Embed Size (px)
Citation preview

Report of the Queensland Maternaland Perinatal Quality Council
MATERNAL AND PERINATALMORBIDITY AND MORTALITYIN QUEENSLAND
2002


MATERNAL AND PERINATAL MORBIDITY AND MORTALITY IN
QUEENSLAND -2000
Contact details for further information
All correspondence should be addressed to:
The Secretariat
Queensland Maternal & Perinatal Quality Council
Office of the Chief Health Officer
Queensland Health
PO Box 48
BRISBANE QLD 4001
Ph: (07) 323 40607
Fax: (07) 322 17535
Email: [email protected]
i

Preface
This is the first report of the Queensland Maternal and Perinatal Quality Council (the Council) and provides an
overview of the activities of the Council since its inception in August 2001. The Council will build on the work
that was undertaken by the former Queensland Council on Obstetric and Paediatric Morbidity and Mortality
(QCOPMM).
The Council was established pursuant to the quality assurance provisions of the
which provides members with legislative protection and enables the Council to undertake confidential
enquiries into perinatal and maternal mortality and morbidity.
The Council considers patterns and trends of mortality and morbidity in Queensland, to enable benchmarking
and comparisons across regions and populations which can be monitored and provide opportunities to
improve health outcomes.
This report contains data sourced from the Perinatal Data Collection Unit of Queensland Health, which largely
underpins the activities of the Council.
Gathering data about maternal mortality remains challenging, as, due to the low incidence of maternal
mortality, a dedicated maternal mortality collection does not exist. However, Council seeks to report on direct,
indirect and incidental deaths and is thankful for the support of colleagues throughout Queensland who
contribute to this effort.
I would like to thank the members of the Council, and those who support them, for their commitment to
improving obstetric and perinatal outcomes. I trust that clinicians throughout Queensland will find this report
helpful and give careful consideration to the Council's recommendations.
Dr Gerry FitzGerald
Chief Health Officer
October 2003
Health Services Act 1991,
ii

iii
Chairman's report
This is the first report of the Queensland Maternal and Perinatal Quality Council (QMPQC) and I would like to
thank the Council members for their participation and enthusiasm. The inaugural meeting of the Council was
held on 8 August 2001, and since then the Council has met on nine occasions and discussed a range of topics,
including linkages with local perinatal mortality committees, classification issues and endorsement of the
classification guidelines and specific maternal morbidities.
In addition, Council has continued to pursue and refine strategies to encourage clinicians to undertake
perinatal mortality reviews and determine and report on the clinical classification, in accordance with the
Australia and New Zealand Antecedent Classification of Perinatal Mortality (ANZACPM), and the Australia and
New Zealand Neonatal Death Classification (ANZNDC).
The Council has established two subcommittees:
1. The Perinatal Morbidity and Mortality Subcommittee which is chaired by Dr David Cartwright and has
two discrete working parties:
Mortality Working Party
Morbidity Working Party
2. The Maternal Morbidity and Mortality Subcommittee, which was chaired by Professor Michael
Humphrey from January 2002 until December 2002.
In 2000, 434 (80%) of 542 perinatal deaths were classified by hospital or regional perinatal mortality
committees with access to relevant data. Council applauds the support of clinicians in regional committees in
auditing perinatal deaths.
While the subcommittees continue to review and analyse mortality data, both subcommittees have taken up
the challenge of analysing morbidity data in an effort to identify opportunities for benchmarking and improving
clinical practice.
I would like to acknowledge and thank Mrs Wendy Rogash (Administration Officer), Mrs Joan Kennedy
(Principal Policy Officer), Mrs Susan Jenkins (Manager-Clinical Audit) and Mr Philip Baker (Epidemiologist)
from the Office of the Chief Health Officer for providing secretariat and epidemiological support.
Professor David Tudehope
Chairman, QMPQC
October 2003
�
�

Table of Contents
Preface ................................................................................................................................................ii
Chairman’s Report..............................................................................................................................iii
1 Introduction.........................................................................................................................................1
2 Membership........................................................................................................................................2
3 Executive Summary .............................................................................................................................3
4 Recommendations ..............................................................................................................................4
5 Maternal mortality ...............................................................................................................................5
5.1 Introduction................................................................................................................................5
5.2 Maternal Morbidity & Mortality Subcommittee Terms of Reference..............................................5
5.3 Definition of maternal mortality...................................................................................................5
5.4 Classification of maternal deaths ................................................................................................5
5.5 Classification of maternal deaths 2000.......................................................................................6
5.6 Maternal mortality ratios and trends ...........................................................................................6
5.7 Avoidable factors - maternal deaths 2000...................................................................................8
6 Maternal morbidity..............................................................................................................................9
7 Perinatal mortality .............................................................................................................................10
7.1 Modus operandi........................................................................................................................10
7.2 Clinical classification.................................................................................................................10
7.3 Data collection ..........................................................................................................................10
7.4 Definitions.................................................................................................................................11
7.5 Perinatal mortality rates and trends ...........................................................................................11
7.6 Comparison with Australian data...............................................................................................12
7.7 Cause specific perinatal mortality..............................................................................................13
7.8 Cause of neonatal death by ANZNDC .........................................................................................15
7.9 Multiple pregnancy ...................................................................................................................16
7.10 Indigenous perinatal mortality ..................................................................................................18
7.11 Gestational age and birth weight specific perinatal mortality rates............................................20
7.12 Perinatal autopsies ...................................................................................................................22
8 References ........................................................................................................................................32
9 Appendices .......................................................................................................................................33
9.1 Appendix 1: Perinatal Mortality and Morbidity Subcommittee ....................................................33
9.2 Appendix 2: Maternal Mortality and Morbidity Subcommittee....................................................33
9.3 Appendix 3: Australia and New Zealand Antecedent Classification of Perinatal Mortality
(ANZACPM) ...............................................................................................................................34
9.4 Appendix 4: Australia and New Zealand Neonatal Death Classification......................................36
9.5 Appendix 5: Perinatal Substance Use Special Interest Group .....................................................37
9.6 Appendix 6: Australia and New Zealand Perinatal Mortality Classification Special Interest
Group .......................................................................................................................................39
9.7 Perinatal Indigenous Network ...................................................................................................40
iv

v
L
L
ist of Figures
ist of Tables
Figure 1: Comparative maternal mortality ratios since 1988....................................................................6
Figure 2: Fetal, neonatal and perinatal mortality rates corrected for late terminations,
Queensland 1987 - 2000.........................................................................................................12
Figure 3: Perinatal mortality rates by usual residence of mother, Queensland and Australia,
1983 - 2000 ............................................................................................................................12
Figure 4: Perinatal mortality rate by plurality, Queensland 2000............................................................17
Table 1: Maternal mortality, Queensland 1988-2000 ............................................................................7
Table 2: Maternal mortality avoidable factors by classification .............................................................8
Table 3: Fetal, neonatal and perinatal deaths, Queensland 2000 ........................................................11
Table 4: Perinatal deaths by cause and type, Queensland 2000..........................................................13
Table 5: Neonatal deaths by cause (ANZNDC) and gestational age, Queensland 2000.........................15
Table 6: Neonatal deaths by cause (ANZNDC) and birth weight, Queensland 2000..............................16
Table 7: Perinatal deaths by plurality, Queensland 2000 ....................................................................16
Table 8: Perinatal deaths by cause and plurality, Queensland 2000 ....................................................17
Table 9: Fetal, neonatal and perinatal deaths, Queensland 2000........................................................18
Table 10: Perinatal deaths by cause and Indigenous status, Queensland 2000.....................................19
Table 11: Perinatal deaths by cause and gestational age, Queensland 2000 ........................................20
Table 12: Perinatal deaths by cause and birth weight, Queensland 2000 ..............................................21
Table 13: Perinatal autopsies by cause and type of death, Queensland 2000 .......................................22
Table 14: Perinatal mortality rates by gestational age, Queensland 2000..............................................23
Table 15: Perinatal mortality rates by birth weight, Queensland 2000...................................................24
Table 16: Perinatal deaths by cause, Queensland 2000........................................................................25
Table 17: Neonatal deaths by cause (ANZNDC), Queensland 2000 .......................................................30

1
1 Introduction
Purpose of the Council
Terms of Reference
The Queensland Maternal and Perinatal Quality Council was established following a review of the Queensland
Council on Obstetric and Paediatric Morbidity and Mortality (QCOPMM). The review found that the scope of
QCOPMM was too broad to enable appropriate consideration of maternal, perinatal and paediatric morbidity
and mortality. The establishment of a separate Maternal and Perinatal Quality Council with suitably focussed
Terms of Reference will provide greater opportunities to review and evaluate morbidity and mortality.
To provide advice to the Minister for Health and Director-General, Queensland Health, through the Chief Health
Officer, on matters relating to maternal and perinatal morbidity and mortality in Queensland.
Utilise the data from the Health Information Centre (HIC), national health guidelines, literature
reviews and members' expertise.
Identify appropriate indicators of quality.
Consider patterns and causation of morbidity and mortality in Queensland so that recommendations
may be made to reduce preventable death and disability.
Provide direction that will assist health providers in Queensland to develop policies that positively
impact on morbidity and mortality.
Identify avoidable factors associated with morbidity and mortality and advise on the implementation
of measures that could assist with the prevention of such deaths, including improvements in health
services.
Provide information and guidance required for members of the health professions and for the
community generally, in order to assist in the reduction of morbidity and mortality.
Co-opt relevant experts to advise the Council on issues related to their functions.
Advise on standards and quality of clinical care and assist with the extension of such standards in both
public and private sectors.
Advise on research directions.
Provide an annual report to the Minister and Director-General through the Chief Health Officer.
�
�
�
�
�
�
�
�
�
�

2 Membership
Membership of the Queensland Maternal and Perinatal Quality Council (QMPQC)
Ex-officio
Secretariat
Professor David Tudehope Director-Division of Neonatology, Mater Mothers’ Hospital
(Chairman)
Dr David Cartwright Director-Neonatology, Royal Women's Hospital
Dr Yogesh Chadha Director-Obstetrics and Gynaecology, Toowoomba Hospital and Health
Service District
Ms Rowena Chapman Member of SANDS (Consumer)
Professor Paul Colditz Neonatologist, Director-Perinatal Research Centre, Royal Women's
Hospital
Ms Sue Cornes Deputy Manager, Health Information Centre
Ms Lynne Dunne Vice-President, Queensland Branch, Australian College of Midwives
Dr John Evans General Practitioner, Emerald
Ms Vicki Flenady Perinatal Researcher, Centre for Clinical Studies, Women and Children's
Health, Mater Hospital
Professor Michael Humphrey Director-Obstetrics and Gynaecology, Cairns Base Hospital
(resigned 8/1/2003)
Ms Christian McClelland Women's Health Adviser, Queensland Health
Ms Heather McCosker Lecturer, School of Nursing, QUT
Dr Robyn McDermott Medical Epidemiologist, Tropical Public Health Unit, (Cairns), Queensland
Health
Professor Jeremy Oats Director - Obstetrics and Gynaecology, Mater Mothers’ Hospital
(resigned 25/9/2001)
Dr Diane Payton Staff Pathologist, QHPSS, Royal Brisbane and Royal Women’s Hospital and
Health Service District
Dr Nikki Whelan Obstetrician and Gynaecologist, Private Practice and VMO Royal Women's
Hospital
Dr John Wilson Senior Obstetrician, Royal Women's Hospital
(appointed 21/11/2001)
Professor Jennifer Batch Chairman, Queensland Paediatric Quality Council
Professor Bryan Campbell Chief Health Officer
Mr Philip Baker Clinical Audit Information Manager, Office of the Chief Health Officer
Mrs Susan Jenkins Clinical Audit Manager, Office of the Chief Health Officer
Ms Joan Kennedy Principal Policy Officer, Office of the Chief Health Officer
Ms Wendy Rogash Administration Officer, Office of the Chief Health Officer
2

3
3 Executive Summary
The overall maternal mortality rate in Queensland was 14.4 per 100,000 mothers, comprised of 2 direct deaths,
3 indirect deaths and 2 incidental deaths.
There were 49,138 births and 542 perinatal deaths in Queensland for 2000, giving a crude perinatal mortality
rate (PMR) of 11 per 1,000 total births. This was comprised of a fetal death rate of 7.3 per 1,000 total births and a
neonatal mortality rate (NMR) of 3.8 per 1,000 live births.
Since 1983, the rate of perinatal deaths in Queensland has been similar to that observed for Australia.
Preterm births (<37 weeks) accounted for 8.5% of infant and 81% of perinatal deaths. Very preterm births (<28
weeks) accounted for 0.9% of infant and 55% of perinatal deaths.
Twins and higher order multiple births accounted for 3.2% of births and 13% of all perinatal deaths. The rates
for multiple births are 5 times that of singleton births (48.2% v 9.8 per 1,000)
The main causes of death according to the ANZACPM were Congenital abnormality (22%), Unexplained
antepartum death (17.9%) and Spontaneous preterm (17.3%). The overall rate of Unexplained antepartum
death was 2.0 per 1,000 births, which is four times greater than the rate of SIDS.
Of all fetal deaths, 13% were attributed to voluntary interruption of pregnancy at 20 weeks gestation. Late
terminations of pregnancy have contributed to a 10% increase in the fetal death rate for the years 1994 to 2000.
In 2000, 6% of births were to Indigenous women, whilst 12% of perinatal deaths were in babies of Indigenous
women. The Indigenous perinatal mortality rate is 2.2 times higher than the non-Indigenous perinatal mortality
rate. The perinatal mortality rates for the Indigenous population were higher in most cause of death categories.
The cause of perinatal death accounting for most of the increased perinatal mortality in the Indigenous
population was Spontaneous preterm, which was more than three times more frequent than in the non-
Indigenous population. The categories of Unexplained antepartum death and Specific perinatal conditions
were more than twice as frequent in the Indigenous population.
The rate of perinatal autopsies for Queensland in 2000 was 39% which compares unfavourably with rates
observed elsewhere in Australia and overseas, and is well below the rate of 75% recommended by the Royal
College of Obstetricians and Gynaecologists and the Royal College of Pathologists.

4 Recommendations
Recommendation 1
Recommendation 2
Recommendation 3
Recommendation 4
Recommendation 5
Recommendation 6
Recommendation 7
Recommendation 8
Recommendation 9
Health professionals should be made aware that pregnancy could be the cause of symptomatic hypertension
in a young woman. If such a woman is found to be pregnant, referral to a specialist obstetrician is appropriate
for investigation, treatment and, if necessary, admission to hospital for monitoring.
Every perinatal death should be reviewed by a local or regional multi-disciplinary clinical committee (including
a pathologist), with direct access to all relevant information. The committee should classify cause of death
according to the Australia and New Zealand Antecedent Classification of Perinatal Mortality (ANZACPM) and
the Australia and New Zealand Neonatal Death Classification (ANZNDC).
To assist clinicians in ANZACPM and ANZNDC classification of perinatal mortality, education programs should
be provided to enable clinicians to ensure accurate completion of the MR63d, confidential perinatal mortality
summary form, perinatal death certificate (Form T) and MR66.
Clinicians should consider the potential value of an autopsy examination in every instance of perinatal death,
and should discuss this with the parents. Clinicians are reminded that when perinatal autopsies are
requested, placental pathology must be included to ensure that the report is complete.
When determining the clinical classification of Specific Perinatal Conditions Antepartum Cord Complications
(Category 6.3), there must be evidence of some or all of the following:
Petechiae distant to the site of complications
Clotting in the cord vessels at site of complications
Distinct indentation around infant or persisting indentations of cord when knot is untied
Differential congestion on either side of the complications
Comprehensive guidelines for review and investigation of fetal deaths should be developed. Further research
and strategies aimed at reducing the risk of unexplained antepartum death should be supported.
A comprehensive congenital abnormality register should be established, which includes notification of
congenital abnormalities resulting in early termination of pregnancy and those detected within the first two
years of life.
The higher rates of perinatal mortality in the Indigenous population highlight the need for continued focussed
research and strategies to reduce this imbalance.
Comprehensive clinical guidelines should be developed for investigation of unexplained antepartum deaths,
which should include an epidemiological analysis on a complete cohort of unexplained antepartum deaths.
�
�
�
�
4

5
5 Maternal mortality
5.1 Introduction
5.2 Maternal Morbidity & Mortality Subcommittee Terms of Reference
5.3 Definition of maternal mortality
5.4 Classification of maternal deaths
Maternal mortality survey is one of the oldest recorded forms of medical care audit. The Maternal Mortality and
Morbidity Sub-Committee of the Queensland Maternal and Perinatal Quality Council, enquired confidentially
into all known maternal deaths in Queensland in 2000. This report contains a review of seven maternal deaths
from 2000, along with a previously unclassified death from 1999.
Contribute to the reduction of preventable maternal mortality and morbidity in Queensland.
Identify and review all maternal deaths in Queensland.
Classify all maternal deaths as to cause and presence of avoidable factors.
Collaborate with the clinical audit managers in the identification and review of all maternal deaths.
Report on patterns and trends of maternal mortality and morbidity in Queensland.
Report information and recommendations to the Queensland Maternal & Perinatal Council.
Identify areas for research into various aspects pertaining to maternal mortality and morbidity.
Liaise with other state and national bodies to monitor maternal mortality and morbidity.
Revise the terms of reference and activities of the subcommittee in response to changing trends and
circumstances.
A maternal death is defined by the World Health Organisation (WHO) as:
The definition used in this report includes, in addition to the WHO definition, incidental deaths and deaths
occurring more than 42 days after termination of pregnancy, when their origin and illness related to the
pregnancy.
It is noted that the most recent 'Report on Maternal Deaths in Australia', for the period 1994 to 1996, used the
definition of 'death of a woman while pregnant or within 42 days of termination of pregnancy'.
are those that result from obstetric complications of the pregnant state (pregnancy, labour and
puerperium) including deaths from interventions, omissions, inappropriate treatment or from a chain of events
resulting from any of the above. They are complications of pregnancy itself.
are those which result from pre-existing disease or disease that developed during pregnancy
and were not due to direct obstetric causes, but which may have been aggravated by physiological effects of
pregnancy.
are those due to conditions occurring during pregnancy, where the pregnancy is unlikely to
have contributed significantly to the death, although it is sometimes possible to postulate a distant
association.
�
�
�
�
�
�
�
�
�
'the death of a woman while pregnant or within 42 days of termination of pregnancy,
irrespective of the duration and the site of the pregnancy, from any cause related to
or aggravated by the pregnancy or its management.'
Direct deaths
Indirect deaths
Incidental deaths

5.5 Classification of maternal deaths 2000
5.6 Maternal mortality ratios and trends
There were seven maternal deaths in Queensland in the year 2000. This report also notes a maternal death
from 1999, which was not able to be classified at the time of publication of the 1999 report of the Queensland
Council on Obstetric and Paediatric Morbidity and Mortality.
Of the two direct maternal deaths in 2000, one was due to intracerebral haemorrhage secondary to severe pre-
eclampsia and the other was due to a massive intra-abdominal haemorrhage of unknown source.
Three deaths were classified as indirect maternal deaths and were due to: congestive cardiac failure secondary
to mitral valve disease; subdural haemorrhage secondary to domestic violence; intracerebral haemorrhage:
renal failure secondary to sporadic thrombotic thrombocytopaenic purpura of unknown cause. The previously
unreported death from 1999 was also classified as an indirect maternal death and, although the cause of death
was not clearly identified, it was thought likely to be associated with hypoglycaemia secondary to treatment for
diabetes mellitus.
There were two incidental maternal deaths, one of which was due to homicide. The cause in the second death
was not apparent.
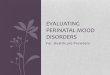
In situations where numerators are small and denominators are large, as with maternal mortality ratios,
interpretation is difficult as small numerator variations lead to large alterations in such ratios. The overall
maternal mortality ratio for Queensland for 2000 was 14.4 per 100,000 mothers (Table 1). This is similar to the
national ratio of 13.0 per 100,000 for the triennium 1994-1996 (Figure 1).
1. Queensland Council on Obstetric and Paediatric Morbidity and Mortality. 1999 Report. Brisbane:
Queensland Health.
2. Advisory Committee on Maternal Mortality and Morbidity, NHMRC. Report on Maternal Deaths in
Australia, 1994-1996. Canberra: NHMRC.
Figure 1:Comparative maternal mortality ratios since 1988
Data sources:
6
0
5
10
15
20
25
30
35
1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Ma
tern
al
mo
rta
lity
rati
o
pe
r1
00
,00
0m
oth
ers
.
Queensland annual reports
Queensland triennia reports
Australian triennia reports

7
Table 1: Maternal mortality, Queensland 1988-2000
Data sources:
Deaths
Year Total Direct Indirect Incidental All deaths
Mothers n ratio n ratio n ratio n ratio
1988 40,628 1 2.5 1 2.5 3 7.4 5 12.3
1989 42,296 3 7.1 0 0.0 1 2.4 4 9.5
1990 44,467 2 4.5 0 0.0 1 2.2 3 6.7
1991 44,131 2 4.5 2 4.5 3 6.8 7 15.9
1992 46,073 0 0.0 3 6.5 3 6.5 6 13.0
1993 46,765 3 6.4 1 2.1 6 12.8 10 21.4
1994 47,356 5 10.6 2 4.2 3 6.3 10 21.1
1995 47,864 5 10.4 3 6.3 2 4.2 10 20.9
1996 47,302 1 2.1 0 0.0 5 10.6 6 12.7
1997 47,163 4 8.5 2 4.2 3 6.4 9 19.1
1998 47,450 0 0.0 0 0.0 4 8.4 4 8.4
1999 48,044 4 8.3 3 6.2 6 12.5 13 27.1
2000 48,524 2 4.1 3 6.2 2 4.1 7 14.4
1. Queensland Council on Obstetric and Paediatric Morbidity and Mortality.
2. Queensland Maternal & Perinatal Quality Council & Perinatal Data Collection, Data Services Unit,
Queensland Health
1 1 1 1
1 per 100,000 mothers

5.7 Avoidable factors - maternal deaths 2000
Avoidable factors
These are defined as departures from the accepted standard of satisfactory care that may have played a part in
the death. It is not suggested that in cases in which avoidable factors are considered present (Table 2), death
could certainly have been averted; such judgements indicate that the subcommittee considered that the risk of
death could have been reduced had the management been different. Avoidable factors were thought to be
related to clinical care, to the setting in which the treatment was provided, to factors associated with the
woman not complying with treatment, or to the social setting within which the pregnancy occurred.
The Maternal Morbidity and Mortality Sub-Committee of the QMPQC agreed that avoidable factors were
present when departures from accepted standards of care occurred and, if such departure had not occurred,
the outcome may have been different. In four of the eight cases reviewed in this report (50%), avoidable factors
were thought to be present. However, please note that more than one factor was noted to be present in one
case.
Whilst these numbers are small, and conclusions from small numbers are unreliable, this incidence of
potentially avoidable factors is similar to that reported in the most recently available Australian report (42% in
the 1994 1996 triennium).
Factor Direct Indirect Incidental Total
n=2 n=3 n=2 n=7
Clinical care Failure to diagnose Significant proteinuria - 2
severe pre-eclampsia. not effectively investigated
immediately.
Clinical setting Lack of continuous access - - 1
to appropriately trained
health professionals.
Woman Concealment of pregnancy Non-compliance with - 2
treatment
Social setting Inability to manage - 1
adequate contraception in
a setting where domestic
violence prevailed.
Total factors 3 factors in 2 deaths 3 factors in 3 deaths 6
Total deaths 2 3 2 7
7 maternal deaths from the year 2000 and 1 maternal death from 1999.
(More than one factor was recognised in some deaths)
Table 2: Maternal mortality avoidable factors by classification
8

9
6 Maternal morbidity
Recognising that maternal death is a rare complication of pregnancy in Queensland, the subcommittee
considered the possibility of examining the incidence of serious episodes of maternal morbidity. Surprisingly,
the subcommittee members were unable to find significant state or national maternal mortality and morbidity
bodies with experience in these matters, due to the perceived difficulties of reliable data collection and review.
In considering topics for initial investigation, the subcommittee took particular note of frequent causes of
maternal death and of causes of maternal morbidity, where evidence exists that such morbidity is potentially
preventable in some cases. The subcommittee has undertaken a co-operative review of data sources and their
reliability, with staff of the Office of the Chief Health Officer and of the Health Information Centre of Queensland
Health.
Topics under consideration for future reporting include:
Wound infection, hysterectomy, unintended damage to urinary or gastro-intestinal tract, the need for
blood transfusion and re-admission to hospital in association with birth via caesarean section.
Thrombo-embolic complications of pregnancy, including deep vein thrombosis and pulmonary
embolism.
Significant anaemia associated with pregnancy and birth.
Antepartum and postpartum haemorrhage.
Major complications of pre-eclampsia.
New admissions to intensive care, coronary care and renal dialysis units relating to pregnancy and
birth.
�
�
�
�
�
�

7 Perinatal mortality
7.1 Modus operandi
7.2 Clinical classification
7.3 Data collection
All perinatal deaths in Queensland are subject to a systematic review. Perinatal mortality data have been
obtained from the Perinatal Data Collection (PDC - Queensland Health), the Registrar General for Births Deaths
and Marriages and case summaries from hospital and regional perinatal mortality committees in Queensland.
During 2000, a number of local mortality committees collaborated with the Council in the perinatal mortality
review process. The working party of the Perinatal Morbidity & Mortality Subcommittee received case
summaries and cause of death classifications assigned by these committees for 80% of perinatal deaths
occurring in 2000.
The Terms of Reference for the subcommittee are:
Review and report on patterns and trends of perinatal morbidity and mortality.
Support and guide clinicians in clinical audit activities, including classification of perinatal deaths
and important perinatal morbidity.
Determine and report on preventable factors.
Liaise with appropriate national and local bodies in the identification of clinical indicators.
Identify evidence-based health care interventions which may reduce morbidity and mortality.
Identify strategies for dissemination of information to clinicians.
Identify research priorities into perinatal morbidity and mortality.
All perinatal deaths in the year 2000 were classified according to the primary cause of death using the new
Australia and New Zealand clinical classification systems - the Australia and New Zealand Antecedent
Classification of Perinatal Death (ANZACPM) and in addition for neonatal deaths, the Australia and New
Zealand Neonatal Death Classification (ANZNDC). These classifications replace the clinical classification
systems used by the Council in previous years: the obstetric antecedent classification Queensland Council
Perinatal Mortality Classification (QCPMC) for all perinatal deaths and the Neonatal Mortality Classification for
all neonatal deaths. The main difference between the current obstetric antecedent classification (ANZACPM)
and the previous QCPMC, is the removal of a specific category for multiple pregnancy. Perinatal deaths in
multiple pregnancies are now classified according to the condition causing the death (eg Twin-twin
transfusion, Hypertension etc). There is very little difference between the previous neonatal death
classification and the current ANZNDC.
The Council acknowledges and thanks the clinicians who have participated in local mortality review and
classification.
The Council has established a perinatal mortality working party. Two of the functions of this working party are to
classify those deaths not classified at the local level and to conduct a quality review of classifications applied
to perinatal deaths at facility/local committee level.
The purpose of classifying deaths according to the ANZACPM and ANZNDC systems is to focus on aetiology, to
enable consideration of preventable factors associated with perinatal deaths through the systematic
application of clinically relevant categories to large populations. (Further information about the classification
systems is to be found in Appendices 3 and 4).
Perinatal mortality data have been obtained from the Perinatal Data Collection (PDC) Queensland Health, the
Registrar General for Births Deaths and Marriages and from hospital and regional perinatal mortality
committees in Queensland. The major data sources are the Perinatal Data Collection Forms (MR63d), the
Medical Certificate of Cause of Perinatal Death (Form T), the Council's Confidential Perinatal Mortality Case
Summary Form and the autopsy and placental pathology report when available.
Perinatal deaths are notified by the Registrar General’s Office to the Perinatal Data Collection (PDC), Data
Services Unit of Queensland Health. The Chief Health Officer then requests that a copy of the autopsy and other
relevant material be sent to the PDC to facilitate classification by the Perinatal Mortality Working Group. The
�
�
�
�
�
�
�
10

11
Council secretariat collates and makes available all information on the deaths for review by the Perinatal
Mortality Working Group
During 2000, a number of regional/facility committees collaborated with the Council in the perinatal mortality
review process. The Council received case summaries and cause of death classifications assigned by these
Committees for 80% of perinatal deaths occurring in 2000.
Defined in the as:
Defined in the as:
The death of an infant within 28 days of birth.
The death of an infant under one year of age and includes neonatal deaths and postneonatal deaths up to 1
year.
The number of fetal and neonatal deaths per 1,000 total births.
The number of fetal deaths per 1,000 total births.
The number of deaths of live born infants under 28 days of age per 1,000 live births.
The number of deaths of infants under one year of age per 1,000 live births.
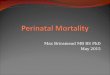
The crude perinatal mortality rate (PMR) for Queensland for the year 2000 was 11.0 per 1,000 total births (Table 3)
comprised of a fetal death rate of 7.3 per 1,000 total births and a neonatal mortality rate (NMR) of 3.8 per 1,000
live births. The total number of births in Queensland increased by 569, from 48,749 in 1999 to 49,318 in 2000.
The small reduction in PMR experienced in 1999 compared with 1994-1998 was sustained in 2000. The fetal
death component of 65.4% of perinatal deaths was similar to previous years. Data on late terminations of
pregnancy (>20 weeks gestation) as a result of voluntary interruption of pregnancy, have been collected since
1994. In the year 2000, voluntary interruption pregnancy contributed 19.4% (37) to the total fetal deaths. It
should be noted, as in previous years, many of the deaths in this category can be attributed to women whose
place of usual residence was outside Queensland. When these fetal deaths are removed from annual
statistics, there is no increase in the fetal death rate. (Figure 2)
Total Live Fetal deaths Neonatal deaths Perinatal deathsbirths births n rate n rate n rate
All Queensland 49,318 48,960 358 7.3 184 3.8 542 11.0
(CI 6.5-8.0) (CI 3.3-4.4) (CI 10.1-11.9)
Perinatal Data Collection, Data Services Unit, Queensland Health
Registration of Births, Deaths, and Marriages Act, 1962
'a child whose heart has not beaten after it has been completely expelled or extracted from its mother and
who is either of not less than 20 weeks gestation or of not less than 400g by weight at birth'.
Registration of Births, Deaths and Marriages Act, 1962
'a child whose heart has beaten after it has been completely expelled or extracted from its mother'.
Table 3: Fetal, neonatal and perinatal deaths, Queensland 2000
Data source:
1 2
1
1
2
per 1,000 births (95% confidence interval)
per 1,000 live births (95% confidence interval)
7.4 Definitions
7.5 Perinatal mortality rates and trends
Fetal death
Live birth
Neonatal death
Infant death
Perinatal mortality rate
Fetal death rate
Neonatal mortality rate
Infant mortality rate

Figure 2: Fetal, neonatal and perinatal mortality rates corrected for late terminations, Queensland1987-2000
Data source:
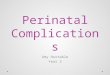
Figure 3: Perinatal mortality rates by usual residence of mother, Queensland and Australia, 1983-2000
Perinatal Data Collection, Data Services Unit, Queensland Health
Differences exist in definitions and reporting practices between the Australian Bureau of Statistics (ABS) and
the Perinatal Data Collection (PDC), making interstate and national comparisons difficult. For example, the
ABS reports deaths of infants according to the place of usual residence, whereas PDC reports deaths of all
infants born in Queensland. The ABS includes fetal deaths where the birth weight was at least 400g the
gestational age was 20 weeks, whereas PDC uses the definition found in the
(birth weight at least 400g the gestational age was 20 weeks).
Figure 3 compares the PMR for Queensland and Australian residents using ABS definitions and data.
Between 1983 and 2000, the Australian PMR declined from 12.6 to 8.3 deaths per 1,000 births and similarly,
the Queensland PMR declined from 12.8 to 8.9 deaths per 1,000 births. Analysis of perinatal mortality by usual
residence of the mother (ABS definition), shows Queensland rates are much closer to the Australian rate (8.9
deaths per 1,000 births vs 8.3 deaths per 1,000 births) than the PDC Queensland rate (of 11.0 deaths per 1,000)
which includes perinatal deaths of mothers from other states. Small year-to-year fluctuations exist between
the Queensland state rate and the Australian rate which should be interpreted with caution. There was no
statistical difference between Queensland and Australian perinatal, fetal and neonatal death rates for the year
2000 (p > 0.05; binomial exact test).
Data source: ABS Causes of deaths, Australia 2000
and
�
�
Registration of Birth, Deaths and
Marriages Act, 1962 or
1rates per 1,000 births (based on 400 grams/20 weeks definition)
7.6 Comparison with Australian data
12
0
2
4
6
8
10
12
14
16
1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000
Year
pe
r1
00
0b
irth
s
Fetal deaths
Neonatal deaths
Perinatal deaths
FD - TOP
PND - TOP

13
7.7 Cause specific perinatal mortality
Cause of perinatal deaths by ANZACPM
Congenital abnormalities (Category 1)
The main causes of death using the Australia and New Zealand Antecedent Classification of Perinatal Mortality
(ANZACPM) clinical classification system, are illustrated in Table 4. The three leading causes of perinatal
deaths were Congenital abnormalities (22.4%), Unexplained antepartum death (17.9%) and Spontaneous
preterm (17.3%) which cumulatively account for 57.8% of all deaths.
Other significant contributions were Specific perinatal conditions (9.8%), Antepartum haemorrhage (8.3%)
and Hypertension (5.4%). The main causes for neonatal deaths were Congenital abnormality (33.2%) and
Spontaneous preterm (28.8%). The main causes of fetal death were Unexplained antepartum death (27.1%)
and Congenital abnormality (16.8%).
Type of Perinatal death
Cause of death Fetal death Neonatal death Total
(ANZACPM) n % rate n % rate n % rate
1. Congenital abnormality 60 16.8 1.2 61 33.2 1.2 121 22.3 2.5
2. Perinatal infection 7 2 0.1 5 2.7 0.1 12 2.2 0.2
3. Hypertension 16 4.5 0.3 13 7.1 0.3 29 5.4 0.6
4. Antepartum haemorrhage 27 7.5 0.5 18 9.8 0.4 45 8.3 0.9
5. Maternal conditions 45 12.6 0.9 4 2.2 0.1 49 9 1
6. Specific perinatal conditions 37 10.3 0.8 16 8.7 0.3 53 9.8 1.1
7. Hypoxic peripartum deaths 9 2.5 0.2 6 3.3 0.1 15 2.8 0.3
8. Fetal growth restriction 16 4.5 0.3 4 2.2 0.1 20 3.7 0.4
9. Spontaneous preterm 41 11.5 0.9 53 28.8 1.1 94 17.3 1.9
10. Unexplained antepartum death 97 27.1 2 0 0 0 97 17.9 2
11. No obstetric antecedent 2 0.6 0 4 2.2 0.1 6 1.1 0.1
Not classified 1 0.3 0 0 0 0 1 0.2 0
Total 358 100 7.3 184 100 3.8 542 100 11.0
Perinatal Data Collection, Data Services Unit, Queensland Health
Of the 121 perinatal deaths classified as Congenital abnormalities, there were 60 fetal deaths and 61 neonatal
deaths.
The most frequent Congenital abnormalities were central nervous system (28), cardiovascular system (24),
chromosomal (18), and other multiple congenital abnormality (30) (Table 16).
Overall, 71 of the 121 deaths (59%) were the result of a single system defect.
Overall, Congenital abnormalities contributed to 22.3% of all perinatal deaths in 2000, (2.5 per 1,000 total
births). This rate has not changed in Queensland since cause specific analyses were conducted in 1994.
These rates are considerably higher than those reported for Australia, where Congenital abnormalities
accounted for 18% of perinatal deaths in 1996 at a rate of 1.6 per 1,000 total births. (Source: Australian Institute
for Health and Welfare)
Table 4: Perinatal deaths by cause and type, Queensland 2000
Data source:
1 2 1
1
2
rate per 1,000 births
rate per 1,000 live births

Central nervous system (CNS)
Congenital cardiovascular system abnormalities
Hypertension (Category 3)
Antepartum haemorrhage (Category 4)
Maternal conditions (Category 5)
Specific perinatal conditions (Category 6)
Spontaneous preterm (<37 weeks gestation) (Category 9)
Unexplained antepartum death (Category 10)
The majority of the 28 deaths from CNS abnormalities were due to neural tube defects. No data are available
on terminations of pregnancy prior to 20 weeks gestation for neural tube defects. Data are also lacking on
folate ingestion for the 28 women whose babies had lethal CNS malformations. This lack of information is a
major barrier to monitoring the rate of central nervous system congenital malformations, and renders it
impossible to gauge the effectiveness, or otherwise, of the public health program of peri-conceptual folate
supplementation.
There were 24 (4.4%) perinatal deaths attributed to this category in 2000, which is similar to 1998 and 1999
(4.2%).
In the year 2000, there were 28 perinatal deaths (5.2% of all perinatal deaths) attributed to hypertension,
compared to 16 in 1998 and 9 in 1999. Whether this represents a genuine increase in deaths due to
hypertension, or a change in classification is difficult to assess.
There were 45 perinatal deaths attributed to Antepartum haemorrhage (8.3% of all perinatal deaths), the
majority being due to placental abruption (32) and 11 of undetermined origin. There were two deaths
attributed to placenta praevia and none to vasa praevia.
In the year 2000, there were 49 perinatal deaths (6.8% of all perinatal deaths). Thirty-seven (37) perinatal
deaths were assigned to the category of Voluntary interruption of pregnancy. This category specifically
excludes termination of pregnancy relating to major Congenital abnormalities. There appears to be a
progressive increase in this category, with 30 in 1998, 35 in 1999 and 37 in 2000.
This group contributed 53 (9.3%) to all perinatal deaths. The main contributing conditions were Twin/twin
transfusion (23), and Uterine abnormalities (13). In 1998, there were 16 perinatal deaths attributed to
Twin/twin transfusion (2.9% of all perinatal deaths), and only 8 (1.5%) in 1999. The increase in 2000 may have
resulted from elective referral patterns to maternal fetal medicine units, improved accuracy with diagnosis
and/or changes in the classification system used. The 13 deaths due to Uterine abnormalities include deaths
resulting from bi-cornuate uterus and cervical incompetence.
Preterm birth accounted for 8.5% of all births and 81% of perinatal deaths, of which 44% were fetal deaths and
56% neonatal deaths. Of the 437 preterm deaths, 94 (17.3%) of all perintal deaths were assigned to the
category of Spontaneous preterm as there were no other identified antecedents. There has been no reduction
in the rate of preterm birth over the past 10 years in Queensland.
There were 97 perinatal deaths attributed to unexplained antepartum death, accounting for 27.1% of fetal
deaths and 17.9% of all perinatal deaths. In only 61 of 97 cases (62.9%) was there an autopsy and in 4 cases
there was not a formal examination of placenta.
The overall rate of unexplained fetal death is 2.0 per 1,000 births, which is greater than the rate of Sudden
Infant Death Syndrome. (Reference Paediatric Council Report.)
Of the 97 Unexplained antepartum deaths, 27 (28%) occurred at <28 weeks gestation, 29 (30%) at 28-36 weeks
gestation and 41 (42%) at 37 weeks. For the first time, systematic information was collected on placental
pathology (Table 16) for this category. This revealed evidence of utero-placental insufficiency in 16%-18% of
cases, the relevance of which is uncertain.
Analysis is currently underway in Queensland Health to identify the epidemiological factors associated with
Unexplained antepartum deaths for the years 1994 to 2000.
�
14

15
7.8 Cause of neonatal death by ANZNDC
Extreme prematurity (Category 2)
Cardio-respiratory (Category 3)
Infection (Category 4)
Neurological (Category 5)
Gastrointestinal (Category 6)
Of the 184 neonatal deaths (Tables 5 & 17), 65 (35.3%) were due to Congenital abnormality, 48 (26.1%), to
Extreme prematurity and 29 (15.8%) to Cardio-respiratory disorders. Other causes were Neurological (16
deaths - 8.7%) and Infection (12 deaths - 6.5%). There were four more neonatal deaths attributed to Congenital
abnormality in the ANZNDC classification than in the obstetric antecedent classification of ANZACPM. The
purpose of the neonatal death classification is to identify the most important factor occurring at, or after, the
birth of the baby, which triggers the cascade of events leading to eventual neonatal death. For this reason,
there may be differences in the congenital abnormality numbers between ANZACPM and ANZNDC
classifications.
Gestational age (weeks)
Cause of death <28 28-36 37+ Total
(Neonatal classification) n % n % n % n %
1. Congenital abnormality 15 15 27 56.2 23 64.9 65 35.3
2. Extreme prematurity 46 46.0 2 4.2 0 0.0 48 26.1
Not resuscitated 43 43.0 2 4.2
Unsuccessful resuscitation 3 3.0 0 0.0
3. Cardio-respiratory disorders 23 23.0 5 10.4 2 2.8 29 15.8
4. Infection 6 6.0 3 6.2 3 8.3 12 6.5
5. Neurological 5 5.0 5 10.4 6 16.7 16 8.7
6. Gastrointestinal 2 2.0 2 4.2 1 2.8 5 2.8
7. Other 3 3.0 4 8.3 2 5.6 9 4.9
Total 100 100 48 100 36 100 184 100
Perinatal Data Collection, Data Services Unit, Queensland Health
Deaths from extreme prematurity (typically infants <24 weeks gestation of <600g birth weight) were reported in
48 cases (Table 6), predominantly in infants who were considered to be pre-viable and not resuscitated (45),
with only three infants having an unsuccessful resuscitation.
Cardio-respiratory disorders contributed to 29 neonatal deaths, with 20 babies dying as a result of hyaline
membrane disease. The single death attributed to chronic neonatal lung disease highlights the difficulty with
definition of this sub-category because this diagnosis is usually restricted to babies beyond 28 days of age.
The low rate of acquired bacterial (nosocomial) infections occurring in only eight babies does not fully
represent the contribution to neonatal deaths by this complication. There were two neonatal deaths due to
congenital bacterial infection. Unlike the ANZACPM classification, the neonatal classification does not identify
causative organism.
There were 16 neonatal deaths assigned to this category, of which 11 were due to hypoxic ischaemic
encephalopathy and 5 to intracranial haemorrhage.
There were five deaths attributed to necrotising enterocolitis, four of which were low birth weight babies.
Table 5: Neonatal deaths by cause (ANZNDC) and gestational age, Queensland 2000
Data source:

Other (Category 7)
7.9 Multiple pregnancy
In 2000, there was one neonatal death attributed to SIDS (at <day 28 of life), compared to four in 1999.
However, there were seven deaths attributed to other causes (Category 7.8 see Appendix 4). Of these, four
were of <28 weeks gestation. The obstetric antecedent classification (ANZACPM) categories assigned to these
deaths are as follows: Twin/twin transfusion in three deaths; Idiopathic hydrops in a further two deaths;
Spontaneous preterm in one death; and No obstetric antecedent-other, for the remaining death which was
ascribed to a sleeping accident.
Birth weight (g)
Cause of death <1000 1000-2499 2500+ Total
(Neonatal classification) n % n % n % n %
1. Congenital abnormality 16 15.7 25 53.2 24 64.9 65 35.3
2. Extreme prematurity 46 45.1 2 4.3 0 0.0 48 26.1
Not resuscitated 44 43.1 1 2.1 0 0.0 45 24.5
Unsuccessful resuscitation 2 2.0 1 2.1 0 0.0 3 1.6
3. Cardio-respiratory disorders 23 22.5 5 10.6 1 2.7 29 15.8
4. Infection 7 6.9 3 6.4 2 5.4 12 6.5
5. Neurological 4 3.9 5 10.6 7 18.9 16 8.7
6. Gastrointestinal 2 2.0 2 4.3 1 2.7 5 2.7
7. Other 4 3.9 3 6.4 2 5.4 9 4.9
Total 102 100 47 100 37 100 184 100
Perinatal Data Collection, Data Services Unit, Queensland Health
In the year 2000, there were 1,556 births from multiple pregnancies, contributing to 3.16% of all births. The
incidence of twins in 2000 was 2.9% with a PMR of 47.1 per 1,000 births (Table 7, Figure 4). The incidence of
triplets and higher order multiples was 0.18% with a PMR of 67 per 1,000 births. Overall, multiple births
contributed to 75 of the 542 perinatal deaths (13%) with a PMR of 66.7.
The main causes of perinatal deaths in singleton births were Congenital abnormality, Unexplained antepartum
deaths and Spontaneous preterm. The main causes of perinatal deaths in multiple births were Specific
perinatal conditions, Spontaneous preterm and Congenital abnormalities.
Total Live Fetal deaths Neonatal deaths Perinatal deaths
Plurality births births n rate n rate n rate
Singleton 47,762 47,436 326 6.8 141 3.0 467 9.8
Twins 1,466 1,438 28 19.1 41 28.5 69 47.1
Triplets or higher 90 86 4 44.4 2 23.3 6 66.7
Total multiple 1,556 1,524 32 20.6 43 28.2 75 48.2
Total 49,318 48,960 358 7.3 184 3.8 542 11.0
Perinatal Data Collection, Data Services Unit, Queensland Health
Table 6: Neonatal deaths by cause (ANZNDC) and birth weight, Queensland 2000
Data source:
Table 7: Perinatal deaths by plurality, Queensland 2000
Data Source:
1 2 1
1
2
rate per 1,000 births
rate per 1,000 live births
16

17
Figure 4: Perinatal mortality rate by plurality, Queensland 2000
Data source:
Table 8: Perinatal deaths by cause and plurality, Queensland 2000
Data source:
.
Perinatal Data Collection, Data Services Unit, Queensland Health
Cause of death Singleton Multiple
(ANZACPM) n % rate n % rate RR (95% CI)
1. Congenital abnormality † 109 23.3 2.3 12 16.0 7.7 3.34 (1.7-6.1)
2. Perinatal infection 12 2.6 0.3 0 0.0 0.0 0.00 (0.0-11.0)
3. Hypertension † 17 3.6 0.4 12 16.0 7.7 21.7 (9.4-48.1)
4. Antepartum haemorrhage 42 9.0 0.9 3 4.0 1.9 2.2 (0.4-6.9)
5. Maternal conditions 49 10.5 1.0 0 0.0 0.0 0.0 (0.0-2.4)
6. Specific perinatal conditions † 31 6.6 0.6 22 29.3 14.1 21.8 (12.0-38.9)
7. Hypoxic peripartum deaths 14 3.0 0.3 1 1.3 0.6 2.2 (0.1-14.4)
8. Fetal growth restriction 19 4.1 0.4 1 1.3 0.6 1.6 (0.1-10.2)
9. Spontaneous preterm † 72 15.4 1.5 22 29.3 14.1 9.4 (5.5-15.3)
10. Unexplained antepartum death 95 20.3 2.0 2 2.7 1.3 0.6 (0.1-2.4)
11. No obstetric antecedent 6 1.3 0.1 0 0.0 0.0 0.0 (0.0-26.1)
Not classified 1 0.2 0.0 0 0.0 0.0 0.0
Total † 467 100.0 9.8 75 100.0 48.2 4.9 (3.8-6.3)
Perinatal Data Collection, Data Services Unit, Queensland Health
1 1 2
1
2
per 1,000 births
RR relative risk with 95% confidence intervals
† mortality rates for singleton and multiple birth statistically different using Fisher's Exact (P < 0.05)
total includes one unclassified death
9.8
47.1
66.7
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
Singleton Twins Triplets or higher
Plurality
pe
r1
00
0b
irth
s

7.10 Indigenous perinatal mortality
In the year 2000, there were 2,843 births to Indigenous women, contributing to 5.8% of total births. The term
Indigenous refers to an Aboriginal or Torres Strait Islander person. The definition of an Aboriginal or Torres
Strait Islander person, as accepted by Queensland Health and other agencies including the Commonwealth
Government, is: “a person of Aboriginal/Torres Strait Islander descent who identifies as an Aboriginal or Torres
Strait Islander, and is accepted as such by the community in which he or she lives.” In this report, an
Indigenous birth is one that occurs to an Indigenous woman as defined above. Although there are differences
between the two groups that should be considered for health policy, they are grouped together for statistical
purposes. There were 65 perinatal deaths, with an overall PMR of 22.9 per 1,000 total births comprising 46 fetal
deaths (16.2 per 1,000 total births) and 19 neonatal deaths (6.8 per 1,000 live births).
From the period 1994 to 1996, the overall PMR was 24.2, comprised of a fetal death rate of 15.4 and an NMR of
8.9 per 1,000; in 1998, the comparable figures were 21.4, 12.3 and 9.2 respectively, and in 1999, 16.6, 9.7 and
7.0 respectively. Overall, there has been no improvement in the closure of the gap between Indigenous women
and non Indigenous women. The relative risk for perinatal mortality in the Indigenous population in
comparison with non Indigenous women is 2.2 (95% confidence intervals, 1.7 to 2.9). The absolute risk
difference is 12.6 per 1,000. This absolute risk difference estimates 179 deaths over a 5 year period (95% CI 99-
258)(see Table 9). These rates may be low as they are based only on the mother's status.
Table 9 illustrates the number of Indigenous deaths that could potentially be avoided if the Indigenous
mortality rate were the same as the non Indigenous mortality rate over 5 years.
Total Live Fetal deaths Neonatal deaths Perinatal deathsbirths births n rate n rate n rate
Indigenous 2,843 2,797 46 16.2 19 6.8 65 22.9
(11.9-21.5) (4.1-10.6) (17.7-29.0)
Not Indigenous 46,465 46,154 311 6.7 165 3.6 476 10.2
(6.0-7.5) (3.0-4.2) (9.3-11.2)
Relative risk for 2.4 1.9 2.2
Indigenous (1.8-3.3) (1.2-3.1) (1.7-2.9)
Absolute risk 9.5 3.2 12.6
difference for (4.8-14.2) (0.1-6.3) (7.0-18.2)
Indigenous
5-year 134 (68-201) 45 (1-88) 179 (99-258)
potentially avoidable
Indigenous deaths
Perinatal Data Collection, Data Services Unit, Queensland Health
Table 9: Fetal, neonatal and perinatal deaths, Queensland 2000
Data source:
4
1 2 1
3
5
1
2
3
4
5
rate per 1,000 births (95% confidence interval)
rate per 1,000 births (95% confidence interval)
Neither Australian Aboriginal nor Torres Strait Islander, total births excludes 10 live births where the Indigenous status was not stated
Indigenous and not Indigenous death figures exclude one fetal death where the Indigenous status was not stated
The number of Indigenous deaths that could potentially be avoided if the Indigenous mortality rate were the same as the not
Indigenous mortality rate for 5 years. Does not refer to a specific condition or intervention that could reduce the rates for Indigenous
people.
18

19
Table 10: Perinatal deaths by cause and Indigenous status, Queensland 2000
Data source:
Cause of death Indigenous Not Indigenous
(2,843 births) (46,465 births)
(ANZACPM) n % rate n % rate RR (95% CI)
1. Congenital abnormality 9 13.8 3.2 112 23.5 2.4 1.31(0.58-2.58)
2. Perinatal infection 1 1.5 0.4 11 2.3 0.2 1.49 (0.03-10.2)
3. Hypertension 10 15.4 3.5 19 4.0 0.4 8.6 (3.5-19.4)
4. Antepartum haemorrhage 2 3.1 0.7 43 9.0 0.9 0.76 (0.89-2.92)
5. Maternal conditions 2 3.1 0.7 47 9.9 1.0 0.70 (0.08-2.66)
6. Specific perinatal conditions 9 13.8 3.2 44 9.2 0.9 3.34 (1.43-6.94)
7. Hypoxic peripartum deaths 0 0.0 0.0 15 3.2 0.3 0.00 (0-4.56)
8. Fetal growth restriction 2 3.1 0.7 18 3.8 0.4 1.82 (0.2-7.58)
9. Spontaneous preterm 16 24.6 5.6 78 16.4 1.7 3.35 (1.83-5.79)
10. Unexplained antepartum 12 18.5 4.2 84 17.6 1.8 2.33 (1.16-4.30)
death
11. No obstetric antecedent 1 1.5 0.4 5 1.1 0.1 3.27 (0.07-29.2)
Not classified 1 1.5 0.4 0 0.0 0.0
Total 65 100.0 22.9 476 100.0 10.2 2.23 (1.69-2.89)
Perinatal Data Collection, Data Services Unit, Queensland Health
2 3
1 1 5
4
1
2
3
4
5
rate per 1,000 births
Indigenous status: Australian Aboriginal, Torres Strait Islander or Australian Aboriginal and Torres Strait Islander
Neither Australian Aboriginal nor Torres Strait Islander, total births excludes 10 live births where the Indigenous status was not stated
excludes 1 stillbirth where Indigenous status was not stated
RR relative risk for Indigenous vs not Indigenous with 95% confidence intervals

7.11 Gestational age and birth weight specific perinatal mortality rates
Analyses of perinatal mortality rate by gestational age and birth weight are displayed in Tables 11, 12 and 15 as
crude rates and rates corrected for deaths from congenital abnormalities. Preterm births (<37 weeks)
accounted for 8.5% of all births, and 81% of perinatal deaths. Very preterm births (<28 weeks gestation),
contributed to 0.9% of all births and 300 (55.4%) perinatal deaths. For infants born at term, the risk of perinatal
death is 1.6 per 1,000 total births, comprised of a fetal death rate of 1.4 per 1,000 total births, and neonatal
death rate of 0.2 per 1,000 live births. The rate of post-term birth (>42 weeks) was 1.9% of total births, with a
PMR corrected for congenital abnormality of 4.3 per 1,000. Once again, this increased risk for post-term
women supports the widely-disseminated results of randomised trials for post-term deliveries, indicating the
benefit of induction of labour for women at >42 completed weeks of gestation (Crowley, 2003).
The corrected PMR for babies with birth weights between 3000-4499 grams was 1.3 per 1,000. The corrected
PMR for infants 500 to 999 grams was 485 in 1998, 461 per 1,000 in 1999 and 409 in 2000 representing a
gradual improvement.
The clinical classification systems for perinatal mortality are also used to analyse fetal and neonatal mortality
by gestational age and birth weight.
Cause of death Gestational age (weeks)
<28 28-36 37+ Total
(ANZACPM) n % n % n % n %
1. Congenital abnormality 53 17.7 39 28.5 29 27.6 121 22.3
2. Perinatal infection 8 2.7 4 2.9 0 0 12 2.2
3. Hypertension 14 4.7 12 8.8 3 2.8 29 5.4
4. Antepartum haemorrhage 32 10.7 11 8.0 2 1.9 45 8.3
5. Maternal conditions 43 14.3 3 2.2 3 2.9 49 9.0
6. Specific perinatal conditions 31 10.3 16 11.7 6 5.7 53 9.8
7. Hypoxic peripartum deaths 1 0.3 5 3.6 9 8.6 15 2.8
8. Fetal growth restriction 6 2.0 8 5.8 6 5.7 20 3.7
9. Spontaneous preterm 84 28.0 10 7.3 0 0.0 94 17.3
10. Unexplained antepartum 27 9.0 29 21.2 41 39 97 17.9
death
11. No obstetric antecedent 0 0.0 0 0.0 6 5.7 6 1.1
Not classified 1 0.3 0 0.0 0 0 1 0.2
Total 300 100 137 100 105 100.0 542 100.0
Rate per 1,000 births 681.8 36.8 2.3 11.0
Perinatal Data Collection, Data Services Unit, Queensland Health
Note: Babies born at <28 weeks contributed 55.4% of perinatal deaths, babies born at 28-36 weeks
contributed 25.2% of perinatal deaths, babies born 37+ weeks contributed 19.3% of perinatal deaths
The main causes of deaths in babies of <28 weeks were Spontaneous preterm (28%), Congenital abnormalities
(17.7%) and Maternal conditions (14.3%).
The main causes of deaths in babies from 28-36 weeks were Congenital abnormalities (28.5%), Unexplained
antepartum deaths (21.2%) and Specific perinatal conditions (11.7%).
The main causes of deaths in babies at 37+ weeks were Unexplained antepartum deaths (39%) and Congenital
abnormalities (27.6%).
Table 11: Perinatal deaths by cause and gestational age, Queensland 2000
Data source:
20

21
Table 12: Perinatal deaths by cause and birth weight, Queensland 2000
Data source:
Birth weight (g)
Cause of death <1000 1000-2499 2500+ Total
(ANZACPM) n % n % n % n %
1. Congenital abnormality 55 17.8 35 30.2 31 26.5 121 22.3
2. Perinatal infection 7 2.3 3 2.6 2 1.7 12 2.2
3. Hypertension 17 5.5 9 7.8 3 2.6 29 5.4
4. Antepartum haemorrhage 31 10.0 10 8.6 4 3.4 45 8.3
5. Maternal conditions 43 13.9 2 1.7 4 3.4 49 9.0
6. Specific perinatal conditions 30 9.7 11 9.5 12 10.3 53 9.8
7. Hypoxic peripartum deaths 2 0.6 2 1.7 11 9.4 15 2.8
8. Fetal growth restriction 9 2.9 7 6.0 4 3.4 20 3.7
9. Spontaneous preterm 82 26.5 11 9.5 1 0.9 94 17.3
10. Unexplained antepartum 33 10.7 23 19.8 41 35.0 97 17.9
death
11. No obstetric antecedent 0 0.0 2 1.7 4 3.4 6 1.1
Not classified 0 0.0 1 0.9 0 0.0 1 0.2
Total 309 100.0 116 100.0 117 100.0 542 100.0
Perinatal Data Collection, Data Services Unit, Queensland Health
Low birth weight babies (<2500g) contributed to 7.1% of all births and accounted for 78.5% of all perinatal
deaths.
The major causes of perinatal deaths in extremely low birth weight infants were Spontaneous preterm (26.5%)
and Congenital abnormalities (17.8%).
The major causes of perinatal deaths for those babies 1000g-2499g were Congenital abnormalities (30.2%)
and Unexplained antepartum deaths (19.8%).
The major causes of perinatal deaths for those babies >2500g were Unexplained antepartum deaths and
Congenital abnormalities.

7.12 Perinatal autopsies
The rate of autopsy for all 542 perinatal deaths in 2000 was 213 (39.3%), with autopsies being performed in
44.1% of fetal deaths and only 29.9% of neonatal deaths (Table 13). This compares unfavourably with autopsy
rates of 45.2% in 1999 and 43.5% in 1998. The autopsy rate in this state falls considerably short of the 75%
recommended by the Royal College of Obstetricians and Gynaecologists and the Royal College of Pathologists,
and is lower than that achieved elsewhere in Australia and overseas. Of particular concern is the autopsy rate
of only 62.9% for deaths attributed to the category Unexplained antepartum fetal deaths.
Type of perinatal death
Cause of death Fetal Neonatal Total
(ANZACPM) n Autopsy n Autopsy n Autopsy
rate rate rate
1. Congenital abnormality 35 58.3 25 41.0 60 49.6
2. Perinatal infection 5 71.4 0 0.0 5 41.7
3. Hypertension 8 50.0 5 38.5 13 44.8
4. Antepartum haemorrhage 4 14.8 5 27.8 9 20.5
5. Maternal conditions 3 6.7 0 0.0 3 6.7
6. Specific perinatal conditions 13 35.1 3 18.8 16 30.2
7. Hypoxic peripartum deaths 4 44.4 1 16.7 5 33.3
8. Fetal growth restriction 8 50.0 2 50.0 10 50.0
9. Spontaneous preterm 16 39.0 12 22.6 28 29.8
10. Unexplained antepartum 61 62.9 0 0.0 61 62.9
death
11. No obstetric antecedent 1 50.0 2 50.0 3 50.0
Total 158 44.1 55 29.9 213 39.3
Perinatal Data Collection, Data Services Unit, Queensland Health
Autopsy rate: number of autopsies per 100 deaths
Table 13: Perinatal autopsies by cause and type of death, Queensland 2000
Data Source:
1 1 1
1
Note: The autopsy status was unknown in 6 cases.
Total includes 1 unclassified death
22

23
Tab
le14
:P
eri
na
tal
mo
rtal
ity
rate
sb
yg
est
ati
on
ala
ge
,Q
ue
en
sla
nd
20
00
Da
taso
urc
e:
Ge
sta
tio
na
l ag
e(w
ee
ks)
<22
22
-2
42
5-
27
28
-2
93
0-
31
32
-3
43
5-
36
37
-4
14
2+
Tota
l
Tota
l bir
ths
89
176
175
181
29
51,
04
62
,20
34
4,2
09
93
34
9,3
18
%o
fto
tal b
irth
s0
.20
.40
.40
.40
.62
.14
.58
9.6
1.9
100
.0
Tota
l liv
eb
irth
s16
7015
416
22
78
1,0
172
,179
44
,14
69
27
48
,96
0
Tota
l fe
tal d
ea
ths
73
106
21
1917
29
24
63
63
58
%o
fto
tal f
eta
l de
ath
s2
0.4
29
.65
.95
.34
.78
.16
.717
.61.
710
0.0
Feta
l de
ath
rate
82
0.2
60
2.3
120
.010
5.0
57.6
27.
710
.91.
46
.47.
3
Tota
l ne
on
ata
l de
ath
s16
55
29
910
1217
35
118
4
%o
fto
tal n
eo
na
tal d
ea
ths
8.7
29
.915
.84
.95
.46
.59
.219
.00
.510
0.0
Ne
on
ata
l de
ath
rate
1,0
00
.07
85
.718
8.3
55
.63
6.0
11.8
7.8
0.8
1.1
3.8
Tota
l pe
rin
ata
l de
ath
s8
916
15
02
82
74
14
19
87
54
2
%o
fto
tal d
ea
ths
16.4
29
.79
.25
.25
.07.
67.
618
.11.
310
0.0
Pe
rin
ata
l mo
rta
lity
rate
1,0
00
.09
14.8
28
5.7
154
.79
1.5
39
.218
.62
.27.
511
.0
Co
rre
cte
dp
eri
na
tal m
ort
ali
ty
Feta
l de
ath
wit
hC
A2
416
23
26
23
26
0
Feta
l de
ath
rate
753
.856
2.5
109
.88
9.9
51.2
22
.110
.01.
44
.36
.0
Ne
on
ata
l de
ath
wit
hC
A5
42
14
912
23
16
1
Ne
on
ata
l de
ath
rate
1,0
00
.07
72.7
177.
64
9.7
21.
93
.02
.30
.30
.02
.5
Pe
rin
ata
l de
ath
sw
ith
CA
29
20
44
615
142
63
121
Pe
rin
ata
l de
ath
sw
ith
ou
tC
A6
014
14
62
42
12
62
772
44
21
Co
rre
cte
dp
eri
na
tal m
ort
ali
tyra
te10
00
.09
03
.82
69
.013
5.6
72.7
25
.212
.31.
64
.38
.6
Pe
rin
ata
l Da
taC
oll
ect
ion
,D
ata
Se
rvic
es
Un
it,
Qu
ee
nsl
an
dH
ea
lth
1
2
3
2
4
5
2
5
3
5
5
2
12
3
45
incl
ud
es
“no
tst
ate
d”
-11
live
bir
ths.
rate
pe
r1,
00
0b
irth
sra
tep
er
1,0
00
live
bir
ths
corr
ect
edfo
rco
ng
en
ita
lab
no
rma
lity
con
ge
nit
ala
bn
orm
ali
ty

24
Tab
le15
:P
eri
na
tal
mo
rtal
ity
rate
sb
yb
irth
we
igh
t,Q
ue
en
sla
nd
20
00
Da
taso
urc
e:
Bir
thw
eig
ht
(g)
<50
05
00
-74
975
0-
100
0-
125
0-
150
0-
175
0-
20
00
-2
25
0-
25
00
-3
00
0-
35
00
-4
00
0-
99
912
49
149
917
49
199
92
24
92
49
92
99
93
49
93
99
94
49
9>4
50
0To
tal
Tota
l bir
ths
182
142
143
152
187
27
14
45
68
21,
28
16
,92
617
,00
315
,43
95
,50
59
55
49
,318
%o
fto
tal b
irth
s0
.40
.30
.30
.30
.40
.50
.91.
42
.614
.03
4.5
31.
311
.21.
910
0.0
Tota
l liv
eb
irth
s3
69
612
813
617
32
66
42
86
741,
270
6,8
93
16,9
83
15,4
24
5,4
97
951
48
,96
0
Tota
l fe
tal d
ea
ths
146
46
1516
145
178
113
32
015
84
35
8
%o
fto
tal f
eta
l de
ath
s4
0.8
12.8
4.2
4.5
3.9
1.4
4.7
2.2
3.1
9.2
5.6
4.2
2.2
1.1
100
.0
Feta
l de
ath
rate
80
2.2
32
3.9
104
.910
5.3
74.9
18.5
38
.211
.78
.64
.81.
21.
01.
54
.27.
3
Tota
l ne
on
ata
l de
ath
s3
44
919
73
88
109
1214
92
018
4
%o
fto
tal n
eo
na
tal d
ea
ths
18.5
26
.610
.33
.81.
64
.34
.35
.44
.96
.57.
64
.91.
10
.010
0.0
Ne
on
ata
l de
ath
rate
94
4.4
510
.414
8.4
51.5
17.3
30
.118
.714
.87.
11.
70
.80
.60
.40
.03
.8
Tota
l pe
rin
ata
l de
ath
s18
09
53
42
317
132
518
20
45
34
24
104
54
2
%o
fto
tal d
ea
ths
33
.217
.56
.34
.23
.12
.44
.63
.33
.78
.36
.34
.41.
80
.710
0.0
Pe
rin
ata
l mo
rta
lity
rate
98
9.0
66
9.0
23
7.8
151.
39
0.9
48
.056
.22
6.4
15.6
6.5
2.0
1.6
1.8
4.2
11.0
Co
rre
cte
dp
eri
na
tal m
ort
ali
ty
Feta
l de
ath
wit
hC
A2
912
31
30
41
15
01
00
60
Feta
l de
ath
rate
764
.72
61.
58
5.7
99
.359
.818
.52
9.5
10.3
7.8
4.0
1.2
0.9
1.5
4.2
6.0
Ne
on
ata
l de
ath
wit
hC
A5
42
21
63
94
710
71
06
1
Ne
on
ata
l de
ath
rate
93
5.5
48
9.1
134
.93
7.3
11.6
7.7
11.8
1.5
3.9
0.7
0.2
0.1
0.2
0.0
2.5
Pe
rin
ata
l de
ath
sw
ith
CA
34
165
34
67
105
1210
81
012
1
Pe
rin
ata
l de
ath
sw
ith
ou
tC
A14
679
29
20
137
188
153
32
416
94
42
1
Co
rre
cte
dp
eri
na
tal m
ort
ali
tyra
te9
86
.56
27.
02
10.1
134
.27
1.0
26
.44
1.1
11.9
11.8
4.8
1.4
1.0
1.6
4.2
8.6
Pe
rin
ata
l Da
taC
oll
ect
ion
,D
ata
Se
rvic
es
Un
it,
Qu
ee
nsl
an
dH
ea
lth
1
2
3
2
4
5
2
5
3
5
5
2
1 2 3 4 5
incl
ud
es
“no
tst
ate
d”
-5
live
bir
ths.
rate
pe
r1,
00
0b
irth
s
rate
pe
r1,
00
0li
veb
irth
s
corr
ect
edfo
rco
ng
en
ita
lan
om
aly
con
ge
nit
ala
no
ma
ly

25
Tab
le16
:P
eri
na
tal
dea
ths
by
cau
se,
Qu
ee
nsl
an
d2
00
0
Cla
ssif
ica
tio
nD
ea
thty
pe
Feta
l de
ath
Ne
on
ata
l de
ath
Pe
rin
ata
l de
ath
n%
n%
n%
1.C
ON
GE
NIT
AL
AB
NO
RM
ALI
TY(i
ncl
ud
ing
term
ina
tio
ns
wh
ere
the
fetu
sh
as
con
ge
nit
al a
bn
orm
ali
tie
s)6
016
.86
13
3.2
121
22
.4
1.1
Ce
ntr
al n
erv
ou
ssy
ste
m17
4.8
116
.02
85
.2
1.2
Ca
rdio
vasc
ula
rsy
ste
m7
2.0
179
.22
44
.4
1.3
Uri
na
rytr
act
41.
13
1.6
71.
3
1.4
Ga
stro
inte
stin
al t
ract
20
.62
1.1
40
.7
1.5
Ch
rom
oso
ma
l14
3.9
42
.218
3.3
1.6
Me
tab
oli
c3
0.8
52
.78
1.5
1.7
Mu
ltip
le9
2.5
63
.315
2.8
1.8
Oth
er
con
ge
nit
al a
bn
orm
ali
ty2
0.6
137.
115
2.8
1.9
Un
spe
cifi
ed
con
ge
nit
al a
bn
orm
ali
ty2
0.6
10
.52
0.4
2.
PE
RIN
ATA
LIN
FEC
TIO
N7
2.0
52
.712
2.2
2.1
Ba
cte
ria
l-
-1
0.5
10
.2
2.1
1G
rou
pB
Str
ep
toco
ccu
s2
0.6
10
.53
0.6
2.1
2E
.co
li-
-1
0.5
10
.2
2.1
3Li
ste
ria
mo
no
cyto
ge
ne
s1
0.3
--
10
.2
2.1
8O
the
rb
act
eri
al
--
10
.51
0.2
2.1
9U
nsp
eci
fie
db
act
eri
al
--
--
--
2.2
Vir
al
--
--
--
2.2
1C
yto
me
ga
lovi
rus
10
.31
0.5
20
.4
2.2
2P
arv
ovi
rus
--
--
--
2.2
3H
erp
es
sim
ple
xvi
rus
--
--
--

26
Cla
ssif
ica
tio
nD
ea
thty
pe
Feta
l de
ath
Ne
on
ata
l de
ath
Pe
rin
ata
l de
ath
n%
n%
n%
2.2
4R
ub
ell
avi
rus
--
--
--
2.2
8O
the
rvi
ral
--
--
--
2.2
9U
nsp
eci
fie
dvi
ral
10
.3-
-1
0.2
2.3
Pro
tozo
al e
gto
xop
lasm
a-
--
--
-
2.4
Sp
iro
cha
eta
l eg
syp
hil
is-
--
--
-
2.5
Fun
ga
l-
--
--
-
2.8
Oth
er
20
.6-
-2
0.4
3.
HY
PE
RTE
NS
ION
164
.713
7.1
29
5.4
3.1
Ch
ron
ich
ype
rte
nsi
on
:e
sse
nti
al
30
.86
3.3
91.
7
3.2
Ch
ron
ich
ype
rte
nsi
on
:se
con
da
ry,
eg
ren
al d
ise
ase
10
.32
1.1
30
.6
3.3
Ch
ron
ich
ype
rte
nsi
on
:u
nsp
eci
fie
d-
--
--
-
3.4
Ge
sta
tio
na
l hyp
ert
en
sio
n-
--
--
-
3.5
Pre
-ecl
am
psi
a11
3.1
42
.215
2.8
3.6
Pre
-ecl
am
psi
asu
pe
rim
po
sed
on
chro
nic
hyp
ert
en
sio
n-
-1
0.5
10
.2
3.9
Un
spe
cifi
ed
hyp
ert
en
sio
n1
0.3
--
10
.2
4.
AN
TEP
AR
TUM
HA
EM
OR
RH
AG
E(A
PH
)2
77.
618
9.8
45
8.3
4.1
Pla
cen
tal a
bru
pti
on
21
5.9
116
.03
25
.9
4.2
Pla
cen
tap
rae
via
10
.31
0.5
20
.4
4.3
Va
sap
rae
via
--
--
--
4.8
Oth
er
AP
H-
--
--
-
4.9
AP
Ho
fu
nd
ete
rmin
ed
ori
gin
51.
46
3.3
112
.0

27
Cla
ssif
ica
tio
nD
ea
thty
pe
Feta
l de
ath
Ne
on
ata
l de
ath
Pe
rin
ata
l de
ath
n%
n%
n%
5.
MA
TER
NA
LC
ON
DIT
ION
S4
512
.64
2.2
49
9.1
5.1
Term
ina
tio
no
fp
reg
na
ncy
37
10.4
--
37
6.8
such
as
rup
ture
of
me
mb
ran
es
(RO
M)
aft
er
am
nio
cen
tesi
s)
5.2
Dia
be
tes/
ge
sta
tio
na
l dia
be
tes
30
.81
0.5
40
.7
5.3
Ma
tern
al i
nju
ry-
--
--
-
5.3
1A
ccid
en
tal
--
--
---
5.3
2N
on
-acc
ide
nta
l-
--
--
-
5.4
Ma
tern
al s
ep
sis
20
.6-
-2
0.4
5.8
Oth
er
ma
tern
al c
on
dit
ion
s,e
gLu
pu
so
bst
etr
icsy
nd
rom
e3
0.8
31.
66
1.1
6.
SP
ECIF
ICP
ER
INA
TAL
CO
ND
ITIO
NS
37
10.4
168
.753
9.8
6.1
Twin
-to
-tw
intr
an
sfu
sio
n16
4.5
73
.82
34
.2
6.2
Feto
ma
tern
al h
ae
mo
rrh
ag
e5
1.4
--
50
.9
6.3
An
tep
art
um
cord
com
pli
cati
on
s(e
gco
rdh
ae
mo
rrh
ag
e;
tru
ek
no
tw
ith
evi
de
nce
of
occ
lusi
on
)4
1.1
--
40
.7
6.4
Ute
rin
ea
bn
orm
ali
tie
s,e
gb
ico
rnu
ate
ute
rus,
cerv
ica
l in
com
pe
ten
ce.
61.
77
3.8
132
.4
6.5
Bir
thtr
au
ma
(typ
ica
lly
infa
nts
of
>24
we
ek
sg
est
ati
on
or
>60
0g
bir
thw
eig
ht)
--
--
--
6.6
Ha
em
oly
tic
dis
ea
se-
--
--
-
6.7
Idio
pa
thic
hyd
rop
s2
0.6
21.
14
0.7
6.8
Oth
er
spe
cifi
cp
eri
na
tal c
on
dit
ion
s(i
ncl
ud
es
ute
rin
eru
ptu
re,
iatr
og
en
icco
nd
itio
ns
41.
1-
-4
0.7
7.H
YP
OX
ICP
ER
IPA
RTU
MD
EA
TH(t
ypic
all
yin
fan
tso
f>2
4w
ee
ks
ge
sta
tio
no
r>
60
0g
bir
thw
eig
ht)
92
.56
3.3
152
.8
7.1
Wit
hin
tra
pa
rtu
mco
mp
lica
tio
ns
82
.22
1.1
101.
8
7.2
No
intr
ap
art
um
com
pli
cati
on
s-
--
--
-
7.9
Un
spe
cifi
ed
hyp
oxi
cp
eri
pa
rtu
md
ea
th1
0.3
42
.25
0.9

28
Cla
ssif
ica
tio
nD
ea
thty
pe
Feta
l de
ath
Ne
on
ata
l de
ath
Pe
rin
ata
l de
ath
n%
n%
n%
acu
tea
the
rosi
s,m
ate
rna
l va
scu
lar
thro
mb
osi
so
rm
ate
rna
l flo
or
infa
rcti
on
<24
ho
urs
be
fore
de
live
ry
--
--
--
9.3
9U
nsp
eci
fie
do
rn
ot
kn
ow
nw
he
the
rp
lace
nta
exa
min
ed
30
.89
4.9
122
.2
8.
FETA
LG
RO
WTH
RE
STR
ICTI
ON
(FG
R)
164
.54
2.2
20
3.7
8.1
Wit
he
vid
en
ceo
fu
tero
pla
cen
tal i
nsu
ffic
ien
cye
gsi
gn
ific
an
tin
farc
tio
n8
2.2
31.
611
2.0
8.2
Wit
hch
ron
icvi
llit
is-
--
--
-
8.3
Wit
ho
ut
the
ab
ove
pla
cen
tal p
ath
olo
gy
61.
71
0.5
71.
3
8.4
No
exa
min
ati
on
of
pla
cen
ta-
--
--
-
8.9
Un
spe
cifi
ed
FGR
or
no
tk
no
wn
wh
eth
er
pla
cen
tae
xam
ine
d2
0.6
--
20
.4
9.
SP
ON
TAN
EOU
SP
RE
TER
M(<
37
we
ek
sg
est
ati
on
)4
111
.553
28
.89
417
.3
9.1
Sp
on
tan
eo
us
pre
term
lab
ou
rw
ith
inta
ctm
em
bra
ne
s,o
rm
em
bra
ne
rup
ture
--
--
--
9.1
1W
ith
cho
rio
am
nio
nit
is6
1.7
137.
119
3.5
9.1
2W
ith
ou
tch
ori
oa
mn
ion
itis
20
.62
1.1
40
.7
9.1
3N
oe
xam
ina
tio
no
fp
lace
nta
10
.31
0.2
9.1
9U
nsp
eci
fie
do
rn
ot
kn
ow
nw
he
the
rp
lace
nta
exa
min
ed
10
.34
2.2
50
.9
9.2
Sp
on
tan
eo
us
pre
term
lab
ou
rw
ith
me
mb
ran
eru
ptu
re2
4h
ou
rsb
efo
red
eli
very
--
--
--
9.2
1W
ith
cho
rio
am
nio
nit
is16
4.5
84
.42
44
.4
9.2
2W
ith
ou
tch
ori
oa
mn
ion
iti s
--
21.
12
0.4
9.2
3N
oe
xam
ina
tio
no
fp
lace
nta
--
--
--
9.2
9U
nsp
eci
fie
do
rn
ot
kn
ow
nw
he
the
rp
lace
nta
exa
min
ed
--
42
.24
0.7
9.3
Sp
on
tan
eo
us
pre
term
lab
ou
rw
ith
me
mb
ran
eru
ptu
reo
fu
nk
no
wn
du
rati
on
be
fore
de
live
ry-
--
--
-
9.3
1W
ith
cho
rio
am
nio
nit
i s6
1.7
21.
18
1.5
9.3
2W
ith
ou
tch
ori
oa
mn
ion
iti s
61.
79
4.9
152
.8
9.3
3N
oe
xam
ina
tio
no
fp
lace
nta

29
Cla
ssif
ica
tio
nD
ea
thty
pe
Feta
l de
ath
Ne
on
ata
l de
ath
Pe
rin
ata
l de
ath
n%
n%
n%
ath
ero
sis,
ma
tern
al v
asc
ula
rth
rom
bo
sis
or
ma
tern
al f
loo
rin
farc
tio
n
10.
UN
EX
PLA
INE
DA
NTE
PA
RTU
MD
EA
TH9
72
7.2
00
97
17.9
10.1
Wit
he
vid
en
ceo
fu
tero
pla
cen
tal i
nsu
ffic
ien
cy,
eg
sig
nif
ica
nt
infa
rcti
on
,a
cute
164
.5-
-16
3.0
10.2
Wit
hch
ron
icvi
llit
is1
0.3
--
10
.2
10.3
Wit
ho
ut
the
ab
ove
pla
cen
tal p
ath
olo
gy
29
8.1
--
29
5.4
10.4
No
exa
min
ati
on
of
pla
cen
ta4
1.1
--
40
.7
10.9
Un
spe
cifi
ed
un
exp
lain
ed
an
tep
art
um
de
ath
or
no
tk
no
wn
wh
eth
er
pla
cen
tae
xam
ine
d4
713
.2-
-4
78
.7
11.
NO
OB
STE
TRIC
AN
TEC
ED
EN
T2
0.6
42
.26
1.1
11.1
SID
S-
--
--
-
11.1
1C
on
sist
en
tw
ith
SID
S-
--
--
-
11.1
2P
oss
ible
SID
S-
-1
0.5
10
.2
11.2
Po
stn
ata
lly
acq
uir
ed
infe
ctio
n-
-2
1.1
20
.4
11.3
Acc
ide
nta
l asp
hyx
iati
on
--
--
--
11.4
Oth
er
acc
ide
nt,
po
iso
nin
go
rvi
ole
nce
(po
stn
ata
l)1
0.3
--
10
.2
11.8
Oth
er
10
.31
0.5
20
.4
11.9
Un
kn
ow
n/u
ne
xpla
ine
d-
--
--
-
Tota
l3
5710
018
410
05
41
100
Pe
rin
ata
l Da
taC
oll
ect
ion
,D
ata
Se
rvic
es
Un
it,
Qu
ee
nsl
an
dH
ea
lth
Da
taS
ou
rce
:

30
Tab
le17
:N
eo
na
tald
eath
sb
yca
use
(AN
ZN
DC
),Q
ue
en
sla
nd
20
00
Ca
use
ofd
ea
th(N
eo
na
tal c
lass
ific
ati
on
)n
%
1.C
ON
GE
NIT
AL
AB
NO
RM
ALI
TY6
53
5.3
1.1
Ce
ntr
aln
erv
ou
ssy
ste
m14
7.6
1.2
Ca
rdio
vasc
ula
r sys
tem
1910
.3
1.3
Uri
na
rytr
act
31.
6
1.4
Ga
stro
inte
stin
al t
ract
21.
1
1.5
Ch
rom
oso
ma
l4
2.2
1.6
Me
tab
oli
c5
2.7
1.7
Mu
ltip
le6
3.3
1.8
Oth
erc
on
ge
nit
ala
bn
orm
ali
ty12
6.5
1.9
Un
spe
cifi
ed
con
ge
nit
ala
bn
orm
ali
ty
2.E
XTR
EM
EP
RE
MA
TUR
ITY
(typ
ica
lly
infa
nts
of
24
we
ek
sg
est
ati
on
or
60
0g
bir
thw
eig
ht)
48
26
.1
2.1
No
t re
susc
ita
ted
45
24
.5
2.2
Un
succ
ess
ful r
esu
scit
ati
on
31.
6
2.9
Un
spe
cifi
ed
orn
otk
no
wn
wh
eth
er r
esu
scit
ati
on
att
em
pte
d
3.C
AR
DIO
-RE
SP
IRA
TOR
YD
ISO
RD
ER
S2
915
.8
3.1
Hya
lin
em
em
bra
ne
dis
ea
se/r
esp
ira
tory
dis
tre
sssy
nd
rom
e(R
DS
)2
010
.9
3.2
Me
con
ium
asp
ira
tio
nsy
nd
rom
e1
0.5
3.3
Pri
ma
ryp
ers
iste
ntp
ulm
on
ary
hyp
ert
en
sio
n
3.4
Pu
lmo
na
ryh
ypo
pla
sia
73
.8
3.5
Ch
ron
icn
eo
na
tal l
un
gd
ise
ase
(typ
ica
lly
bro
nch
op
ulm
on
ary
dys
pla
sia
)1
0.5
3.8
Oth
er
4. I
NFE
CTI
ON
126
.5
4.1
Ba
cte
ria
l10
0.5
4.1
1C
on
ge
nit
alb
act
eri
al
21.
1
<<

31
Ca
use
ofd
ea
th(N
eo
na
tal c
lass
ific
ati
on
)n
%
4.1
2A
cqu
ire
db
act
eri
al
84
.4
4.2
Vir
al
1
4.2
1C
on
ge
nit
al v
ira
l
4.2
2A
cqu
ire
dvi
ral
10
.5
4.3
Pro
tozo
al e
gto
xop
lasm
a
4.4
Sp
iro
cha
eta
l eg
syp
hil
is
4.5
Fun
ga
l
4.8
Oth
er
4.9
Un
spe
cifi
ed
org
an
ism
5.N
EU
RO
LOG
ICA
L16
8.7
5.1
Hyp
oxi
cis
cha
em
ice
nce
ph
alo
pa
thy/
pe
rin
ata
lasp
hyx
ia11
6
5.2
Intr
acr
an
ialh
ae
mo
rrh
ag
e5
2.7
5.8
Oth
er
6.G
AS
TRO
INTE
STI
NA
L5
2.7
6.1
Ne
cro
tisi
ng
en
tero
coli
tis
52
.7
6.8
Oth
er
7.O
THE
R9
4.9
7.1
SID
S
7.11
Co
nsi
ste
ntw
ith
SID
S
7.12
Po
ssib
leS
IDS
10
.5
7.2
Mu
lti-
syst
em
fail
ure
-on
lyif
un
kn
ow
np
rim
ary
cau
seo
r tri
gg
ere
ven
t
7.3
Tra
um
a
7.8
Oth
er
73
.8
7.9
Un
de
term
ine
d/u
nk
no
wn
10
.5
Tota
l18
410
0

32
8 References
Advisory Committee on Maternal Mortality and Morbidity, NHMRC. Report on Maternal Deaths in Australia,
1994-1996. Canberra: NH & MRC
Crowley P. Interventions for preventing or improving the outcome of delivery at or beyond term (Cochrane
Review). In: The Cochrane Library, Issue 1, 2003. Oxford: Update Software.
Maternal Deaths in Australia 1994-1996. Perinatal Data Collection, Data Services Unit, Queensland Health.
Report of the Queensland Council on Obstetric and Paediatric Morbidity and Mortality, 1999. Queensland
Health.

33
9 Appendices
9.1 Appendix 1: Perinatal Mortality and Morbidity Subcommittee
9.2 Appendix 2: Maternal Mortality and Morbidity Subcommittee
Members
Members
Dr David Cartwright (Chair) Director-Neonatology, Royal Women's Hospital
Mr Philip Baker Clinical Information Manager, Clinical Audit Program
Ms Rowena Chapman Member of SANDS (Consumer)
Dr Paul Colditz Director-Perinatal Research Centre, Royal Women's Hospital
Ms Sue Cornes Deputy Manager-Health Information Centre
Ms Lynne Dunne Vice President-Queensland Branch, Australian College of Midwives
Dr John Evans General Practitioner, Emerald
Ms Vicki Flenady Perinatal Researcher-Centre for Clinical Studies, Women & Children's
Health, Mater Hospital
Professor Michael Humphrey Director-Obstetrics and Gynaecology, Cairns Base Hospital (to December
2002)
Mrs Joan Kennedy Principal Policy Officer, Office of the Chief Health Officer
Dr Guan Koh Senior Staff Specialist, NICU, The Townsville Hospital
Dr Lucinda Pallis Obstetrician & Gynaecologist, Gold Coast Hospital
Dr Diane Payton Staff Pathologist, QHPSS, Royal Brisbane and Royal Women’s
Hospital and Health Service District
Professor David Tudehope Director, Division of Neonatology, Mater Mothers' Hospital
Mrs Wendy Rogash Administration Officer, Office of the Chief Health Officer
Dr Nikki Whelan Obstetrician & Gynaecologist (Private Practice)
Professor Michael Humphrey Director-Obstetrics and Gynaecology, Cairns Base Hospital (Chairman) (to
December 2002)
Ms Rowena Chapman Member SANDS (Consumer)
Ms Vicki Flenady Perinatal Researcher-Centre for Clinical Studies Women's and Children's
Health, Mater Misericordiae Hospital
Dr Karen Lust Obstetric Physician, Royal Women's Hospital
Mrs Heather McCosker Lecturer, Queensland University of Technology
Dr Diane Payton Staff Pathologist, QHPSS, Royal Brisbane and Royal Women’s
Hospital and Health Service District
Dr David Watson Consultant Obstetrician, The Townsville Hospital
Dr Nikki Whelan Obstetrician & Gynaecologist (Private Practice) and VMO Royal Women's
Hospital
Dr John Wilson Senior Staff Specialist, Royal Womens Hospital

34
9.3 Appendix 3: Australia and New Zealand Antecedent Classification of Perinatal
Mortality (ANZACPM)
Australia and New Zealand Antecedent Classification of Perinatal Mortality (ANZACPM)
1. CONGENITAL ABNORMALITY (including terminations where the fetus has congenital
abnormalities)
1.1 Central nervous system
1.2 Cardiovascular system
1.3 Urinary tract
1.4 Gastrointestinal tract
1.5 Chromosomal
1.6 Metabolic
1.7 Multiple
1.8 Other congenital abnormality
1.9 Unspecified congenital abnormality
2. PERINATAL INFECTION
2.1 Bacterial
2.11 Group B Streptococcus
2.12 E coli
2.13 Listeria monocytogenes
2.18 Other bacterial
2.19 Unspecified bacterial
2.2 Viral
2.21 Cytomegalovirus
2.22 Parvovirus
2.23 Herpes simplex virus
2.24 Rubella virus
2.28 Other viral
2.29 Unspecified viral
2.3 Protozoal eg Toxoplasma
2.4 Spirochaetal eg Syphilis
2.5 Fungal
2.8 Other
2.9 Unspecified organism
3. HYPERTENSION
3.1 Chronic hypertension: essential
3.2 Chronic hypertension: secondary, eg renal disease
3.3 Chronic hypertension: unspecified
3.4 Gestational hypertension
3.5 Pre-eclampsia
3.6 Pre-eclampsia superimposed on chronic hypertension
3.9 Unspecified hypertension
4. ANTEPARTUM HAEMORRHAGE (APH)
4.1 Placental abruption
4.2 Placenta praevia
4.3 Vasa praevia
4.8 Other APH
4.9 APH of undetermined origin
5. MATERNAL CONDITIONS
5.1 Termination of pregnancy
5.2 Diabetes/gestational diabetes

35
Australia and New Zealand Antecedent Classification of Perinatal Mortality (ANZACPM)
5.3 Maternal injury
5.31 Accidental
5.32 Non-accidental
5.4 Maternal sepsis
5.8 Other maternal conditions, eg Lupus obstetric syndrome
6. SPECIFIC PERINATAL CONDITIONS
6.1 Twin-to-twin transfusion
6.2 Fetomaternal haemorrhage
6.3 Antepartum cord complications (eg cord haemorrhage; true knot with evidence of occlusion)
6.4 Uterine abnormalities, eg bicornuate uterus, cervical incompetence.
6.5 Birth trauma (typically infants of >24 weeks gestation or >600g birth weight)
6.6 Haemolytic disease
6.7 Idiopathic hydrops
6.8 Other specific perinatal conditions (includes uterine rupture, iatrogenic conditions such as
rupture of membranes (ROM) after amniocentesis)
7. HYPOXIC PERIPARTUM DEATH (typically infants of >24 weeks gestation or >600g birthweight)
7.1 With intrapartum complications
7.2 No intrapartum complications
7.9 Unspecified hypoxic peripartum death
8. FETAL GROWTH RESTRICTION (FGR)
8.1 With evidence of uteroplacental insufficiency eg significant infarction, acute atherosis,
maternal vascular thrombosis or maternal floor infarction
8.2 With chronic villitis
8.3 Without the above placental pathology
8.4 No examination of placenta
8.9 Unspecified FGR or not known whether placenta examined
9. SPONTANEOUS PRETERM (<37 weeks gestation)
9.1 Spontaneous preterm labour with intact membranes, or membrane rupture <24 hours before
delivery
9.11 with chorioamnionitis
9.12 without chorioamnionitis
9.13 no examination of placenta
9.19 unspecified or not known whether placenta examined
9.2 Spontaneous preterm labour with membrane rupture 24 hours before delivery
9.21 with chorioamnionitis,
9.22 without chorioamnionitis,
9.23 no examination of placenta
9.29 unspecified or not known whether placenta examined
9.3 Spontaneous preterm labour with membrane rupture of unknown duration before
delivery,
9.31 with chorioamnionitis,
9.32 without chorioamnionitis,
9.33 no examination of placenta
9.39 unspecified or not known whether placenta examined
10. UNEXPLAINED ANTEPARTUM DEATH
10.1 With evidence of uteroplacental insufficiency, eg significant infarction, acute atherosis,
maternal vascular thrombosis or maternal floor infarction
10.2 With chronic villitis
10.3 Without the above placental pathology

36
Australia and New Zealand Antecedent Classification of Perinatal Mortality (ANZACPM)
10.4 No examination of placenta
10.9 Unspecified unexplained antepartum death or not known whether placenta examined
11 NO OBSTETRIC ANTECEDENT
11.1 SIDS
11.11 Consistent with SIDS
11.12 Possible SIDS
11.2 Postnatally acquired infection
11.3 Accidental asphyxiation
11.4 Other accident, poisoning or violence (postnatal)
11.8 Other
11.9 Unknown/unexplained
Australia and New Zealand Neonatal Death Classification
1 CONGENITAL ABNORMALITY
1.1 Central nervous system
1.2 Cardiovascular system
1.3 Urinary tract
1.4 Gastrointestinal tract
1.5 Chromosomal
1.6 Metabolic
1.7 Multiple
1.8 Other congenital abnormality
1.9 Unspecified congenital abnormality
2 EXTREME PREMATURITY (Typically infants of <24 weeks gestation or <600g birth weight)
2.1 Not resuscitated
2.2 Unsuccessful resuscitation
2.9 Unspecified or not known whether resuscitation attempted
3 CARDIO-RESPIRATORY DISORDERS
3.1 Hyaline membrane disease/Respiratory distress syndrome (RDS)
3.2 Meconium aspiration syndrome
3.3 Primary persistent pulmonary hypertension
3.4 Pulmonary hypoplasia
3.5 Chronic neonatal lung disease (typically, bronchopulmonary dysplasia)
3.8 Other
4 INFECTION
4.1 Bacterial
4.11 Congenital bacterial
4.12 Acquired bacterial
4.2 Viral
4.21 Congenital viral
4.22 Acquired viral
4.3 Protozoal eg toxoplasma
4.4 Spirochaetal eg syphilis
4.5 Fungal
4.8 Other
4.9 Unspecified organism
5. NEUROLOGICAL
5.1 Hypoxic ischaemic encephalopathy/perinatal asphyxia (typically infants of >24 weeks gestation
or >600g birth weight)
9.4 Appendix 4: Australia and New Zealand Neonatal Death Classification

37
Australia and New Zealand Neonatal Death Classification
5.2 Intracranial haemorrhage
5.8 Other
6. GASTROINTESTINAL
6.1 Necrotising enterocolitis
6.8 Other
7. OTHER
7.1 SIDS
7.11 Consistent with SIDS
7.12 Possible SIDS
7.2 Multi-system failure-only if unknown primary cause or trigger event
7.3 Trauma
7.8 Other
7.9 Undetermined/unknown
B
PSANZ Council has endorsed the interest group on Substance Use in Pregnancy as a Special Interest Group
affiliated with the Perinatal Society of Australia and New Zealand, at its council meeting in March 2003.
A special meeting was held in March 2000 to discuss Perinatal Substance Use issues. Attending this meeting
were two hundred and sixty registrants from across Australia and New Zealand and representing all
disciplines. During this meeting, extreme interest was expressed in ongoing commitment to this topic by
promoting communication via a special forum.
Many of these interested persons are PSANZ members; others work within the field of alcohol and drug
treatment services or associated health services. It is imperative that any proposed special interest group
attracts health professionals in all relevant disciplines.
A national group of interested health professionals has been formed and has held two tele-conferences (in
November 2001 and February 2002) as well as a breakfast meeting in Christchurch in March 2003.
Development of a networking and communication system for stakeholders in the area of perinatal substance
use.
Currently there is a lack of state-wide and national epidemiological data on the prevalence of substance use
(illicit and licit) in pregnancy and the effect on the family and neonate.
This impacts on clinical management issues in the areas of: -
antenatal management
neonatal abstinence syndrome
family and social outcomes
intellectual, developmental and behavioural outcomes for the infant.
There is a lack of Australian and New Zealand research in this area to support evidence-base practice for
clinical management and prevention strategies.
To establish and maintain a forum of stakeholders in perinatal substance use.
y David Tudehope and Kei Lui (Co-chairpersons Perinatal Substance Use Special Interest Group)
�
�
�
�
9.5 Appendix 5: Perinatal Substance Use Special Interest Group
Background to the formation of this special interest group
Project Definition
Problem being addressed
Goal

38
Objectives
Outcomes
Scope
The objectives of the interest forum are: -
Advance members' knowledge and skills in managing perinatal substance use.
Promote research and data collection in perinatal substance use.
Provide expert advice to government and other bodies on matters pertaining to perinatal substance
use.
To develop best practice models in prevention and management.
Examine the feasibility of establishment of clinical indicators and/or national database for
benchmarking purposes.
Maintain liaison with international bodies in perinatal substance use through the promotion of this
interest forum.
Improved clinical management (evidence-based) specifically for antenatal, neonatal abstinence syndrome,
long term outcomes for the infant, and family and social outcomes
Increased education and information for health care professionals
Increased networking between community and hospital based agencies and other related services
Improved outcomes for mother, infants and families
Increased opportunities for research in this field.
Networking and communication of stakeholders (within Australia and New Zealand) through the
establishment of an Executive, including secretariat, a register of members, newsletters and web-site.
Stakeholders will represent the following disciplines:
Paediatricians
Neonatal nurses
Midwives
Obstetricians
Allied Health, Physiotherapist, Social Workers, Pharmacist, Nutritionists
General Practitioners
Alcohol and Drug Case Managers and Counsellors
There will be representation from other services, including:
Mental Health services
Child Health services
Non-Government Organisations (eg. Queensland Intravenous AIDS Association, Alcohol & Drug
Foundation of Australia, Hepatitis C Council)
Any enquiries regarding membership to this special interest group, please provide your mailing address
/contact details to one of the persons listed below:
Ann Kingsbury (Acting secretariat)
David Tudehope*
Kei Lui*
*Co-chairpersons Perinatal Substance Use Special Interest Group
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�
�

39
9.6 Appendix 6: Australia and New Zealand Perinatal Mortality Classification Special
Interest Group
Introduction
Terms of reference
The Perinatal Classification System
THE PERINATAL SOCIETY of
AUSTRALIA & NEW ZEALAND
The Perinatal Society of Australia and New Zealand (PSANZ) Perinatal Mortality Classification Group (PMC-SIG)
has been established from foundations laid by a group of PSANZ members who had met informally over a
number of years to develop a systematic approach to the review and classification of perinatal deaths. The
main objective of this activity was to accurately identify the main contributing factors of perinatal mortality to
enable the development, implementation and ongoing monitoring of strategies to reduce the risk of perinatal
death.
The importance of a clinically orientated classification system, which could be easily and consistently applied
to all perinatal deaths across ANZ to allow the assembly of a large epidemiological dataset to inform
prevention strategies, was recognised. To this end, a clinical classification system (ANZ Antecedent
Classification of Perinatal Mortality and the ANZ Neonatal Death Classification) was developed and piloted and
is now implemented in most States and Territories in Australia and in some regions of New Zealand.
The classifications have been endorsed by the National Perinatal Data Development Committee and accepted
for future publication in the National Perinatal Statistics Unit publication Australia's Mothers and Babies.
Following endorsement of this activity as a SIG of the PSANZ in March 2003, the classifications have been
renamed to the Perinatal Society of Australia and New Zealand - Antecedent Classification for Perinatal
Mortality (PSANZ-ACPM) and the Perinatal Society of Australia and New Zealand Neonatal Death Classification
(PSANZ-NDC).
To develop, implement and manage a clinical classification system for perinatal mortality for use
across Australia and New Zealand
To review the classification annually in terms of required amendments
To develop guidelines for perinatal mortality audit and reporting
To provide advice for Colleges and other bodies on perinatal mortality review
Membership
All PSANZ members with an interest in perinatal mortality classification are welcome to join the SIG. The aim is
to have multidisciplinary membership with geographic representation from across ANZ and to also have
representation from the following:
State and Territory Perinatal Committees; the National Perinatal Statistics Unit; and the Perinatal Data
Collections within ANZ.
The perinatal mortality classification is known as the Australian and New Zealand Antecedent Classification
System for Perinatal Mortality (ANZACPM) and the neonatal system is called the Australian and New Zealand
Neonatal Death Classification (ANZNDC) .
�
�
�
�
�
2,3

40
The purpose of the classification is to focus on aetiology thereby enabling consideration of preventable factors
associated with perinatal death through the systematic application of clinically relevant categories to large
populations.
The two systems have been endorsed by the (Australian) National Perinatal Data Development Committee and
are presently being submitted to the (Australian) National Centre for the Classification of Health. Endorsement
by NCCH will give the classifications official status so that they may be accepted for publication in AIHW reports
such as Australia's Mothers and Babies. The classifications are now being applied in States and Territories
across Australia and some Hospitals in New Zealand.
The Perinatal Indigenous Network was founded in response to the poor state of Indigenous perinatal health as
a formally constituted special interest group of the Perinatal Society of Australia and New Zealand. It
recognises that there is much expertise both among Society members, but also that there is a large workforce
involved in perinatal Indigenous health care outside of the 1000+ current membership of PSANZ. As
Australia's and New Zealand's premier perinatal multidisciplinary group, it is fitting that this initiative be within
PSANZ It has received funding from 2000 by PSANZ in the form of a special initiative grant. The broad aim of PIN
is to both promote awareness and opportunities for Indigenous perinatal health advancement within and
beyond PSANZ.
A PIN web page is accessible from the PSANZ Home Page. A major focus has been highlighting perinatal
Indigenous health issues within the PSANZ Annual Congress. Issues addressed include epidemiological and
cultural issues and the need to incorporate structural and managerial change to deal with issues that tend to be
fragmented by current structures.
Key areas identified by PIN workshop participants as in need of change to improve Indigenous health outcomes
included housing (overcrowding); immunization; alcohol and drugs; knowledge; education and training;
antenatal protocols; breastfeeding; recognition and respect; supporting clients; funding; strategies to address
problems; length of programs; accessing health providers; role of men; supporting decentralized models;
supporting local services; partnerships; networking support, building community capacity and maintaining a
positive focus.
This year has seen several activities.
1. Efforts have been made to establish whether Indigenous Health Workers could be attracted to the
annual PIN meeting. These efforts have identified that the IHW workforce is loosely organised,
fragmented and has very limited funding for conference attendance.
2. In light of the above, and in an environment where PIN was unable to immediately identify sources of
funding, a restructure of how PIN conducts its core business of being a network of PSANZ members and
other interested people who can provide a structure within PSANZ to highlight and deal with perinatal
Indigenous health matters was undertaken. The direct outcome of this has been a reformatting of PIN
involvement at the PSANZ Congress so that:
There be a dedicated session on Indigenous Health (as opposed to a satellite meeting) at every PSANZ ASM
from and including Hobart 2003.
The Indigenous abstracts be assessed along with all abstracts and 4 selected for presentation in the dedicated
session.
The dedicated Indigenous Health session be constituted as 4 papers (total 1 hour) with 30 minutes for an
invited Indigenous speaker and questions.
A complex set of issues underpins poor Indigenous Perinatal health outcomes. PIN, by its multidisciplinary
nature may have an important role in drawing together those involved in the various policy issues,
jurisdictions, service providers, researchers, epidemiologists, statisticians and most importantly the
Indigenous people involved in perinatal health.
1. Whitfield CR, Smith NC, Cockburn F, Gibson AAM. Perinatally related wastage a proposed classification of primary obstetric factors. Br J Obstet Gynaecol 1986;93:694-703.
2. King J, Chan A, Haslam R, Flenady V, Tudehope D, Hockey R. ANZACPM and ANZNDC classifications for perinatal mortality: an analysis of agreement between clinicians. Proceedings Perinatal Society of Australia and
New Zealand 4th Annual Congress, Canberra, March 2001.
3. Flenady V, King J, Hockey R, Tudehope D, Woodgate P. Trends in cause specific perinatal mortality in a tertiary maternity hospital using a new clinical classification (ANZACPM). Proceedings Perinatal Society of
Australia and New Zealand 5th Annual Congress, Christchurch, March 2002.
9.7 Perinatal Indigenous Network (PIN)

41
10 Glossary of terms
Avoidable factor Some departure from the accepted standard of satisfactory care which
may have played a part in the death, injury or complication resulting
from the delivery of a health service.
Child Section 5 (2) The Registration of Births, Deaths and Marriages Act 1962
defines a child as follows:
For the purposes of the Act
(a) a child born alive is one whose heart has beaten after it has been
completely expelled or extracted from its mother; and
(b) a child not born alive is one whose heart has not beaten after it has
been completely expelled or extracted from its mother and who is
either-
(i) of not less than 20 weeks gestation; or
(ii) of not less than 400g by weight at birth
Fetal Death Commonly known as stillbirth, is a child of less than 20 weeks gestation
or 400grams and who shows no signs of life after birth.
Fetal Death Rate The number of fetal deaths per 1,000 total births.
Five-year avoidable excess The absolute difference in the mortality rates of Indigenous and non-
Indigenous status Indigenous populations, multiplied by the number of Indigenous births
in 2000, multiplied by five years, and truncated to an integer value. Does
not refer to a specific condition or intervention to reduce the rates for
Indigenous populations.
Indigenous Status Mother’s ethnicity indicated as Australian Aboriginal, Torres Strait
Islander or both Australian Aboriginal and Torres Strait Islander.
Although there are differences between the two groups that should be
considered for health policy, they are grouped together for statistical
purposes.
Live Birth A child whose heart has beaten after it has been extracted from its
mother.
Maternal Death Direct deaths are those that result from obstetric complications of the
pregnant state (pregnancy, labour and puerperium) including deaths
from interventions, omissions, inappropriate treatment, or from a chain
of events resulting from any of the above. They are complications of
pregnancy itself.
Indirect deaths are those which result from pre-existing disease or
disease that developed during pregnancy and was not due to direct
obstetric causes, but which may have been aggravated by physiological
effects of pregnancy.
Incidental deaths are those due to conditions occurring during
pregnancy, where the pregnancy is unlikely to have contributed
significantly to the death, although it is sometimes possible to postulate
a distant association.
Maternal Mortality Rate Maternal Mortality rate is:
Number of maternal deaths X 100,000
Number of births (live births and still births)
Neonatal Death The death of a child within twenty-eight days of its birth.
Neonatal Mortality Rate The number of deaths of live born infants under 28 days of age per 1,000
live births.
Perinatal Mortality Rate The number of fetal and neonatal deaths for 1,000 total births.
Still Birth See fetal death.

Acknowledgments
The Queensland Maternal & Perinatal Quality Council would like to thank the following people and
organisations for their assistance and hard work in preparing this report
Australian Bureau of Statistics
Client Services, Health Information Centre, Queensland Health
Health Statistics Unit, Australian Bureau of Statistics
Members of the Council
Office of the Government Statistician, Queensland
Queensland Coroners
Registrar General of Births, Death and Marriages, Queensland

Notes