Embed Size (px)
Citation preview

Early Warning and Disease Surveillance System
1
Republic of South Sudan
EARLY WARNING AND DISEASE SURVEILLANCE BULLETIN (IDP CAMPS AND SETTLEMENTS)
Week 37 7 - 13 September 2015
General Overview
Completeness for weekly reporting in week 37 of 2015 was 84%, which is higher when compared to 83% in week 36 of 2015 and 58% in week 37 of 2014.
In week 37 of 2015, malaria was the top cause of morbidity among IDPs and registered a proportionate morbidity of 43.4% as compared to 41.2% in week 36 of 2015. The malaria incidence in week 37 of 2015 was highest in Bentiu PoC followed by Renk, Bor, Malakal PoC, Melut, and UN House PoC and consistent with a malaria upsurge that has reached epidemic proportions.
In week 37 of 2015, 10 new measles cases have been reported from Bentiu PoC and one from Renk. Since the beginning of 2015, Bentiu has reported 433 measles cases including 13 deaths (CFR 3%). An integrated measles and polio vaccination campaign was conducted in Bentiu PoC reaching 84.8% (43,931) children aged six months to 15 years. Plans for reactive measles vaccination are underway in response to the measles outbreak in Renk.
Cholera cases have risen to 1,743 including 46 deaths [CFR 2.64%] in Juba and Bor Counties. Following a coordinated and comprehensive response, a declining trend has been registered. Evaluation of the cholera response is underway. The findings will be used to update preparedness and contingency planning.
In week 37 of 2015, 144 new cases of HEV have been reported from Bentiu PoC and one from Lankien. The total HEV is 1,342 cases including 13 deaths (CFR 0.97%) in Bentiu; 153 cases including seven deaths (CFR 4.6%) in Mingkaman; and 35 HEV cases including one death (CFR 2.9%) in Lankien.
In week 36 of 2015, a Global Acute Malnutrition Rate (GAM) of 20.8% and Severe Acute Malnutrition (SAM) rate of 4.9% were registered in Bentiu with both rates exceeding the emergency threshold of 15% and 2% respectively.
In week 37 of 2015, the under-5 mortality rate for Bentiu PoC is 1.760 deaths per 10,000 per day, which is below the U5MR emergency threshold of 2 deaths per 10,000 per day. The notable causes of death in children under five years in Bentiu during week 37 of 2015 included malaria, perinatal complications, and pneumonia.
Editorial not This bulletin presents disease trends from data submitted through the Early Warning Alert and Disease Network (EWARN) by health partners providing health services to internally displaced persons in South Sudan. Additional integrated disease surveillance and response (IDSR) data is also presented for select diseases like cholera, Kala-azar and AFP. All other IDSR weekly reports are published through IDSR weekly bulletin of the EPR department in the MoH-RSS.
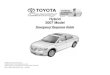
Completeness and Timeliness of Reporting Figure 1 shows the completeness for weekly reporting from week 01 of 2014 to week 37 of 2015. During week 37 of 2015, weekly disease surveillance reports were expected from 63 health facilities. In week 37 of 2015, timeliness for weekly reporting is 35 (56%) as compared to 36 (57%) in week 36 of 2015 and
18/48 (38%) in week 37 of 2014.
Figure 1
0
20
40
60
80
100
120
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Co
mp
lete
nes
s [%
]
Reporting Completeness for IDP Health Facilities, 2014 - 2015
2014
2015
Target

Early Warning and Disease Surveillance System
2
In week 37 of 2015, completeness for weekly reporting is 53 (84%) as compared to 52 (83%) in week 36 of 2015 and 28/48 (58%) in week 37 of 2014. This week 10 facilities have not their reports (Table 1).
Table 1: No. Health Facility Partner
1 HLSS Mingkaman PHCC site 2 HLSS
2 HLSS Site 1 Hospital HLSS
3 Malual PHCU IRC
4 Janglow PHCU IRC
5 Machar PHCU IRC
6 Kol PHCU IRC
7 Jiech PHCU COSV
8 Yuai MSF-OCA
9 Ruath PHCU CARE
10 Melut MSF-E
Consultations (All patients seen at Outpatient and Inpatient facilities)
In week 37 of 2015, the total consultations is 34,333 as compared to 32,430 in week 36 of 2015 and 12,065 in week 37 of 2014 (Figure 2). The cumulative consultations since week 01 of 2015 have risen to 707,756 (Figure 2.1)
The annualised outpatients department (OPD) utilization for 2015 is 1.2 consultations per person per year (Figure 2.2). The IDP site-specific annualised OPD utilization rates are shown in Figure 2.2.
Figure 2
Figure 2.1
Figure 2.2
387
620
20341975 883
36131551
4379
520
5214
912 353 3723
299
2215
0 0
166
2357 442 141 177 216
275 146
332 378235
790
0%10%20%30%40%50%60%70%80%90%
100%
Aw
eria
l
Ben
tiu
Bo
r
Lan
kie
n
Mal
akal
Mel
ut
Nas
ir
UN
HO
USE
Ren
k
Ko
do
k
Lu
l
Ogo
d
Ak
ob
o
Wau
Sh
illu
k
Tw
ic E
ast
DU
K
Pan
yij
iar
May
om
Lee
r
May
end
it
Nu
mb
er
of
con
sult
ati
on
s
Consultations by IDP site and implementing Partner, week 37 2015
CCM IMC IOM IRC MSF-E MSF-OCA CARE Medair HealthLink GOAL IMA SMC UNKEA World Relief
75
207
1033
86
037
2
55
12 0 9
80
11 5 9 18 12 8 2 10 0 1 3 171 20
50
100
150
200
250
Nu
mb
er
of
con
sult
ati
on
s
Th
ou
san
ds
Cumulative Consultations by IDP Site from week 01 of 2015 to week 37 of 2015
1.5 2.8
5.6
1.9 2.6
1.0 3.2
0.3 2.7
6.5
1.7 1.2
8.1
2.0 0.7
5.6
0.5 0.4 0.6 0.1 0.4 0.0 0.1 0.1 0.3 0.0 0.9 1.2 -
1.0
2.0
3.0
4.0
5.0
6.0
Aw
eria
l
Ben
tiu
Bo
r
Lan
kie
n
Mal
akal
Man-…
Mel
ut
Nas
ir
UN…
Yu
ai
Man-…
Ak
ok
a
Ren
k
Ko
do
k
Lu
l
Ogo
d
Ak
ob
o
Wau…
Tw
ic E
ast
Ny
iro
l
DU
K
Ayo
d
Man
yo
Pan
yiji
ar
May
om
Lee
r
May
end
it
Ove
rall
con
sult
atin
s p
er p
erso
n p
er
yea
r
Consultations per person per year, week 37, 2015

Early Warning and Disease Surveillance System
3
Overall Trends of Priority Epidemic-prone Diseases
Table 2 shows the top five causes of morbidity among IDPs with malaria being at the top, followed by Acute Respiratory tract Infections (ARI), Acute Watery Diarrhoea (AWD), Acute Bloody Diarrhoea (ABD) and measles.
Figures 3 and 4 show the proportionate morbidity trends for Malaria, ARI, AWD, suspected measles and ABD.
Table 2
No. Disease
New cases for weeks Cumulative cases since week 01 of 2015 37 of 2014 37 of 2015
1 Malaria 3,081 14,905 167,343
2 AWD 869 1,719 64,281
3 ARI 1,953 5,245 133,910
4 ABD 185 230 8,315
5 Measles 3 11 499
Figure 3
Figure 4
During week 37 of 2015, malaria is the top cause of morbidity followed by ARI, AWD, ABD and suspect measles. During the corresponding week of 2014, malaria was the top cause of morbidity followed by ARI, AWD, ABD and
suspect measles. The proportionate morbidity for malaria increased while ARI, ABD, AWD, and measles decreased in week 37 of
2015 when compared to week 36 of 2015 (Figures 3 and 4).
Specific Priority Epidemic-Prone Diseases
Acute Respiratory Infection (ARI)
During week 37 of 2015, ARI registered the second highest proportionate morbidity of 15.3% (Figures 4 and 5) which is lower when compared to 16.2% in week 37 of 2014 and 18.4% in week 36 of 2015 (Figure 5).
During week 37 of 2015, UN House PoC registered the highest ARI incidence (cases per 10,000) of 267 followed by Bentiu (224), and Kodok (145).
In week 37 of 2014, the ARI incidence (cases per 10,000) was 141 in Bentiu, 138 in UN House, and 103 in Malakal PoC. (Figure 5.1).
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
0%
10%
20%
30%
40%
50%
60%
51 01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37
2013 2014 2015
Co
mp
lete
ne
ss
Pe
rce
nt
of
all
co
nsu
lta
tio
ns
Epidemiologic Week
Priority Disease Proportionate Morbidity from week 51 of 2013 to week 37 of 2015
Completeness ARI Bloody Diarrhea Malaria Suspected Measles Watery Diarrhoea
16.2% 15.3%
1.5%0.67%
25.5%
43.4%
0.025%
0.032%
7.2%
5.0%
0.0%
10.0%
20.0%
30.0%
40.0%
50.0%
60.0%
70.0%
wk 37 of 2014 wk 37 of 2015
Pe
rce
nt
of
all
co
nsu
lta
tio
ns
Priority Disease Proportionate Morbidity for week 37 of 2014 and 2015
ARI
Bloody Diarrhea
Malaria
Suspected Measles
Watery Diarrhoea

Early Warning and Disease Surveillance System
4
Figure 5
Figure 5.1
Acute Watery Diarrhoea (AWD)
During week 37 of 2015, AWD registered the 3rd highest proportionate morbidity of 5.0% but it is lower when compared to 7.2% in week 37 of 2014 and 5.2% in week 36 of 2015. Despite the cholera outbreaks in Juba and Bor, the overall, the AWD trend among IDPs has remained stable since the beginning of 2015. (Figures 4 and 6)
During week 37 of 2015, Renk registered the highest AWD incidence (cases per 10,000) of 219, followed by Bor (125), and Melut (71). In the corresponding week of 2014, the AWD incidence (cases per 10,000) was 54 in Bentiu and 53 in UN House. (Figure 7)
Figure 6
Figure 7
0.0
5.0
10.0
15.0
20.0
25.0
30.0
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Pe
rce
nt
of
tota
l co
nsu
lta
tio
ns
Epidemiologic Week
ARI Proportionate Morbidity from week 51 of 2013 to week 37 of 2015
2013 2014 2015
88141
10321
138
0 1166
0 0 0 16 0 0 0 0 0 0
43
224
97 95
93
92
267
145
41 12 -
100
200
300
400
500
Ca
ses
pe
r 1
0,0
00
ARI Incidence, by IDP Site , for week 37 of 2014 and 2015
wk 37 of 2014
wk 37 of 2015
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51Pe
rce
nt
of
tota
l co
nsu
lta
tio
ns
Epidemiologic Week
AWD Proportionate Morbidity from week 51 of 2013 to week 37 of 2015
2013
2014
2015
2954
5 4 23 1353
16 128 40
15 0 0 0 0
15
27 125
11
51 71
51
26
219
30 8 18 8 9 15 9 -
50
100
150
200
250
300
Ca
ses
pe
r 1
0,0
00
AWD Incidence, by IDP Site , for week 37 of 2014 and 2015
wk 37 of 2014
wk 37 of 2015

Early Warning and Disease Surveillance System
5
Dysentery / Acute Bloody Diarrhoea (ABD)
During week 37 of 2015, ABD registered the 4th highest proportionate morbidity of 0.67% which is lower when compared to 1.5% in week 37 of 2014 and 0.79% in week 36 of 2015. Overall, the ABD trend has remained stable since the beginning of 2015 (Figure 4 and 8).
Figure 8
During week 37 of 2015, Renk registered the highest ABD incidence (cases per 10,000) of 35, followed by Melut (27), and Kadok (20). In week 37 of 2014, the ABD incidence (cases per 10,000) was 43 in Lankien, 14 in Akoka, and 5 in Bentiu (Figure 9). Figure 9
Measles
During week 37 of 2015, measles registered the 5th highest proportionate morbidity of 0.032% which is lower when compared to 0.034% in week 36 of 2015 but higher when compare 0.025% week 37 of 2014 (Figure 4 and 10).
During week 37 of 2015, 10 new measles cases have been reported from Bentiu PoC and one from Renk.
Since the beginning of 2015, a total of 433 measles cases including 13 deaths (CFR 3%) have been registered in
Bentiu PoC (Figure 10.1). Following a vaccination campaign in week 15 that reached 91% (21,361) of children aged
six months to 15 years, the cases declined significantly. However, with the new arrivals since June 2015, low-level
transmission persisted despite the ongoing measles vaccination on arrival. Consequently, a follow up integrated
Polio and measles vaccination campaign was conducted in week 36 reaching 84.8% (43,931) of the targeted 51,832
children aged 6 months to 15 years with measles containing vaccine.
A total of seven measles cases have been reported from Renk since 12 June 2015. In week 31 of 2015, one of four
samples tested from Renk was confirmed as measles IgM positive. Preparations are underway for reactive measles
vaccination targeting children aged six months to five years.
Since the beginning of 2015, 440 suspect measles cases have been registered countrywide as part of the measles
case based and laboratory backed surveillance system, of which 204 (46%) were clinically confirmed, 79 (18%)
epidemiological link, 127 (29%) laboratory negative, 28 (6%) laboratory confirmed as measles and results of 2
(0.5%) is still pending.
3.2
0.0
1.0
2.0
3.0
4.0
5.0
6.0
7.0
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Pe
rce
nt
of
tota
l co
nsu
lta
tio
ns
Epidemiologic Week
ABD Proportionate Morbidity from week 51 of 2013 to week 37 of 2015
2013
2014
2015
3 5
43
4 314
3 0 0 0
2 12 5
27
5
35
20
3 5 0 -
10
20
30
40
50
Ca
ses
pe
r 1
0,0
00
ABD Incidence, by IDP Site , for week 37 of 2014 and 2015
wk 37 of 2014
wk 37 of 2015

Early Warning and Disease Surveillance System
6
The 28 confirmed measles cases were from Duk (3), Wulu (2), Rubkona (14), Maridi (1), Tambura (1), Wau (1), Kajo Keji
(2), Yei (2) Morobo (1), and Renk (1) counties.
Since the beginning of 2015, a total of 41 Rubella cases have been confirmed from Central Equatoria (15), Eastern
Equatoria (12), Lakes (3), Unity (1), Upper Nile (6), Western Bahr el Ghazal (2), and Western Equatoria (2).
Figure 10
Figure 10.1
Malaria
During week 37 of 2015, malaria registered the highest proportionate morbidity of 43.4% which is higher when compared to 25.5% in week 37 of 2014 and 41.2% in week 36 of 2015. (Figures 4 and 11)
The malaria trend was stable from the beginning of 2015 up to week 19 of 2015 when it started rising steadily. The rising malaria trend is largely driven by transmission in Bentiu PoC, Malakal PoC, UN House PoC, Renk, and Mingkaman (Figures 11.1, 11.2, 11.3, 11.4, and 11.5).
During week 37 of 2015, Bentiu PoC registered the highest malaria incidence (cases per 10,000) of 714, followed by Renk (536), Bor (386), Malakal (262), Melut (194), and UN House PoC (181) as seen in Figure 12.
As seen from Figures 12.1, 12.2, 12.3, and 12.4 showing the malaria incidence by IDP site for 2014 and 2015; the malaria incidence in week 37 of 2015 shows that Bentiu PoC, Malakal PoC, UN House PoC, and Renk are experiencing a malaria upsurge that is consistent with a malaria epidemic.
In response to the current malaria trends in Bentiu PoC, health-implementing partners have increased from three to five to improve access to primary health care services. Hence, MSF, IOM and World Relief have opened additional clinics in response to the increased caseload. Malaria diagnostics and medicines have been enhanced and integrated community case management of malaria is ongoing. In addition, the malaria mass presumptive treatment campaign of all fever cases at household level was conducted from 10-16 September 2015. Children were treated during based on history of fever, current fever, and history malaria treatment. The preliminary results revealed that 14,000 out of the targeted 30,000 children under-five years were reached.
To interrupt transmission at community level, the first round of vector control interventions [distribution of Long Lasting Insecticide Treated Nets (LLINs), larviciding, and indoor residual spraying (IRS) was conducted in Bentiu PoC. The second round is planned for a week after the first one and the third round will be implemented two weeks after the second round. Advocacy is on-going to extend to other IDP sites where malaria upsurges have been
0.0
0.5
1.0
1.5
2.0
2.5
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Pe
rce
nt
of
tota
l co
nsu
lta
tio
ns
Epidemiologic Week
Suspected measles Proportionate Morbidity from week 51 of 2013 to week 37 of 2015
2013
2014
2015
0
10
20
30
40
50
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35
Nu
mb
er o
f m
easl
es c
ases
Week of rash onset in 2014
Measles epidemic curve in Bentiu PoC, week 1-37, 2015
alive
died

Early Warning and Disease Surveillance System
7
reported. In addition, behavioural change communication for prompt care seeking and malaria prevention is ongoing.
Figure 11
Figure 11.1
Figure 11.2
Figure 11.3
47.8
26
43
0.0
10.0
20.0
30.0
40.0
50.0
60.0
01 03 05 07 09 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Pe
rce
nt
of
tota
l co
nsu
lta
tio
ns
Epidemiologic Week
Malaria Proportionate Morbidity from week 51 of 2013 to week 37 of 2015
2013
2014
2015
19
62
-
10
20
30
40
50
60
70
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Pro
po
rtio
na
te m
orb
idit
y [
%]
Week of reporting
Malaria Proportionate Morbidity, Bentiu PoC, 2014-2015
Prop mob 2014
Prop mob 2015
21
48
-
10
20
30
40
50
60
70
80
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Pro
po
rtio
na
te m
orb
idit
y [
%]
Week of reporting
Malaria Proportionate Morbidity, Malakal PoC, 2014-2015Prop mob 2014
Prop mob 2015
19
26
-
10
20
30
40
50
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Pro
po
rtio
na
te m
orb
idit
y [
%]
Week of reporting
Malaria Proportionate Morbidity, UN House PoC, 2014-2015
Prop mob 2014
Prop mob 2015

Early Warning and Disease Surveillance System
8
Figure 11.4
Figure 11.5
Figure 12
Figure 12.1
Figure 12.2
-
20
40
60
80
100
120
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51Pro
po
rtio
na
te m
orb
idit
y [
%]
Week of reporting
Malaria Proportionate Morbidity, Renk, 2014-2015Prop mob 2014
Prop mob 2015
-
10
20
30
40
50
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51Pro
po
rtio
na
te m
orb
idit
y [
%]
Week of reporting
Malaria Proportionate Morbidity, Mingkaman, 2014-2015
Prop mob 2014
Prop mob 2015
128 108 34 0100 37
13510 0 0 21
1500 0 17
67
714
386 262194
181
0
536
16946 39 35 2
1832 -
200
400
600
800
1,000
Ca
ses
pe
r 1
0,0
00
Malaria Incidence, by IDP Site , for week 37 of 2014 and 2015
wk 37 of 2014
wk 37 of 2015
108
752
-
100
200
300
400
500
600
700
800
900
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
case
s p
er
10
,00
0
Week of reporting
Malaria incidence trends, Bentiu PoC 2014 to 2015 incidence 2014
incidence 2015
mean 2014
mean 2014+1SD
mean+2SD
229
271
-
100
200
300
400
500
600
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
case
s p
er
10
,00
0
Week of reporting
Malaria incidence trends, Malakal PoC 2014 to 2015 incidence 2014
incidence 2015
mean 2014
mean 2014+1SD
mean+2SD

Early Warning and Disease Surveillance System
9
Figure 12.3
Figure 12.4
Figure 12.4
Hepatitis E Virus (HEV)
Hepatitis E Virus remains a major public health problem among IDPs and has been confirmed in three out of eight
IDP sites where Acute Jaundice Syndrome (AJS) cases have been reported (Figures 13 and 14).
The first AJS cases were reported in Juba 3 PoC in week 04 of 2014. Since then, HEV cases were confirmed in three
IDP sites including Mingkaman [8 by ELISA/PCR]; Bentiu [2 by ELISA; 27 by PCR]; and Lankien [3 by PCR]. Figure 14.
During week 37 of 2015, four new HEV cases have been admitted in MSF hospital in Bentiu PoC giving an overall, 87
admitted cases including 13 deaths (CFR 14.9%). Majority of cases were aged 2-4 (30%) and 15-44 (29%). Similarly,
most 7 (53%) of the deaths among hospitalised HEV cases in Bentiu PoC were 15-44 years of age.
In week 37 of 2015, 144 new cases of HEV were reported from Bentiu PoC and one from Lankien. Hence the
cumulative for HEV is 1,342 cases including 13 deaths (CFR 0.97%) in Bentiu; 153 cases including seven deaths (CFR
4.6%) in Mingkaman; and 35 HEV cases including one death (CFR 2.9%) in Lankien.
Of the 1,304 HEV cases line listed in Bentiu, 708 (54%) are male while the rest 592 (45%) are female (Table 5.1). The
majority of the HEV cases detected in Bentiu are 5-9 years of age [32%], 2-4 years of age [27%], and 15-44 years
[21%] (Table 5.1).
135
182
-
50
100
150
200
250
300
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
case
s p
er
10
,00
0
Week of reporting
Malaria incidence trends, UN House PoC 2014 to 2015 incidence 2014
incidence 2015
mean 2014+1SD
mean+2SD
mean 2014
453
536
-
100
200
300
400
500
600
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
case
s p
er
10
,00
0
Week of reporting
Malaria incidence trends, Renk, 2014 to 2015 incidence 2014
incidence 2015
mean 2014
mean 2014+1SD
mean+2SD
77
67
-
20
40
60
80
100
120
140
160
180
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
case
s p
er
10
,00
0
Week of reporting
Malaria incidence trends, Mingkaman, 2014 to 2015 incidence 2014
incidence 2015
mean 2014
mean 2014+1SD
mean+2SD

Early Warning and Disease Surveillance System
10
Figure 13
Figure 14
Table 5.1 HEV cases by age and gender in Bentiu PoC
Age in years Female n (%)
Male n (%) (Unknown)
Total n (%)
<2 years 21 (4) 22 (3) 0 43 (3)
2-4 years 132 (22) 216 (31) 0 348 (27)
5-9 years 177 (30) 238 (34) 0 415 (32)
10-14 years 86 (15) 91 (13) 1 178 (14)
15-44 years 154 (26) 121 (17) 0 275 (21)
≥45 years 18 (3) 9 (1) 0 27 (2)
(Blank) 4(1) 11 (2) 3 18 (1)
Grand Total 592 (45) 708 (54) 4 1304 (100)
Most cases in Bentiu have originated from Sectors 5, 4, and 3 as shown in Table 5.2. Table 5.2 HEV case distribution by PoC/sector in Bentiu PoC
Camp Positive
n (%) Negative
n (%) Unknown Grand Total
n (%)
Outside 5 (2.2) 4 (0.5) 7 16 (1.2)
PoC 1 14 (6.3) 20 (2.6) 1 35 (2.7)
PoC 2 13 (5.8) 18 (2.3) 5 36 (2.8)
PoC 3 18 (8.1) 37 (4.8) 9 64 (4.9)
PoC 4 34 (15.2) 42 (5.4) 0 76 (5.8)
PoC 5 23 (10.3) 21 (2.7) 0 44 (3.4)
PoC 6 6 (2.7) 29 (3.8) 4 39 (3.0)
Sector 1 4 (1.8) 50 (6.5) 36 90 (6.9)
Sector 2 3 (1.3) 24 (3.1) 3 30 (2.3)
Sector 3 26 (11.7) 149 (19.3) 54 229 (17.6)
Sector 4 29 (13.0) 162 (21.0) 94 285 (21.9)
Sector 5 39 (17.5) 190 (24.6) 94 323 (24.8)
(Blank) 9 (4.0) 27 (3.5) 1 37 (2.8)
Grand Total 223 (17.1) 773 (59.3) (308) 1304 (100)
During the current HEV outbreak in Bentiu, 13 deaths have been registered giving an overall CFR of 0.97%. Case
fatality rates were highest among individuals aged 15-44 [2.5%] and under two [2.3%] years; male [1.3%]; and
individuals living outside the PoC 18.8% followed by residents of PoC 4 [3.9%], PoC 1 [2.9%], and PoC 5 [2.3%].
Among pregnant women, the CFR remains at 28.6%.
0
50
100
150
200
250
300
350
0
2
4
6
8
10
12
14
16
3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37
2014 2015
No
ca
ses
in B
en
tiu
No
ca
ses
in t
he
r ID
P s
ite
s
Epidemiological week
Acute Jaundice Syndrome cases by IDP site from week 03, 2014 to week 37, 2015
Awerial Bor Malakal Tongping Lul Juba 3 Lankien Bentiu
0
50
100
150
200
250
300
350
0
2
4
6
8
10
12
14
16
3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51 1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37
2014 2015
No
. cas
es i
n B
enti
u
No
, ca
ses
in o
the
r si
tes
Epidemiological week
Hepatitis E Virus trends in Mingkaman, Bentiu, and Lankien, week 10, 2014 - week 37, 2015
Awerial Lankien Bentiu

Early Warning and Disease Surveillance System
11
A comprehensive HEV response strategy has been developed to guide the response with priority interventions being supportive case management, targeted preventive interventions during antenatal visits, soap distribution, shock chlorination of boreholes, as well as house-to-house hygiene and sanitation promotion.
Nutrition in Bentiu PoC_source Nutrition Cluster in Bentiu
In week 36, the total number of Severe Acute Malnutrition (SAM) cases U5 admitted in Outpatient Therapeutic Programs (OTP) was 504, marking a consistently increase compared to 332 in week 35 and 335 in week 34. Admissions in OTP are registering a significant escalation since week 27 of 2015, especially if compared to the same epidemiological weeks in 2014 (Figure 15).
Similarly in week 36 of 2015, the inpatient admission trend of severely malnourished children with medical complications is increasing, with 42 children admitted in the stabilization centre, as compared to 34 admitted in week 35 of 2015 (Figure 15.1).
In week 36, the Global Acute Malnutrition (GAM) rate remains 20.8%, exceeding the WHO emergency threshold of 15%, with associated SAM of 4.9% which is above the WHO emergency threshold of 2% for SAM (SMART Survey 2014). The situation in Bentiu PoC remains critical.
Figure 15
Source: Nutrition cluster Bentiu Poc
Figure 15.1
Source: Nutrition cluster Bentiu Poc
Cholera
As of 12 September 2015, a total of 1,743 cholera cases including 46 deaths (CFR 2.64%) have been reported in Juba County and in Bor, Jonglei State. In Juba County 1,605 cases including 45 deaths (CFR 2.80%) have been reported from seven Payams. In Bor, 138 cases including one death (CFR 0.72%) were reported from Malou and other areas around the county. Evaluation of the cholera response is underway. The findings are expected to inform better preparedness and contingency planning.
The initial cases in Juba were traced back to 18 May 2015 in UN House PoC where the first cholera case was confirmed on 1 June 2015 (Figure 15.2). Most of the cholera cases in Juba have been reported from Gumbo followed by New site, Juba3 PoC, Gudele 2, Atlabara B, and Munuki. In Bor County, the majority of the cases originated from Malou 41 (36%) and Langbar 12 (10.4%) in Makuach Payam.
National and state level cholera taskforce committees are coordinating the ongoing cholera preparedness and
20 14 21 24
6953
76
153116
7696
132 145126
55
278
94 108 100
47 6133
72 65 6847
65 5334
9268 83
214
149
93104 112
128 11982
61 66 75
141117 106
80
186168
197 185
140156
118
228
278
480
615
511
358
466484
436
507514
500
355358
336 332
504
0
100
200
300
400
500
600
700
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39 41 43 45 47 49 51
Ad
mis
sio
ns
Epidemiological Week
Severe Acute Malnutrition Treated in the Out Patient Therapeutic Program in Bentiu PoC in 2014 and 2015
Admissions 2014
Admissions 2015
5 5 69
5
17
117
1612 11
97 8
1513
7 8
13
6
11 1215
19
24 24
19
28
18
34
46
37
2927
34
42
05
101520253035404550
1 3 5 7 9 11 13 15 17 19 21 23 25 27 29 31 33 35 37 39
Nu
mb
er
of
ad
mis
sio
ns
Epidemiological week of reporting
SAM with Medical Complications Admissions at MSF stabilisation Center in Bentiu PoC in 2015

Early Warning and Disease Surveillance System
12
response activities. As a result, a drastic decline in cases has been registered in the affected counties. Figure 15.2
JS: Jonglei State; CES: Central Equatoria State; CFR: Case Fatality Rate
Acute Flaccid Paralysis (AFP)
A cumulative of 221 AFP cases have been reported countrywide since the beginning of 2015 (Table 5). The annualized non-Polio AFP (NPAFP) rate (cases per 100,000 population children 0-14 years) is 3.99 per 100,000
population of children 0-14 years (target ≥2 per 100,000 children 0-14 years) (Table 5). All but three states (Jonglei, Unity, and Upper Nile) have attained the targeted NPAFP rate of ≥2 per 100,000
children 0-14 years. The non-Polio Enterovirus (NPEV) isolation rate (a measure of the quality of the specimen cold chain) is 13.9% (target ≥10%) (Table 5).
Stool adequacy stands at 95%, a rate that is higher than the target of ≥80% (Table 5). The cumulative for circulating Vaccine Derived Poliovirus type 2 (cVDPV2) cases now stands at three cases with only
one case reported in 2015. Table 5
Other Diseases of Public Health Importance
Guinea worm (Dracunculiasis)
There was no new suspect Guinea worm disease case reported during week 37 of 2015.
Viral Haemorrhagic Fever
The Republic of South Sudan continues to enhance its readiness capacities for Ebola/Marburg virus disease. The national Ebola/Marburg taskforce is coordinating the implementation of interventions guided by a national
Ebola/Marburg contingency plan.
4 2 7 56
130
229
235
160
237
149
100
77 86
45 3932
17- -
14.3
17.9
6.2
3.8
1.4 1.6 1.6 1.9
-1.2
2.2
4.3
- - - -
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
18.0
20.0
0
50
100
150
200
250
300
20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37
Cas
e F
atal
ity
Rat
e [%
]
Nu
mb
er
of
case
s
Week of onset
JS
CES
CFR[%]

Early Warning and Disease Surveillance System
13
No Ebola/Marburg cases have been confirmed in South Sudan but six alerts have been investigated in Ezo, Nzara, Terekeka (Tali) and Juba (Hai Jalaba and Gudele) since 2014.
Visceral Leishmaniasis (Kala-azar)
In week 37 of 2015, three health facilities (Ulang, Walgak, and Kajo-keji County Hospital) reported 10 cases (8 new and 2 secondary cases).
From week 1 to date, a total of 2,631 cases (2,088 [79.4%] new cases; 543 [20.6%] relapses/PKDL; 98 [3.7% defaulters]; and 88 [3.3%] deaths) have been reported from 21 treatment centres. In week 37 of 2014, a total of 4,023 cases (3,692 new cases; 331 relapses/PKDL; 174 defaulters and; 138 deaths (CFR 3.4%) were reported from 15 treatment centres.
Of the 2,631 cases, majority of cases [1,470 (55.9%)] are male and aged 15 years [1171 (44.5%)] followed by 5-14 years [1072 (40.7%)] and <5years [382 (14.5%)].
During 2015, Lankien has reported the highest number of cases (1,226); followed by Walgak (306); Ulang (163); Akobo (133), Chuil (126); Pagil (108), Melut IDP (110); Narus ([MOH/ARC)] (106); and Rom (64).
Generally the number of cases reported in 2015 is lower when compared to 2014 which could be attributed to the low reporting completeness, withdrawal of some partners from health facilities due to insecurity, and the tail end of the transmission season.
WHO and partners continue to support enhanced surveillance, case management and interventions to interrupt transmission through the following: supporting implementing partners with case management supplies; training frontline healthcare workers on Kala-azar case management; support supervision of treatment facilities; supporting community sensitisation on Kala-azar; and distribution of LLITNs in affected and high-risk areas.
Meningitis
One suspect meningitis death (involving a neonate) was reported from Nyal, Panyijiar in week 37 of 2015. A cumulative of four suspect meningitis cases including one death have been reported among under-fives in Nyal since 18 August 2015.
Animal bites (suspect rabies)
There was no new suspect rabies case reported in week 37 of 2015.
All-Causes Mortality Data
During week 37 of 2015, mortality lists were received from Bentiu PoC, Juba 3 PoC, Akobo, and Malakal PoCs. A total of 45 deaths were reported during week 37 of 2015, with 38 (84%) deaths being reported from Bentiu PoC;
while 32 (71%) occurred in children under five years of age see Table 6. During the corresponding week of 2014, a comparatively lower number of deaths (26) were reported as seen in Table 6.
Table 6: Number of deaths by IDP camp during week 37 of 2015 and 2015 Cause of Death by IDP site
2014 2015
<5yrs ≥5yrs <5yrs ≥5yrs
Bentiu 3 8 29 9
Juba 3 2 4 2 1
Malakal 1 3 1 3
Melut 0 2 0 0
Mingkaman 2 1 0 0
Grand Total 8 18 32 13
During week 37 of 2015, malaria registered the highest proportionate mortality of 37.8% (36.1% in week 36 of
2015), followed by perinatal deaths (8.9%), TB/HIVAIDS (6.7%), and pneumonia (6.7) (Table 6.1).
Of the 17 malaria deaths reported in week 37 of 2015, 16 (94%) occurred in Bentiu PoC with the majority 12 (71%)
occurring in children under five years of age (Table 6.1).

Early Warning and Disease Surveillance System
14
Table 6.1: Proportionate mortality by cause of death in week 37 of 2015 and 2015
Cause of Death by IDP site
Bentiu Juba 3 Malakal
Grand Total Proportionate mortality [%] <5yrs ≥5yrs <5yrs ≥5yrs <5yrs ≥5yrs
Chronic illness 0 1 0 0 0 0 1 2.2
Malaria 12 4 0 0 0 1 17 37.8
Perinatal death 3
0 0 1 0 4 8.9
Pneumonia 1 1 1 0 0 0 3 6.7
SAM 1 0 0 0 0 0 1 2.2
Sepsis 1 0 0 0 0 0 1 2.2
TB/HIV/AIDS 1 0 1 1 0 0 3 6.7
Unknown 8 3 0 0 0 1 12 26.7
Heart failure 1 0 0 0 0 0 1 2.2
Kala azar 1 0 0 0 0 0 1 2.2
Acute viral hepatitis 0 0 0 0 0 1 1 2.2
Grand Total 29 9 2 1 1 3 45 100.0
Under-five Mortality Rate (U5MR)
In week 37 of 2015, with a total population of 117,669 and 29 new deaths among under-fives in Bentiu PoC, the under-5 mortality rate is 1.760 deaths per 10,000 per day, which is below the U5MR emergency threshold of 2 deaths per 10,000 per day (Figures 16 and 16.1).
The notable causes of death in children under five years in Bentiu during week 37 of 2015 included malaria, perinatal complications, and pneumonia.
Figure 16
Figure 16.1
Crude Mortality Rate
The crude mortality rates (CMR) from week 51 of 2013 to week 37 of 2015 are shown in Figure 17. During week 37 of 2015, the CMRs were below the emergency threshold for the four IDP sites that submitted
mortality data. The CMR for Bentiu PoC in week 37 of 2015 was 0.461 deaths per 10,000 per day.

Early Warning and Disease Surveillance System
15
Figure 17
Disease specific Mortality Mortality due to Acute Watery Diarrhoea
Since the beginning of 2015, a total of 58 AWD deaths have been reported. Out of the 58 AWD deaths reported in 2015, 36 (62.1%) occurred in Bentiu, 9 (15.5%) in UN House, 4 (6.9%) in Wau Shiluk, 3 (5.2%) in Akobo, 3 (5.2%) in Mingkaman, and 3 (5.2%) in Malakal PoC. Overall, 210 AWD deaths have been reported since the onset of the crisis with Bentiu PoC having the highest number of AWD deaths (Figure 18).
During week 37 of 2015, a total of 16 malaria deaths were reported from Bentiu PoC. Overall, Bentiu PoC has reported the highest number of deaths (590 deaths) since the beginning of the year with 119 (20%) of the deaths attributed to malaria (Figure 18.1 and Table 7).
Figure 18
Figure 18.1
Overall Mortality
Since the beginning of 2015, a total of 999 deaths have been reported from the IDP sites of which 473 (47%) were children under-5 years. The majority of the deaths occurred in Bentiu, Malakal, Juba 3 PoC and, Wau Shiluk.
Since the beginning of 2015, malaria has registered the highest proportionate mortality of 14.9% followed by malnutrion (7.8%), TB/HIVAIDS (7.8%), acute watery diarrhoea (5.8%), perinatal deaths (5.3%), and pneumonia (5.2%) (Table 7).
0
2
4
6
8
10
12
14
5152 1 2 3 4 5 6 7 8 9 1011121314151618192021222324252627283537434546495051 2 3 5 7 12131415161718192021222324252627282930323334
2013 2014 2015
Nu
mb
er o
f d
eath
s
Epidemiological week
Mortality due to AWD by camp, week 51 of 2013 to week 37 of 2015
Wau Shiluk AkoboMingkaman MalakalJuba 3 BorBentiu

Early Warning and Disease Surveillance System
16
Table 7: Mortality trend by IDP site, week 1 of 2015 to week 37 of 2015
IDP camps Acu
te J
aun
dic
e
Syn
dro
me
Acu
te w
ater
y
dia
rrh
oe
a
Can
cer
Gu
nsh
ot
wo
un
d
Hea
rt d
ise
ase
Hyp
erte
nsi
on
Kal
a-A
zar
Mal
aria
Mat
ern
al d
eath
Mea
sles
Per
inat
al d
eath
Pn
eum
on
ia
SAM
Sep
tice
mia
TB/H
IV/A
IDS
Trau
ma
Hep
atit
is E
Oth
ers
Tota
l dea
ths
Bentiu 6 36 8 9 3 0 1 119 0 10 17 30 52 14 26 1 13 245 590
Bor 1
0 0 0
0 0 5
1 0 0 2 9
Juba 3 0 9 1 1
4 0 10 1 0 15 9 7 1 24 0 0 36 118
Malakal 0 3
1 8 0 4 6
0 14 8 14 0 15 0 0 70 143
Melut 0
1
0 0 3 1 1 0 1 1
0 7 0 0 9 24
Mingkaman 0 3 0
0 0
2 0 0
2 4 0 1 0 1 15 28
Akobo 0 3 0 2 0 0 3 3 0 0 1 2 1 0 2 0 0 9 26
Wau Shiluk 0 4 0
4 2
8 0 1 0
0 2 0 0 40 61
Total deaths 7 58 10 13 15 6 11 149 2 11 53 52 78 15 78 1 14 426 999
Proportionate mortality [%] 0.7 5.8 1.0 1.3 1.5 0.6 1.1 14.9 0.2 1.1 5.3 5.2 7.8 1.5 7.8 0.1 1.4 42.6 100
General recommendations
In response to the current malaria trends in Bentiu PoC, Malakal PoC, UN House PoC, and Renk a coordinated response has been initiated to improve access to treatment, interrupt transmission, and engage communities. This includes mass presumptive treatment of fever cases for malaria, distribution of LLINs, larviciding, indoor residual spraying, and behavioral change communication.
Consistent and sustained implementation of a comprehensive HEV response is already underway and includes supportive case management for symptomatic cases, targeted preventive interventions during antenatal visits; improving access to safe drinking water and improved sanitation facilities; instituting interventions for a safe water chain; preventive vaccination using HEV vaccine for groups with a high risk for adverse clinical outcomes including mortality; and house-to-house hygiene and sanitation promotion including distribution of NFIs like soap and jerry cans.
An integrated measles and polio vaccination campaign was conducted in Bentiu PoC in week 36 and in addition, vaccination on arrival and routine vaccination at existing fixed and outreach units is ongoing.
Enhanced nutrition screening at designated clinics, mobile clinics, and during the house-to-house visits are underway to identify and initiate early treatment for malnourished cases.
The national and state level cholera taskforce committees should continue implementing cholera response interventions to control the outbreaks in Juba and Bor.
Integrate TB/HIV/AIDS prevention and control into the routine healthcare services in all the IDP sites.
Biological samples should be obtained and shipped to Juba to allow laboratory confirmation of emerging outbreaks of measles, AJS, bloody diarrhea, and cholera.
The ongoing integrated response to Kala-azar that entails enhanced surveillance, improved access to diagnosis and treatment facilities, refresher training of healthcare workers on Kala-azar case management, replenishing of drug stocks in endemic areas, as well as communication on Kala-azar prevention and control should be sustained.
Support the implementation of the Ebola preparedness and response so as to enhance capacities for case detection, investigation, response and community awareness on Ebola prevention and control.
Please send all disease surveillance information and any outbreak rumours to [email protected]. IDSR reports should be submitted by COB Monday after the close of each epidemiologic week.
For comments or questions, please contact
Department of Epidemics, Preparedness and Response, MoH-RSS E-mail: [email protected],
HF radio frequency: 8015 USP; Selcall: 7002