.3
4.583.051.736.654.611.15
Total
33333333333333333333333333333333333333333333333
129
Weight
9.1%0.9%0.4%5.7%1.8%2.3%
9.1%
1.2%
0.4%2.7%2.3%1.8%
0.9%3.5%0.5%
0.4%5.7%4.1%2.1%2.3%2.3%5.7%3.5%0.6%3.5%0.3%0.8%5.7%2.0%1.9%
2.5%1.6%0.8%0.9%2.3%0.4%1.1%0.8%0.2%0.4%5.7%
100.0%
IV, fixed, 95% CI
−4.34 [−5.79, −2.89]2.33 [−2.23, 6.89]
−1.34 [−8.00, 5.32]−1.34 [−3.18, 0.50]
1.67 [−1.60, 4.94]−0.34 [−3.26, 2.58]
Not estimable−1.00 [−2.45, 0.45]
Not estimable1.67 [−2.30, 5.64]
Not estimable−5.33 [−12.24, 1.58]−1.00 [−3.69, 1.69]
0.00 [−2.91, 2.91]0.33 [−2.93, 3.59]
Not estimable1.67 [−2.89, 6.23]
−1.33 [−3.68, 1.02]−2.00 [−8.47, 4.47]
Not estimable0.66 [−6.73, 8.05]0.00 [−1.84, 1.84]0.34 [−1.82, 2.50]2.67 [−0.39, 5.73]
−0.66 [−3.57, 2.25]−2.00 [−4.91, 0.91]
0.66 [−1.18, 2.50]0.33 [−2.02, 2.68]0.33 [−5.36, 6.02]0.33 [−2.02, 2.68]
−3.67 [−11.77, 4.43]0.00 [−4.88, 4.88]0.00 [−1.84, 1.84]
−1.66 [−4.78, 1.46]0.00 [−3.20, 3.20]
Not estimable0.00 [−2.77, 2.77]
−0.67 [−4.12, 2.78]0.66 [−4.22, 5.54]0.00 [−4.52, 4.52]
−2.00 [−4.91, 0.91]0.00 [−7.33, 7.33]
−1.33 [−5.46, 2.80]1.67 [−3.30, 6.64]
−3.66 [−14.06, 6.74]1.66 [−5.28, 8.60]1.34 [−0.50, 3.18]
LDD Placebo Mean difference Mean differenceIV, fixed, 95% CI
−10 −5 0 5 10Favours experimental Favours control
−0.53 [− 0.97, − 0.10]
Test for overall effect: Z = 2.39 (P = 0.02)Heterogeneity: 53.53, df = 40 (P = 0.07); I2 = 25%𝜒2 =
Figure 3: Meta-analysis of individual Likert score between LDD and placebo.
The fundamentality of TCM is syndrome differentiationand treatment. In our study, all the patients were includedbased on syndrome differentiation and had a clinical diag-nosis of deficiency of Kidney Yin. According to the theory oftraditional Chinesemedicine, which deems that sideeffects ofChinese medicine will not appear as long as syndrome differ-entiation is accurate, we guess that syndrome differentiation
in our study is accurate. That could explain why the drug’sside effects are not found in our study.
The n-of-1 or single subject clinical trial considers anindividual patient as the sole unit of observation in a studyinvestigating the efficacy or side-effect of different interven-tions. The ultimate goal of an n-of-1 trial is to determine theoptimal or best intervention for an individual patient using

6 Evidence-Based Complementary and Alternative Medicine
Study or subgroup
NO1NO10NO12NO13NO15NO16NO17NO18NO19NO2NO20NO21NO22NO23NO24NO25NO26NO27NO28NO3NO30NO31NO32NO33NO34NO35NO36NO37NO38NO39NO4NO40NO41NO42NO43NO44NO45NO46NO47NO48NO49NO5NO50NO6NO7NO8NO9
Total (95% CI)
Mean
789.89555.61693.11765.89
645427.17696.33724.67426.17707.67
633631.06
727736.56692.33673.78
691554.5
740718.33
709743740
733.78631.61452.44
733647.67731.67553.17712.83554.67649.33671.33749.33587.78535.89648.44668.83703.33473.17
775509.67
741791.33727.89493.28
SD
151.8655.3848.2331.9478.0812.4114.18
9.2935.55
880.8139.5292.89
935.7618.58
50.858.19
213.799.5333.59.52
15.095
23.7642.0117.92
5.2916.4411.7118.07
85.337.5444.7610.01
2.8884.1721.8146.0375.49
4.6160.54.58
41.05355.52
14.1818.4757.92
Total
33333333333333333333333333333333333333333333333
Mean
691.72646.56681.56753.67
686472.94680.67720.22427.17710.67
665572.33602.17743.67
697682.67
699587.06
722700.22
700739.33741.67
0583.44446.06725.33632.67727.33554.17706.17
588663.67635.33747.67691.67505.44662.67691.83705.67
370770.33
516771.67779.33744.32572.28
SD
230.335.4364.1234.4444.0356.1554.01
25.572.5
612.48.32
99.02126.95
9.4522.8618.1435.79154.323.0628.93
2.752.882.88
0106.18
72.224.16
35.9215.94
6.0463.1145.1710.9630.74
6.6554.8554.6448.1455.3213.79
102.4319.0837.2412.0923.1814.84
115.39
Total
33333333333333333333333033333333333333333333333
Weight
0.0%0.2%0.1%0.4%0.1%0.3%0.3%1.2%0.1%0.0%0.5%0.0%0.1%0.6%1.0%0.3%0.2%0.0%1.4%0.4%9.0%3.7%
26.4%
0.1%0.2%
19.4%0.6%2.2%2.4%0.1%0.3%0.4%0.8%
16.8%0.1%0.3%0.2%0.1%4.2%0.1%2.3%0.3%0.0%1.2%1.6%0.1%
IV, fixed, 95% CI
98.17 [−213.99, 410.33]−90.95 [−165.34, −16.56]
11.55 [−79.24, 102.34]12.22 [−40.93, 65.37]
−41.00 [−142.43, 60.43]−45.77 [−110.84, 19.30]
15.66 [−47.53, 78.85]4.45 [−26.26, 35.16]
−1.00 [−92.37, 90.37]−3.00 [−1216.94, 1210.94]
−32.00 [−77.70, 13.70]58.73 [−94.91, 212.37]
124.83 [−19.19, 268.85]−7.11 [−48.96, 34.74]−4.67 [−38.00, 28.66]−8.89 [−69.93, 52.15]−8.00 [−85.30, 69.30]
−32.56 [−330.91, 265.79]18.00 [−10.23, 46.23]18.11 [−31.98, 68.20]
9.00 [−2.21, 20.21]3.67 [−13.71, 21.05]−1.67 [−8.20, 4.86]
Not estimable48.17 [−81.04, 177.38]
6.38 [−77.82, 90.58]7.67 [0.05, 15.29]
15.00 [−29.70, 59.70]4.34 [−18.04, 26.72]
−1.00 [−22.56, 20.56]6.66 [−113.41, 126.73]−33.33 [−99.79, 33.13]−14.34 [−66.49, 37.81]
36.00 [−0.58, 72.58]1.66 [−6.54, 9.86]
−103.89 [−217.57, 9.79]30.45 [−36.12, 97.02]
−14.23 [−89.60, 61.14]−23.00 [−128.90, 82.90]−2.34 [−18.79, 14.11]
103.17 [−31.45, 237.79]4.67 [−17.53, 26.87]
−6.33 [−69.05, 56.39]−30.67 [−433.20, 371.86]
12.00 [−18.75, 42.75]−16.43 [−43.24, 10.38]−79.00 [−225.10, 67.10]
LDD Placebo Mean difference Mean differenceIV, fixed, 95% CI
−100 −50 0 50 100Favours experimental Favours control
141 138 100.0% 2.41 [− 0.95, 5.76]
Test for overall effect: Z = 1.41 (P = 0.16)Heterogeneity: 38.13, df = 45 (P = 0.76); I2 = 0%𝜒2 =
Figure 4: Meta-analysis of SF-36 total score between LDD and placebo.
Table 5: Repeated measure of SF-36 total score.
Source Sum of squares df Mean square 𝐹 𝑃
Group 10.150 1 10.150 0.000 0.985Pair 60248.979 1.775 33936.371 10.660 0.000Group ∗ pair 3261.686 1.775 1837.206 0.577 0.543Error (group) 2668184.506 92 29002.005Error (pair) 519956.205 163.332 3183.425Test statistics of Mauchly’s test of sphericity:𝑊 = 0.873, 𝑃 = 0.002. Greenhouse-Geisser was used to adjust df. SF-36 total score improved significantly atdifferent pair. No significant differences between LDD and placebo. No interaction between group and pair.

Evidence-Based Complementary and Alternative Medicine 7
objective data-driven criteria. So, extrapolation of n-of-1clinical trial will be weak. Unlike previously reported studies[8] which were used to treat diabetes when combined withantidiabetic and applied blood sugar as therapeutic effectindex, our study used kidney-Yin deficiency syndrome andhealth-scale and the group results showed no trend in favorof LDD being of benefit.
4.5. Implications from the Study. Despite obvious appeal andwide use in educational settings of n-of-1 trial, it has beenused sparingly inmedical and general clinical settings [9].Wecan only speculate why. Perhaps we only slightly penetrateddoctors’ awareness; the process requires considerable inputfrom doctors [7]. We briefly reviewed the literatures andfound only one n-of-1 clinical trials report about botanicalthat is the spirulina to treat chronic fatigue in four n-of-1randomized controlled trials [10].
Traditional Chinese medicine holds a large market inChina. Many people seek health care treatment using tradi-tional Chinese medicine. Some TCM compound prescrip-tions benefit some symptoms such as cough and frequenturination. The primary purpose of this study is to restrictthe abuse of Chinese patent drugs, but due to the charac-teristics of differentiation-based treatment in TCM, it is notappropriate to evaluate these compound prescription effectsin population-based clinical trials that may not be resolvethe question of clinical equipoise in these clinical settingsbecause these symptoms exist in many diseases. It has beensuggested that themain role of n-of-1 trials in clinical practiceis to cancel useless treatment rather than advocate drugtreatment [11]. The n-of-1 trial may be a promising approachthat essentially starts out small and focused and then worksits way towards insights that would prevent unnecessary useof Chinese patent drugs.
In summary, this study does not support the generalapplication of LDD for patients with deficiency of kidney Yin.Our data also suggest that more attention should be paid tochoose experienced TCM doctor as investigator and keep thesimulant samewith testmedication in n-of-1 trial of TCMandsufficiently biological half-life period of Chinese medicinecompound.
Conflict of Interests
All the authors declare that they have no competing financialinterests.
Acknowledgment
This study was supported by Young Scientist Research Foun-dation of the National Natural Science Foundation of China(30801465).
References
[1] L. Yang, J. Sun, and L. Han, “Clinical application and studyon Liuwei Dihuang pill composition,” Journal of ZhejiangUniversity of TCM, vol. 34, pp. 796–798, 2010.
[2] I. S. Shin, M. Y. Lee, H. K. Ha, C. S. Seo, and H. K. Shin,“Inhibitory effect of Yukmijihwang-Tang, a traditional herbalformula against testosterone-induced benign prostatic hyper-plasia in rats,” Complementary and Alternative Medicine, vol. 12,article 48, 2012.
[3] H. Chen, Q. Zhu, X. Tang, M. Min, L. Jie, and L. Chen, “Effectof Shen-Qi-Di-Huang decoction on reducing proteinuria bypreserving nephrin in adriamycin-induced nephropathy rats,”African Journal of Traditional, Complementary and AlternativeMedicines, vol. 8, no. 4, pp. 467–476, 2011.
[4] J. S. Sangha, X. Sun, O. S. D. Wally et al., “Liuwei Dihuang(LWDH), a traditional Chinese medicinal formula, protectsagainst 𝛽-amyloid toxicity in transgenic Caenorhabditis ele-gans,” PloS ONE, vol. 7, no. 8, Article ID e43990, 2012.
[5] B. Perry, J. Zhang, C. Sun, T. Saleh, and Y. Wang, “LiuweiDihuang lowers body weight and improves insulin and leptinsensitivity in obese rats,” Evidence-Based Complementary andAlternative Medicine, vol. 2012, Article ID 847167, 8 pages, 2012.
[6] S. Li, B. Zhang, D. Jiang, Y. Wei, and N. Zhang, “Herbnetwork construction and co-module analysis for uncoveringthe combination rule of traditional Chinese herbal formulae,”BMC Bioinformatics, vol. 11, no. 11, article S6, 2010.
[7] C. J. Nikles, G. K. Mitchell, C. B. Del Mar, A. Clavarino, and N.McNairn, “An n-of-1 trial service in clinical practice: testing theeffectiveness of stimulants for attention-deficit/hyperactivitydisorder,” Pediatrics, vol. 117, no. 6, pp. 2040–2046, 2006.
[8] L. Ning, Q. Luguang, and W. Haisong, “Clinical observation ofLiuwei Dihuang pill treatment of type 2 diabetes,” Journal ofChengdu University of TCM, vol. 23, no. 4, pp. 46–47, 2000.
[9] E. O. Lillie, B. Patay, J. Diamant, B. Issell, E. J. Topol, and N.J. Schork, “The n-of-1 clinical trial: the ultimate strategy forindividualizing medicine?” Personalized Medicine, vol. 8, no. 2,pp. 161–173, 2011.
[10] C. Baicus and A. Baicus, “Spirulina did not ameliorate idio-pathic chronic fatigue in four N-of-1 randomized controlledtrials,” Phytotherapy Research, vol. 21, no. 6, pp. 570–573, 2007.
[11] T. Johannessen, “Controlled trials in single subjects: 1. Valuein clinical medicine,” The British Medical Journal, vol. 303, no.6795, pp. 173–174, 1991.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com