Embed Size (px)
Citation preview

J Clin Pathol 1986;39:933-944
Review article
Terminology in gynaecological cytopathology: reportof the Working Party of The British Society forClinical CytologyD M D EVANS (CHAIRMAN),* E A HUDSON (SECRETARY),t C L BROWN,ttM M BODDINGTON,¶T H E HUGHES,¶ E F D MACKENZIE,** T MARSHALL§From *St David's Hospital, Cardiff, tNorthwick Park Hospital, Harrow, ttThe London Hospital, ¶RoyalBerkshire Hospital, Reading, ¶Glasgow Royal Infirmary. **Southmead General Hospital, Bristol, §CentralPathology Laboratory, Stoke on Trent
SUMMARY The report defines and recommends terms for use in cervical cytology.
Most cervical smear reports are received by medicalpractitioners who do not have specialised knowledgeof pathology or gynaecology. Therefore it isimportant that the report is not only scientificallyaccurate but also easily understood so that the patientreceives appropriate management and advice. Topromote these aims the British Society for ClinicalCytology set up a working party to make recommen-dations on the reporting of cervical smears and theterms used. It was suggested that common use of asmall but clearly defined vocabulary would improvethe communication of results to users of the cytologyservices and provide an accurate basis for widerreference.
The cytology report
The cytology report on abnormal findings shouldconsist of a concise description of cells in preciselydefined and generally accepted cytological terms. Thismay be followed, if appropriate, by a prediction of thehistological condition based on the overall pictureand should include a recommendation for the furthermanagement of the patient.When a prediction of histology is included as a sup-
plementary statement to a description of the cytologyuse of the terminology, cervical intraepithelial neo-plasia (CIN) is preferred: it has the advantage ofrelating the histological report more clearly to theprognosis and management than the artificial sepa-ration implied by classification into dysplasia and car-cinoma in situ. Caution is advised, however, in the
Accepted for publication 18 March 1986
firm prediction of CIN 3 because the cytologist can-not reliably exclude a microinvasive or invasivelesion. The histological prediction is more accuratelyrecorded on the National Cytology Form, HMR101/5 (1982), where severe dysplasia or carcinoma insitu-(C-IN 3), or-carcinoma in situ (CIN 3) or? invasivecarcinoma are the alternatives provided.
INFLAMMATORY NUCLEAR CHANGES ANDDYSKARYOSISA continuous range of nuclear abnormalities occurs,from minor changes that are usually associated withinflammatory conditions and which are believed to beessentially benign, through to more striking nuclearabnormalities that correlate with CIN. Cytologistsshould be encouraged to say precisely what abnor-mality is present in as many cases as possible, butthere will be some in which the abnormality is on theborderline. These abnormalities may be referred to as"borderline nuclear abnormalities." In these circum-stances follow up with repeat smears usually allows amore exact cytological diagnosis to be made.The morphological abnormalities of the nucleus
comprise a combination of any number of the follow-ing:(1) disproportionate nuclear enlargement;(2) irregularity in form and outline;(3) hyperchromasia;(4) irregular chromatin condensation, appearing asstippling, clumps, or strands, and sometimes as con-densation beneath the nuclear membrane producingapparent irregularities in thickness of the nuclearmembrane;(5) abnormalities of the number, size, and form of
933
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Evans, Hudson, Brown, Boddington, Hughes, Mackenzie, Marshall
oS.
S
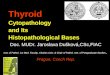
Fig I Normal superficial and intermediate squamous cells. Both cell types have abundant translucent cytoplasm with angularborders. Nuclei ofboth intermediate squamous cells have evenly distributedfinely granular chromatin, whereas three superficialcells have smaller pyknotic nuclei. (Papanicolaou.) Original magnification x 1.60, enlarged x 5.
Fig 2 Endocervical cells. These columnar epithelial cells are seen lined up in characteristic palisade pattern andfrom analternative aspect in a sheet with nuclei surrounded by narrow rim ofcytoplasm. Nuclei appear vesicular apartfrom one ormore prominent nucleoli. (Papanicolaou.) Original magnification x 160, enlarged x 5.
934
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Terminology in gynaecological cytopathology
I
I'lL"
Fig 3 Normalparabasal squamous cells. These cells usually have rounded outlines with opaque cytoplasm and vesicularnuclei. Chromatin pattern isfinely granular but nucleoli may be prominent. (Papanicolaou.) Original magnification x 160,enlarged x 5.
-'NI(
V4e !'s} .'SO ';
::::: :*_ s ...
w ."ESE.... o. w .}ws _ _
!pv *
v v * _,.
i_8a.4
*S s.4s
i *d,S
i
pA
_ .
.
t~~~~~~~~~~~ 7". `;
Fig 4 Inflammatory changes in parabasal squamous cells. Inflammatory nuclear changes may be particularly pronounced insmearsfrom atrophic cervical squamous epithelium, as shown here. Hyperchromasia is striking and chromatin is coarselyclumped but clumps are evenly distributed. An impression ofanisonucleosis is created by coexistence ofreactive anddegenerative changes in nuclei. (Papanicolaou.) Original magnification x 160, enlarged x 5.
935
..: 11:. 4.
Wt:-
*S::
IP
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Evans, Hudson, Brown, Boddington, Hughes, Mackenzie, Marshallnucleoli;(6) multinucleation associated with any of the above.
Figs I and 3 show examples of normal squamouscells; fig 2 shows glandular cells.
InflammationInflammation alone causes minor nuclear abnormal-ities (fig 4). These are usually disproportionatenuclear enlargement with or without hyperchromasia.Wrinkling of the nuclear membrane due to degener-ative change may also be associated with inflam-mation but must be distinguished from the irregu-larities of form and outline of dyskaryosis.Karyorrhexis and pyknosis must also be dis-tinguished from nuclear abnormalities with malig-nant potential. There is no need to report simpleinflammatory changes.
DyskaryosisDyskaryosis literally means "abnormal nucleus" andis liable to be used in different ways-for example, bysome to describe abnormal cells expected to beobtained from CIN 1 or CIN 2, and by others it isonly used for severely abnormal cells expected tocome from CIN 3.
Dyskaryosis should be used to describe nuclearabnormalities more numerous or more severe than
those associated with inflammation alone. Irregu-larity of chromatin distribution is the most importantchange in nuclear morphology. It may be accom-panied by irregularity of form and outline, multi-nucleation, further disproportionate nuclear enlarge-ment, and hyperchromasia. Artefactual cell distortionmust be distinguished from dyskaryosis.The Working Party endorses the recommendation
by Spriggs et al' that "dyskaryosis" and "dys-karyotic" should be used to describe the nuclearabnormalities seen in cells from CIN and it recognisesthat some cases of invasive carcinoma exfoliate simi-lar cells.The term dyskaryosis is appropriate when referring
to both squamous and endocervical cell abnormalitieswith the same implication of intraepithelial orinvasive carcinoma.
CLASSIFICATION OF DYSKARYOTIC CELLSSpriggs et al' recommended a classification thatdepends on the cytoplasmic characteristics of the dys-karyotic squamous cells. Thus superficial cell, inter-mediate cell, and parabasal cell dyskaryosis weredescribed. After considerable deliberation this Work-ing Party prefers to emphasise the overridingimportance of nuclear abnormalities. This does notexclude cytoplasmic changes from cell assessment,
p
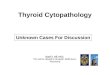
Fig 5 Mild dyskaryosis. Nuclei are enlarged and hyperchromatic. Clumps and ridges ofchromatin are unevenly distributedand there are alsofolds in some of the nuclear membranes. Three cells are binucleate. Abnormal nuclei occupy less than halfarea ofcytoplasm ofmost ofthese cells. Cytoplasm retains translucent quality ofnormal, superficial, or intermediate squamouscells. (Papanicolaou.) Original magnification x 160, enlarged x 5.
936
40010dik
AM&
ABLII.
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Terminology in gynaecological cytopathology
* .:: .:*.E:
*Q9R<-r Se 4
Fig 6 Nuclear abnormalities associated with human papiloma virus infection. These koilocytes show typical central clearingand peripheral condensation ofcytoplasm. It is impossible to be certain whether uneven chromatin pattern in larger nucleus isdyskaryotic or degenerate: patient would therefore befollowed up. (Papanicolaou.) Original magnification x 160, enlarged x5.
'p.I.
.*
S.
4 )
...~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~~-1-..
Fig 7 Moderate dyskaryosis. Disproportionate nuclear enlargement is greater than that infig5 and morphologicalabnormalities ofnuclei more severe. Dyskaryosis is classified as moderate in most of the cells but could be called severe infewin which area ofnucleus exceeds two thirds ofarea ofcytoplasm of cell. (Papanicolaou.) Original magnification x 160,enlarged x 5.
937
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Evans, Hudson, Brown, Boddington, Hughes, Mackenzie, Marshall
AL,-~ ~ ~ ~ "
juMEw * F g s xYss X
a'
t~~~~~~~f
C. t_. ... .............. 41{4
it
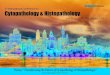
Fig 8 Severe dyskaryosis. (a) Dyskaryotic cells show wide range ofnuclear abnormalities, ofwhich uneven chromatindistribution and irregularities ofnuclear membranes are most important. Differences in size and shape of cells and their nucleiare striking in this example. Abnormal nuclei occupy more than two thirds of all cytoplasm. (b) Uniformly small size of theseseverely dyskaryotic cells may cause diagnostic difficulty.
Fig 8 continued opposite
938
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Terminology in gynaecological cytopathology
A~~rtL.&..
(c)
*Sa
4'I
939
I
C.
CI(d}
Fig 8 continuedIrregular chromatin condensation is predominant abnormalfeature ofnuclei, although some show degenerative changes.Hyperchromasia is present but is not always afeature in this type ofabnormal cell. Afew cells in which nucleus occupies lessthan two thirds could be classified as moderately dyskaryotic. (c) Cluster ofseverely dyskaryotic cells contrasts with singlenormal superficial squamous cell and both intermediate squamous cells. Although abnormal cells have irregular chromatindistribution patterns, size and shape is generallyfairly uniform. Nuclei are crowded together and this appearance contrasts withorderly pattern ofsheet ofendocervical cells seen infig 2. (d) Fragment ofepithelium is breaking up in characteristic manner toshow severely dyskaryotic cells in clusters of various sizes, single cells, and bare nuclei.
Fig 8 continued overleaf
k
Vkp Is...
Aaw' 4o"o % " 4
T-r
VW
dk
4, P.
00 41iAik
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Evans, Hudson, Brown, Boddington, Hughes, Mackenzie, Marshall
._l_
PS,0
oo..*_0
4,
tA..r*A
az
cSp..
_JO NL
...
-
.ailt'F
% q
-
r ---
-
--5ql!,
---
4
0*
Fig 8 continued(e) Abnormal nuclear chromatin pattern ofthese severely dyskaryotic cells distinguishes themfrom parabasal squamous cells.(f) Thesefour severely dyskaryotic cells with little cytoplasm show such gross aggregation ofchromatin that translucent areasare seen within nuclei. (Papanicolaou.) Original magnification x 160, enlarged x 5.
940
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Terminology in gynaecological cytopathologybut when nuclear abnormalities are particularlysevere they should outweigh any apparent cyto-plasmic maturation. It is recommended that dys-karyotic cells are classified as mild, moderate, orsevere according to:I The diversity of abnormal nuclear characteristics
listed above and the degree of morphologicalabnormality.
2 Cytoplasmic characteristics, which include quan-tity, density, shape, and staining quality.
Mild dyskaryosisMildly dyskaryotic cells usually have plentiful, thin,translucent cytoplasm with angular borders, resem-bling superficial or intermediate squamous cells(fig 5). The nucleus occupies less than half the totalarea of the cytoplasm. Mild dyskaryosis correlateswith cells from the surface of CIN 1. It is doubtful,however, if it can be reliably distinguished from thenuclear abnormalities associated with human papillo-mavirus infection (fig 6).
Moderate dyskaryosisModerately dyskaryotic cells have more dis-proportionate nuclear enlargement than mildlydyskaryotic cells, so that the nucleus occupies onehalf to two thirds of the total area of the cytoplasm(fig7). The nuclear morphology tends to be moreabnormal than that seen in mild dyskaryosis. Thecytoplasm may resemble that of intermediate, para-basal, or sometimes superficial type squamous cells.
Severe dyskaryosisSeverely dyskaryotic cells typically have a narrow rimof thick dense cytoplasm and they are round, oval,polygonal, or elongated in shape (figs 8a-f). Thus theabnormal nucleus practically fills the cell, or at leasttwo thirds of it. Occasionally, there are severely dys-karyotic cells in which there is plentiful abnormallyshaped, often keratinised, cytoplasm accompanied byabnormal nuclear morphology that is more pro-nounced in degree and diversity than that usuallyassociated with CIN I or CIN 2. Their correct inter-pretation is facilitated by the presence of more char-acteristic cells showing the changes described above.In those cases the cells should be described as severelydyskaryotic. In severe dyskaryosis the abnormal cellsmay occur in clumps as well as singly. Severely dys-karyotic cells correlate with cells from the surface ofcervical epithelium showing CIN 3 or invasive car-cinoma.
Intercellular relationEvaluation of sheets of epithelial cells in a smearrequires slightly different criteria, which may be moredifficult to define than the diagnostic characteristics
941of single cells (figs 8c and d). Loss of normal regulararrangement (polarity) may distinguish neoplasiafrom severe inflammation when the nuclear appear-ances are equivocal. Papillary processes, sheets ofmetaplastic cells, fragments of CIN 3, anddesquamated glands from adenocarcinoma provideexamples of the importance of intercellular relation ininterpretation (fig 9).
INVASIVE AND MICROINVASIVE CARCINOMA OFTHE CERVIXInvasive carcinoma cannot be diagnosed reliablyfrom a smear. There are cytological features, how-ever, which infer a strong possibility of a moreadvanced abnormality than that suggested by CIN 3(fig I Oa). It may be useful to refer to these in the cytol-ogy report to convey the more urgent need for biopsy.The following characteristics, often several at once,are associated with invasive tumours:1 Variation in size and shape of dyskaryotic cell
nuclei beyond that usually associated with CIN 3and often including unusually small cells ofbizarre shape.
2 Aggregations of nuclear chromatin, so coarse thattranslucencies appear.
3 Large irregular sometimes multiple nucleoli indyskaryotic cells.
4 Cytoplasmic keratinisation of dyskaryotic cellsand the presence of thick anucleate fragments ofkeratinised cytoplasm.
5 Irregularly shaped dyskaryotic squamous cellsincluding fibre cells and tadpole cells as well asother bizarre forms (figs 10b and c).
6 Tissue fragments composed of dyskaryotic cells.The term "malignant diathesis" is sometimes used
to describe the necrotic debris, inflammatory exudate,and blood that predominate in smears from ulceratedinvasive tumours. These constituents may contributeto an unreliable smear. They are insufficiently specificfor diagnosis.The term "malignant cells" may be read as
implying invasive carcinoma. It is preferable todescribe the cells as dyskaryotic, and a secondarystatement could be added to draw attention to char-acteristics associated with an invasive tumour. It isa long established custom of reporting at somecentres to mention malignant cells before suitablediagnostic and therapeutic measures are undertaken,even for an intraepithelial abnormality. The WorkingParty feels that this should be discouraged, unlessthere is firm evidence of invasive tumour.
SMEARS. SHOWING BORDERLINE ABNORMALITIESThe report is made after careful scrutiny of all the
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Evans, Hudson, Brown, Boddington, Hughes, Mackenzie, Marshall
Fig 9 Severe dyskaryosis from endocervical adenocarcinoma. Desquamated gland shows characteristic rosette pattern.(Papanicolaou.) Original magnification x 160, enlarged x 5.
material on the smear and rarely depends on theappearance of one cell. Some cells will be on theborderline between the accepted definitions, but theproblem of classification can usually be resolved bythe time the whole specimen has been examined. Inthe relatively few smears that remain equivocal arepeat smear for a mild abnormality or referral forcolposcopy and biopsy for more severe abnormalitieswill be necessary to resolve the problem.The Working Party has considered the use of the
term atypia or another single word for the equivocalsmear. It has decided against such a recommendationbecause the word can be used too often as a substitutefor careful observation and definition.
Atypia has been used in a number of senses includ-ing that for which this report recommends dys-karyosis. It should be avoided because its previousloose and diverse application makes it unlikely thatusers will adhere to any definition suggested now.There are smears in which the evidence is such that itis impossible to decide if the cells are the product ofinflammation or if they have neoplastic potential. It issuggested that the report should explain briefly thediagnostic dilemma (bordering on mild dyskaryosis).This is more helpful than a word of uncertainmeaning.
METAPLASIASmears may contain endocervical cells that have somesquamous characteristics. These appearances cor-relate with the surface of immature metaplastic epi-thelium from the transformation zone of the cervix.Sometimes the squamous features are so pronouncedthat the cells cannot be distinguished from parabasalsquamous cells from immature primary squamousepithelium. Dyskaryosis often occurs in these cellsand should be reported and managed accordingly.
CYTOPATHIC CHANGES DUE TO WART VIRUSThe human papillomavirus causes a variety ofappearances in smears.2 These maymimic some char-acteristics of well differentiated squamous carcinomabut the severe dyskaryosis of squamous carcinomawill not be present. Wart virus changes accompaniedby dyskaryosis should be managed according to thedegree of dyskaryosis.3
NUMERICAL CLASSIFICATIONSThe Papanicolaou classification of cytology reportsinto classes I to V has been discouraged for some timebecause of the different interpretations which itsbroad definitions have been given. It is retained insome centres in which there is a clear understanding
942
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Terminology in gynaecological cytopathology
90tEliFi~~~~~~ eqb
.e Jqb(a)
41~~~~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~4
(b}
Fig 10 Severe dyskaryosisfrom invasive squamous carcinoma. (a) All of these cells are severely dyskaryotic. They appear invarious shapes and there arefragments ofdegenerative cells in the background. (b) Elongated severely dyskaryotic cells aresometimes calledfibre cells. These and other bizarreforms are particularly characteristic of invasive carcinoma but may also beseen in smearsfrom CIN 3. ingIII...
*~~~~~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~ ~~~~i iu wrsnuuuvru
943
rig 1u coniinuea overteaj
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from

Evans, Hudson, Brown, Boddington, Hughes, Mackenzie, Marshall
Fig 10 continued(c) This severely dyskaryotic cell has plentiful abnormally shaped keratinised cytoplasm accompanied by severely abnormalnuclear morphology. Elongated tail ofcytoplasm has led to description of this bizarreform as a tadpole cell. (Papanicolaou.)Original magnification x 160, enlarged x 5.
between cytopathologist and gynaecologist about itsuse but it lacks the precision necessary for wider refer-ence. Similarly, attempts to subdivide or redefine thePapanicolaou classification or the introduction ofother numerical or alphabetic shorthands will resultin varied interpretations.
ENDOMETRIAL CELLSEndometrial cells can be identified in smears, but thecervical smear is not a reliable test for endometrialabnormalities. The cause of endometrial exfoliationmay not be reflected in the morphology of the cells-for example, cells from a well differentiated ade-nocarcinoma may be barely distinguishable from
endometrial cells exfoliated from a benign lesion orduring menstruation.References
I Spriggs AJ, Butler EB, Evans DMD, Grubb C, Husain OAN,Wachtel GE. Problems of cell nomenclature in cervical cytol-ogy smears. J Clin Pathol 1978;31:1226-7.
2 Butler EB, Stanbridge CM. Condylomatous lesions of the lowerfemale genital tract. Clin Obstet Gynaecol 1984;1 1:171-87.
3 Kaufman R, Koss LG, Kurman RJ, et al. Statement of caution inthe interpretation of papillomavirus-associated lesions of theepithelium of the uterine cervix. Acta Cytol 1983;27:107-8.
Requests for reprints to: Dr E A Hudson, Departmentof Histopathology, Northwick Park Hospital, Harrow,Middlesex HAl 3UJ, England.
944
copyright. on January 26, 2020 by guest. P
rotected byhttp://jcp.bm
j.com/
J Clin P
athol: first published as 10.1136/jcp.39.9.933 on 1 Septem
ber 1986. Dow
nloaded from