Embed Size (px)
Citation preview

DOCUMENT RESUME
ED 443 054 CG 030 131
AUTHOR Cook, Paddy; Davis, Carolyn; Howard, Deborah L.; Kimbrough,Phyllis; Nelson, Anne; Paul, Michelle; Shuman, Deborah;Brooks, Margaret K.; Dogoloff, Mary Lou; Vitzthum, Virginia;Hayws, Elizabeth
TITLE Substance Abuse among Older Adults. Treatment ImprovementProtocol (TIP) Series 26.
INSTITUTION Substance Abuse and Mental Health Services Administration(DHHS/PHS), Rockville, MD. Center for Substance AbuseTreatment.
REPORT NO SMA-98-3179PUB DATE 1998-00-00NOTE 191p.; For other documents in the TIP Series, see CG 030
099-103 and CG 030 130-134.CONTRACT 270-95-0013AVAILABLE FROM National Clearinghouse for Alcohol and Drug Information,
P.O. Box 2345, Rockville, MD 20847-2345. Tel: 800-729-6686(Toll Free).
PUB TYPE Guides Non-Classroom (055) Information Analyses (070)Tests/Questionnaires (160)
EDRS PRICE MF01/PC08 Plus Postage.DESCRIPTORS *Alcohol Abuse; Behavior Modification; Counseling;
*Counselor Training; *Drug Rehabilitation; *Gerontology;Intervention; Mental Health; Motivation; *Older Adults;*Substance Abuse
IDENTIFIERS Nonprescription Drugs; Prescription Drugs; Solution FocusedBrief Therapy
ABSTRACTAs alcohol and other drug disorders become acknowledged as
major problems, the need increases for current information on the scope ofthe problem and appropriate treatment. This TIP serves to educate treatmentproviders with information about older adults who, in general, are morelikely to hide their substance abuse, less likely to seek professional help,and mistake symptoms of substance abuse for another ailment. It bringstogether literature on substance abuse and gerontology to recommend bestpractices for identifying, screening, assessing, and treating alcohol,prescription drugs, and other medication abuse among people age 60 and older.Brief intervention is recommended as the first step of treatment, followed bymotivational interviewing, and intervention. Brief interventions may includemotivation for change strategies, patient education, assessment and directfeedback, contracting and goal setting, and behavioral modificationtechniques. Treatment programs take a holistic approach since a number ofinterrelated emotional, social, medical, and spiritual problems characterizeolder adults' experiences with substance abuse. It also includes informationon cognitive-behavioral, group, individual, and family therapy approaches totreatment. Appendixes include: "Legal and Ethical Issues," "Tools,""Bibliography," "Resource Panel," and "Field Reviewers." (Contains 19 figuresand approximately 400 resources.) (JDM)
Reproductions supplied by EDRS are the best that can be madefrom the original document.

U.S. DEPARTMENT'OF HEALTH ANDH ,_,MAN SERVICES
Public Health Service
Substance Abuse andMental Health ServicesAdministration
Substance Abuse and Mental Health Services Administration
Center for Substance Abuse Treatment
SubstanceAbuseAmongOlderAdults
Treatment Improvement Protocol (TIP) Series
26
U.S. DEPARTMENT OF EDUCATIONMee of Educational Research and Improvement
EDUCATIONAL RESOURCES INFORMATIONCENTER (ERIC)
O This document has been reproduced asreceived from the person or organizationoriginating it.
O Minor changes have been made toimprove reproduction quality.
lsay Points of view or opinions stated in thisdocument do not necessarily represent
CZ official OERI position or policy.
111
)1.0
-WWWW1a
=NM ailiMENIMM=1Mi=INN ETMZMINEZINZEN
dri;. salmIrEZIMINIDESN
a232=i=i 1-"=MiisimmstiMSWINIIEW
amM=SMRs..eammi 111111111111
.;1- COPY AVAILABLE

EST COPY AVAIILABLE
RESOURCES FOR PROVIDERS
American Association of Retired Persons601 E St., NWWashington, DC 20049202-434-2277202-434-2562 (fax)www.aarp.org
National Center on Addiction andSubstance Abuse at Columbia University
152 West 57th St.New York, NY 10019212-841-5200212-956-8020 (fax)www.casacolumbia.org
Join Together441 Stuart St.Boston, MA 02116617-437-1500617-437-9394 (fax)www.jointogether.org
National Aging Information CenterU.S. Administration on Aging330 Independence Ave., SW, Rm. 4656Washington, DC 20201202-619-7501202-401-7620 (fax)202-401-7575 (TTY)www.ageinfo.org
a
ZZ-71 Trl 0
rn C)M 0
0 3)

Ple
ase
mai
l thi
s re
gist
ratio
n fo
rm to
rec
eive
not
ice
of fu
ture
pub
licat
ions
Tll'
26
Sub
stan
ce A
buse
Am
ong
Old
er A
dults
Ple
ase
indi
cate
you
r fie
ld:
Adm
inis
trat
or U
Clin
icia
nC
ouns
elor
0 R
esea
rche
rO
ther
Nam
e:T
itle:
88
L'1,
t,: 0
%.°
: 7 '2
4,-.
'84,
.t(''-
,--)
.).
.t:L)
.:
7.8
'6'1
-.t-
L6)
'5 ''
!.::
-'1!
!O
rgan
iLat
ion:
eo 8
0 .<
=1.
., la
.-' l
a' o
ay
ts.)
ras.
0ad
.00
,-,
..-.
p,o
6 Ld
u.,
a.to
Add
ress
:'
'sl
) E
(4,"
5' E
l1,
- 8s
. &:-
.. 0'
..i.:
N N
cp
ta. F
.0-
, %.
2 9
Pao
(i)F
1.1.
)4C
O11
3 IT
X tj
.1.
psF
ax: (
)E
-mai
l0
,j,13
;_ii
0 T
.-9
Si
Q.3
8 ?
(/10
Ca
coQ
., 6.
5o-
,;1
.,ui
LN2
rT,
Pho
ne: (
)0,
1I'
t.).-
--.
.9'
.-,
'4.
taC
l.4
..
V I
V 0
zr)
.S: 1
1,..;
dr,
,.c.
". 1
.O1
0.Is
,:,0.
1-,
Roo
ui
.....
c4
co_,
as
0::-
..H
ow d
id y
ou o
btai
n th
is T
IP?
0 W
as s
ent a
cop
y0
Ord
ered
from
NC
AD
Iui
al
---
-:-
CJ
O O
btai
ned
from
pro
fess
iona
l mee
ting
0 O
ther
,r R
ate
this
TIP
on
the
follo
win
g ch
arac
teris
tics:
The
TIP
is in
form
ativ
e.N
oI
The
TIP
is u
nder
stan
dabl
e.N
oI
The
TIP
is c
ompr
ehen
sive
.N
oI
The
TIP
is w
ell .
grou
nded
in r
esea
rch
and
scho
lars
hip.
No
I
this
TIP
will
be
usef
ul in
my
wor
k.N
oI
ra,..
..,
El.1 ..,
_,
23
45
Yes
ro
23
45
Yes
s...
23
45
Yes
g2
34
5Y
es
'23
45
Yes
How
will
you
use
this
Tip
? (c
heek
all
that
app
ly)
0 P
erso
nal r
efer
ence
0 A
udit
of p
ract
ice
stan
dard
s0
For
niaV
in-
serv
ice
trai
ning
0 C
omm
unity
edu
catio
n0
Oth
er
Wha
t top
ics
wou
ld y
ou s
ugge
st fo
r fu
ture
TIP
S?
ts)
r ' )
a. :
,.u,
NO
G-0
--1:
-: ir
6-IQ
r. g
..ri
03 (
L)
IV 0
(o
,,,n-
-lz
0..
01
--x
CE
Si's
-';'
'3
cpx
..:::.
Cl
or-
1...
.)D
.,.1
:1te
1`)
0F
.)N
to'
>4.
Is.)
..1.
-.)
cs. 0
,9ts
ar°
.
>c.
no
<O
ttcr
az
-1i..
n>0 71
i
cra
>or'T
.ri
l0
0to
..z...
-

SubstanceAbuseAmongOlderAdults
Treatment Improvement Protocol (TIP) Series
26Frederic C. Blow, Ph.D.Consensus Panel Chair
U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICESPublic Health ServiceSubstance Abuse and Mental Health Services AdministrationCenter for Substance Abuse Treatment
Rockwall II, 5600 Fishers LaneRockville, MD 20857
5

This publication is part of the Substance AbusePrevention and Treatment Block Grant technicalassistance program. All material appearing inthis volume except that taken directly fromcopyrighted sources is in the public domain andmay be reproduced or copied withoutpermission from the Substance Abuse andMental Health Services Administration's(SAMHSA) Center for Substance AbuseTreatment (CSAT) or the authors. Citation ofthe source is appreciated.
This publication was written under contractnumber ADM 270-95-0013. Sandra Clunies,M.S., I.C.A.D.C., served as the CSAT
Government project officer. Writers were PaddyCook, Carolyn Davis, Deborah L. Howard,Phyllis Kimbrough, Anne Nelson, Michelle Paul,Deborah Shuman, Margaret K. Brooks, Esq.,Mary Lou Dogoloff, Virginia Vitzthum, andElizabeth Hayes. Special thanks go to RolandM. Atkinson, M.D.; David Os lin, M.D.; Edith
6
Gomberg, Ph.D.; Kristen Lawton Barry, Ph.D.;Richard E. Finlayson, M.D.; Mary Smolenski,Ed.D., C.R.N.P.; Mary Lou Leonard; Annie
Thornton; Jack Rhode; Cecil Gross; Niyati
Pandya; Mark A. Meschter; and Wendy Carterfor their considerable contributions to thisdocument.
The opinions expressed herein are the views ofthe Consensus Panel members and do not reflectthe official position of CSAT, SAMHSA, or the
U.S. Department of Health and Human Services(DHHS). No official support or endorsement ofCSAT, SAMHSA, or DHHS for these opinions or
for particular instruments or software that maybe described in this document is intended orshould be inferred. The guidelines in thisdocument should not be considered substitutesfor individualized patient care and treatmentdecisions.
DHHS Publication No. (SMA) 98-3179Printed 1998

Contents
What Is a TIP? vii
Editorial Advisory Board ix
Consensus Panel xi
Foreword xiii
Executive Summaryand Recommendations xv
Alcohol Abuse xv
Abuse of Prescription Drugs xvi
Identification, Screening, and Assessment xvii
Treatment xix
Outcomes and Cost Issues in Alcohol Treatment xxii
Future Research xxiii
Chapter 1Substance Abuse Among Older Adults: An Invisible Epidemic 1
The Problem Projected 2
The Problem Now 3
Older Adults' Unique Vulnerabilities 5
Barriers To Identifying and Treating Older Adults With Substance Abuse Problems 5
Summary 10
Chapter 2Alcohol 13
Alcohol and Aging 13
Classifying Drinking Practices and Problems Among Older Adults 15
Drinking Patterns Among Older Adults 19
Risk Factors for Alcohol Abuse 22
Concomitant Substance Use 25
Chapter 3Use and Abuse of Psychoactive Prescription Drugs and Over-the-Counter Medications 29
Evolution of Psychoactive Prescribing 29
Patterns of Use 31
Risk Factors for Misuse and Abuse of Psychoactive Drugs 31
Adverse Effects 35
iii
7

Contents
Interactions With Other Drugs and With Alcohol 43
Chapter 4Identification, Screening, and Assessment 47
Screening for Alcohol and Prescription Drug Abuse 48Screening Instruments 53Communicating Positive Screening Results 53Communicating Negative Screening Results 56Assessment 56Special Assessments 57Moving the Older Adult Into Treatment 63
Chapter 5Referral and Treatment Approaches 65
Least Intensive Options 65Specialized Treatment of Older Problem Drinkers and Substance Abusers 68Levels of Treatment Services 69Program Philosophy and Basic Principles 73Treatment Approaches 77Specialized Treatment Issues for Prescription Drug Abuse 88Staffing Considerations 91
Chapter 6Outcomes and Cost Issues in Alcohol Treatment for Older Adults 95
Spectrum of Alcohol Treatment Outcomes 95Measurement of Multidimensional Outcomes for Older Adults 99Costs of Alcohol Treatment 102Reimbursement Issues in the Treatment of Older Adults 103Areas Requiring Future Research 104
Appendix ALegal and Ethical Issues 107
Autonomy and the Provider's Mission: A Dilemma 107Privacy and Confidentiality 108Conclusion 117Endnotes 118
Appendix BTools 121
The Alcohol Use Disorders Identification Test (AUDIT) 122Index of Activities of Daily Living (Index of ADLs) 129
Instrumental Activities of Daily Living (IADL) Scale 132
Geriatric Depression Scale (GDS) Short Form 134
The Center for Epidemiologic Studies Depression Scale (CES-D) 135Health Screening Survey (HSS), Revised 137
Appendix CBibliography 141
Appendix DResource Panel 169
Appendix EField Reviewers 171
iv

Contents
Figures1-1: Percentage Distribution of the U.S. Population by Age: 1995, 2010, 2025 3
2-1: DSM-IV Diagnostic Criteria for Substance Abuse 16
2-2: DSM-IV Diagnostic Criteria for Substance Dependence 17
2-3: Applying DSM-IV Diagnostic Criteria to Older Adults With Alcohol Problems 18
2-4: Clinical Characteristics of Early and Late Onset Problem Drinkers 21
3-1: Continuum of Psychoactive Prescription Drug Use 32
3-2: Effect of Aging on Response to Drug Effect 34
3-3: Commonly Prescribed Anxiolytics 36
3-4: Commonly Prescribed Sedative/Hypnotics 39
3-5: Commonly Prescribed Opiate/Opioid Analgesics 43
3-6: DrugAlcohol Interactions and Adverse Effects 44
4-1: Spokane's Gatekeeper Program 48
4-2: Physical Symptom Screening Triggers 49
4-3: The CAGE Questionnaire 53
4-4: Michigan Alcoholism Screening TestGeriatric Version (MAST-G) 55
4-5: Comparison of Dementia and Delirium: Characteristics and Causes 60
5-1: ASAM-PPC-2 Assessment Dimensions 70
5-2: Life Changes Associated With Substance Abuse in Older Adults 76
5-3: Treatment Objectives and Approaches 78
9

What Is a TIP?
Treatment Improvement Protocols (TIPs)
are best practice guidelines for thetreatment of substance abuse, provided
as a service of the Substance Abuse and MentalHealth Service Administration's Center forSubstance Abuse Treatment (CSAT). CSAT'sOffice of Evaluation, Scientific Analysis, andSynthesis draws on the experience andknowledge of clinical, research, andadministrative experts to produce the TIPs,which are distributed to a growing number offacilities and individuals across the country.The audience for the TIPs is expanding beyondpublic and private substance abuse treatmentfacilities as alcohol and other drug disorders areincreasingly recognized as a major problem.
The TIPs Editorial Advisory Board, adistinguished group of substance abuse expertsand professionals in such related fields asprimary care, mental health, and social services,works with the State Alcohol and Other DrugAbuse Directors to generate topics for the TIPsbased on the field's current needs forinformation and guidance.
After selecting a topic, CSAT invites staff
from pertinent Federal agencies and nationalorganizations to a Resource Panel thatrecommends specific areas of focus as well asresources that should be considered indeveloping the content of the TIP. Thenrecommendations are communicated to aConsensus Panel composed of non-Federalexperts on the topic who have been nominatedby their peers. This Panel participates in a series
of discussions; the information andrecommendations on which they reachconsensus form the foundation of the TIP. Themembers of each Consensus Panel representsubstance abuse treatment programs, hospitals,community health centers, counselingprograms, criminal justice and child welfareagencies, and private practitioners. A PanelChair (or Co-Chairs) ensures that the guidelinesmirror the results of the group's collaboration.
A large and diverse group of experts closelyreviews the draft document. Once the changesrecommended by these field reviewers havebeen incorporated, the TIP is prepared forpublication, in print and online. The TIPs can beaccessed via the Internet on the National Libraryof Medicine's home page at the URL:http: / /text.nlm.nih.gov. The move to electronicmedia also means that the TIPs can be updatedmore easily so they continue to provide the fieldwith state-of-the-art information.
Although each TIP strives to include anevidence base for the practices it recommends,CSAT recognizes that the field of substanceabuse treatment is evolving, and researchfrequently lags behind the innovationspioneered in the field. A major goal of each TIPis to convey "front-line" information quickly butresponsibly. For this reason, recommendationsproffered in the TIP are attributed to eitherPanelists' clinical experience or the literature. Ifthere is research to support a particularapproach, citations are provided.
10
vii

What Is a TIP?
This TIP, Substance Abuse Among Older
Adults, presents treatment providers with much-needed information about a population that isunderdiagnosed and underserved. Substanceabuse, particularly of alcohol and prescriptiondrugs, often goes undetected among adults over60 in part due to societal reasonsolder adultstend to be ashamed about drinking or drugproblems and see them as a moral failing.Providers, for their part, may confuse symptomsof substance use disorders with age-relatedchanges. Because so much of older adults'substance abuse is never even identified, thisTIP is aimed at not only substance abusetreatment providers but also primary careclinicians, social workers, senior center staff, and
viii11
anyone else who has regular contact with olderadults.
The TIP discusses the relationship betweenaging and substance abuse and offers guidanceon identifying, screening, and assessing not onlysubstance abuse but also disorders such asdementia and delirium that can mask or mimican alcohol or prescription drug problem.Practical accommodations to treatment for olderadults and a discussion of how to assessoutcomes and treat within a managed carecontext round out the document.
Other TIPs may be ordered by contacting the
National Clearinghouse for Alcohol and Drug
Information (NCADI), (800) 729-6686 or (301) 468-
2600; TDD (for hearing impaired), (800) 487-4889.

E itorial Advisory Board
Karen Allen, Ph.D., R.N., C.A.R.N.President of the National Nurses Society on
AddictionsAssociate ProfessorDepartment of Psychiatry, Community
Health, and Adult Primary CareUniversity of MarylandSchool of NursingBaltimore, Maryland
Richard L. Brown, M.D., M.P.H.
Associate ProfessorDepartment of Family MedicineUniversity of Wisconsin School of Medicine
Madison, Wisconsin
Dorynne Czechowicz, M.D.Associate DirectorMedical/Professional AffairsTreatment Research BranchDivision of Clinical and Services Research
National Institute on Drug AbuseRockville, Maryland
Linda S. Foley, M.A.
Former DirectorProject for Addiction Counselor TrainingNational Association of State Alcohol and
Drug DirectorsWashington, D.C.
Wayde A. Glover, M.I.S., N.C.A.C. II
DirectorCommonwealth Addictions Consultants and
TrainersRichmond, Virginia
12
Pedro J. Greer, M.D.Assistant Dean for Homeless EducationUniversity of Miami School of Medicine
Miami, Florida
Thomas W. Hester, M.D.Former State DirectorSubstance Abuse ServicesDivision of Mental Health, Mental
Retardation and Substance AbuseGeorgia Department of Human ResourcesAtlanta, Georgia
Gil HillDirectorOffice of Substance AbuseAmerican Psychological AssociationWashington, D.C.
Douglas B. Kamerow, M.D., M.P.H.
DirectorOffice of the Forum for Quality and
Effectiveness in Health CareAgency for Health Care Policy and Research
Rockville, Maryland
Stephen W. Long
DirectorOffice of Policy AnalysisNational Institute on Alcohol Abuse and
AlcoholismRockville, Maryland
Richard A. Rawson, Ph.D.Executive DirectorMatrix CenterLos Angeles, California
ix

Editorial Advisory Board
Ellen A. Renz, Ph.D.
Former Vice President of Clinical SystemsMEDCO Behavioral Care CorporationKamuela, Hawaii
Richard K. Ries, M.D.
Director and Associate Professor
Outpatient Mental Health Services and DualDisorder Programs
Harborview Medical CenterSeattle, Washington
x
11 3
Sidney H. Schnoll, M.D., Ph.D.
ChairmanDivision of Substance Abuse MedicineMedical College of VirginiaRichmond, Virginia

Consensus Panel
ChairFrederic C. Blow, Ph.D.
Assistant Professor and Assistant Research
ScientistDepartment of PsychiatryAlcohol Research CenterUniversity of MichiganAnn Arbor, Michigan
Workgroup LeadersRoland M. Atkinson, M.D.
ProfessorHead of Division of Geriatric PsychiatryDepartment of PsychiatrySchool of MedicineOregon Health Sciences UniversityPortland, Oregon
James Campbell, M.D., M.S.
Associate ProfessorActing ChairmanDepartment of Family MedicineCase Western Reserve UniversityMedical DirectorSenior Health Recovery ResourcesMetrohealth Medical CenterCleveland, Ohio
Anne M. Gurnack, Ph.D.Professor and Director of AssessmentDepartment of Political ScienceUniversity of Wisconsin at ParksideKenosha, Wisconsin
Jeanie L. Holt, R.N.C.
Clinical Staff NurseHeritage Home Health and HospiceMeredith, New Hampshire
David Os lin, M.D.
Assistant ProfessorAddiction and Geriatric PsychiatryDepartment of PsychiatryUniversity of PennsylvaniaPhiladelphia, Pennsylvania
Gerald D. Shulman, M.A., F.A.C.A.T.A.
ConsultantWinter Haven, Florida
PanelistsCharles Bearcomesout
Traditional CoordinatorTraditional ComponentNorthern Cheyenne Recovery CenterLame Deer, Montana
Larry W. Dupree, Ph.D.ProfessorDepartment of Aging and Mental HealthFlorida Mental Health InstituteUniversity of South FloridaTampa, Florida
xi

Consensus Panel
Richard E. Finlayson, M.D.
Consultant in Adult PsychiatryFormer Medical Director of Addiction
Services
Department of Psychiatry and PsychologyMayo Clinic
Associate Professor of PsychiatryMayo Medical SchoolRochester, Minnesota
Lissy F. Jarvik, M.D., Ph.D.
Distinguished Physician (11L)Psychiatry DepartmentWest Los Angeles VA Medical CenterProfessor Emerita
Department of Psychiatry and BiobehavioralSciences
University of California-Los AngelesLos Angeles, California
xii
15
Hi la Richardson, Dr.P.H.
Deputy DirectorMedical Research and Practice Policy
National Center on Addiction and SubstanceAbuse
Columbia UniversityNew York, New York
Marguerite T. Saunders, M.S.
Saunders Consulting ServicesAlbany, New York
Sharon L. Sheahan, Ph.D., C.F.N.P.
Associate Professor of NursingCollege of NursingUniversity of KentuckyLexington, Kentucky
Erma Polly Williams, M.R.E.
Program Support SpecialistRobert Wood Johnson Medical School
University of Medicine and Dentistry of NewJersey
New Brunswick, New Jersey

Foreword
The Treatment Improvement Protocol(TIP) series fulfills SAMHSA/CSAT'smission to improve treatment of
substance use disorders by providing bestpractices guidance to clinicians, programadministrators, and payers. TIPs are the resultof careful consideration of all relevant clinicaland health services research findings,demonstration experience, and implementationrequirements. A panel of non-Federal clinicalresearchers, clinicians, program administrators,and patient advocates debates and discussestheir particular area of expertise until they reacha consensus on best practices. This panel's workis then reviewed and critiqued by fieldreviewers.
The talent, dedication, and hard work thatTIPs panelists and reviewers bring to this highly
participatory process have bridged the gapbetween the promise of research and the needsof practicing clinicians and administrators. Weare grateful to all who have joined with us tocontribute to advances in the substance abusetreatment field.
Nelba Chavez, Ph.D.AdministratorSubstance Abuse and Mental Health
Services Administration
David J. Mactas
DirectorCenter for Substance Abuse TreatmentSubstance Abuse and Mental Health
Services Administration

Executive Summary andRecommendations
Researchers are only beginning to realizethe pervasiveness of substance abuseamong people age 60 and older. Until
relatively recently, alcohol and prescriptiondrug misuse, which affects as many as 17percent of older adults, was not discussed ineither the substance abuse or the gerontologicalliterature.
The reasons for this silence are varied:Health care providers tend to overlooksubstance abuse and misuse among olderpeople, mistaking the symptoms for those ofdementia, depression, or other problemscommon to older adults. In addition, olderadults are more likely to hide their substanceabuse and less likely to seek professional help.Many relatives of older individuals withsubstance use disorders, particularly their adultchildren, are ashamed of the problem andchoose not to address it. The result is thousandsof older adults who need treatment and do notreceive it.
This TIP brings together the literature onsubstance abuse and gerontology to recommendbest practices for identifying, screening,assessing, and treating alcohol and prescriptiondrug abuse among people age 60 and older. TheConsensus Panel, whose members includeresearchers, clinicians, treatment providers, andprogram directors, supplements this researchbase with its considerable experience treatingand studying substance abuse among older
adults. Because so much of older people'ssubstance abuse is never identified, this TIP isaimed not only at substance abuse treatmentproviders but also at primary care clinicians,social workers, senior center staff, and anyoneelse who has regular contact with older adults.
The TIP aims to advance the understandingof the relationships between aging andsubstance abuse and to provide practicalrecommendations for incorporating thatunderstanding into practice. The TIP'srecommendations appear below in italic type.Those based on research evidence are marked(1), whereas those based on Panel members'clinical experience are marked (2). Citationsfor the former can be found in the body of thetext.
Alcohol AbusePhysiological changes, as well as changes in thekinds of responsibilities and activities pursuedby older adults, make established criteria forclassifying alcohol problems often inadequatefor this population.
One widely used model for understandingalcohol problems is the medical diagnosticmodel as defined in the American PsychiatricAssociation's Diagnostic and Statistical Manual of
Mental Disorders, Fourth Edition (DSM-IV). TheDSM-IV criteria for substance dependence (seeFigure 2-2, p. 17) include some that do not apply
1 7

Executive Summary and Recommendations
to many older adults and may lead tounderidentification of drinking problems.
Diagnostic criteria for alcohol dependenceare subsumed within the DSM-IV's generalcriteria for substance dependence. Dependenceis defined as a "maladaptive pattern ofsubstance use, leading to clinically significantimpairment or distress, as manifested by three(or more) of the following, occurring at any timein the same 12-month period" (American
Psychiatric Association, 1994, p. 181).
The Panel recommends that clinicians consider
that the DSM-IV criteria for substance abuse and
dependence may not be adequate to diagnose older
adults with alcohol problems. (2) See Figure 2-3 (p.
18) for an outline of special considerations.
Some experts use the model of at-risk, heavy,and problem drinking in place of the DSM-IVmodel of alcohol abuse and dependence becauseit allows for more flexibility in characterizingdrinking patterns. In this classification scheme,an at-risk drinker is one whose patterns of alcohol
use, although not yet causing problems, maybring about adverse consequences, either to thedrinker or to others. As their names imply, theterms heavy and problem drinking signify more
hazardous levels of consumption. Although thedistinction between the terms heavy and problemis meaningful to alcohol treatment specialists
interested in differentiating severity of problemsamong younger alcohol abusers, it is lessrelevant to older adults. To differentiate older
drinkers, the Panel recommends using the terms at-
risk and problem drinkers only. (2) In the two-stage conceptualization recommended by thePanel, the problem drinker category includes
those who would otherwise fall into the heavyand problem classifications in the moretraditional model as well as those who meet theDSM-IV criteria for abuse and dependence.
The Consensus Panel recommends that older menconsume
N No more than one drink per day (1)
xvi 18
A maximum of two drinks on any drinking
occasion (e.g., New Year's Eve, weddings). (1)
The Panel recommends somewhat lower limits forwomen. (1)
Abuse of PrescriptionDrugsPeople 65 and older consume more prescribedand over-the-counter medications than anyother age group in the United States.
Prescription drug misuse and abuse is prevalentamong older adults not only because moredrugs are prescribed to them but also because,as with alcohol, aging makes the body morevulnerable to drugs' effects.
Any use of drugs in combination withalcohol carries risk; abuse of these substancesraises that risk, and multiple drug abuse raises iteven further. For example, chronic alcoholicswho use even therapeutic doses ofacetaminophen may experience severehepatoxicity. Alcohol can increase lithiumtoxicity and enhance central nervous systemdepression in persons taking tricyclic
antidepressants. High doses of benzodiazepinesused in conjunction with alcohol or barbituratescan be lethal. The many possible unfavorablereactions between prescription drugs andalcohol are summarized in Figure 3-6 (p. 44).
BenzodiazepinesBenzodiazepine use for longer than 4 months is not
recommended for geriatric patients. (2)
Furthermore, among the differentbenzodiazepines, longer acting drugs such asflurazepam (Dalmane) have very long half-livesand are more likely to accumulate than theshorter acting ones. They are also more likely toproduce residual sedation and such otheradverse effects as decreased attention, memory,cognitive function, and motor coordination, andincreased falls or motor vehicle crashes. Bycontrast, some shorter acting benzodiazepines

such as oxazepam (Serax) and lorazepam(Ativan) have very simple metabolic pathwaysand are not as likely to produce toxic ordependence-inducing effects with chronicdosing. Because of these side effects, the Panel
recommends caution in selecting the most
appropriate benzodiazepines for elderly patients. (2)
Sedative/HypnoticsAging changes sleep architecture, decreasing theamount of time spent in the deeper levels ofsleep (stages three and four) and increasing thenumber and duration of awakenings during thenight. However, these new sleep patterns donot appear to bother most medically healthyolder adults who recognize and accept that theirsleep will not be as sound or as regular as whenthey were young. Although benzodiazepinesand other sedative/hypnotics can be useful forshort-term amelioration of temporary sleepproblems, no studies demonstrate their long-term effectiveness beyond 30 continuous nights,
and tolerance and dependence develop rapidly.The Panel recommends that symptomatic treatment
of insomnia with medications be limited to 7 to 10
days with frequent monitoring and reevaluation if
the prescribed drug will be used for more than 2 to 3
weeks. Intermittent dosing at the smallest possible
dose is preferred, and no more than a 30-day supply
of hypnotics should be prescribed. (1)
The Panel further recommends that clinicians
teach older patients to practice good sleep hygiene
rather than prescribe drugs in response to insomnia.
(1) The former includes regularizing bedtime,restricting daytime naps, using the bedroomonly for sleep and sexual activity, avoidingalcohol and caffeine, reducing evening fluidintake and heavy meals, taking somemedications in the morning, limiting exerciseimmediately before retiring, and substitutingbehavioral relaxation technique's.
Executive Summary and Recommendations
AntihistaminesOlder persons appear to be more susceptible toadverse anticholinergic effects fromantihistamines and are at increased risk fororthostatic hypotension and central nervoussystem depression or confusion. In addition,antihistamines and alcohol potentiate oneanother, further exacerbating the aboveconditions as well as any problems with balance.Because tolerance also develops within days orweeks, the Panel recommends that older persons
who live alone do not take antihistamines. (1)
Identification, Screening,and AssessmentThe Consensus Panel recommends that every 60-
year -old should be screened for alcohol and
prescription drug abuse as part of his or her regular
physical examination. (2) However, problems candevelop after the screening has been conducted,and concurrent illnesses and other chronicconditions may mask abuse. Although no hard-and-fast rules govern the timing of screening, thePanel recommends screening or rescreening if certain
physical symptoms (detailed in Chapter 4) are
present or if the older person is undergoing major
life changes or transitions. (2)
Although it is preferable to use standardizedscreening questionnaires, friendly visitors,Meals-On-Wheels volunteers, caretakers, andhealth care providers also can interject screeningquestions into their normal conversations witholder, homebound adults. Although the line ofquestioning will depend on the person'srelationship with the older person and theresponses given, the Panel recommends that anyone
who is concerned about an older adult's drinking
practices try asking direct questions. (2) (Examples
of these and of less direct questions appear in
Chapter 4.)
19xvii

Executive Summary and Recommendations
The Panel recommends that health care providers
preface questions about alcohol with a link to a
medical condition when screening older people. (2)
For example, "I'm wondering if alcohol may bethe reason why your diabetes isn't respondingas it should," or "Sometimes one prescriptiondrug can affect how well another medication isworking. Let's go over the drugs you're takingand see if we can figure this problem out." Donot use stigmatizing terms like alcoholic or drugabuser during these encounters. (2)
Although it is important to respect the olderperson's autonomy, in situations where a
coherent response is unlikely, collateralparticipation from family members or friendsmay be necessary. In this case, the screener shouldfirst ask for the older adult's permission to question
others on his or her behalf. (2)
InstrumentsThe Panel recommends use of the CAGE
Questionnaire and the Michigan Alcohol Screening
TestGeriatric Version (MAST-G) to screen foralcohol use among older adults. (1)
The Alcohol Use Disorders Identification Test
(AUDIT) is recommended for identifying alcohol
problems among older members of ethnic minoritygroups. (2)
Assessment
Substance abuseThe Panel recommends a sequential approach that
looks at various dimensions of an older adult's
suspected problem in stages, so that unnecessarytests are not conducted. (1)
The Panelists recommend the use of two
structured assessments with older adults: the
substance abuse sections of the Structured Clinical
Interview for DSM-III-R (SCID) and the Diagnostic
Interview Schedule (DIS) for DSM-IV. (2)
FunctioningTo identify functional impairments, the Panelrecommends measuring the activities of daily living
xviii 20
(ADLs) and the instrumental activities of daily
living (IADLs) with the instruments in AppendixB. (1) Another useful instrument is the SF-36, a 36-item self-report questionnaire that measureshealth-related quality of life, including bothADLs and IADLs. (1)
Cognitive dysfunctionPatients who have been medically detoxified should
not be screened for cognitive dysfunction until
several weeks after detoxification is completed,
because a patient not fully recovered fromdetoxification may exhibit some reversiblecognitive impairment. (2)
The Panel recommends use of the
Orientation/Memory/Concentration Test (1), whichis simple and can be completed in the office. TheFolstein Mini-Mental Status Exam (MMSE) is anacceptable alternative (1), although it can beinsensitive to subtle cognitive impairments
among older problem drinkers who haverecently attained sobriety (past 30-60 days). TheMMSE is weak on visualspatial testing, whichis likely to show some abnormality in manyrecent heavy drinkers. The draw-a-clock task is a
good additional task to complement the MMSE. (1)
The Neurobehavioral Cognitive Status Examination,
which includes screening tests of abstract thinking
and visual memory (not measured on the MMSE), isalso recommended for assessing mental status in thispopulation. (1)
The Confusion Assessment Method (CAM) is
widely used as a brief, sensitive, and reliable
screening measure for detecting delirium. (I) The
Panel recommends that a positive delirium screen befollowed by careful clinical diagnostics based on
DSM-IV criteria and that any associated cognitive
impairment be followed clinically using the MMSE.(1)
Medical statusThe Panel recommends that initial medical
assessment of older persons should routinely include
screening for visual and auditory problems, and anyproblems discovered should be corrected as quickly as

possible. (2) To assess the medication use ofolder adults, the Panel recommends the "brown bag
approach." The practitioner can ask older adults to
bring every medication they take in a brown paper
bag, including over-the-counter and prescription
medications, vitamins, and herbs. (1)
Sleep disordersThe Panel recommends that sleep history be recorded
in a systematic way in order to both document the
changes in sleep problems over time and to heighten
the awareness of sleep hygiene. (2)
DepressionThe Geriatric Depression Scale (GDS) and the
Center for Epidemiological Studies DepressionScale (CES-D), reproduced in Appendix B, havebeen validated in older age groups although notspecifically in older adults with addictionproblems. The Panel recommends the CES-D for
use in general outpatient settings as a screen for
depression among older patients. (1)
TreatmentThe Consensus Panel recommends that the least
intensive treatment options be explored first with
older substance abusers. (1) These initial
approaches, which can function either aspretreatment strategy or treatment itself, arebrief intervention, intervention, andmotivational counseling. They may be sufficientto address the problem; if not, they can helpmove a patient toward specialized treatment.
The Consensus Panel recommends that everyreasonable effort be made to ensure that oldersubstance abusers, including problem drinkers,enter treatment. Brief intervention is therecommended first step, supplemented or followed by
intervention and motivational interviewing. (1)
Because many older problem drinkers areashamed about their drinking, interventionstrategies need to be nonconfrontational andsupportive.
Executive Summary and Recommendations
Conducting Brief InterventionsA brief intervention is one or more counselingsessions, which may include motivation forchange strategies, patient education, assessmentand direct feedback, contracting and goalsetting, behavioral modification techniques, andthe use of written materials such as self-helpmanuals. An older adult-specific brief intervention
should include the following steps (2):
1. Customized feedback on screening questionsrelating to drinking patterns and other healthhabits such as smoking and nutrition.
2. Discussion of types of drinkers in the UnitedStates and where the patient's drinkingpatterns fit into the population norms for hisor her age group.
3. Reasons for drinking. This is particularlyimportant because the practitioner needs tounderstand the role of alcohol in the contextof the older patient's life, including copingwith loss and loneliness.
4. Consequences of heavier drinking. Someolder patients may experience problems inphysical, psychological, or social functioningeven though they are drinking below cutofflevels.
5. Reasons to cut down or quit drinking.Maintaining independence, physical health,financial security, and mental capacity can bekey motivators in this age group.
6. Sensible drinking limits and strategies forcutting down or quitting. Strategies that areuseful in this age group include developingsocial opportunities that do not involvealcohol, getting reacquainted with hobbiesand interests from earlier in life, andpursuing volunteer activities, if possible.
7. Drinking agreement in the form of aprescription. Agreed-upon drinking limitsthat are signed by the patient and thepractitioner are particularly effective in
changing drinking patterns.
xix

Executive Summary and Recommendations
8. Coping with risky situations. Socialisolation, boredom, and negative familyinteractions can present special problems inthis age group.
9. Summary of the session.
If the older problem drinker does notrespond to the brief intervention, two otherapproachesintervention and motivationalinterviewingshould be considered.
InterventionIn an intervention, several significant people in asubstance-abusing patient's life confront thepatient with their firsthand experiences of his orher drinking or drug use. The formalizedintervention process includes a progressiveinteraction by the counselor with the family orfriends for at least 2 days before meeting withthe patient.
The Panel recommends the following
modifications to interventions for older patients. Nomore than one or two relatives or close associates
should be involved along with the health care
provider; having too many people present maybe emotionally overwhelming or confusing forthe older person. Inclusion of grandchildren is
discouraged, because many older alcoholics
resent their problems being aired in the presenceof much younger relatives. (2)
Motivational CounselingMotivational counseling acknowledgesdifferences in readiness and offers an approachfor "meeting people where they are" that hasproven effective with older adults. (1) Anunderstanding and supportive counselor listensrespectfully and accepts the older adult'sperspective on the situation as a starting point,helps him or her to identify the negativeconsequences of drinking and prescription drugabuse, helps him or her shift perceptions aboutthe impact of drinking or drug-taking habits,empowers him or her to generate insights aboutand solutions for his or her problem, and
xx
expresses belief in and support for his or hercapacity for change. Motivational counseling isan intensive process that enlists patients in theirown recovery by avoiding labels, avoiding
confrontation (which usually results in greaterdefensiveness), accepting ambivalence about theneed to change as normal, inviting clients toconsider alternative ways of solving problems,and placing the responsibility for change on theclient.
22
DetoxificationSome older patients should be withdrawn fromalcohol or from prescription drugs in a hospitalsetting. Medical safety and removal fromcontinuing access to alcohol or the abused drugsare primary considerations in this decision.
Indicators that inpatient hospital supervision is
needed for withdrawal from a prescription drug
include the following (2):
A high potential for developing dangerousabstinence symptoms such as a seizure ordelirium because the dosage of abenzodiazepine or barbiturate has beenparticularly high or prolonged and has beendiscontinued abruptly or because the patienthas experienced these serious symptoms atany time previouslySuicidal ideation or threatsThe presence of other majorpsychopathology
Unstable or uncontrolled comorbid medicalconditions requiring 24-hour care orparenterally administered medications (e.g.,renal disease, diabetes)
Mixed addictions, including alcoholA lack of social supports in the livingsituation or living alone with continuedaccess to the abused drug(s).
In general, the Panel recommends that the initialdose of a drug for suppression and management of
withdrawal symptoms should be one-third to one-half
the usual adult dose, sustained for 24 to 48 hours to

observe reactions, and then gradually tapered with
close attention to clinical responses. (1)
Treatment SettingsThe Panel recommends that patients who are brittle,
frail, acutely suicidal, or medically unstable or who
need constant one-on-one monitoring receive 24-hour
primary medical/psychiatric/nursing inpatient care
in medically managed and monitored intensive
treatment settings. (2)
As part of outpatient treatment, the Panelrecommends drawing the physician into the
treatment planning process and enrolling him or her
as a player in the recovery network. (2)
The Panel also recommends serving older people
who are dependent on psychoactive prescription
drugs in flexible, community-oriented programs with
case management services rather than in traditional,
stand-alone substance abuse treatment facilities with
standardized components. (2)
Treatment ApproachesThe Panel recommends incorporating the following
six features into treatment of the older alcohol abuser
(1):
Age-specific group treatment that issupportive and nonconfrontational and aimsto build or rebuild the patient's self-esteemA focus on coping with depression,loneliness, and loss (e.g., death of a spouse,retirement)A focus on rebuilding the client's socialsupport networkA pace and content of treatment appropriatefor the older personStaff members who are interested andexperienced in working with older adultsLinkages with medical services, services forthe aging, and institutional settings forreferral into and out of treatment, as well ascase management.
Building from these six features, theConsensus Panel recommends that treatment
programs adhere to the following principles (2):
Executive Summary and Recommendations
Treat older people in age-specific settingswhere feasibleCreate a culture of respect for older clientsTake a broad, holistic approach to treatmentthat emphasizes age-specific psychological,social, and health problemsKeep the treatment program flexibleAdapt treatment as needed in response toclients' gender.
To help ensure optimal benefits for olderadults, the Consensus Panel recommends that
treatment plans weave age-related factors into the
contextual framework of the American Society of
Addiction Medicine (ASAM) criteria. (2)
The Consensus Panel recommends the following
general approaches for effective treatment of older
adult substance abusers (2):
Cognitivebehavioral approachesGroup-based approachesIndividual counselingMedical/psychiatric approachesMarital and family involvement/familytherapyCase management/community-linkedservices and outreach.
The Panel recommends that cognitivebehavioral
treatment focus on teaching skills necessary for
rebuilding the social support network; self-
management approaches for overcoming depression,
grief, or loneliness; and general problem solving. (1)
Within treatment groups, the Panelrecommends that older clients should get more than
one opportunity to integrate and act on new
information. (2) For example, information onbereavement can be presented in an educationalsession, then reinforced in therapy. To helpparticipants integrate and understand material,it may be helpful to expose them to all units of
information twice. (2)
Older people in educational groups canreceive, integrate, and recall information betterif they are given a clear statement of the goaland purpose of the session and an outline of the
xxi

Executive Summary and Recommendations
content to be covered. The leader can post thisoutline and refer to it throughout the session.The outline may also be distributed for use inpersonal note-taking and as an aid in reviewand recall. Courses and individual sessions should
be conceived as building blocks that are added to the
base of the older person's life experience and needs.
Each session should begin with a review of previously
presented materials. (2)
Groups should accommodate clients' sensorydecline and deficits by maximizing the use of asmany of the clients' senses as possible. The Panelrecommends use of simultaneous visual and audible
presentation of material, enlarged print, voice
enhancers, and blackboards or flip charts. (2) It is
important to recognize clients' physicallimitations. Group sessions should last no longer
than about 55 minutes. The area should be well
lighted without glare; and interruptions, noise, and
superfluous material should be kept to a minimum.
(2)
The Panel recommends that counselors providing
individual psychotherapy treat older clients in a
nonthreatening, supportive manner and assure the
client that they will honor the confidentiality of the
sessions. (2)
Medications used to modify drinkingbehavior in older adults must take into accountage- and disease-related increases invulnerability to toxic drug side effects, as well aspossible adverse interactions with otherprescribed medications. Disulfiram (Antabuse) is
not generally recommended by the Panel for use in
older patients because of the hazards of the alcohol
disulfiram interaction, as well as the toxicity of
disulfiram itself (1) Of the other
pharmacotherapies for alcohol abuse, naltrexone(ReVia) is well tolerated by older adults andmay reduce drinking relapses. (1)
Depression for several days or longerimmediately after a prolonged drinking episodedoes not necessarily indicate a true comorbiddisorder or the need for antidepressanttreatment in most cases, but when depressive
24
symptoms persist several weeks following cessation of
drinking, specific antidepressant treatment is
indicated. (1)
The advantages of quitting smoking areclear, even in older adults. The Panel recommends
that efforts to reduce substance abuse among older
adults also include help in tobacco smoking cessation.
Staffing ConsiderationsThe Consensus Panel recommends that the following
principles guide staffing choices in substance abuse
treatment programs (2):
Whenever possible, employ staff who havecompleted training in gerontologyEmploy staff who like working with olderadultsProvide training in empirically demonstratedprinciples effective with older adults to allstaff who will interact with these clients.
Panel members believe that any programthat treats even a few older adults should haveat least one staff person who is trained in thespecialization of gerontology within his or herdiscipline. This training should consist of atleast a graduate certificate program (6- to 12-month) in the subfield of aging commonly calledsocial gerontology. Staff with professionaldegrees should have a specialization ingerontology, geriatrics, or psychogeriatrics.
Outcomes and Cost IssuesIn Alcohol TreatmentOutcome assessment is invaluable from both amanagement and a referral perspective. Theproviders of treatment, the clinicians andagencies referring patients, and patientsthemselves need to have information regardingthe likely outcomes of treatment. Becausetreatment options range from brief interventionsto structured outpatient and inpatient treatmentprograms, the Panel recommends evaluation of
outcomes at varying points in the treatment process.

(1) Baseline data should be obtained at thebeginning of the intervention or treatment; firstfollowup evaluations should be conducted 2weeks to 1 month after the patient leaves theinpatient setting. The literature on patientsreceiving substance abuse treatment indicatesthat 60 to 80 percent of people who relapse do sowithin 3 to 4 months. Therefore, outpatientoutcomes should be assessed no sooner than 3 months
and possibly as long as 12 months after treatment.
(1)
The Panel recommends that outcome
measurement include not only abstinence or reduced
consumption but also patterns of alcohol use, alcohol-
related problems, physical and emotional health
functioning, and quality of life and well-being. (1)
One of the most widely used measures ofphysical and emotional health is the MedicalOutcomes Study 36-Item Short Form HealthSurvey (SF-36). (1) Another measure ofpsychological distress useful for alcoholoutcomes assessment with older adults is theSymptom Checklist-90-Revised (SCL-90-R) and
its abbreviated version, the Brief SymptomInventory (BSI). (1) For measuring quality of life,
Executive Summary and Recommendations
an important measure for older adults with alcohol
problems, the Panel recommends the Quality of Life
Interview (QLI). (1)
Future ResearchThe Panel believes that future research needs tobe focused in some specific areas to advance thefield and to address future problems that willarise in the coming years. Those areas are alcohol
and other drug consumption, treatment, biomedical
consequences, behavioral and psychological effects,
and special issues. (1)
This TIP lays a foundation that research inthe above areas must build upon if providers areto meet the treatment challenges on the horizon.In particular, providers must prepare forchanges in demographics and in treatmentdelivery. As the country's over-60 populationexplodes and the health care system shifts tomanaged care, providers must adjustaccordingly. The treatment protocols outlinedin this book provide a roadmap for treating thisunique and growing population into the nextcentury.
23

1 Substance Abuse Among OlderAdults: An Invisible Epidemic
Substance abuse, particularly of alcoholand prescription drugs, among adults 60and older is one of the fastest growing
health problems facing the country. Yet, even asthe number of older adults suffering from thesedisorders climbs, the situation remainsunderestimated, underidentified,underdiagnosed, and undertreated. Untilrelatively recently, alcohol and prescriptiondrug misuse, which affects up to 17 percent ofolder adults, was not discussed in either thesubstance abuse or the gerontological literature(D'Archangelo, 1993; Bucholz et al., 1995;
National Institute on Alcohol Abuse andAlcoholism, 1988; Minnis, 1988; Atkinson, 1987,
1990).
Because of insufficient knowledge, limitedresearch data, and hurried office visits, healthcare providers often overlook substance abuseand misuse among older adults. Diagnosis maybe difficult because symptoms of substanceabuse in older individuals sometimes mimicsymptoms of other medical and behavioraldisorders common among this population, suchas diabetes, dementia, and depression. Oftendrug trials of new medications do not includeolder subjects, so a clinician has no way ofpredicting or recognizing an adverse reaction orunexpected psychoactive effect.
Other factors responsible for the lack ofattention to substance abuse include the currentolder cohort's disapproval of and shame about
use and misuse of substances, along with areluctance to seek professional help for whatmany in this age group consider a privatematter. Many relatives of older individuals withsubstance use disorders, particularly their adultchildren, are also ashamed of the problem andchoose not to address it. Ageism also contributesto the problem and to the silence: Youngeradults often unconsciously assign differentquality-of-life standards to older adults. Suchattitudes are reflected in remarks like,"Grandmother's cocktails are the only thing thatmakes her happy," or "What difference does itmake; he won't be around much longeranyway." There is an unspoken but pervasiveassumption that it's not worth treating olderadults for substance use disorders. Behaviorconsidered a problem in younger adults doesnot inspire the same urgency for care amongolder adults. Along with the impression thatalcohol or substance abuse problems cannot besuccessfully treated in older adults, there is theassumption that treatment for this population isa waste of health care resources.
These attitudes are not only callous, they reston misperceptions. Most older adults can anddo live independently: Only 4.6 percent ofadults over 65 are nursing home or personalhome care residents (Altpeter et al., 1994).Furthermore, Grandmother's cocktails aren'tcheering her up: Older adults who "self-medicate" with alcohol or prescription drugs are
21

Chapter 1
more likely to characterize themselves as lonelyand to report lower life satisfaction (Hendrickset al., 1991). Older women with alcoholproblems are more likely to have had a problem-drinking spouse, to have lost their spouses todeath, to have experienced depression, and tohave been injured in falls (Wilsnack andWilsnack, 1995).
The reality is that misuse and abuse ofalcohol and other drugs take a greater toll onaffected older adults than on younger adults. Inaddition to the psychosocial issues that areunique to older adults, aging also ushers inbiomedical changes that influence the effectsthat alcohol and drugs have on the body.Alcohol abuse, for example, may accelerate thenormal decline in physiological functioning thatoccurs with age (Gambert and Katsoyannis,1995). In addition, alcohol may elevate olderadults' already high risk for injury, illness, andsocioeconomic decline (Tarter, 1995).
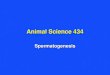
The Problem ProjectedIt will be increasingly difficult for older adults'substance abuse to remain a hidden problem asthe demographic bulge known as the BabyBoom approaches old age early in the nextcentury. Census estimates predict that 1994'solder adult population of 33 million will morethan double to 80 million by 2050 (Spencer, 1989;U.S. Bureau of the Census, 1996). Most of thatgrowth will occur between 2010 and 2030, whenthe number of adults over 65 will grow by anaverage of 2.8 percent annually (U.S. Bureau ofthe Census, 1996). In 1990, 13 percent ofAmericans were over 65; by 2030, that bloc willrepresent 21 percent of the population (U.S.Bureaus of the Census, 1996). The demographicincreases among older adults are summarizedbelow and in Figure 1-1.
Life expectancy in the United States hasincreased. In 1950, it was 68 years, and by 1991,it had reached 79 years for women and 72 years
2 27
for men (U.S. Bureau of the Census, 1996). Notonly are adults in general living longer,substance abusers are also living longer thanever before (Gomberg, 1992b). Thus, moreAmericans face chronic, limiting illnesses orconditions such as arthritis, diabetes,osteoporosis, and senile dementia, becomingdependent on others for help in performingtheir activities of daily living (U.S. Bureau of theCensus, 1996).
Alcohol use was less common in the 1930s,1940s, and 1950s than it has been since the 1960s.Many of those who are now 60 and older,influenced by prevailing cultural beliefs andProhibition, never drank at all, and a negligiblenumber used illicit drugs. Younger birthcohorts in this century tend to have increasinglyhigher rates of alcohol consumption andalcoholism (Atkinson et al., 1992). Thus, "theprevalence of alcohol problems in old age mayincrease, especially among women, for birthcohorts entering their 60s in the 1990s andbeyond"(Atkinson and Ganzini, 1994, p. 302). Arecent study in Sweden found that the male-to-female ratio among older alcohol abusersadmitted for addiction treatment decreasedfrom 7.8:1 to 3.4:1 in the span of a decade
(Osterling and Berglund, 1994).Because there is a clear relationship between
early alcohol problems and the development ofalcohol problems in later life, drinking amongolder adults is likely to become an even greaterproblem in the near future (Rosin and Glatt,1971; Gomberg, 1992; Zimberg, 1974; Helzer et
al., 1991a; Beresford, 1995a). Liberto andcolleagues concluded that the overall increase inalcOhol problems throughout the population,coupled with the aging of the Baby Boomers,suggests that the number of older adults withalcohol-related problems will rise alarmingly(Liberto et al., 1992). Taken together, thesefactors raise the prospect of tomorrow's healthservices facing a "potentially preventable 'tide'of alcohol-induced morbidity" (Saunders, 1994,

p. 801). Further research is needed on thephysiological effects of marijuana on olderadults, because many children of the 1960s canbe expected to carry this habit into old age.
The Problem NowHealth care and social service providers whocurrently care for Americans age 60 and older
Substance Abuse Among Older Adults
will mainly encounter abuse or misuse ofalcohol or prescribed drugs. Abuse of heroinand other opioids is rare, although some olderadults misuse over-the-counter drugs that havea high alcohol content, such as coughsuppressants. Many of these over-the-counterdrugs negatively interact with other medicationsand alcohol.
Figure 1-1Percentage Distribution of U.S. Population by Age:1995, 2010, and 2025
60
50
40
b.0
30
P-1
20
10
Under 20 Years
Source: U.S. Censits Bureau, 1996
Year01995
02010
IN2025
20-64 Years 65 Years and Over
3

Chapter 1
Alcohol Disorders: Older Adults'Major Substance Abuse ProblemProblems stemming from alcohol consumption,including interactions of alcohol with prescribedand over-the-counter drugs, far outnumber anyother substance abuse problem among olderadults. Community prevalence rates range from3 to 25 percent for "heavy alcohol use" and from2.2 to 9.6 percent for "alcohol abuse" dependingon the population sampled (Liberto et al., 1992).(Chapter 2 defines levels of use and adjuststhem for older adults.) A recent study foundthat 15 percent of men and 12 percent of womenage 60 and over treated in primary care clinicsregularly drank in excess of limitsrecommended by the National Institute onAlcohol Abuse and Alcoholism (i.e., no morethan one drink per day) (Saunders, 1994; Adamset al., 1996; National Institute on Alcohol Abuseand Alcoholism, 1995).
The differences in the prevalence rates aboveillustrate the difficulty in identifying howwidespread the current problem is. Oneresearcher suggests that alcohol abuse amongolder adults is easily hidden, partly because ofits similarities to other diseases common as oneages and partly because elders remind cliniciansof a parent or grandparent (Beresford, 1995b).Recent studies in Australia (McInnes andPowell, 1994) and a corroboration of similar datafrom the United States (Curtis et al., 1989) foundthat clinicians recognized alcoholism in onlyone-third of older hospitalized patients who hadthe disorder. Furthermore, many of the signsand symptoms of alcohol abuse among youngerpopulations do not apply to older adults: Mostolder adults are no longer in the work force,have smaller social networks, and drive less(reducing the potential for being recognized asabusing alcohol).
Chapter 2 details drinking practices andproblems among older adults. Identification,screening, and assessment of alcohol and drug
4
29
usespecifically targeted to this populationare discussed in Chapter 4.
Prescription DrugsThe abuse of narcotics is rare among olderadults, except for those who abused opiates intheir younger years (Jinks and Raschko, 1990).Prescribed opioids are an infrequent problem aswell: Only 2 to 3 percent of noninstitutionalizedolder adults receive prescriptions for opioidanalgesics (Ray et al., 1993), and the vastmajority of those do not develop dependence.One study, for example, found that only 4 ofnearly 12,000 patients who were prescribedmorphine for self-administration becameaddicted (Hill and Chapman, 1989). The use ofillicit drugs is limited to a tiny group of agingcriminals and long-term heroin addicts (Myerset al., 1984). Although little publishedinformation exists, Panelists report that a fargreater concern for drug misuse or abuse is thelarge number of older adults using prescriptiondrugs, particularly benzodiazepines, sedatives,and hypnotics, without proper physiciansupervision (Gomberg, 1992). Older patients areprescribed benzodiazepines more than any otherage group, and North American studiesdemonstrate that 17 to 23 percent of drugsprescribed to older adults are benzodiazepines(D'Archangelo, 1993). The dangers associatedwith these prescription drugs includeproblematic effects due to age-related changes indrug metabolism, interactions amongprescriptions, and interactions with alcohol.
Unfortunately, these agents, especially thosewith longer half-lives, often result in unwantedside effects that influence functional capacityand cognition, which place the older person atgreater risk for falling and forinstitutionalization (Roy and Griffin, 1990).Older users of these drugs experience moreadverse effects than do younger adults,including excessive daytime sedation, ataxia,and cognitive impairment. Attention, memory,

physiological arousal, and psychomotor abilitiesare often impaired as well (Pomara et al., 1985),and drug-related delirium or dementia maywrongly be labeled Alzheimer's disease. Misuseof psychoactive prescription drugs is discussedin Chapter 3.
Older Adults' UniqueVulnerabilitiesFor the purposes of this TIP, an older adult isdefined as a person age 60 or older. Any agecutoff is somewhat arbitrary because age-relatedchanges vary tremendously across individualsand even within one person from body systemto body system. An 80-year-old can have betterhealth functioning than a 50-year-old, and a 70-year -old can have "the spine of an 80-year-old, aheart typical of a 60-year-old, and a centralnervous system equal in functioning to anaverage 60-year-old" (Altpeter et al., 1994, p. 30).Although some recommendations in this TIPmay apply more to adults 70 and older, some ofthe age-related changes that affect the body'sreactions to alcohol and other drugs begin asearly as 50.
The age at which such changes occur variesfrom person to person, but invariably they dooccur. Because many of the definitions, models,and classifications of alcohol consumption levelsare static and do not account for age-relatedphysiological and social changes, they simply donot apply to older adults. Drinking can be
medically hazardous for this group even if thefrequency and amount of consumption do notwarrant a formal diagnosis of alcohol abuse ordependence. Weekly quantity of drinking levelscan only serve as a rough parameter in thispopulation; it is crucial for providers to viewolder drinkers and drug-takers as on a spectrumand to resist placing them into rigid categoriesfor purposes of assessment and treatment.(Diagnosis, however, may require use of those
Substance Abuse Among Older Adults
classifications, as they often are the basis forreimbursement.)
Chapter 2 examines classifications such as at-risk, problem, and dependent alcohol consumption
patterns, which have been the focus of majordiagnostic systems, particularly the Diagnosticand Statistical Manual of Mental Disorders, Fourth
Edition (DSM-IV) (American Psychiatric
Association, 1994), and reconfigures them to suitolder adults' unique responses to andexperiences with alcohol and drug use.
Further complicating treatment of oldersubstance abusers is the fact that they are morelikely to have undiagnosed psychiatric and
medical comorbidities. According to one study,30 percent of older alcohol abusers have aprimary mood disorder (Koenig and Blazer,1996). A thorough evaluation of all problems isessential when caring for older adults: Failureto do so will undoubtedly increase the numberof false diagnoses and diminish the quality ofolder patients' lives (Gomberg, 1992). Physicaland mental comorbidities are discussed in detailin Chapter 4.
Barriers To IdentifyingAnd Treating OlderAdults With SubstanceAbuse ProblemsThe sheer number and the interconnectedness ofolder adults' physical and mental healthproblems make diagnosis and treatment of theirsubstance abuse more complex than for otherpopulations. That complexity contributesdirectly or indirectlyto the following barriersto effective treatment:
AgeismLack of awarenessClinician behaviorComorbidity.
305

Chapter 1
6
AgeismThe term ageism was coined in the mid-1960s(Butler, 1969) to describe the tendency of societyto assign negative stereotypes to older adultsand to explain away their problems as a functionof being old rather than looking for specificmedical, social, or psychological causes. InAmerican culture, ageism reflects a personalrevulsion about growing old, comprising in partfear of powerlessness, uselessness, and death.Older adults often internalize such stereotypesand thus are less likely to seek out mental healthand substance abuse care (Patterson andDupree, 1994). Ageism may result in an olderadult being classified as "senile," when in realityhe or she may be afflicted with specific andsometimes treatable comorbid conditions suchas Alzheimer's disease, depression, multi-infarctdementia, and alcoholism.
Not only is a younger adult with comorbidconditions more likely to receive a correctdiagnosis for substance abuse, but a youngerpatient diagnosed with, say, hypertension, willmore likely be examined for underlyingetiologies, including substance abuse. Witholder adults, providers often do not look beyondthe presenting problem for which the patient isseeking care (Curtis et al., 1989). Despitecaregivers' good intentions, instances of ageismalso occur in congregate meal settings and in theprovision of homemaker services to thehomebound. Changes in eating habits, forexample, may not be explored because "olderpeople get fussy about their food." Confusion inolder adults may go unchallenged because homehealth aides attribute it to "a bad night" or age-related "spaciness." Older patients aresignificantly less likely to have substance abuseproblems identified during routine medical care.If a diagnosis of substance abuse is made, anolder patient is less likely to have treatmentrecommended (Curtis 'et al., 1989).
Ageism is reflected in some providers' beliefthat older adults' quality of life will remain poor
31
even if they are successfully treated for theirsubstance abuse. Such lowered expectationsmay also be compounded by "therapeuticnihilism": Older substance abusers may bedeemed not worthy of the effort involved intreating or changing behavior because "they arelikely to die soon anyway."
Lack of AwarenessA second barrier to treatment is a lack ofawareness of the problem that is often shared bythe older substance abuser, his or her lovedones, the community, and society as a whole. Alack of awareness or denial of the signs ofalcohol abuse (more common among olderadults), combined with the personal orcommunity-specific stigma of the disease, mayeffectively raise one or more barriers totreatment.
Stigma, shame, or denial associated withsubstance abuse may be related to generation,religion, gender, culture, or a combination ofthese and other factors. Many older adultsformed their attitudes about alcohol before the1950s, when advertising and wider accessibilityhelped change the use of alcohol from a moralfailing to an accoutrement of postwarprosperity. If adults attribute their alcoholproblems to a breakdown in morals, they are notlikely to seek substance abuse treatment.
Many older adults are also very sensitive tothe stigma associated with psychiatric disorders.They are much more willing to accept a medicaldiagnosis than a mental or psychiatric one, andthey may translate this bias into a reluctance todescribe mood disturbances or to acknowledgesymptoms that might be interpreted asmanifestations of weakness, irresponsibility, or"craziness." They may genuinely think manyproblems are simply related to old age or bereluctant to complain too much (Weiss, 1994). Inaddition, many older adults do not accept thatalcohol- or other drug-related disorders arehealth care problems or diseases.

It may be difficult for other adults toconceive of an older person, especially a woman,as having problems with alcohol or othersubstances. This particular limitation can betrue of an alcohol abuser's daughter or of anentire community, which may have decided thatalcoholism is a youth problem. Drinking amongolder adults is often perceived as a pleasure theyhave earned and, lacking work and familyresponsibilities, should be allowed to enjoy:Because social drinking is an acceptablebehavior, it can serve to mask a more seriousdrinking problem.
Clinicians' and ServiceProfessionals' BehaviorHealth care and older adult service providersmay be as slow to spot a substance abuseproblem as everyone else is: Despite itsfrequency, there is often a low index ofsuspicion for this problem. Even when there isthe suspicion of a substance abuse disorder, thepractitioner may have difficulty applying thediagnostic criteria to a wide variety ofnonspecific symptoms. With a younger patient,serious physical problems (e.g., heart disease,diabetes) can be more easily ruled out, leadingquickly to a diagnosis of substance abuse in thepresence of certain symptoms. With an olderpatient, health care providers are often in aquandarysymptoms such as fatigue,irritability, insomnia, chronic pain, or impotencemay be produced or influenced by substanceabuse, common medical and mental disorders,or a combination of these conditions. Anotherclinician barrier to diagnosing alcohol problemsin older adults is stereotyping. Clinicians areless likely to detect alcohol problems in women,the educated, and those with highersocioeconomic status (Moore et al., 1989).
Other barriers related to clinician behaviorare noted in the literature. Keeler andcolleagues studied the effect of patient age andlength of physician encounter. They found that
Substance Abuse Among Older Adults
the amount of time physicians spend with apatient decreases as the age of the patientincreases (Keeler et al., 1982). (Obviously, this isnot due to older patients' having fewer medicalcomplaints.) It is unlikely that abbreviated officevisits are sufficient to identify an older adult'sunderlying problem with alcoholism.
Not only do the physician encountersbecome shorter, but problems related to alcoholand drugs increasingly compete for discussiontime against other health problems. During ashort office visit, there are many topics to coverin patient-provider discourse, ranging fromrenewal of multiple prescriptions to the impactof the death of a spouse. Substance abuse oftenends up at the bottom of the list or is notconsidered at all when a patient presents withmany medical or personal problems. Providers,older patients, and family members typicallyplace higher priority on physical conditionssuch as heart problems and renal failure than onalcohol abuse.
Providers may also believe that oldersubstance abusers do not benefit from treatmentas much as younger patients, despite studiesthat have dispelled this persistent myth.Research indicates that, compared with youngerpatients, older adults are more likely tocomplete treatment (Linn, 1978; Cartensen et al.,1985) and have outcomes that are as good as orbetter than those of younger adults (Kashner etal., 1992; Atkinson, 1995; in press). Yet healthcare providers still need more education aboutsubstance abuse treatment options and successrates (see Chapter 6).
Clinicians may not know that certain drugsare habit-forming or about specific druginteractions and side effects. One diagnosticbarrier is that many physicians believealcoholics must be heavy drinkers and oftenmiss the opportunity to intervene because theirdefinition of problem drinking rests on amountsand frequencies that do not apply to olderadults (see Chapter 2). Those treating older
32 7

Chapter 1
8
substance abusers should receive training ondrug-to-drug interaction, drug-to-diseaseinteraction, drug-to-alcohol interaction, andalcohol-to-disease interaction (discussed inChapters 2 and 3).
ComorbidityMedical and psychiatric comorbidities presentyet another challenge to the effective treatmentof the older substance abuser. Comorbidconditions such as medical complications,cognitive impairment, mental disorders such asmajor depression, sensory deficits, and lack ofmobility not only can complicate a diagnosis butcan sway the provider from encouraging olderpatients to pursue treatment for their substanceabuse problems. For example, older patientswho cannot walk up stairs or drive after darkmay not be encouraged to attend eveningAlcoholics Anonymous (AA) meetings. Olderpatients may also be screened out of treatmentprograms because of poor cognitive tests orsimply because health professionals do not thinkthey will benefit. In addition, treatmentprograms may be reluctant to accept them ormay not have the facilities to accommodate theirspecial needs. Comorbid depression andanxiety pose other barriers. Although inpatientpsychiatric hospitals generally have staff trainedto treat dually diagnosed patients, outpatientprograms may not. These programs may notaccept medicated older adults with mentaldisorders.
Special PopulationsWomen, minorities, and those who arehomebound, including adults with physicaldisabilities, confront more specific barriers totreatment.
WomenAlthough women constitute the majority ofolder adults, their treatment challenges areconsidered here in part because most of theresearch in the substance abuse field has studied
33
male subjects. In 1994, among adults 65 to 69,there were 82 men for every 100 women.
Among those 85 to 89, there were 44 men forevery 100 women, and the disparity is evengreater for those 90 and older (U.S. Bureau ofthe Census, 1996). Despite women's greaternumbers, they constitute the minority of oldersubstance abusers. There are, however, moreolder women living alone, and their substanceabuse can be difficult to identify (Moore et al.,1989). Older women as a group conceal theirdrinking or drug use vigilantly because theirstigma is greater than that for men. Othertreatment obstacles particular to women includethe following:
Compared with men, women have lessinsurance coverage and supplementalincome (such as a pension). Women are lesslikely to have worked, more likely to loseinsurance coverage with the death of aspouse, and more likely to live in poverty.Women drink less often in public places andare therefore less likely to drive whileintoxicated or engage in other behaviors thatmight reveal an alcohol problem.Many older women never learned to drive,and they are more likely to live at homealone. Overall, women are healthier andmore independent but are also more isolated.They often drink alone.Older women are prescribed more andconsume more psychoactive drugs,particularly benzodiazepines, than are menand are more likely to be long-term users ofthese substances (Gomberg, 1995).
Racial and ethnic minoritiesAlthough little research has been done on olderminority populations, the Panelists agreed thatolder minority individuals also face barriers totreatment. Recent data suggest that oldermembers of minority groups, particularlyAfrican-Americans, may be more vulnerable to

late-life drinking than previously thought(Gomberg, 1995).
For many older minority adults in urbanareas, health care is delivered in busy hospitaloutpatient departments or in emergency rooms.These settings further diminish the likelihoodthat alcohol and other drug issues will beaddressed.
Language is another major issue inidentifying and treating substance abuse amongminority elders because many of them werefirst-generation immigrants who never learnedEnglish. In order to access services, thesepatients need an interpreter or a family memberwho can serve as an interpreter. This raises anadditional issue: Interpreters can biascommunications, adding yet another barrier toeffective treatment.
Non-English-speaking minorities have alsobeen at a disadvantage in treatment and therapyin many areas of the country. Culturalcompetence is crucial when the treatmentprovider has a different ethnic or culturalbackground than the client. The clinician needssome knowledge of the belief systems of theclient to effectively interview and interpretresponses from, for example, Native Americans.Although some progress has been made inproviding culturally appropriate prevention andtreatment programs for the Hispanicpopulation, much less is available for othercultural or linguistic minorities, such as EasternEuropeans and Asians.
Homebound older adultsThe barriers that prevent identification andtreatment of substance abuse among all olderadults are even greater for the homebound,particularly comorbidities, transportation andhandicapped accessibility, isolation, and gender(over 70 percent of home care patients arewomen [Dey, 1996]).
Older adults are often restricted to theirhomes by an array of health problems that limittheir mobility. Heart disease, diabetes, chronic
Substance Abuse Among Older Adults
lung diseases, and other conditions diminisholder adults' ability to perform the basicactivities of daily living, making it less likelythey will seek treatment for their substanceproblems. Adults bound to their homes byphysical disabilities are at particularly high riskfor alcoholism.
The weakness and frail physical condition ofmany homebound older adults also limitmobility and transportation options beyond theproblems faced by older adults in general. Bydefinition, homebound older adults cannot getout of their homes without "considerable andtaxing effort" and almost always require theassistance of another person (Health CareFinancing Administration, 1997). In practicalterms, this means these older adults cannotdrive or take public transportation, taxicabs, orrides from friends who are also frail. They mustdepend on able-bodied others, who they maynot want to bother in nonemergency situations.Such dependency can be embarrassing anddepressing, which may trigger alcohol or druguse.
Finally, homebound older adults are oftenvery isolated socially. Limited contacts withothers may allow serious abuse to goundetected. Lack of a social support networkmakes these older adults even more susceptibleto depression and despair.
Other Barriers to Identification andTreatmentOther barriers to treatment in the olderpopulation are
Transportation (may be available to go to a
hospital but not to AA or aftercare orevening programs): This is especiallyproblematic in rural communities that lackpublic transportation or in poor urbancommunities where accessing transportationcan be dangerous (Fortney et al., 1995).
34 9

Chapter 1
m Shrinking social support network: Fewer
friends to support them, participate in thetreatment process, or take them places.
m Time: Despite the assumption that olderadults have an excess of free time, they maywell have to provide 24-hour supervision toa spouse, other relative, or friend, or have tocare for grandchildren while the parentworks.
in Lack of expertise: Few programs have
specialists in geriatrics, treat many olderadults, or are designed to accommodatefunctional disabilities such as hearing loss orambulation problems.
g Financial: The structure of insurance policiescan be a barrier to treatment. The carvingout of mental health services from physicalhealth services under managed care inparticular can prevent older adults fromreceiving inpatient substance abusetreatment.
Because of the increased potential forenhanced reactions to alcohol and to alcohol incombination with other drugs, it is importantthat clinicians, family members, and socialservice providers be on the lookout for signs ofproblems. Communities can implement"gatekeeper" systems, wherein meter readers,credit office workers, repair personnel, postalcarriers, police, apartment managers, and otherswatch for and report signs of depression andother psychiatric disorders (often exacerbated bysubstance abuse) (see Chapter 4). Suggestionsfor who can help move older adults intotreatment and various treatment approaches arediscussed in Chapter 5.
SummaryGiven the scope of the problem, the literature onsubstance abuse problems among older adults issurprisingly sketchy. Substance abuse amongolder adults as a distinct subgroup withdefinable characteristics was first described in
10
37
the research literature in 1964 (Droller, 1964).
Researchers in the 1960s and 1970s wereconvinced that substance abuse was rare amongolder adults (Atkinson and Ganzini, 1994).Thus, researchers and clinicians alike widelybelieved that substance use disorders amongthis age group did not merit the attention givento drinking and drug abuse among youngeradults (Bucholz et al., 1995).
Most professional service providers thoughtthat lifelong alcohol- and other drug-addictedindividuals either died early or recoveredspontaneously, "maturing out" of theirproblems (Saunders, 1994; Vaillant et al., 1983).Older drinkers tended to be viewed "merely assurvivors of a long, dissolute history of heavyalcohol use followed by predictably poor healthand early demise" (Beresford, 1995b, p. 3), andalcoholism was considered predominantly amale problem, affecting four males for everyfemale (Bucholz et al., 1995). Therefore, thetypical older adult with a drinking problem wasconsidered most often to be a man with a longhistory of drinking. Even as recently as 1987,the Diagnostic and Statistical Manual of Mental
Disorders, Third Edition, Revised (DSM-III-R), the
standard diagnostic manual the AmericanPsychiatric Association used at that time, stated,"In males, symptoms of alcohol dependence orabuse rarely occur for the first time after age 45"(American Psychiatric Association, 1987, p. 174).
The last decade has seen as much research asthe 35 years preceding, and manymisperceptions have been corrected. Yet theproblem remains elusive even as it grows.Many Americans who are now young ormiddle-aged will carry their use and abuse ofalcohol and other drugs with them into oldageand they will also live longer. Lifeexpectancy jumped almost 30 years between1900 and 1989, and it continues to climb. By theyear 2050, one out of four Americans over age 65will be 85 and older (U.S. Bureau of the Census,
1996). Substance use disorders, if not diagnosed

and treated, may ruin the last stage of life forcountless Americans.
This TIP illuminates this invisible epidemicand advises how to treat it, combining the bestof the existing literature with the years of theConsensus Panelists' experience in researching
Substance Abuse Among Older Adults
and treating older substance abusers. The Panelaims to advance the understanding of therelationships between aging and substanceabuse and to provide practicalrecommendations for incorporating thatunderstanding into practice.
3(311

2 Alcoho:
Alcohol abuse and misuse is the majorsubstance abuse problem among olderadults. "In the United States, it is
estimated that 2.5 million older adults haveproblems related to alcohol, and 21 percent ofhospitalized adults over age 40 . . . have adiagnosis of alcoholism with related hospitalcosts as high as $60 billion per year" (Schonfeld
and Dupree, 1995, p. 1819). In 1990, those overthe age of 65 comprised 13 percent of the U.S.
population; by the year 2030, older adults willaccount for 21 percent of the population (U.S.Bureau of the Census, 1996). This projectedpopulation explosion has serious implicationsfor both the number of alcohol-related problemslikely to occur among older adults and thesubsequent costs involved in responding tothem. Currently, rates for alcohol-relatedhospitalizations among older patients aresimilar to those for heart attacks (Adams et al.,1993). Those rates vary greatly by geographiclocation, from 19 per 10,000 admissions inArkansas to 77 per 10,000 in Alaska.
As disturbing as these figures are, theyprobably represent a gross underestimation ofthe true problem. Studies consistently find thatolder adults are less likely to receive a primarydiagnosis of alcoholism than are younger adults(Booth et al., 1992; Stinson et al., 1989; Beresford
et al., 1988). A study of 417 patients found thathouse officers accurately diagnosed the diseasein only 37 percent of older alcoholic patientscompared with 60 percent of the youngeralcoholic patients (Geller et al., 1989).
Alcoh 11 and A ingDespite a certain heterogeneity in drinkingpractices, there are substantial differencesbetween an older and a younger adult'sresponse to alcohol, the majority of which stemfrom the physiological changes wrought by theaging process.
Adults over the age of 65 are more likely tobe affected by at least one chronic illness, manyof which can make them more vulnerable to thenegative effects of alcohol consumption(Bucholz et al., 1995).
In addition, three age-related changessignificantly affect the way an older personresponds to alcohol:
E Decrease in body waterEl Increased sensitivity and decreased tolerance
to alcoholE Decrease in the metabolism of alcohol in the
gastrointestinal tract.
As lean body mass decreases with age, totalbody water also decreases while fat increases.Because alcohol is water-soluble and not fat-soluble, this change in body water means that,for a given dose of alcohol, the concentration ofalcohol in the blood system is greater in an olderperson than in a younger person. For thisreason, the same amount of alcohol thatpreviously had little effect can now causeintoxication (Smith, 1995; Vestal et al., 1977).
This often results in increased sensitivity anddecreased tolerance to alcohol as people age
3 713

Chapter 2
14
(Rosin and Glatt, 1971). Researchers speculatethat the change in relative alcohol contentcombined with the slower reaction timesfrequently observed in older adults may beresponsible for some of the accidents andinjuries that plague this age group (Bucholz etal., 1995; Salthouse, 1985; Ray, 1992).
The decrease in gastric alcoholdehydrogenase enzyme that occurs with age isanother factor that exacerbates problems withalcohol. This enzyme plays a key role in themetabolism of alcohol that occurs in the gastricmucosa. With decreased alcoholdehydrogenase, alcohol is metabolized moreslowly, so the blood alcohol level remains raisedfor a longer time. With the stomach less activelyinvolved in metabolism, an increased strain isalso placed on the liver (Smith, 1995).
ComorbiditiesAlthough alcohol can negatively affect a personof any age, the interaction of age-relatedphysiological changes and the consumption ofalcohol can trigger or exacerbate additionalserious problems among older adults, including
E Increased risk of hypertension, cardiacarrhythmia, myocardial infarction, andcardiomyopathy
El Increased risk of hemorrhagic strokeia Impaired immune system and capability to
combat infection and cancero Cirrhosis and other liver diseasesgl Decreased bone densityo Gastrointestinal bleedingE Depression, anxiety, and other mental health
problemsEl Malnutrition.
Other biomedical changes of aging arecognitive impairments, which are both confusedwith and exacerbated by alcohol use. Chronicalcoholism can cause serious, irreversiblechanges in brain function, although this is morelikely to be seen in older adults who have a long
38
history of alcoholism. Alcohol use may havedirect neurotoxic effects leading to acharacteristic syndrome called alcohol-related
dementia (ARD) or may be associated with thedevelopment of other dementing illnesses suchas Alzheimer's disease or Wemicke-Korsakoffsyndrome, an illness characterized byanterograde memory deficits, gait ataxia, andnystagmus. Indeed several researchers havecast doubt on the existence of ARD as a
neuropathological disease and suggest that themajority of cases of ARD are in fact Wernicke-Korsakoff syndrome (Victor et al., 1989).
Sleep patterns typically change as people age(Haponik, 1992). Increased episodes of sleepwith rapid eye movement (REM), decreasedREM length, decreased stage III and IV sleep,and increased awakenings are common patterns,all of which can be worsened by alcohol use.Moeller and colleagues demonstrated inyounger subjects that alcohol and depressionhad additive effects on sleep disturbances whenoccurring together (Moeller et al., 1993). Onestudy concluded that sleep disturbances,especially insomnia, may be a potential etiologicfactor in the development of late-life alcoholproblems or in precipitating relapse (Oslin andLiberto, 1995). This hypothesis is supported bya study demonstrating that abstinent alcoholicsexperienced insomnia, frequent awakenings,and REM fragmentation (Wagman et al., 1977).However, when these subjects ingested alcohol,sleep periodicity normalized and REM sleepwas temporarily suppressed, suggesting thatalcohol can be used to self-medicate sleepdisturbances.
Positive Effects of AlcoholConsumptionSmall amounts of alcohol have been shown toprovide some health benefits, althoughabstinence is still recommended for anyone whohas a history of alcoholism or drug abuse, whois taking certain medications (see Chapter 3), or

who is diagnosed with certain chronic diseasessuch as diabetes and congestive heart failure.Some studies, largely conducted on malesamples, show that low levels of alcoholconsumption (one standard drink per day orless) reduce the risks of coronary heart disease(Shaper et al., 1988). However, thiscardiovascular benefit may not apply to adultsalready diagnosed with heart disease. Olderadults in this category should not drink unlesstheir physician says otherwise.
"An intriguing epidemiologic finding is theassociation of regular, but moderate, alcohol use(up to two drinks per day) with lower morbidityand mortality from coronary artery disease,"especially in men, when compared with heavyalcohol users and abstainers (Atkinson andGanzini, 1994, p. 302). "This 'U' or 'J' shapedrelationship appears to be quite robust,"occurring in diverse cultural and nationalcohorts (Atkinson and Ganzini, 1994, p. 302).That heavy drinkers have more coronary diseaseis to be expected, but why should abstainershave higher morbidity and mortality thanmoderate drinkers? One explanation may bethat the abstainer group was heterogeneous incomposition and may have included formeralcoholics as well as others predisposed tocardiac disease (Atkinson et al., 1992). Anumber of other studies, including the only onereported to date that consisted of exclusivelyolder adult subjects, likewise failed to accountfor this possibility in their study designs (Scherret al., 1992).
Other analyses of abstainer groups reportconflicting findings (Shaper et al., 1988; Klatskyet al., 1990). Further study is needed todetermine the contributions of alcohol-inducedrise in high-density lipoproteins (HDLs)(Srivastava et al., 1994; Davidson, 1989) and
antioxidant effects of beverage alcohol (Artaud-Wild et al., 1993) to the association betweenabstinence and coronary artery disease.
399
Alcohol
Although moderate alcohol consumption hasbeen shown to improve HDL levels in women(Fuchs et a1.,1995), it also has been linked tobreast cancer in postmenopausal women(Bucholz et al., 1995). More studies on the risksand benefits of alcohol consumption for olderwomen are needed to clarify this issue.
Low levels of alcohol consumption alsoappear to promote and facilitate socializationamong older adults, suggesting that alcoholplays an important role in community life forolder adults (Gomberg, 1990). However, thehealth of some older adults (e.g., those withchronic conditions, those using certainmedications) may be compromised by anyalcohol consumption. Again, recommendationsfor use of alcohol should always beindividualized.
Classifying DrinkingPractices and Pr >blemsAmong Older AdultsPhysiological changes, as well as changes in thekinds of responsibilities and activities pursuedby older adults, make established criteria forclassifying alcohol problems largely irrelevantfor this population.
Two classic models for understandingalcohol problemsthe medical diagnosticmodel and the at-risk, heavy, and problemdrinking classificationinclude criteria thatmay not adequately apply to many older adultsand may lead to underidentification of drinkingproblems (Atkinson, 1990).
ISM -IVMost clinicians rely on the conventional medicalmodel defined in the American PsychiatricAssociation's Diagnostic and Statistical Manual of
Mental Disorders, Fourth Edition (DSM-IV)
(American Psychiatric Association, 1994) forclassifying the signs and symptoms of alcohol-related problems. The DSM-IV uses specific
15

Chapter 2
criteria to distinguish between those drinkerswho abuse alcohol and those who aredependent on alcohol. Figures 2-1 and 2-2present the DSM-IV criteria, which subsumealcohol abuse indicators within the generalcategories of substance abuse and dependence.
Although widely used, the DSM-IV criteriamay not apply to many older adults whoexperience neither the legal, social, norpsychological consequences specified. Forexample, "a failure to fulfill major roleobligations at work, school, or home" is lessapplicable to a retired person with minimalfamilial responsibilities. Nor does the criterion"continued use of the substance(s) despitepersistent or recurrent problems" always apply.Many older alcoholics do not realize that theirpersistent or recurrent problems are in factrelated to their drinking, a view likely to bereinforced by health care clinicians who may
attribute these problems, in whole or in part, tothe aging process or age-related comorbidities.
Although tolerance is one of the DSM-IVcriteria for a diagnosis of substancedependenceand one weighted heavily byclinicians performing an assessment forsubstance dependencethe thresholds ofconsumption often considered by clinicians asindicative of tolerance may be set too high forolder adults because of their altered sensitivityto and body distribution of alcohol (Atkinson,1990). The lack of tolerance to alcohol does not
necessarily mean that an older adult does nothave a drinking problem or is not experiencingserious negative effects as a result of his or herdrinking. Furthermore, many late onsetalcoholics have not developed physiologicaldependence, and they do not exhibit signs ofwithdrawal. Figure 2-3 presents the DSM-IVcriteria for substance dependence as they applyto older adults with alcohol problems.
Figure 2-1
DSIVI-1V Diagnostic Criteria for Substance Ab
The DSM-IV defines the diagnostic criteria for substance abuse as a maladaptive pattern of substanceuse leading to clinically significant impairment or distress, as manifested by one or more of thefollowing, occurring within a 12-month period:1. Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or
home (e.g., repeated absences or poor work performance related to substance use; substance-related absences, suspensions, or expulsions from school; neglect of children or household).
2. Recurrent substance use in situations in which it is physically hazardous (e.g., driving anautomobile or operating a machine when impaired by substance use).
3. Recurrent substance-related legal problems (e.g., arrests for substance-related disorderly conduct).4. Continued substance use despite having persistent or recurrent social or interpersonal problems
caused or exacerbated by the effects of the substance (e.g., arguments with spouse aboutconsequences of intoxication, physical fights).
Source: Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, Fourth
Edition. Copyright 1994, American Psychiatric Association.
4016

Alcohol
Figure 2-2 .
DSM-IV Diagnostic Criteria for Substance Dependence .
The DSM-IV defines the diagnostic criteria for substance dependence as a maladaptive pattern ofsubstance use, leading to clinically significant impairment or distress, as manifested by three or more ofthe following, occurring at any time in the same 12-month period:1. Tolerance, as defined by either of the following:
The need for markedly increased amounts of the substance to achieve intoxication or desiredeffect.
Markedly diminished effect with continued use of the same amount of the substance.2. Withdrawal, as manifested by either of the following:
The characteristic withdrawal syndrome for the substance.The same (or closely related) substance is taken to relieve or avoid withdrawal symptoms.
3. Taking the substance often in larger amounts or over a longer period than was intended.
4. A persistent desire or unsuccessful efforts to cut down or control substance use.
5. Spending a great deal of time in activities necessary to obtain or use the substance or to recover fromits effects.
6. Giving up social, occupational, or recreational activities because of substance use.7. Continuing the substance use with the knowledge that it is causing or exacerbating a persistent or
recurrent physical or psychological problem.Source: Reprinted with permission from the Diagnostic and Statistical Manual of Mental Disorders, FourthEdition. Co. ri:ht 1994, American Ps chiatric Association.
The drinking practices of many older adultswho do not meet the diagnostic criteria forabuse or dependence place them at risk ofcomplicating an existing medical or psychiatricdisorder. Consuming one or two drinks perday, for example, may lead to increasedcognitive impairment in patients who alreadyhave Alzheimer's disease, may lead toworsening of sleep problems in patients withsleep apnea, or may interact with medicationsrendering them less effective or causing adverseside effects. A barrier to good clinical
management in these cases may be the lack ofunderstanding of the risks of so-called"moderate drinking." Limiting access totreatment because symptoms do not meet therigorous diagnostic criteria of the DSM-IV may
preclude an older patient from makingsignificant improvements in his or her life.
At-Risk, Heavy, and ProblemDrinkingSome experts use the model of at-risk, heavy,
and problem-drinking in place of the DSM-IVmodel of alcohol abuse and dependence becauseit allows for more flexibility in characterizingdrinking patterns. In this classification scheme,an at-risk drinker is one whose patterns of alcoholuse, although not yet causing problems, maybring about adverse consequences, either to thedrinker or to others. Occasional moderatedrinking at social gatherings and then drivinghome is an example of at-risk drinking.Although an accident may not have occurred, allthe elements for disaster are present.
4117

Chapter 2
18
Applying DSM-IV Diagnostic Criteria
Figure 2-3
to Older Adults With Alcohol Problems
are subsumed within the DSM-IV's general criteria foras a "maladaptive pattern of substance use, leading to
as manifested by three (or more) of the following, occurring(American Psychiatric Association, 1994, p. 181). There are
criteria to older adults with alcohol problems.
Diagnostic criteria for alcohol dependence
substance dependence. Dependence is definedclinically significant impairment or distress,at any time in the same 12-month period"
special considerations when applying DSM-IV
Criteria Special Considerations for Older Adults1. Tolerance May have problems with even low intake due to increased
sensitivity to alcohol and higher blood alcohol levels2. Withdrawal Many late onset alcoholics do not develop physiological
dependence3. Taking larger amounts or over a
longer period than was intendedIncreased cognitive impairment can interfere with self-monitoring; drinking can exacerbate cognitive impairmentand monitoring
4. Unsuccessful efforts to cut down orcontrol use
Same issues across life span
5. Spending much time to obtain anduse alcohol and to recover fromeffects
Negative effects can occur with relatively low use
6. Giving up activities due to use May have fewer activities, making detection of problemsmore difficult
7. Continuing use despite physical orpsychological problem caused byuse
May not know or understand that problems are related touse, even after medical advice
As their names imply, the terms heavy andproblem drinking signify more hazardous levelsof consumption than at-risk drinking. Althoughthe distinction between the terms heavy andproblem is meaningful to alcohol treatmentspecialists interested in differentiating severityof problems among younger alcohol abusers, itmay have less relevance for older adults(Atkinson and Ganzini, 1994), who mayexperience pervasive consequences with lessconsumption due to their heightened sensitivityto alcohol or the presence of such coexistingdiseases as diabetes mellitus, hypertension,cirrhosis, or dementia.
In general, the threshold for at-risk alcoholuse decreases with advancing age. Although an
4 r'
individual's health and functional statusdetermine the degree of impact, the
pharmacokinetic and pharmacodynamic effectsof alcohol on aging organ systems result inhigher peak blood alcohol levels (BALs) andincreased responsiveness to doses that causedlittle impairment at a younger age. For example,body sway increases and the capacity to thinkclearly decreases with age after a standardalcohol load, even when controlling for BALs(Beresford and Lucey, 1995; Vogel-Sprott andBarret, 1984; Vestal et al., 1977).
Certain medical conditions, for example,hypertension and diabetes mellitus, can be madeworse by regular drinking of relatively smallamounts of alcohol. In addition, the tendency

"to take the edge off" with alcohol during timesof stress, and its subsequent impact on cognitionand problem-solving skills, may provokeinadequate or destructive responses, even inthose older adults whose overall consumptionover 6 months is lower than that for someyounger, problem-free, social drinkers.Furthermore, older drinkers who do not meetthe substance abuse criteria for "recurrent use"behavior or consequences may, nonetheless,pose potential risk to themselves or others.
For many adults, the phenomenon of aging,with its accompanying physical vulnerabilitiesand distinctive psychosocial demands, may bethe key risk factor for alcohol problems. Todifferentiate older drinkers, the Consensus Panelrecommends using the terms at-risk and problemdrinkers only. As discussed above, not only dothe concepts of quantity/frequency implicit inthe term heavy drinking have less application toolder populations, but the "distinction betweenheavy and problem drinking narrows with age"(Atkinson and Ganzini, 1994, p. 300). In thetwo-stage conceptualization recommended bythe Panel, the problem drinker category includesthose who would otherwise fall into the heavy
and problem classifications in the moretraditional model as well as those who meet theDSM-IV criteria for abuse and dependence.
Age-Appropriate Levels ofConsumptionIn its Physician's Guide to Helping Patients With
Alcohol Problems, the National Institute on
Alcohol Abuse and Alcoholism (NIAAA) offersrecommendations for low-risk drinking. Forindividuals over the age of 65, NIAAArecommends "no more than one drink per day"(National Institute on Alcohol Abuse andAlcoholism, 1995). The Consensus Panelendorses that recommendation and theaccompanying refinements presented below(Dufour et al., 1992):
No more than one drink per day
43
Alcohol
o Maximum of two drinks on any drinkingoccasion (New Year's Eve, weddings)
o Somewhat lower limits for women.
A standard drink is one can (12 oz.) of beeror ale; a single shot (1.5 oz.) of hard liquor; aglass (5 oz.) of wine; or a small glass (4 oz.) ofsherry, liqueur, or aperitif. The Panel's purposein promoting these limits is to establish a "safetyzone" for healthy older adults who drink. Oldermen and women who do not have serious orunstable medical problems and are not takingpsychoactive medications are unlikely to incurproblems with alcohol if they adhere to theseguidelines. The goal is to foster sensibledrinking that avoids health risks, while allowingolder adults to obtain the beneficial effects thatmay accrue from alcohol. Older adults' alcoholuse should be considered as spanning aspectrum from abstinence to dependence ratherthan falling into rigid categories.
Drinking Patterns AmongOlder AdultsAlthough more research on substance abuseamong older adults is needed, studies to datesuggest three ways of categorizing older adults'problem-drinkingearly versus late onsetdrinking, continuous versus intermittentdrinking, and binge drinking.
Early Onset Versus Late OnsetProblem DrinkingOne of the most striking and potentially usefulfindings in contemporary geriatric research isthe new understanding about the age at whichindividuals begin experiencing alcohol-relatedproblems. Although it appears that alcohol usedeclines with increasing age for most adults(Temple and Leino, 1989; Fillmore, 1987), some
begin to experience alcohol-related problems ator after age 55 or 60.
Early onset drinkers tend to havelongstanding alcohol-related problems that
19

Chapter 2
generally begin before age 40, most often in the20s and 30s. In contrast, late onset drinkersgenerally experience their first alcohol-relatedproblems after age 40 or 50 (Atkinson, 1984,1994; Liberto and Os lin, 1995; Atkinson et al.,1990).
Early onset drinkersEarly onset drinkers comprise the majority ofolder patients receiving treatment for alcoholabuse, and they tend to resemble youngeralcohol abusers in their reasons for use.Throughout their lives, early onset alcoholabusers have turned to alcohol to cope with arange of psychosocial or medical problems.Psychiatric comorbidity is common among thisgroup, particularly major affective disorders(e.g., major depression, bipolar disorder) andthought disorders. For the most part, theycontinue their established abusive drinkingpatterns as they age (Schonfeld and Dupree,1991; Atkinson, 1984; Atkinson et al., 1985, 1990;Stall, 1986).
Late onset drinkersIn comparison, late onset drinkers appearpsychologically and physically healthier. Somestudies have found that late onset drinkers aremore likely to have begun or to have increaseddrinking in response to recent losses such asdeath of a spouse or divorce, to a change inhealth status, or to such life changes asretirement (Hurt et al., 1988; Finlayson et al.,1988; Rosin and Glatt, 1971). Because late onset
problem drinkers have a shorter history ofproblem drinking and therefore fewer healthproblems than early onset drinkers do, healthcare providers tend to overlook their drinking.Panelists report that, in addition, this group'spsychological and social pathology, familyrelationships, past work history, and lack ofinvolvement with the criminal justice systemcontradict the familiar clinical picture ofalcoholism. Late onset drinkers frequently
20 44
appear too healthy, too "normal," to raisesuspicions about problem drinking.
The literature suggests that about one-thirdof older adults with drinking problems are lateonset abusers ( Liberto and Oslin, 1995). Lateonset alcoholism is often milder and moreamenable to treatment than early onset drinkingproblems (Atkinson and Ganzini, 1994), and itsometimes resolves spontaneously. Whenappraising their situation, late onset drinkersoften view themselves as affected bydevelopmental stages and circumstances relatedto growing older. Early onset drinkers are morelikely to have exacerbated their adverse
circumstances through their history of problemalcohol use (Atkinson, 1994).
Data from the Epidemiologic CatchmentArea Project (ECA), a large-scale, community-based survey of psychiatric disorders includingalcohol abuse and dependence, provide relevantinformation on the occurrence of late onsetalcoholism, which has been defined by variousresearchers as occurring after ages 40, 45, 50, or60 (Bucholtz et al., 1995). From the ECA study, 3
percent of male alcoholics between 50 and 59reported first having a symptom of alcoholismafter 49, compared with 15 percent of thosebetween 60 and 69 and 14 percent of thosebetween 70 and 79. For women, 16 percentbetween 50 and 59 reported a first symptom ofalcoholism after the age of 50, with 24 percent ofwomen between 60 and 69 and 28 percent ofwomen between 70 and 79. These percentagessuggest that late onset alcoholism is a significantproblem, especially among women. (Genderdifferences are discussed further below.)
Both early and late onset problem drinkersappear to use alcohol almost daily, outsidesocial settings, and at home alone. Both aremore likely to use alcohol as a palliative, self-
medicating measure in response to hurts, losses,and affective changes rather than as a socializingagent.

Although there is controversy over the issueof whether early and late onset distinctionsinfluence treatment outcomes (Atkinson, 1994),the Panel believes that problem onset affects thechoice of intervention. Panelists believe, forexample, that late onset problem drinkers mayrespond better than early onset drinkers to briefintervention because late onset problems tend tobe milder and are more sensitive to informalsocial pressure (Atkinson, 1994; Moos et al.,
Alcohol
1991). Figure 2-4 outlines the essentialsimilarities and differences between early andlate onset drinkers. The most consistentfindings concern medical and psychiatriccomorbidity; demographic and psychosocialfactors are less consistent. Little is known aboutthe impact of early versus late onset on thecomplications and treatment outcomes ofconcomitant medication and alcohol use.
Clinical Characteristics
Variable
Figure 2-4
of Early and Late Onset Problem
Earl Onset
Drinkers
Late Onset
A:e at onset Various, e.:., < 25, 40, 45 Various, e.:., > 55, 60, 65
Gender Higher proportion of men thanwomen
Higher proportion ofwomen than men
Socioeconomic status Tends to be lower Tends to be hi her
Drinkin: in res onse to stressors Common Common
Famil histor of alcoholism More prevalent Less prevalent
Extent and severity of alcoholroblems
More psychosocial, legalroblems, reater severit
Fewer psychosocial, legalroblems, lesser severit
Alcohol-related chronic illness(e.g., cirrhosis, pancreatitis,
cancers)
More common Less common
Psychiatric comorbidities Cognitive loss more severe, less
reversible
Cognitive loss less severe,more reversible
Age-associated medical problemsaggravated by alcohol (e.g.,hypertension, diabetes mellitus,dru:--alcohol interactions)
Common Common
Treatment compliance andoutcome
Possibly less compliant;Relapse rates do not vary by ageof onset (Atkinson et al., 1990;
Blow et al., 1997; Schonfeld and
Dupree, 1991)
Possibly more compliant;Relapse rates do not vary byage of onset (Atkinson et al.,1990; Blow et al., 1997;
Schonfeld and Dupree,1991)
45 21

Chapter 2
22
Continuous Versus IntermittentDrinkingAnother way of understanding the patterns ofdrinking over a life span is to look at the timeframes in which people drink and the frequencyof their drinking. In contrast to ongoing,continuous drinking, intermittent drinking refersto regular, perhaps daily, heavy drinking thathas resumed after a stable period of abstinenceof 3 to 5 years or more (National Institute onAlcohol Abuse and Alcoholism, 1995).
Intermittent drinking problems are easy tooverlook, but crucial to identify. Even thoseproblem drinkers who have been sober formany years are at risk for relapse as they age.For this reason, during routine healthscreenings, it is important for clinicians to take ahistory that includes both current and lifetimeuse of alcohol in order to identify prior episodesof alcoholism. When armed with thisinformation, caregivers can help their olderpatients anticipate situations that tend toprovoke relapse and plan strategies foraddressing them when they occur.
Binge DrinkingBinge drinking is generally defined as shortperiods of loss of control over drinkingalternating with periods of abstinence or muchlighter alcohol use. A binge itself is usuallydefined as any drinking occasion in which anindividual consumes five or more standarddrinks. For older adults, the Consensus Paneldefines a binge as four or more drinks peroccasion. People who are alcohol-freethroughout the work week and celebrate withFriday night or holiday "benders" would beconsidered binge drinkers.
Identifying older binge drinkers can bedifficult because many of the usual clues,
including disciplinary job actions or arrests fordriving while intoxicated, are infrequently seenamong aging adults who no longer work or
46'
drive. Although research is needed on thenatural history of binge drinkers as they age,anecdotal observations indicate that youngerbinge drinkers who survive to their later yearsoften become continuous or near-daily drinkers.
Risk Factors for AlcoholAbuse
GenderStudies indicate that older men are much morelikely than older women to have alcohol-relatedproblems (Myers et al., 1984; Atkinson, 1990;
Bucholz et al., 1995). Since the issue was firststudied, most adults with alcohol problems inold age have been found to have a long historyof problem drinking, and most of them havebeen men (D'Archangelo, 1993; Helzer et al.,1991b). About 10 percent of men report ahistory of heavy drinking at some point in theirlives. Being a member of this group predictsthat one will have widespread physical,
psychological, and social dysfunction in later life(Colsher and Wallace, 1990) and confers agreater than fivefold risk of late-life psychiatricillness despite cessation of heavy drinking(Saunders et al., 1991). Forty-three percent ofveterans (who can be assumed to be mostlymale and mostly alcoholas opposed to drugabusers) receiving long-term care were found tohave a history of substance abuse problems(Joseph et al., 1995; D'Archangelo, 1993). Menwho drink have been found to be two to sixtimes more likely to have medical problems thanwomen who drink (Adams et al., 1993), eventhough women are more vulnerable to thedevelopment of cirrhosis.
Older women are less likely to drink and lesslikely to drink heavily than are older men(Bucholz et al., 1995). The ratio of male-to-
female alcohol abusers, however, is an openquestion. Bucholz and colleagues noted a"substantial excess of men over women," larger

than the gap observed in younger age groups(Bucholz et al., 1995, p. 30). Another study,however, found "a higher than expectednumber of females," (Beresford, 1995b, p. 11),whereas a study of older patients in treatmentfacilities found a ratio of 2:1 (83 men to 42
women) (Gomberg, 1995).Both epidemiological research, including the
findings of the ECA studies of the NationalInstitute of Mental Health (Holzer et al., 1984),and clinical research consistently report lateronset of problem drinking among women(Gomberg, 1995; Hurt et al., 1988; Moos et al.,
1991). In one study by Gomberg, for example,women reported a mean age at onset of 46.2years, whereas men reported 27.0 years.Furthermore, 38 percent of older female patientsbut only 4 percent of older male patientsreported onset within the last 10 years(Gomberg, 1995).
A number of other differences between oldermale and female alcohol abusers have beenreported: In contrast to men, women are morelikely to be widowed or divorced, to have had aproblem drinking spouse, and to haveexperienced depression (Gomberg, 1993).Women also report more negative effects ofalcohol than men (Gomberg, 1994), greater useof prescribed psychoactive medication (Brennanet al., 1993; Gomberg, 1994; Graham et al., 1995),
and more drinking with their spouses.Although research has not identified any
definite risk factors for drinking among olderwomen, Wilsnack and colleagues suggest thatincreased amounts of free time and lessening ofrole responsibilities may serve as an etiologicalfactor (Wilsnack et al., 1995). It should also be
noted that women generally are morevulnerable than men to social pressure, so theirmove into retirement communities wheredrinking is common probably has an impact.
Differences between men and women haveimplications for treatment. Women of all agesare less likely than men to appear at treatment
Alcohol
facilities. Among older women who may besocially isolated or homebound, outreach isparticularly important. Families, physicians,senior centers and senior housing staff, and thepolice play important roles in helping to identifywomen who abuse alcohol (see Chapter 5 formore on community outreach). To be effective,however, all of these potential outreach agentsmust be sensitive to women's feelings of stigma,shame, and social censure.
Loss of SpouseAlcohol abuse is more prevalent among olderadults who have been separated or divorced andamong men who have been widowed (Bucholzet al., 1995). Some researchers havehypothesized that a significant triad of disordersmay be triggered in older men when their wivesdiedepression, development of alcoholproblems, and suicide. The highest rate ofcompleted suicide among all population groupsis in older white men who become excessivelydepressed and drink heavily following the deathof their spouses (National Institute on AlcoholAbuse and Alcoholism, 1988; Brennan and
Moos, 1996).
Other LossesAs individuals age, they not only lose theirspouse but also other family members andfriends to death and separation. Retirementmay mean loss of income as well as job-relatedsocial support systems and the structure andself-esteem that work provides. Other lossesinclude diminished mobility (e.g., greaterdifficulty using public transportation whereavailable, inability to drive or driving limited tothe daylight hours, problems walking); impairedsensory capabilities, which may be isolatingeven when the elder is in physical proximity toothers; and declining health due to chronic
illnesses.
4723

Chapter 2
24
Health Care SettingsHigh rates of alcoholism are consistentlyreported in medical settings, indicating the needfor screening and assessment of patients seen forproblems other than substance abuse (Douglass,1984; Liberto et al., 1992; Adams et al., 1996).
Among community-dwelling older adults,investigators have found a prevalence ofalcoholism between 2 and 15 percent (Gomberg,1992b; Adams et al., 1996) and between 18 and44 percent among general medical and
psychiatric inpatients (Colsher and Wallace,1990; Saunders et a1.,1991).
Substance Abuse Earlier in LifeA strong relationship exists between developinga substance use disorder earlier in life andexperiencing a recurrence in later life. Somerecovering alcoholics with long periods ofsobriety undergo a recurrence of alcoholicdrinking as a result of major losses or an excessof discretionary time (Atkinson and Ganzini,1994). Among the 10 percent of older men whoreported a history of heavy drinking at somepoint in their lives, widespread physical andsocial problems occurred in later life (Colsherand Wallace, 1990). Drinking problems early inlife confer a greater than fivefold risk of late-lifepsychiatric illness despite cessation of heavydrinking. Indeed, some research suggests that aprevious drinking problem is the strongestindicator of a problem in later life (Welte andMirand, 1992) and that "studying olderalcoholics today may help to anticipate thedemands that these younger alcoholics willeventually place on our resources and society"(Bucholz et al., 1995, p. 19).
Comorbid Psychiatric DisordersEstimates of primary mood disorder occurringin older alcohol abusers vary from 12 to 30percent or more (Finlayson et al., 1988; Koenigand Blazer, 1996). Although research does notsupport the notion that mood disorders precede
48
alcoholism in older adults, there is evidence thatthey may be either precipitating or maintenancefactors in late onset drinking. Depression, forexample, appears to precipitate drinking,particularly among women. Some problemdrinkers of both sexes who do not meet theclinical criteria for depression often reportfeeling depressed prior to the first drink on a
drinking day (Dupree et al., 1984; Schonfeld andDupree, 1991).
Patients with severe cognitive impairmentgenerally drink less than nonimpaired alcoholusers. Panelists report that, among individualswho are only mildly impaired, however, alcoholuse may increase as a reaction to lower self-esteem and perceived loss of memory. Axis IIdisorders are more likely to be associated withearly onset interpersonal and alcohol-relatedproblems and less likely to affect the individualfor the first time at age 60 or older. Late onsetalcohol abuse is less associated withpsychological or psychiatric problems and morelikely linked to age-associated losses. Theexception might be the intermittent drinker whohas been in control and whose alcohol or
psychiatric problems surface again later in life.See Chapter 4 for more on psychiatriccomorbidity.
Family History of Alcohol ProblemsThere is substantial cumulative evidence thatgenetic factors are important in alcohol-relatedbehaviors (Cotton, 1979). Some studies havesuggested that there may be a greater geneticetiology of problem drinking in early onset thanin late onset male alcohol abusers (Atkinson etal., 1990). Researchers studying the genetictendency of a group of male alcohol abusersassert that these men often have an early historyof drinking that worsens over time (Goodwinand Warnock, 1991; Schuckit, 1989).
Although most human genetic studies ofalcohol use have been conducted on relativelyyoung subjects, several studies using a twin

registry of U.S. veterans have focused onsignificantly older individuals (Carmel li et al.,1993; Swan et al., 1990). The results of thesestudies provide strong evidence that drinkingbehaviors are greatly influenced by geneticsthroughout the lifespan (Heller and McClearn,1995; Atkinson, 1984).
ConcomitantSubstance UseThe substances most commonly abused by olderadults besides alcohol are nicotine andpsychoactive prescription medications. (SeeChapter 3 for further discussion of psychoactivedrug abuse and of drug interactions.) Bothnicotine and prescription drug abuse are farmore prevalent among older adults who alsoabuse alcohol than among the generalpopulation of this age group (Gronbaek et al.,1994; Goldberg et al., 1994; Colsher et al., 1990;Finlayson et al., 1988). The Panel recognizes thatthe concomitant use of prescribedbenzodiazepines and alcohol is also commonamong older adults, especially older women.This includes nonabusive use of bothsubstances, which may be harmful even atmodest dosesfor example, consuming one ortwo drinks plus a small dose of a sedative atnight. A similar concern is raised with theconcomitant use of alcohol and opiatesprescribed for pain relief. Although there islittle empirical evidence in this area, clinical
practice suggests that dual addiction decreasesthe effectiveness of specific interventions andincreases the individual's severity of symptoms.
Although there is little research on the abuseof other illicit substances (e.g., heroin, cocaine,marijuana) by older adults, therapists and healthcare personnel are seeing more older adults whopresent with symptoms of illicit drug abuse.Panel members believe that many of these olderillicit drug abusers receive drugs from a
4J
Alcohol
younger relative or partner who uses or sellsdrugs.
TobaccoSmoking is the major preventable cause ofpremature death in the United States,accounting for an estimated five million years ofpotential life lost (U.S. Preventive Services TaskForce, 1996). Every year, tobacco smoking isresponsible for one out of every five Americandeaths (U.S. Preventive Services Task Force,1996). Despite these compelling statistics,however, 25.5 percent or 48 million adults arecurrent smokers (National Center for Health
Statistics, 1996).
Surveys show that cigarette smoking,although fairly widespread among older adults,declines sharply after age 65. In 1994,approximately 28 percent of men ages 45 to 64reported current use of cigarettes; among thoseage 65 and older, however, this figure was onlyabout 13 percent. In the younger age group(ages 45 to 64), women have lower smokingrates than men, but after age 65, the levels aresimilar. Approximately 23 percent of womenages 45 to 64 reported smoking cigarettes in1994, whereas about 11 percent of those age 65
and older currently smoked (National Center forHealth Statistics, 1996). Although the trend inuse declines with age, the problem remainssignificant with over 4 million older adultssmoking regularly (Salive et al., 1992).
Smoking is a "major risk factor for at least 6
of the 14 leading causes of death amongindividuals 60 years and older (i.e., heartdisease, cerebrovascular disease, chronicobstructive pulmonary disease,pneumonia/influenza, lung cancer, colorectalcancer) and a complicating factor of at leastthree others" (Cox, 1993, p. 424). Currentcigarette smoking is also "associated with anincreased risk of losing mobility in both menand women" (LaCroix et al., 1993). Notsurprisingly, older adult smokers have a "70
25

Chapter 2
percent overall risk of dying prematurely"(Carethers, 1992, p. 2257), and fewer smokers"make it to the ranks of older adults ascompared with non-smokers and quitters" (Cox,1993, p. 423). In addition to increasing the riskof disease, smoking may also affect theperformance of prescription drugs. Forexample, smokers tend to require higher dosesof benzodiazepines to achieve efficacy than dononsmokers (Ciraulo et al., 1995).
Smoking in older problem drinkers is farmore prevalent than in the general older adultpopulation, making tobacco use the mostcommon substance use disorder among olderadults. Some researchers estimate that 60 to 70percent of older male alcohol users smoke apack a day (Finlayson et al., 1988), an
assessment consistent with studies indicatingthat the prevalence of smoking among alcoholicsgenerally is above 80 percent (Jarvik andSchneider, 1992).
Although there have been few studies oninterventions that are especially useful to olderadults regarding smoking cessation, theadvantages of quitting at any age are clear (Fioreet al., 1990; Orleans et al., 1994a; Rimer and
Orleans, 1994; Orleans et al., 1994b). Two yearsafter stopping, for example, the risk of strokebegins to decrease. Mortality rates for chronicobstructive pulmonary disease decline;bronchitis, pneumonia, and other infectionsdecrease; and respiratory symptoms such ascough, wheezing, and sputum production lessen(U.S. Preventive Services Task Force, 1996). Asanother example, a 60-year-old male smokerwho quits can expect to reduce his risk of
smoking-related illness by about 10 percent overthe next 15 years (Cox, 1993).
As with alcohol and drug abuse, studiessuggest that many clinicians fail to counselpatients about the health effects of smoking,despite the fact that "older smokers are morelikely to quit than younger smokers" (Salive etal., 1992, p. 1268). However, tailoring smoking
26
cessation strategies to older adults so that theirunique concerns and barriers to quitting areaddressed improves success rates. Briefintervention, for example (see Chapter 5), canmore than double 1-year quit rates for olderadults (Rimer and Orleans, 1994). In one studyof older smokers using transdermal nicotinepatches, 29 percent of the subjects quit smokingfor 6 months (Orleans et al., 1994). Becausethere is little evidence that adults in recoveryfrom alcohol problems relapse when they stopsmoking, the Panel recommends that efforts toreduce substance abuse among older adults alsoinclude tobacco smoking (Hurt et al., 1993).
Psychoactive DrugsOlder adults' use of psychoactive drugscombined with alcohol is a growing concern (seeChapter 3). In a study of inpatients age 65 andolder in a chemical dependency program, 12
percent had combined dependence on alcoholand one or more prescription drugs ( Finlaysonet al., 1988). In addition, an early report bySchuckit and Morrissey found that two-thirds ofwomen in an alcohol treatment center hadreceived prescriptions for abusable drugs,usually hypnotic and antianxiety drugs, andone-third reported abusing them (Schuckit andMorrissey, 1979). The drug-abusing women inthis study reported more suicide attempts andearly antisocial problems and had received morepsychiatric care than the alcoholic women whodid not abuse their prescriptions. Thesefindings are of particular concern becauseanxiolytics, hypnotics, and stimulants may beused to treat alcohol and other drug abusers.
An additional concern is that psychoactivedrugs may combine with alcohol to createadverse drug reactions. A recent study foundthat the combination of alcohol and over-the-
counter pain medications was the most commonsource of adverse drug reactions among olderpatients (Forster et al., 1993). Such druginteractions result from a lack of understanding

Alcohol
among physicians, pharmacists, and older consuming alcohol when taking certain
adults themselves about the potential dangers of medications.
27
5 I

3 Use an Abuse of PsychoactivePrescription Drugs and Over-the-Counter Medications
Adults age 65 and older consume moreprescribed and over-the-countermedications than any other age group
in the United States. Although older adultsconstituted less than 13 percent of thepopulation in 1991, they received 25 to 30percent of all prescriptions (Woods and Winger,1995; Ray et al., 1993; Sheahan et al., 1989) and
experienced more than half of all reportedadverse drug reactions leading tohospitalization (Chastain, 1992). Some 80 to 86percent of older adults over age 65 reportedlysuffer from one or more chronic diseases orconditions (Administration on Aging and Staffof the U.S. Senate Special Committee on Aging,1991; U.S. Bureau of the Census, 1996), and anestimated 83 percent of adults over 65 take at
least one prescription drug (HazeldenFoundation, 1991; Ray et al., 1993). In fact, 30
percent of those over 65 take eight or moreprescription drugs daily (Sheahan et al., 1989).
A large share of prescriptions for older adultsare for psychoactive, mood-changing drugs thatcarry the potential for misuse, abuse, ordependency. In 1983, one-fourth of communitydwelling older adults used psychotherapeuticdrugs on a regular basis for sleep disorders orchronic pain as well as for anxiety and labilemood (Finlayson, 1995b). Approximately 25 to28 percent of older adults reported use of a
psychoactive drug within the last year, and 20percent used a tranquilizer daily. Indeed, 27percent of all tranquilizer prescriptions and 38percent of hypnotic prescriptions in 1991 werewritten for older adults. Moreover, older adultsare apparently more likely to continue use ofpsychoactive drugs for longer periods than theiryounger counterparts (Sheahan et al., 1995;
Woods and Winger, 1995).This chapter focuses on the most commonly
prescribed abusable psychoactive medicationsfor older adultsbenzodiazepines,antidepressants, and opiate/ opioid analgesics.Also covered are risk factors that make olderadults more vulnerable to misuse and abuse ofthese substances; adverse effects associated withconsumption of psychoactive medications; anduses for, effects of, and alternatives to differentcategories of prescription drugs.
Evolution of PsychoactivePrescribingSince their introduction in the late 1950s,benzodiazepines have become the most widelyprescribed anxiolytics and hypnotics in medicalpractice. Their growing use throughout the1960s prompted many to ask whether theUnited States was becoming an overmedicatedsociety in which people would take a pill for any
5229

Chapter 3
30
physical or emotional pain rather than exertsome simple self-control. Some researchersfeared that use of prescribed psychoactive drugsfor a vast array of conditions would inexorablylead to irresponsible recreational use orphysiological dependence on licit or illicitsubstances. Others thought that prevalence ofassociated psychosocial problems would risealong with the prescription drug use (Baiter,1973; Manheimer et al., 1973; Cooperstock andParnell, 1982).
Yet studies of older populations conductedover the past 20 years have generally found thatmost adults who take psychoactive medicationsdo not intend to abuse them. The drugs usuallyare obtained with an appropriate prescriptionfrom a primary care physician for a specifichealth-related purpose and are primarily used inconjunction with a physical condition or toalleviate symptoms of emotional stress (Pi land,1979; Guttmann, 1977; Cooperstock and Parnell,1982). In fact, there has been a steady
improvement in prescribing practices and safeand appropriate medication use in the last 25years.
Misuse and abuse of prescriptions havedwindled over that time for several reasons: (1)safer drugs with fewer undesirable side effectsare constantly being developed bypharmaceutical companies, especially forcommon health and mental health problems; (2)ever-changing Federal and State regulationsseek to protect consumers from hazardoussubstances and to restrict undesirable providerpractices; (3) guidelines and protocolsrecommending best practices are beingdeveloped and disseminated to health careproviders; (4) more physicians are receivingtraining relevant to the care of older patients(from geriatric research, education, and clinicalcenters); and (5) consumers are being educatedby their physicians and other health careproviders, pharmacists, and various mediasources regarding the dangers of drug
53
interactions and the importance of medicationcompliance for positive therapeutic outcomes.
More specifically, benzodiazepines with a
lower addiction potential and fewer adverseinteractions with other medications havereplaced many of the older barbiturates,bromides, meprobamate, and neuroleptics formanagement of anxiety, especially acute
situational anxiety, generalized anxiety disorder,and associated transient insomnia. Similarly, inthe 1960s, the benzodiazepine flurazepam
(Dalmane) replaced many of the barbituratesand nonbarbiturates routinely used for sleepdisorders and insomnia complaints. Displaceddrugs included such barbiturates aspentobarbital (Nembutal), secobarbital(Seconal), and the combination aprobarbital andsecobarbital (Tuinal), as well as thenonbarbiturates chloral hydrate, ethchlorvynol(Placidyl), and glutethimide (Doriden) (Foutsand Rachow, 1994; Finlayson, 1995b; Rickels andSchweizer, 1993). Sales reports and pharmacyprescription audits reflect the overall decline inthe numbers of stimulant and barbiturateprescriptions, with minor tranquilizers and/orsedatives exceeding other classes since the 1980s(Cooperstock and Parnell, 1982). Prescriptionsfor the popular arixiolytic benzodiazepines havemore recently shifted from diazepam (Valium)to the shorter acting compounds, particularlyalprazolam (Xanax) and lorazepam (Ativan),and from the earlier long-acting benzodiazepine
hypnotic, flurazepam, to the shorter actingtriazolam (Halcion) and temazepam (Restoril).Overall, sales of benzodiazepine anxiolytics
have decreased, whereas use of benzodiazepinesas sleep-inducing hypnotics has increased orremained stable (Winger, 1993; Woods andWinger, 1995).
In 1996, the top 10 drugs prescribed innursing homes included two selective serotoninreuptake inhibitors (SSRIs), sertraline (Zoloft)and fluoxetine (Prozac), as well as the
nonbenzodiazepine anxiolytic, buspirone

(BuSpar). This represents a decrease from 1970,when 8 of the top 10 nursing home prescriptionswere for psychoactive drugs (Prentice, 1979).Furthermore, chronic pain from such conditionsas arthritis is more frequently treated now withnonsteroidal anti-inflammatory agents ratherthan with opiate-containing drugs such asacetaminophen with codeine (Finlayson, 1995b).
Yet even though fewer prescriptions forpsychoactive drugs are being written for olderadults, many patients prescribed these drugsstill misuse and abuse them, and some healthcare providers continue to exhibit poorjudgment in their prescribing and monitoringpractices.
Patterns ®f UseThe drug-taking patterns of psychoactiveprescription drug users can be described as acontinuum that ranges from appropriate use formedical or psychiatric indications throughmisuse by the patient or the prescribing healthcare practitioner to persistent abuse anddependence as defined by the AmericanPsychiatric Association's criteria in theDiagnostic and Statistical Manual of Mental
Disorders, Fourth Edition (DSM-IV) (AmericanPsychiatric Association, 1994) (see Figure 3-1).
Because older adults are less likely to usepsychoactive medications nontherapeutically,problems with drugs generally fall into themisuse category and are unintentional. Forexample, older patients are more likely tomisunderstand directions for appropriateuse a problem that is compounded by themultiple prescriptions they receive, often frommultiple physicians unaware of a colleague'streatments. In these circumstances, overdose,additive effects, and adverse reactions fromcombining drugs are more likely to occur.Unintentional misuse can, however, progressinto abuse if an older adult continues to use amedication nontherapeutically for the desirable
Prescription Drugs
effects it provides, much as an abuser of anydrug does.
Adults can become physiologicallydependent on psychoactive medications withoutmeeting dependence criteria. Tolerance andphysical dependence can develop when somepsychoactive medications (e.g.,benzodiazepines, opioids) are taken regularly atthe therapeutically appropriate dose forrelatively brief periods. An abstinencesyndrome or withdrawal effects may occur if thedrug is stopped precipitously. This type ofiatrogenically induced physiologicaldependence is not usually accompanied by anytendency on the part of the patient to escalatedosage during or after medically supervisedwithdrawal, to experience cravings afterdiscontinuation, or to subsequently continue useor addictive behavior (Woods and Winger, 1995;Portenoy, 1993). In other words, adults canbecome dependent on psychoactive medicationswithout realizing it.
Risk Factors for i isuseAny Abr =se ofPsychoactive DrugsA variety of factors influence the use andpotential for misuse or abuse of psychoactiveprescription drugs and over-the-countermedications by older adults. The aging process,with its physiological changes, accumulatingphysical health problems, and otherpsychosocial stressors, makes prescription druguse both more likely and more risky. The mostconsistently documented correlates ofpsychoactive prescription drug use are old age,
poor physical health, and female gender(Cooperstock and Parnell, 1982; Sheahan et al.,
1989; Finlayson, 1995b).
5431

Chapter 3
Figure 3-1Continuum of Psychoactive Prescription Drug Use.
Proper Use
MisuseBy Patient
Dose level more or less than recommendedUse for contraindicated purposesUse in conjunction with other medications with undesirable interactionsSkipping doses/hoarding drugsUse with alcohol
By Doctor
Prescribing unnecessarily high dosePrescribing without determining what other medication patient is taking
3Not
clearly explaining regimen
AbuseBy Patient
Use resulting inDecline in work, school, or home performanceLegal problems
Use in risky situations (e.g., driving while impaired)Continued use despite adverse social or interpersonal consequences
Source: American Psychiatric Association, 1994
DependenceBy Patient
Use resulting inToleranceWithdrawal symptomsDecline in normal activitiesUnsuccessful attempts or a desire to cut down or control use
Use of a substance in larger amounts or for a longer period than was intendedUse that consumes a lot of time (including time to acquire and use the drug and to recover from its effects)Continued use despite knowledge that it has caused or aggravated a physical or psychological problem
Source: American Psychiatric Association, 1994
Among older women, use of psychoactivedrugs is correlated with middle- and late-lifedivorce, widowhood, less education, poorerhealth and chronic somatic problems, higherstress, lower income, and more depression andanxiety (Gomberg, 1995; Closser and Blow,1993). Major losses of economic and social
supports, factors related to the provider and
32
health care system, and previous or coexistingdrug, alcohol, or mental health problems alsoseem to increase vulnerability for misusing orabusing prescribed medications.
Data from the 1984 Epidemiological
Catchment Area (ECA) survey (Regier et al.,1988) confirm that anxiety disorders arerelatively prevalent in the general population of
55

adults older than 65, with 7.3 percent of olderrespondents reporting an incidence within thepast month. Older women are nearly twice aslikely as older men to develop a diagnosableanxiety disorder. Bereavement precipitatesanxiety in nearly one-fourth of survivors duringthe first 6 months following the death of a lovedone and in nearly two-fifths of those left behindduring the second 6-month period. Anxiety isalso common after a severe traumatic event(Salzman, 1993a).
System and EnvironmentalInfluencesA variety of health care system-related andenvironmental factors also place older adultusers of psychoactive prescription drugs at riskfor misuse of these substances, serious adverseeffects, or abuse and dependence. Potentiallydangerous prescribing practices includeordering medications without adequatediagnoses or other documented indicators ofsymptoms, prescribing them for too long a timewithout appropriate medical monitoring of drugreactions and patient compliance with theprescribed regimen, selecting drugs known tohave a high potential for side effects in older
adults at the doses given, ordering drugswithout knowing or reviewing whether theyinteract adversely with other medications thepatient is taking, and failing to provide adequateand comprehensible instructions for patientsregarding how and when to take medicationsand what side effects to expect and report. Drugmisuse also includes failure to consider theinfluence of aging on the effects of drugs in the
body (see Figure 3-2).
5:6
Prescription Drugs
Previous History of SubstanceAbuse or Psychiatric DisorderAlthough most experts agree that nonmedicaluse or abuse of benzodiazepines is rare at anyage and household surveys indicate thatnonmedical use is declining (Salzman, 1993b;Barnas et al., 1992), some liability for abuse ofthe benzodiazepines does seem to exist in thefollowing cohorts: (1) light-to-moderate alcoholdrinkers who have been demonstrated to preferdiazepam over placebo and may be vulnerableto the reinforcing properties of these drugs; (2)adults with histories of sedative abuse, abuse ofmultiple drugs, and methadone-maintainedclients; and (3) patients who have developedphysiological dependence on benzodiazepinesafter long-term use and are experiencing acutewithdrawal effects following abruptdiscontinuation (Salzman, 1993b; Barnas et al.,
1992).
However, continued craving for themedication does not seem to persist amongadults who fit none of the categories above andwho have successfully been withdrawn frombenzodiazepines. By contrast, adults withhistories of substance abuse preferbenzodiazepines to placebo. They also prefer,however, older anxiolytics and hypnotics suchas methaqualone (Quaalude) or meprobamate(Miltown) to benzodiazepines (Winger, 1993;Woods and Winger, 1995). The benzodiazepinespreferred by sedative abusers and methadonemaintenance clients seem to be diazepam,lorazepam, and alprazolam (Woods andWinger, 1995). Unfortunately, little is knownabout the risk potential for these individuals inlate life.
33

Chapter 3
'igure 3-2,f
gnagoop,Response to Drug EffectDrug Action Effects of A in:Analgesics
Aspirin
Morphine
Pentazocine
Anticoagulants
Heparin
Warfarin
Acute gastroduodenal mucosal damage
Acute analgesic effect
Analgesic effect
Activated partial thromboplastin time
Prothrombin time
No change
Increased
Increased
No change
Increased
Bronchodilators
Albuterol Bronchodilation No changeIpratropium Bronchodilation No change
Cardiovascular Drugs
Adenosine Minute ventilation and heart rate No changeDiltiazem Acute antihypertensive effect IncreasedEnalepril Acute antihypertensive effect IncreasedIsoproterenol Chronotropic effect DecreasedPhenylephrine Acute vasoconstriction No change
Acute antihypertensive effect No changePrazocin Chronotropic effect DecreasedTimolol Chronotropic effect No changeVera p amil Acute antihypertensive effect Increased
Diuretics
Furosemide Latency and size of peak diuretic response Decreased
Psychotropics
Diazepam Acute sedation IncreasedDip henhyd rami ne Psychomotor function No changeHaloperidol Acute sedation DecreasedMidazolam Electroencephalographic activity IncreasedTemazep am Postural sway, psychomotor effect, and sedation IncreasedTriazolam Psychomotor activity Increased
Others
Levodopa
TolbutamideDose elimination due to side effects
Acute hypoglycemic effectIncreased
DecreasedSource: Adapted from Cusack and Vestal, 1986.
34
5 7

Data from the Mayo Clinic further suggestthat psychiatric diagnoses may be a risk factoramong older adults for abuse of anddependence on prescription drugs (Finlayson,1995a). In this study, rates of mental disorderdiagnosis in 100 older adults hospitalized forprescription drug dependence included thefollowing disorders: mood (32 percent), organicmental (28 percent), personality (27 percent),somatoform (16 percent), and anxiety (12
percent). The patient group was predominantlyfemale, and some patients had more than onemental disorder diagnosis. The patient groupwas identified as having considerablepsychopathology by several other measures aswell (Finlayson, 1995a). Although research onolder drug addicts is rare, at least one studyindicates that older patients with substancedependence disorders are more likely thanyounger drug addicts to have a dual diagnosis.In this investigation, only 15 percent of olderdrug-dependent patients had a substance abusediagnosis without a coexisting psychiatricdisorder compared with 64 percent of youngercounterparts. These researchers concluded thatolder adults with a preexisting psychiatricdisorder may be more at risk for concurrentprescription drug dependence (Solomon et al.,
1993).
Adverse EffectsThe chronic administration of psychoactivesubstances to older adults, even at therapeuticdoses, has been associated with a variety ofadverse central nervous system effects,including diminished psychomotorperformance, impaired reaction time, loss of
Prescription Drugs
coordination, ataxia, falls, excessive daytimedrowsiness, confusion, aggravation of emotionalstate, rage, and amnesia as well as thedevelopment of physiological dependencemanifested by withdrawal effects when thedrugs are suddenly discontinued (Fouts andRachow, 1994). Psychoactive medications havebeen implicated in 23 percent of adverse drugreactions among nursing home residents(Joseph, 1995). Side effects from these drugsrange from constipation, dry mouth, or urinarydifficulty to such severe reactions as hipfractures from falls, withdrawal seizures ordelirium, and worsened depression leading tosuicide attempts (American PsychiatricAssociation, 1994). However, all undesirablereactions may be more serious in frail olderadults and in those with multiple chronicdiseases and cannot be ignored (Lapane et al.,
1995; Solomon et al., 1993).
AnxiolyticsFigure 3-3 summarizes information about someof the anxiolytics most frequently prescribed foracute or chronic anxiety in older adults. Thefigure depicts the generic and most usual brandname for these medications as well as theelimination half-life or duration of action in thebody. Note that Figures 3-3 and 3-4 bothcontain the names of benzodiazepinestheirdesignations as anxiolytics or sedative/hypnotics
are based on properties that drive marketingdecisions. Some physicians may choose, forexample, to use lorazepam as either ananxiolytic or sedative depending on the
circumstances.
53 35

Chapter 3
Class
CommonlyFigure 3-3Prescribed Anxiolytics'
Brand NameDru Elimination Half-Life for Older AdultsBenzodiazepines Al razolam Xanax 9-20 hours
Chlordiazepoxide Librium 5-30 hours, with short- and long-actingactive metabolites
Diazepam Valium 20-50 hours, with short- and long-actingactive metabolites effective up to 200hours
Lorazepam Ativan 18-24 hours; clearance may be reduced inolder adults
Oxaze am Serax 3-25 hoursSerotonin a onist Bus iron BuS ar 1-11 hours
'Refer to product information insert for each drug as to its suitability for use in older adults.
An estimated 95 percent of benzodiazepineprescriptions for older adults in this country areordered for anxiety and insomnia, with only 5percent used as adjuncts for general anesthesia,as muscle relaxants, or as anticonvulsants (Rayet al., 1993). Numerous studies, including the1990 American Psychiatric Association Task
Force report, have concluded that the vastmajority of use of these agents is appropriate,with only occasional overprescribing byphysicians for some patient subgroups ormisuse by patients (Salzman, 1990, 1993b;
Winger, 1993; Woods and Winger, 1995). Evenamong the small group of respondents tohousehold surveys who have acknowledgedtaking benzodiazepines that were not prescribedfor them (less than 6 percent), the vast majority
borrowed pills from significant others and usedthem for symptom relief, not recreationalpurposes. Moreover, worldwide experiencewith the short-term use of benzodiazepines torelieve acute anxiety, situational stress, andtransient insomnia indicates that thesemedications are unusually safe and efficacious,with very little liability for dose increases,prolonged use, or addictive dependence(Salzman, 1993b).
36
Although most people use benzodiazepinesfor short periods of time without developingproblems, others take them past the point wherethey are effective and thus are at risk for adverseeffects including tolerance and abuse. By 1990,as many as a fourth of anxiolytic users had takenthese medications for a year or more (Winger,1993). Several studies in the United States andBritain confirm that long-term users (for a yearor more) of benzodiazepines are likely to beolder than age 45 and female with substantial
psychological stress, dysphoric or depressivesymptoms, and multiple chronic physicalillnesses or somatic problems (Salzman, 1993b;
Winger, 1993). Benzodiazepine use for longerthan 4 months is of particular concern amongolder adults. The physiological aging processdecreases the body's ability to absorb andmetabolize drugs, allowing the drug toaccumulate more rapidly than in youngerpeople and increase the likelihood of toxicityand adverse effects. Benzodiazepines havevariable rates of absorption, with metabolismoccurring primarily in the liver. Because thelonger acting benzodiazepines have activemetabolites, some of which have very long half-livesup to 200 hours in the case offlurazepamthe duration of action is often
59

longer than expected. They are also more likelyto produce residual sedation and other adverseeffects such as decreased attention, memory,cognitive function, and motor coordination andincreased injurious falls or motor vehicle crashes(Weiss, 1994; Solomon et al., 1993; Fouts and
Rachow, 1994; Ray et al., 1993; Winger, 1993).
By contrast, some shorter actingbenzodiazepines are not as likely to producetoxic or dependence-inducing effects withchronic dosing. One reason is that these drugshave no active metabolites. Furthermore,because the oxidative pathway is often impairedin older adults and in those with liver disease, itis best to choose drugs that are not metabolizedby this pathway. Such drugs include oxazepam(Serax) and lorazepam. Because of theseunpleasant and potentially hazardous sideeffects of many benzodiazepines, the Panelrecommends caution in selecting the mostappropriate benzodiazepine for elderly patients.
Unfortunately, both long- and short-actingbenzodiazepines tend to result in physiologicaldependence, even when these medications aretaken at therapeutic doses and for as short aperiod as 2 months (Woods and Winger, 1995).Many of the most unpleasant withdrawal effectscan be alleviated by gradually tapering the doserather than stopping it abruptly. Even if thedose is tapered, however, withdrawalsymptoms are experienced by 40 to 80 percent ofpeople who discontinue benzodiazepines after 4to 6 months of regular use (Miller et al., 1985;Speirs et al., 1986). Such symptoms as anxiety,agitation, lethargy, nausea, loss of appetite,insomnia, dizziness, tremor, poor coordination,difficulty concentrating, depersonalization, orconfusion may occur after stopping either longor short half-life benzodiazepines. Symptomsusually peak toward the end of the tapereddiscontinuation and disappear altogether within3 to 5 weeks (Winger, 1993; Rickels andSchweizer, 1993). In a few psychiatric patients,
Prescription Drugs
the withdrawal syndrome has been known topersist for several months (Solomon et al., 1993).
The rebound effects experienced inwithdrawal usually mimic the originalsymptoms for which the benzodiazepine wasprescribed (e.g., anxiety, insomnia, panic).Those effects occur in as many as one-third toone half of patients after even 1 or 2 months ofbenzodiazepine therapy, may be more intensethan before treatment began, and are frequentlymisperceived by frightened patients as a returnof the initial problem (Rickels and Schweizer,1993; Salzman, 1993b). Rebound effects,however, are sudden and transient, whereas arelapse entails a gradual but persistent return ofthe original symptoms that may continueunabated unless treated again withbenzodiazepines or other appropriatemedications (Rickels and Schweizer, 1993).
Unfortunately, misperceived rebound effectsmay lead some patients to self-medicate bysupplementing doses during withdrawal unlessthe tapering is sufficiently gradual to amelioratesymptoms and the patient is counseled thatthese rebound effects are transient and to beexpected (Rickels and Schweizer, 1993). Unlikewithdrawing from alcohol, however, thedifficulty in abstaining during the acute phase ofbenzodiazepine withdrawal is not followed byany further craving once the patient is drug-free(Winger, 1993). It appears that most patientswithdrawn from benzodiazepines can maintainabstinence.
The question of whether the benefitsoutweigh the disadvantages of chronicbenzodiazepine therapy is far from settled.Followup studies have found that more thanhalf of patients (50 to 66 percent) treated withbenzodiazepine anxiolytics or hypnoticsexperience a relapse of the original symptomswithin a year of discontinuing benzodiazepineuse (Atkinson et al., 1992). Half of these patientsresume use of benzodiazepines. Longerfollowup studies indicate that a majority
GO37

Chapter 3
eventually resume use, whether intermittentlyor chronically (Finlayson, 1984). The reasons fordiscontinuation have to be examined in anindividually calculated riskbenefit model byweighing the linkage between untreated anxietyor insomnia and alcoholism, depression, andsuicide (Woods and Winger, 1995). Manyresearchers, moreover, argue that anxiety isundermedicated with benzodiazepines and thatas many as 60 percent of patients who havelegitimate medical or psychological reasons forhigh levels of stress and anxiety do not seek orobtain relief for these conditions (Salzman,1993a).
Salzman (1993b) makes a compelling casethat chronic benzodiazepine use may beappropriate for patients he characterizes asolder (but not necessarily elderly), with anumber of chronic illnesses and compromisedphysical and/or psychosocial functioning. Thisgroup includes patients who are often in pain,dysphoric, or depressed as well as anxious,suffering from insomnia, or willing to visit theirphysicians. Chronic users of this type mayexperience side effects from benzodiazepines orincur mild interactions with other drugs they aretaking, but they are not purposefully abusingpsychoactive drugs or mixing them with
alcohol. Benzodiazepine prescriptions seem tobe clearly indicated for patients withoverwhelming stress or anxiety thatcompromises functioning for short periods oftime and for chronically medically ill, usuallyolder, patients (Salzman, 1993b).
One new drug, the serotonin agonistbuspirone, is a promising alternative tobenzodiazepines for the treatment of chronicanxiety with associated depressive symptoms.It apparently produces minimal sedative effectsand little or no impairment of cognitive orpsychomotor functioning, is not synergistic withmost other psychoactive drugs or alcohol, andhas little observed potential for causingtolerance or dependence, withdrawal, or
38
overdose. Buspirone does not have the musclerelaxant or anticonvulsant properties ofbenzodiazepines. However, it does have someside effects at higher doses, and it is notimmediately or invariably effective inameliorating anxiety. The efficacy of buspironefor older patients is still being examined; it mayprecipitate some manic effects. Also, dosagesshould be reduced for those with decreasedrenal or hepatic functioning (Winger, 1993;Weiss, 1994; Ray et al., 1993; Bezchlibnyk-Butlerand Jeffries, 1995).
Sedative/HypnoticsSleep disturbances are a common complaintamong older adults, occurring in approximatelyhalf of Americans over age 65 who live at homeand in two-thirds of those in long-term carefacilities. Complaints about insomnia, whichincrease with advancing age, occur inconjunction with a variety of psychiatric,medical, or pharmacological problems as well asthe changing circadian rhythms that accompanythe aging process (National Institutes of Health,1990; Fouts and Rachow, 1994; Mullan et al.,1994).
As previously noted, benzodiazepines havereplaced older and more toxic hypnotics (e.g.,secobarbital, ethchlorvynol, glutethimide),which have a high addiction liability and
difficult-to-treat overdose potential and whichalso tend to accumulate in older adults withchronic dosing as their capabilities for drugabsorption and elimination diminish (Solomonet al., 1993; Bezchlibnyk-Butler and Jeffries,
1995). Nearly two out of five prescriptions forbenzodiazepines (38 percent). in 1991 werewritten for older patients (National Institutes ofHealth, 1990; Fouts and Rachow, 1994). As withanxiolytics, the shorter acting hypnoticbenzodiazepines are generally favored overlonger acting ones that tend to accumulate inolder adults and produce undesirable effects inthe central nervous system. Today, the most
61

commonly prescribed hypnotic benzodiazepinesare oxazepam, temazepam, triazolam, andlorazepam (Fouts and Rachow, 1994).
Unfortunately, hypnotic benzodiazepines,like the anxiolytics, also tend to be prescribedfor longer than needed for efficacy, a situationthat leads to the well-known drawbacks ofwithdrawal and rebound insomnia (Fouts andRachow, 1994). In 1990, for example, 23 percent
of adults who used benzodiazepine hypnotics(mostly the short-acting triazolam) had usedthem nightly for at least 4 months (Woods andWinger, 1995).
Figure 3-4 displays information about somesedative/hypnotics frequently prescribed forinsomnia, listing the generic name, the commontrade name, and the elimination half-life orexpected duration of action in the body. The
Prescription Drugs
commonly prescribed oxazepam and lorazepamare listed with the benzodiazepine anxiolytics.
Although aging changes sleep architecture,decreasing the amount of time spent in thedeeper levels of sleep (stages three and four)and increasing the number and duration ofawakenings during the night, these new sleeppatterns do not appear to bother most medicallyhealthy older adults who recognize and acceptthat their sleep will not be as sound or as regularas when they were younger (National Institutesof Health, 1990; Mullan et al., 1994). Rather,insomnia complaints among older adults areusually associated with a secondary medical orpsychiatric disorder, psychosocial changes andstressors, or the use of medications that interferewith sleep (National Institutes of Health, 1990;Mullan et al., 1994).
Class
Commonly
Drug
Figure 3-
Prescribed Sedative/Hypnotics', . ,. ,
Brand Name
;-t,-, 1,; .,, 1c):,;11,-,..;, 1: 4,-(. b. t,
I tC, -., ....1 . 1 `,0 a t; I ,Y1'=.Vt .1 cr tl',1-;.;.. 1.1- iilElimination Half-Life for Older Adults
Benzodiazepines Flurazepam Dahnane 72 hours, with short- and long-acting activemetabolites
Prazepam Centrax Less than 3 hours, with long-acting activemetabolites
Quazepam Doral 25-41 hours, with long-acting activemetabolites
Temazep am Restoril 10-20 hours
Triazolam Halcion 2-6 hours, with reports of clinical effects upto 16 hours following a single dose
Imidazopyridine Zolpidem Ambien 1.5-4.5 hours (longer in older adults)
Chloralderivatives
Chloral hydrate Noctec 4-8 hours (loses effect in 2 weeks)
Antihistamines Hydroxyzine Atarax 1-3 hours
Diphen-hydramine
Benadryl
(over-the-counter)
8-10 hours
Doxylamine Unisom(over-the-counter)
8-10 hours
'Refer to product information insert for each drug as to its suitability for use in older adults.
6439

Chapter 3
Among the drugs causing poor sleeppatterns are the antidepressant monoamineoxidase (MAO) inhibitors and SSRIs; anti-Parkinson medications; appetite suppressors;the beta-blocker for hypertension, propranolol(Inderal); and alcohol. Sleep apnea, inparticular, may be aggravated by the use of abenzodiazepine (Culebras, 1992). Insomnia hasalso been related to depression and anxiety,Alzheimer's disease, Parkinson's disease,cardiovascular disease, arthritis, pain, urinaryproblems, prostate disease, pulmonary disease,hyperthyroidism, and endocrinopathies. Sleepdisruption as well as anxiety commonlyaccompany other psychosocial adjustments suchas retirement, bereavement, dislocation, ortraumatic situations (National Institutes ofHealth, 1990; Mullan et al., 1994). Sleep
complaints are also associated with femalegender, living alone or in a nursing facility,activity limitations, and sleep habits such asexcessive daytime napping (Mullan et al., 1994).
With respect to treatment of insomnia, a 1990National Institutes of Health consensusdevelopment conference statement pertaining tosleep disorders of older adults specificallycautioned against relying on hypnoticbenzodiazepines as the mainstay for managinginsomnia (National Institutes of Health, 1990).Although these medications can be useful forshort-term amelioration of temporary sleepproblems, no studies demonstrate their long-term effectiveness beyond 30 continuous nights,and tolerance and dependence develop rapidly(Mullan et al., 1994; National Institutes ofHealth, 1990; Salzman, 1993b). In fact,
symptomatic treatment of insomnia withmedications should be limited to 7 to 10 dayswith frequent monitoring and reevaluation if theprescribed drug will be used for more than 2 to3 weeks. Intermittent dosing at the smallestpossible dose is preferred, and no more than a30-day supply of hypnotics should beprescribed. Given the changes associated with
40
drug metabolism among older patients, allhypnotic medications should be used withcaution, especially those with long half-lives(National Institutes of Health, 1990; Fouts andRachow, 1994; Mullan et al., 1994). As with theanxiolytic benzodiazepines, withdrawal effectssignifying physiological dependence arecommon concomitants of precipitousmedication discontinuation, especially of theshort-acting compounds. The REM sleeprebound effects from abruptly stopping achronically administered benzodiazepinehypnotic can last 1 to 3 weeks or longer (Mullanet al., 1994; Fouts and Rachow, 1994).
Furthermore, sedative/hypnotics, as well asbenzodiazepines, used for sleep induction maycause confusion and equilibrium problems inolder users who get up frequently during thenight (e.g., to go to the bathroom). When
treating older adults, situations likely to increasethe incidence of falls with subsequent injuryshould be avoided at all costs. In addition,drugs taken at night for sleep induction will bepotentiated by any alcohol the individual hasused during the evening.
Instead of relying on drugs as a first line ofapproach, treatment should initially be directedtoward any underlying disorder (e.g.,depression, alcoholism, panic states, anxiety)(Mullan et al., 1994). Having the patient keep asleep diary may be useful for obtaining a moreobjective clarification of sleep patterns becauseinsomnia is notoriously subjective. Also, theimportance of good sleep hygiene cannot beunderestimated (Mullan et al., 1994; NationalInstitutes of Health, 1990; Fouts and Rachow,1994). Patients may need to be educated aboutregularizing bedtime, restricting daytime naps,using the bedroom only for sleep and sexualactivity, avoiding alcohol and caffeine, reducingevening fluid intake and heavy meals, takingsome medications in the morning, limitingexercise immediately before retiring, andsubstituting behavioral relaxation techniques

(National Institutes of Health, 1990; Fouts andRachow, 1994).
Withdrawal from sedative/hypnoticmedications (as well as anxiolytics) should becarefully monitored. Withdfawal ischaracterized by increased pulse rate, handtremor, insomnia, nausea or vomiting, andanxiety. A grand mal seizure may occur in asmany as 20 to 30 percent of dependent persons ifwithdrawal symptoms are untreated.Hallucinations similar to those associated withalcoholic delirium tremens (DTs) may also bepresent.
Several precautions about particular drugsshould be noted. Specifically, triazolam rapidlyachieved notoriety and was banned in theUnited Kingdom and other European countriesafter its 1979 introduction with accompanyingreports of bizarre, idiosyncratic panic anddelusional reactions as well as adverse sideeffects of confusion, agitation, and anxiety(Woods and Winger, 1995; Winger, 1993). Moreserious side effects are still more consistentlyand more frequently reported with triazolamthan with temazepam, a similar short-actinghypnotic benzodiazepine (Woods and Winger,1995). It appears that older patients are morelikely than younger ones to experience increasedsedation and psychomotor impairment with thismedication and to report an increased incidenceof adverse behavioral reactions if the dose isgreater than 0.125 mg (Fouts and Rachow, 1994).
Another recently introduced but popularhypnotic, zolpidem (Ambien), does not have theanxiolytic, muscle relaxant, or anticonvulsantproperties of benzodiazepines. It has beentouted as a safer sleep medication because itdoes not disrupt physiological sleep patterns atlow doses and appears to have relatively mild,dose-related adverse effects. However,zolpidem is much more costly than thebenzodiazepines, an important consideration forlow-income older patients. Also, lower doses(beginning at 5 mg) must be used in older
Prescription Drugs
patients to avoid hazardous confusion and falls(Winger, 1993; Fouts and Rachow, 1994; Ray et
al., 1993; Bezchlibnyk-Butler and Jeffries, 1995).
Because of its recent introduction, there islimited information available on the possibleundesirable effects of zolpidem for the olderpatient.
Several antihistamines, usually used for reliefof allergies and available as over-the-countermedications, are also taken as sleeping aidsbecause of their sedating properties (e.g.,Benadryl). Antihistamines are also combinedwith over-the-counter analgesics and marketedas nighttime pain medications (e.g., TylenolPM). However, older adults appear to be moresusceptible to adverse anticholinergic effectsfrom these substances and are at increased riskfor orthostatic hypotension and central nervoussystem depression or confusion. In addition,antihistamines and alcohol potentiate oneanother, further exacerbating the aboveconditions as well as any problems with balance.Because tolerance develops within days orweeks, these antihistamines have questionableefficacy and are not recommended for olderadults who are living alone (Ray et al., 1993;Fouts and Rachow, 1994; National Institutes ofHealth, 1990; Bezchlibnyk-Butler and Jeffries,
1995).
Opiate/Opioid AnalgesicsAn estimated 2 to 3 percent ofnoninstitutionalized older adults receiveprescriptions for opioid analgesics (Ray et al.,1993). Opioids are undeniably effective formanagement of severe pain such as thatoccurring after surgery and serious trauma andperiodically in some medical illnesses (e.g., gout,inflammatory bowel disease). This acute pain isusually short-lived and resolves within days toweeks at most. Opioid analgesics are also usedto treat cancer-related pain, which isexperienced by nearly all patients withadvanced disease and by one-third-to-one-half
6 441

Chapter 3
of patients in earlier stages. The use of opioidmedications for these purposes is widelyacceptable in medical practice (Portenoy, 1993).
In addition to the rapid development oftolerance and physiological dependence, otherproblems are associated with opioidprescriptions for older patients. Opioid doserequirements decrease with age: The onset ofaction is slowed by the decreased rate ofgastrointestinal absorption of orally ingestednarcotics, and the duration of action is longerbecause of older patients' decreased metabolismand liver functioning. Older adults also havemore adverse side effects because of changes inreceptor sensitivity with age. The less potentopioids, codeine and propoxyphene (Darvon),cause sedation and mild, dose-relatedimpairment of psychomotor performance,whereas the more potent opioids, oxycodone(Percodan) and intramuscular meperidine(Demerol), induce substantial impairment ofvision, attention, and motor coordination. Noapparent relation between age and sedation isobserved in patients treated with morphine andpentazocine (Talwin) (Solomon et al., 1993; Rayet al., 1993).
The prescribing of opioid analgesics forchronic nonmalignant pain (not associated withcancer) is a controversial issue. Although long-term treatment of chronic pain with opiates oropioids has not traditionally been accepted byeither patients or physicians, a growing body ofevidence suggests that prolonged opioidtherapy may be both effective and feasible.Convincing and persuasive testimony has alsobeen given by a number of clinicians andmedical associations regarding the successfulmanagement of lengthy opioid treatment inpatients with chronic nonmalignant pain(Portenoy, 1993).
These advocates note that both acute andchronic pain in the United States is more usuallyunder- than overmedicated for a variety ofpatient- and provider-related reasons, not the
42
least of which is fear of addiction. In addition,patients may believe that stoicism is virtuous,that pain is an inevitable and intractable part ofthe illness or disease, or that prescribedmedications are too costly, too complex tomanage, or likely to have numerous andundesirable side effects. Clinicians also mayunderprescribe because of fear of sanctions(Portenoy, 1993).
The disagreements among cliniciansregarding management of long-term opioidtherapy reflect different perspectives regardingthe dangers and persistence of psychologicaldependence following physical addiction andthe potential for psychosocial disintegration intoan addictive, drug-abusing lifestyle. Manyresearchers point out that clinical populationscan be successfully withdrawn from opiates andopioids without dire consequences. One study,for example, found that only 4 of nearly 12,000
patients who were prescribed morphine for self-administration became addicted (Chapman andHill, 1989). Other practitioners argue thatpatients' quality of life improves (e.g., lessmedical care utilization) if they are kept onopioids and manage pain without addiction(Finlayson et al., 1986a, 1986b). Also, opioid
analgesics are usually contraindicated if thepatient has a history of alcoholism or anothersubstance abuse or dependence disorder.
Opioid withdrawal is accompanied byrestlessness, dysphoric mood, nausea orvomiting, muscle aches, tearing and yawning,diarrhea, fever, and insomnia. Although opioidwithdrawal is uncomfortable, it is not life-threatening or particularly dangerous comparedwith untreated withdrawal frombenzodiazepines.
Figure 3-5 displays information about someof the more commonly prescribed opiate/opioidanalgesics, listing the generic and brand nameswith comments about indications and effects.
65

Interactions ith OtherDrugs and With AlcoholDrugdrug and drugalcohol interactions are ofincreased importance in older adults for severalreasons. Because older adults take moreprescription and over-the-counter drugs thanyounger adults and many continue to drink, thepotential for interactions is enhanced. Aninteraction is likely to be more problematic in anolder adult because of slowed metabolic andclearance mechanisms, resulting in a delay in
Prescription Drugs
the resolution of the unfavorable reaction. Theaging body is also more susceptible to adverseinteractions. The presence of chronic diseasestends to increase the number of medicationsused by older adults. Thus the risk for druginteractions is increased in those for whom anadverse reaction would be most dangerous.Further research is needed on specific drugdrug interactions and on drug-alcoholcombinations that can be deadly, such as alcoholand diazepam.
Class
Commonly
Dru
Figure 3-5
Prescribed opiate/Opiold
Brand Name
Analgesics'
CommentsOpiates Methylmorphine
Mor hineCommon ingredient of analgesics.
Codeine e.g., Tylenol III,
Robitussin A-CCommon ingredient of analgesics andantitussives. Can cause sedation and mild,dose-related impairment of psychomotorcoordination.
Opioids(synthetic)
Hydrocodone Lortab Can produce dose-related respiratorydepression and irregular breathing if takenin lar:e amounts.
Meperidine Demerol Contraindicated if patient is taking MAOinhibitors.
Can produce psychomimetic effects andimpair vision, attention, and motorcoordination.
Oxycodone Percodan/Percocet
Can produce substantial impairment ofvision, attention, and motor coordination.
Propoxyphene Darvon Can produce sedation and mild, dose-relatedim airment of .s chomotor coordination.
Pentazocine Talwin Age does not appear to increase sedativeeffects.
'Refer to product information insert for each drug as to its suitability for use in older adults.
43

Chapter 3
Drug
Figure 3-6
DrugAlcohol Inte.ractions and Adverse EffectsAdverse Effect With Alcohol
AcetaminophenAnticoagulants, oral
Antidepressants, tricyclic
Aspirin and othernonsteroidal anti-inflammatory drugs
Barbiturates
Benzodiazepines
Beta-adrenergic blockers
BromocriptineCaffeine
Cephalosporins andChloramphenicol
Chloral hydrateCimetidine
Cycloserine
Digoxin
Disulfiram
GuanadrelGlutethimideHeparinHypoglycemics,
sulfonylureaTolbutamide,
chlorpropamideIsoniazid
Ketoconazole, griseofulvin
LithiumMeprobamateMethotrexate
MetronidazoleNitroglycerinPhenforminPhenothiazinesPhenytoin
QuinacrineTetracyclines
Severe hepatoxicity with therapeutic doses of acetaminophen in chronic alcoholicsDecreased anticoagulant effect with chronic alcohol abuse
Combined central nervous system depression decreases psychomotor performance,especially in the first week of treatment
Increased the possibility of gastritis and gastrointestinal hemorrhage
Increased central nervous system depression (additive effects)
Increased central nervous system depression (additive effects)Masked signs of delirium tremens
Combined use increases gastrointestinal side effects
Possible further decreased reaction time
Disulfiram-like reaction with some cephalosporins and chloramphenicol
Prolonged hypnotic effect and adverse cardiovascular effects
Increased central nervous system depressant effect of alcohol
Increased alcohol effect or convulsions
Decreased digitalis effect
Abdominal cramps, flushing, vomiting, hypotension, confusion, blurred vision, andpsychosis
Increased sedative effect and orthostatic hypotensionAdditive central nervous system depressant effectIncreased bleeding
Acutely ingested, alcohol can increase the hypoglycemic effect of sulfonylurea drugs;
chronically ingested, it can decrease hypoglycemic effect of these drugs
Disulfiram-like reaction
Increased liver toxicity
Disulfiram-like reaction
Increased lithium toxicitySynergistic central nervous system depression
Increased hepatic damage in chronic alcoholics
Disulfiram-like reaction
Possible hypotension
Lactic acidosis (synergism)
Additive central nervous system depressant activity
Acutely ingested, alcohol can increase the toxicity of phenytoin; chronically ingested,
it can decrease the anticonvulsant effect of phenytoin
Disulfiram-like reaction
Decreased effect of doxycycline
Source: Korrapati and Vestal, 1995.
4467

Any use of drugs and alcohol carries risk,abuse of these substances raises the risk, andmultiple drug abuse (polypharmacy) furtherincreases the risk. A recent study documentedthe many possible unfavorable reactionsbetween prescription drugs and alcohol(Korrapati and Vestal, 1995) (see Figure 3-6).
For example, chronic alcoholics who use eventherapeutic doses of acetaminophen mayexperience severe hepatoxicity. Alcohol canincrease lithium toxicity and enhance centralnervous system depression in persons takingtricyclic antidepressants. High doses ofbenzodiazepines used in conjunction withalcohol or barbiturates can be lethal (AmericanPsychiatric Association, 1994).
Drugdrug interactions can be extremelydangerous and dramaticthe combination of
Prescription Drugs
meperidine with an MAO inhibitor can causemarked blood pressure fluctuations, excitability,rigidity, hyperreflexia, hyperthermia, coma, andeven death. More often, however, suchinteractions produce subtle or mild quantitativeeffects. A change in sleep, appetite, or anincrease in anxiety may be the only sign andcould lead a clinician to increase the dose of amedication that is already contributing to theadverse reaction. To use psychoactiveprescription and over-the-counter drugs wisely,both physicians and consumers need tounderstand how the aging process influencesresponses to medication and to recognize howvulnerable older adults are both to their misuseand abuse.
68.
45

I en-64kSS SS
Sc Asee-iinent
Although the vast majority of olderadults (87 percent) see physiciansregularly, their service providers
estimate that 40 percent of those who are at riskdo not self-identify or seek services forsubstance abuse problems on their own(Raschko, 1990). Moreover, they are unlikely tobe identified by their physicians despite thefrequency of contact. Because most older adultslive in the community and fewer than 5 percentolder than 65 live in nursing or personal carehomes, training supervisors in such residencesdoes not offer a reasonable strategy forincreasing problem identification. To ensurethat older adults receive needed screening,assessment, and intervention services, stepped-up identification efforts by health care providersand multitiered, nontraditional case-findingmethods within the community are essential(Raschko, 1990; De Hart and Hoffmann, 1995).
Most older adults see a medical practitionerseveral times per year, often for conditions thatlend themselves to collateral discussion of thepatients' drinking habits. Thus the primary caresetting provides an opportunity for screeningthat is currently underutilized, as is the hospital(Adams et al., 1992). Home health care
011, and
providers have unparalleled opportunities toobserve isolated, homebound seniors forpossible problems and, if substance abuse issuspected, administer a nonthreatening screen.
Identification of substance abuse amongolder adults should not be the purview of healthcare workers alone. Friends and family of olderadults and staff of senior centers, includingdrivers and volunteers who see older adults on aregular basis, are intimately acquainted withtheir habits and daily routines. Frequently theyare in the best position to detect thosebehavioral changes that signal a possibleproblem. Leisure clubs, health fairs, congregatemeal sites, Meals-On-Wheels, and senior daycare programs also provide venues in whicholder adults can be encouraged to self-identify.The National Council on Aging, for example,sponsors a depression awareness program foruse in senior programs that features acomputerized, self-administered depression test.The computer offers anonymity and immediateresults. It also avoids confidentiality problemsand seems to offer a feasible model for massscreening of drinking problems. See Figure 4-1for an example of successful community casefinding.
47

Chapter 4
Figure 4-1
Spokane's Gatekeeper Program .
The Elderly Services at the Community Mental Health Center in Spokane, Washington, created theGatekeeper Program to recruit, organize, and train nontraditional referral sources who may be incontact with at-risk older adults during their daily activities. The Gatekeepersapartment managers,meter readers, bank personnel, postal carriers, utility repair personnel, and othersare the ElderlyServices' eyes within the community. They are trained to identify at-risk older adults and providereferrals back to the program, which in turn will send a case manager and a nurse team leader to theindividual's home for an evaluation. The program integrates case management for older adults withmental health and substance abuse treatment services, with the Gatekeepers serving as the case-finding component. Overall, the Gatekeepers now account for 4 out of every 10 admissions to thismultidisciplinary in-home evaluation, treatment, and case management program. Nearly half of theolder adults treated specifically for substance abuse were referred by the Gatekeepers (Raschko, 1990).
In contrast to younger substance abuserswhose problems are frequently identified as aresult of an action initiated by a family member,spouse, employer, school, police, or the courts, asubstantial proportion of older adults' substanceabuse problems remains undetected. Unlesshealth, social service, and community serviceproviders understand that alcohol andprescription drugs can pose serious problemsfor older adults and take the initiative in gettingthem the help they need, quality of life will bediminished, independence compromised, andphysical deterioration accelerated.
Screening for Alcohol andPrescription Drug Abuse
Barriers to ScreeningAgeist assumptions, failure to recognizesymptoms, and lack of knowledge aboutscreening are among the barriers that inhibitfamily members, service providers, and othersconcerned about older adults from raising theissue of alcohol and prescription drug abuse.Although these are the two primary substancesof abuse now, providers are likely to see moremarijuana and other drug use among adultsover 60 in the coming years.
48 d0
Health care providers sometimes share theageist attitudes discussed in Chapter 1. Theymay not be trained to recognize signs ofsubstance abuse and furthermore may beunwilling to listen attentively to older patients.The latter type of provider often dismisses olderpatients' observations about their ownsymptoms and attempts at self-diagnosis andattributes all complaints or changes in healthstatus to the aging process.
Family members also can impede problemrecognition. Biases persist against perceivingolder adults as alcoholics or recognizing thatdrinking or prescription drugs, rather than ageor disease, may be a cause or chief contributor tosleep problems, mood changes, or memorydeficits (Finlayson, 1995b). Another assumptioninhibiting identification is the belief that olderadults do not respond to treatment, amisperception flatly contradicted by studiesshowing that older adults are more likely tocomplete treatment (Linn, 1978; Cartensen et al.,1985) and have outcomes that are as good as orbetter than those of younger patients whentreated as outpatients (Atkinson, 1995; in press).
Identifying an older abuser of alcohol orprescription drugs can also be complicated bythe number of other conditions with similarsymptoms. Warning signs can be easilyconfused with or masked by concurrent illnesses

and chronic conditions. For example, sleepproblems, falls, anxiety, or confusion can beattributed to a variety of nonalcohol-relateddiseases and disorders or dismissed assymptomatic of old age. Screeners who useamount and frequency levels appropriate foryounger adults as a gauge can also miss an olderadult's alcohol problem (see Chapter 2).
Finally, many health care and social serviceproviders are unaware that effective, validatedinstruments are available for screening olderadults or are intimidated by the prospect ofusing them. Many screens, moreover, take onlya few minutes to administer and require little orno specialized training to score and interpret.Screening instruments are discussed in moredetail below.
Who and When To ScreenIdeally, every 60-year-old should be screened foralcohol and prescription drug abuse as part of
Identification, Screening, and Assessment
his or her regular physical examination.However, problems can develop after thescreening has been conducted, and concurrentillnesses and other chronic conditions may maskabuse. Although no hard and fast rules governthe timing of screening, the Panel recommendsscreening or rescreening if the physicalsymptoms listed in Figure 4-2 are present or ifthe older person is undergoing major lifechanges or transitions such as those discussedbelow.
As older patients undergo key life transitionsor take on new and stressful roles, vulnerabilityto alcohol or prescription drugs may increase.Risk factor life transitions include menopause, anewly "empty nest," and approachingretirement. Assuming new roles such ascaretaker for an ailing relative or custodian ofyoung grandchildren also makes older adultsmore vulnerable. Any of these changes shouldtrigger an alcohol screen.
Figure 4-2
Physital Syniptom Screening Triggers.
Sleep complaints; observable changes in sleeping patterns; unusual fatigue, malaise, or daytimedrowsiness; apparent sedation (e.g., a formerly punctual older adult begins oversleeping and is notready when the senior center van arrives for pickup)
Cognitive impairment, memory or concentration disturbances, disorientation or confusion (e.g.,family members have difficulty following an older adult's conversation, the older adult is no longerable to participate in the weekly bridge game or track the plot on daily soap operas)
Seizures, malnutrition, muscle wastingLiver function abnormalities
Persistent irritability (without obvious cause) and altered mood, depression, or anxietyUnexplained complaints about chronic pain or other somatic complaintsIncontinence, urinary retention, difficulty urinatingPoor hygiene and self-neglectUnusual restlessness and agitationComplaints of blurred vision or dry mouthUnexplained nausea and vomiting or gastrointestinal distressChanges in eating habitsSlurred speechTremor, motor uncoordination, shuffling gaitFresuent falls and unex .lained bruisin:
7 4 49

Chapter 4
Introducing the Topic of ScreeningDepending on the setting, the topic of screeningcan be introduced in a number of ways. Selfadministered and self-scored mass screeningscan be a part of a larger presentation at anAmerican Association of Retired Persons orleisure club meeting on the topic of alcohol'seffects on older adults. Self-administered butmachine-scored computerized screens can beoffered as part of a similar program conductedat senior centers, retirement homes, or assistedliving residences with access to computers.
Visiting nurses and home health aides canintegrate a brief alcohol screen into the list ofhealth questions normally posed to patients. Forexample, in asking about medication, the healthcare provider could say, "We understand moretoday about the effects of even small amounts ofalcohol on medication, and I want to be sure thatnothing is interfering with your coumadin oraffecting your overall progress in any way.Let's review how much alcohol you're drinkingand take a look at all your medications."
It is preferable to use standardized screeningquestionnaires, but friendly visitors, Meals-On-Wheels volunteers, caretakers, and health careproviders also can interject screening questionsinto their normal conversations with older,homebound adults. Comfort with this line ofquestioning will depend on the person'srelationship with the older person and theresponses given; however, anyone who isconcerned about an older adult's drinkingpractices can try asking direct questions, such as
"Do you ever drink alcohol?""How much do you drink when you dodrink?"
m "Do you ever drink more than four drinks onone occasion?""Do you ever drink and drive?""Do you ever drink when you're lonely orupset?"
50
"Does drinking help you feel better [or get tosleep more easily, etc.]? How do you feel theday after you have stopped drinking?""Have you ever wondered whether yourdrinking interferes with your health or anyother aspects of your life in any way?"
oi "Where and with whom do you typicallydrink?" (Drinking at home alone signals at-risk or potentially abusive drinking.)"How do you typically feel just before yourfirst drink on a drinking day?""Typically, what is it that you expect whenyou think about having a drink?" (Note:Positive expectations or consequences ofalcohol use in the presence of negative affectand inadequate coping skills have beenassociated with problem drinking.)
If less direct questioning seems appropriate,other useful questions for identifyingproblematic alcohol or prescription drug useinclude
"Are you having any medical or healthproblems? What symptoms do you have?What do you think these mean? Have youfelt this way before?"
"Do you see a doctor or other health careprovider regularly? When was the last time?Do you see more than one? Why? Have youswitched doctors recently? Why?""Have you experienced any negative orunwanted events that altered the way youlived (in the last 5 years)? Any since we lastmet? How much of an impact did the eventhave on the way you lived or felt? Whatfeelings or beliefs did it cause or change? Doyou believe that you are coping with thechanges in a healthy fashion? How(specifically) do you manage (control) thecircumstances (consequences) of theproblem(s) or event(s)?"
"What prescription drugs are you taking?Are you having any problems with them?May I see them?" (This question will need to
7 2

be followed by an examination of the actualcontainers to ascertain the drug name,prescribed dose, expiration date, prescribingphysician, and pharmacy that filled eachprescription. Note whether there are anypsychoactive medications. Ask the patient tobring the drugs in their original containers.)"Where do you get prescriptions filled? Doyou go to more than one pharmacy? Do youreceive and follow instructions from yourdoctor or pharmacist for taking theprescriptions? May I see them? Do youknow whether any of these medicines caninteract with alcohol or your otherprescriptions to cause problems?""Do you use any over-the-counter drugs(nonprescription medications)? If so, what,why, how much, how often, and how longhave you been taking them?"
Nonmedical caretakers, volunteers, and aidesmay opt to ask only the four CAGE questions,reproduced in Figure 4-3 and discussed in theScreening Instruments section. If the older adultanswers yes to any of the four, refer to aclinician for evaluation. If the questionersuspects that prescription drug abuse may beoccurring and the older adult is defensive abouthis or her use, confused about variousprescription drugs, seeing more than one doctor,or using more than one pharmacy, a clinicianshould probably be notified to probe further.Other warning signs that may emerge inconversation and should prompt a more in-depth screen or an assessment include
Excessively worrying about whetherprescription psychoactive drugs are "reallyworking" to alleviate numerous physicalcomplaints; complaints that the drugprescribed has lost its effectiveness over time(evidence of tolerance)Displaying detailed knowledge about aspecific psychoactive drug and attaching
Identification, Screening, and Assessment
great significance to its efficacy and personalimpactWorrying about having enough pills orwhether it is time to take them to the extentthat other activities revolve around thedosage schedule
O Continuing to use and to request refills whenthe physical or psychological condition forwhich the drug was originally prescribed hasor should have improved (e.g., prescriptionof sleeping pills after the death of a lovedone); resisting cessation or decreasing dosesof a prescribed psychoactive drugComplaining about doctors who refuse towrite prescriptions for preferred drugs, whotaper dosages, or who don't take symptomsseriouslySelf-medicating by increasing doses ofprescribed psychoactive drugs that aren't"helping anymore" or supplementingprescribed drugs with over-the-countermedications of a similar type
ES Rating social events by the amount of alcohol
dispensedEll Eating only at restaurants that serve alcoholic
beverages (and wanting to know whetherthey do in advance)
Ell Withdrawing from family, friends, andneighbors
E Withdrawing from normal and life-longsocial practicesCigarette smokingInvolvement in minor traffic accidents(police do not typically suspect older adultsof alcohol abuse and may not subject them toBreathalyzerTM and other tests for sobriety)
Sleeping during the dayEg Bruises, burns, fractures, or other trauma,
particularly if the individual does notremember how and when they wereacquiredDrinking before going to a social event to"get started"; gulping drinks, guarding the
'7 51

Chapter 4
supply of alcoholic beverages, or insisting onmixing own drinksChanges in personal grooming and hygieneExpulsion from housingEmpty liquor, wine, or beer bottles or cans inthe garbage or concealed under the bed, inthe closet, or in other locations.
Asking Screening QuestionsScreening questions should be asked in aconfidential setting and in a nonthreatening,nonjudgmental manner. Many older adults areacutely sensitive to the stigma associated withalcohol and drug abuse and are far more willingto accept a "medical" as opposed to a"psychological" or "mental health" diagnosis asan explanation for their problems. Prefacingquestions with a link to a medical condition canmake them more palatable. For example, "I'mwondering if alcohol may be the reason whyyour diabetes isn't responding as it should," or,"Sometimes one prescription drug can affecthow well another medication is working. Let'sgo over the drugs you're taking and see if wecan figure this problem out." It is vitallyimportant to avoid using stigmatizing terms likealcoholic or drug abuser during these encounters.
Another technique that may help whentalking with older adults is active listening(Egan, 1994). The four components of activelistening are (1) observing and reading theperson's nonverbal behaviorposture, facialexpressions, movement, and tone of voice; (2)listening to and understanding the person'sverbal communication; (3) listening in context,that is, to the whole person in the context of thesocial settings of his or her life; and (4) listeningto sour notes, that is, things the person says thatmay have to be challenged. Motivationalinterviewing techniques also can be appliedwhen screening older adults. Essentially thisapproach, which is described in more detail inChapter 5, assumes that the patient is bothcapable of and responsible for initiating needed
52
changes. Motivational interviewing isnonconfrontational, egalitarian, and supportive.
When screening anyone, especially olderadults, empathy is crucial. However, inattempting to he nonconfrontational andcircumspect, it is also important to avoid usingeuphemisms that minimize the problem. Olderadults with alcohol and prescription drugproblems are just as likely to engage in denialand rationalization as younger adults; thosewho are inadvertently misusing a prescriptiondrug or who are unaware that their customarydrink before dinner may now be causingproblems are unlikely to be defensive aboutacknowledging the need to change.
Cognition and Collateral ReportingImpaired cognition interferes with screening,making it difficult to obtain complete andaccurate answers. Although it is important torespect the older adult's autonomy, collateralparticipation from family members or friendsmay be necessary in situations where a coherentresponse is unlikely. In this case, the screenershould first ask for the older adult's permissionto question others on his or her behalf. Ifpossible, the screen should be administered tocollaterals in private, using a nonconfrontationalapproach. "I'm concerned about your father'sdeteriorating condition and wonder if his use ofalcohol may be having a negative impact. Haveyou or anybody else in the family had anyconcerns about his drinking?" Becausecircumstances differ within families, familymembers may not know or may be unwilling torespond honestly to that query. Anotherquestion that skilled clinicians find useful incollateral screening is, "Has anybody in yourfamily ever had a problem with drinking?" Apositive response suggests that a problem mayexist and that more in-depth questioning shouldfollow.
Sometimes collateral screening unleashes afamily member's simmering anger toward the
74

older adult for both past and current alcohol-related behavior. It is important to be alert tothis possibility and to be prepared to work withthe family member to discourage aconfrontation with the older adult when thescreen concludes.
Screening InstrumentsThe CAGE Questionnaire (Ewing, 1984) and theMichigan Alcoholism Screening TestGeriatricVersion (MAST-G) (Blow et al., 1992a) are twowell-known alcohol screening instruments thathave been validated for use with older adults.One of the most widely used alcohol screens, theCAGE consists of four questions, can be self-administered even by those with low literacyreading skills (see Figure 4-3), and can bemodified to screen for use of other drugs.Positive responses on the CAGE are for lifetimeproblems, not current ones. Beforeadministering the CAGE, the MAST-G, or anyother screen, ascertain that the person doescurrently drink alcohol and that the questionsthat are endorsed are for problems that theyhave experienced recently, usually within thelast year.
Figure 4-3
The CAGE Questionnaire
1. Have you ever felt you should cut down onyour drinking?
2. Have people annoyed you by criticizing yourdrinking?
3. Have you ever felt bad or guilty about yourdrinking?
4. Have you ever had a drink first thing in themorning to steady your nerves or to get ridof a hangover (eye opener)?
Scoring: Item responses on the CAGE are scored0 for "no" and 1 for "yes" answers, with ahigher score an indication of alcohol problems.A total score of 2 or greater is consideredclinically significant.Source: Ewing, 1984.
Identification, Screening, and Assessment
Although two or more positive responses areconsidered indicative of an alcohol problem, apositive response to any one of these questionsshould prompt further exploration among olderadults. The CAGE is most effective inidentifying more serious problem drinkers,including those with abuse and dependence,and less effective for women problem drinkersthan their male counterparts.
The MAST-G was developed specifically forolder adults (see Figure 4-4) and has highsensitivity and specificity among older adultsrecruited from a wide range of settings,including primary care clinics, nursing homes,and older adult congregate housing locations.
Although the Alcohol Use DisordersIdentification Test (AUDIT) (Babor et al., 1992)
has not been evaluated for use with older adults,it has been validated cross-culturally. Becausethere are few culturally sensitive screeninginstruments, the AUDIT (in the opinion of theConsensus Panel) may prove useful foridentifying alcohol problems among oldermembers of ethnic minority groups (seeAppendix B).
Laboratory tests are generally used only tosupplement the screens detailed above(Beresford et al., 1990; Finlayson and Hurt, inpress). Some researchers have found, however,that certain abnormalities associated withalcoholism appeared more often amongalcoholics older than 64 than among youngeralcoholics. Those abnormalities appeared intests of mean corpuscular volume, uric acid,serum albumin, mean corpuscular hemoglobin,and aspartate aminotransferase (Hurt et al.,1988).
Communicating PositiveScreening ResultsTo ease the process of communicating positivescreening results to older patients, the Panelrecommends the following approach:
7 5 53

Chapter 4
Describe the impact that alcohol orprescription drug abuse is having on theolder adult's health or functional status:"The screening results indicate that alcoholmay be having a negative effect on yourblood pressure."
o Immediately follow up by noting: "This isvery treatable. Cutting down on the amountyou drink" or "giving up drinkingaltogether" or "reducing your use ofchlordiazepoxide (Librium)" or "using othermethods to help you sleep . . . will help youmaintain your independence" or "help keepyou out of a nursing home" or "decrease thelikelihood of future hip fractures" or "keepyou from getting so confused." In otherwords, spell out how reduction or cessationof use will improve the person's life. Mostproblem drinkers cannot address theirproblems by reducing use, so emphasize theimportance of abstinence by sayingsomething like: "Though I stronglyrecommend you stop altogether, cuttingdown is a good start."Present the options for addressing theproblem: If the problem seems severe, "I'dlike to do a complete assessment (or referyou to someone for assessment) so we knowhow to proceed"; or if the problem appearsto be in the early stages of development, "I'dlike to see you change your drinking habitsto no more than one beer (drink) per day.We'll monitor your progress over the nextfew weeks and see if this will help with yourhypertension." This is a good time to explorethe patient's willingness to change byadding, for example, "Would you be willingto change your drinking habits if the otherproblems we have discussed improve?"Occasionally, a situation may appear dire,and the clinician suspects that the older adult
54
needs to be detoxified. In this case,admission to an inpatient unit fordetoxification may be the most prudentchoice. Referral to an outpatientdetoxification center that can monitor theperson daily is appropriate if there is socialsupport at home.
Before discussing results with an older adult,clinicians must be prepared with informationabout community resources available to assist incoping with this problem (e.g., meeting dates,times, and locations of Alcoholics Anonymousand other self-help recovery groups whosemembership is largely 55 and older; contact andeligibility information for treatment programsthat respond to the special needs of olderadults); the older adult's available supports (e.g.,Is transportation available? Is the recommendedprogram affordable or covered by insurance?);and the older adult's special needs (e.g., Is theprogram bilingual or wheelchair accessible?).See Chapter 5 for more on treatment options. Inaddition, a strategy for responding to denial orrefusal to follow through with a plan of actionshould be in place. With the agreement of anolder adult involved in a self-help group ortreatment program, clinicians can broker anintroduction to a peer "who's been there."Frequently, these "veterans" will accompanyprospective members to meetings and mentorthem through the treatment process.
For some older adults coming to grips withan alcohol or prescription drug problem,repeated contacts will be necessary before theyare willing to cooperate with a referral.Clinicians have observed that this process isakin to planting and nurturing a seed. Bringingthe seed to fruition, however, ultimatelydepends on the older adult.
76

Identification, Screening, and Assessment
Figure 4-4-
Michigan Alcoholism Screening TestGeriatric Version; (MAST-C)
1. After drinking have you ever noticed an increase in your heart rate or beating in your
chest?2. When talking with others, do you ever underestimate how much you actually drink? YES NO
3. Does alcohol make you sleepy so that you often fall asleep in your chair? YES NO
4. After a few drinks, have you sometimes not eaten or been able to skip a meal becauseyou didn't feel hungry? YES NO
5. Does having a few drinks help decrease your shakiness or tremors? YES NO
6. Does alcohol sometimes make it hard for you to remember parts of the day or night? YES NO
7. Do you have rules for yourself that you won't drink before a certain time of the day? YES NO
8. Have you lost interest in hobbies or activities you used to enjoy? YES NO
9. When you wake up in the morning, do you ever have trouble remembering part of thenight before? YES NO
10. Does having a drink help you sleep? YES NO
11. Do you hide your alcohol bottles from family members? YES NO
12. After a social gathering, have you ever felt embarrassed because you drank too much? YES NO
13. Have you ever been concerned that drinking might be harmful to your health? YES NO
14. Do you like to end an evening with a nightcap? YES NO
15. Did you find your drinking increased after someone close to you died? YES NO
16. In general, would you prefer to have a few drinks at home rather than go out to social
YES NO
events? YES NO
17. Are you drinking more now than in the past? YES NO
18. Do you usually take a drink to relax or calm your nerves? YES NO
19. Do you drink to take your mind off your problems? YES NO
20. Have you ever increased your drinking after experiencing a loss in your life? YES NO
21. Do you sometimes drive when you have had too much to drink? YES NO
22. Has a doctor or nurse ever said they were worried or concerned about your drinking YES NO
23. Have you ever made rules to manage your drinking? YES NO
24. When ou feel lonel , does havin: a drink helm? YES NO
Scoring: Five or more "yes" responses are indicative of an alcohol problem. For further information,contact Frederic C. Blow, Ph.D., at University of Michigan Alcohol Research Center, 400 E. Eisenhower
Parkway, Suite A, Ann Arbor, MI 48108; (734) 998-7952.
Source: Blow, F.C.; Brower, K.J.; Schulenberg, J.E.; Demo-Dananberg, L.M.; Young, J.P.; and Beresford,
T.P. The Michigan Alcoholism Screening TestGeriatric Version (MAST-G): A new elderly-specificscreening instrument. Alcoholism: Clinical and Experimental Research 16:372, 1992.
© The Regents of the University of Michigan, 1991.
77 55

Chapter 4
Communicating NegativeScreening ResultsThe process of conveying negative screeningresults provides an important opportunity toreinforce healthy practices and educate olderadults about the impact that alcohol andprescription drugs have on aging systems.However, even older adults who have hadnegative screening results may need screeningrepeated in the future. As discussed previously,life events render older adults vulnerable todeveloping problems; as the changes occur,screening questions should be asked again andthe benefits of maintaining healthy habitsreemphasized.
AssessmentFor older adults with positive screens, anassessment is needed to confirm the problem, tocharacterize the dimensions of the problem, andto develop an individualized treatment plan.For purposes of insurance or other fundingresources, the assessment should follow criteriain the Diagnostic and Statistical Manual of Mental
Disorders, Fourth Edition (DSM-IV) (American
Psychiatric Association, 1994) or other relevantcriteria, bearing in mind that these criteria maynot apply directly to planning older adults'treatment. The unqualified application of suchcriteria is problematic in older adult populationsbecause the symptoms of other medical diseasesand psychiatric disorders overlap to aconsiderable extent with substance-relateddisorders.
In addition, as discussed in Chapter 2, thealtered social roles and circumstances of olderadults may further reduce the applicability ofthe criteria. For example, interference withoccupational activities or work obligations mayno longer be relevant as a manifestation ofmaladaptive functioning, although the emphasis
56
for a retired person can still be placed onmaintaining a dwelling, managing finances, orparticipating in social or recreational activities."Recurrent substance use in situations in whichit is physically hazardous," a substance abusecriteria in the DSM-IV (American Psychiatric
Association, 1994, p. 183), need not meandriving drunk: Climbing a ladder, crossing astreet, or taking a bath while impaired byalcohol is dangerous for a frail, older person.
With respect to toleranceone of the DSM-IV criteria for a diagnosis of substancedependencethe aging process itself, as well asother concurrent medical diseases commonlyfound in older patients, lowers the threshold foronset of physiological dependence onprescription drugs. The presence of toleranceamong older adults is not necessarilycharacteristic of substance-related psychologicaldependence. Conversely, the absence oftolerance to alcohol does not necessarily meanthat an older adult does not have a drinkingproblem. To be useful in assessing older adults,the DSM-IV criteria must be interpreted age-appropriately. (See Figure 2-3, which presentsthe DSM-IV criteria for substance dependence asthey apply to older adults with alcoholproblems.)
Because the assessment process can be time-consuming and expensive, the Institute ofMedicine (IOM) recommends (and the Panelsupports) a sequential approach that looks atvarious dimensions of an older adult'ssuspected problem in stages so that unnecessarytests are not conducted (Institute of Medicine,1990).
Substance Abuse AssessmentInstrumentsAlthough informed clinical judgment is essentialfor a sound assessment, validated substanceabuse assessment instruments can provide auseful structured approach for many cliniciansas well as a convenient checklist of items that
78

should be consistently evaluated during theassessment. In general, specialized assessmentis conducted by treatment program personnel orspecially trained health care providers. Asdescribed by the IOM, structured assessmentinterviews "possess (at least potentially) thedesired qualities of quantifiability, reliability,validity, standardization, and recordability"(Institute of Medicine, 1990, pp. 267-268).
Based on their experience, the ConsensusPanelists recommend the use of two structuredassessments with older adults: the StructuredClinical Interview for DSM-III-R (SCID) (Spitzer
and Williams, 1985) and the DiagnosticInterview Schedule (DIS) for DSM-IV (Robins et
al., 1981).
The SCID is a multimodule assessment thatcovers
Substance use disordersPsychotic disordersMood disordersAnxiety disordersSomatoform disordersEating disordersAdjustment disordersPersonality disorders.
It takes a trained clinician approximately 30minutes to administer the 35 SCID questionsthat probe for alcohol abuse or dependence.
The DIS is a highly structured interview thatdoes not require clinical judgment and can beused by nonclinicians. The DIS assesses bothcurrent and past symptoms and is available in acomputerized version. It has been translatedinto a number of languages including Spanishand Chinese.
Special AssessmentsFor some older adults, it may be impossible tounderstand the true impact of their alcohol anddrug use or to recommend appropriatetreatment services without a full assessment oftheir physical, mental, and functional health.
Identification, Screening, and Assessment
Assessing Functional AbilitiesFunctional health refers to a person's capacity toperform two types of everyday tasks: activitiesof daily living (ADLs), which includeambulating, bathing, dressing, feeding, andusing the toilet, and instrumental activities ofdaily living (IADLs), which include managingfinances, preparing meals, shopping, takingmedications, and using the phone. Limitationsin these domains, sometimes referred to asdisabilities, can result in an inadequate diet,mismanagement of medications or finances, orother serious problems. These disabilities aremajor risk factors for institutionalization and aremore likely than physical illness or mentalhealth problems to prompt older adults to seektreatment.
Impairments in functional abilities arecommon in older adults with medical andpsychiatric disorders. For instance, 90 percent ofadults over the age of 65 require the use ofglasses and 50 percent of adults over 65 havesome degree of hearing loss (Hull, 1989; Plomp,1978). Sensory impairments affect older adultsin subtle ways that are not always immediatelyobvious to health practitioners but need to beanticipated, identified, and incorporated intotreatment practices. Clinicians should ensurethat older patients, for example, can read theirprescriptions or hear what is said in a grouptherapy session. When not considered andcompensated for, functional impairments canobstruct treatment. For example, it would befutile to enroll an older patient who is obese andhas limited mobility in a program housed in afacility with steep flights of stairs and noelevator. Likewise, it makes little sense torecommend an evening program to older adultswho cannot drive at night and do not havesomeone else to drive them.
Alcohol use can diminish IADLs and ADLs.Although alcohol-related functionalimpairments are potentially reversible, theyshould be considered when planning a
Q o
57

Chapter 4
treatment regimen. There are knowncomplications of and differences betweenalcohol use in men and women related tocompromised functional abilities and ADLs. Ina recent study of older adults with a formerhistory of alcohol abuse, impairment in ADLswas twice as common in women as in men(Ensrud et al., 1994). In addition, alcohol usewas more strongly correlated with functionalimpairment than were smoking, age, use ofanxiolytics, stroke, or diminished grip strength.
To identify functional impairments, the Panelrecommends measuring the ADLs and theIADLs with the instruments in Appendix B.Another useful instrument is the MedicalOutcomes Study 36-Item Short Form HealthSurvey (SF-36), a self-report questionnaire thatmeasures health-related quality of life, includingboth ADLs and IADLs (McHorney et al., 1994).Although this instrument is morecomprehensive, it is also more difficult to usebecause of complex scoring of the varioussubscales. The SF-36 does provide, however, acomprehensive assessment of health and not justfunctional abilities. These instruments can beused by health care providers in a range ofsettings.
Assessing Comorbid DisordersThe relationship between alcohol use and acoexisting physical or mental disorder can takemany different forms. At one extreme, medicaland psychiatric problems can coexist withalcohol use with no specific relationship todrinking. Alternatively, those problems may beprecipitating or maintenance factors fordrinking. The use of alcohol to anesthetize painis an example of a maintenance factor; alcoholuse can then become its own problem or causedrug interaction problems with prescribed painmedications. Medical or psychiatric problemssuch as alcoholic cirrhosis or cognitive deficitsare other possible consequences of drinking.Even when the link is not so direct, alcohol use
58
can worsen other conditions such ashypertension or congestive heart failure.
The existence of comorbid medical andpsychiatric disorders will influence treatmentchoice and priorities and will affect treatmentoutcome. Frail or medically compromisedalcohol abusers, for example, may require moreintensive monitoring during the detoxificationperiod of treatment than their more robustpeers. When disorders such as uncontrolledhypertension or depression are detected,reducing alcohol consumption becomes apriority; until drinking is curbed, medicationprescribed for those conditions will not workeffectively. In contrast, for older adultssuffering from chronic pain, the priority wouldbe to identify an effective painkiller, then taperthe amount of alcohol consumed.
Physical comorbiditiesStudies have shown that the most commonhealth problem among alcohol-dependent olderadults is alcoholic liver disease. Chronicobstructive pulmonary disease, peptic ulcerdisease, and psoriasis also are found much morefrequently in older alcoholics than in olderadults with no alcohol problems. Alcohol alsoappears to be a risk factor for myopathy,cerebrovascular disease, gastritis, diarrhea,pancreatitis, cardiomyopathy, sleep disorders,HIV/AIDS-related diseases, and bothintentional and unintentional injuries (Tobias etal., 1989).
Malnutrition among older adults may be dueto such conditions as poverty or a cognitivedysfunction and is especially important todiagnose and correct. Older substance-abusingadults on fixed incomes frequently have tochoose among buying food, the prescriptionsthey need to manage illness, or the substancethey abuse. If malnutrition is caused byeconomic conditions, it is appropriate for socialservice agencies or private food-relatedprograms to be brought into the equation tohelp alleviate the problem.
0

Poor nutrition also may stem from a lifechange such as a spouse dying: An older personmay stop preparing meals if he or she no longerhas someone to cook for or eat with; a bereavedor frail person may not have the energy to shopor cook. Many adults with alcohol problems,however, "drink their calories" instead of eatingfood. Along these same lines, a provider shoulddetermine whether or not the older person isdehydrated, another possible indicator ofalcohol problems.
Acute alcohol withdrawal syndrome is moreprotracted and severe in older adults than inyounger adults (Brower et al., 1994; Liskow etal., 1989). Because there is no research on therecent practice of outpatient detoxification forolder adults, very careful assessment iswarranted before detoxification from any drug;outpatient detoxification may not be appropriatefor older adults who are frail or who have acomorbidity.
Psychiatric comorbiditiesData from the Epidemiologic Catchment Area(ECA) study have strengthened support for apossible link between alcohol use and abuse andthe development of other psychiatric illnesses(Regier et al., 1990). Adults with a lifetimediagnosis of alcohol abuse or dependence hadnearly three times the risk of being diagnosedwith another mental disorder. Comorbiddisorders associated with alcohol use includeanxiety disorders, affective illness, cognitiveimpairment, schizophrenia, and antisocialpersonality disorder (Finlayson et al., 1988; Blow
et al., 1992b; Blazer and Williams, 1980;
Saunders et al., 1991; Os lin and Liberto, 1995;
Wagman et al., 1977). According to one study,older alcohol abusers are more likely to havetriple diagnosesalcohol, depression, andpersonality disorderswhereas youngersubstance abusers are more likely to havediagnoses of schizophrenia (Speer and Bates,
1992).
Identification, Screening, and Assessment
Cognitive impairmentsThe presence of cognitive impairment ordementia significantly alters treatmentdecisions. It is particularly important todistinguish between dementia and delirium,which are often mistaken for each other byclinicians diagnosing older patients (see Figure4-5).
Dementia is a chronic, progressive, andgenerally irreversible cognitive impairmentsufficient to interfere with an individual's dailyliving. Dementia will also limit an individual'sability to interact in traditional group settings.Common causes of dementia includeAlzheimer's disease, vascular disorders (e.g.,multi-infarct dementia), and alcohol-relateddementia. Dementia also makes it more difficultto monitor outcomes of drinking (patients mayforget they drank), to get into treatment, and tobenefit from the treatment.
Delirium is a potentially life-threateningillness that requires acute interventionusuallyhospitalization. The cognitive lossesexperienced with delirium, unlike the effects ofdementia, can often be reversed with propermedical treatment.
DementiaChanges in cognition are not unusual as peopleage, and they increase in frequency with eachdecade. Such changes, which are experienced invarying degrees, include minor short-termmemory loss and difficulty with certainmathematical functions. However, significantmemory loss, impaired abstract thinking,confusion, difficulty communicating, extremeemotional reactions and outbursts, anddisorientation to time, place, and person aresigns of cognitive impairment and are not part of
the normal aging process.
Dementia can range from a mild level ofcognitive impairment that is easily managed to asevere stage that may require intensivetreatment and nursing home care. Commonsymptoms of dementia are presented in Figure
8 .1.
59

Chapter 4
60
4-5. Symptoms described may not be equallypresent in all older adults experiencingdementia. The most common causes ofdementia in older adults are Alzheimer's diseaseand vascular dementia.
Screening for significant cognitivedysfunction can be accomplished easily by anyof a number of screening instruments. Patientswho have been medically detoxified should notbe screened for several weeks afterdetoxification. Until they are fully recovered,they may exhibit some reversible cognitiveimpairment. The Panel recommends twoscreens: the Orientation/Memory/Concentration Test (Katzman et al., 1983), whichis simple and can be completed in the office, and
the Folstein Mini-Mental Status Exam (MMSE)(Folstein et al., 1975), which is an acceptablealternative. It should be noted that in theassessment of older problem drinkers who haverecently (in the past 30 to 60 days) attainedsobriety in an outpatient setting, the MMSE canbe insensitive to subtle cognitive impairments.
Furthermore, because the MMSE is weak onvisual-spatial testing, which is likely to showsome abnormality in many recent heavydrinkers, and does not include screening tests ofabstract thinking and visual memory, the Panelrecommends using the "draw-a-clock task"(Watson et al., 1993) and the NeurobehavioralCognitive Status Examination (NCSE) (Kiernanet al., 1987) as supplements.
Figure 4-5
CoMparison of Dementia and Delirium: Characteristics and Causes
Dementia Delirium
Characteristics Impairments in short- and long-term
memory, abstract thinking, and
judgment
Aphasia (language disorder)
Apraxia (inability to carry out motor
activities despite intact comprehension
and motor function)
Agnosia (inability to recognize or identify
items despite intact sensory function)
Constructional difficulty (inability to copy
three-dimensional figures, assemble
blocks, or arrange sticks in specific
designs)
Personality change or alteration and
accentuation of premorbid traits
Mood disturbances
Loss of self-care abilities
Inability to appreciate and respond
normally to the environment, often with
altered awareness, disorientation, inability
to process visual and auditory stimuli, and
other signs of cognitive dysfunction
Potentially life-threatening
Acute onset
Clouding of consciousness
Reduced wakefulness
Disorientation to time and space
Increased motor activity (e.g., restlessness,
plucking, picking)
Impaired attention and concentration
Impaired memory
Anxiety, suspicion, and agitation
Variability of symptoms over time
Misinterpretation, illusions, or
hallucinations
Disrupted thinking, delusions, speech
abnormalities
86.

Identification, Screening, and Assessment
Figure 4-5 (Continued)
Dementia Delirium
Causes Most Common Causes Common Intracranial Causes
Alzheimer's disease Infections (e.g., meningitis, encephalitis)
Vascular dementia Seizures
Alcohol-related dementia Stroke
Common Metabolic/Toxic Causes Subdural hematomas
Chronic drug-alcohol-nutritional abuse Tumors
(e.g., Wernicke-Korsakoff syndrome) Common Extracranial Causes
Organ system failure Anesthesia
Anoxia Drugdrug or alcoholdrug interactions
Folic acid deficiency Intoxication and/or withdrawal from
Hypothyroidism alcohol or drugs (particularly psychoactive
Bromide intoxication drugs)
Hypoglycemia Toxic effects of prescribed or over-the-
counter drugsCommon Infectious Causes
Giant cell arteritis (a chronic inflammatoryNeurosyphilis paresis (a syphilitic
infection manifested as dementia,
seizures, and problems walking and
process involving the extracranial arteries)
Hip fracture
standing) Hydrocephalus (increased fluid in the brain)
AIDS/HIV-related disorders Hypercapnia (reduced ventilation often
Meningitisassociated with chronic obstructive
pulmonary disease)Encephalitis
InfectionsOther Common Causes
DehydrationHuntington's Chorea Malnutrition
Parkinson's disease Metabolic disturbances (e.g., liver or kidney
Jakob-Creutzfeldt disease failure, electrolyte disturbances, hyper- or
hypoglycemia, diabetes, thyroid disorders)Lewy body's dementia
Myocardial infarction (heart attack)
Sudden environmental changes
Depression
DeliriumDelirium, also known as acute confusional state
and acute brain syndrome, is an alteration of
mental status that can usually be reversed withmedical treatment. Figure 4-5 presents the
characteristics of this syndrome and its commoncauses. Symptoms presented may occur in anycombination and may be intermittent. Inaddition to the causes listed in Figure 4-5,benzodiazepine use prior to hospitalization has
8361

Chapter 4
been demonstrated to be a significant risk factorfor the development of delirium amonghospitalized older adults. This suggests thatthese individuals had classical withdrawaldelirium from the benzodiazepines or that mildwithdrawal in addition to other risk factorsgreatly increases the incidence of delirium. TheConfusion Assessment Method (CAM) (Inouyeet al., 1990) is widely used as a brief, sensitive,
and reliable screening measure for detectingdelirium. The Panel recommends that a positivedelirium screen be followed by careful clinicaldiagnostics based on DSM-IV criteria and thatany associated cognitive impairment befollowed clinically using the MMSE.
Other cognitive impairmentsAlcohol abuse and dependence are directlycorrelated with other potential causes ofcognitive impairment, including trauma fromfalls, motor vehicle crashes or other accidents,and the development of Wernicke-Korsakoffsyndrome (Smith and Atkinson, 1997). Thelatter is clinically characterized by cognitivedeficits (especially anterograde memorydeficits), gait ataxia, and nystagmus. Itspathophysiology usually involves the lack of thevitamin thiamine. It is important to screen forWernicke-Korsakoff syndrome because it is apotentially reversible cause of cognitiveimpairment (Victor et al., 1989; Grant, 1987).
The extent to which alcohol use interfereswith performance on neuropsychological testinghas been well reviewed (Victor et al., 1989; Grantet al., 1984). Several studies have demonstratedacute effects of alcohol on abstraction and
visual-spatial problems but not on verbal skills.Less is known about the role of alcohol use incausing permanent cognitive changes. Studieshave demonstrated that among nondementedalcoholics, abstinence leads to markedimprovement in cognitive deficits (Brandt et al.,1983; Grant et al., 1984). However, Brandt andcolleagues demonstrated that among subjectswith prolonged periods of abstinence, there
62
were long-term deficits in learning novel
associations (Brandt et al., 1983). It should benoted that most of these patients were moderateconsumers of alcohol, and all were healthy withno history of dementia. A more recentepidemiologic study of older African-Americanmen found that increasing amounts of alcoholconsumption were associated with worseningperformance on dementia screening scales(Hendrie et al., 1996).
Affective disordersAffective disorders, common in older patients,also influence treatment choices. For example, a
patient with an affective disorder who takespsychotropic drugs requires a treatmentprogram with a staff familiar with thesemedications. Suicidal patients require intensiveinpatient programs and an immediateintervention. Significant depressive symptoms,which are a common reaction afterdetoxification, can be worse in older adults thanin younger patients and may require prescribedmedicines to alleviate the depression before theabuse or addiction therapy is resumed. Asnoted below, research in the area of mentalhealth comorbidities supports these findings.
Comorbid depressive symptoms are not onlycommon in late life, but are also an importantfactor in the course and prognosis of psychiatricdisorders. Depressed alcoholics have beenshown to have a more complicated clinicalcourse of depression with an increased risk ofsuicide and more social dysfunction than
nondepressed alcoholics (Conwell, 1991; Cook etal., 1991). Moreover, they were shown to seekmore treatment. However, relapse rates foralcoholics did not appear to be influenced by thepresence of depression. Alcohol use prior to latelife has also been shown to influence treatmentof late-life depression. Cook and colleaguesfound that a prior history of alcohol abusepredicted a more severe and chronic course fordepression (Cook et al., 1991).
84

Screening instruments for depression can beextremely useful as methods of detectingsignificant affective illness and for monitoringchanges in affective states. The GeriatricDepression Scale (GDS) Short Form (Sheikh andYesavage, 1986) and the Center forEpidemiological StudiesDepression Scale(CES-D) (Radloff, 1977), reproduced in
Appendix B, have been validated in older agegroups although not specifically in older adultswith addiction problems. The Panelrecommends the CES-D for use in generaloutpatient settings as a screen for depressionamong older patients.
Sleep disordersAs discussed in Chapter 2, sleep disorders andsleep disturbances represent another group ofcomorbid disorders associated with excessivealcohol use and with aging (Os lin and Liberto,1995; Wagman et al., 1977; Moeller et al., 1993).
Older adults sometimes self-medicate their sleepdisturbances with alcohol (Wagman et al., 1977):
Panel members had all heard older patients saythat drinking helps them sleep.
The Panel recommends that sleep history berecorded in a systematic way in order to bothdocument the changes in sleep problems overtime and heighten the awareness of sleephygiene. The Pittsburgh Sleep Quality Index(Buysse et al., 1988) is useful as both a researchand screening scale but is difficult for cliniciansto interpret and cumbersome to use. Cliniciansmay opt to carefully document sleep patternsand disturbances themselves rather than use thisinstrument (Nitcher et al., 1993).
Other psychiatric disordersThere are other psychiatric disorders (e.g.,schizophrenia, obsessive and compulsivebehaviors) that complicate the treatment ofabuse and addiction. In these instances,treatment options must be evaluated on a case-by-case basis, although all programs consideredfor referral should include medical and mental
Identification, Screening, and Assessment
health personnel skilled in responding to thosedisorders.
Although suicide is not a specific psychiatricdisorder, the Panel believes that there is asignificant relationship among aging, alcoholuse, and suicide. People older than 65 accountfor 25 percent of the national suicide rate(Conwell, 1991). Patients who attempt suiciderequire immediate and intensive inpatienttherapy for as long as the illness persists.Providers must be alert to the possibility ofmajor depression, which is common in olderadults, evolving into suicidal tendencies. Ithelps if family and significant others, clergy,social workers, and home health care providersare knowledgeable about the warning signs forsuicide, because these symptoms are morefrequently manifested in nonclinical settings.
Moving the Older AdultInto TreatmentAfter determining that an older adult maybenefit from a reduction in or completeabstention from alcohol use, the clinician mustnext assess the patient's understanding of thisbenefit. Many older adults may not know thattheir alcohol use is affecting their health.Because patient understanding and cooperationare essential both in eliciting accurateinformation and following through on thetreatment plan prescribed, clinicians should usethe assessment process as an opportunity toeducate the older adult and to motivate him orher to accept treatment.
Interacting With Older AdultsMany health care professionals rarely interactwith older adults. To facilitate the assessmentprocess with this population, the ConsensusPanel recommends that clinicians adhere to thefollowing guiding principles:
Areas of concern most likely to motivateolder substance abusers are their physical
8563

Chapter 4
health, the loss of independence andfunction, financial security, and maintenanceof independence.
Assessment and treatment decisions mustinclude the patient in order to be successful.This is particularly relevant for older adults,who may be very uncomfortable in
formalized addiction treatment programsthat do not include many of their peers oraddress their specific developmental andhealth needs.Depending on an individual's particularsituation, it may be important to includefamily members in treatment or interventiondiscussions (understanding that childrenmay vacillate between a desire to help anddenial and that patient confidentiality mustalways be respected).
Addiction is a chronic illness that ebbs andflows. Thus, patients' needs will change overtime and will require different types andintensities of treatment.Because many older adults have severalhealth care providers (e.g., visiting nurses,social workers, adult day care staff, religiouspersonnel), it is important to include this
64
network as a resource in assessment and inproviding treatment.Given the complex health needs of olderadults, health care providers may needassistance from experienced nonmedicalpersonnel to adequately assess the totality oftreatment issues and choices. Providersshould be aware of their limitations both inproviding addiction treatment and inassessing and treating mental or physicalhealth needs.
All treatment strategies must be culturallycompetent and, to the extent possible,incorporate appropriate ethnicconsiderations (e.g., rituals).
Overarching continuity of care issues andconsiderations should be identified andaddressed, especially in rural and minoritycommunities where emergency room stafffunction as primary care providers.
The next chapter builds on these guidingprinciples in describing referral and treatmentoptions for older adults with substance abuseproblems.
8 6

5 Ref rrol TreatA r aches
Once screening and assessment haveidentified a problem, the clinician andpatient must choose the most
appropriate treatment. The Consensus Panelrecommends that the least intensive treatmentoptions be explored first: brief intervention,
intervention, and motivational counseling.
Although these three approaches can besufficient to address the problem for some olderpatients, for others they will function aspretreatment strategies. These less intensiveoptions will not resolve the latter type ofpatients' alcohol or other drug problems but canmove them into specialized treatment byhelping them overcome resistance to andambivalence about changing their drinkingbehavior.
Like treatment itself, pretreatment activitiesin some cases may be conducted best in theclient's home and can be coupled with otherpersonal or social services (Fredriksen, 1992;Graham et al., 1995b) or with home-baseddetoxification services (Cooper, 1995). Thisapproach is ideal for the large number of at-riskolder individuals who are homebound; it can beconducted by visiting nurses, housingauthorities, and social workers. Communityhealth services often have staff designated tomake visits to older adults in their homes, andsome in-home treatment programs have avisiting nurse who identifies and treatssubstance abuse in the home.
Least Intensive Options
Brief Intervention for At-RiskDrinkersResearch has shown that 10 to 30 percent ofnondependent problem drinkers reduce theirdrinking to moderate levels following a briefintervention by a physician or other clinician. Abrief intervention is one or more counselingsessions, which may include motivation-for-change strategies, patient education, assessmentand direct feedback, contracting and goalsetting, behavioral modification techniques, andthe use of written materials such as self-helpmanuals (Fleming et al., 1997b). Briefintervention techniques have been used toreduce alcohol use in adolescents, in adultsunder age 65 who are nondependent problemdrinkers, and most recently, in older adults(Blow, in press; Fleming et al., 1997a). All of
these activities can be conducted by trainedclinicians, home health care workers,psychologists, social workers, and professionalcounselors (e.g., physicians, nurses, physicians'
assistants).Brief intervention strategies range from
relatively unstructured counseling and feedbackto more formal structured therapy and relyheavily on concepts and techniques from themotivational psychology and behavioral self-control training literature (Miller and Taylor,
8765

Chapter 5
1980; Miller and Hester, 1986; Miller andMunoz, 1976; Miller and Rollnick, 1991). Thegoal is to motivate the problem drinker tochange his behavior, not to assign blame.Drinking goals accordingly should be flexible,allowing the individual to choose drinking inmoderation or abstinence.
In a trial conducted in Malmo, Sweden, inthe late 1970s, non-older adult subjects (allunder age 65) were advised in a series of healtheducation visits to reduce their alcohol use.They subsequently demonstrated significantreductions in gamma-glutamyl transferaselevels and health care utilization for up to 5years after the brief intervention (Kristenson etal., 1983). The Medical Research Council trial,conducted in 47 general practitioners' offices inGreat Britain, found significant reductions inalcohol use by the intervention group comparedwith the control group 12 months after theintervention (Wallace et al., 1988). The WorldHealth Organization trial, conducted in 10countries, found similar differences in alcoholuse between the two groups (Babor and Grant,1992). Meta-analyses found an effect size of 20to 30 percent in studies conducted in health caresettings (Bien et al., 1993; Kahan et al., 1995).
There are several ongoing studies of briefalcohol interventions for older adults, one ofwhich is described below on page 94.
Conducting brief interventions witholder adultsOlder adults present unique challenges to thoseapplying brief intervention strategies forreducing alcohol consumption. Because manyolder at-risk and problem drinkers are ashamedabout their drinking, intervention strategiesneed to be especially nonconfrontational andsupportive. In addition, as discussed in Chapter2, the consumption level that constitutes at-riskdrinking is lower than that for youngerindividuals (Chermack et al., 1996), so even lowlevels can be dangerous. Chronic medicalconditions may make it more difficult for
66 88
clinicians to recognize the role of alcohol in
decreases in functioning and quality of life.These issues must be kept in mind during briefinterventions with this vulnerable population.
Following identification of at-risk or problemdrinkers through screening techniques (seeChapter 4), a semistructured brief interventioncan be conducted. An older adult-specific briefintervention should include the following steps:
1. Customized feedback on patient's responsesto screening questions about drinkingpatterns and other health habits such assmoking and nutrition.
2. Discussion of types of drinkers in the UnitedStates and where the patient's drinkingpatterns fit into the population norms for hisor her age group.
3. Reasons for drinking. This is particularlyimportant because the practitioner needs tounderstand the role of alcohol in the contextof the older patient's life, including copingwith loss and loneliness.
4. Consequences of heavier drinking. Someolder patients may experience problems inphysical, psychological, or social functioningeven though they are drinking below cutofflevels.
5. Reasons to cut down or quit drinking.Maintaining independence, physical health,financial security, and mental capacity can bekey motivators in this age group.
6. Sensible drinking limits and strategies forcutting down or quitting. Strategies that areuseful in this age group include developingsocial opportunities that do not involvealcohol, getting reacquainted with hobbiesand interests from earlier in life, andpursuing volunteer activities, if possible.
7. Drinking agreement in the form of aprescription. Agreed-upon drinking limitsthat are signed by the patient and thepractitioner are particularly effective inchanging drinking patterns.

8. Coping with risky situations. Socialisolation, boredom, and negative familyinteractions can present special problems inthis age group.
9. Summary of the session.
One approach devised to facilitate briefinterventions is known by the acronymFRAMES. This approach emphasizes
la Feedback of personal risk or impairment asderived from the assessmentPersonal responsibility for changeClear advice to changeA menu of change options to increase thelikelihood that an individual will find aresponsive treatment (although multipleattempts may be necessary)An empathic counseling styleEnhanced client self-efficacy and ongoingfollowup (Miller and Sanchez, 1994).
Panel members agree that when older adultsare motivated to take action on their own behalf,the prognosis for positive change is extremelyfavorable. Key to inspiring motivation is theclinician's caring style, willingness to view theolder adult as a full partner in his or herrecovery, and capacity to provide hope andencouragement as the older adult progressesthrough the referral, treatment, and recoveryprocess.
Intervention and MotivationalCounselingIf the older problem drinker does not respond tothe brief intervention, two other approachesintervention and motivational counselingshould be considered.
InterventionIn an intervention, which occurs under theguidance of a skilled counselor, severalsignificant people in a substance abuser's lifeconfront the individual with their firsthandexperiences of his or her drinking or drug use(Johnson, 1973; Twerski, 1983). The formalized
Referral and Treatment
process begins before the intervention andincludes a progressive interaction between thecounselor and the family or friends for at least 2days before meeting with the patient. Duringthis time, the counselor not only helps plan theintervention but also educates the family aboutsubstance abuse and its prevention (Johnson,1973). Participants are coached about offeringinformation in an emotionally neutral, factualmanner while maintaining a supportive,nonaccusatory tone, thus presentingincontrovertible evidence to the loved one that aproblem exists.
When using this approach with older adults,Panel members recommend some modifications.No more than one or two relatives or closeassociates should be involved along with thecounselor; having too many people present maybe emotionally overwhelming or confusing forthe older person. The most influential person toinclude in interventions or any otherpretreatment activity may be a spouse,cohabitant, caregiving son or daughter, clergymember, or visiting nurse or caseworker,depending on the particular social network ofthe client. Inclusion of grandchildren isdiscouraged: Panel members report that manyolder alcoholics describe long-lasting resentmentand shame about the airing of their problems inthe presence of much younger relatives.
Because denial is as much a part ofpsychoactive prescription drug dependence as itis of alcoholism and addiction to illicit drugs, anintervention may help move psychoactive drugabusers toward detoxification or other formaltreatment, although extra caution is advisable.Both the diagnosis of abuse or dependence andthe need for treatment are particularly difficultfor older patients to accept because their initialuse of psychoactive prescription drugs was, inalmost all cases, originally sanctioned by ahealth care provider and prescribed as a remedyfor a legitimate medical problem or complaint.As a group, older adults tend to have even
67
89

Chapter 5
greater disdain for "drug addicts" than thegeneral population: Any implied linkage withthe criminalized population of illicit drug usersis unnecessarily stigmatizing and appropriatelyresented. Such labels as addict, alcoholic; anddrunkard should be avoided.
Motivational counselingAs a result of the work pioneered by Prochaskaand Di Clemente, clinicians now understand thatpeople may respond quite differently torecommendations to alter or give uplongstanding or previously pleasurablebehaviors. Reactions depend, to a great extent,on an individual's readiness to change(Prochaska et al., 1992). For example, thescreening or assessment findings may confirmone individual's suspicions about the negativeeffect of alcohol on personal health and may
prompt an immediate commitment to abstain orbegin tapering off. For others, the assessmentmay be a revelation that must be processed overtime before they can effect any changes. Stillothers may be unconvinced by the findings andthe need to make any changes at all.
Research on stages of change, initiallyapplied to smoking cessation studies, hasdemonstrated that smokers enrolled intreatment trials fall into one of five stages:
precontemplation, contemplation, ready foraction, action, and maintenance (Prochaska andDi Clemente, 1986). Categorizing smokers thisway helps predict who is most likely to succeedin quitting smoking and what kinds ofinterventions work best with smokers indifferent stages (Di Clemente et al., 1991;
Prochaska and Di Clemente, 1985; Velicer et al.,1992). More recently, it has been suggested thatresearch on brief interventions for problemdrinkers could examine stages of change as ameans of tailoring interventions to anindividual's readiness (Hodgson and Rol "nick,1992). Studies have already begun to examinereadiness for change as predictor of outcome in
68
the alcohol field (Di Clemente and Hughes, 1990;Prochaska et al., 1992).
Motivational counseling acknowledgesdifferences in readiness and offers an approachfor "meeting people where they are" that hasproven effective with older adults (Miller andRollnick, 1991). In this approach, an
understanding and supportive counselor listensrespectfully and accepts the older adult'sperspective on the situation as a starting point,helps the individual identify the negativeconsequences of drinking and prescription drugabuse, helps him or her shift perceptions aboutthe impact of drinking or drug-taking habits,empowers the individual to generate insightsabout and solutions for his or her problem, andexpresses belief in and support for the olderadult's capacity for change. Motivationalcounseling is an intensive process that enlistspatients in their own recovery by avoiding
labels, avoiding confrontation (which usuallyresults in greater defensiveness), accepting
ambivalence about the need to change asnormal, inviting clients to consider alternativeways of solving problems, and placing theresponsibility for change on the client. Thisprocess also can help offset the denial,resentment, and shame invoked during anintervention and can serve as a prelude tocognitivebehavioral therapy (Miller andRollnick, 1991).
Specialized Treatment ofOlder Problem DrinkersAnd Substance AbusersFor some older adults, especially those who arelate onset drinkers or prescription drug abuserswith strong social supports and no mentalhealth comorbidities, pretreatment approachesmay prove quite effective, and followup briefinterventions and empathic support for positivechange may be sufficient for continued recovery.
00

There is, however, a subpopulation of olderadults who will need more intensive treatment.
Despite the resistance that some olderproblem drinkers or drug abusers exert,treatment is worth pursuing. Studies show thatolder adults are more compliant with treatmentand have treatment outcomes as good as orbetter than those of younger patients (Os lin etal., 1997; Atkinson, 1995).
Patient Placement and PatientMatchingTriage refers to the process of organizing andprioritizing treatment service. Typically,decisions regarding triage are made up of twocomponents: patient placement and patientmatching.
Patient placement describes a process by
which a recommendation is made for placementin a specific level (intensity) of care, whichranges from medically managed (high intensity)inpatient services to outpatient services (lowintensity). The most commonly used patientplacement criteria are found in the AmericanSociety of Addiction Medicine (ASAM) PatientPlacement Criteria for the Treatment of Substance-
Related Disorders, Second Edition (ASAM-PPC-2)
(American Society of Addiction Medicine, 1996).
Figure 5-1 shows the six problems orassessment dimensions that ASAM-PPC-2 usesto make patient placement decisions bothamong and within levels of service.
The answers to these questions should helpthe health care provider assess the severity ofthe problem and the intensity of the servicesrequired. For older adults, the triage process isoften greatly influenced by factors other than theseverity of a drinking or prescription drugproblem. For example, physical accessibility offacilities will influence treatment choices forwheelchair-bound patients; hearing-impairedpatients will need programs with individualtherapy and/or modified small group therapy.
Referral and Treatment
Language barriers, illiteracy, and differentcultural views of and customs surroundingsubstance abuse add to the complex of factorsrequired to assess functional abilities in olderadult patients. To help ensure optimal benefitsfor older adults, the Consensus Panelrecommends that treatment plans weave age-related factors into the contextual framework ofthe ASAM criteria.
Levels of TreatmentServicesThe following section provides an overview oftreatment services from the most to the leastintensive, with examples demonstrating howvarious circumstances may affect the level ofcare at which a service is offered.
Inpatient/Outpatient DetoxificationTreatment
One of the first issues to consider for an olderpatient with a substance dependence diagnosisis whether detoxification management isnecessary and, if so, whether it should beundertaken in an inpatient hospital-basedsetting or managed on an outpatient basis. Nostudies or reports specifically assess thepotential risks or benefits of outpatientdetoxification among older adults, butdetoxification is generally seen as medicallyriskier for an older person. Until more researchis available, best clinical judgment must guidesuch decisions. For more information ondetoxification, see TIP 19, Detoxification From
Alcohol and Other Drugs (CSAT, 1995a). Medical
safety and potential access to the abused drugsare primary considerations when decidingwhether an older patient's withdrawal fromprescription drugs requires supervision in ahospital. Factors indicating the need forinpatient detoxification include
9 1,
69

Chapter 5
Figure 5-1
ASAM-PPC-2.Assessment Dimensions,Dimension 1Acute Intoxication and/or Withdrawal PotentialWhat risk is associated with the patient's current level of acute intoxication? Is there significant risk ofsevere withdrawal symptoms or seizures, based on the patient's previous withdrawal history, amount,frequency, and recency of discontinuation or significant reduction of alcohol or other drug use? Are therecurrent signs of withdrawal? Does the patient have supports to assist in ambulatory detoxification, ifmedically safe?
Dimension 2Biomedical Conditions and ComplicationsAre there current physical illnesses, other than withdrawal, that need to be addressed or that maycomplicate treatment? Are there chronic conditions that affect treatment?Dimension 3Emotional/Behavioral Conditions and ComplicationsAre there current psychiatric illnesses or psychological, behavioral, or emotional problems that need to beaddressed or which complicate treatment? Are there chronic conditions that affect treatment? Do anyemotional/behavioral problems appear to be an expected part of addiction illness, or do they appear tobe autonomous? Even if connected to the addiction, are they severe enough to warrant specific mentalhealth treatment?Dimension 4Treatment Acceptance/ResistanceIs the patient actively objecting to treatment? Does the patient feel coerced into treatment? How ready isthe patient to change? If willing to accept treatment, how strongly does the patient disagree with others'perceptions that he or she has an addiction problem? Does the patient appear to be compliant only toavoid a negative consequence, or does he or she appear to be internally distressed in a self-motivated wayabout his or her alcohol/other drug use problems?Dimension 5Relapse/Continued Use PotentialIs the patient in immediate danger of continued severe distress and drinking/drug-taking behavior?Does the patient have any recognition of, understanding of, or skills with which to cope with his or heraddiction problems in order to prevent relapse or continued use? What severity of problems and furtherdistress will potentially continue or reappear if the patient is not successfully engaged in treatment at thistime? How aware is the patient of relapse triggers, ways to cope with cravings to use, and skills tocontrol impulses to use?Dimension 6Recovery EnvironmentAre there any dangerous family members, significant others, living situations, or school/workingsituations that pose a threat to treatment engagement and success? Does the patient have supportivefriendships, financial resources, or education/vocational resources that can increase the likelihood ofsuccessful treatment? Are there legal, vocational, social service agency, or criminal justice mandates thatmay enhance the patient's motivation for engagement in treatment?Source: American Society of Addiction Medicine, 1996.
A high potential for developing dangerousabstinence symptoms such as a seizure ordelirium because (1) the dosage of alcohol ordrug has been particularly high or prolongedand has been discontinued abruptly or (2) the
70
patient has experienced these serioussymptoms at any time previously
gi Suicidal ideation or threatsThe presence of other majorpsychopathology
92

Unstable or uncontrolled comorbid medicalconditions requiring 24-hour care orparenterally administered medications (e.g.,renal disease, diabetes)Mixed addictions, (e.g., alcohol,sedative/hypnotic drugs)A lack of social supports at home or livingalone with continued access to the abusedsubstance(s)A failure to respond to outpatient treatment.
Older patients detoxifying from psychoactiveprescription drugs on an inpatient basis shouldnot be stabilized on high doses ofbenzodiazepines or barbiturates with a long orintermediate half-life. These drugs canaccumulate and result in toxicity and somepersisting cognitive impairment after hospitaldischarge, which can interfere with functionalcapabilities in general and also hamper anyimmediate participation in continuingtreatment. The choice of drug and drugschedule should also be guided by the length ofthe hospitalization. If a long-acting drug such asclonazepam (Klonopin) or an intermediate-acting one such as chlordiazepoxide is used todetoxify an older patient, the hospitalizationwill likely be extended. An additional risk isthat the patient will exhibit no signs of theabstinence syndrome until days or even weeksafter leaving the hospital. In general, the initialdose of a drug for suppression and managementof withdrawal symptoms should be one-third toone-half the usual adult dose, sustained for 24 to48 hours to observe reactions and then graduallytapered with close attention to clinical responses(Finlayson, 1995b).
The clinician overseeing detoxification fromalcohol or presCription drugs must decide on thelevel of care necessary to maintain abstinence.Patients with high relapse or withdrawalpotential and patients with severe medical orpsychiatric comorbidity will requirehospitalization. Regular monitoring of thepatient's vital signs and objective symptoms of
Referral and Treatment
withdrawal also is needed. Short-actingbenzodiazepines (e.g., oxazepam, lorazepam)are customarily used as detoxification agentsbecause alcohol-addicted patients are cross-tolerant to these substances. The use ofoxazepam or lorazepam is warranted in patientswith severe liver disease. Metabolism of thesebenzodiazepines does not depend onhydroxylation by the liver, and thus they do notaccumulate in the liver and cause adverse effects(Brower et al., 1994). The benzodiazepinedosage is decreased daily over the course of thedetoxification process. Medications such asclonidine and methadone for opiate withdrawaland phenobarbitol for barbiturate withdrawalshould be used more cautiously than withyounger patients.
In general, older patients require lower dosesof many medications, and the principle ofstarting at a lower dose and titrating at a slowerrate should be followed for detoxification. Inaddition to treating acute withdrawalsymptoms, clinicians are reminded thatalcoholic patients require supplemental doses ofthiamine, folate, and multivitamins tocounteract the vitamin depletion that is oftenassociated with excessive alcohol use.
Inpatient RehabilitationPatients who are brittle, frail, acutely suicidal, ormedically unstable or who need constant one-on-one monitoring, should receive 24-hourprimary medical/psychiatric/nursing inpatientcare in medically managed and monitoredintensive treatment settings. Recent changes inthe health care system have dramaticallyreduced the availability of this level of care.Inpatient rehabilitation (traditional 14- , 21- , or28-day programs) are not readily available andoften no longer reimbursed by health careinsurers. Because of these reimbursement gaps,inpatient care may have to be arranged on amedical or psychiatric unit of an acute carehospital.
71

Chapter 5
72
Residential RehabilitationResidential programs provide a slower paced,more repetitive treatment approach for olderpatients. Services range from high to lowintensity and can be delivered in specializedcare settings (e.g., halfway house, group homefor people with addiction problems, board andcare facilities, domiciliary facilities for veterans)and in nonspecialized settings (e.g., extendedcare facilities, life care programs, subacutenursing homes where primary care doctorsmake rounds and visiting nurses attendoccasionally). Specialized rehabilitationprograms include those designed for individualswho are cognitively impaired by chronic illnessor traumatic injuries. These facilities work wellfor patients who lack significant social resources(such as family) or have no social network andfor those with no mobility to stabilize care(which justifies the expense of this treatmentoption).
Outpatient ServicesSpecialized outpatient programs vary greatly inthe intensity of treatment. Partialhospitalization/day treatment programs requirepatients to attend day-long treatment 5 days perweek, whereas intensive outpatient programsare sometimes hospital-based and provide 2 to 3hours of treatment each day. Finally, traditionallow-intensity outpatient care normally providesfor one group session per week and oneindividual session per month.
Nonspecialized, nonresidential services areprovided by many partial day treatmentprograms structured for outpatient care. Theseinclude community-based drop-in centers andsenior centers, generally less available in ruralareas. These facilities are good for peoplewaiting for inpatient care and who require alevel of interim care, for people with no familyat home on a daily basis, and for retirees whoneed a structured daily regimen to keep thefocus on their addiction. Some of these
94
structured programs have the expertise to dealwith comorbidities in an intensive outpatientsetting.
If an older patient needs more help andstructure than is readily available, anindividually tailored, case-managed approachmay work well for coordinating outpatienttreatment. This would entail professionalassessment of the patient's problems andstrengths, assistance with the development of arealistic treatment plan in the context of knownand reasonably available resources in thecommunity, and linkage with the identifiedprograms. Usually the patient's primaryphysician and his or her team will be the chiefplayers in ongoing case management. Providersof primary drug dependence treatment shouldnot overlook the physicianwho will prescribeall medicationsin their planning. The Panelrecommends drawing the physician into thetreatment planning process and enrolling him asa player in the recovery network. Without thephysician's knowledgeable participation, theentire plan may unravel.
The Panel also recommends serving olderadults who are dependent on psychoactiveprescription drugs in flexible, community-oriented programs with case managementservices rather than in traditional, stand-alonesubstance abuse treatment facilities withstandardized components. Case management isdiscussed in more detail below.
Specialized outpatient treatment generallyincludes psychiatric consultation andindividualized or group psychotherapy.Outpatient programs frequently encouragepatients to attend regular meetings of self-helpgroups such as Alcoholics Anonymous,Alcoholics Victorious, Rational Recovery, orNarcotics Anonymous and often assign aproactive case manager to help an older patientconnect with an appropriate group. After apatient's release from the formal and time-limited outpatient substance abuse treatment

program, a case manager plays an importantaftercare role by coordinating community-basedsupport and monitoring to reinforce gains madeduring treatment and prevent or minimize theimpact of slips.
Although the success of treatment for olderadults has been documented, the literature onsubstance abuse lacks empirically derived,proven methods for treating older alcoholicsand substance abusers. Instead, individualpractices borrow heavily from what is known inthe general fields of addictions treatment,geriatric medicine and psychiatry, and socialgerontology, as well as the cumulativeexperience of existing programs that havespecialized in treating older alcoholics(Atkinson, 1995; Schonfeld and Dupree, 1996).
Before referring an older adult to a community-based treatment program, health care providersshould carefully consider the program'sphilosophy and practices regarding olderclients.
Program Philosophy andBasic PrinciplesBased on a review of the older adult-specificalcohol treatment literature, the Panelrecommends incorporating the following sixfeatures into treatment of the older alcoholabuser (Schonfeld and Dupree, 1996):
1. Age-specific group treatment that issupportive and nonconfrontational andaims to build or rebuild the patient's self-esteem
2. A focus on coping with depression,loneliness, and loss (e.g., death of a spouse,retirement)
3. A focus on rebuilding the client's socialsupport network
4. A pace and content of treatment appropriatefor the older person
5. Staff members who are interested andexperienced in working with older adults
Referral and Treatment
6. Linkages with medical services, services forthe aging, and institutional settings forreferral into and out of treatment, as well ascase management.
Building from these six features, theConsensus Panel recommends that treatmentprograms adhere to the following principles:
Treat older adults in age-specific settingswhere feasibleCreate a culture of respect for older clientsTake a broad, holistic approach to treatmentthat emphasizes age-specific psychological,social, and health problemsKeep the treatment program flexibleAdapt treatment as needed in response toclients' gender.
Age-Specific TreatmentAge-specific treatment is group treatment in
which older individuals come togetherexclusively with their peers. Such treatment canbe provided in one of two formats. The first is adiscrete program designed for older alcoholicsand substance abusers in which the entireprogram provides age-specific services and allof the patients are older. The second option isage-specific groups within an all-ages treatmentprogram.
In contrast, mixed-age treatment and
mainstreaming integrate adults of all ages with
similar substance abuse problems in the sameprogram. The question of whether older adultsachieve better outcomes in age-specifictreatment has not received adequate study, butthere is some evidence that age-specifictreatment improves older adults' complianceand outcomes (Kashner et al., 1992; Kofoed etal., 1987; Thomas-Knight, 1978).
Treatment works best when the issues dealtwith are congruent with the life stage of theclient. Younger and older adults' problemdrinking can usually be traced to different typesof problems, even when the emotional responses
9 5 73

Chapter 5
to the problems seem similar. For example, thedrinking of younger and older clients may bothbe attributed to depression, but the causes ofthat depression may be as different as beingunable to find one's first job and facing theprospect of retirement. Older adults willrecognize the problems of younger adults butmay no longer find them particularly relevant.Younger adults, with no knowledge of what it'slike to grow old, may lack empathy and becomeimpatient with older adults. The design ofeducational groups, the skills clients need toacquire, and the linkages that need to be madethrough case management are all different forolder adults than for younger adults. For all ofthese reasons, treating the older client in an age-specific setting is preferable.
Of course, this is not always possible,particularly for prescription drug abusers.Because very few older adults with prescriptiondrug problems seek treatment or are referred forcare, most drug treatment facilities do not havespecialty "older adult track" programming. Ifspecialized treatment is not available, olderadults can at least be grouped with youngerpeople whose lifestyles and problems are mostcompatible and with whom they feel mostcomfortable. It is difficult to treat older adultswho have only abused prescription drugstogether with consumers of illicit substances, oreven alcoholics who have "hit bottom."
Some clinicians argue that commonality inthe drug of choice is the most important factorin grouping patients. Because lifestyles varydramatically among different drug cultures, itmay be more important to group older patientswith other patients who also have a primaryproblem with legal drugs rather than by agecohort, gender, or socioeconomic status(Finlayson, 1995b).
If circumstances preclude treatment in anage-specific setting, a program can still addressthe age-specific themes of older clients by hiringat least one person specializing in work with
74
older adults. In mixed-age settings, casemanagement can provide an effective means ofaddressing age-specific themes.
A Culture of RespectTreatment programs should cultivate a cultureof respect for older clients. Nurturing clients'self-esteem and reawakening their sense ofthemselves as valuable, competent humanbeings are central to the process. Older adultsfrequently enter treatment depleted physically,socially, and emotionally, convinced that theirsituation is hopeless. Adding the stigma ofaddiction to the stigma of aging can compoundtheir despair. They may have been disowned bytheir families and rejected by friends because oftheir drinking or drug abuse. If they seek helpoutside the family, their experiences withagencies are often impersonal, dehumanizing,and humiliating.
To increase clients' self-esteem, staffmembers should express confidence in eachclient's ability to participate, persevere, andsucceed in treatment. Staff members need tostate this confidence frequently and at eachphase in the treatment process in a way that isupbeat but not patronizing. They should avoidacting overly helpful and implying that theindividual is impaired and helpless, at the sametime recognizing he or she, does need help withthe substance abuse problem. Managing his orher own life helps an older client regain self-esteem. Treatment providers should take care totreat all their clients with an unconditionalpositive regard, whether they are wealthy or onwelfare.
Many actions and speaking mannersdemonstrate respect in ways the older client willunderstand:
96
Abide by the manners that the older clientsees as customary (e.g., do not swear).Ask the individual how he or she would liketo be addressed and introduced to others.

Use surnames and formal terms of addressuntil given permission to be more familiar.
El Avoid condescending or patronizingbehavior.
m Speak directly to the client, not the client'sspouse or adult child, when the client ispresent.
m Recognize the client's privacy and personalspace. If making home visits or entering theclient's personal space at the treatmentfacility, acknowledge the client's ownershipof the space. Knock and gain permission toenter, ask where the person would like youto sit, and respond graciously to any offer ofhospitality, whether accepting the offer ornot. Make adequate provision for personalprivacy and the security of the person'spossessions, in both inpatient, and outpatientsettings.
m Talk to the client. Interacting spontaneouslycommunicates appreciation for the person asan individual. Honoring the client's pain,needs, and joys validates the person in his orher attempt to process life's experiences insobriety.
m Fulfill the client's request to speak to his orher clinician, immediately if possible.
m In a treatment program, a number of shorter,informal sessions, particularly in response toa patient's request, may be more valuablethan a longer, scheduled session. Honoring apatient's requests sends the message, "Youare important."
m Respect the client's spiritual concerns anddesire to discuss meaning and purpose inlife. Spiritual issues may be addressed byprofessional counselors or pastoralcounselors in addition to ministers or othermental health professionals trained inexistential interventions. Often, older adultshave a need to discuss these issues, andalcohol misuse may be a symptom of adeeply felt lack of purpose in life.
Referral and Treatment
Holistic Treatment Based on Age-Specific ProblemsTreatment programs are generally advised totake a broad, holistic approach. In treating theolder substance abuser in particular, it isnecessary to focus on more than just thedrinking or substance abuse problem. Aspeople age, the likelihood of multipleantecedent conditions for problem behaviorincreases. In other words, the individual'spsychological and health problems tend tobecome more complex, multiply determined,and interactive. Recent research suggests thatolder adults with alcohol problems often drinkin response to loneliness, depression, and poorsocial support networks (Schonfeld and Dupree,1995). Researchers have also noted chronic painas a high-risk condition for substance abuse.
A number of interrelated emotional, social,medical, spiritual, and practical problems orchanges characterize the older adult'sexperiences (see Figure 5-2). Some of these canprecipitate abuse of alcohol or other drugs.Those that initiate, sustain, or interact with thesubstance abuse problem provide the focus of aholistic treatment approach tailored to the needsof the individual.
Discussing life changes with patients canhelp them develop insight into the causes oftheir substance abuse problems. For example,while discussing salient nondrinking problemswith an older adult, the drinking problem oftenemerges naturally as a topic of discussion.Although the problems associated with agingcan be overwhelming, patients need not acceptthem passively. They can develop a self-careskill or positive attitude and can obtainappropriate help, such as the pharmacologicalalleviation of pain, management of grief, orskills for improving relationships.
0 7 75

Chapter 5
Figure 5-2
Life Changes Associated With Substance Abuse in Older Adults
Emotional and Social Problems
Bereavement and sadness Consequent sense of being a "nonperson"Loss of Social isolation and loneliness
Friends Reduced self-regard or self-esteemFamily members Family conflict and estrangementSocial status Problems in managing leisure time/boredomOccupation and sense of professionalidentity
Loss of physical attractiveness (especiallyimportant for women)
Hopes for the futureAbility to function
Physical distressChronic painPhysical disabilities and handicappingconditionsInsomnia
Medical Problems
Sensory deficits
HearingSight
Reduced mobilityCognitive impairment and change
Practical Problems
Impaired self-careReduced coping skillsDecreased economic security or new povertystatus due to
Loss of incomeIncreased health care costs
DislocationMove to new housing, or family moves awayHomelessnessInadequate housing
76
Program FlexibilityThe goals, setting, and duration of treatmentmay well be different for each client. The firststep toward ending problem drinking mayinvolve finding safe, affordable housing for oneclient, resolving depression for a second, orimproving relationships with a caregivingdaughter for a third. Elements of treatment,such as work assignments or exercise programs,will need to be tailored for the individualpatient.
It may be necessary to stop treatment whenillnesses or hospitalization intervene. Schedule
98
adjustments may be needed in recognition of thefatigue levels of older clients. The setting oftreatment may need to shift from clinic to homeduring a period of convalescence from a hipfracture or an illness. One client may need twiceas many treatment sessions to master stepstoward self-sufficiency as another client. Oneindividual may need to continue treatment for 2years to meet the goals another client reacheswithin 6 months.
Gender IssuesSome women patients may be better served byall-female treatment groups and facilities,

although studies comparing the effectiveness ofsingle-sex and mixed-gender programs arelacking. Panel members have observed thatmany older women defer to men and may takesubservient roles in a treatment group. Thesewomen could be less likely to become leaders inthe group or to build their self-esteem, althougha talented group therapist can turn the roles ofmen and women in the group into therapeuticassets.
Both women and men may have personalissues related to their drinking that they wouldbe reluctant to discuss with, or in the presenceof, members of the opposite sex. This reluctanceis likely to be greater for older adults, becausemany have a heightened need for privacy thatdiscourages open discussions of personal issuesand socialization with members of the oppositesex. In response, programs involving grouptreatment might afford opportunities forseparate meetings of males and females on anas-needed basis without disrupting the largerprogram. Such meetings may never benecessary, or take place intermittently,depending on the group members' needs orpreferences to discuss certain topics in same-sexsettings.
Although most problem drinkers are men,more women misuse prescription drugs, andthere are more women than men overall in theaging population. Women use morepsychoactive drugs than men do (Falvo et al.,1990; Ostrom et al., 1985; Venner et al., 1980;
Gomberg, 1995), and some researchers considerprescription drug abuse a major substance abuse
Referral and Treatment
issue among older women. Some studies reportthat older men are prescribed antidepressants asoften as or more often than women, but it is notknown whether this is a function of greater useof medical services by aging men or a differencein the diagnosis of depression among olderadults (Gomberg, 1992a, 1995).
Treatment ApproachesThe Consensus Panel recommends the followinggeneral approaches for effective treatment ofolder adult substance abusers:
Cognitivebehavioral approachesGroup-based approachesIndividual counselingMedical/psychiatric approachesMarital and family involvement/familytherapyCase management/community-linkedservices and outreach.
Not every approach will be necessary forevery client. Instead, the program leaders canindividualize treatment by choosing from thismenu to meet the needs of the particular client.Planning information comes from interviews;mental status examinations; physicalexaminations; laboratory, radiological, andpsychometric tests; and social networkassessments, among others.
Figure 5-3 lists the major treatment objectivesthat the Panel recommends for older substanceabusers and the approaches that can bestaccomplish them.
9977

Chapter 5
78
General Objectives/Examples
Figure 5 -3
Treatment Qhjectives and ApproachesGeneral Approaches/Examples
Eliminate or reduce substanceabuse
Cognitivebehavioral (group or individual)Alcohol (drug) effects
19 Relapse preventionStress management
Group approachesAlcohol (drug) effects education
MedicalNaltrexone, acamprosate (alcohol)
Safely manage intoxicationepisodes during treatment
MedicalRemove patient from activities and observeLink and refer to detoxification program
Enhance relationships Cognitivebehavioral (group or individual)Social skills and network building
Group approachesSocial supportSocialization skill educationGender-specific issues
Marital and family approachesSpouse counselingMarital therapy
11 Family therapy
Case managementLinkage to community social programsHome visitation
Individual counselingFocus on psychodynamic issues in relationships
Promote healthImprove sleep habitsImprove nutritionIncrease exerciseReduce tobacco useReduce stress
MedicalProvide primary medical care
Cognitivebehavioral (group or individual)Self-management skills training
Group approachesC Health educationili Education on nutrition, diet, cooking, shoppingIN Sleep hygiene
Stabilize and resolvecomorbidities
MedicalPsychiatric (e.g.,depression, anxiety)
II Sensory deficits
MedicalE Consultation and special assessments, including medication assessment
Primary and specialized medical carePsychiatric care for chronic mental disorders (by geriatric psychiatrist, ifpossible)
il Pain management for chronic pain disordersAntidepressants, antianxiety medication
Cognitivebehavioral (group or individual)I Relaxation training111 Depression
1 0 0

CognitiveBehavioral ApproachesThere are three broad categories of cognitive-behavioral approaches: behaviormodification/therapy, self-managementtechniques, and cognitive-behavioral therapies.Behavior modification applies learning andconditioning principles to modifying overtbehaviorsthose behaviors obvious to everyonearound the client (Powers and Osborne, 1976;Spiegler and Guevremont, 1993). Self-management refers to teaching the client tomodify his or her overt behaviors as well asinternal or covert patterns. Cognitive-behaviormodification involves altering covert patterns orbehaviors that only the client can observe.
Cognitive-behavioral techniques teachclients to identify and modify self-defeatingthoughts and beliefs (Dobson, 1988; Scott et al.,1989). The cognitive-behavioral model offers anespecially powerful method for targetingproblems or treatment objectives that affectdrinking behavior. Together, provider andclient analyze the behavior itself, constructing a"drinking behavior chain." The chain iscomposed of the antecedent situations,thoughts, feelings, drinking cues, and urges thatprecede and initiate alcohol or drug use; thedrinking or substance-abusing behavior (e.g.,pattern, style); and the positive and negativeconsequences of use for a given individual.When exploring the latter, it is particularlyimportant to note the positive consequences ofuse: those that maintain abusive behavior.
Researchers have developed an instrumentthat can elicit by interview the individual'sdrinking or drug use behavior chain (Dupreeand Schonfeld, 1986). Immediate antecedents todrinking include feelings such as anger,frustration, tension, anxiety, loneliness,boredom, sadness, and depression.Circumstances and high-risk situationstriggering these feelings might include marital
Referral and Treatment
or family conflict, physical distress, or unsafehousing arrangements, among others. Manyolder adults drink excessively in response toperceived losses and changes associated withaging and their affective and behavioralresponse to those losses. Alcohol use is often aform of "self-medication," a means to soften theimpact of unwanted change and feelings. Forthe patient, new knowledge of his or herdrinking chain often clarifies for the first timethe relationship between thoughts and feelingsand drinking behavior, a discovery one Panelmember calls "taking the mystery out ofdrunkenness." This method provides insightinto individual problems, demonstrates the linksbetween psychosocial and health problems anddrinking, and provides the data for a rationaltreatment plan and an explicit individualizedprevention strategy.
Breaking drinking behavior into the links of adrinking chain serves treatment in other ways,too. It suggests elements of the communityservice network that may be helpful inestablishing an integrated case managementplan to resolve antecedent conditions (e.g.,housing, financial, medical problems) thatnecessitate involvement from the communitybeyond the treatment program (see CaseManagement section).
Behavioral treatment can be used with olderadults individually or in groups, with the groupprocess particularly suited to older adults (seeGroup-Based Approaches section below).Equipped with the knowledge of theindividual's drinking or drug abuse behaviorchain, the group leader begins to teach the clientthe skills necessary to cope with high-riskthoughts or feelings. The leader teaches theolder person to initiate alternative behaviors todrinking, then reinforces such attempts. Theleader may demonstrate through role-playingalternative ways to manage high-risk situations,permitting the client to select coping behaviors
101 79

Chapter 5
80
that he or she feels willing and able to acquire.The leader may also ask for feedback from thegroup and use that feedback to work graduallytoward a workable behavioral response specificto the individual.
The behaviors are rehearsed within thetreatment program until a level of skill isacquired. The patient is then asked to try outthe behaviors in the real world as "homework."For example, a client who has been practicingways to overcome loneliness or social isolationmay receive a community-based assignment inwhich to carry out the suggested behaviors. Theindividual reports back to the group, then thetherapist and group members provide feedbackand reinforce the individual's attempt at self-management (whether the outcome was asuccess or not). This process continues until theindividual develops coping skills and brings theantecedents for abuse under self-control or self-management. Typically, as patients learn tomanage the conditions (thoughts, feelings,situations, cues, urges) that prompt alcoholabuse, abstinence can be maintained.
Defining drinking behavior antecedents isalso useful for determining when a client isready for discharge. When the individual hasacquired and can successfully use copingbehaviors specific to his or her antecedents fordrinking, the treatment team might begin toassist the person in gradually phasing out of theprogram. Discharge that takes place before theclient has acquired specific coping behaviors isalmost certain to result in relapseprobablyvery soon after discharge.
One older adult-specific treatment programthat has used these cognitivebehavioral andself-management approaches is the GerontologyAlcohol Project (GAP) (Dupree et al., 1984). Theprogram assessed antecedents on a typical dayof drinking for each person entering treatment.Group treatment involved skill acquisition inorder to cope with problems such as anger and
I,0
frustration, depression and grief, tension andanxiety, lack of social support, passivity, and anunstructured life. GAP staff were encouraged toteach skills at a slower pace than might be usedwith younger adults and to limit the amount ofinformation taught per session by followingwritten curriculum manuals. These teachingguides provided age-specific examples andmaintained consistency in teaching.
Confrontation was not permitted. Thisfacilitated more open discussion between staffand clients, encouraging clients to reportinstances when they slipped. This informationwas used in the group to help both the personwho slipped and other clients. Each slip wasdiagrammed in terms of that person's drinkingbehavior chain, with the antecedent conditionsand consequences, in order to teach groupmembers how to avoid or manage their ownhigh-risk situations. The group engaged inexercises or rehearsals of the necessary actionsand cognitions to prevent one drink (a slip) frombecoming a full relapse. A 1-year followup ofclients completing GAP indicated a high rate ofsuccess. Seventy-five percent of clientsmaintained their drinking reduction goals andincreased the size of their social supportnetworks (Dupree et al., 1984).
Later studies comparing early and late-onsetolder problem drinkers showed great similaritybetween these two groups' antecedents todrinking and treatment outcomes (Schonfeldand Dupree, 1991). Another study described abehavioral regimen that includedpsychoeducation, self-management skillstraining, and marital therapy. A followup studyof 16 male inpatients, ages 65 to 70, undertaken2 to 4 years after discharge, indicated that halfwere abstaining, two had reduced theirdrinking, and the remaining patients' drinkingwas destructive (Carstensen et al., 1985). Thesestudies recommend (and the Panel concurs) thattreatment focus on teaching skills necessary for

rebuilding the social support network; self-management approaches for overcomingdepression, grief, or loneliness; and generalproblem solving (Schonfeld and Dupree, 1990,1991).
Group-Based ApproachesGroup experiences are particularly beneficial toolder adults in treatment. They provide thearena for giving and sharing information;practicing skills, both new and long-unused;and testing the clients' perceptions againstreality. Perhaps the most beneficial aspect ofgroups for older adults is the opportunity tolearn self-acceptance through accepting othersand in return being accepted. Guilt andforgiveness are often best dealt with in groups,where people realize that others have gonethrough the same struggles. Special groups mayalso deal with the particular problems of aging;the group format can help patients learn skillsfor coping with any of the life changes identifiedin Figure 5-2.
Self-paced learning is best for older adults.To allow clients to set their own pace in a groupsetting, the leader can give individualized ortake-home assignments. Clients who have notreached the needed level of expertise on a topiccan receive an individualized "booster session"while remaining in the group. Older clients alsoshould get more than one opportunity tointegrate and act on new information. Forexample, information on bereavement can bepresented in an educational session, thenreinforced in therapy. To help participantsintegrate and understand material, it may evenbe helpful to expose them to all units ofinformation twice.
Groups help create a sense of camaraderieand high morale. Research on group work witholder adults suggests that older adults bond intogroups at a faster pace than younger adults do(Finkel, 1990). One successful treatment
Referral and Treatment
program made use of this phenomenon byassigning each person to another client whoserved as a "buddy," explaining and facilitatingthe day's events.
Some of the most effective types of groupsare socialization, therapy, educational, and self-help or support groups.
Socialization groupsGroups may focus on socialization skills:teaching clients skills for meeting new people,interacting better with peers, and giving themopportunities to practice. These skills are honedwhenever clients gather together, whether inrecreation, on coffee breaks, or at lunch. Thistype of activity is particularly valuable for thosewho live with loneliness or who have becomesocially isolated.
Panel members report that many older adultskeep in touch with friends they made duringtreatment, especially if the treatment programsponsored social activities. Some treatmentprograms sponsor an evening a week whereclients can socialize, which helps them rebuildor expand their social contacts in thecommunity.
Therapy groupsSome therapy groups engage in behavioralinteraction, as discussed above, others in morepsychodynamic therapy. Both types of groupsallow clients to test the accuracy of theirinterpretations of social interactions, measurethe appropriateness of their responses to others,and learn and practice more appropriateresponses. Groups provide each client withfeedback, suggestions for alternative responses,and support as the individual tries out andpractices different actions and responses.
Some people may need help in entering thegroup, particularly if they are accustomed toisolation. This help could include individualcounseling sessions in which the counselorexplains how a group works and answers the
10 381

Chapter 5
82
client's questions regarding confidentiality. Theclient's entry into the group may be eased byjoining in stages, at first observing, then overtime moving into the circle. The counselor mayformally introduce the new person to themembers of the group so that upon entering thegroup, he or she is at least somewhat familiarwith them.
Older adults grew up before psychologicalterms had been integrated into the everydaylanguage. Therefore, therapy groups for olderadults should avoid the use of jargon, acronyms,and "psychspeak." If leaders do use such terms,they should begin by teaching the group theirmeanings. If a participant uses an unfamiliarterm, the leader should explain it. It may behelpful to develop a vocabulary list on a chartand for any individual notebooks. Similarly,because many older individuals were raised notto "air their dirty laundry," they should neverbe pressured to reveal personal information in agroup setting before they are ready. Nor shouldolder patients be pressured into "role-playing"before they are ready.
Educational groupsEducational groups are an integral part ofaddiction treatment. Patients need informationabout addiction, the substances, their use, andtheir impact. Older adults also benefit fromshared information about the developmentaltasks of the later stages of life, support systems,medical aspects of aging and addiction, theconcepts and processes of cognitivebehavioraltechniques, and experiences they are likely to befacing, such as retirement, loss, partner's illness,and family concerns. Educational units can bedesigned to teach practical skills for coping withany aspect of daily life, such as nutrition,household management, or exercise.
Some basic principles for designingeducational groups follow:
104
Older adults can receive, integrate, and recallinformation better if they are given a clearstatement of the goal and purpose of thesession and an outline of the content to becovered. The leader can post this outline andrefer to it as she moves through the session.The outline may also be distributed for use inpersonal note-taking and as an aid in reviewand recall. Courses and individual sessionsshould be conceived as building blocks thatare added to the base of the older adult's lifeexperience and needs. Each session shouldbegin with a review of previously presentedmaterials.
Members of the group may range ineducational level from being functionallyilliterate to possessing advanced degrees.Many older adults are adept at hiding a lackof literacy skills. These individuals need tobe helped in a way that maintains their self-respect. Group leaders should choosevocabulary carefully to comply with clients'communication skills.Groups should accommodate clients' sensorydecline and deficits by maximizing the use ofas many of the clients' senses as possible.Simultaneous visual and audiblepresentation of material, enlarged print,voice enhancers, and blackboards or flipcharts can be helpful. An overhead projectorallows the leader to display written materialon a screen while facing and speaking to thegroup. Group members may also take homesupplemental audiotapes and videotapes forreview.
It is important to recognize clients' physicallimitations. Group sessions should last nolonger than about 55 minutes. The area shouldbe well lighted without glare, and interruptions,noise, and superfluous material should be keptto a minimum. Distractions generally interfere

more with learning for older patients than foryounger ones (Myers and Schwiebert, 1996).
Alcoholics Anonymous and otherself-help groupsMany treatment programs refer patients toAlcoholics Anonymous (AA) and other self-helpgroups as part of aftercare. Providers shouldwarn older patients that these groups mightseem confrontational and alienating. Thereferring program should tell patients exactlywhat to expectthat the group discussions maywell include profanity and younger members'accounts of their antisocial behavior. To orientclients to these groups, the treatment programmay ask that local AA groups provide aninstitutional meeting as a regular part of thetreatment program. Other options are to helpclients develop their own self-help groups oreven to facilitate the development ofindependent AA groups for older adults in thearea.
Individual Counseling or Short-Term PsychotherapyIndividual counseling is especially helpful to theolder substance abuser in treatment's beginningstages, but the counselor often must overcomeclients' worries about privacy. Subjects thatmany older adults are loath to discuss includetheir relationships to their spouses, familymatters and interactions, sexual function, andeconomic worries. It is essential to assure theclient that the sessions are confidential and toconduct the sessions in a comfortable, self-contained room where the client can be certainthe conversation will not be overheard.
Older clients often respond best tocounselors who behave in a nonthreatening,supportive manner and whose demeanorindicates that they will honor the confidentialityof the sessions. Clients frequently describe thesuccessful relationship in familial terms: "It is
Referral and Treatment
like talking to my son," or, "It is as though shewere my sister." Older clients value spontaneityin relationships with the counselor and otherstaff members; a counselor's appropriate self-disclosure often enhances or facilitates abeneficial relationship with the patient.
Because receiving counseling may be a newexperience for the client, the provider shouldexplain the basics of counseling and clearlypresent the responsibilities of the counselor andthe client. Summarizing at the beginning ofeach session helps to keep the session moving inthe appropriate direction. Summarizing at theend of a session and providing tasks to bethought about or completed before the nextsession help reinforce any knowledge or insightsgained and contribute to the older client'sfeeling that she is making progress.
In individual sessions, counselors can helpclients prepare to participate in a therapy group,building their understanding of how the groupworks and what they are expected to do.Private sessions can also be used to clarify issueswhen the individual is confused or is tooembarrassed to raise a question in the group. Asthe client becomes more comfortable in thegroup setting, the counselor may decide to taperthe number of individual counseling sessions.Likewise, the client may prepare for dischargeby reducing the frequency or length of sessions,secure in the knowledge that more time isavailable if needed.
Medical/Psychiatric ApproachesOlder substance-abusing clients differ from theiryounger counterparts in the number andcomplexity of associated health problems.Unless these problems are recognized and eithercorrected or stabilized, the patient'sparticipation in substance abuse treatment willbe compromised and chances for recoverydiminished. Especially in older adults, healthproblems interact with and impair social and
105 83

Chapter 5
84
psychological function, adding to the complex ofcauses for the patient's dysfunction anddisability.
Medications used to modify drinkingbehavior in older adults must take into accountage- and disease-related increases invulnerability to toxic drug side effects, as well aspossible adverse interactions with otherprescribed medications. Disulfiram is notgenerally recommended by the Panel for use inolder patients because of the hazards of thealcoholdisulfiram interaction, as well as thetoxicity of disulfiram itself.
Naltrexone, an opioid receptor blocker withmild opioid agonist actions, has been shown toreduce drinking in younger alcoholics incontrolled studies. A controlled pilot study ofits use among older men under age 70 foundthat these patients tolerated the drug well (Os linet al., 1997). Moreover, there was suggestive
evidence for reduction in drinking relapses innaltrexone treated patients. Acamprosate, aglutaminergic drug, has shown considerablesuccess in reducing drinking in youngeralcoholics in European controlled trials (Litten etal., 1996). Acamprosate has not been specificallystudied with older adults.
Visual and hearing problems compromiseeffective coping and the accomplishment of thetasks of daily living, interfere with socialfunctioning, and may prevent effectiveparticipation in substance abuse treatment.Accordingly, initial medical assessment of olderadults should routinely include screening forvisual and auditory problems, and anyproblems discovered should be corrected asquickly as possible.
Many older alcoholics do without neededhealth care; linking them to a health careprovider can be a profoundly valuable service.The substance abuse treatment program shouldconsider, whenever possible, educating olderclients on such health promotion themes as
1 0 (3
desirable diet and nutrition, daily exercise, sleephygiene and the benefits of routine healthchecks.
A thorough, age-specific medical evaluationshould be completed for each patient at entryinto alcoholism treatment if it was not done bythe referring source. The evaluation can becompleted in-house in larger programs thathave a primary care provider on staff, by aconsulting provider, or by the patient's personalphysician. Trained nonmedical staff can easilydo portions of the evaluation, such as screeningfor age-related macular degeneration (AMD), aleading cause of blindness in older adults.Positive results would indicate the need forfurther evaluation by a professional (e.g.,referral to an opthalmologist). The treatmentprogram should review this evaluation.
The medical evaluation should alwaysinclude an assessment of medication use,because of the potential for medication andalcohol interactions. To determine themedication use of older adults, the "brown bagapproach" is helpful (Finch and Barry, 1992).The practitioner can ask older adults to bringevery medication they take in a brown paperbag (e.g., all medications prescribed by a doctor;all medications, vitamins, etc., they got at thedrugstore; any herbs that anyone gave them totry). This will provide an opportunity to betterdetermine potential medication interactionproblems.
Chronic mental illness such as depression,bipolar and recurrent major depressivedisorders, chronic schizophrenia, and severeanxiety disorders will require ongoing care.Research suggests that some patients withschizophrenia cannot manage the interpersonalintensity of group therapy for addictions and aremore suitably managed on a one-to-one basiswith an addictions counselor who consults witha psychiatrist (Finlayson, 1995a). Some patientswith severe disorders, including some with

dementia, may be better managed in a mentalhealth or long-term care setting than in asubstance abuse program, provided a geriatricpsychiatrist is involved, at least for consultation.
The epidemiology of depression among olderadults is controversial (Weiss, 1994). Accordingto the Epidemiologic Catchment Area Study,depressive symptoms occur in an estimated 15percent of community residents over the age of65. Estimates of major depression among thesame age group are usually less than 3 percent.Rates of major or minor depression among olderadults seeking care from primary care cliniciansor residing in nursing homes range from 15 to 25percent (National Institutes of Health, 1991).Among those hospitalized for physical illnesses,approximately 10 percent suffer from a majordepressive disorder, whereas an estimated 30percent experience minor depressions (Koenigand Blazer, 1996). Despite expectations thatrates of depression among older adults wouldbe high, studies have not generally confirmedthis view. One reason for this failure may bethat "many depressions in this age group aresubsyndromal and do not fit well into thecurrent nomenclature" (Koenig and Blazer, 1996,p. 417). Another explanation may be thatsymptoms "are often lost amid 'real' medicalproblems of the aged" (Weiss, 1994, p. 5).Researchers estimate that between 10 and 30percent of older alcoholics have long-lasting orrecurrent depressive symptoms (Blazer et al.,1987b). Some fulfill criteria for major depressivedisorder, dysthymic disorder, or cyclothymicdisorder. Others do not meet criteria for any ofthese diagnoses yet suffer from depressivesymptoms that fall under the category ofsubsyndromal depression. Depression forseveral days or longer immediately following aprolonged drinking episode does not necessarilyindicate a true comorbid disorder or the need forantidepressant treatment in most cases(Atkinson and Ganzini, 1994; Brown and
Referral and Treatment
Schuckit, 1988; Schuckit, 1994). When
depressive symptoms persist several weeksfollowing cessation of drinking, specificantidepressant treatment is indicated (Brown etal., 1995).
Family Involvement and Therapy
Involving family members intreatmentThe Panel recommends gathering detailedinformation about the client's relationships fromfamily members in the evaluative and planningphases of treatment. This information will affecttreatment planning whether or not familymembers currently share a home or remaininvolved in each other's lives, as past eventsmay bear upon the substance abuse. On thebasis of the individual's drinking antecedents,the treatment team can decide whether family ormarital therapy is appropriate.
Family members, including adult children,can play a critical role in the older client'streatment (Dunlop, 1990; Dunlop et al., 1982;Myers, 1989). Married older alcoholics are morelikely to comply with treatment if their spousesalso become involved in the treatment process(Atkinson et al., 1993).
The types of individuals who are appropriateto involve in the client's treatment will varyfrom one client to the next. Some older clientsmay be out of touch with family members ormay live far away from relatives. Dupree andcolleagues found that, on average, late onsetalcoholics had a total of four friends and fourfamily members with whom they were incontact (Dupree et al., 1984). Daily contactsaveraged less than one a day. The person who isclosest to the client may be a golfing partner, ahousemate, a caseworker or health provider, thebank trustee of the person's estate, or a privatesocial service worker hired by the bank. Someolder adults cohabit in long-standing common-
107 85

Chapter 5
law relationships without marrying out ofconcern for grandchildren's opinions or forfinancial or other reasons. Such nontraditionalfamily members may be considered "family" forpurposes of treatment.
Eliciting family information requiressensitivity and skill: Older adults are lesswilling than younger adults to discuss "familybusiness." The client's family may close ranksas well and choose not to disclose events thatthey fear could hurt or disturb the client. Inworking with family issues or family groups, aprovider should emphasize airing and bringingclosure to past conflicts and concerns and negateany blame.
Treatment staff need to be cautious indeciding what information to share, with whichfamily members, and when (if at all). Forexample, the role of adult children in the client'slife can be problematic. Although adult childrenmay have new responsibilities for taking care ofthe patient, they may also be problem drinkerswho collude in the client's drinking, supply theclient with alcohol, or help the client rationalizethe drinking problem.
Family and marital therapyThe dynamics of a marriage can changedrastically as couples grow older. Thesechanges stem from retirement, the deaths offriends, and health issues that affect maritalrelationships, such as changes in sexual functionor the need for caregiving. Any of the issuestypically experienced by older adults, such asfinancial concerns or fear of the death of aspouse, can affect the stability of the marital
relationship and place additional stress on theclient in treatment.
The best setting for providing counseling tosubstance-abusing older patients with maritalproblems may be individual couple counselingor in a group setting with other couples ofsimilar age. Counseling the couple separately
86
108
from the group is advisable for addressing verypersonal concerns such as sexual problems orother highly sensitive issues that could bedamaging to the couple's marriage.
Case Management, Community-Linked Services, and OutreachCase management is the coordination and
monitoring of the varied social, health, andwelfare services needed to support an olderadult's treatment and recovery. Casemanagement starts at the beginning of treatmentplanning and continues through aftercare. Oneperson, preferably a social worker or nurse,should link all staff who play a role in theclient's treatment as well as key family membersand other important individuals in the client'ssocial network.
The multiple causes of older adults'problems require multiple linkages tocommunity services and agencies. Thetreatment program that seeks to be the solesource of all services for its older clients is likelyto fail. Even in very isolated areas, programscan strengthen their services for older adultsthrough linkages to local resources such as thefaith community.
The case manager will likely refer the clientto a combination of several community
resources in response to the issues associatedwith the substance abuse problem. Casemanagers must have strong linkages throughboth formal and informal arrangements withcommunity agencies and services such as
Medical practitioners, particularly mentalhealth providers, geriatricians, and geriatriccounselors
E Medical facilities for detoxification and otherservices
Home health agencies.

Housing services for specialized housing(i.e., wheelchair-accessible housing,congregate living)Public and private social services providingin-home support for housekeeping, meals,etc.
Faith community (e.g., churches,synagogues, mosques, temples)Transportation servicesSenior citizen centers and other socialactivitiesVocational training and senior employmentprogramsCommunity organizations that place clientsin volunteer workLegal and financial servicesThe Area Agency on Aging (funded underTitle 20).
If a program includes outreach services, casemanagement may offer the best means ofproviding them (Graham et al., 1995b;Fredriksen, 1992). Case managers may, forexample, initiate outreach services forhomebound clients, although it is important tomaintain continuity and assign only one casemanager to an older client. If clients in atreatment program become seriously ill ordysfunctional and temporarily require servicesat home, a case manager may be the ideal staffperson to broker services on their behalf.(Comprehensive case management for substanceabuse treatment will be described in detail in aforthcoming TIP to be published in 1998.)
Other Adjunctive ApproachesA number of other treatment approaches areuseful in responding to older substance abusers.Generally, however, they work best when theycomplement the major approaches alreadydiscussed.
Spiritual or religious counseling with aclergy member, either in a group or individual
Referral and Treatment
setting, may be an important adjunct to therapyfor individuals who feel more comfortableaddressing their concerns in a religious context.Many older adults are concerned about theirspiritual preparation for death, even when it isnot imminent, and welcome opportunities toexplore that topic.
Substance abuse treatment providers aremoving toward a greater recognition of the roleof spirituality in recovery, and providers shouldnot hesitate to build on the religious beliefsystems of older clients, when appropriate.From its inception, Alcoholics Anonymous hasspoken of "a higher power," and much of itseffectiveness may derive from its spiritualaspects. One caution: Older adults who havenever subscribed to a religious belief systemmay not be ideal candidates for spirituallyoriented therapy or referral to 12-Stepfellowship programs.
One Panelist observed that spirituality isoften a key element in brief interventions,especially in minority communities. Programsthat specialize in the treatment of a particularethnic or racial group may adopt strategiesspecific to that group (e.g., the use of tribalrituals in the treatment of Native Americansubstance abusers). A variety of nontraditionalmethods for tension reduction (e.g., therapeuticmassage, meditation, acupuncture) have beensuggested as applicable to older adults,although these methods remain largelyuntested.
Discharge Plans and AftercareEffective discharge planning is essential to
case management for older clients because theirsocial networks may have shrunk as a result oftheir substance abuse problems, physicallimitations, or the loss of family members andfriends. In this context, it is vitally important forclients' counselors or case managers to helpthem tap into available community resources by
W9 87

Chapter 5
88
assisting them in identifying ongoing needs(e.g., income maintenance, housing), schedulingservices (e.g., Homemakers, eye care, hearingtests, financial planning), and obtainingequipment (e.g., large-number telephones, homebanking systems, walkers and other devices).
As part of the discharge process, a counseloror case manager also develops an aftercareprogram with the client. For older adults, thismay entail arranging transportation to follow-up appointments and reminders to note datesand times on the calendar, as well as fulfillingmore traditional functions like monitoringprogress to prevent or reduce the negativeimpact of relapse. Standard features of mostdischarge plans for older adults include
Age-appropriate Alcoholics Anonymous,Pills Anonymous, Rational Recovery,women's or other support groupsAncillary services needed to maintainindependence in the communityOngoing medical monitoringInvolvement of an appropriate case managerif needed to advocate for the client andensure needed services are provided.
Aftercare and recovery services for olderclients differ in some respects from thosetypically offered by some substance abusetreatment programs where fraternization isdiscouraged. Programs oriented to older clientsoften sponsor socialization groups or weeklytreatment alumnae meetings run by long-soberpeer counselors. Others allow clients to returnto the program to participate in group theiapy.Still others initiate a network of contacts forolder clients and teach them how to expand it.
Some communities have established,integrated social service networks that enableclients to receive coordinated care. However,stand-alone programs in communities withoutdefined networks may have to initiate linkageswith other services themselves. Some treatment
110
programs have begun this process of networkbuilding by publicizing their services to otherlocal agencies and health care facilities. Priorconsultation with the local Office on Aging andother resources in the community that targetolder adults helps to ensure that the resultingnetwork is responsive to their special needs. Inrural areas, treatment programs serving olderadults face additional challenges. In thesesettings, collaboration among health and socialservice programs is crucial to resolve problemsposed by geography, lack of public
transportation, sparse and distant services, andsocial isolation. CSAT's Technical AssistancePublications Rural Issues in Alcohol and Other
Drug Abuse Treatment (CSAT, 1996), Treating
Alcohol and Other Drug Abusers in Rural and
Frontier Areas (CSAT, 1995b), and Bringing
Excellence to Substance Abuse Services In Rural and
Frontier America (CSAT, 1997) have more
information on surmounting these barriers.
Specialized TreatmentIssues for PrescriptionDrug AbuseBecause so many problems with prescriptiondrug abuse stem from unintentional misuse,approaches for responding to these clients differin some important respects from treatment foralcohol abuse and dependence. Issues that needto be addressed as part of treatment includeeducating and assisting patients who misuseprescribed medications to comply consistentlywith dosing instructions, providing informal orbrief counseling for patients who are abusing aprescribed substance with deleteriousconsequences, and engaging drug-dependentpatients in the formal treatment system at theappropriate level of care. In addition, it isimportant for providers to understand howpractitioners' prescribing behavior contributes

to the problem so they can address it both withclients and uninformed health care practitionersin the community.
Misuse by the PatientSome experts estimate that as many as 70
percent of depressed older patients fail to take25 to 50 percent of their medications, producingwide fluctuations in blood levels andjeopardizing the efficacy of therapy (NationalInstitutes of Health, 1991). Such widespreadmisuse of prescriptions requires intensive effortsto determine the reasons for noncompliance andto educate patients about medicationmanagement. In general, the causes ofnoncompliance with a prescribed medicationregimen can be categorized as
A lack of judgment or misconceptions about
the drugsAn inability to manage the medicationregimen, either because it is complex or thepatient has persistent memory problems andwill need regular supervisionInsufficient resources for purchasing orstoring the medicationsIntentional misuse to obtain results otherthan for those prescribed (e.g., pain pills tosleep, relax, soften negative affect).
Unless patient interventions address the realreasons for noncompliance, they are not likely tobe effective. If initial observations and questionsabout prescription drug use suggest misuse,more information will be needed so thatremedies can be appropriately targeted. Forexample, if a 73-year-old woman is skippingdoses of her blood pressure medication, theprovider needs to learn whether this happensbecause (1) the patient only takes the medicinewhen she feels ill rather than on the prescribedschedule, (2) the medicine sometimes makes herfeel unpleasantly dizzy, (3) the patientfrequently forgets whether she took the
Referral and Treatment
medicine, or (4) the patient cannot afford thedrug and tries to do without from time to timeso that she will have a supply available whenshe feels she needs it.
If the patient's noncompliance is due toeconomic considerations, then teaching her howto manage medications by separating them intocontainer compartments for each day of theweek (or hour of the day) will not be helpful.That strategy might be appropriate, however,for another patient who has suffered a strokeand has real difficulty with short-term memory.
Medication noncompliance may take the
following forms:
Omitting doses or changing the frequency ortiming of dosesDoubling up on the dosage after forgetting totake the previous doseTaking the entire day's medications in themorning for fear of forgetting to take all the
doses of all the medications as prescribedIncreasing doses or dosing frequencyTaking the wrong drugsBorrowing or sharing drugsSupplementing prescribed drugs with otherover-the-counter medications or "leftover"medicines from an earlier illnessContinuing to use alcohol or othercontraindicated drugs or foods while takingthe prescribed medicinesEngaging in contraindicated activities whiletaking the medications (e.g., driving motorvehicles, spending time in the sun)Failing to tell the prescribing physician aboutall the other medications (prescribed andover-the-counter) being used or to reportsignificant or unexpected side effects or
adverse reactionsStoring medications improperly (notrefrigerating those that require a continuedcold temperature) or using prescriptionswith expired expiration dates.
111 89

Chapter 5
The patient and the health care practitionershare responsibility for ensuring that the patientunderstands all dosing instructions, thepurposes of the medications prescribed, and theunpleasant side effects or adverse reactions thatshould be reported to the doctor. However,providers can also instruct patients to takeadvantage of pharmacists' services in providingpersonal advice and computer-generatedinstructions regarding specific drugs, sideeffects of varying intensity and seriousness,contraindications for use, and when beneficialeffects can be anticipated. Many materials havealready been developed and are widelyavailable for educating older adults and othersabout medication compliance strategies andtheir importance. These can be obtained from,numerous sources, including home health careagencies, State and local offices on aging, theSubstance Abuse and Mental Health ServicesAdministration (through the NationalClearinghouse for Alcohol and DrugInformation), the National Council on Aging,and the American Association of RetiredPersons.
Treatment providers can help empower olderadults to ask more questions and optimize thebenefits of their contacts with medical
professionals. Older patients with somecognitive or sensory impairment may not beable to adhere to complicated medicationregimens. In these cases, treatment providerscan identify and educate family members orother professional or volunteer advocates andcaregivers about the need to assist the olderadult with this task.
Once the substance abuse treatment provideridentifies a medication misuse problem,arrangements should be made for an initial butintensive monitoring of the patient's use of theproblematic drug. Monitoring may beundertaken by visiting or public health nursesor other designated medical staff. The objective
90
is to determine whether misuse continuesdespite all attempts to correct underlyingreasons for noncompliance. If the patientappears to be knowingly noncompliant, thebehavior is characteristic of abuse.
The intervention for this behavior willdepend on an accurate and in-depth assessmentof the social, medical, and psychologicalproblems that may be driving the substanceabuse (e.g., depression, bereavement, a medicalcondition, social isolation, physical pain,insomnia). Assessment results then provide thebasis for an individualized treatment plan thatincludes and ranks mechanisms for addressingeach issue. Unless the abuse has resulted in a
serious crisis, it is usually appropriate to try
psychosocial approaches first, including grieftherapy, sleep management training, relaxationtechniques, socialization (day care) programs,psychotherapy, and acupuncture.
Once treatment begins to resolve theunderlying issues, the provider must conferwith the health care practitioner to determinewhether the older adult should remain on theproblematic drug at a reduced dose, discontinueuse altogether, or switch to an alternativeprescription with less addictive potential. Thechoice will depend on what options areavailable and the severity of the problemsexperienced as a result of the substance abuse.The Panel recommends an open discussion ofthese issues with the patient, substance abusetreatment provider, and health care practitioner.
Misuse (Misprescribing) by theHealth Care ProviderHealth care professionals need to keep abreastof current information about appropriateprescribing practices for older patients as well asnew drugs with less hazardous profiles. Olderadult-specific protocols must stress medicationassessments for all patients; lower initial dosesand time-limited dosing patterns for
1

psychoactive and other agents; use of new andless complex drugs with simple metabolicpathways and less dangerous side effects;avoidance of more hazardous substances withlong half-lives that cannot easily be absorbed oreliminated by older adults; and appropriate,consistent monitoring of patients' reactions toprescribed drugs.
Health care professionals also need to bereminded of ways to convey information thatare easily understood and used by older patients(e.g., written as well as spoken, disseminated tofamily caregivers and advocates as well as thepatient). When prescribing medications forolder adults, it is also useful to consider thefamily situation. Are other family memberslikely to share their medication with the patientor use it themselves? Is there a family memberwho will help the older patient track hismedications, comply with the practitioner'srequest to bring unused medications to thepractitioner, remind the patient to discardexpired medication, or remove the medication atthe practitioner's request? Family members canbe important allies in preventing problems fromdeveloping or escalating.
Some ways in which health careprofessionals might be motivated to adopt"best" prescribing practices for older patientsinclude
Making relevant publications such as this TIPand other resources easily available on theInternet and widely disseminated throughmedical societies, other health-relatedprofessional groups, and health carepractitioner training programsAdding or updating older adult-specificinformation in the Physician's Desk Referenceand other pharmacist-approved publicationsregarding psychoactive prescription drugswith abuse potential
Referral and Treatment
Is Providing Continuing Education Units forattending workshops at medical conferencesand other health care professional meetingson prescription drug use and abuse amongolder patientsTraining primary care physicians and otherhealth care providers to consult morefrequently with pharmacists, psychiatrists,and other psychopharmacologists regardingthe risk and benefit profiles of thepsychoactive drugs they prescribe ratherthan relying on outdated materials or theirown authorityEmpowering older patients and theiradvocates to ask health care providersquestions about the rationale for all profferedprescription medications as well as dosingprotocols, schedules, expected anddangerous side effects, and interactions withother medications or foodEnsuring that any attempts to restrictprescribing practices through legislation andregulations do not encourage prescriptions ofmore hazardous substances or makelegitimately needed medications even moredifficult for patients to obtain.
Staffing ConsiderationsThe Consensus Panel recommends that thefollowing principles guide staffing choices insubstance abuse treatment programs:
Whenever possible, employ staff who havecompleted training in gerontologyEmploy staff who like working with olderadultsProvide training in empirically demonstratedprinciples effective with older adults to allstaff who will interact with these clients.
91

Chapter 5
Credentials and Training forProgram StaffStaff working with older adults need tounderstand the developmental tasks of agingand the basic principles of educational
gerontologyhow older adults learn andprocess material. For this reason, Panelmembers believe that any program that treatseven a few older adults should have at least onestaff person who is trained in the specializationof gerontology within his or her discipline. Thistraining should consist of at least a graduatecertificate program (6 to 12 months) in thesubfield of aging commonly called socialgerontology. Staff with professional degreesshould have a specialization in gerontology,
geriatrics, or psychogeriatrics. If staff lackappropriate credentials, it can be difficult for theprogram to receive reimbursement frominsurance companies or funding from otherfunding streams.
Any program that seeks to serve older adultsshould also have a registered nurse on staff.Ideally, this nurse would have a background inphysical health, addictions, and gerontology. Infreestanding programs that assign only oneperson to older clients (common in rural areas),a master's degree in nursing with a specialty ingerontology is preferred.
Large programs with interdisciplinary teamsshould include a registered nurse, a socialworker, and chemical dependency counselors.All staff should have master's-level trainingwith specialties in gerontology. The socialworker should be prepared to carry out casemanagement roles including liaison tocommunity agencies.
The Panel recognizes that some programs inisolated areas may serve only a few older adultsin a mixed-age setting and may be unable toretain staff members with optimal training. Insuch instances, the staff person chosen to workwith older clients should have a strong desire to
92
do so and should have some knowledge of thedevelopmental tasks of aging, even if this isgained through experience rather than formaleducation. Wherever feasible, programs thathave no appropriately trained staff shouldencourage at least one staff member to attaincertification.
Programs with linkages to layers ofserviceslarge addictions programs orprograms linked to hospitals, health caresystems, or multiservice agenciesare commonin urban settings. The following professionalsshould ideally be available to a treatmentprogram, whether as members of the program'streatment teams or as resources availablethrough the program's linkages with otherservices:
114
A geriatricianA geriatric psychiatrist
I A geropsychologistA gerontological counselor
E A nutritionist
An activities director or recreational therapist(to make home visits, increase socialization,teach activities to fill leisure time)
A chaplain or other member of the clergyOccupational therapistsSocial workers (clinical, community,administrative)Peer counselors (particularly valuablebecause they have many life experiences incommon with clients).
Orientation and training of all staff is a
necessity. Staff should understand and believethat the prognosis for recovery for adults in thisage group is favorable. They should understandthat older adults can learn and change, and theyshould be capable of showing respect to theirolder clients. Special training on counselingskills and their application with older adultsshould be available to peer counselors and otherprogram clinicians on an ongoing basis.

Attributes and Personal TraitsFacilities should project the attitude that theywant to serve older adults. When centers offerage-specific programs with staff experienced inaging issues and interested in working witholder adults, use by older adults increases(Fleming et al., 1984; Lebowitz, 1988; Lebowitz
et al., 1987; Light et al., 1986). Similarly, in the
treatment of alcohol abuse, research suggeststhat age-specific programs may be moreattractive and effective (Atkinson, 1995; Kofoed
et al., 1987).
It is important that all staff who work witholder clients actually like adults of this agegroup. When hiring, program staff should try todetermine how older adults fit into theapplicant's life. Does the applicant interact withan older person by choice, as a friend? Does heor she interact with older family members on aregular basis? Does he or she interact with olderadults on a regular basis through volunteeractivities or other activities in the community?
Staff need a sense of the issues involved inaging. This understanding can be gainedthrough training, empathy, or the personal
Referral and Treatment
experience of growing older. With thisunderstanding comes a willingness to listen andto be patient with the older adult's pace ofmovement and speech. A sense of humor is alsoimportant. Nonconfrontational personalitiestypically work better with older adults. Peoplewho prefer an emotional or confrontationalapproach to therapeutic interaction are notappropriate candidates for work with olderadults. Staff should be able to work in groups astrainers or teachers. Staff who work with olderadults also need to be flexible and willing tocarry out tasks that may not be considered"professional."
Staff members and volunteers need to beopen to multiple avenues to recovery. Ifrecovering staff see their own route to recoveryas superior or the only way, it may limit theirability to work effectively with older adults,who tend to require more flexible approaches inorder to find their path. Effective treatment forthe older adult is more holistic, moresupportive, and often a great deal morecomplicated than standard addiction treatment.
93

6 Outcomes and Cost Issues inAlcohol Treatment for 01 erAdults
Outcomes research is concerned not onlywith results of studies but also withdetermining what exactly should be
studied. For alcohol treatment among olderadults, for example, should the measure ofsuccess be treatment compliance? Amount ofalcohol consumed? Level of physical health?Psychological well-being? This chapter reviewscompliance studies and prospective studies ontreatment for older adults and examines themeasures used. Because there have been fewsystematic studies of alcoholism treatmentoutcome (Atkinson et al., 1993) or the costs oftreatment (Institute of Medicine, 1990) for olderadults, this chapter also applies more generalstudies to that population. There are virtuallyno outcome studies of prescription drug usetreatment for older adults, so this chapteraddresses alcohol use only.
The chapter also provides an overview ofinstruments for measuring various treatmentoutcomes, instruments that are more importantthan ever as the health care system movestoward managed care. Payers increasingly arereimbursing only treatment approaches thathave been validated by outcome studiesinparticular, studies that quantify resourcesavings. Treatment costs and reimbursement
issues are discussed, and the chapter ends withrecommendations for future research.
Spectrum of AlcoholTreatment Outcomes
Brief Intervention OutcomesRandomized controlled trials in other countrieshave demonstrated that brief interventions canreduce alcohol use and related problems in at-risk or nondependent problem drinkers underage 65 (Saunders et al., 1993; Anderson and
Scott, 1992; Persson and Magnusson, 1989;Wallace et al., 1988; Kristenson et al., 1983). (For
a more complete discussion of briefinterventions, see Chapter 5.) Brief interventionstudies have been conducted in health caresettings ranging from hospitals and primaryhealth care locations (Chick et al., 1988; Wallaceet al., 1988; Babor and Grant, 1992a; Fleming et
al., 19976) to mental health clinics (Harris andMiller, 1990). The first randomized controlledU.S. trial in community-based primary carepractices, the Trial for Early Alcohol Treatment(Project TREAT), which studied adults age 65and younger (Fleming et al., 19976), found thatbrief intervention for alcohol problems in
Ltd95

Chapter 6
96
primary care patients reduced both alcoholconsumption and consequences.
A study of brief physician advice with at-riskdrinkers age 65 and over, Guiding Older AdultLifestyles (Project GOAL), also found positivechanges in drinking patterns of the experimental(n = 158) compared with the control group (n =
71) (Fleming et al., 1997a). At the time of the 12-month followup, there was a significantreduction in 7-day alcohol use (t = 3.77; p < .001),episodes of binge drinking (t = 2.68; p < .005),and frequency of excessive drinking (t = 2.65; p <.005). The results indicated that brief physicianadvice made a difference in the drinkingpatterns of older at-risk and problem drinkers.
Most studies of alcohol brief interventionshave only included patients early in theirdrinking careers, explicitly excluding dependentdrinkers with significant withdrawal symptoms.The rationale for this practice has been that
alcohol-dependent individuals or those affectedmost severely by alcohol should be referred toformal specialized alcoholism treatment
programs because their conditions are not likelyto be amenable to a low intensity intervention(Institute of Medicine, 1990; Babor, 1994).
However, only one study to date has addressedthe validity of this assumption. Sanchez-Craigand colleagues found that when comparing the12-month treatment outcomes of men who wereseverely dependent and men who were not,both receiving brief treatment, there were nosignificant differences in "successful" outcomesas measured by rates of abstinence or moderatedrinking (Sanchez-Craig et al., 1991).
Alcohol Treatment OutcomesThe study of treatment outcomes for olderadults who meet criteria for alcohol abuse ordependence has become a critical issue becauseof older adults' unique needs for targetedinterventions. Because traditional residentialalcoholism treatment programs generally
117
provide services to few older adults, sample sizeissues have been a barrier to studying treatmentoutcomes for older alcoholics. The developmentof elder-specific programs in recent years has,however, yielded sufficient data on olderalcoholics to permit more comprehensivestudies of this population (Atkinson, 1995).
Previous research on alcoholism treatment inolder adults can be divided into two broadcategories: compliance studies and outcomesstudies.
Studies of treatment complianceMost treatment outcome research on olderalcoholics has focused on compliance with
treatment program expectations, in particularthe patient's fulfillment of prescribed treatmentactivities and goals, including drinking behavior(Atkinson, 1995). Results from compliancestudies have shown that age-specific
programming improved treatment completionand resulted in higher rates of attendance atgroup meetings than did mixed-age treatment(Kofoed et al., 1987). Studies also show thatolder alcoholics were significantly more likelythan younger patients to complete treatment(Schuckit, 1977; Wiens et al., 1982/1983).
Atkinson and colleagues also found that,proportionately, twice as many older malealcoholics completed treatment than youngermen (Atkinson et al., 1993).
Age of onset of alcohol problems has been amajor focus of research for older adult treatmentcompliance studies. In one study using amatched-pairs, post hoc design, rates ofcompletion of 6-month day treatment for 23older men and women alcoholics (age 55 andolder) whose problem drinking began beforeage 50 (early onset) were compared with 23 whobegan problem drinking after age 50 (late onset)(Schonfeld and Dupree, 1991).
In another study of 132 male alcoholicveterans age 60 and older, the sample was

divided into three subgroups: early onset (age40 and younger, n = 50), midlife onset (age 41 to59, n = 62), and late onset (age 60 and older, n =20) (Atkinson et al., 1990). Age of onset wasrelated to program completion and to weeklygroup therapy meeting attendance, with the lateonset subgroup showing the best compliance inbivariate analyses. However, a subsequentmultivariate analysis of 128 men age 55 andolder in alcoholism treatment found thatdrinking relapses during treatment wereunrelated to age of onset (Atkinson et al., 1993).
Furthermore, age of onset did not predictprogram completion but was related toattendance rate at scheduled visits (Atkinson etal., 1993). The studies on the effect of age ofonset on treatment compliance have thereforeyielded mixed results.
In a study of treatment matching, Rice andcolleagues compared drinking outcomes forrandomly assigned male and female alcoholics 3months after beginning one of three mixed-ageoutpatient cognitivebehavioral treatmentconditions scheduled to last for 4 months (Riceet al., 1993). The sample included 42 individualsage 50 and older, 134 patients age 30 to 49, and53 patients age 18 to 29. There were nosignificant effects of age or treatment conditionon treatment compliance. However, there weresignificant age group-by-treatment conditioneffects. For older patients, the number of daysabstinent was greatest and the number of heavydrinking days fewest among those treated witha focus on self-efficacy rather than a focus onoccupation or family issues.
Major limitations remain in the treatmentcompliance literature, including lack of drinkingoutcome data, failure to report on treatmentdropouts, and variations in definitions oftreatment completion. Few carefully controlledprospective treatment outcome studies, eventhose with sufficiently large numbers of older
Outcomes and Cost Issues
alcoholics, address the methodologicallimitations inherent in compliance studies.
Prospective studies of treatmentoutcomesAlthough it is important to examine the factorsrelated to completion of treatment, studies thusfar have inherent selectivity bias and provide noinformation on treatment dropouts or on short-or long-term outcomes of treatment. Othersampling issues may limit the applicability ofsuch studies to larger groups, such as theexclusion of women in some studies and the useof varying age cutoffs that sometimes placeindividuals as young as 45 in the "older"category.
Problems with previous outcome studiesextend beyond sampling to study methods. Themajority of studies used relatively unstructuredtechniques for assessing drinking patterns andalcohol-related symptoms. Furthermore, theassessment of outcomes has been narrow infocus. Most studies have dichotomizedtreatment outcome (abstention vs. relapse)based solely on drinking behavior. Givenevidence from numerous studies that heavy orbinge drinking is more strongly related toalcohol consequences than average alcoholconsumption (Anda et al., 1988; Chermack et al.,
1996; Kranz ler et al., 1990), there may be
important differences in outcome fornonabstinent individuals depending on whetherbinge drinking was part of the posttreatmentpattern. Current recommendations includecategorizing nonabstinent drinking outcomesalong dimensions, such as whether drinkersever drink to the point of intoxication (Heatherand Tebbutt, 1989). Furthermore, most studieshave not addressed other relevant domains thatmay be positively affected by treatment, such asphysical and mental health status andpsychological distress.
118 97

Chapter 6
One reason for the lack of prospectivetreatment outcome studies is that studying olderalcoholics during and after treatment is socomplex. One exception is a study of 137 maleveterans (age 45 to 59 years, n = 64; age 60 to 69years, n = 62; age 70 years and older, n = 11)with alcohol problems who were randomlyassigned after detoxification to age-specifictreatment or standard mixed-age treatment(Kashner et al., 1992). Outcomes at 6 monthsand 1 year showed that elder-specific programpatients compared with mixed-age grouppatients were 2.9 times more likely at 6 monthsand 2.1 times more likely at 1 year to reportabstinence. The two treatment groups, however,could not be adequately compared at baselinebecause baseline alcohol consumption andalcohol severity data were not included in thestudy.
Recognizing that older individuals have beenunderrepresented in standard alcoholismtreatment programs (Booth et al., 1992; Higuchiand Kono, 1994), as well as in treatmentoutcome studies (Atkinson, 1995), the Instituteof Medicine published a special report callingfor specific longitudinal studies focused onfactors associated with more successfultreatment outcomes in older adults (Institute ofMedicine, 1990).
Blow and colleagues conducted a study todetermine outcomes for older adults receivingspecialized elder-specific inpatient alcoholismtreatment (Blow et al., 1997). A range oftreatment outcomes was assessed using aprospective longitudinal design. To addresslimitations of previous studies, this study usedvalidated techniques to assess baseline alcoholsymptoms and psychiatric comorbidity, age ofonset of alcohol problems, drinking patterns,
98
physical and emotional health functioning, andpsychological distress. Followup wasconducted 6 months after discharge. This studyalso examined a range of different drinkingoutcomes, including abstinence, nonbingedrinking, and binge drinking.
Adults over the age of 55 in the treatmentprogram (n = 90) were interviewed. Thephysical health functioning of the sample wassimilar to that reported by seriously medically illinpatients in other studies, whereaspsychosocial functioning was significantlyworse. Nearly one-third of the sample had oneor more comorbid psychiatric disorders, withanxiety disorders and major depression mostcommon.
Participants who completed the 6-monthfollowup assessment (n = 68; 76 percent of theoriginal sample) were classified into thefollowing outcome groups: abstainers (n = 38),nonbinge drinkers (who never exceeded fourdrinks on any drinking day during the followupperiod; n = 12), binge drinkers (who had one ormore days in which they consumed five or moredrinks; n = 18), and noncompleters (who did notcomplete the 6-month followup assessment; n =22). These groups did not differ significantly ondemographic variables, pretreatment drinkingpatterns and symptoms, age of onset of alcohol
problems, psychiatric comorbidity, or length ofstay in treatment. For all groups who completedthe 6-month followup, there were improvementsin general health. Psychological distressdecreased significantly between baseline andfollowup for abstainers and nonbinge drinkers.However, binge drinkers did not show a declinein psychological distress and were significantlymore distressed at 6-month followup than boththe abstainers and nonbinge drinkers.
119

Measurement ofMultidimensionalOutcomes for OlderAdultsConsumption levels are not the only measure ofsuccess: Drinking patterns, alcohol-relatedproblems, physical and emotional healthfunctioning, and quality of life can also be usedto assess alcohol intervention and treatmentoutcomes with populations of older adults. It isparticularly important to use benchmarkedmethods to assess older adults to determinewhether treatment regimens are effective. Olderadults have unique issues based on changes inphysical functioning, changes in tolerance toalcohol, and internal (e.g., hearing, eyesight) andexternal (e.g., death of spouse, retirement) lossesrequiring a multidimensional approach toassessment and outcome evaluation toameliorate potential reasons for relapse or areturn to hazardous drinking.
Outcome assessment is invaluable from botha management and a referral perspective. Theproviders of treatment, the clinicians andagencies referring patients, and patientsthemselves need to have information regardingthe likely outcomes of treatment. Becausetreatment options range from brief interventionsto structured outpatient and inpatient treatmentprograms, evaluation is recommended atvarying points in the treatment process(McLellan and Durell, 1996). Initial evaluationin any setting should take place at the beginningof the intervention or treatment to obtainbaseline data. McLellan and Durell recommendconducting first followup evaluations 2 weeks to1 month after the patient leaves the inpatientsetting. The short time frame reflects the need todetermine if the patient is engaged in aftercare
with an outpatient program to maximize theeffect of inpatient treatment.
A review of the literature on patientsreceiving substance abuse treatment indicatedthat 60 to 80 percent of people who relapse do sowithin 3 to 4 months (McLellan et al., 1992).Older adults who comply fully with andcomplete the intervention or treatment,however, are more likely than younger adults topositively change their drinking behavior (Finchand Barry, 1992). Therefore, outpatientoutcomes should be assessed no sooner than 3months and possibly as long as 12 months aftertreatment (McLellan and Durell, 1996). For alltypes of intervention and treatment, ongoingoutcome evaluation is important since thecourse of alcohol problems in older adults isdynamic and changes over time withcircumstances. Additional life stressors canchange the pattern of alcohol use in this agegroup.
In response to the rising costs of treatmentand concerns about the effectiveness of alcoholtreatment for both younger and older adults, thedemand to evaluate and demonstrate the qualityof a variety of treatment options has also grown.For the purposes of this section, outcomemeasurement will include methods to measurealcohol use and alcohol-related problems,physical and emotional health functioning, andquality of life and well-being.
Measures of Alcohol UseDrinking patterns can be assessed usingapproximations such as average number ofdrinking days per week and average number ofdrinks per occasion or day. Two of theinstruments assessing average consumption arethe Alcohol Use Disorders Identification Test(AUDIT) (Babor et al., 1992b) and the HealthScreening Survey (HSS) (Fleming and Barry,1991), both of which are reproduced inAppendix B. The AUDIT, which has been
140 99

Chapter 6
validated internationally and with populationsunder age 65 in the United States, assesses
quantity and frequency of alcohol use as well as
alcohol-related problems (Babor et al., 1987;Fleming et al., 1991; Barry and Fleming, 1993;Schmidt et al., 1995).
The HSS, originally developed by Wallaceand Haines and adapted by Fleming and Barry,measures average quantity and frequency ofalcohol use in the previous 3 months (Wallaceand Haines, 1985; Fleming and Barry, 1991) andincludes parallel questions about weight,exercise, and smoking. It has been validated inpeople under 65 in primary care settings in theUnited States (Fleming and Barry, 1991) and hasbeen used with older adults as part of a briefintervention trial (Fleming et al., 1997a).
The most accurate method used to assesscurrent alcohol consumption is the Time LineFollow Back (TLFB) procedure. TLFB is astructured interview that uses calendar cues(e.g., holidays, family events, trips) to quantifydaily alcohol use over a period of time rangingfrom 7 days to a number of months (Sobell et al.,1988, 1996). Researchers have used this methodto obtain up to 1 year of drinking data. Thismethod has shown high test-retest reliability ina variety of drinking populations ranging fromnormal drinkers to heavy drinkers to personsparticipating in inpatient or outpatienttreatment. Fleming and colleagues used thisprocedure to assess 7-day alcohol use withadults age 65 and older as part of the initialassessment in a clinical trial to test theeffectiveness of brief physician advice with olderat-risk and problem drinkers (Fleming et al.,1997a).
Measures of Alcohol ProblemsIt is necessary but not sufficient to determinequantity and frequency of alcohol use for initialand followup assessments in older adults. Theuse of multidimensional screening and outcome
1001
instruments provides clinicians, programs, andreferral agencies with measurements regardingthe nature and severity of problems presentedby persons who abuse alcohol.
An important multidimensional screeninginstrument for use specifically with older adultsis the Michigan Alcoholism Screening TestGeriatric version (MAST-G) (Blow et al., 1992a)(See Figure 4-4). This tool was developedbecause many of the screening measures did notidentify alcoholism among older adults asreliably as among younger populations. TheMAST-G was validated using criteria for alcoholdependence in the Diagnostic and Statistical
Manual of Mental Disorders, Third Edition,
Revised (American Psychiatric Association,1987) as the gold standard on 305 older adultsincluding (1) persons currently meeting alcoholdependence criteria but not in treatment, (2)those currently in treatment, (3) those with a
previous history of alcoholism but in recovery,(4) social drinkers, and (5) abstainers.
The MAST-G is a 24-item scale (sensitivity =
0.94; specificity = 0.78) in which a score of five ormore "yes" responses indicates an alcoholproblem. Scores do not discriminate betweencurrent and past problems, although some itemsaddress the current situation and others addressproblems in the past. Tolerance is not measuredin light of data indicating that older adults witheven low consumption can experience alcohol-related problems due to physiological changesthat occur with age.
The Addiction Severity Index (ASI)(McLellan et al., 1985; McLellan et a1.,1990) was
developed specifically to assess over time thealcohol-related problems and the severity ofsymptoms of patients in treatment for alcoholand drug abuse and dependence. The ASI is asemistructured interview that providesinformation about aspects of the patient's lifethat may contribute to the substance abusesyndrome. The focus of the interview is on

seven functional areas that have been shown tobe affected by substance abuse: medical status,employment and support, drug use, alcohol use,legal status, family and social status, andpsychiatric status. Each area is assessedindividually for past and present (last 30 days)status. Each area has a 10-point interviewer-determined severity rating of lifetime problemsand a multi-item composite score indicatingseverity of the problems in the last 30 days.
The ASI is targeted to all adult populationsin substance abuse treatment or in treatment forco-occurring psychiatric and substance abusedisorders. The ASI has good interraterreliability as well as good predictive, concurrent,and discriminant validity (McLellan et al., 1985).Although it has not been widely used orvalidated with older patients and is notgenerally used with patients who are at-risk orproblem drinkers in primary care orcommunity-based settings, it is included in thisreview because it is a standard measure in thefield and can provide important informationregarding older adults in treatment settings,particularly in areas of greatest concern withthis populationmedical status, alcohol use,family and social status, and psychiatric status.
Measures of Physical and EmotionalHealthOne of the most widely used measures ofphysical and emotional health is the MedicalOutcomes Study 36-Item Short Form HealthSurvey (SF-36). This instrument was originallydeveloped for use with adults as a 20-item scalefor the Medical Outcomes Study (MOS) (Wareand Sherbourne, 1992; Tar lov et al., 1989;
Stewart et al., 1988) from more detailedmeasures used in the Rand Health Experiment.It was subsequently expanded to 36 items thatmeasure physical functioning, limitations infunctioning due to physical health problems,social functioning, bodily pain, general mental
Outcomes and Cost Issues
health, limitations in role functioning due toemotional problems, vitality, and general healthperceptions. The SF-36 has published norms forthese various subscales over distinct age groups,including older adults (McHorney et al., 1993).
In addition to the subscales addressed in theSF-36, other measures of psychological distressare useful in alcohol outcomes assessment witholder adults. The Symptom Checklist -90-Revised (SCL-90-R) (Derogatis, 1994b) is a self-
report symptom inventory designed to measurepsychological distress. The Brief SymptomInventory (BSI) is a brief form of the SCL-90-R
(Derogatis and Melisaratos, 1983). These testsprovide an overview of a patient's symptomsand identify the level of distress that a patient isexperiencing during a specific time period (e.g.,"the last 7 days"). Both the SCL-90-R (90 items)and the BSI (53 items) measure nine symptomdimensions: somatization, obsessive-compulsiveness, interpersonal sensitivity,depression, anxiety, hostility, phobic anxiety,paranoid ideation, and psychoticism. Each ofthe tests also has three global measures ofdistress, a measure of the intensity of distress,and a measure of the total number of patientsymptoms.
Depending on the population being assessed,the internal consistency for the SCL-90-R rangesfrom 0.77 to 0.90; for the BSI, from 0.71 to 0.85.
Test-retest reliability ranges from 0.80 to 0.90 for
the SCL-90-R (with a 1-week interval betweentests) and from 0.61 to 0.91 for the BSI. Whenused for outcome measurement, these measuresare often administered at intake, duringtreatment, at discharge, and at followupintervals (Smith, 1996).
Measures of Quality of LifeQuality of life measures have most frequentlybeen used for outcomes assessment in mentalhealth treatment. One of the most widely usedinstruments is the Quality of Life Interview
101

Chapter 6
(QLI) (Lehman, 1988). Research suggests thatquality of life, as perceived by the patient, is animportant factor in maintaining optimalfunctioning. The quality of life measure isconstructed to include a single-item measure ofgeneral well-being and seven dimensions ofwell-being. The constructs and dimensions inthis scale are applicable to the alcohol treatmentfield, particularly in outcomes assessment witholder adults for whom concerns about housing,leisure, family, social relationships, health,safety, and finances are salient factors infunctioning and relapse.
Internal consistency reliabilities range from0.79 to 0.88 for the life satisfaction scales andfrom 0.44 to 0.82 for the objective quality of lifescales. Normative data are available for varioussubgroups of patient populations, and the lifesatisfaction items can be compared with nationalnorms in the general population.
Costs of Alcohr.1TreatmentOutcomes studies obviously can help treatmentproviders and health care professionals improvetreatment. They also play an important role inpaying for treatment: Third-party payers wantvalidated proof that the treatment approachesthey are reimbursing actually work. The otherside of this equation is the costto individuals,the health care system, and society at largeofalcohol-related problems. If costs of treatmentcan be measured against these larger costs, it ismore likely that treatment will be reimbursed.
The costs of alcohol abuse and dependenceare estimated to be over $100 billion a year, duein part to increased mortality, significant socialcosts, and health consequences (NationalInstitute on Alcohol Abuse and Alcoholism,1995; Brower et al., 1994; Holder and Blose, 1992;Goodman et al., 1991). Individuals who havealcohol disorders are among the highest cost
102
users of medical care in the United States.Persons with alcohol dependence, whorepresent between 3 and 14 percent of the U.S.population, consume more than 15 percent ofthe national health care budget (Rice et al.,1993). Although a number of cost studies haveexamined drinking in younger adults (Holder etal., 1991; Holder and Blose, 1992; Finney and
Monahan, 1996), few studies have separated thecosts of alcohol disorders for older adults oreven included older adults in cost analyses. In astudy of Federal employees, one half of whomwere over age 60, Holder and Blose analyzed 4years of claims data (Holder and Blose, 1986).They found that alcohol treatment contributedto sustained reductions in total health careutilization and costs and that reductions inposttreatment costs appeared to be sustainedinto the fourth and fifth years followingtreatment.
In a review of studies of alcohol treatmentand potential health care cost savings thatincluded Medicare studies, Holder found thatmean monthly medical care costs increased forpersons with alcohol problems before initiationof treatment, declined immediately followingtreatment, and continued to decline 2 yearsfollowing treatment (Holder, 1987). The oldestgroup in the study (age 65 and older)experienced the highest medical care costs andshowed the least convergence to levels prior tothe initiation of alcohol treatment. Reasons forthis might include increased general morbiditywith age and the potentially more serious healthproblems due to a longer period of chronicalcohol abuse or dependence.
Among all of the economic analyses ofalcohol programs, there has been little workregarding the cost savings of substance abuseprevention and early intervention in managedcare settings. One of the few recent studies ofmanaged care (Holder et al., 1995) estimatedthat for every $10,000 spent on brief intervention

for alcohol or drug abuse, $13,500 to $25,000 is
saved in medical spending for the managed careprovider. Gaps remain in the literatureregarding the economic effectiveness andimplications of brief interventions in managedcare settings. Filling in the gaps is particularlyimportant because managed care providers arechallenged to provide needed services withfewer dollars.
Findings on the efficacy and cost-effectiveness of brief intervention, however, canbe misleading (Heather, 1995; Pee le, 1990).
These reviews generally do not assess costs andneeds of older adults in these settings.Methodologies across cost analysis studies havenot been consistent, making comparisons moredifficult. In addition, Heather points outproblems in interpreting the data from briefintervention studies because brief interventionsare not a homogeneous entity (they vary inlength, structure, targets of intervention, andpersonnel responsible for delivery), and there isa distinction between treatment seekers (e.g.,persons who answer ads indicating that theywould like to decrease their drinking) andnontreatment seekers (e.g., individuals withregularly scheduled appointments for medicalproblems who receive interventions from theirhealth care providers) (Heather, 1995). Cleardelineation of the type of study and thepotential audience for the research can help toalleviate problems of misinterpretation.
Most economic studies of alcohol treatmenthave focused on hospital inpatient andoutpatient treatment for abuse and dependence(Pee le, 1990; Annis, 1986). Pee le's review of the
literature revealed that, although hospitaltreatment is no more effective than outpatienttreatment, reimbursement systems have oftensupported the more costly, medically basedinpatient treatment options (Pee le, 1990).
Some experts suggest that effectively treatingalcoholism and reducing the social and medical
Outcomes and Cost Issues
consequences of alcohol disorders will yield thelargest savings in a reformed American healthcare system (McCrady and Langenbucher, 1996).
Reimbursement Issues inThe Treatment of OlderAdultsThe barriers to care experienced by manyindividuals who need intervention or treatmentfor problems related to their alcohol use havebeen of great concern to the alcohol treatmentfield. A further concern has been theobservation that only a small minority of thosewho need treatment has received it (Institute ofMedicine, 1990). It has not always been clear ifthis is due to the lack of identification andreferral of those who need treatment, the lack oftreatment options, or financial barriers to care.All of these barriers may affect older adults.Currently, however, the financial barriers arechanging the fastestand some of the shifts inreimbursement are alarming.
Private third-party insurers are fundedthrough premiums paid by purchasers, withpremiums adjusted based on claims made byany subscriber group. Generally, except for self-insured plans, coverage minimums andpremiums are regulated by States through theirinsurance departments. Medicare is generallythought of as a public third-party payer forhealth care services. The benefits provided areauthorized through legislation.
The current trend, however, is for States toturn their Medicare programs over to managedcare companies. Although, since its inception in1965, Medicare has generally covered 12 days ofinpatient alcohol treatment, most managed carecompanies eliminate coverage for as muchinpatient treatment as possible and often cutservices for alcohol treatment altogether to keepcosts down.
124 103

Chapter 6
These cuts in coverage are antithetical to allthat is known about treating older adults withalcohol problems. Coverage of 12 days ofinpatient treatment is extremely important forolder adults because they are likely to have agreater number of physical and cognitiveproblems than younger adults. For example,older adults often have more prolonged andsevere alcohol withdrawal than younger adults(Brower et al., 1994), and participation in grouptreatment is more difficult for them in the earlystages of treatment. They are also more likely toneed more intensive outpatient care after aninpatient stay than younger adults.
Furthermore, Medicare should reimburse foralcohol prevention and early intervention effortsin primary care settings, because researchindicates that early intervention programs areeffective with a large proportion of older at-riskand problem drinkers. Such initiatives will savethe medical community money by preventingmore costly complications of heavier alcoholintake.
With ongoing changes in the delivery ofalcohol treatment services from inpatient tooutpatient settings coupled with the shiftingreimbursement structure from fee-for-serviceMedicare to managed Medicare, coverage ofeffective treatment is increasingly uncertain.The changes in treatment venue and feestructures underscore the importance ofconducting multidimensional outcomesassessments in the context of qualitymanagement. Convincing research is animportant component of efforts to ensure thatolder adults who need intervention andtreatment for alcohol problems receive theappropriate level of treatment and adequatefollowup. Ongoing evaluation of patientoutcomes can help safeguard the health of at-risk older adults and foster the development ofinnovative treatment approaches to meet theneeds of this vulnerable population.
104
125
Areas Requiring FutureResearchAs the number of older adults rises, the use ofmood-altering drugs such as alcohol andtranquilizers by older adults is a growing area ofconcern from a clinical and research perspective.As the Baby Boom generation reaches traditional
retirement age, the field of substance abusetreatment and research will be faced with bothgrowing numbers of individuals who havealcohol-related problems and emergingproblems unique to the aging population,namely a potential increased prevalence of illicitdrug use and drug-related problems.
Even though the prevalence of alcohol anddrug use decreases with age, alcohol andprescription drug use continue to be importanthealth problems in the current cohort of olderadults. To advance the field and addresscoming needs of future older adults, researchneeds to be focused in some specific areas. Thegeneral areas for new research initiatives are (1)alcohol and other drug consumption, (2)treatment, (3) biomedical consequences, (4)behavioral and psychological effects, and (5)special issues.
In the area of alcohol and other drug
consumption, future research directions shouldinclude
Life course variations among alcohol, illicitdrug, and prescription drug use patternsGender and ethnic variabilityReasons for changes in drinking and druguse patterns with agingEarly and late onset of alcohol and drugproblemsHealth care costs for older adultsmaintaining abstinence compared with costsfor those who reduce their consumptionDevelopment of valid screening instrumentsfor illicit and prescription drug use.

Issues related to treatment have traditionallybeen studied in males and younger cohorts ofadults. Some of the issues requiring both newand renewed study with older adults include
Prevention and early intervention techniquesThe use of technology (e.g., computers,interactive voice recognition) in thetreatment of substance abuse problems inolder adultsThe effectiveness of various older adult-specific alcohol and drug treatmentmodalitiesAlcohol and drug withdrawal issuesThe effect of physical and psychiatriccomorbidity on treatment outcomesOlder subgroups (i.e., 60-65, 65- 70, 70-75,75-80, 80+)
Relationship of provider characteristics (e.g.,age, similarity to client) to completion oftreatmentRisk factors for drinking and drug userelapse, including a better understanding ofspecific treatment needs for older adults.
Biomedical research can forge a new andimportant path in the understanding of alcoholuse and abuse in older adults. Directionsinclude
The effects of alcohol and drugs on agingorganismsAlcohol and drug medication interactionsPhysiological reasons for increasedsensitivity to alcohol as people ageMedical consequences of moderate andheavy drinking and illicit drug useInteractions of alcohol, nicotine, and illicitdrugs.
Outcomes and Cost Issues
Behavioral and psychological research
initiatives may be focused in the followingdirections:
Demographics relating to older adult alcoholand drug use and abuse (relationshipbetween drinking and drug use status andemployment, marital status, residence,education, and other variables specificallyaffecting older adults)Older adults' reasons for changing theirdrinking patternsStress, coping, and adaptation, and theirrelationship to alcohol and drug useCognitive effects of moderate and heavydrinking and drug use in this age group.
Finally, there are some special issues related toolder adult substance abuse that have been thetarget of clinical concern and some initialresearch, which needs to be expanded in orderto address the needs of the current and futurecohorts of older adults:
Elder abuse and neglectHomelessness
Underrepresentation of older adults intreatment settings.
Researchers in gerontology, substance abusetreatment, and related fields must take the leadin providing the above information. Only withsuch knowledge can clinicians and policymakersimprove the identification and treatment ofsubstance use disorders among older adults.Without the informationand the responsesuch disorders will take a greater and greatertoll on one of the most vulnerable and fastestgrowing sectors of the population.
12G

Appe ix ALegal and Ethical Issues
by Margaret K. Brooks, Esq.1
Screening any population for substanceabuse raises key legal and ethicalconcerns: how one can inquire about an
individual's alcohol and drug use whilecontinuing to respect that person's autonomyand privacy. Screening of older adults forsubstance abuse brings these concerns intoparticularly sharp focuswhether the personscreening is a clinician, a staff member at asenior center, a member of the clergy, an adultprotective service worker, a Meals-On-Wheelsvolunteer, a pharmacist, a community healthworker, an adult day care worker, or staffmember at a long-term care facility.
This appendix examines how the issues ofautonomy and privacy (or confidentiality) affectthe way providers working with older adultsmay screen for substance use problems. Thefirst section discusses the relationship betweenpatient or client autonomy and the provider'sobligation to inform and counsel the olderindividual about the health risks of alcohol orother drug use. The second section concernsprivacy of information about substance use
problems: How can a provider keep accuraterecords and communicate with others concernedabout the older individual's welfare withoutdisclosing information that may subject theindividual to scorn or create problems withfamily or third-party payers?
Autonomy and theProvider's Mission: ADilemmaAmericans attach extraordinary importance tobeing left alone. We pride ourselves on havingperfected a social and political system that limitshow far the governmentand otherscancontrol what we do. The principle of autonomyis enshrined in our Constitution, and our courtshave repeatedly confirmed our right to makeour own decisions for ourselves.
Most of us cherish our autonomy and fear itsloss, particularly as we age. Although providerswho screen or assess for substance abuse do sobecause they are genuinely concerned about anindividual's health or functioning, screening
I Margaret K. Brooks is an independent consultant in Montclair, New Jersey.
12 107

Appendix A
means seeking very personal informationanunavoidable intrusion on a person's autonomyand privacy. Alert to suggestions that theirjudgment or abilities are impaired, older adultsmay not always see a provider's effort to "help"as benign.
Performed insensitively, screening orassessment may intensify denial. A person ofany age who is "in denial" may not realize, orwant to realize, that he has to cut back on orgive up his intake of alcohol or prescriptionmedications; an older person may view theprovider's questions and suggestions asintrusive, threatening, and offensive.Suggestions that an older individual's complainthas an emotional basis may tap an underlyingreluctance to acknowledge an emotionalcomponent to any problem and reinforce theindividual's resistance. Because the substanceabuse label carries a powerful stigma, an olderindividual may become alarmed if a providerintimates that alcohol or drug abuse may beinvolved. It will be tempting for the olderindividual to point to the "normal" infirmities ofold age as the source of his difficulty rather thanacknowledge a problem with alcohol or otherdrugs.
How can the provider raise the question ofalcohol and drug use constructively, withouteliciting a defensive response? Should she raisethe issue and then drop it at the slightest hint ofresistance on the part of the older individual?Or should she intervene more forcefullywithargument or by involving the family?
To fulfill her ethical responsibility, theprovider should do more than simply raise theissue. As the Consensus Panel suggests, mostolder adults are unaware that their metabolismof alcohol and prescription drugs changes asthey age and that lower amounts of alcohol andmedicines may incapacitate them. Respect for aperson's autonomy means informing him of allrelevant medical facts and engaging him in a
108
1 2. 8
discussion about his alternatives. If there is asubstance abuse problem, the provider cansupply the information and encouragement, butonly the person with the problem has the powerto change what he is doing. Respecting thepatient's autonomyhis right to make choicesis central to encouraging that change.
Privacy andConfidentialityAside from perceived threats to autonomy, anolder person may also be concerned about thepractical consequences of admitting a substanceuse problem. Such patients may find it difficultor impossible to obtain coverage forhospitalization costs if an insurer or healthmaintenance organization (HMO) learns thattheir traumatic injuries were related toalcoholism. Relationships with a spouse,children, grandchildren, or friends may suffer.Adverse consequences such as these maydiscourage patients with substance useproblems from seeking treatment.
Concern about privacy and confidentiality isfueled by the widespread perception that peoplewith substance use disorders are weak and/ormorally impaired. For an older person, thisconcern may well be compounded by anapprehension that others may viewacknowledgment of a substance use disorder asa sign of inability to continue livingindependently. If the individual is havingfamily problemswith a spouse or withchildreninformation about substance usecould have an adverse impact on resolution ofthose problems. Or the individual mayexperience difficulties with health insurance.
Federal LawThe concern about the adverse effects that socialstigma and discrimination have on patients inrecovery (and how those adverse effects might

deter people from entering treatment) led theCongress to pass legislation and the U.S.Department of Health and Human Services toissue a set of regulations to protect informationabout individuals' substance abuse. The law iscodified at 42 U.S.C.§ 290dd-2. Theimplementing Federal regulations,"Confidentiality of Alcohol and Drug AbusePatient Records," are contained in 42 CFR Part 2(Vol. 42 of the Code of Federal Regulations, Part2).
The Federal law and regulations severelyrestrict communications about identifiableindividuals by "programs" providing substanceuse diagnosis, treatment, or referral fortreatment (42 CFR§ 2.11). The purpose of thelaw and regulations is to decrease the risk thatinformation about individuals in recovery willbe disseminated and that they will be subjectedto discrimination and to encourage people toseek treatment for substance use disorders.
In most settings where older adults receivecare or services, Federal confidentiality laws andregulations do not apply.' Providers should beaware, however, that if a health care practice orsocial service organization includes someonewhose primary function is to provide substanceabuse assessment or treatment and if thepractice or organization benefits from "Federalassistance,"2 that practice or organization mustcomply with the Federal law and regulationsand implement special rules for handlinginformation about patients who may havesubstance abuse problems.3
Moreover, the fact that most providers forolder adults are not subject to the Federal rulesdoes not mean that they can handle informationabout their clients' substance use problems in acavalier manner. Because of the potential fordamage, providers should always handle suchinformation with great care.
Legal and Ethical Issues
State LawAlthough Federal rules do not restrict how mostproviders gather and handle information aboutan older individual's substance abuse, there areother rules that may limit how such informationmay be handled. State laws offer someprotection to medical and mental healthinformation about patients and clients. Mostdoctors, social service workers, and clients thinkof these laws as the "doctor-patient privilege" or"social worker-client privilege" or"psychotherapist-patient privilege."
Strictly speaking, these privileges are rules ofevidence that govern whether a professionalprovider can be asked or compelled to testify ina court case about a patient or client. In manyStates, however, laws offer wider protection.Some States have special confidentiality lawsthat explicitly prohibit physicians, socialworkers, psychologists, and others fromdivulging information about patients or clientswithout consent. States often include suchprohibitions in professional licensing laws; suchlaws generally prohibit licensed professionalsfrom divulging information about patients orclients, and they make unauthorized disclosuresgrounds for disciplinary action, includinglicense revocation.
Each State has its own set of rules, whichmeans that the scope of protection offered byState law varies widely. Whether acommunication is "privileged" or "protected"may depend on a number of factors:
The type of professional provider holding theinformation and whether he or she islicensed or certified by the StateThe context in which the information wascommunicatedThe context in which the information will beor was disclosedExceptions to any general rule protectinginformation, and
12:9109

Appendix A
ei How the protection is enforced.
Professionals covered by the"doctor-patient" or "therapist-client" privilegeWhich professions and which practitionerswithin each profession are covered depends onthe State where the professional practices.California, which grants its citizens "aninalienable right to privacy" in its Constitution,has what may be the most extensive protectionsfor medical (including mental health)information. California law protectscommunications with a wide variety ofprofessionals, including licensed physicians,nurses, and psychotherapists (which includesclinical social workers, psychologists, marriageand family counselors), as well as manycommunications with trainees practicing underthe supervision of a number of theseprofessionals. A California court has held thatinformation given to an unlicensed professionalby an uneducated patient may be privileged ifthe patient reasonably believes the professionalis authorized to practice medicine.'
Other States' laws cover fewer kinds ofprofessionals. In Missouri, for example,protection is limited to communications withState-licensed psychologists, clinical socialworkers, professional counselors, andphysicians.
Depending on their professional training(and licensing), primary care physicians,physician assistants, nurse-practitioners, nurses,psychologists, social workers, and others may becovered by State prohibitions on divulginginformation about patients or clients. Note thateven within a single State, the kind of protectionafforded information may vary from professionto profession. Professional providers shouldlearn whether any confidentiality law in theState where they practice applies to theirprofession.
1 o110
The context in which the informationwas communicatedState laws vary tremendously in this area, too.Some States protect only the information that apatient or client communicates to a professionalin private, in the course of the medical or mentalhealth consultation. Information disclosed to aclinician in the presence of a third party (like aspouse) is not protected. Other States, such asCalifornia, protect all information the patient orclient tells the professional or the professionalgains during examination.5 California alsoprotects other information acquired by theprofessional about the patient's mental orphysical condition, as well as the advice theprofessional gives the patient.' When Californiacourts are called upon to decide whether aparticular communication of information isprivileged, State law requires them to presumethat it is.
California affords great protection tocommunications between patients andpsychotherapists, a term that covers a widerange of professions. Not only arecommunications by and to the patient protected,information communicated by a patient'sintimate family members to therapists andpsychiatric personnel7 is also protected.California also protects information the patientdiscloses in the presence of a third party or in agroup setting.
Understanding what medical information isprotected requires professional providers toknow whether State law recognizes theconfidentiality of information in the manycontexts in which the professional acquires it.
Circumstances in which"confidential" information isprotected from disclosureSome States protect medical or mental healthinformation only when that information issought in a court proceeding. If a professional

divulges information about a patient or client inany other setting, the law in those States will notrecognize that there has been a violation of theindividual's right to privacy. Other Statesprotect information in many different contextsand may discipline professionals who violatetheir patients' privacy, allow patients to suethem for damages, or criminalize behavior thatviolates patients' privacy. The diversity of Staterules in this area compounds the difficultyprofessionals face in becoming knowledgeableabout what rules apply to them.
Exceptions to State laws protectingmedical and mental healthinformation
ConsentAll States permit health, mental health, andsocial service professionals to disclose
information if the patient or client consents.However, each State has different requirementsregarding consent. In some States, consent canbe oral; in others, it must be written. States thatrequire written consent sometimes require thatcertain elements be included in the consent formor that everyone use a State-mandated form.Some States have different consent forms withdifferent requirements for particular diseases.
Other exceptionsConsent is not the only exception. All Statesalso require the reporting of certain infectiousdiseases to public health authorities and somerequire the reporting of elder abuse to protectiveservice agencies, although definitions of"infectious disease" and "elder abuse" vary.And most States require health careprofessionals and mental health counselors toreport to the authorities threats patients make toinflict harm on others. There are States thatpermit or require health care professionals toshare information about patients with otherhealth care professionals without the patients'
Legal and Ethical Issues
consent, but some limit the range of disclosurefor certain diseases, like HIV. Most States makesome provision for communicating informationto health insurance or managed care companies.
Many of the situations that physicians andsocial service workers face dailyprocessinghealth claims or public benefit applications, forexampleare covered by one of theseexceptions. To fully understand the "rules"regarding privacy of medical and mental healthinformation, professionals must also knowabout the exceptions to those rules. Thoseexceptions are generally in the statute booksineither the sections on evidence or theprofessional licensing sections, or both. Thestate licensing authority as well as professionalassociations can usually help answer questionsabout State rules and the exceptions to thoserules.
Enforcing confidentiality protections
The role of the courtsTo determine the "law"that is, the rule onemust followin any particular area, an attorneywill search for statutes, regulations,administrative rulings, and court decisions.There is no question that in this country, thecourts play a large role in "making" lawparticularly in an area like privacy, whichinvolves human behavior, shades of meaning,and intent. No legislator drafting a statute (orbureaucrat drafting a regulation) can foresee allthe circumstances under which it may beapplied. When one party sues another, a courtis forced to decide whether a provider'sdisclosure of medical information wasappropriate or whether such information shouldbe disclosed during the lawsuit itself.
For example, after a car crash, the driversmay sue each other and ask the court to orderthe disclosure of medical records. Or the victimof an assault by an adolescent may sue theparents and seek disclosure of medical records
131 111

Appendix A
to prove they knew their child was dangerous.How a court decides whether to order disclosurein such cases will depend on a variety of factors,including State law and regulation, court rules,and the relevance of the information sought tothe dispute at hand. Similarly, when a patientor client sues a professional for releasing
information to someone without her consent, thecourt will be called upon to weigh a variety offactors to decide whether the disclosure violatedwhat the State recognizes as the patient'sprivacy.
Over time, court decisions like these addflesh to the bare statutory and regulatory rulesand suggest how those rules will be applied thenext time. When a difficult case arises that doesnot fit neatly within the rule of law asunderstood, it may be helpful to consult with anattorney familiar with the rules and how theState's courts are likely to interpret them.
Penalties for violationsStates differ in the ways they disciplineprofessionals for violations of patients' orclients' privacy. In some States, violation ofconfidentiality is a misdemeanor, punishable bya fine or short jail term. In many States, theprofessional licensing agency has the power tobring disciplinary charges against a professionalwho violates a client's privacy. Such chargesmay result in censure or license suspension orrevocation. Finally, the State may permit theaggrieved patient or client to sue theprofessional for damages caused by theviolation of his right to confidentiality.
The reality is, these enforcement mechanismsare rarely used. States rarely prosecute privacyviolation offenses and professional disciplinarycommittees in most States are more concernedwith other kinds of professional infractions.That is not to say that violation of a patient'sprivacy is cost-free. A patient or client whothinks he has been hurt by a professional's
112 13..9
indiscretion is free to sue; while such cases aredifficult for clients to win, they can cause theprofessional and the organization employing hera good deal of grieffinancial, emotional, andprofessional. Even short of litigation, noprofessional wants to acquire the reputation ofbeing thoughtless or indiscreet.
Strategies for Dealing WithCommon Situations
Charting substance use informationOne way for a professional to safeguard clients'privacy and avoid breaking the rules is todevelop a charting, or record-keeping, systemthat is accurate but still protects clients' rights toprivacy and confidentiality. It is important toremember how many people could see a client'smedical, mental health, or social service record.A medical chart, for example, will be seen by themedical office staff, the insurance company (orHMO or managed care organization [MCO]),and in the event of a referral, another set ofclinicians, nurses, clerical workers, and insurers.If the patient is involved in litigation and hismedical or mental health is in issue, the courtwill most likely order disclosure of his chart orfile in response to a subpoena.
When a provider documents the results ofsubstance abuse screening or assessment or flagsan issue to be raised the next time he sees theclient, he should use neutral notations orreminders that do not identify the problem asbeing substance-use-related. Following arethree record-keeping systems that comply withthe stringent Federal confidentiality regulations,protect clients' autonomy and privacy, and canbe used in a wide variety of settings (TIP 16,Alcohol- and Other-Drug Screening of Hospitalized
Trauma Patients, CSAT, 1995):
gi The "minimalist" approach, which relies onthe provider to enter only that information in

the chart that is required for accuracy and touse neutral terms wherever possible.The "rubber band" approach, whichsegregates substance abuse information in aseparate "confidential" section in the chart.Information in this section would be sharedwith other providers only on a need-to-knowbasis, without being open to the view ofevery staff person who picked up the chart.
o The "separate location" approach, whichkeeps sensitive information separate fromthe rest of the client's chart. The other placemight be a locked cabinet or other similarlysecure area. A "gatekeeper" familiar withthe provider's record-keeping system and thereasons for the extra security would beresponsible for deciding when otherswithin or outside the officewill have accessto this information. This approach provides,in effect, a stronger "rubber band" than thatdescribed in the second approach.8
The push toward computerization of medicalrecords will complicate the problem of keepingsensitive information in medical records private.Currently, there is protection afforded by thecumbersome and inefficient way many, if notmost, medical, mental health, and social servicerecords make their way from one provider toanother. When records are stored in computers,retrieval can be far more efficient.Computerized records may allow anyone with adisc and access to the computer in which theinformation is stored to instantly copy and carryaway vast amounts of information withoutanyone's knowledge. Modems that allowcommunication about patients among differentcomponents of a managed care network extendthe possibility of unauthorized access to anyonewith a modem, the password(s), and thenecessary software. The ease with whichcomputerized information can be accessed canlead to "casual gossip" about a client,
Legal and Ethical Issues
particularly one of importance in a community,making privacy difficult to preserve.
Communicating with othersOne of the trickiest issues is whether and howproviders of older adults health care shouldcommunicate with others about their clients'substance use problems. Communications withothers concerned about the client may confirmthe provider's judgment that the client has asubstance use problem or may be useful inpersuading a reluctant client that treatment isnecessary.
Before a provider attempts to gatherinformation from other sources or enlist help fora patient or client struggling with recovery, heshould ask the older client's permission to do so.Speaking with relatives (including children),doctors, or other health and mental healthprofessionals not only intrudes on the client'sautonomy, it also poses a risk to her right toprivacy. Gathering information (or respondingto questions about a client's problems) from aspouse, child, or other provider can involve anexplicit or implicit disclosure that the providerbelieves the client or patient has a substance useproblem. And the provider making such adisclosure may be inadvertently stepping on aland mine.
Making inquiries or answering questionsbehind the client's back may seriouslyjeopardize the trust that has developed betweenthe provider and the client and undermine hisattempt to offer help. The professional whotalks to the client's son and then confronts herwith their joint conclusions runs the risk that hewill damage his relationship with the client.Feeling she can no longer trust the provider andangry that he has shown little respect for herautonomy or privacy, the client may refuse toparticipate in any further discussions about herproblems.
13 O;)

Appendix A
Dealing with questions of incapacityMost older clients or patients are fully capable ofcomprehending the information and weighingthe alternatives offered by a provider andmaking and articulating decisions. A smallpercentage of older patients or clients are clearlyincapable of participating in a decision-makingprocess. In such cases, the older person mayhave signed a health care proxy or may have acourt-appointed guardian to make decisions inhis stead.
The real difficulty arises when a provider isscreening or assessing an older person whosemental capacity lies between those twoextremes. The client or patient may havefluctuating capacity, with "good days" and "baddays" or periods of greater or lesser alertnessdepending upon the time of day. His conditionmay be transient or deteriorating. Hisdiminished capacity may affect some parts of hisability to comprehend information but notothers.
How can the provider determine whether thepatient or client understands the informationshe is presenting, appreciates the implication ofeach alternative, and is able to make a "rational"decision, based on his own best interests? Thereis no easy answer to this question. One can,however, suggest several approaches.
Maximizing autonomy. The provider can helpthe patient or client who appears to havediminished capacity through a gradualinformation-gathering and decisionmakingprocess. Information the client needs should bepresented in a way that allows the patient orclient to absorb it gradually. The providershould clarify and restate information asnecessary and may find it helpful to summarizethe issues already covered at regular intervals.Each alternative and its possible consequencesshould be laid out and examined separately.Finally, the provider can help the client identifyhis values and link those values to the
114 134
alternatives presented. By helping the patient orclient narrow his focus and proceed step-by-step, the provider may be able to assure herselfthat the client, despite his diminished capacity,has understood the decision to be made andacted in his own best interest.
Enlisting the help of a health or mental health
professional. If working with the patient or clientin a process of gradual information-gatheringand decision-making is not making headway,the provider can suggest that together theyconsult a health or mental health professional.Perhaps there is someone who has known thepatient or client for a number of years who has agrasp of the client's history and betterunderstanding of the obstacles to decision-making. Or, the provider may suggest aspecialist who can help determine why thepatient is having difficulty and whether he hasthe capacity to make this kind of decision.
Enlisting the help of family or close friends.
Another approach is for the provider to suggestto the patient or client that they call in a familymember or close friend who can help themorganize the information and sort through thealternatives. Asking the client who he thinkswould be helpful may win his endorsement ofthis approach.
When the client cannot grasp the information or
come to a decision. If the provider's efforts to
inform the patient or client and help him reach adecision are unsuccessful, she might seek hispermission to consult a family member or closefriend to discuss the problem. If the clientconsents, the provider should lay out herconcerns for the family member or friend. Itmay be that the client has already planned forthe possibility of his incapacity and has signed adurable power of attorney or a health careproxy.
Guardianship. A guardian9 is a personappointed by a court to manage some or allaspects of another person's life. Anyone seeking

appointment of a guardian must show the court(1) that an individual is disabled in some way bydisease, illness, or senility, and (2) that thedisability prevents him from performing thetasks necessary to manage an area or areas of hislife.
Each state handles guardianship proceedingsdifferently, but some principles apply across theboard: Guardianship is not an all-or-nothingstate. Courts generally require that the personseeking appointment of a guardian prove theindividual's incapacity in a variety of tasks orareas. Courts may apply different standards todifferent life tasksmanaging money,managing a household, making health caredecisions, entering contracts. A person may befound incompetent to make contracts andmanage money but not to make his own healthcare decisions (or vice versa), and theguardianship will be limited accordingly.
Guardianship diminishes the older adult'sautonomy and is an expensive process. Itshould, therefore, be considered only as a lastresort.
Making referrals to substance abusetreatment programsThe provider has persuaded the patient or clientto try outpatient treatment and knows thedirector of an excellent program in theimmediate area. Rather than simply picking upthe phone and letting the director know she hasreferred the patient, she should consult thepatient about the specific treatment facility.Though it may seem that consent to treatment isthe same as consent to referral to a particularfacility, it takes very little time to get thepatient's consent, demonstrates respect for theclient or patient, and protects the provider if,say, the treatment program's director is arelative or has some other connection to theclient.
Legal and Ethical Issues
Communications with insurers,HMOs, and other third-party payersThe structure of health, mental health, andancillary social service care for older adults ischanging rapidly. Of course, older adults arecovered by Medicare, but many havesupplementary insurance or have joined HMOsor are entitled to government-sponsored socialservices because of particular medical, physical,or mental disabilities. How should theprofessional provider communicate with thesedifferent types of entities?
Traditional health insurance programsoffering reimbursement to patients for healthcare expenditures typically require patients tosign claim forms containing languageconsenting to the release of information abouttheir care. The patient's signature authorizes thepractitioner to release such information.Although HMOs do not require patients tosubmit claim forms, both practitioners andpatients understand that the HMO or MCO canreview clinical records at any time and may wellreview records if it has questions about thepatient's or client's care.
Should the provider rely on the patient'ssigned consent on the health insurance form orthe HMO contract and release what she has inher chart (or a neutral version of thatinformation)? Or should she consult thepatient?
The better practice is for the provider tofrankly discuss with the patient whatinformation she intends to disclose, thealternatives open to the client (disclosure andrefusal to disclose), and the likely consequencesof those alternatives. Will the information theprovider sends explicitly or implicitly reveal thenature of the patient's problem? Does theclient's chart contain a substance abusediagnosis? Once again, the provider confrontsthe question of how such information should berecorded. Has she balanced the need for
135 115

Appendix A
accuracy with discretion and a respect forpatients' privacy? Finally, even if the chart orfile contains explicit information about theclient's substance use problem, can the providercharacterize the information and her diagnosisin more neutral terms when releasinginformation to the third-party payer?
Once the client understands what kind andamount of information the provider intends tosend a third-party payer, he can decide whetherto agree to the disclosure. The provider shouldexplain that if she refuses to comply with thethird-party payer's request for information, it islikely that at least some related services will notbe covered. If the client expresses concern, sheshould not mislead him, but confirm that once athird-party payer learns he has had a substanceuse problem, he could and may lose either someof his insurance coverage or parts of otherentitlements and be unable to obtain othercoverage. 10
The final decision should be the client's. Hemay well decide to pay out of pocket. Or hemay agree to the limited disclosure and ask theprovider to inform him if more information isrequested.
As managed care becomes more prevalentthroughout the country, medical and mentalhealth providers are finding that third-partypayers demand more and more informationabout patients and about the treatment providedto those patients in order to monitor care andcontain costs. Providers need to be sensitiveabout the amount and kind of information theydisclose because there is a risk that thisinformation may be used to deny future benefitsto the client. Chart notes may also containdetailed and very personal information aboutfamily life that may be unnecessary for a third-party payer to review in order to determinewhether and what kind of treatment should becovered.
116130
As in so many other areas involving patients'privacy, it is best to follow two simple rules:First, keep notations and documentation asneutral as possible while maintainingprofessionally acceptable standards of accuracy.Second, consult the client and let the clientdecide whether to agree to the disclosure.
Communicating with the legalsystemIf a doctor, psychologist, social worker, or otherprovider gets a call from a lawyer asking about apatient or client, or a visit from a lawenforcement officer asking to see records, or asubpoena to testify or produce medical records,what should he or she do? As in other matters ofprivacy and confidentiality, (1) consult thepatient, (2) use common sense, and (3) as a lastresort, consult State law (or a lawyer familiarwith State law).
Responding to lawyers' inquiries. Say a lawyercalls and asks about Emma Bailey's medical,mental health, or social service history ortreatment. As a first approach to the question,the provider could tell the lawyer, "I don't knowthat I have a client with that name. I'd have tocheck my records "" or tell the caller that hemust consult with his client before having aconversation about her: "I'm sure youunderstand that I am professionally obligated tospeak with Emma Bailey before I speak withyou." It will be hard for any lawyer to disagreewith this statement.
The provider should then ask the client if sheknows what information the caller is seekingand whether the client wants him to disclosethat or any other information. He should leavethe conversation with a clear understanding ofthe client's instructionswhether he shoulddisclose the information, and if so, how muchand what kind. It may be that the lawyer isrepresenting the client in a case and the clientwants the provider to share all the information

he has. On the other hand, the lawyer mayrepresent someone with whom the client has adispute. There is nothing wrong with refusingto answer a lawyer's questions.12
If the lawyer represents the client and theclient asks the provider to share all information,the provider can speak freely with the lawyer.However, if the provider is answering thequestions of a lawyer who does not represent theclient (but the client has consented to thedisclosure of some information), the providershould listen carefully to each question, choosehis words with care, limit each answer to thequestion asked, and take care not to volunteerinformation not called for.
Visits by law enforcement. A police officer,
detective, or probation officer who asks aprovider to disclose medical, mental health, orsocial service information about a client or aclient's case records can usually be handled in asimilar manner:13 The provider can safely tell theofficer, as he might a lawyer, "I'm sure youunderstand that I am professionally obligated tospeak with my patient before I speak to you.""
The provider should then speak with theclient to find out whether she knows the subjectof the officer's inquiry, whether she wants theprovider to disclose information and if so, howmuch and what kind. The caretaker might endthe conversation by asking whether there areany particular areas the client would prefer henot discuss with the officer.
When a law enforcement officer comesarmed with a search warrant, the answer isdifferent. In this case, the provider has nochoice but to hand over the records listed in thewarrant.
Responding to subpoenas. Subpoenas come intwo varieties. One is an order requiring aperson to testify, either at a deposition out ofcourt or at a trial. The otherknown as a
Legal and Ethical Issues
subpoena duces tecumrequires a person toappear with the records listed in the subpoena.Depending on the State, a subpoena can besigned by a lawyer or a judge. Unfortunately, itcannot be ignored.
In this instance, the provider's first stepshould be to call Emma Baileythe client aboutwhom he is asked to testify or whose records aresoughtand ask what the subpoena is about. Itmay be that the subpoena has been issued by oron behalf of Emma's lawyer, with Emma'sconsent. However, it is equally possible that thesubpoena has been issued by or on behalf of thelawyer for an adverse party. If that is the case,the provider's best option is to consult withEmma's lawyer to find out whether the lawyerwill objectask the court to "quash" thesubpoenaor whether the provider shouldsimply get the client's consent to testify or turnover her records!' An objection can be based ona number of grounds and can be raised by anyparty as well as by the person whose medicalinformation is sought. If the provider is coveredby a State statutory privilege, he may be able toassert the client's privilege for her.
ConclusionIt is essential for those who work with olderadults to respect their clients' autonomy andrights to privacy and confidentiality if they areto be effective in screening and assessing clientsfor substance use disorders and persuadingthem to cut down their use or enter treatment.In most situations, providers can follow thesesimple rules: (1) consult the client, (2) let theclient decide, and (3) be sensitive to howinformation is recorded or disclosed. It is onlyas a last resort that the provider will have toconsult State law or a lawyer.
137 117

Appendix A
EndnotesFor many years, there was confusion about
whether general medical care settings such asprimary care clinics or hospital emergencyrooms were subject to the Federal law andregulations because they provided substanceabuse diagnosis, referral, and treatment as partof their services. In 1995, DHHS revised thedefinition of the kinds of "programs" subject tothe regulations that made it clear that theregulations do not generally apply to a general
medical care facility unless that facility (or person)holds itself out as providing, and provides,alcohol or drug abuse diagnosis, treatment, orreferral for treatment . . . (42 CFR§ 2.11).
The full text of § 2.11 now reads:Program means:
(a) An individual or entity (other than a
general medical care facility) who holds itselfout as providing, and provides, alcohol or drugabuse diagnosis, treatment, or referral fortreatment; or
(b) An identified unit within a general medicalfacility which holds itself out as providing andprovides, alcohol or drug abuse diagnosis,treatment, or referral for treatment; or
(c) Medical personnel or other staff in a
general medical care facility whose primaryfunction is the provision of alcohol or drugabuse diagnosis, treatment, or referral fortreatment and who are identified as suchproviders. (See § 2.12(e)(1) for examples.)60 Federal Register 22,297 (May 5, 1995).
2 The regulations provide that "federallyassisted" programs include:
Programs run directly by or under contractfor the Federal government;
Programs carried out under a Federal license,certification, registration, or otherauthorization, including certification under
118 138
the Medicare Program, authorization toconduct a methadone maintenance treatmentprogram, or registration to dispense a drugthat is regulated by the ControlledSubstances Act to treat alcohol or drugabuse;
Programs supported by any federaldepartment or agency of the United States,even when the federal support does notdirectly pay for the alcohol or drug abusediagnosis, treatment, or referral activities;Programs conducted by State or localgovernment units that are supported byFederal funding that could be (but is notnecessarily) spent for the substance abusetreatment program;Tax-exempt programs.
42 C.F.R.§ 2.12(b).
For a full explanation of the Federal law andregulations, see TIP 8, Intensive OutpatientTreatment for Alcohol and Other Drug Abuse
(CSAT, 1994) and TAP 13, Confidentiality of
Patient Records for Alcohol and Other Drug
Treatment (CSAT, 1994).
4
Luhndorff v. The Superior Court of Tulare County,
166 CA 3d 485, 212 Cal. Rptr. 516 (5th District,1985). Interestingly, Luhndorffwas a criminalcase in which the prosecution sought the recordsof an unlicensed social worker who interviewedthe defendant, diagnosed his problem,determined the appropriate treatment, andtreated him for 3 months. The social workerwas working under a licensed individual'ssupervision. The defendant thought the socialworker was a psychiatrist.
'Section 451 of the California Evidence Codecodifies the doctor-patient privilege. SeeGrosslight v. Superior Court of Los Angeles, 42 CA
3d 502, 140 Cal. Rptr. 278 (1977), in which the
court held that information communicated by

the parents of a minor psychiatric patient to herdoctor and his secretary was privileged, eventhough the parents were being sued by someonethe child injured on the theory that the parentsknew their child was a danger to others.
6 Note that the breadth of the protection mayvary according to the clinician's profession.
7 Gross light v. Superior Court of Los Angeles, 72
Cal. App. 3d 502, 140 Cal. Rptr. 278 (1977),
interpreting Section 451 of the CaliforniaEvidence Code (see footnote 5).
8 The Consensus Panel for TIP 16 noted:"Physical separation of clinical information isnot unusual. Patient charts from past years aregenerally kept in a separate location. Physiciansroutinely request charts to be sent to them fromthis location so that they can review historicalclinical information about the patient. Inaddition, nurses are quite accustomed tokeeping some medications locked up andaccessible only to designated personnel." (TIP16, CSAT, 1995, p. 76)
9 In some States, a guardian is referred to as afiduciary, conservator, or committee. Theperson who has a guardian is generally called a"ward" or an "incapacitated person."
io Some States prohibit insurance companiesfrom discriminating against individuals whohave received substance abuse treatment;however, these kinds of discriminatory practicescontinue. Insurance companies routinely shareinformation about applicants for life anddisability insurance through the MedicalInformation Bureaua data bank maintained by
Legal and Ethical Issues
a private organization and supported by theindustry.
In fact, in some States, depending on theprovider's profession, the identity of patients orclients as well as their records are protected.Therefore, professionals should find outwhether disclosing a patient's name oracknowledging that the individual about whomthe lawyer is inquiring is a client would beconsidered a violation of the client's right toconfidentiality.
12 A firm, but polite, tone is best. If confrontedby what could be characterized as"stonewalling," a lawyer may be tempted tosubpoena the information he is asking for, andmore. The clinician will not want to provoke thelawyer into taking action that will harm thepatient.
13 The only exception to this advice would be ifthe provider knew the patient was a fugitivebeing sought by law enforcement. In that case,in some States, a refusal to assist or give officersinformation might be a criminal offense.
14 As noted above, in those States where theidentity of clients or patients as well as theirmedical or mental health records are protected,the professional should give a noncommittalresponse, such as "I'll have to check my recordsto see whether I have such a patient."
15 In most instances, the provider is not legallyrequired to notify the client or get his consent torelease records that have been subpoenaed.However, notifying the client shows respect forhis autonomy and privacy and gives him anopportunity to object to the subpoena.
139 119

Appendix
Appendix B contains the following items:
o The Alcohol Use Disorders Identification Test (AUDIT)O Index of Activities of Daily Living (Index of ADLs)O Instrumental Activities of Daily Living (IADL) Scaleo Geriatric Depression Scale (GDS) Short Formo Center for Epidemiologic StudiesDepression Scale (CES-D)o Health Screening Survey (HSS), Revised.
140121

Appendix B
The Alcohol Use Disorders Identification Test (AUDIT)The following guidelines, questions, and scoring instructions are excerpted from Babor, T.F.; de la Fuente, J.R.;Saunders, J.; and Grant, M. AUDIT: The Alcohol Use Disorders Identification Test: Guidelines for Use inPrimary Health Care. Geneva, Switzerland: World Health Organization, 1992.
How To Use AUDITScreening with AUDIT can be conducted in a variety of primary care settings by persons who havedifferent kinds of training and professional backgrounds. The core AUDIT is designed to be used as abrief structured interview or self-report survey that can easily be incorporated into a general healthinterview, lifestyle questionnaire, or medical history. When presented in this context by a concerned andinterested interviewer, few patients will be offended by the questions. The experience of the WHOcollaborating investigators (Saunders and Aasland, 1987) indicated that AUDIT questions were answeredaccurately regardless of cultural background, age, or gender. In fact, many patients who drank heavilywere pleased to find that a health worker was interested in their use of alcohol and the problemsassociated with it.
In some patients, the AUDIT questions may not be answered accurately because they refer specificallyto alcohol use and problems. Some patients may be reluctant to confront their alcohol use or to admitthat it is causing them harm. Individuals who feel threatened by revealing this information to a healthworker, who are intoxicated at the time of the interview, or who have certain kinds of mental impairmentmay give inaccurate responses. Patients tend to answer most accurately when
The interviewer is friendly and nonthreateningThe purpose of the questions is clearly related to a diagnosis of their health statusThe patient is alcohol- and drug-free at the time of the screeningThe information is considered confidentialThe questions are easy to understand
Health workers should try to establish these conditions before AUDIT is given. When theseconditions are not present, the Clinical Screening Instrument following the AUDIT questionnaire may bemore useful. Alternatively, health workers may also use AUDIT to guide an interview with a concernedfriend, spouse, or family member. In some settings (such as waiting rooms), AUDIT may beadministered as a sell-report questionnaire, with instructions for the patient to discuss the meaning of theresults with the primary care worker. In addition to these general considerations, the followinginterviewing techniques should be used:
Try to interview patients under the best possible circumstances. For patients requiring emergencytreatment or who are severely impaired, it is best to wait until their condition has stabilized and theyhave become accustomed to the health setting where the interview is to take place.Look for signs of alcohol or drug intoxication. Patients who have alcohol on their breath or whoappear intoxicated may be unreliable respondents. Consider conducting the interview at a later time.If this is not possible, make note of these findings on the patient's record.If AUDIT is embedded, as recommended, in a longer health interview, then a transitional statementwill be needed when the AUDIT questions are asked. The best way to introduce the AUDIT questions
122
14 1

Tools
is to give the patient a general idea of the content of the questions, the purpose for asking them, andthe need for accurate answers. The following is an illustrative introduction: "Now I am going to askyou some questions about your use of alcoholic beverages during the past year. Because alcohol use
can affect many areas of health (and may interfere with certain medications), it is important for us to
know how much you usually drink and whether you have experienced any problems with yourdrinking. Please try to be as honest and as accurate as you can be." This statement should befollowed by a description of the types of alcoholic beverages typically consumed in the population towhich the patient belongs (e.g., "By alcoholic beverages we mean your use of wine, beer, vodka,sherry, and so on."). If necessary, include a description of beverages that may not be considered
alcoholic (e.g., cider, low alcohol beer).It is important to read the questions as written and in the order indicated. By following the exactwording, better comparability will be obtained between your results and those obtained by other
interviewers.Most of the questions in AUDIT are phrased in terms of "how often" symptoms occur. It is useful tooffer the patient several examples of the response categories (for example, "Never," "Several times amonth," "Daily") to suggest how he might answer. When he has responded, it is useful to probeduring the initial questions to be sure that the patient has selected the most accurate response (forexample, "You say you drink several times a week. Is this just on weekends or do you drink more orless every day?"). If responses are ambiguous or evasive, continue asking for clarification byrepeating the question and the response options, asking the patient to choose the best one. At times,answers are difficult to record because the patient may not drink on a regular basis. For example, ifthe patient was drinking intensively for the month prior to an accident, but not before or since, then itwill be difficult to characterize the "typical" drinking sought by the question. In these cases it is best
to record the amount of drinking and related symptoms for the heaviest drinking period of the past
year, making note of the fact that this may be atypical or transitory for that individual.
Record answers carefully, using the comments section of the interview brochure to explain any specialcircumstances, additional information, or clinical inferences. Often patients will provide the interviewerwith useful comments about their drinking that can be valuable in the interpretation of the total AUDIT
score.
142123

Appendix B
The AUDIT QuestionnaireCircle the number that comes closest to the patient's answer.
1. How often do you have a drink containing alcohol?
(0) Never (1) Monthly or (2) Two to four (3) Two to three (4) Four or moreless times a month times a week times a week
2. How many drinks containing alcohol do you have on a typical day when you are drinking?[Code number of standard drinks.')
(0) 1 or 2 (1) 3 or 4 (2) 5 or 6 (3) 7 to 9 (4) 10 or more
3. How often do you have six or more drinks on one occasion?
(0) Never (1) Less than (2) Monthly (3) Weekly (4) Daily ormonthly almost daily
4. How often during the last year have you found that you were not able to stop drinking once youhad started?
(0) Never (1) Less than (2) Monthly (3) Weekly (4) Daily ormonthly almost daily
5. How often during the last year have you failed to do what was normally expected from you becauseof drinking?
(0) Never (1) Less than (2) Monthly (3) Weekly (4) Daily ormonthly almost daily
6. How often during the last year have you needed a first drink in the morning to get yourself goingafter a heavy drinking session?
(0) Never (1) Less than (2) Monthly (3) Weekly (4) Daily ormonthly almost daily
7. How often during the last year have you had a feeling of guilt or remorse after drinking?
(0) Never
124
(1) Less than (2) Monthly (3) Weekly (4) Daily ormonthly almost daily
14 3

Tools
8. How often during the last year have you been unable to remember what happened the night beforebecause you had been drinking?
(0) Never (1) Less than (2) Monthly (3) Weekly (4) Daily or
monthly almost daily
9. Have you or someone else been injured as a result of your drinking?
(0) No (2) Yes, but not in the last year (4) Yes, during the last year
10. Has a relative or friend or a doctor or other health worker been concerned about your drinking orsuggested you cut down?
(0) No (2) Yes, but not in the last year (4) Yes, during the last year
In determining the response categories it has been assumed that one drink contains 10 g alcohol. Incountries where the alcohol content of a standard drink differs by more than 25 percent from 10 g, the
response category should be modified accordingly.
Record sum of individual item scores here.
144125

Appendix B
Procedure for scoring AUDITQuestions 1-8 are scored 0, 1,follows:
2, 3, or 4. Questions 9 and 10 are scored 0, 2, or 4 only. The response is as
0 1 2 3 4
Question 1 Never Monthly or less Two to fourtimes permonth
Two to threetimes per week
Four or moretimes per week
Question 2 1 or 2 3 or 4 5 or 6 7 to 9 10 or more
Questions 3-8 Never Less thanmonthly
Monthly Weekly Daily or almostdaily
Questions 9-10 No Yes, but not inthe last year
Yes, during thelast year
The minimum score (for nondrinkers) is 0 and the maximum possible score is 40. A score of 8 or moreindicates a strong likelihood of hazardous or harmful alcohol consumption.
126 145

Tools
AUDIT "Clinical" Questions and Procedure
Trauma history
1. Have you injured your head since your 18th birthday?
(3) Yes (0) No
2. Have you broken any bones since your 18th birthday?
(3) Yes (0) No
Clinical examination
1. Conjunctival injections
(0) NOT PRESENT (1) MILD (2) MODERATE (3) SEVERE
2. Abnormal skin vascularization
(0) NOT PRESENT (1) MILD (2) MODERATE (3) SEVERE
3. Hand tremor
(0) NOT PRESENT (1) MILD (2) MODERATE (3) SEVERE
4. Tongue tremor
(0) NOT PRESENT (1) MILD (2) MODERATE (3) SEVERE
5. Hepatomegaly
(0) NOT PRESENT (1) MILD (2) MODERATE
GGT Values' Lower normal (0-30 IU/1) = (0)Upper normal (30- 501U/1) = (1)
Abnormal (50 IU/1) = (3)
(3) SEVERE
'These values may change with laboratory methods, and standards may vary with sex and age of the
drinker.
Record sum of individual item scores here.
146 127

Appendix B
Scoring and Interpretation of AUDITAs indicated by the AUDIT questions, each item is scored by checking the response category that comesclosest to the patient's answer.
On the basis of evidence from the validation study (Saunders et al., in press), two cutoff points aresuggested, depending on the purpose of the screening program or the nature of the research project. Ascore of 8 or more produces the highest sensitivity, while a score of 10 or more results in higherspecificity. In general, high scores on the first three items in the absence of elevated scores on theremaining items suggest hazardous alcohol use. Elevatedscores on items 4 through 6 imply the presenceor emergence of alcohol dependence. High scores on the remaining items suggest harmful alcohol use. Asdiscussed in the following section on diagnosis, each of these areas of alcohol-related problems impliesdifferent types of management.
The Clinical Screening Instrument is considered to be elevated when the total score is 5 or greater.Here, too, the examiner should give careful consideration to the different meanings attributed to alcohol-related trauma, physical signs, and the elevated liver enzyme. It should be noted that false positives canoccur when the individual is accident prone, uses drugs (such as barbiturates) that induce GGT, or hashand tremor because of nervousness, neurological disorder, or nicotine dependence.
References
Saunders, J.B., and Aasland, O.G. WHO Collaborative Project on the Identification and Treatment ofPersons with Harmful Alcohol Consumption. Report on Phase I: Development of a ScreeningInstrument. Geneva, Switzerland: World Health Organization, 1987.
Saunders, J.B.; Aasland, O.G.; Babor, T.F.; de la Fuente, J.R.; and Grant, M. WHO collaborative project onearly detection of persons with harmful alcohol consumption. II. Development of the screeninginstrument "AUDIT." British Journal of Addictions, in press.
128 147

Tools
'Index of Activities ®f Daily Living (ADLs)
Index of independence in Activities of Daily LivingThe Index of Independence in Activities of Daily Living is based on an evaluation of the functionalindependence or dependence of patients in bathing, dressing, going to the toilet, transferring, continence,and feeding. Specific definitions of functional independence and dependence appear below the index.
(These definitions can be used to convert the data recorded in the evaluation form in the next section into
an Index of ADL grade.)
AIndependent in feeding, continence, transferring, going to the toilet, dressing, and bathing.BIndependent in all but one of these functions.CIndependent in all but bathing and one additional function.DIndependent in all but bathing, dressing, and one additional function.EIndependent in all but bathing, dressing, going to the toilet, and one additional function.FIndependent in all but bathing, dressing, going to toilet, transferring, and one additional
function.GDependent in all six functions.
OtherDependent in at least two functions, but not classifiable as C, D, E, or F.
Independence means without supervision, direction, or active personal assistance, except as specifically
noted below. This is based on actual status and not on ability. A patient who refuses to perform a
function is considered as not performing the function, even though he is deemed able.
Bathing (Sponge, Shower, or Tub)Independent: assistance only in bathing a singlepart (as back or disabled extremity) or bathes self
completelyDependent: assistance in bathing more than onepart of body; assistance in getting in or out of tub
or does not bathe selfDressingIndependent: gets clothes from closets anddrawers; puts on clothes, outer garments, braces;manages fasteners; act of tying shoes is excludedDependent: does not dress self or remains partly
undressed
Going to ToiletIndependent: gets to toilet; gets on and off toilet;arranges clothes; cleans organs of excretion; (maymanage own bedpan used at night only and mayor may not be using mechanical supports)Dependent: uses bedpan or commode or receivesassistance in getting to and using toilet
TransferIndependent: moves in and out of bed independentlyand moves in and out of chair independently (may ormay not be using mechanical supports)Dependent: assistance in moving in or out of bedand/or chair; does not perform one or more transfers
ContinenceIndependent: urination and defecation entirely self-
controlledDependent: partial or total incontinence in urinationor defecation, partial or total control by enemas,catheters, or regulated use of urinals and/or bedpans
FeedingIndependent: gets food from plate or its equivalentinto mouth; (precutting of meat and preparation offood, as buttering bread, are excluded from
evaluation)Dependent: assistance in act of feeding (see above);
does not eat at all or parental feeding
148 129

Appendix B
Evaluation Form
Name Day of Evaluation
For each area of functioning listed below, check description that applies. (The word "assistance" meanssupervision, direction, or personal assistance.)
Bathingeither sponge bath, tub bath, or shower.
Receives no assistance (gets inand out of tub by self if tub isusual means of bathing)
Receives assistance in bathing Receives assistance in bathingonly one part of the body more than one part of the(such as back or a leg) body (or not bathed)
Dressinggets clothes from closets and drawersincluding underclothes, outer garments, and usingfasteners (including braces if worn)
0Gets clothes and getscompletely dressed withoutassistance
0Gets clothes and gets dressed
without assistance except forassistance in tying shoes
0Receives assistance in gettingclothes or in getting dressed,or stays partially orcompletely undressed
Toiletinggoing to the "toilet room" for bowel and urine elimination, cleaning self after elimination, andarranging clothes
0Goes to "toilet room," cleansself, and arranges clothes
without assistance (may useobject for support such ascane, walker, or wheelchairand may manage nightbedpan or commodeemptying same in morning)
Transfer-
0Receives assistance in going to"toilet room" or in cleansingself or in arranging clothes
after elimination or in use ofnight bedpan or commode
0Doesn't go to room termed"toilet" for the eliminationprocess
Moves in and out of bed as Moves in and out of bed or Doesn't get out of bedwell as in and out of chair chair with assistancewithout assistance (may beusing object for support suchas cane or walker)
130 14

Continence0
Controls urination and bowel Has occasional "accidents"
movement completely by self
Feeding-0
Feeds self without assistance
Supervision helps keep urineor bowel control; catheter isused, or is incontinent
Feeds self except for getting Receives assistance in feeding
assistance in cutting meat or or is fed partly or completely
buttering bread by using tubes or intravenousfluids
Tools
After filling out the form, convert the data collected into an ADL grade by using the definitions provided
in the introductory section.
Source: Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; and Jaffe, M.W. Studies of Illness in the
Aged. The Index of ADL: A standardized measure of biological and psychosocial function. Journal of the
American Medical Association 185:914-919, 1963.
References
Katz, S.; Downs, T.D.; Cash, H.R.; and Grotz, R.C. Progress in development of the Index of ADL.
Gerontologist 10(420-30, 1970.
Katz, S., and Akpom, C.A. Index of ADL. Medical Care 14(suppl. 5):116-118. 1976.
150131

Appendix B
Instrumental Activities of Daily Living (IADL) ScaleSelf-Rated Version Extracted From the Multilevel Assessment Instrument (MAI)
132
1. Can you use the telephone:
Without help, 3With some help, or 2Are you completely unable to use the telephone? 1
2. Can you get to places out of walking distance:
Without help, 3With some help, or 2
Are you completely unable to travel unless special arrangements are made? 1
3. Can you go shopping for groceries:
Without help, 3With some help, or 2Are you completely unable to do any shopping? 1
4. Can you prepare your own meals:
Without help, 3With some help, or 2
Are you completely unable to prepare any meals? 1
5. Can you do your own housework:
Without help, 3
With some help, or 2
Are you completely unable to do any housework? 1
6. Can you do your own handyman work:
Without help, 3
With some help, or 2
Are you completely unable to do any handyman work? 1
151

Tools
7. Can you do your own laundry:
Without help, 3
With some help, or 2
Are you completely unable to do any laundry at all? 1
8a. Do you take any medications or use any medications?
(ASK Q. 8b) Yes
(ASK Q. 8c) No
8b. (ASK IF SUBJECT TAKES MEDICINE NOW)
Do you take your own medicine: (CHECK BELOW)
8c. (ASK IF SUBJECT DOES NOT TAKE MEDICINE NOW)
If you had to take medicine, can you do it: (CHECK BELOW)
Without help (in the right doses at the right time),With some help (take medicine if someone prepares it for you
and/or reminds you to take it), or(Are you/would you be) completely unable to take your own medicines?
9. Can you manage your own money:
1
2
3
2
1
Without help, 3
With some help, or 2
Are you completely unable to handle money? 1
Note on Scoring:
If fewer than 5 items are valid, then scoring cannot be done reliably.
Source: Lawton, M.P.; Moss, M.; Fulcomer, M.; and Kleban, M.H. A research and service-orientedMultilevel Assessment Instrument. Journal of Gerontology 37:91-99, 1982.
References
Lawton, M.P. Scales to measure competence in everyday activities. Psychopharmacology Bulletin
24(4):609-614, 1988.
Lawton, M.P., and Brody, E.M. Assessment of older people: Self-maintaining and instrumental activitiesof daily living. Gerontologist 9:179-186, 1969.
Reproduced with permission from M. Powell Lawton, Ph.D.
152 133

Appendix B
Geriatric Depression Scale (GDS) Short FormChoose the best answer for how you have felt over the past week:
1. Are you basically satisfied with your life? YES/NO
2. Have you dropped many of your activities and interests? YES/NO
3. Do you feel that your life is empty? YES/NO
4. Do you often get bored? YES/NO
5. Are you in good spirits most of the time? YES/NO
6. Are you afraid that something bad is going to happen to you? YES/NO
7. Do you feel happy most of the time? YES/NO
8. Do you often feel helpless? YES/NO
9. Do you prefer to stay at home, rather than going out and doingnew things? YES/NO
10. Do you feel you have more problems with memory than most? YES/NO
11. Do you think it is wonderful to be alive now? YES/NO
12. Do you feel pretty worthless the way youare now? YES/NO
13. Do you feel full of energy? YES/NO
14. Do you feel that your situation is hopeless? YES/NO
15. Do you think that most people are better off than you are? YES/NO
Answers in bold indicate depression, and each answer counts as one point. For clinical purposes, a scoregreater than 5 suggests depression and warrants a followup interview. Scores greater than 10 are almostalways depression.
Source: Sheikh, J.I., and Yesavage, J.A. Geriatric Depression Scale (GDS): Recent evidence anddevelopment of a shorter version. Clinical Gerontologist 5(1&2):165-173, 1986.
References
Brink, T.L.; Yesavage, J.A.; Lum, O.; Heersema, P.; Adey, M.B.; and Rose, T.L. Screening tests for geriatricdepression. Clinical Gerontologist 1:37-44, 1982.
Yesavage, J.A.; Brink, T.L.; Rose, T.L.; Lum, O.; Huang, V.; Adey, M.B.; and Leirer, V.O. Developmentand validation of a geriatric depression screening scale: A preliminary report. Journal of PsychiatricResearch 17:37-49, 1983.
134
153

Tools
The Center for Epidemiologic Studies DepressionScale (CES-D)For the 20 items below, circle the number next to each item that best reflects how frequently the indicatedevent was experienced in the past 7 days.
Rarely or Some or a Occasionally Most or allnone of the little of the or a of the time
time time moderateamount of
time(Less than (1-2 days) (3-4 Days) (5-7 Days)
1 Day)
DURING THE PAST WEEK:
1. I was bothered by things that usuallydon't bother me. 0 1 2 3
2. I did not feel like eating: my appetitewas poor. 0 1 2 3
3. I felt that I could not shake off the blueseven with help from my family orfriends. 0 1 2 3
4. I felt that I was just as good as otherpeople. 0 1 2 3
5. I had trouble keeping my mind on whatI was doing. 0 1 2 3
6. I felt depressed. 0 1 2 3
7. I felt that everything I did was an effort. 0 1 2 3
8. I felt hopeful about the future. 0 1 2 3
9. I thought my life had been a failure. 0 1 2 3
10. I felt fearful. 0 1 2 3
11. My sleep was restless. 0 1 2 3
12. I was happy. 0 1 2 3
13. I talked less than usual. 0 1 2 3
14. I felt lonely. 0 1 2 3
15. People were unfriendly. 0 1 2 3
16. I enjoyed life. 0 1 2 3
17. I had crying spells. 0 1 2 3
18. I felt sad. 0 1 2 3
19. I felt that people disliked me. 0 1 2 3
20. I could not get "going." 0 1 2 3
154 135

Appendix B
Scoring: Since items 4, 8, 12, and 16 reflect positive experiences rather than negative ones, the scale shouldbe reversed on these items so that 0 = 3, 1 = 2, 2 = 1, and 3 = 0. To determine the "depression score,"add together the number for each answer. The score will be somewhere in the range of 0 to 60. A scoreof 16 or greater indicates that some depression may have been experienced in the past week.
Source: Radloff, L.S. The CES-D Scale: A self-report depression scale for research in the generalpopulation. Applied Psychological Measurement 1(3):385-401, 1977.
136 135

Tools
Health Screening Survey (MISS), RevisedCheck the appropriate answer
1. In the last three months, have you been dieting to lose weight?YES NO
IF YES: How many pounds have you managed to lose?0 1-3 4-7 8 or more
2. In the last three months, have you performed physical activity or exercise in your leisure time atleast 20 minutes without stopping, enough to make you breathe hard and/or sweat?
YES NOIF YES: On average, how many days per week have you been exercising
_1 -2 _3 -4 _5 -6 _Every day
3. In the last three months, have you been smoking cigarettes at all?YES NO
IF YES: On average, how many cigarettes have you been smoking each day?1-9 10-19 20-29 30 or more
4. In the last three months, have you been drinking alcoholic drinks at all (e.g., beer, wine, sherry,vermouth, or hard liquor)?
YES NOIF NO, go to question 5.IF YES, ANSWER 4a through 4c.
4a. On average, how many days per week have you been drinking beer or wine coolers?_None 1-2 _3-4 5-6 Every day
On a day when you have had wine, sherry, or vermouth to drink, how many glasses, bottles, or canshave you been drinking?
1-2 3-4 5-8 9-14 15 or more
AND4b. On average how many days per week have you been drinking wine, sherry, or vermouth?
None _1-2 3-4 5-6 Every day
On a day when you have had wine, sherry, or vermouth to drink, how many glasses have you beendrinking?
1-2 3-4 5-8 9-14 15 or moreAND
15 6 BEST COPY AVAILABLE137

Appendix B
4c. On average how many days per week have you been drinking liquor (gin, vodka, rum, brandy,whiskey, etc.)?
_None _1 -2 _3 -4 5-6 _Every day
On a day when you have had liquor to drink, how many single shots have you been drinking?1-2 3-4 5-8 9-14 15 or more
5. In the last three months have you felt you should:a. lose some weight
b. cut down or stop smoking
c. cut down or stop drinking
d. do more to keep fit
No Often Very OftenNo
_Sometimes _QuiteOften Very Often
No_Sometimes _Quite
Quite Often Very Often_No
_Sometimes_Sometimes _Quite Often Very Often
6. In the last three months has anyone annoyed you or got on your nerves by tellingyou to:a. change your weight _No _Sometimes _Quite Often Very Oftenb. cut down or stop smoking _No _Sometimes Quite Often _Very Oftenc. cut down or stop drinking No _Sometimes Quite Often Very Oftend. do more to keep fit No _Sometimes _Quite Often _Very Often
7. In the last three months, have you felt guilty or bad about:a. your weight _No _Sometimes _Quite Often _Very Oftenb. how much you smoke _No Sometimes _Quite Often _Very Oftenc. how much you drink _No _Sometimes _Quite Often _Very Oftend. how unfit you are _No _Sometimes _Quite Often _Very Often
8. In the last three months, have you been waking up wanting to:a. exercise to keep fit _No _Sometimes Quite Often Very Oftenb. smoke a cigarette No _Sometimes _Quite Often _Very Oftenc. have an alcoholic drink No _Sometimes _Quite Often Very Oftend. have something to eat No _Sometimes _Quite Often Very Often
9. Now that you have completed this form, do you think you currently have:a. a weight problem _Definitely _Probably _No _Don't Knowb. a smoking problem _Definitely Probably _No Don't Knowc. a drinking problem Definitely Probably No _Don't Knowd. a fitness problem Definitely Probably No Don't Know
10. Thinking back, would you say at any time in the past you had:a. a weight problem _Definitely _Probably _No Don't Knowb. a smoking problem _Definitely _Probably _No _Don't Knowc. a drinking problem _Definitely Probably _No _Don't Knowd. a fitness problem _Definitely _Probably _No _Don't Know
138
157

Tools
Scoring: The HSS contains four subscales: one measuring amount of alcohol consumption (question 4 a,b, c; Kristenson and Trell, 1982), the CAGE questionnaire (questions 5-8; Mayfield et al., 1974), one forself-perception of current problem with alcohol (question 9), and one for self-perception of past problemwith alcohol (question 10). Consumption of 20 or more drinks per week, two or more positive responsesto the four CAGE questions, self-perception of a current problem with alcohol use, or self-perception of apast problem with alcohol use indicates problem drinking.
Source: Fleming, M.F., and Barry, K.L. A three-sample test of a masked alcohol screening questionnaire.Alcohol and Alcoholism 26(1):81-91, 1991.
ReferencesKristenson, H., and Trell, E. Indicators of alcohol consumption: Comparisons between a questionnaire(Mm-MAST), interviews, and serum y-glutamyl transferase (GGT) in a health survey of middle-agedmales. British Journal of Addiction 77, 297-304, 1982.
Mayfield, D.; McLeod, G.; and Hall, P. The CAGE questionnaire: Validation of a new alcoholismscreening instrument. American Journal of Psychiatry 131:1121-1128, 1974.
Reproduced with permission.
i5 139

Appendix CBibliography
Adams, W.L.; Barry, K.L.; and Fleming, M.F.
Screening for problem drinking in olderprimary care patients. Journal of the American
Medical Association 276(24):1964-1967, 1996.
Adams, W.L.; Magruder-Habib, K.; Trued, S.;and Broome, H.L. Alcohol abuse in elderlyemergency department patients. Journal ofthe American Geriatric Society 40:1236-1240,
1992.
Adams, W.L.; Yuan, Z.; Barboriak, J.J.; and
Rimm, A.A. Alcohol-related hospitalizationsof elderly people: Prevalence andgeographic location in the United States.Journal of the American Medical Association
270(10):1222-1225, 1993.
Administration on Aging and Staff of the U.S.Senate Special Committee on Aging. AgingAmerica: Trends and Projections. Washington,
DC: Administration on Aging, 1991.
Administration on Aging. A Profile of OlderAmericans: 1995. Rockville, MD:
Administration on Aging, U.S. Departmentof Health and Human Services.http: / / www.aoa.dhhs.gov /aoa /pages /profi195.html [Accessed Sept 23, 1996].
Aldrich, M.S. Effects of alcohol on sleep. In:Gomberg, E.; Hedgedus, A.M.; and Zucker,R.A., eds. Alcohol Problems and Aging.
Washington DC: National Institute onAlcohol Abuse and Alcoholism, in press.
Alterman, A.I.; Kushner, H.; and Holahan, J.M.Cognitive functioning and treatmentoutcome in alcoholics. Journal of Nervous and
Mental Disorders 178(8):494-499, 1990.
Altpeter, M.; Schmall, V.; Rakowski, W.; Swift,
R.; and Campbell, J. Alcohol and Drug
Problems in the Elderly: Instructor's Guide
[Project ADEPT Curriculum for PrimaryCare Physician Training]. Providence, RI:Center for Alcohol and Addiction Studies,1994.
American Psychiatric Association. Diagnosticand Statistical Manual of Mental Disorders, 3rd
ed., revised. Washington, DC: AmericanPsychiatric Association, 1987.
American Psychiatric Association. Diagnosticand Statistical Manual of Mental Disorders, 4th
ed. Washington, DC: American PsychiatricAssociation, 1994.
159141

Appendix C
American Society of Addiction Medicine.Patient Placement Criteria for the Treatment of
Substance-Related Disorders, 2nd ed.
Washington, DC: American Society ofAddiction Medicine, 1996.
Anda, R.F.; Williamson, D.F.; and Remington,P.L. Alcohol and fatal injuries among U.S.adults. Journal of the American Medical
Association 260:2529-2532,1988.
Anderson, P., and Scott, E. The effect of generalpractitioners' advice to heavy drinking men.British Journal of Addiction 87:891 -900, 1992.
Annis, H.M. Is inpatient rehabilitation of thealcoholic cost effective? Con position.Advances in Alcohol and Substance Use 5:175,
1986.
Artaud-Wild, S.M.; Connor, S.L.; Sexton, G.; andConnor, W.E. Differences in coronarymortality can be explained by differences incholesterol and saturated fat intakes in 40countries but not in France and Finland.Circulation 88:2771 -2779, 1993.
Atkinson, R. Alcohol problems of the elderly.Alcohol and Alcoholism 22(4):415 -417, 1987.
Atkinson, R. Persuading alcoholic patients toseek treatment. Comprehensive Therapy11(11):16 -24, 1985.
Atkinson, R.M. Age-specific treatment of olderadult alcoholics. In: Gomberg, E.S.L.;Hegedus, A.M.; and Zucker, R.A., eds.Alcohol Problems and Aging. Rockville, MD:
National Institute on Alcohol Abuse andAlcoholism, in press.
Atkinson, R.M. Aging and alcohol usedisorders: Diagnostic issues in the elderly.International Psychogeriatrics 2:55 -72, 1990.
142
Atkinson, R.M. Late onset problem drinking inolder adults. International Journal of GeriatricPsychiatry 9:321 -326, 1994.
Atkinson, R.M. Substance use and abuse in latelife. In: Atkinson, R.M., ed. Alcohol and DrugAbuse in Old Age. Washington, DC:
American Psychiatric Press, 1984. pp. 1-21.
Atkinson, R.M. Treatment programs for agingalcoholics. In: Beresford, T., and Gomberg,E., eds. Alcohol and Aging. New York:
Oxford University Press, 1995. pp.186-210.
Atkinson, R.M., and Ganzini, L. Substanceabuse. In: Coffey, C.E., and Cummings, J.L.,eds. Textbook of Geriatric Neuropsychiatry.
Washington, DC: American PsychiatricPress, 1994. pp. 297-321.
Atkinson, R.M.; Ganzini, L.; and Bernstein, M.J.
Alcohol and substance-use disorders in theelderly. In: Birren, J.E.; Sloane, R.B.; and
Cohen, G.D., eds. Handbook of Mental Health
and Aging, 2nd ed. San Diego, CA:Academic Press, 1992. pp. 515-555.
Atkinson, R.M., and Kofoed, L.L. Alcohol anddrug abuse in old age: A clinical perspective.Substance and Alcohol Actions and Misuse
3(6):353-368,1982.
Atkinson, R.M., and Schuckit, M.A. Geriatricalcohol and drug misuse and abuse.Advances in Alcohol and Substance Abuse
3:195 -237, 1983.
Atkinson, R.M.; Tolson, R.L.; and Turner, J.A.
Factors affecting outpatient treatmentcompliance of older male problem drinkers.Journal of Studies on Alcohol 54:102-106,1993.

Atkinson, R.M.; Tolson, R.L.; and Turner, J.A.
Late versus early onset problem drinking inolder men. Alcoholism: Clinical and
Experimental Research 14:574 -579, 1990b.
Atkinson, R.M.; Turner, J.A.; Kofoed, L.L.; andTolson, R.L. Early versus late onsetalcoholism in older persons: Preliminaryfindings. Alcoholism: Clinical and
Experimental Research, 9:513 -515, 1985.
Avorn, J.; Monane, M.; Everitt, D.E.; Beers, M.H.;and Fields, D. Clinical assessment ofextrapyradimal signs in nursing homepatients given antipsychotic medication.Archives of Internal Medicine
154(10):1113 -1117, 1994.
Babor, T.; Korner, P.; Wilber, C.; and Good, S.
Screening and early intervention strategiesfor harmful drinkers: Initial lessons from theAMETHYST Project. Australian Drug andAlcohol Review 6:325 -339, 1987.
Babor, T.F. Avoiding the horrid and beastly sinof drunkenness: Does dissuasion make adifference? Journal of Consulting and Clinical
Psychology 62:1127-1140,1994.
Babor, T.F.; de la Fuenta, J.R.; Saunders, J.; and
Grant, M. AUDIT: The Alcohol Use Disorders
Identification Test: Guidelines for Its Use in
Primary Health Care. Geneva, Switzerland:World Health Organization, 1992.
Babor, T.F., and Grant, M. Project on
Identification and Management of Alcohol-
Related Problems. Report on Phase II: A
Randomized Clinical Trial of Brief Interventions
in Primary Health Care. Geneva, Switzerland:World Health Organization, 1992.
Bibliography
Babor T.F.; Grant, M.; Acuda, W.; Burns, F.H.;
Campillo, C.; DelBoca, F.K.; Hodgson, R.;
Ivanets, N.N.; Lukomskya, M.; and Machuna,M. A randomized clinical trial of briefinterventions in primary care: Summary of aWHO project. Addiction 89:657 -660, 1994.
Baker, S.L. Substance abuse disorders in agingveterans. In: Gottheil, E.; Druley, R.A.;Skiloday, T.E.; and Waxman, H., eds.Alcohol, Drug Addiction and Aging.
Springfield, IL: Charles C Thomas, 1985. pp.303-311.
Balter, M.B. An analysis of psychotherapeuticdrug consumption in the United States. In:Bowen, R.A., ed. Proceedings of the Anglo-
American Conference on Drug Abuse: Etiology
of Drug Abuse I. London: Royal Society ofMedicine, 1973. pp. 58-68.
Barnas, C.; Rossmann, M.; Roessler, H.; Reimer,Y.; and Fleischhacker, W.W. Benzodiazepineand other psychotropic drug abuse bypatients in a methadone maintenanceprogram: Familiarity and preference. Journalof Clinical Psychopharmacology 12(6):397-402,
1992.
Barry, K., and Fleming, M. A comparison of theAlcohol Use Disorders Identification Test(AUDIT) to the SMAST-13 in a primary caresample. Alcohol and Alcoholism 2:33 -42, 1993.
Beresford, T.P. Alcohol and aging: Lookingahead. In: Beresford, T.P., and Gomberg, E.,eds. Alcohol and Aging. New York: OxfordUniversity Press, 1995a. pp. 327-336.
Beresford, T.P. Alcoholic elderly: Prevalence,screening, diagnosis, and prognosis. In:Beresford, T.P, and Gomberg, E., eds. Alcoholand Aging. New York: Oxford UniversityPress, 1995b. pp. 3-18.
161. 143

Appendix C
Beresford, T.P.; Blow, F.C.; Brower, K.J.; Adams,
K.M.; and Hall, R.C.W. Alcoholism andaging in the general hospital. Psychosomatics29:61 -72, 1988.
Beresford, T.P.; Blow, F.C.; Hill, E.; Singer, K.;
and Lucey, M.R. Comparison of CAGEquestionnaire and computer-assistedlaboratory profiles in screening for covertalcoholism. Lancet 336:482-485, August 25,1990.
Beresford, T.P., and Lucey, M.R. Ethanolmetabolism and intoxication in the elderly.In: Beresford, T.P., and Gomberg, E.S., eds.Alcohol and Aging. New York: Oxford
University Press, 1995. pp. 117-127.
Bezchlibnyk-Butler, K.Z., and Jeffries, J.J., eds.
Clinical Handbook of Psychotropic Drugs, 5th
ed. Toronto, Canada: Hogrefe & Huber,1995.
Bien, T.H.; Miller, W.R.; and Tonigan, J.S. Brief
interventions for alcohol problems: Areview. Addiction 88:315 -335, 1993.
Blazer, D.; Cromwell, B.A.; and George, L.K.
Alcohol abuse and dependence in the ruralSouth. Archives of General Psychiatry
44:736 -740, 1987a.
Blazer, D.; Hughes, D.C.; and George, L.K. Theepidemiology of depression in an elderlycommunity population. Gerontologist27(3):281 -287, 1987b.
Blazer, D., and Williams, C.D. Epidemiology ofdysphoria and depression in an elderlypopulation. American Journal of Psychiatry137:439- 444, 1980.
144
Blow, F.C. The spectrum of alcoholinterventions for older adults. In: Gomberg,E.S.L.; Hegedus, A.M.; and Zucker, R.A., eds.Alcohol Problems and Aging. Rockville, MD:
National Institute on Alcohol Abuse andAlcoholism, in press.
Blow, F.C.; Brower, K.J.; Schulenberg, J.E.;
Demo-Dananberg, L.M.; Young, J.P.; andBeresford, T.P. The Michigan AlcoholismScreening TestGeriatric Version (MAST-G):A new elderly-specific screening instrument.Alcoholism: Clinical and Experimental Research
16:372, 1992a.
Blow, F.C.; Cook, C.A.; Booth. B.M.; Falcon, S.P.;
and Friedman, M.J. Age-related psychiatriccomorbidities and level of functioning inalcoholic veterans seeking outpatienttreatment. Hospital and Community Psychiatry
43:990-995,1992.
Blow, F.C.; Walton, M.A.; Chermack, S.T.;
Mudd, S.A.; Brower, K.J.; and Comstock,M.A. Treatment outcome for elderlyalcoholics following elder-specific inpatienttreatment. Manuscript submitted forpublication, 1997.
Booth, B.M.; Blow, F.C.; Cook, C.A.; Bunn, J.Y.;
and Fortney, J.C. Age and ethnicity amonghospitalized alcoholics: A nationwide study.Alcoholism: Clinical and Experimental Research
16:1029 -1034, 1992.
Brandt, J.; Butters, N.; Ryan, C.; and Bayog, R.
Cognitive loss and recovery in long-termalcohol abusers. Archives of General Psychiatry
40:435 -442, 1983.
162

Brennan, P.L., and Moos, R.H. Late-life problemdrinking: Personal and environmental riskfactors for 4-year functioning outcomes andtreatment seeking. Journal of Substance Abuse
8:167-180, 1996.
Brennan, P.L.; Moos, R.H.; and Kim, J.Y. Gender
differences in the individual characteristicsand life contexts of late-middle-aged andolder problem drinkers. Addiction88:781-790, 1993.
Brower, K.J.; Mudd, S.; Blow, F.C.; Young, J.P.;
and Hill, E.M. Severity and treatment ofalcohol withdrawal in elderly versusyounger patients. Alcoholism: Clinical andExperimental Research 18(1):196-201, 1994.
Brown, S.A.; Inaba, R.K.; Gillin, J.C.; Shuckit,
M.A.; Stewart, M.A.; and Irwin, M.R.
Alcoholism and affective disorders: Clinicalcourse of depressive symptoms. AmericanJournal of Psychiatry 152:45-52, 1995.
Brown, S.A., and Schuckit, M.A. Changes indepression among abstinent alcoholics.Journal of Studies on Alcohol 49(5):412-417,
1988.
Bucholz, K.K.; Sheline Y.; and Helzer, J.E. The
epidemiology of alcohol use, problems, anddependence in elders: A review. In:Beresford, T.P, and Gomberg, E., eds. Alcoholand Aging. New York: Oxford UniversityPress, 1995. pp. 19-41.
Butler, R.N. Age-ism: Another form of bigotry.Gerontologist 9:243-246, 1969.
Butler, R.N., and Lewis, M.I. Aging and Mental
Health, 2nd ed. St. Louis: C.V. Mosby, 1977.
Bibliography
Buysse, D.J. III; Monk, T.H.; Berman, S.R.; and
Kupfer, D.J. The Pittsburgh Sleep QualityIndex: A new instrument for psychiatricpractice and research. Psychiatry Research28:193-213, 1988.
Campbell, P.R. Population Projections for States by
Age, Sex, Race, and Hispanic Origin: 1995 to
2025. Washington, DC: U.S. Bureau of theCensus, Population Division, PP1-47, 1996.
Carethers, M. Health promotion in the elderly.American Family Physician 45:2253-2259,
1992.
Carlen, P.L.; McAndrews, M.P.; Weiss, R.T.;
Dongier, M.; Hill, J.M.; Menzano, E.; Farcnik,
K.; Abarbanel, J.; and Eastwood, M.R.Alcohol-related dementia in theinstitutionalized elderly. Alcoholism: Clinical
and Experimental Research 18:1330-1334, 1994.
Carmelli, D.; Heath, A.C.; and Robinette, D.Genetic analysis of drinking behavior inWorld War II veteran twins. GeneticEpidemiology 10:201-213, 1993.
Cartensen, L.L.; Rychtarik, R.G.; and Prue, D.M.Behavioral treatment of the geriatric alocoholabuser: A long-term follow-up study.Addictive Behaviors 10(3):307-311, 1985.
Center for Substance Abuse Treatment. BringingExcellence to Substance Abuse Services in Rural
and Frontier America. Technical AssistancePublication (TAP) Series, Number 20. DHHSPub. No. (SMA) 97-3134. Washington, DC:U.S. Government Printing Office, 1997.
1 6 6 145

Appendix C
Center for Substance Abuse Treatment.
Detoxification from Alcohol and Other Drugs.
Treatment Improvement Protocol (TIP)Series, Number 19. DHHS Pub. No. (SMA)95-3046. Washington, DC: U.S. GovernmentPrinting Office, 1995a.
Center for Substance Abuse Treatment. RuralIssues in Alcohol and Other Drug Abuse
Treatment. Technical Assistance Publication(TAP) Series, Number 10. DHHS Pub. No.(SMA) 96-3099. Washington, DC: U.S.Government Printing Office, 1996.
Center for Substance Abuse Treatment. TreatingAlcohol and Other Drug Abusers in Rural and
Frontier Areas. Technical Assistance
Publication (TAP) Series, Number 17. DHHSPub. No. (SMA) 95-3054. Washington, DC:
U.S. Government Printing Office, 1995b.
Chapman, C.R., and Hill, C.F. Prolongedmorphine self-administration and addictionliability. Cancer 63:1636-1644, 1989.
Chastain, S. The accidental addict. ModernMaturity February/March, 1992.
Chermack, S.T.; Blow, F.C.; Hill, E.M.; and
Mudd S.A. The relationship between alcoholsymptoms and consumption among olderdrinkers. Alcoholism: Clinical and
Experimental Research 20(7):1153-1158, 1996.
Chick, J. Early intervention for hazardousdrinking in the general hospital setting.Australian Drug and Alcohol Review
7(3):339-343, 1988.
Chick, J.; Ritson, B.; Connaughton, J.; and
Stewart, A. Advice versus treatment foralcoholism: A controlled trial. British Journalof Addictions 83:159-170, 1988.
146
Christian, J.C.; Reed, T.; Carmelli, D.; Page, W.F.;
Norton, J.A.; and Breitner, J.C.S. Self-reported alcohol intake and cognition inaging twins. Journal of Studies on Alcohol56 :414-416, 1995.
Ciraulo, D.A.; Shader, R.I.; Greenblatt, D.J.; andCreelman, W. Drug Interactions in Psychiatry,2nd ed. Baltimore: Williams & Wilkins,1995.
Clark, W.D. Alcoholism: Blocks to diagnosisand treatment. American Journal of Medicine71:275-286, 1981.
Closser, M.H., and Blow, F.C. Specialpopulations: Women, ethnic minorities, andthe elderly. Psychiatric Clinics of North
America 16(1):199-209, 1993.
Colsher, P.L., and Wallace, R.B. Elderly menwith histories of heavy drinking: Correlatesand consequences. Journal of Studies on
Alcohol 51:528-535, 1990.
Colsher, P.L.; Wallace, R.B.; Pomrehn, P.R.;
LaCroix, A.Z.; Cornoni-Huntley, J.; Blazer,D.; Scherr, P.A.; Berkman, L.; and
Hennekens, C.H. Demographic and healthcharacteristics of elderly smokers: Resultsfrom established populations forepidemiologic studies of the elderly.American Journal of Preventative Medicine
6:61-70, 1990.
Conwell, Y. Suicide in elderly patients. In:Schneider, L.S.; Reynolds, C.F.; Lebowitz,
B.D.; and Friedhoff, A.J., eds. Diagnosis and
Treatment of Depression in Late Life.
Washington, DC: American PsychiatricPress, 1991. pp. 397-418.
1 6 4

Cook, B.; Winokur, G.; Garvey, M.; and Beach,
V. Depression and previous alcoholism inthe elderly. British Journal of Psychiatry
158:72 -75, 1991.
Cooper, D.B. Alcohol home detoxification: Away found. British Journal of Nursing
4:1315 -1318, 1995.
Cooperstock, R., and Parnell, P. Research onpsychotropic drug use: A review of findingsand methods. Social Science and Medicine
16:1179 -1196, 1982.
Cotton, N.S. The familial incidence ofalcoholism: A review. Journal of Studies of
Alcohol 40:89 -116, 1979.
Cox, J.L. Smoking cessation in the elderlypatient. Clinics in Chest Medicine
14(3):423 -428, 1993.
Culebras, A. Update on disorders of sleep andthe sleepwake cycle. Psychiatric Clinics ofNorth America 15:467 -489, 1992.
Curtis, J.R.; Geller, G.; Stokes, E.J.; Levine, D.M.;
and Moore, R.D. Characteristics, diagnosis,and treatment of alcoholism in elderlypatients. Journal of the American Geriatrics
Society 37:310-316,1989.
Cusack, B.J., and Vestal, R.E. Clinicalpharmacology: Special considerations in theelderly. In: Calkins, E.; Dovin, P.J.; andFord, A.B., eds. Practice of Geriatric Medicine.
Philadelphia: W.B. Saunders, 1986. pp. 115-136.
D'Archangelo, E. Substance abuse in later life.Canadian Family Physician 39:1986-1993,
1993.
Bibliography
Davidson, D.M. Cardiovascular effects ofalcohol. Western Journal of Medicine
151:430 -439, 1989.
DeHart, S.S., and Hoffmann, H.G. Screeningand diagnosis of "alcohol abuse anddependence" in older adults. InternationalJournal of the Addictions 30:1717 -1747, 1995.
Derogatis, L.R. Brief Symptom Inventory (BSI):
Administration, Scoring, and Procedures
Manual, 3rd ed. Minneapolis, MN: NationalComputer Systems, 1994a.
Derogatis, L.R. Symptom Checklist-90-Revised
(SCL-90-R): Administration, Scoring, and
Procedures Manual, 3rd ed. Minneapolis, MN:National Computer Systems, 1994b.
Derogatis, L.R.; and Melisaratos, N. The BriefSymptom Inventory: An introductoryreport. Psychological Medicine 13(3):595-605,
1983.
Dey, A.N. Characteristics of elderly homehealth care users: Data from the 1994National Home and Hospice Care Survey.Advance Data From Vital and Health Statistics,
No. 279. Hyattsville, MD: National Centerfor Health Statistics, 1996.
DiClemente, C.C., and Hughes, S.O. Stages ofchange profiles in alcoholism treatment.Journal of Substance Abuse 2(2):217 -235, 1990.
DiClemente, C.C.; Prochaska, J.0.; FairhurstS.K.; Velicer, W.F.; Velasquez, M.M.; and
Rossi, J.S. The process of smoking cessation:
An analysis of precontemplation,contemplation, and preparation stages ofchange. Journal of Consulting and Clinical
Psychology 59(2):295-304, April 1991.
1, 6 5 147

Appendix C
Dobson, K.S., ed. Handbook of Cognitive
Behavioral Therapies. New York: GuilfordPress, 1988.
Douglass, R.L. Aging and alcohol problems:Opportunities for socioepidemiologicresearch. In: Galanter, M., ed. RecentDevelopments in Alcoholism. New York:
Plenum Press, 1984. pp. 251-266.
Droller, H. Some aspects of alcoholism in theelderly. Lancet 1:137-139,1964.
Dufour, M., and Fuller, R.K. Alcohol in theelderly. Annual Review of Medicine46:123- 132, 1995.
Dufour, M.C.; Archer, L.; and Gordis, E.Alcohol and the elderly. Clinics in GeriatricMedicine 8:127 -141, 1992.
Dunlop. J. Peer groups support seniors fightingalcohol and drugs. Aging 361:28-32,1990.
Dunlop, J.; Skorney, B.; and Hamilton, J. Grouptreatment for elderly alcoholics and theirfamilies. Social Work in Groups 5:87 -92, 1982.
Dupree, L., and Schonfeld, L. Assessment and
Treatment Planning for Alcohol Abusers: A
Curriculum Manual. FMHI Publication Series,Number 109. Tampa: Florida Mental HealthInstitute, University of South Florida, 1986.
Dupree, L.W.; Broskowski, H.; and Schonfeld, L.The Gerontology Alcohol Project: Abehavioral treatment program for elderlyalcohol abusers. Gerontologist 24:510-516,1984.
Dupree, L.W., and Patterson, R. Older adults.In: Hersen, M., and Turner, S.M., eds.Diagnostic Interviewing. New York: PlenumPress, 1985. pp. 337-359.
148
Egan, G. The Skilled Helper: A Problem-
Management Approach to Helping, 5th ed.
Pacific Grove, CA: Brooks/Cole, 1994.
Ensrud, K.E.; Nevitt, M.C.; Yunis, C.; Cauley,
J.A.; Seeley, D.G.; Fox, K.M.; and Cummings,
S.R. Correlates of impaired function in olderwomen. Journal of the American Geriatrics
Society 42:481 -489, 1994.
Ewing, J.A. Detecting alcoholism: The CAGEQuestionnaire. Journal of the American
Medical Association 252:1905 -1907, 1984.
Falvo, D. Effective Patient Education: A Guide to
Increased Compliance, 2nd ed. Gaithersburg,MD: Aspen, 1994.
Falvo, D.R.; Holland, B.; Brenner, J.; and
Benshoff, J.J. Medication use practices in theambulatory elderly. Health Values14(3):10 -16, 1990.
Fillmore, K. Prevalence, incidence, andchronicity of drinking patterns and problemsamong men as a function of age: Alongitudinal cohort analysis. Journal ofAddiction 82:77 -83, 1987.
Finch, J., and Barry, K.L. Substance use in older
adults. In: Fleming, M., and Barry, K., eds.Addictive Disorders. St. Louis, MO:
Mosby/Yearbook Medical Publishers, 1992.pp. 270-286.
Finkel, S.I. Group psychotherapy with olderpeople. Hospital and Community Psychiatry
41:1189-1191,1990.
Finlayson, R.; Hurt, R.; Davis, L.; and Morse, R.
Alcoholism in elderly persons: A study ofthe psychiatric and psychosocial features of216 inpatients. Mayo Clinic Proceedings
63:761-768,1988.
1 (3 6

Finlayson, R.E. Comorbidity in elderlyalcoholics. In: Beresford, T., and Gomberg,E., eds. Alcohol and Aging. New York:
Oxford University Press, 1995a. pp. 56-69.
Finlayson, R.E. Misuse of prescription drugs.International Journal of the Addictions
30(13&14):1871-1901, 1995b.
Finlayson, R.E. Prescription drug abuse in olderpersons. In: Atkinson, R.M., ed. Alcohol andDrug Abuse in Old Age. Washington, DC:
American Psychiatric Press, 1984. pp. 61-70.
Finlayson, R.E., and Hurt, R.D. Medicalconsequences of heavy drinking by theelderly. In: Gomberg, E.; Hedgedus, A.M.;and Zucker, R.A., eds. Alcohol Problems and
Aging. Washington DC: National Instituteon Alcohol Abuse and Alcoholism, in press.
Finlayson, R.E.; Maruta T.; Morse, R.M.; andMartin, M.A. Substance dependence andchronic pain: Experience with treatment andfollow-up results. Pain 26(2):175-180, 1986a.
Finlayson, R.E.; Maruta, T.; Morse, R.M.;Swenson, W.M.; and Martin, M.A. Substancedependence and chronic pain: Profile of 50patients treated in an alcohol and drugdependence unit. Pain 26(2):167-174, 1986b.
Finney, J.W., and Monahan, S.C. The cost-effectiveness of treatment for alcoholism: Asecond approximation. Journal of Studies on
Alcohol 57:229-243, 1996.
Fiore, M.C.; Novotny, T.E.; Pierce, J.P.; Giovino,
G.A.; Hatziandreu, E.J.; Newcomb, P.A.;Surawicz, T.S.; and Davis, R.M. Methodsused to quit smoking in the United States:Do cessation programs help? Journal of theAmerican Medical Association 263:2760-2765.
167
Bibliography
First, M.B.; Spitzer, R.L.; Gibbon, M.; andWilliams, J.B.W. Structured ClinicalInterview for DSM-IV Axis I DisordersPatient Edition (SCID-I/P, Version 2.0). NewYork: Biometrics Research Department, NewYork State Psychiatric Institute, 1996.
Fitzgerald, J.L., and Mulford, H.A. Elderlyversus younger problem drinker "treatment"and recovery experiences. British Journal ofAddiction 87:1281-1291, 1992.
Fleming, A.S.; Buchanan, J.G., Santos, J.F.; andRickards, L.D. Mental Health Services for the
Elderly: Report on a Survey of Community
Mental Health Centers, Vol. I. Washington,
DC: The Action Committee to Implemeritthe Mental Health Recommendations of the1981 White House Conference on Aging,
1984.
Fleming, M., and Barry, K. A three-sample testof a masked alcohol screening questionnaire.Alcohol and Alcoholism 26:81-91, 1991.
Fleming, M.; Barry, K.; and MacDonald, R. TheAlcohol Use Disorders Identification Test incollege sample. International Journal ofAddiction 26:1173-1185, 1991.
Fleming, M.; Barry, K.L.; Adams, W.; Manwell,
L.B.; and Krecker, M. Guiding Older AdultLifestyles (Project GOAL): The effectiveness
of brief physician advice for alcoholproblems in older adults. Manuscriptsubmitted for publication, 1997a.
Fleming, M.F.; Barry, K.L.; Manwell, L.B.;
Johnson, K.; and London, R. Brief physicianadvice for problem alcohol drinkers: Arandomized controlled trial in community-based primary care practices. Journal of the
American Medical Association 277:1039-1045,
1997b.
149

Appendix C
Folstein, M.F.; Folstein, S.E.; and McHugh, P.R.
Mini-Mental State: A practical method forgrading the cognitive state of patients for theclinician. Journal of Psychiatric Research
12:189 -198, 1975.
Forster, L.E.; Follow, R.; and Stoller, E.P.
Alcohol use and potential risk for alcohol-related adverse drug reactions amongcommunity-based elderly. Journal ofCommunity Health 18:225 -239, 1993.
Fortney, J.C.; Booth, B.M.; Blow, F.C.; and Bunn,
J.Y. The effects of travel barriers and age onthe utilization of alcoholism treatment
aftercare. American Journal of Drug and
Alcohol Abuse 21(3):391 -406, 1995.
Fouts, M., and Rachow, J. Choice of hypnoticsin the elderly. P&T News 14(8):1 -4, 1994.
Foy, A.; O'Connell, D.; Henry, D.; Kelly, J.;Cocking, S.; and Halliday, J. Benzodiazepineuse as a cause of cognitive impairment inelderly hospital inpatients. Journal ofGerontology: Biological Sciences and Medical
Sciences 50(2):99 -106, 1995.
Fredriksen, K.I. North of Market: Olderwomen's alcohol outreach program.Gerontologist 32:270-272,1992.
Fuchs, C.S.; Stampfer, M.J.; Colditz, J.A.;
Giovannucci, F.I.; Manson, T.E.; Kawachi,M.B.; Hunter, D.J.; Hankinson, S.E.;
Hennekens, C.H.; Rosner, B.; Spelzer, F.E.;and Willet, W.C. Alcohol consumption andmortality among woman. New EnglandJournal of Medicine 332:1245 -1250, 1995.
150
Gambert, S.R. Substance abuse in the elderly.In: Lowinson, J.H.; Ruiz, P.; and Millman,R.B., eds. Substance Abuse: A Comprehensive
Textbook, 2nd ed. Baltimore: Williams &Wilkins, 1992. pp. 843-851.
Gambert, S.R., and Katsoyannis, K.K. Alcohol-related medical disorders of older heavydrinkers. In: Beresford, T.P., and Gomberg,E., eds. Alcohol and Aging. New York:
Oxford University Press, 1995. pp. 70-81.
Gatz, M., ed. Emerging Issues in Mental Health
and Aging. Washington, DC: AmericanPsychological Association, 1995.
Geller, G.; Levine, D.M.; Mamon, J.A.; Moore,
R.D.; Bone, L.R.; and Stokes, E.J. Knowledge,
attitudes, and reported practices of medicalstudents and house staff regarding thediagnosis and treatment of alcoholism.Journal of the American Medical Association
261:3115-3120,1989.
George, L.K.; Landerman, R.; Blazer, D.G.; and
Anthony, J.C. Cognitive impairment. In:Robins, L.N., and Regier, D.A., eds.Psychiatric Disorders in America: The
Epidemiologic Catchment Area Study. New
York: Free Press, 1991. pp. 291-327.
Glantz, M.D., and Backenheimer, M.S.
Substance abuse among elderly women.Clinical Gerontologist 8(1):3-26,1988.
Glazer, W.M.; Morgenstern, H.; Doucette, J.T.
Predicting the long-term risk of tardivedyskinesia in outpatients maintained onneuroleptic medications. Journal of ClinicalPsychology 54(4):133-139,1993.
168

Goldberg, R.J.; Burchfiel, C.M.; Reed, D.M.;
Wergowske, G.; and Chiu, D. A prospectivestudy of the health effects of alcoholconsumption in middle-aged and elderlymen: The Honolulu Heart Program.Circulation 89:651 -659, 1994.
Gomberg, E.S.L. Drugs, alcohol, and aging. In:Kozlowski, L.T., ed. Research Advances in
Alcohol and Drug Problems. New York:
Plenum Press, 1990. pp. 171-213.
Gomberg, E.S.L. "Elderly alcoholic men andwomen in treatment." Paper presented atthe Research Society on Alcoholism AnnualScientific Meeting, San Diego, California,
1992a.
Gomberg, E.S.L. Medication problems and drugabuse. In: Turner, F.J., ed. Mental Health andthe Elderly. New York: Free Press, 1992b.
pp. 355-374.
Gomberg, E.S.L. Older women and alcohol useand abuse. In: Galanter, M., ed. RecentDevelopments in Alcoholism: Volume 12.
Alcoholism and Women. New York: Plenum
Press, 1995. pp. 61-79.
Gomberg, E.S.L. Overview: Issues of alcoholuse and abuse in the elderly population.Pride Institute Journal of Long Term Health Care
7:4 -17, 1988.
Gomberg, E.S.L. Recent developments inalcoholism: Gender issues. In: Galanter, M.,ed. Recent Developments in Alcoholism:
Volume. 11. New York: Plenum Press, 1993.
pp. 95-107.
Gomberg, E.S.L. Risk factors for drinking over awoman's life span. Alcohol Health andResearch World 18:220 -227, 1994.
Bibliography
Goodman, A.C.; Holder, H.D.; and Nishiura, E.Alcoholism treatment offset effects: A costmodel. Inquiry 28:168 -178, 1991.
Goodwin, D.W. Family studies on alcoholism.Journal of Studies of Alcohol 42:156 -162, 1981.
Goodwin, D.W., and Warnock, L.K. Alcoholism:A family disease. In: Grances, R.G., andMiller, S.L., eds. Clinical Textbook of Addictive
Diseases. New York: Guiliford, 1991. pp.
458-500.
Gordon, T., and Kamel, W.B. Drinking and itsrelation to smoking, blood pressure, bloodlipids, and uric acid. Archives of Internal
Medicine 143:1366 -1374, 1983.
Graham, K.; Carver, V.; and Brett, P.J. Alcoholand drug use by older women: Results of anational survey. Canadian Journal of Aging
14(4):769 -791, 1995a.
Graham, K.; Clarke, D.; Bois, C.; Carver, V.;
Dolenki, L.; Smythe, C.; Harrison, S.;
Marshenan, J.; and Brett, P. Addictivebehavior of older adults. Addictive Behaviors
21(3):331-348,1996.
Graham, K.; Saunders, S.J.; Flower, M.C.;
Timney, C.B.; White-Campbell, M.; and
Pietropaolo, A.Z. Addictions Treatment forOlder Adults: Evaluation of an Innovative
Client-Centered Approach. New York:
Haworth Press, 1995b.
Grant, I. Alcohol and the brain:Neuropsychological correlates. Journal ofConsulting and Clinical Psychology 55:310-324,
1987.
169 151

Appendix C
Grant, I.; Adams, K.; and Reed, R. Aging,
abstinence, and medical risk factors in theprediction of neuropsychologic deficit
among long-term alcoholics. Archives ofGeneral Psychiatry 41:710-718, 1984.
Gronbaek, M.; Deis, A.; Sorensen, T.I.; Becker,
U.; Borch-Johnsen, K.; Muller, C.; Schnohr,P.; and Jensen, G. Influence of sex, age, bodymass index, and smoking on alcohol intakeand mortality. British Medical Journal308:302-306, 1994.
Gurnack, A.M. Older Adults' Misuse of Alcohol,
Medicines, and Other Drugs. New York:Springer, 1997.
Guttmann, D. A Study of Legal Drug Use by Older
Americans. Department of Health, Education,and Welfare Publication No. (ADM) 79-495.
Washington, DC: Government PrintingOffice, 1977.
Haponik, E.F. Sleep disturbances of olderpersons: Physicians' attitudes. Sleep15(2):168-172, 1992.
Harris, KB., and Miller, W.R. Behavioural self-control training for problem drinkers:Components of efficacy. Psychology of
Addictive Behaviour 4(2):90-92, 1990.
Hayakawa, K.; Kumagai, H.; Suzuki, Y.;
Furusaw, N.; Haga, T.; Hoshi, T.; Fujiwara,Y.; and Yamaguchi, K. MR imaging ofchronic alcoholism. Acta Radiologica33:201-206, 1992.
Hazelden Foundation. How To Talk to an OlderPerson Who Has a Problem With Alcohol or
Medications. Center City, MN: HazeldenFoundation, 1991.
152
Health Care Financing Administration. Medicareand Medicaid Program Manual: Publication 11.
Home Health Agency Manual: Health Insurancefor the Aged.
http: / / www.hcfa.gov /pubforms/progman.
htm [Accessed November 5, 1997; updatedSeptember 17, 1997].
Heather, N. Interpreting the evidence on briefinterventions for excessive drinkers: Theneed for caution. Alcohol and Alcoholism
30:287-296, 1995.
Heather, N.; Campion, P.D.; Neville, R.G.; andMacCabe, D. Evaluation of a controlleddrinking minimal intervention for problemdrinkers in general practice (the DRAMSscheme). Journal of the Royal College for the
General Practitioner 37(301):358-363, 1987.
Heather, N., and Tebbutt, J. Definitions ofnonabstinent and abstinent categories inalcoholism treatment outcome classifications:A review and proposal. Drug and AlcoholDependence 24:83-93, 1989.
1 7 0
Heller, D.A., and McClearn, G.E. Alcohol,aging, and genetics. In: Beresford, T.P, andGomberg, E., eds. Alcohol and Aging. New
York: Oxford University Press, 1995. pp.99-114.
Helzer, J.E.; Bucholz, K.; and Robins, L.N. Five
communities in the United States: Results ofthe Epidemiologic Catchment Area Survey.In: Helzer, J.E., and Canino, G.J., eds.
Alcoholism in North America, Europe, and Asia.
New York: Oxford University Press, 1991a.pp. 71-95.

Helzer, J.E.; Burnam, A.; and McEvoy, L.T.
Alcohol abuse and dependence. In: Robins,L.N., and Reigier, D.A., eds. PsychiatricDisorders in America: The Epidemiologic
Catchment Area Study. New York: Free Press,
1991b. pp. 81-115.
Hendricks, J.; Johnson, T.P.; Sheahan, S.L.; and
Coons, S.J. Medication use among olderpersons in congregate living facilities.Journal of Geriatric Drug Therapy 6(1):47-61,
1991.
Hendrie, H.C.; Gao, S.; Hall, K.S.; Hui, S.L.; and
Unversagt, F.W. The relationship betweenalcohol consumption, cognitive performance,and daily functioning in an urban sample ofolder Black Americans. Journal of the
American Geriatrics Society 44:1158-1165,
1996.
Herings, R.M.; Stricker, B.H.; de Boer, A.;
Bakker, A.; and Sturmans, F.Benzodiazepines and the risk of fallingleading to femur fractures: Dosage moreimportant than elimination half-life. Archivesof Internal Medicine 155(16):1801- 1807, 1995.
Higuchi, S., and Kono, H. Early diagnosis andtreatment of alcoholism: The Japaneseexperience. Alcohol and Alcoholism
29:363-373,1994.
Hill, H.F., and Chapman, C.R. Clinicaleffectiveness of analgesics in chronic painstates. In: NIDA Research MonographSeries, Number 95. Rockville, MD: NationalInstitute on Drug Abuse, 1989. pp. 102-109.
Bibliography
Hodgson, R., and Rollrtick, S. How briefintervention works: Representative cases asviewed by the health advisers. In: Babor,T.F., and Grant, M., eds. Project on
Identification and Management of Alcohol-
Related Problems: Report on Phase II. A
Randomized Clinical Trial of Brief Interventions
in Primary Health Care. Geneva, Switzerland:World Health Organization, 1992. pp. 221-232.
Holder, H.; Boyd, G.; Howard, J.; Flay, B.; Voas,
R.; and Grossman, M. Alcohol-problemprevention research policy: The need for aphases research model. Journal of PublicHealth Policy 16:324-346,1995.
Holder, H.D. Alcoholism treatment andpotential health care cost saving. MedicalCare 25:52 -71, 1987.
Holder, H.D., and Blose, J.O. Alcoholismtreatment and total health care utilizationand costs: A four year longitudinal analysisof federal employees. Journal of the American
Medical Association 256:1456 -1460, 1986.
Holder, H.D., and Blose, J.O. The reduction ofhealth care costs associated with alcoholismtreatment: A 14 year longitudinal study.Journal of Studies on Alcohol 53:293 -302, 1992.
Holder, H.D.; Longabaugh, R.; Miller, W.R.; and
Rubonis, A.V. The cost-effectiveness oftreatment for alcoholism: A firstapproximation. Journal of Studies on Alcohol
52:517-540,1991.
171 153

Appendix C
Holzer, C.E., III; Robins, L.N.; Myers, J.K.;
Weissman, M.M.; Tisch ler, G.L.; Leaf, P.J.;
Anthony, J.; and Bednarski, P.B. Antecedentsand correlates of alcohol abuse anddependence in the elderly. Maddox, G.L.;Robins, L.N.; and Rosenberg, N., eds. Natureand Extent of Alcohol Problems Among the
Elderly. NIAAA Research Monograph Series,Number 14. DHHS Pub. No. (ADM) 84-1321.Rockville, MD: National Institute on AlcoholAbuse and Alcoholism, 1984. pp. 217-244.
Hrubec, Z., and Omenn, G. Evidence of geneticpredisposition to alcoholic cirrhosis andpsychosis: Twin concordance for alcoholismand its end points by zygosity among maleveterans. Alcoholism 5:207 -215, 1981.
Hull, R. Incidence of selected language, speechand hearing disorders among the elderly. In:Hull, R., and Griffin, K.M., eds.
Communication Disorders in Aging. NewburyPark, CA: Sage, 1989.
Hurt, R.D.; Eberman, K.A.; Slade, J.; and KaramL. Treating nicotine addiction in patientswith other addictive disorders. In: Orleans,C.T., and Slade, J., eds. Nicotine Addiction:
Principles and Management. New York:
Oxford University Press, 1993. pp. 310-326.
Hurt, R.D.; Finlayson, R.E.; Morse, R.M.; andDavis, L.J. Alcoholism in elderly persons:Medical aspects and prognosis of 216patients. Mayo Clinic Proceedings 63:753-760,1988.
Inouye, S.K.; Van Dyck, C.H.; Balkin, S.; Seigal
A.P.; and Horowitz, R.J. Clarifyingconfusion: The Confusion Assessment
Method. A new method for the detection ofdelerium. Annals of Internal Medicine
113:941-948,1990.
172154
Institute of Medicine. Broadening the Base ofTreatment for Alcohol Problems. Washington,
DC: National Academy Press, 1990.
Institute of Medicine. Federal Regulation of
Methadone Treatment. Rettig, R., andYarmolinsky, A., eds. Washington, DC:National Academy Press, 1995.
Janik, S., and Dunham, R. A nationwideexamination of the need for specific
alcoholism treatment programs for theelderly. Journal of Studies on Alcohol
44:307-317,1983.
Jarvik, M.E., and Schneider, N.G. Nicotine. In:Lowinson, J.H.; Ruiz, P.; and Millman, R.B.,eds. Substance Abuse: A Comprehensive
Textbook. Baltimore: Williams & Wilkins,1992. pp. 334-356.
Jinks, M.J., and Raschko, R.R. A profile of
alcohol and prescription drug abuse in ahigh-risk community-based elderlypopulation. Drug Intelligence and ClinicalPharmacy 24:971 -975, 1990.
Johnson, V.E. I'll Quit Tomorrow. New York:Harper and Row, 1973.
Joseph, C.L. Alcohol and drug misuse in thenursing home. International Journal of theAddictions 30(13&14):1953-1983,1995.
Joseph, C.L.; Ganzini, L.; and Atkinson, R.
Screening for alcohol use disorders in thenursing home. Journal of the American
Geriatrics Society 43:368 -373, 1995.
Joseph, C.L.; Rasmussen, J.; Ganzini, L.; and
Atkinson, R.M. Outcome of nursing homecare for residents with alcohol use disorders.International Journal of Geriatric Psychiatry
12(7):767 -772, 1997.

Kahan, M.; Wilson, L.; and Becker, L.
Effectiveness of physician-basedinterventions with problem drinkers:review. Canadian Medical Journal
152(6):851-856,1995.
Bibliography
Klatsky, A.L.; Armstrong, M.A.; and Friedman,G.D. Risk of cardiovascular mortality in
A alcohol drinkers, ex-drinkers, and non-drinkers. American Journal of Cardiology
66:1237 -1242, 1990.
Kashner, T.M.; Rodell, D.E.; Ogden, S.R.;Guggenheim, F.G.; and Karson, C.N.Outcomes and costs of two VA inpatientprograms for older alcoholic patients.Hospital and Community Psychiatry
43:985-989,1992.
Kaslow, F., and Robison, J.A. Long-termsatisfying marriages: Perceptions ofcontributing factors. American Journal of
Family Therapy 24:153-170,1996.
Katzman, R.; Brown, T.; Fuld, P.; Peck, A.;Schechter, R.; and Schimmel, H. Validation
of a short OrientationMemoryConcentration Test of cognitive impairment.American Journal of Psychiatry 140(6):734-739,
1983.
Keeler, E.B.; Solomon, D.H.; Beck, J.C.;
Mendenhall, R.C.; and Kane, R.L. Effect of
patient age on duration of medicalencounters with physicians. Medical Care20:1101 -1108, 1982.
Kiernan, R.J.; Mueller, J.; Langston, J.W.; and
Van Dyke, C. The NeurobehavioralCognitive Status Examination: A brief butdifferentiated approach to cognitiveassessment. Annals of Internal Medicine
107:481 -485, 1987.
King, M.B. Alcohol abuse and dementia.International Journal of Geriatric Psychiatry
1:31 -36, 1986.
X73
Knegtering, H.; Eijck, M.; and Huijsman, A.Effects of antidepressants on cognitivefunctioning of elderly patients: A review.Drugs and Aging 5(3):192- 199, 1994.
Koenig, H.G, and Blazer, D.G., II. Depression.In: Birren, J.E., ed. Encyclopedia of
Gerontology: Age, Aging, and the Aged. Vol. I.
San Diego, CA: Academic Press, 1996. pp.
415-428.
Kofoed, L.L.; Tolson, R.L.; Atkinson, R.M.; Toth,
R.L.; and Turner, J.A. Treatment complianceof older alcoholics: An elder-specificapproach is superior to "mainstreaming."Journal of Studies on Alcohol 48:47-51,1987.
Korrapati, M.R., and Vestal, R.E. Alcohol andmedicaitons in the elderly: Complexinteractions. In: Beresford, T.P., andGomberg, E., eds. Alcohol and Aging. NewYork: Oxford University Press, 1995. pp.
42-69.
Kovar, M. Health of the elderly and use ofhealth services. Public Health Reports
92:9-19,1977.
Kranzler, H.R.; Babor, T.F.; and Lauerman, R.J.Problems associated with average alcoholconsumption and frequency of intoxicationin a medical population. Alcoholism: Clinicaland Experimental Research 14:119 -126, 1990.
155

Appendix C
Kristenson, H.; Oh lin, H.; Hulten- Nosslin, M.B.;
Trell, E.; and Hood, B. Identification and
intervention of heavy drinking in middle-aged men: Results and follow-up of 24-60months of long-term study with randomizedcontrols. Alcoholism: Clinical and
Experimental Research 7(2):203-209, 1983.
LaCroix, A.Z.; Guralnik, J.M.; Berkman, L.F.;
Wallace, R.B.; and Satterfield, S. Maintainingmobility in late life: Smoking, alcohol
consumption, physical activity, and bodymass index. American Journal of Epidemiology
137:858-869, 1993.
Lapane, K.L.; Zierler, S.; Lasater, T.M.; Barbour,
M.M.; Carleton, R.; and Hume, A.L. Is theuse of psychotropic drugs associated withincreased risk of ischemic heart disease?Epidemiology 6(4):376-381, 1995.
Lawton, M.P., and Brody, E.M. Assessment ofolder people: Self-maintaining andinstrumental activities of daily living.Gerontologist 9:179-188, 1969.
Lebowitz, B.D. Correlates of success incommunity mental health programs for theelderly. Hospital and Community Psychiatry39:721-722, 1988.
Lebowitz, B.D.; Light, E.; and Bailey F. Mental
health center services for the elderly: Theimpact of coordination with area agencies onaging. Gerontologist 27(6):699-702, December1987.
Lehman, A.F. A quality of life interview for thechronically mentally ill. Evaluation and
Program Planning 11:51-62, 1988.
156 174
Leveille, S.G.; Buchner, D.M.; Koespell, T.D.;
McCloskey, L.W.; Wolf, M.E.; and Wagner,
E.H. Psychoactive medications and injuriousmotor vehicle collisions involving older
drivers. Epidemiology 5(6):591-598, 1994.
Liberto, J.G., and Oslin, D.W. Early versus lateonset of alcoholism in the elderly.International Journal of the Addictions
30:1799-1818, 1995.
Liberto, J.G.; Oslin, D.W.; and Ruskin, P.E.
Alcoholism in older persons: A review of theliterature. Hospital and Community Psychiatry43(10):975-984, 1992.
Light, E.; Lebowitz, B.D.; and Bailey, F.
CMHC's and elderly services: An analysis ofdirect and indirect services. CommunityMental Health Journal 22(4):294-302, 1986.
Linn, M.W. Attrition of older alcoholics fromtreatment. Addictive Diseases: An
International Journal 3:437-447, 1978.
Liskow, B.I.; Rinck, C.; Campbell, J.; and
DeSouza, C. Alcohol withdrawal in theelderly. Journal of Studies on Alcohol
50:414-421, 1989.
Litten, R.Z.; Allen, J.; and Fertig, J.
Pharmacotherapies for alcohol problems: Areview of research with focus ondevelopments since 1991. Alcoholism:
Clinical and Experimental Research 20:859-876,1996.
Lord, S.R.; Antsey, K.J.; Williams, P.; and Ward,
J.A. Psychoactive medication use, sensori-motor function and falls in older women.British Journal of Clinical Pharmacology
39(3):227-234, 1995.

Maisto, S.A.; McKay, J.R.; and Connors, J.J. Self-
report issues in substance abuse: State of theart and future directions. BehavioralAssessment 12(1):117 -134, 1990.
Mammo, A., and Weinbaum, D.F. Some factorsthat influence dropping out from outpatientalcoholism treatment facilities. Journal ofStudies on Alcohol 54:92 -101, 1993.
Manheimer, D.I.; Davidson, S.T.; Baiter, M.B.;
Mellinger, G.D.; Cisin, I.H.; and Parry, H.J.Popular attitudes and beliefs abouttranquilizers. American Journal of Psychiatry
130(11):1246 -1253, 1973.
McCrady, B.S., and Langenbucher, J.W.Alcoholism treatment and health care systemreform. Archives of General Psychiatry
53:737 -746, 1996.
McHorney, C.A.; Ware, J.E.; Lu, J.F.R.; andSherbourne, C.D. The MOS 36-Item Short-Form Health Survey (SF-36): III. Tests ofdata quality, scaling assumptions, andreliability across diverse patient groups.Medical Care 32:40 -66, 1994.
McHorney, C.A.; Ware, J.E.; and Raczek, A.E.
The MOS 36-Item Short-Form Health Survey(SF-36): II. Psychometric and clinical tests ofvalidity of measuring physical and mentalhealth constructs. Medical Care 31:247-263,
1993.
McInnes, E., and Powell, J. Drug and alcoholreferrals: Are elderly substance abusediagnoses and referrals being missed? BritishJournal of Medicine 308:444 446,1994.
Bibliography
McLellan, A.T., and Duren, J. Outcomeevaluation in psychiatric and substanceabuse treatments: Concepts, rationale, andmethods. In: Sederer, L., and Dickey, B.,eds. Outcomes Assessment in Clinical Practice.
Baltimore, MD: Williams & Wilkins, 1996.
pp. 34-44.
McLellan, A.T.; Luborsky, L.; Cacciola, J.; and
Griffith, J. New data from the addictionseverity index: Reliability and validity inthree centers. Journal of Nervous Disease
173:412-423,1985.
McLellan, A.T.; Luborsky, L.; O'Brien, C.P.; and
Woody, G.E. An improved diagnosticinstrument for substance abuse patients: Theaddiction severity index. Journal of Nervousand Mental Disorders 168:26 -33, 1990.
McLellan, A.T.; O'Brien, C.P.; Metzger, D.;Alterman, A.I.; Cornish, J.; and Urschel, H.How effective is substance abuse treatmentcompared to what? In: O'Brien, C.P., andJaffee, J., eds. Advances in Understanding the
Addictive States. New York: Raven Press,
1992. pp. 231-252.
Meichenbaum, D., and Turk, D. FacilitatingTreatment Adherence: A Practitioner's
Guidebook. New York: Plenum Press, 1987.
Mellinger, G.D.; Baiter, M.B.; and Uhlenhuth,E.H. Prevalence and correlates of the long-term use of anxiolytics. Journal of theAmerican Medical Association 251:375-379,
1985.
Mertens, J.R.; Moos, R.H.; and Brennan, P.L.Alcohol consumption, life context, andcoping predict mortality among late-middle-aged drinkers. Alcoholism: Clinical andExperimental Research 20:313 -319, 1996.
1 7 5157

Appendix C
Miller, F.; Whitcup, S.; Sacks, M.; and Lynch,
P.E. Unrecognized drug dependence andwithdrawal in the elderly. Drug and AlcoholDependence 15:177, 1985.
Miller, W.R., and Hester, R.K. Inpatientalcoholism treatment: Who benefits?American Psychologist 41:794-805, 1986.
Miller, W.R., and Munoz, R.F. How To Control
Your Drinking. Englewood Cliffs, NJ:Prentice-Hall, 1976.
Miller, W.R., and Rollnick, S. Motivational
Interviewing. New York: Guilford Press,1991.
Miller, W.R., and Sanchez, V.C. Motivatingyoung adults for treatment and lifestylechange. In: Howard, G.S., and Nathan, P.E.Alcohol Use and Misuse by Young Adults.
South Bend, IN: University of Notre DamePress, 1994.
Miller, W.R., and Taylor, C.A. Relative
effectiveness of bibliotherapy, individual andgroup self-control training in the treatment ofproblem drinkers. Addictive Behaviors5:13-24, 1980.
Miller, W.R.; Tonigan, J.S.; and Longabaugh, R.The Drinker Inventory of Consequences (Drinc).
National Institute on Alcohol Abuse andAlcoholism Project MATCH MonographSeries, Volume 4. NIH Pub. No. 95-3911.Washington, DC: U.S. Government PrintingOffice, 1995.
Minnis, J. Toward an understanding of alcoholabuse among the elderly: A sociologicalperspective. Journal of Alcohol and DrugEducation 33(3):32-40, 1988.
158
Moeller, F.G.; Gillin, J.C.; Irwin, M.; Golshan, S.;
Kripke, D.F.; and Schuckit, M. A comparisonof sleep EEGs in patients with primary majordepression and major depression secondaryto alcoholism. Journal of Affective Disorders27:39-42, 1993.
Moore, R., and Pearson, T. Moderate alcohol
consumption and coronary artery disease: Areview. Medicine 65:242-267, 1986.
Moore, R.D.; Bone, L.R.; Geller, G.; Mamon, J.A.;Stokes; E.J.; and Levine, D.M. Prevention,
detection and treatment of alcoholism inhospitalized patients. Journal of the AmericanMedical Association 261:403-407, 1989.
Moos, R.H.; Brennan, P.L.; and Moos, B.S.
Short-term processes of remission andnonremission among late-life problemdrinkers. Alcoholism: Clinical andExperimental Research 15:948-955, 1991.
Moos, R.H.; Mertens, J.R.; and Brennan, P.L.
Patterns of diagnosis and treatment amonglate-middle-aged and older substance abusepatients. journal of Studies on Alcohol54:479-488, 1993.
Mullan, E.; Katona, C.; and Bellew, M. Patternsof sleep disorders and sedative hypnotic usein seniors. Drugs and Aging 5(1):49-58, 1994.
Myers, J.E. Adult Children and Aging Parents.
Alexandria, VA: American CounselingAssociation, 1989.
Myers, J.E., and Schwiebert, V. Competencies for
Gerontological Counseling. Alexandria, VA:
American Counseling Association, 1996.
17 (i

Myers, J.K.; Weissman, M.M.; Tisch ler, G.L.;
Holzer, C.E., III; Leaf, P.J.; Orvaschel, H.;
Anthony, J.C.; Boyd, J.H.; Burke, J.D., Jr.;
Kramer, M.; and Stolzman, R. Six-monthprevalence of psychiatric disorders in threecommunities: 1980-1982. Archives of General
Psychiatry 41:959, 1984.
National Center for Health Statistics. Cigarettesmoking among adultsUnited States, 1994.Morbidity and Mortality Weekly Report
45(27):588 -590, 1996.
National Institute on Alcohol Abuse andAlcoholism. Alcohol and aging. Alcohol
Alert 2:1 -5, 1988.
National Institute on Alcohol Abuse andAlcoholism. The Physicians' Guide to Helping
Patients With Alcohol Problems. NIH Pub. No.
95-3769. Rockville, MD: National Instituteon Alcohol Abuse and Alcoholism, 1995.
National Institutes of Health. ConsensusDevelopment Conference Statement.Diagnosis and Treatment of Depression in Late
Life 9(3):1-27,1991.
National Institutes of Health. ConsensusDevelopment Conference Statement. TheTreatment of Sleep Disorders in Older People
8(3):1 -22, 1990.
Nitcher, R.L.; Burke, W.J.; Roccaforte, W.H.; and
Wengel, S.P. A collateral source version of
the geriatric depression rating scale.American Journal of Geriatric Psychiatry
1:143 -152, 1993.
Oppenheimer, C., ed. Psychiatry in the Elderly,2nd ed. New York: Oxford University Press,1997. pp. 661-686.
Bibliography
Orleans, C.T.; Jepson, C.; Resch, N.; and Rimer,B.K. Quitting motives and barriers amongolder smokers. Cancer 74:2055 -2061, 1994a.
Orleans, C.T.; Resch, N.; Noll, E.; Keintz, M.K.;
Rimer, B.K.; Brown, T.V.; and Snedden, T.M.
Use of transdermal nicotine in a state-levelprescription plan for the elderly. Journal ofthe American Medical Association 271:601-607,
1994b.
Oslin, D.; Liberto, J.G.; O'Brien, J.; Krois, S.; and
Norbeck, J. Naltrexone as an adjunctivetreatment for older patients with alcoholdependence. American Journal of Geriatric
Psychiatry 5:324 -332, 1997.
Oslin, D.W, and Liberto, J.G. Substance abuse inthe elderly. In: Wilner, P., ed. Psychiatry.Philadelphia: J.B. Lippincott, 1995.
Oslin, D.W.; Pettinati, H.; Volpicelli, J.R.; and
Katz, I.R. "Enhancing treatment compliancein elderly alcoholics: A new psychosocialintervention model." Paper presented at theannual meeting of the Gerontologic Societyof America, Washington, DC, November
1997.
Osterling, A., and Berglund, M. Elderly firsttime admitted alcoholics: A descriptivestudy on gender differences in a clinicalpopulation. Alcoholism: Clinical andExperimental Research 18:1317 -1321, 1994.
Ostrom, J.R.; Hammarlund, E.R.; Kristenson,D.B.; Plein, J.B.; and Kethley, A.B.
Medication usage in an elderly population.Medical Care 23:157 -164, 1985.
177 159

Appendix C
Parker, D.A.; Parker, E.S.; Brody, J.A.; and
Schoenberg, R. Alcohol use and cognitiveloss among employed men and women.American Journal of Public Health 73:521-526,1983.
Patterson, R.L., and Dupree, L. Older adults. In:Hersen, M., and Turner, S., eds. DiagnosticInterviewing, 2nd ed. New York: PlenumPress, 1994. pp. 373-397.
Peele, S. Research issues in assessing addictiontreatment efficacy: How cost effective areAlcoholics Anonymous and privatetreatment centers? Drug and AlcoholDependency 25:179-182,1990.
Persson, J., and Magnusson, P.H. Earlyintervention in patients with excessiveconsumption of alcohol: A controlled study.Alcohol 6(5):403-408,1989.
Pfefferbaum, A.; Lim, K.; Zipursky, R.;
Mathalon, D.H.; Rosenbloom, M.J.; Lane, B.;
Ha, C.N.; and Sullivan, E.V. Brain gray andwhite matter volume loss accelerates withaging in chronic alcoholics: A quantitativeMRI study. Alcoholism: Clinical and
Experimental Research 16:1078 -1089, 1992.
Piland, B. The aging process and psychoactivedrug use in clinical treatment. In: The AgingProcess and Psychoactive Drug Use. NationalInstitute on Drug Abuse Services Research
Monograph. Department of Health,Education, and Welfare Pub. No. (ADM) 79-813. Washington, DC: U.S. GovernmentPrinting Office, 1979. pp. 1-16.
Plomp, R. Auditory handicap of hearingimpairment and the limited benefit ofhearing aids. Journal of the Acoustic Society ofAmerica 63:533-549,1978.
160
Pollock, V.; Schneider, L.; Zemansky, M.;
Gleason, R.; and Pawluczyk, S. Topographicquantitative EEG amplitude in recoveredalcoholics. Psychiatry Research: Neuroimaging45:25 -32, 1992.
Pomara, N.; Stanley, B.; Block R.; Berchou, R.C.;Stanley, M.; Greenblatt, D.J.; Newton, R.E.;and Gershon, S. Increased sensitivity of theelderly to the central depressant effects ofdiazepam. Journal of Clinical Psychiatry46:185 -187, 1985.
Portenoy, R.K. Therapeutic use of opioids:Prescribing and control issues. In: CooperJ.R.; Czechowicz D.J.; Molinari S.P.; Petersen,R.C., eds. Impact of Prescription Drug
Diversion Control Systems on Medical Practice
and Patient Care. NIDA Research MonographSeries, Number 131. NIH Pub. No. 93-3507.Washington, DC: U.S. Government PrintingOffice, 1993. pp. 35-50.
Powers, R.B., and Osborne, J.G. Fundamentals ofBehavior. New York: West Publishing Co.,1976.
Prentice, R. Patterns of psychoactive drug useamong the elderly. In: The Aging Process andPsychoactive Drug Use. National Institute onDrug Abuse Services Research Monograph.DHEW Pub. No. (ADM) 79-813.
Washington, DC: U.S. Government PrintingOffice, 1979. pp. 17-41.
Prochaska, J., and DiClemente, C. Toward acomprehensive model of change. In: Miller,W.R., and Heather, N., eds. Treating
Addictive Behaviors: Processes of Change. NewYork: Plenum Press, 1986, pp. 3-27.
178

Prochaska, J.O., and DiClemente, C.C. Processesand stages of change in smoking, weightcontrol, and psychological distress. In:Schiffman, S., and Wills, T., eds. Coping and
Substance Abuse. New York: Academic
Press, 1985, pp. 319-245.
Prochaska, J.O.; DiClemente, C.C.; and Norcross,
J.C. In search of how people change:Applications to addictive behaviors.American Psychologist 47(9):1102- 1114, 1992.
Radloff, L.S. The CES-D Scale: A new self-report depression scale for research in the
general population. Applied Psychological
Measurement 1:385-401,1977.
Rains, V., and Ditzler, T. Alcohol use disordersin cognitively impaired patients referred forgeriatric assessment. Journal of Addictive
Diseases 12:55-64,1993.
Raschko, R. "Gatekeepers" do the casefindingin Spokane. Aging 361:38-40,1990.
Ray, W.A. Psychotropic drugs and injuriesamong the elderly: A review. Journalof
Clinical Psychopharmacology 12:386-396,1992.
Ray, W.A.; Thapa, P.B.; and Shorr, R.I.Medications and the older driver. Clinics inGeriatric Medicine 9(2):413-438,1993.
Regier, D.A.; Boyd, J.H.; Burke, J.D., Jr.; Rae,
D.S.; Myers, J.K.; Kramer, M.; Robins, L.N.;
George, L.K.; Karns, M.; and Locke, B.Z. Onemonth prevalence of mental disorders in theUnited States: Based on five EpidemiologicalCatchment Area sites. Archives of General
Psychiatry 45:977 -986, 1988.
Bibliography
Regier, D.A.; Farmer, M.E.; Rae, D.S.; Locke,
B.Z.; Keith, S.J.; Judd, L.L.; and Goodwin,
F.K. Comorbidity of mental disorders withalcohol and other drug abuse. Journal of theAmerican Medical Association
264(19):2511-2518,1990.
Reich, T.; Cloninger, C.R.; Van Eerdewegh, P.;
Rice, J.P.; and Mullaney, J. Secular trends inthe familial transmission of alcoholism.Alcoholism: Clinical and Experimental Research
12:458-464,1988.
Rice, C.; Longabaugh, R.; Beattie, M.; and Noel,
N. Age group differences in response totreatment for problematic alcohol use.Addiction 88:1369 -1375, 1993.
Rickels, K., and Schweizer, E. Anxiolytics:Indications, benefits, and risks of short- andlong-term benzodiazepine therapy: Currentresearch data. In: Cooper, J.R.; Czechowicz,D.J.; Molinari, S.P.; and Petersen, R.C., eds.
Impact of Prescription Drug Diversion Control
Systems on Medical Practice and Patient Care.
NIDA Research Monograph Series, Number131. NIH Pub. No. 93-3507. Washington,DC: U.S. Government Printing Office,1993.
pp. 51-67.
Rimer, B.K. and Orleans, C.T. Tailoringsmoking cessation for older adults. Cancer
74:2051-2054,1994.
Robins, L.N.; Helzer, J.E.; Croughan, J.; andRatcliffe, K.S. National Institute of MentalHealth Diagnostic Interview Schedule: Itshistory, characteristics, and validity. Archives
of General Psychiatry 38:381-389,1981.
Rodrigo, E.K.; King, M.B.; and Williams, P.
Health of long term benzodiazepine users.British Medical Journal (Clinical Research
Edition) 296:603-606,1988.
179 161

Appendix C
Rosin, A.J., and Glatt, M.M. Alcohol excess inthe elderly. Quarterly Journal of Studies on
Alcohol 32:53 -59, 1971.
Roy, W., and Griffin, M. Prescribed medicationsand the risk of falling. Topics in Geriatric
Rehabilitation 5(20):12-20,1990.
Roy-Byrne, P.P., and Hommer, D.
Benzodiazepine withdrawal: Overview andimplications for the treatment of anxiety.American Journal of Medicine 84:1041-1052,1988.
Ruthazer, R., and Lipsitz, L.A. Antidepressants
and falls among elderly people in long-termcare. American Journal of Public Health
83(5):746-749,1993.
Salive, M.E.; Cornoni-Huntley, J.; LaCroix, A.Z.;Ostfield, A.M.; Wallace, R.B.; and
Hennekens, C.H. Predictors of smokingcessation and relapse in older adults.American Journal of Public Health
82(9):1268 -1271, 1992.
Salthouse, T.A. Speed of behavior and itsimplications for cognition. In: Birren. J.E.,and Schaie, K.W., eds. Handbook of the
Psychology of Aging. New York: Van
Nostrand and Reinhold, 1985. pp. 400-426.
Salzman, C. (Task Force Chair). Benzodiazepine
Dependence, Toxicity, and Abuse: A Task Force
Report of the American Psychiatric Association.
Washington, DC: American Psychiatric Press,1990.
Salzman, C. Benzodiazepine treatment of panicand agoraphobia syndromes: Use,dependence, toxicity, abuse. Journal ofPsychiatric Research 27:97 -110, 1993a.
Salzman, C. Issues and controversies regardingbenzodiazepine use. In: Cooper, J.R.;Czechowicz, D.J.; Molinari, S.P.; andPetersen, R.C., eds. Impact of Prescription
Drug Diversion Control Systems on Medical
Practice and Patient Care. NIDA Research
Monograph Series, Number 131. NIH Pub.No. 93-3507. Washington, DC: U.S.Government Printing Office, 1993b. pp.68-88.
Sanchez-Craig, M.; Neumann, B.; Souza-Formigoni, M.; and Rieck, L. Brief treatmentfor alcohol dependence: Level ofdependence and treatment outcome. Alcoholand Alcoholism Supplement 1:515-518,1991.
Saunders, J.B.; Aasland, 0.G.; Babor, T.F.; de laFuente, J.R.; and Grant, M. Development ofthe Alcohol Use Disorders Identification Test(AUDIT): WHO collaborative project onearly detection of persons with harmfulalcohol consumptionII. Addiction88:791-804,1993.
Saunders, P.A. Epidemiology of alcoholproblems and drinking patterns. In: John,R.M.; Copeland, M.T.; Aboou-Saleh, M.T.;
and Blazer, D.G., eds. Principles and Practice
of Geriatric Psychiatry. New York: Wiley,1994. pp. 801-805.
Saunders, P.A.; Copeland, J.R.; Dewey, M.E.;
Davidson, I.A.; McWilliam, C.; Sharma, V.;
and Sullivan, C. Heavy drinking as a riskfactor for depression and dementia in elderlymen: Findings from the Liverpool
Longitudinal Community Study. BritishJournal of Psychiatry 159:213 -216, 1991.
162 1U 0

Scherr, P.A.; LaCroix, A.Z.; Wallace, R.B.;
Berkman, L.; Curb, J.D.; Cornoni-Huntley, J.;Evans, D.A.; and Hennekens, C.H. Light tomoderate alcohol consumption and mortalityin the elderly. Journal of the American
Geriatrics Society 40:651 -657, 1992.
Schmidt, A.; Barry, K.; and Fleming, M. A new
screening test for the detection of problemdrinkers: The Alcohol Use DisordersIdentification Test (AUDIT). Southern
Medical Journal 88:52-59,1995.
Schonfeld, L., and Dupree, L. Older problemdrinkers: Long-term and late-life onsetabusers: What triggers their drinking? Aging361:5 -9, 1990.
Schonfeld, L., and Dupree, L.W. Antecedents ofdrinking for early- and late-onset elderlyalcohol abusers. Journal of Studies on Alcohol
52:587 -592, 1991.
Schonfeld, L., and Dupree, L.W. Treatmentalternatives for older alcohol abusers. In:Gurnack, A., ed. Older Adults' Misuse ofAlcohol, Medicines, and Other Drugs: Research
and Practice Issues. New York: Springer,1996, pp. 113-131.
Schonfeld, L., and Dupree, L.W. Treatmentapproaches for older problem drinkers.International Journal of the Addictions
30(13 &14):1819 -1842, 1995.
Schuckit, M.A. Alcohol and depression: Aclinical perspective. Acta PsychiatraScandinavica Supplement 337:28 -32, 1994.
Schuckit, M.A. Drug and Alcohol Abuse, 3rd ed.
New York: Plenum Press, 1989.
Schuckit, M.A. Geriatric alcoholism and drugabuse. Gerontologist 17:168 -174, 1977.
Bibliography
Schuckit, M.A., and Morrissey, E.R. Drug abuseamong alcoholic women. American Journal of
Psychiatry 136:607 -611, 1979.
Scott, E., and Anderson, P. Randomizedcontrolled trial of general practitionerintervention in women with excessivealcohol consumption. Drug and Alcohol
Review 10:313 -321, 1990.
Scott, J.; Williams, J.M.G.; and Beck, A. Cognitive
Therapy in Clinical Practice: An Illustrative
Casebook. London, UK: Routledge, 1989.
Shaper, A.G.; Wannamethee, G.; and Walker, M.
Alcohol and mortality in British men:Explaining the U-shaped curve. Lancet2:1267 -1273, 1988.
Sheahan, S.L.; Coons, S.J.; Robbins, C.A.; Martin,
S.S.; Hendricks, J.; and Latimer, M.Psychoactive medication, alcohol use andfalls among older adults. Journal of Behavioral
Medicine 18(2):127 -140, 1995.
Sheahan, S.L.; Hendricks, J.; and Coons, S.J.
Drug misuse among the elderly: A covertproblem. Health Values 13(3):22 -29, 1989.
Shear, P.K.; Jerrigan, T.L.; and Butters, N.
Volumetric magnetic resonance imagingquantification of longitudinal brain changesin abstinent alcoholics. Alcoholism: Clinicaland Experimental Research 18:172 -176, 1994.
Sheikh, J.I., and Yesavage, J.A. GeriatricDepression Scale (GDS): Recent evidenceand development of a shorter version.Clinical Gerontologist 5(1 &2):165 -173, 1986.
Shipman, A. Communities aren't helpless:Outreach to older alcoholics works. Aging361:18 -21, 1990.
Jai163

Appendix C
Simon, A.; Epstein L.; and Reynolds L.
Alcoholism in the geriatric mentally ill.Geriatrics 23:125-131, 1968.
Smith, D.M., and Atkinson, R.M. Alcoholismand dementia. In: Gurnack A., ed. OlderAdults' Misuse of Alcohol, Medicines, and Other
Drugs: Research and Practice Issues. New
York: Springer, 1997. pp. 132-158.
Smith, J.W. Medical manifestations ofalcoholism in the elderly. InternationalJournal of the Addictions 30(13&14):1749-1798,
1995.
Smith, V. Symptom checklist-90-revised (SCL-
90-R) and the brief symptom inventory (BSI).
In: Sederer, L., Dickey, B., eds. OutcomesAssessment in Clinical Practice. Baltimore:Williams & Wilkins, 1996.
Sobell, L.C.; Brown, J.; Leo, G.I.; and Sobell, M.B.The reliability of the alcohol timeline
followback when administered by telephoneand by computer. Drug and Alcohol
Dependence 42(1):49-54, 1996.
Sobell, L.C.; Sobell, M.B.; Leo, G.I.; and Cancilla,A. Reliability of a timeline method:
Assessing normal drinkers' reports of recentdrinking and a comparative evaluation
across several populations. British Journal ofAddiction 83(4): 393-402, 1988.
Solomon, K.; Manepalli, J.; Ireland, G.A.; and
Mahon, G.M. Alcoholism and prescriptiondrug abuse in the elderly: St. LouisUniversity grand rounds. Journal of theAmerican Geriatric Society 41(1):57-69, 1993.
Speer, D.C., and Bates, K. Comorbid mental andsubstance disorders among older psychiatricpatients. Journal of the American Geriatric
Society 40:886-890, 1992.
164
Speirs, C.J.; Navey, F.L.; Broods, D.J.; and
Impallomeni, M.G. Opisthotonos andbenzodiazepine withdrawal in the elderly.Lancet 2:1101, 1986.
Spencer G. Projections of the Population of the
United States, by Age, Sex, and Race: 1988 to
2080. Series P-25, No. 1018. Washington,DC: U.S. Department of Commerce, 1989.
Spiegler, M.D., and Guevremont, D.C.
Contemporary Behavior Therapy. Pacific Grove,CA: Brooks/Cole, 1993.
Spitzer, R.L., and Williams, J.B. Structured
Clinical Interview for DSM-III (SCID). New
York: Biometrics Research Division, NewYork State Psychiatric Institute, 1985.
Spitzer, R.L.; Williams, J.B.; Gibbon, M.; and
First, M.B. The Structured Clinical Interviewfor DSM-HI-R (SCID): I. History, rationale,and description. Archives of General
Psychiatry 49:624-629, 1992.
Srivastava, L.M.; Vasisht, S.; Agarwal, D.P.; andGoedde, H.W. Relation between alcoholintake, lipoproteins and coronary arterydisease: The interest continues. Alcohol andAlcoholism 29:11-24, 1994.
Stall, R. Change and stability in quantity andfrequency of alcohol use among aging males:A 19-year follow-up study. British Journal ofAddiction 81:537-544, 1986.
Stewart, A.L.; Hays, R.D.; Ware, J.E., Jr. The
MOS Short-Form General Health Survey:Reliability and validity in a patientpopulation. Medical Care 26:724-735, 1988.
13b

Stinson, F.S.; Dufour, M.C.; and Bertolucci, D.Alcohol-related morbidity in the agingpopulation. Alcohol Health and Research World
13:80 -87, 1989.
Strang J., and Gurling, H. Computerizedtomography and neuropsychologicalassessment in long-term high-dose heroinaddicts. British Journal of Addiction
84:1011 -1019, 1989.
Swan, G.E.; Carmelli, D.; Rosenman, R.H.;
Fabsitz, R.R.; and Christian, J.C. Smokingand alcohol consumption in adult maletwins: Genetic heritability and sharedenvironmental influences. Journal ofSubstance Abuse 2:39-50,1990.
Tarlov, A.R.; Ware, J.E., Jr.; Greenfield, S.;
Nelson, E.C.; Perrin, E.; and Zubkoff, M. TheMedical Outcomes Study: An application ofmethods for monitoring the results ofmedical care. Journal of the American Medical
Association 262:925-930,1989.
Tarter, R.E. Cognition, aging, and alcohol. In:Beresford, T.P., and Gomberg, E., eds.Alcohol and Aging. New York: Oxford
University Press, 1995. pp. 82-97.
Temple, M.T., and Leino, E.V. Long-termoutcomes of drinking: A 20 yearlongitudinal study of men. British Journal of
Addiction 84:889 -899, 1989.
Thapa, P.B.; Gideon, P.; Fought, R.L.; and Ray,
W.A. Psychotropic drugs and risk ofrecurrent falls in ambulatory nursing homeresidents. American Journal of Epidemiology
142(2):202 -211, 1995.
183
Bibliography
Thomas-Knight, R. Treating alcoholism amongthe aged: The effectiveness of a specialtreatment program for older problemdrinkers. Dissertation Abstracts International
39:3009, 1978.
Tobias, C.; Lippmann, S.; Pary, R.; Oropilla, T.;
and Embry, C.K. Alcoholism in the elderly:How to spot and treat a problem the patientwants to hide. Postgraduate Medicine
86:67-70,75-79,1989.
Twerski, A.J. Early intervention in alcoholism:Confrontational techniques. Hospital andCommunity Psychiatry 34:1027 -1030, 1983.
Tyas, S.L., and Rush, B.R. Trends in the
characteristics of clients of alcohol/drugtreatment in Ontario. Canadian Journal of
Public Health 85:13 -16, 1994.
U.S. Bureau of the Census. 65+ in the UnitedStates. Current Population Reports, SpecialStuides, Number P23-190. Washington, DC:U.S. Government Printing Office, 1996.
U.S. Preventive Services Task Force. Guide to
Clinical Preventive Services. Baltimore:
Williams & Wilkins, 1996.
Vaillant, G.E.; Clark, W.; Cyrus, C.; Milofsky,
E.S.; Kopp, J.; Wulsin, V.W.; and Mogielnicki,
N.P. Prospective study of alcoholismtreatment: Eight-year follow-up. AmericanJournal of Medicine 75:455 -460, 1983.
Vance, D.E. Barriers to use of services by older
homeless people. Psychological Reports
75:1377 -1378, 1994.
Velicer, W.F.; Prochaska, J.0.; Rossi, J.S.; and
Snow, M.G. Assessing outcome in smokingcessation studies. Psychological Bulletin
111(1):23 -41, January 1992.
165

Appendix C
Venner, A.M.; Krupka, L.R.; and Climo, J.J.
Drug usage and health characteristics innoninstitutionalized retired persons. Journalof the American Geriatrics Society 27:83-90,
1980.
Vestal, R.E.; McGuire, E.A.; Tobin, J.D.; Andres,
R.; Norris, A.H.; and Mezey, E. Aging andethanol metabolism. Clinical Pharmacologyand Therapeutics 21:343 -354, 1977.
Victor, M.; Adams, R.C.; and Collins, G.H. TheWernicke-Korsakoff Syndrome and Related
Neurological Disorders Due to Alcoholism and
Malnutrition, 2nd ed. Philadelphia: F.A.Davis, 1989.
Vogel-Sprott, M., and Barret, P. Age, drinkinghabits, and the effects of alcohol. Journal ofStudies on Alcohol 45:517-521,1984.
Wagman, A.M.; Allen, R.P.; and Upright, D.Effects of alcohol consumption uponparameters of ultradian sleep rhythms inalcoholics. Advances in Experimental Medicine
and Biology 85A:601 -616, 1977.
Wallace, P.; Cutler, S.; and Haines A.
Randomized controlled trial of generalpractitioner intervention in patients withexcessive alcohol consumption. BritishMedical journal 297(6649):663 -668, 1988.
Wallace, P., and Haines, A. Use of aquestionnaire in general practice to increasethe recognition of patients with excessivealcohol consumption. British Medical Journal290:1949 -1953, 1985.
Ware, J.E., Jr., and Sherbourne, C.D. The MOS36-Item Short-Form Health Survey (SF-36): I.Conceptual framework and item selection.Medical Care 30:473 -481, 1992.
166 134
Watson, Y.I.; Arfken, C.L.; and Birge, S.J. Clock
completion: An objective screening test fordementia. Journal of the American Geriatrics
Society 41:1235 -1240, 1993.
Waugh, M.; Jackson, M.; Fox, F.A.; Hawke, S.H.;
and Tuck, R.R. Effect of social drinking onneuropsychological performance. BritishJournal of Addiction 84:659 -667, 1989.
Weintraub, M., and Handy, B.M.Benzodiazepines and hip fractures: The NewYork State experience. Clinical Pharmacology
Therapy 54(3):252 -256, 1993.
Weiss, K.J. Management of anxiety anddepression syndromes in the elderly. Journalof Clinical Psychiatry 55(suppl. 2):5 -12, 1994.
Wells, K.B.; Burnam, M.A.; Benjamin, B.; and
Golding, J.M. Alcohol use and limitations inphysical functioning in a sample of the LosAngeles general population. Alcohol andAlcoholism 25:673-684,1990.
Welte, J.W., and Mirand, A.L. Alcohol Use by the
Elderly: Patterns and Correlates: A Report on
the Erie County Elder Drinking Survey.
Buffalo, NY: Research Institute onAddictions, October 1992.
Wiens, A.N.; Menustik, C.E.; Miller, S.L.; andSchmitz, R.E. Medicalbehavioral treatmentof the older alcoholic patient. AmericanJournal of Drug and Alcohol Abuse
9(4):461 -475, 1982/1983.
Willcox, S.M.; Himmelstein, D.U.; andWoolhandler, S. Inappropriate drugprescribing for the community-dwellingelderly. Journal of the American Medical
Association 272(4):292 -296, 1994.

Appendix DResource Panel
Kathleen Austin, CDC III, NCAC IIAlcohol Therapist IIAdult Medicine/Ambulatory CareHarborview Medical CenterSeattle, Washington
James D. Baxendale, Ph.D.Deputy DirectorQuality Assurance and Case ManagementNational Association of State Alcohol and
Drug Abuse DirectorsWashington, D.C.
Gwendolyn G. BennettSpecial Assistant to the DirectorDivision of State and Community Systems
DevelopmentCenter for Mental Health ServicesRockville, Maryland
Gayle Boyd, Ph.D.
Health Scientist AdministratorPrevention Research BranchNational Institute on Alcohol Abuse
and AlcoholismRockville, Maryland
186
Mildred Brooks-McDow, M.S.W., L.I.C.S.W.Public Health AdvisorDivision of State and Community Systems
DevelopmentCenter for Mental Health ServicesRockville, Maryland
Carol CoberActing ManagerSocial Outreach and Support DivisionAmerican Association of Retired PersonsWashington, D.C.
Peter J. Cohen, M.D., J.D.
Special Expert
Medications Development DivisionNational Institute on Drug AbuseRockville, Maryland
Dorynne Czechowicz, M.D.Associate DirectorMedical/Professional AffairsTreatment Research BranchDivision of Clinical and Services Research
National Institute on Drug AbuseRockville, Maryland
Betty Davis
Senior Project SpecialistSocial Outreach and Support DivisionAmerican Association of Retired PersonsWashington, D.C.
169

Appendix D
Loretta Finnegan, M.D.DirectorWomen's Health InitiativeNational Institutes of HealthBethesda, Maryland
Linda S. Foley, M.A.
MemberTIPS Editorial Advisory BoardDirector
Treatment Improvement ExchangeHealth Systems Research, Inc.Washington, D.C.
Rizalina C. GalicinaoProgram AnalystOffice of Minority HealthPublic Health ServiceRockville, Maryland
Deborah HoranManagerSpecial IssuesAmerican College of Obstetrics and
GynecologyWashington, D.C.
Alixe McNeill
Senior Program ManagerNational Council on the AgingWashington, D.C.
Reba L. Novich, M.S.W.
Resource ManagerNational Resource CenterOsteoporosis and Related Bone DiseasesWashington, D.C.
170
Hi la Richardson, Dr.P.H.
Deputy DirectorMedical Research and Practice PolicyNational Center on Addiction and
Substance AbuseColumbia UniversityNew York, New York
Anita Rosen, Ph.D.
Senior Staff Associate for Aging
National Association of Social WorkersWashington, D.C.
Eleanor SargentDirector
Clinical Issues
National Association of Alcoholism andDrug Abuse Counselors
Arlington, Virginia
Joanne G. Schwartzberg, M.D.Director
Department of Geriatric HealthAmerican Medical AssociationChicago, Illinois
Dora lie L. Segal, M.S.
Senior AdvisorPHS Office of Women's Health
Medical Development DivisionNational Institute on Drug AbuseRockville, Maryland
Nancy J. WartowPolicy Specialist
Administration on AgingWashington, D.C.
Paul Wohlford, Ph.D.
Acting Branch ChiefDivision of State and Community Systems
DevelopmentCenter for Mental Health ServicesRockville, Maryland
187

Appendix EField Reviewers
Ruth Airey-VidalCoordinatorWellness Initiative for Senior EducatorsSussex Council on Alcohol and Drug AbuseNewton, New Jersey
Sharon AmattetiPublic Health AnalystOffice of Policy Coordination and PlanningCenter for Substance Abuse TreatmentRockville, Maryland
Mary Candace Burger, Ph.D.Assistant ProfessorDivision of Geriatric PsychiatryDepartment of PsychiatryVanderbilt Medical SchoolNashville, Tennesee
James DonagherDirectorSenior ServicesSpecial Populations of Office of Behavioral
HealthDepartment of Mental Health and Addiction
Services
Hartford, Connecticut
Charles M. Donahue, M.Div.Community LiaisonBehavioral Health NetworkAlexian Brothers HospitalSaint Louis, Missouri
Nancy L. ErckenbrackRegional DirectorOperations and HousingLong-Term Care DivisionProvidence Health SystemsPortland, Oregon
Hugh EvermanStaff AssistantDepartment of SociologyMorehead State UniversityMorehead, Kentucky
Robert S. Geissinger
CounselorDivision of Alcoholism and Substance AbuseWashington State Department of Social and
Health Services
Lacey, Washington
188171

Appendix E
Charles V. Giannasio, M.D.
Senior Consultant for Addictive DisordersNorthwest Institute of PsychiatryJenkintown, Pennsylvania
Robert K. Heaton, Ph.D.Professor of Psychiatry
Neuropsychology LaboratoryUniversity of California at San DiegoSan Diego, California
Robert Holden, M.A.Program DirectorPartners in Drug Abuse Rehabilitation
CounselingWashington, D.C.
Ronald J. Hunsicker
Executive Director
National Association of Addiction TreatmentProviders
Lititz, Pennsylvania
Carol L. Joseph, M.D.
Associate ChiefStaff for Geriatric and Extended CareHonolulu VAMROCHonolulu, Hawaii
Joseph Liberto, M.D.
DirectorUAMC
Baltimore, Maryland
Jane E. Myers, Ph.D.Professor
Department of Counseling andEducational Development
University of North Carolina at GreensboroGreensboro, North Carolina
Reba L. Novich, M.S.W.
Resource ManagerNational Resource CenterOsteoporosis and Related Bone DiseasesWashington, D.C.
172
Robert RawlingsDirector
OBRA and LTC
Community ProgramsOklahoma Department of Mental Health
and Substance Abuse ServicesOklahoma City, Oklahoma
Patricia Reihl
CoordinatorSpring HouseParamus, New Jersey
Anita Rosen, Ph.D.
Senior Staff Associate for AgingNational Association of Social WorkersWashington, D.C.
Margaret M. Salinger, M.S.N., R.N., C.A.R.N.
National Nurses Society on Addictionc/o Department of Veterans Affairs Medical
CenterCoatesville, Pennsylvania
Eleanor SargentDirector
Clinical Issues
National Association of Alcoholism andDrug Abuse Counselors
Arlington, Virginia
Timothy M. ScanlanPresident
Addiction Specialists of KansasWichita, Kansas
Larry I. Schonfeld, Ph.D.Professor
Department of Aging and Mental HealthFlorida Mental Health InstituteUniversity of South FloridaTampa, Florida
189

Appendix E
Charles V. Giannasio, M.D.
Senior Consultant for Addictive DisordersNorthwest Institute of PsychiatryJenkintown, Pennsylvania
Robert K. Heaton, Ph.D.Professor of Psychiatry
Neuropsychology LaboratoryUniversity of California at San DiegoSan Diego, California
Robert Holden, M.A.Program DirectorPartners in Drug Abuse Rehabilitation
CounselingWashington, D.C.
Ronald J. Hunsicker
Executive Director
National Association of Addiction TreatmentProviders
Lititz, Pennsylvania
Carol L. Joseph, M.D.
Associate Chief
Staff for Geriatric and Extended CareHonolulu VAMROCHonolulu, Hawaii
Joseph Liberto, M.D.DirectorUAMC
Baltimore, Maryland
Jane E. Myers, Ph.D.Professor
Department of Counseling andEducational Development
University of North Carolina at GreensboroGreensboro, North Carolina
Reba L. Novich, M.S.W.
Resource ManagerNational Resource Center
Osteoporosis and Related Bone DiseasesWashington, D.C.
172
Robert RawlingsDirectorOBRA and LTC
Community Programs
Oklahoma Department of Mental Healthand Substance Abuse Services
Oklahoma City, Oklahoma
Patricia Reihl
CoordinatorSpring HouseParamus, New Jersey
Anita Rosen, Ph.D.
Senior Staff Associate for Aging
National Association of Social WorkersWashington, D.C.
Margaret M. Salinger, M.S.N., R.N., C.A.R.N.National Nurses Society on Addictionc/o Department of Veterans Affairs Medical
Center
Coatesville, Pennsylvania
Eleanor SargentDirectorClinical Issues
National Association of Alcoholism andDrug Abuse Counselors
Arlington, Virginia
Timothy M. ScanlanPresident
Addiction Specialists of KansasWichita, Kansas
Larry I. Schonfeld, Ph.D.Professor
Department of Aging and Mental HealthFlorida Mental Health InstituteUniversity of South FloridaTampa, Florida
ISJ

Anthony SimsActing DirectorOffice of Communications and External
LiaisonCenter for Substance Abuse TreatmentRockville, Maryland
Richard T. Suchinsky, M.D.
Associate ChiefAddictive DisordersMental Health and Behavioral Sciences
Services
Department of Veterans AffairsWashington, D.C.
Field Reviewers
David 0. TurnerProgram ManagerHealth Aging ProgramSalt Lake County Aging ServicesSalt Lake City, Utah
John W. Welte, Ph.D.
Research ScientistResearch Institute on AddictionBuffalo, New York
Larry W. WhorleyProgram CoordinatorSubstance Abuse Treatment ProgramLexington, Kentucky
190 173

The TIPs Series
TIP 1 State Methadone Treatment Guidelines BKD98TIP 2 Pregnant, Substance-Using Women BKD107TIP 3 Screening and Assessment of Alcohol- and Other Drug-Abusing Adolescents BKD108TIP 4 Guidelines for the Treatment of Alcohol- and Other Drug-Abusing Adolescents BKD109TIP 5 Improving Treatment for Drug-Exposed Infants BKD110TIP 6 Screening for Infectious Diseases Among Substance Abusers BKD131TIP 7 Screening and Assessment for Alcohol and Other Drug Abuse Among Adults in the
Criminal Justice System BKD138TIP 8 Intensive Outpatient Treatment for Alcohol and Other Drug Abuse BKD139TIP 9 Assessment and Treatment of Patients with Coexisting Mental Illness and Alcohol and Other
Drug Abuse BKD134TIP 10 Assessment and Treatment of Cocaine-Abusing Methadone-Maintained Patients BKD157TIP 11 Simple Screening Instruments for Outreach for Alcohol and Other Drug Abuse and
Infectious Diseases BKD143TIP 12 Combining Substance Abuse Treatment With Intermediate Sanctions for Adults in the
Criminal Justice System BKD144TIP 13 The Role and Current Status of Patient Placement Criteria in the Treatment of Substance
Use Disorders BKD161TIP 14 Developing State Outcomes Monitoring Systems for Alcohol and Other Drug Abuse
Treatment BKD162TIP 15 Treatment for HIV-Infected Alcohol and Other Drug Abusers BKD163TIP 16 Alcohol and Other Drug Screening of Hospitalized Trauma Patients BKD164TIP 17 Planning for Alcohol and Other Drug Abuse Treatment for Adults in the Criminal Justice
System BKD165TIP 18 The Tuberculosis Epidemic: Legal and Ethical Issues for Alcohol and Other Drug Abuse Treatment
Providers BKD173TIP 19 DetoXification from Alcohol and Other Drugs BKD172TIP 20 Matching Treatment to Patient Needs in Opioid Substitution Therapy BKD168TIP 21 Combining Alcohol and Other Drug Abuse Treatment With Diversion
for Juveniles in the Justice System BKD169TIP 22 LAAM in the Treatment of Opiate Addiction BKD170TIP 23 Treatment Drug Courts: Integrating Substance Abuse Treatment With Legal Case Processing BKD205TIP 24 A Guide to Substance Abuse Services for Primary Care Clinicians BKD234TIP 25 Substance Abuse Treatment and Domestic Violence BKD239TIP 26 Substance Abuse Among Older Adults BKD250
Other TIPs may be ordered by contacting the National Clearinghouse for Alcohol and Drug Information(NCADI), (800) 729-6686 or (301) 468-2600; TDD (for hearing impaired), (800) 487-4889.
DHHS Publication No. (SMA) 98-3179Substance Abuse and Mental Health Services AdministrationPrinted 1998
BEST COPY AVAILABLE191
SA/WISA

U.S. Department of EducationOffice of Educational Research and Improvement (OERI)
National Library of Education (NLE)Educational Resources Information Center (ERIC)
NOTICE
REPRODUCTION BASIS
IC
This document is covered by a signed "Reproduction Release(Blanket) form (on file within the ERIC system), encompassing allor classes of documents from its source organization and, therefore,does not require a "Specific Document" Release form.
This document is Federally-funded, or carries its own permission toreproduce, or is otherwise in the public domain and, therefore, maybe reproduced by ERIC without a signed Reproduction Release form(either "Specific Document" or "Blanket").
EFF-089 (9/97)