Embed Size (px)
Citation preview
Report of the
MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Copenhagen, Denmark24–27 February 2015
Building Countries’ Capacity for Action against Antimicrobial Resistance
MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Copenhagen, Denmark24–27 February 2015

4
Abstract
Antimicrobial resistance (AMR) is recognized as one of the major health threats of our time. Addressing this complex public health problem requires action in all relevant sectors, including human health, veterinary health, agriculture, environment and education to preserve the effectiveness of antibiotics by discouraging their misuse and overuse, and by gathering data to track resistance and usage patterns. The 2011 European strategic action plan on antibiotic resistance (EUR/RC61/14) outlined seven strategic objectives in a com-prehensive response to AMR. Since then the Regional Office has provided targeted assistance to Member States, building capacity to address the challenges posed by AMR. Continuing to deliver on the objectives of the action plan, the Regional Office invited delegates from 17 countries to participate in eight programmes aimed at providing targeted input, and creating a unique opportunity to share experiences for the different participant profiles, including microbiologists, epidemiologists, pharmacists and clinicians.
Address requests about publications of the WHO Regional Office for Europe to: Publications WHO Regional Office for Europe UN City, Marmorvej 51 DK-2100 Copenhagen Ø, DenmarkAlternatively, complete an online request form for documentation, health information, or for permission to quote or translate, on the Regional Office website (http://www.euro.who.int/pubrequest).
© World Health Organization 2015All rights reserved. The Regional Office for Europe of the World Health Organization welcomes requests for permission to reproduce or translate its publications, in part or in full.
The designations employed and the presentation of the material in this publication do not imply the expression of any opinion whatsoever on the part of the World Health Organization concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. Dotted lines on maps represent approximate border lines for which there may not yet be full agreement.
The mention of specific companies or of certain manufacturers’ products does not imply that they are en-dorsed or recommended by the World Health Organization in preference to others of a similar nature that are not mentioned. Errors and omissions excepted, the names of proprietary products are distinguished by initial capital letters.
All reasonable precautions have been taken by the World Health Organization to verify the information contained in this publication. However, the published material is being distributed without warranty of any kind, either express or implied. The responsibility for the interpretation and use of the material lies with the reader. In no event shall the World Health Organization be liable for damages arising from its use. The views expressed by authors, editors, or expert groups do not necessarily represent the decisions or the stated policy of the World Health Organization.

5MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Foreword
Antimicrobial resistance (AMR) is recognized as one of the major health threats of our time. If we lack the ability to prevent or treat infections, we stand to lose all the progress we have made in modern medicine over the past 70 years. Although the de-velopment of resistance to treatment by pathogens is a natural phenomenon, the misuse and overuse of antimicrobials has greatly accelerated the rate at which it occurs and spreads around the world. AMR is not a problem of any individual country and the successful control of AMR requires that all countries are involved. In April 2014, World Health Organization (WHO) published the first global report on AMR surveillance, showing high proportions of resistance to treatment everywhere in the world, both in health care settings and in the community. As a potential complication of treatment, the ep-idemiology of AMR follows that of infectious dis-eases, spreading from human-to-human, as well as throughout the food chain and the environment. Addressing this complexity requires an intersectoral, interdisciplinary but also international approach. A common understanding of the issues related to AMR is required, and every stakeholder needs to recognize their role and responsibility.
To facilitate this, the WHO Regional Office for Europe organized a multicountry workshop on AMR held on 24–27 February 2015 at UN City in Copenhagen, Denmark. The set-up of the workshop reflected some of the complexity of AMR by bringing together colleagues from different countries, disciplines and sectors. This provided a unique opportunity for interaction between counterparts from different countries and between national colleagues who need to coordinate their activities to control AMR in a comprehensive manner. The workshop was at-tended by individuals from national AMR and medi-cines consumption focal points, microbiologists and
clinicians from almost 20 countries in the Region. Seven countries sent additional colleagues who had received a grant to set up AMR awareness cam-paigns to share their experience.
An impressive number of faculty members from WHO collaborating centres and other partner insti-tutions supported the workshop. These institutions included the following: Copenhagen University, Denmark; The European Committee on Antimi-crobial Susceptibility Testing (EUCAST) Reference Laboratory, Sweden; European Centre for Disease Prevention and Control, Sweden; Groningen Uni-versity, the Netherlands; Karolinska Institute, Swe-den; Memorial Sloan-Kettering Cancer Center, United States of America; National Institute of Public Health and the Environment, the Nether-lands; Norwegian Institute of Public Health, Nor-way; Public Health Agency, Sweden; Public Health England, United Kingdom; Smolensk State Medical Academy, Russian Federation; Stanford University, United States of America; State Medical Univer-sity, Russian Federation; Statens Serum Institut, Denmark; University of Ljubljana, Slovenia; and Za-greb University Hospital, Croatia. The workshop was also supported by colleagues from various technical programmes at WHO headquarters and the Regional Office who are members of the AMR Working Group.
We are very grateful to all the experts who generous-ly donated their expertise and experience of a vari-ety of AMR-related topics and to the governments of Belgium, the Netherlands and the United States of America for their financial support. We hope that the participants left the workshop feeling in-formed and inspired and will want to engage with us in future AMR-related activities across disciplines, sectors and borders.
Danilo Lo Fo Wong Programme Manager Control of Antimicrobial
Hanne Bak Pedersen Programme Manager Health Technologies and Pharmaceuticals

6
Acknowledgements
The meeting was co-hosted by the Control of Anti-microbial Resistance and Health Technologies and Pharmaceuticals (HTP) programmes of the World Health Organization Regional Office for Europe. We acknowledge the valuable contributions from the facilitators, translators, interpreters and the Sec-retariat, all the staff at UN City, Copenhagen, as well
as the workshop participants for their active partici-pation. Financial support was provided by the Min-istry of Health Welfare and Sport of the Netherlands, the Federal Public Service on Health, Food Chain Safety and Environment of Belgium, and the De-fence Threat Reduction Agency of the United States of America, and is gratefully acknowledged.
7MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Table of contents
ABBREVIATIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .8
BACKGROUND OF THE WORKSHOP . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9
PROGRAMME A . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 10–11
PROGRAMME B . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12–13
PROGRAMME C . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 14–15
PROGRAMME D . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 16–19
PROGRAMME E . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 20–21
PROGRAMME F . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22–23
PROGRAMME G . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24-25
PROGRAMME H . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 26–27
COUNTRY AMR ACTIVITIES POSTER SESSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .28
FEEDBACK . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .29
ANNEX 1: LIST OF WORKSHOP PARTICIPANTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 30–32
ANNEX 2: LIST OF WORKSHOP OBSERVERS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .33
ANNEX 3: LIST OF WORKSHOP FACILITATORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 34–35
ANNEX 4: LIST OF WHO COLLABORATORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .36
ANNEX 5: WORKSHOP AGENDA OVERVIEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .37

8
Abbreviations
AMC Antimicrobial medicines consumption
AMR Antimicrobial resistance
AMS Antimicrobial stewardship
ATC/DDD Anatomical, Therapeutic Chemical Classification/Defined Daily Dose
CAESAR Central Asian and Eastern European Surveillance of Antimicrobial Resistance
ECDC European Centre for Disease Prevention and Control
ESAC-Net European Surveillance of Antimicrobial Consumption Network
ESVAC European Surveillance of Veterinary Antimicrobial Consumption
EUCAST European Committee on Antimicrobial Susceptibility Testing
EuroDURG European Drug Utilization Group
HTP Health Technologies and Pharmaceuticals programme (of WHO Regional Office for Europe)
MRSA Methicillin-resistant Staphylococcus aureus
PCR Polymerase chain reaction
RIVM Dutch National Institute for Public Health and the Environment
TAP Tailoring Antimicrobial Resistance Programme
WHO World Health Organization
WHO CC World Health Organization Collaborating Centre

9MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Background of the workshop
WHO Regional Office for Europe hosted a multi-country antimicrobial resistance (AMR) workshop on 24–27 February 2015 in Copenhagen, Denmark to help build countries’ capacity for action against AMR. The workshop focused on sharing experience and methodologies relevant for: (i) rational use of antibiotics and antimicrobial stewardship (AMS) in the hospital setting; (ii) creating awareness of AMR; (iii) AMR surveillance; and (iv) antibiotic consump-tion surveillance.
AMR is a global problem that does not stop at national borders and has already had measurable impact on the countries of the WHO European Re-gion. Resistant infections currently claim at least 50 000 lives each year across Europe and the United States of America alone, with many hundreds of thousands more dying in other areas of the world. In 15 European countries, more than 10% of blood-stream Staphylococcus aureus infections are caused by methicillin-resistant strains (methicillin-resist-ant S. aureus, MRSA). In several of these countries, resistance rates are approaching 50%.
The variation in the AMR problems of individual countries is linked to huge differences in how they use antimicrobial drugs. Global consumption of antibiotics in human medicine rose by nearly 40% between 2000 and 2010, but this figure masks pat-terns of declining usage in some countries and rapid increases in others.
An urgent need for action exists in all relevant sec-tors, including human health, veterinary health, agriculture, environment and education to preserve the effectiveness of antibiotics by discouraging their misuse and overuse, and by gathering data to track resistance and usage patterns. The 2011 European strategic action plan on antibiotic resistance (EUR/RC61/14) built on the momentum created by World Health Day in 2011 and its motto “No action today, no cure tomorrow”, by outlining seven strategic objectives in a comprehensive response to AMR. Since then the Regional Office has provided target-ed assistance to Member States, building capacity to address the challenges posed by AMR.
Continuing to deliver on the objectives of the action plan, the Regional Office invited delegates from al-most 20 countries to participate in eight programmes (A–H) aimed at providing targeted input for the dif-ferent participant profiles, including microbiologists, epidemiologists, pharmacists and clinicians.
More specifically, the primary objectives of the work-shop were to:
1. build capacity for drug utilization research and microbiologic methods to detect AMR;
2. introduce clinicians to concepts of AMS and working in multidisciplinary teams in the hos-pital setting; and
3. encourage cross-sector knowledge exchange and sharing of best practices for AMR awareness raising among countries of the European Region.
The workshop was widely attended with partici-pation from 75 representatives from 17 countries (Albania, Armenia, Azerbaijan, Belarus, Bosnia and Herzegovina, The former Yugoslav Republic of Mac-edonia, Georgia, Kazakhstan, Kyrgyzstan, Republic of Moldova, Montenegro, Russian Federation, Serbia, Tajikistan, Turkey, Ukraine and Uzbekistan), 29 inter-national faculty representing 17 organizations in 10 countries, and WHO staff and consultants (a full list of workshop participants can be found in Annex 1). In addition, a live webcast of the workshop plenary session was accessible online.
The report summarizes all sessions and provides an overview of main discussion points, important issues to consider, and key challenges identified.
10
Programme A 24–25 FEBRUARY LABORATORY WORKSHOP AT THE DANISH STATENS SERUM INSTITUT
SESSION FACILITATORS
Professor Arjana Tambic Andrasevic Professor Elena Barantsevitch Mr Frank Hansen Dr Iva Butic Professor Katja Seme Dr Natali Ivanchik Dr Marc Stegger Dr Marina Sukhorukova Professor Neil Woodford Dr Oskar Ekelund Dr Robert Leo Skov
The laboratory workshop was preceded by a round of presentations and discussion at the Danish Stat-ens Serum Institut. Participants were provided with an English or Russian version of the workshop sylla-bus, EUCAST1 guidelines, rules and quality control recommendations, presentation materials and the recent Central Asian and Eastern European Surveil-lance of Antimicrobial Resistance (CAESAR) surveil-lance manual. These materials were used during interactive exercises in a laboratory at the Statens Serum Institut. Presentations focused on both the main microbiological challenges posed by AMR and the establishment and organization of national reference laboratories, with a case discussion from the United Kingdom.
Main discussion points1. Reference laboratories must not only provide
timely and accurate testing to aid diagnostics but also have a role in identifying new chal-lenges.
2. In many of the participating Member States, the extension of reference laboratory capacity would be welcomed and could aid in the timely and accurate mapping of national and local resistance profiles.
1 EUCAST: European Committee on Antimicrobial Susceptibility Testing
3. Reference laboratories also have a role in creat-ing awareness of AMR and the current national situation (e.g. through newsletters or updates), and in competence building for regional labo-ratory facilities.
4. Gram-negative bacteria producing carbapene-mase and extended-spectrum beta-lactamase are likely to present the greatest challenge for infection control over the next decade. How-ever, some community-acquired gram-positive infections such as community-associated MRSA must also be monitored closely.
5. Laboratories in some countries find it difficult to obtain certain bacterial strains needed as positive controls for testing. This issue and options to address it were discussed by the faculty members.
Key challenges • Resources for national reference laboratories
are not always sufficient to implement a com-prehensive range of services.
• Recruitment of qualified staff and raising aware-ness about the need for laboratory diagnostics often proves difficult. One strategy to address this issue is to raise the profile of microbiologi-cal diagnostics in the curriculum of medical students and to encourage participation of stu-dent in research projects, internships or clinical training rotations.
Laboratory workshopParticipants completed a series of interactive exer-cises, which focused on the following competencies.
Reading prepared platesWhile working with Professor Neil Woodford and supportive faculty, the participants performed anti-biotic susceptibility testing on prepared agar plates containing Klebsiella pneumoniae, Escherichia coli and Citrobacter freundii. The participants were

11MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
shown how to use the EUCAST breakpoint table 5.0, which enables detection of AMR.
Phenotypic methods for beta-lactamase detectionProfessor Arjana Tambic Andrasevic and supportive faculty facilitated this exercise on screening for car-bapenemase production, presence of a carbapen-emase and the Carba Nordmann-Poirel test.
Polymerase chain reaction (PCR) methodsMr Frank Hansen and Dr Marc Stegger, along with supportive faculty led the students in the steps needed to obtain a PCR product from a bacterial lysate. The participants were very enthusiastic about this exercise and requested additional reference and protocol materials to share with their colleagues and students.
Important issues to consider • During the discussion, the facilitators reasoned
that reference laboratories should ideally be lo-cated in dedicated facilities and work separately and independently from hospital laboratories. However, the participants highlighted that this is currently not a realistic prospect in many set-tings. For instance, in many countries reference tasks are performed along with routine tasks serving the community.
• Equipment and testing procedures should be chosen according to current guidelines and must be regularly reviewed.
• National surveillance systems must be strength-ened, partly by identifying so-called geographic hotspots for transfer of resistance-conferring plasmids and high-risk clones.
• Testing for carbapenem resistance must involve susceptibility analysis to available treatment options because many carbapenemases merely reduce susceptibility, rather than confer com-plete resistance.
12
Programme B 24–25 FEBRUARY RESEARCH METHODOLOGY FOR QUALITATIVE ANALYSIS OF USE OF ANTIMICROBIAL MEDICINE
SESSION FACILITATORS
Dr Janine Marie Traulsen Dr Lourdes Cantarero-Arevlao Ms Nina Sautenkova
Throughout the workshop, several sessions on an-timicrobial medicine use were held. Their aim was to support Member States participating in the WHO Regional Office for Europe Antimicrobial Medicines Consumption (AMC) Network and to further de-velop competencies. Participants discussed the investigation of antimicrobial medicine use in their home countries, with the goal to build evidence for policy responses to AMR. Without a better under-standing of how drugs are used at local and national levels, it is difficult to introduce relevant changes into health systems and to adjust drug use.
During the research methodology workshop, a proposal including a semi-structured interview protocol was discussed and finalized in collabo-ration with co-facilitators from Copenhagen Uni-versity. This study protocol will be used as a basis for investigation to learn more about knowledge, behaviour and attitudes related to antibiotic use in a number of eastern European countries, which are a part of the WHO Regional Office for Europe AMC Network. This research is planned to be carried out in 2015 and constitutes an important step in the development of national policies and tools that promote the prudent use of antibiotics. The re-search activities are part of the continuing effort to support countries in the formulation of medicine policy and in the development of efficient medi-cine management systems. Policies aimed at both supply and demand-side are needed to facilitate the appropriate use of medicines.
Main discussion points1. The participants discussed how to gain a better
understanding of the underlying reasons for the inappropriate use of antibiotics, which were identified in a recent quantitative consump-tion study.
2. The participants considered whether the use of interviews is an appropriate method to study knowledge, behaviour and attitudes relating to inappropriate use of antibiotics.
3. The use of a survey on existing guidelines, availability and affordability of medicines was discussed, as well as the inclusion of upper res-piratory tract infections and specific medicines.
Important issues to consider • Research proposals must receive clearance from
ethics committees at the national level. • Research projects should aim to eventually
include all relevant stakeholders, although the initial focus of this project will be on physicians, pharmacists and patients.
• The project focuses on antibiotic treatment in primary care. Consequently, it is important that patients who are included have obtained their antibiotics through a family physician/general practitioner and/or the community pharmacy.
Key challengesThe first part of the project is scheduled to be com-pleted by the end of 2015. It will be critical that the research project receives clearance at the national level in participating countries and that feedback is provided by participants.

13MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
14
Programme C 25 FEBRUARY BASIC PRINCIPLES OF ANTIBIMICROBIAL STEWARDSHIP
SESSION FACILITATORS
Dr Danilo Lo Fo Wong Dr Elizabeth Robilotti Professor Stanley Deresinski
The workshop’s third session focused on the con-tent and basic principles of AMS programmes. According to the definition used by the United States Centers for Disease Control and Prevention (CDC), AMS ensures the use of the right antibiotic for the right patient, at the right time, with the right dose, and the right route, causing the least harm to the patient and future patients2.
In a series of talks, this session addressed the clinical science basis of AMS, the sustainable use of antibi-otics and the role of physicians in the implemen-tation of AMS. In his opening statement, Dr Danilo Lo Fo Wong (WHO Regional Office for Europe) underlined the importance of AMS and infection prevention and control measures for a successful response to AMR and noted that the forthcoming Global AMR Action Plan will emphasize the need for comprehensive stewardship activities. The pres-entations by Professor Stanley Deresinski and Dr Elizabeth Robilotti outlined a number of steps that health care providers must take to ensure the
appropriate use of antibiotics, but also illustrated the complexity of having to potentially balance these steps against favourable clinical outcomes for the individual patient.
Main discussion points1. Appropriate use of antibiotics is a competence
that all health professionals must acquire and use in their practice. However, since physi-cians play a key role in prescribing antibiotics, they have a strong impact on overall use. Con-sequently, specific attention must be given to keeping physicians up-to-date about best prescribing practices and the prudent use of antibiotics.
2. In the discussion, antibiotics were described as an essentially non-renewable resource, which underlined the urgent need for effective AMS and the sustainable use of antibiotics.
3. The role of appropriate dosing of antibiotics is often overlooked: AMS must involve more than just the appropriate choice of therapy for the patient and consider both pharmacoki-netic and pharmacodynamics implications of prescribing. Here, adherence to standard treatment guidelines for specific diseases may be a useful resource.
4. In terms of appropriate prescribing, greater em-phasis must be placed on delivery mode, delivery intervals and dosing.
2 www/cdc.gov/getsmart/healthcare/inpatient-stewardship
15MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
5. Antibiotic prescriptions must be routinely re-viewed after initial treatment. Treatment time-outs and prescription reviews after 48 hours are a useful method to evaluate effectiveness of the chosen therapy option and to assess if the treatment can be de-escalated. These strat-egies not only improve the cost-effectiveness of the treatment but also benefit the patient by reducing the risk of superinfections and reducing the likelihood of selecting for resist-ant bacteria.
6. De-escalation of antibiotic therapy should also involve the switch from intravenous to oral drugs as soon as possible.
7. Different strategies to reduce antibiotic use were identified and discussed. These involved the restriction of particular drug classes, the au-diting of prescriptions with feedback to the prescriber, the provision of educational tools and prescribing guidelines, and the routine review of existing prescriptions.
Important issues to consider • More focus and data is needed to assess the
effects of shortening treatment and to improve clinical decision-making about the appropriate length of antibiotic prescriptions. WHO has already revised classifications and treatment recommendations for a number of diseases, such as pneumonia in children, HIV/AIDS and hepatitis infection; however, it is important that resources are provided to continue and expand this work, which should also include
research on posology, and options for combin-ing/shortening treatment in order to increase patient adherence.
• Implementing an effective AMS programme requires strong leadership, commitment of all stakeholders and clear communication of the programme targets and rationale to those who have to implement it.
• The type of AMS programme suitable for a health care provider will depend on local cir-cumstances. However, it is crucial that all AMS programmes are monitored to permit their eval-uation and to review or adjust them if necessary.
• Clinical prescribing guidelines must be regularly updated and adjusted to reflect changes in regional and local resistance patterns, as well as relevant new research findings. All institutions with a designated AMS programme should clearly assign responsibility for these reviews.
Key challenges • Participants reported that it was challenging
to disseminate knowledge about AMS among health care providers. One suggested solution to this was the use of online teaching modules, many of which can be accessed free of charge.
• Participants also discussed the proportion of AMS activities that should be directed at health professionals who are not physicians. It was agreed that this would vary between health care systems, but that successful AMS programmes must involve input from all rele-vant stakeholders.

16
Programme D 25 FEBRUARY PLENARY SESSION
SESSION FACILITATORS
Dr Danilo Lo Fo Wong Dr Anna Cichowska Dr Arno Müller Dr Danilo Lo Fo Wong Dr Diane Asjori-Oredope Ms Hanne Bak Pedersen Professor Hajo Grundmann Dr Johan Struwe Professor Katja Seme Dr Elizabeth Robilotti Dr Frode Forland Dr Sergey Eremin Professor Stanley Deresinski Mr Tim Nguyen
The first part of the plenary session (session I) provid-ed an update on the development of the forthcom-ing Global AMR Action Plan, which was undergoing review ahead of its presentation at the World Health Assembly in May 2015.
Dr Nedret Emiroglu, Deputy Director of WHO’s Division of Communicable Diseases, commended the partner countries on their efforts and drew special attention
to the countries and project leaders that had initiated the Global Action Plan and hosted consultations. She also emphasized the importance of the CAESAR network for the surveillance, containment and pre-vention of AMR in Central Asia and Eastern Europe.
Her comments were echoed by Dr Hans Kluge, who outlined recent progress towards ensuring better surveillance and containment of AMR in Eu-rope, but also pointed out that much work remains. He underlined the importance of addressing AMR as part of a health systems approach, where all health professionals play their part in supporting appro-priate use of medicines. Dr Kluge thanked Member States for antimicrobial consumption monitoring, which has been carried out since 2011, and stressed the importance of continuing the work as a basis for policy action and working towards prudent use of antimicrobial medicines..
Dr Sergey Eremin from WHO headquarters discussed the progress of the development of the Global AMR Action Plan and its position in the current policy landscape. He emphasized the relevance of the Plan as a platform for further discussion and policy development at the Member State level. Moreo-ver, Dr Eremin stressed the need for a comprehen-sive policy response to AMR. He outlined the key
17MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
components of the Plan and highlighted the role of AMS as an integral part of the strategy. Dr Eremin also mentioned the continued need for improved data to better assess the burden of drug resistance and to develop appropriate policy responses.
The update on the Global AMR Action Plan was concluded by two presentations and a short video on three high-level consultations that took place in Sweden, Norway and the Netherlands. The present-ers gave an overview of the discussion during the meetings and provided summaries of the outcomes and follow-up actions.
The speakers underlined the need for better and more-standardized surveillance data from all
Member States. Data collection has the potential to be broadened to include additional clinical in-formation about the patient.
Agreement was reached that countries that have not yet developed a national strategy for AMR must do so urgently.
Representatives from Member States that partici-pated in the three high-level consultations signalled their willingness to act quickly and to support each other in the development and implementation of national AMR strategies. It was emphasized that the Global AMR Action Plan should be understood as a collaborative effort, rather than a competition between regions and countries.
The second part of the plenary session was dedicat-ed to policy case studies from the United Kingdom and Slovenia, which highlighted a number of suc-cessful policy lessons.
1. National strategies to combat AMR can help to outline the scope of programmes, facilitate coop-eration between agencies and industry, and as-sign clear responsibility for individual tasks.
2. Public awareness of the causes of AMR con-tinues to be a matter that policy makers must address. An effective communication strategy must therefore be a cornerstone of AMR policy. Interventions that have been proven to reach large audiences include television advertising, social media campaigns and dedicated teach-ing materials for schoolchildren.
3. Effective campaigns must target stakeholders directly and involve them in the development of policy responses.
4. AMS should be integrated into medical training programmes for all health professionals and become a part of both undergraduate and post-graduate education. In addition, medical edu-cation should emphasize the need for timely de-escalation of antibiotic treatment.
5. To evaluate progress and assess the effective-ness of interventions, appropriate outcome measures must be defined.
Key challenges • AMR policies must be funded appropriately to
ensure effective and sustainable interventions. In some countries, available funding is insuffi-cient.
• Policies on the use of antimicrobial medicines will be part of the larger agenda on the appro-priate use of medicines, and measures related to both supply and demand must be considered.
• Multisectoral and inter-agency communication and coordination can be challenging.
• Good data on effectiveness of programmes may be difficult to collect; outcome param-eters for policy interventions may have to be specifically defined.
Plenary Session (II): Country Examples

18
The final session of the day focused first on the veterinary use of antimicrobials and concluded by considering both the use of structured surveys as a method of collecting surveillance data and the need for effective AMS.
Main findings and recommendations1. Under the One Health approach, veterinary use
of antibiotics should be considered in all AMR strategies.
2. The European Surveillance of Veterinary An-timicrobial Consumption (ESVAC) now offers an overview of antibiotic use in animals across many European countries.
3. Penicillins and tetracyclines are very commonly used antibiotics in animals.
4. Food-producing animals account for more than 90% of veterinary antibiotic use.
5. ESVAC data indicate that veterinary use of anti-biotics accounts for around 70% of all antibiotic
use in Europe. However, this figure does not adjust for differences in biomass between hu-mans and animals.
6. Some of the surveyed countries have recently re-ported falling consumption figures for veterinary antibiotic use. However, it remains unclear to what extent this may be the result of changes in the size and composition of animal populations.
7. Surveillance measures for antimicrobial re-sistance should consider different levels: the pathogen, the patient and the population. Dividing these levels into separate responsibil-ities makes them more manageable.
8. These different levels of surveillance will re-quire input and data collection from different institutions, including local health care provid-ers, reference laboratories and national health planning agencies.
9. Where sufficient laboratory capacity is not yet available, structured surveys offer a scalable alternative for the identification of bacterial
Plenary Session (III): Veterinary Antimicrobial use and New Surveillance Technologies
19MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
pathogens, their transmission pattern and po-tential high-risk clones.
10. Structured surveys may be of particular interest to countries that cannot yet comply with CAE-SAR surveillance standards.
11. Surveillance must be complemented by AMS pro-grammes to reduce and improve antibiotic use.
Key challenges • The choice of surveillance methods and stew-
ardship strategies should take into account what competencies are regionally available, as these may vary significantly between coun-tries and regions.
• The conduct of surveillance in some of the countries represented at the workshop contin-ues to be hindered by a lack of qualified staff to carry out the relevant tasks.
• Epidemiologists would like to play an active role in surveillance projects and already do so in some of the countries that were represented at the workshop.
• AMS must also address antibiotics available without prescription and involve collaboration with pharmacists and the pharmaceutical in-dustry.
• There is a need to review incentive structures and reimbursement systems for the prescrip-tion of medicines.
20
Programme E 26 FEBRUARY AMS AND THE MULTIDISCIPLINARY TEAM
SESSION FACILITATORS
Ms Ana Paula Coutinho Rehse Dr Danilo Lo Fo Wong Dr Diane Ashiru-Oredope Dr Elizabeth Robilotti Dr Iva Butic Dr Marina Sukhorukova Dr Natali Ivanchik Dr Nienke van de Sande-Bruinsma Dr Oskar Ekelund Dr Saskia A. Nahrgang Professor Stanley Deresinski Dr Tjalling Leenstra
The fifth session focused on the interaction be-tween different team members in the clinical con-text and their respective roles and responsibilities in promoting and ensuring AMS. With input from
clinicians, infectious disease specialists, microbiol-ogists, pharmacists and epidemiologists, the session included both presentations and a panel discussion. In an interactive session, participants were invited to share their own country-specific experiences. They were asked a series of multiple-choice ques-tions related to multidisciplinary work in the context of AMR; the answers were immediately visualized by use of polling devices, enabling the presenters to give direct feedback. From the discussion, a number of characteristic features for successful teamwork on AMS programmes emerged.
Lessons from the panel discussion • At their centre, AMS and infection prevention
and control programmes should seek to pro-actively improve patient safety and patient outcomes, as well as reducing AMR.
• AMS requires a multidisciplinary effort and in-put from health care professionals from a variety of backgrounds. As a result, successful cooper-ation requires mutual support, clear communi-cation paths and regular feedback and review.
• Education of all stakeholders is important and can help to improve clinical decision-making and quality of care. Responsibility for educa-tion programmes should be clearly defined and supported with appropriate resourc-es. To ensure that cooperation is successful, individual responsibilities for necessary tasks should be clearly defined and documented.
• Hospital management and administrators of-ten only support the implementation of AMS programmes after being convinced of their usefulness. This process requires structured communication and continuous updates on progress.
• To document and showcase progress, AMS pro-grammes should define relevant outcome measures in advance and ensure their contin-uous monitoring.
21MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
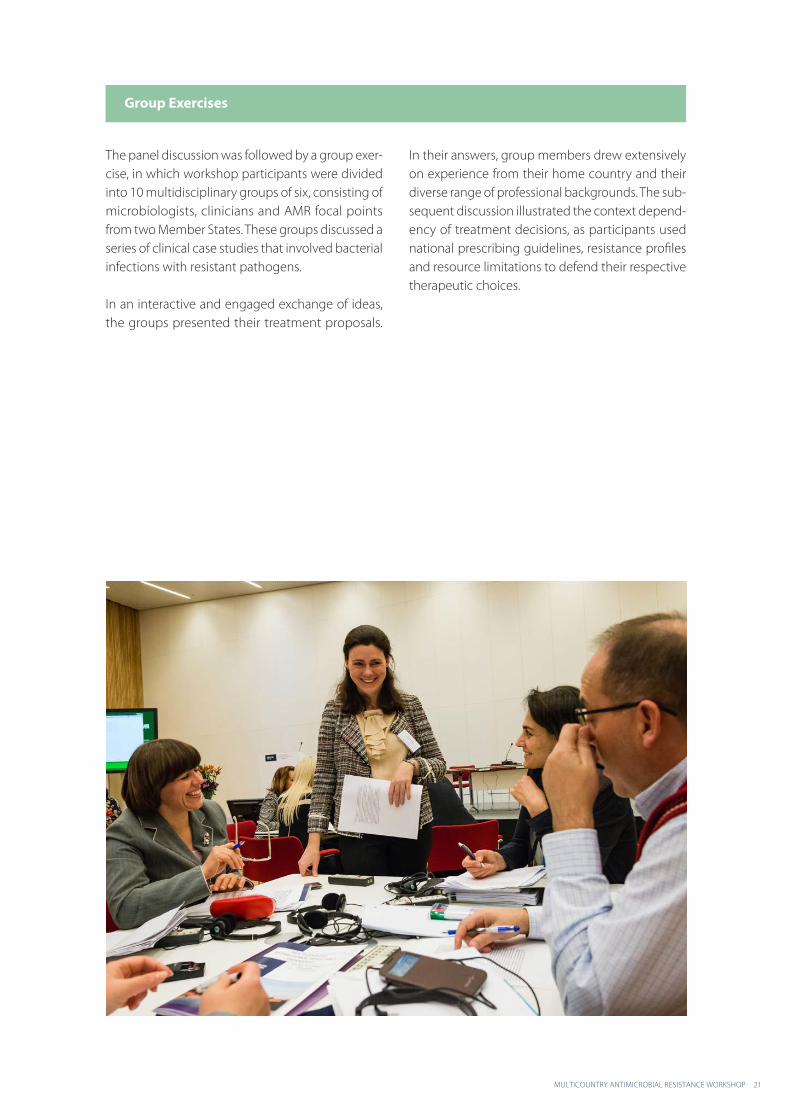
The panel discussion was followed by a group exer-cise, in which workshop participants were divided into 10 multidisciplinary groups of six, consisting of microbiologists, clinicians and AMR focal points from two Member States. These groups discussed a series of clinical case studies that involved bacterial infections with resistant pathogens.
In an interactive and engaged exchange of ideas, the groups presented their treatment proposals.
In their answers, group members drew extensively on experience from their home country and their diverse range of professional backgrounds. The sub-sequent discussion illustrated the context depend-ency of treatment decisions, as participants used national prescribing guidelines, resistance profiles and resource limitations to defend their respective therapeutic choices.
Group Exercises
22
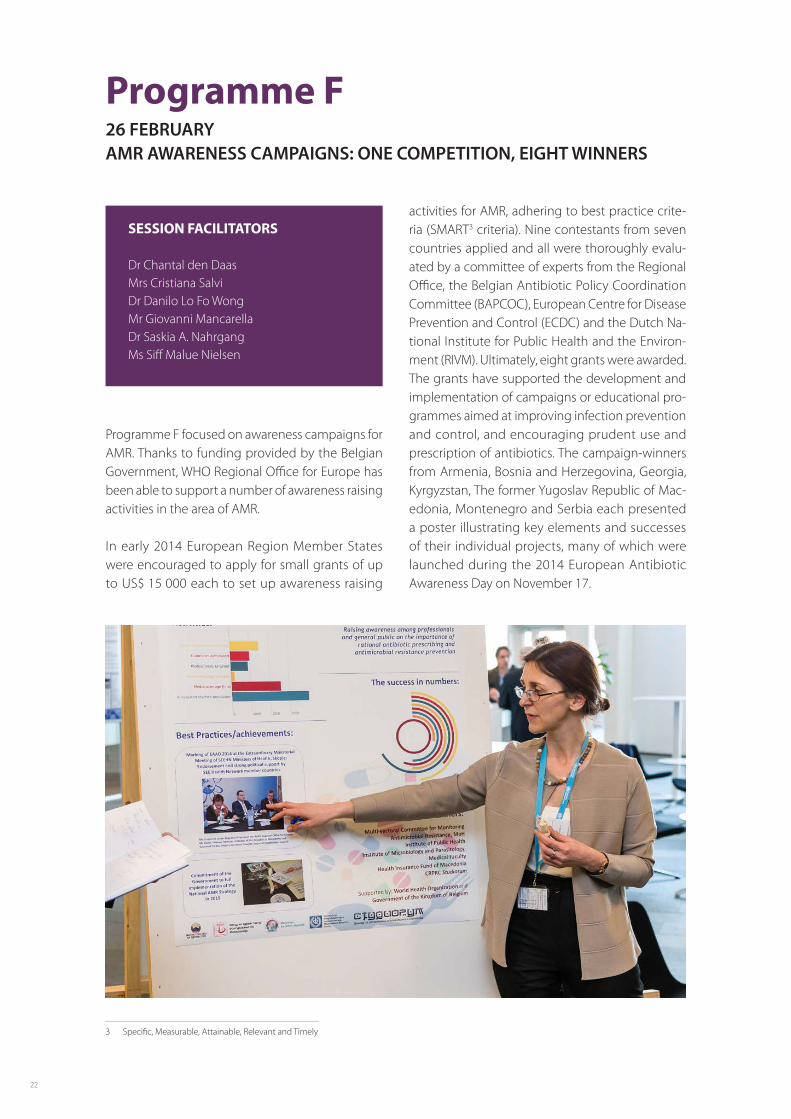
Programme F 26 FEBRUARY AMR AWARENESS CAMPAIGNS: ONE COMPETITION, EIGHT WINNERS
SESSION FACILITATORS
Dr Chantal den Daas Mrs Cristiana Salvi Dr Danilo Lo Fo Wong Mr Giovanni Mancarella Dr Saskia A. Nahrgang Ms Siff Malue Nielsen
Programme F focused on awareness campaigns for AMR. Thanks to funding provided by the Belgian Government, WHO Regional Office for Europe has been able to support a number of awareness raising activities in the area of AMR.
In early 2014 European Region Member States were encouraged to apply for small grants of up to US$ 15 000 each to set up awareness raising
activities for AMR, adhering to best practice crite-ria (SMART3 criteria). Nine contestants from seven countries applied and all were thoroughly evalu-ated by a committee of experts from the Regional Office, the Belgian Antibiotic Policy Coordination Committee (BAPCOC), European Centre for Disease Prevention and Control (ECDC) and the Dutch Na-tional Institute for Public Health and the Environ-ment (RIVM). Ultimately, eight grants were awarded. The grants have supported the development and implementation of campaigns or educational pro-grammes aimed at improving infection prevention and control, and encouraging prudent use and prescription of antibiotics. The campaign-winners from Armenia, Bosnia and Herzegovina, Georgia, Kyrgyzstan, The former Yugoslav Republic of Mac-edonia, Montenegro and Serbia each presented a poster illustrating key elements and successes of their individual projects, many of which were launched during the 2014 European Antibiotic Awareness Day on November 17.
3 Specific, Measurable, Attainable, Relevant and Timely

23MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
The presentation of results was followed by a lively discussion. In each of the presented projects, inter-ventions, activities and information materials had been designed that were tailored to the respective country context. Examples of these were educa-tional sessions for teams in the primary health care setting, and leaflets and posters distributed to the general population. Further examples were infor-mation leaflets sent out to health care professionals signed by the Ministry of Health and pill-shaped candy distributed along with the slogan “antibiotics are not food”.
Each campaign uniquely managed to raise aware-ness about the importance of using antibiotics responsibly and prudently.
The invited experts highlighted several important points: now that a good start has been made, it is important to be even more specific in segmenting the intended target audience and to show the effect of the campaigns in achieving behavioural change. Importantly, a marked difference exists between a so-called spray and pray campaign and a behav-ioural change approach.
Participants also had the opportunity to learn from experts about awareness campaigns during two
presentations. The first was given by Dr Chantal den Daas (RIVM), who discussed the newly established guide for tailoring AMR programmes (TAP). TAP is a tool that can be used to encourage stakeholder involvement, and identify susceptible populations and barriers to prudent use of antibiotics. Moreover, TAP can help in the design of evidence-informed policy responses and to subsequently monitor and evaluate them. The second presentation was delivered by Mr Giovanni Mancarella (ECDC), who talked about good communication practice and illustrated his observations with examples of successful awareness campaigns for the prudent use of antibiotics.
24
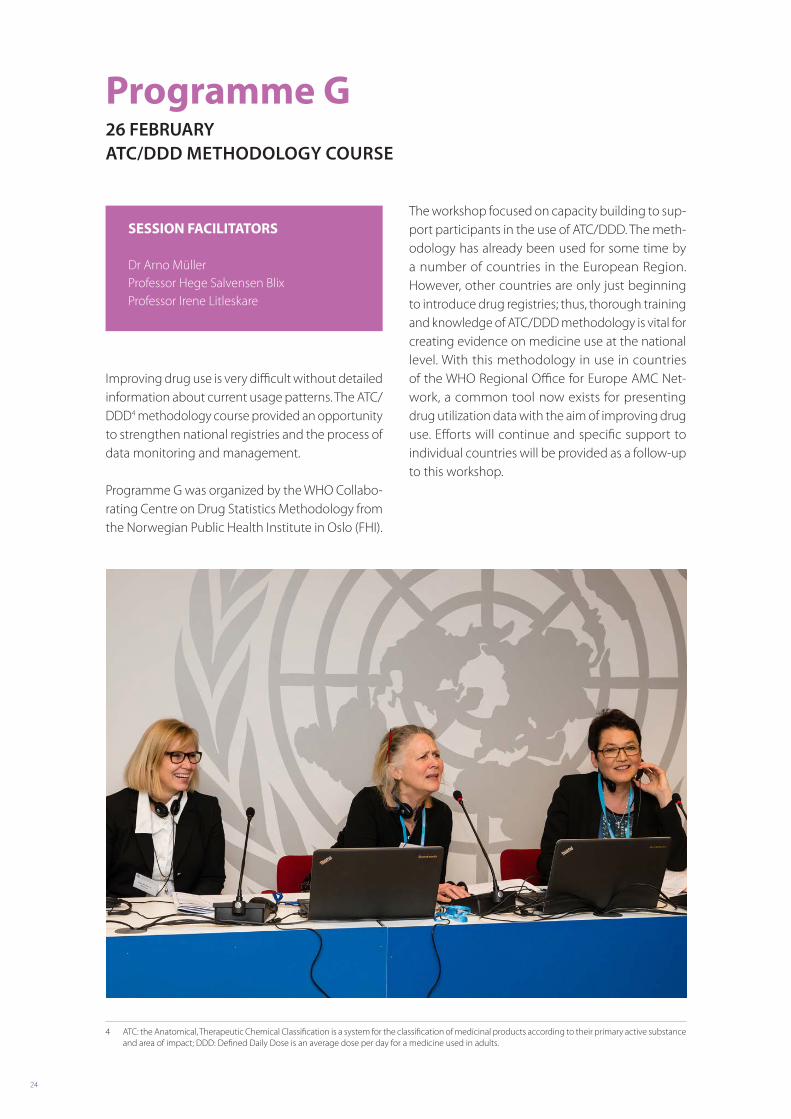
Programme G 26 FEBRUARY ATC/DDD METHODOLOGY COURSE
SESSION FACILITATORS
Dr Arno Müller Professor Hege Salvensen Blix Professor Irene Litleskare
Improving drug use is very difficult without detailed information about current usage patterns. The ATC/DDD4 methodology course provided an opportunity to strengthen national registries and the process of data monitoring and management.
Programme G was organized by the WHO Collabo-rating Centre on Drug Statistics Methodology from the Norwegian Public Health Institute in Oslo (FHI).
The workshop focused on capacity building to sup-port participants in the use of ATC/DDD. The meth-odology has already been used for some time by a number of countries in the European Region. However, other countries are only just beginning to introduce drug registries; thus, thorough training and knowledge of ATC/DDD methodology is vital for creating evidence on medicine use at the national level. With this methodology in use in countries of the WHO Regional Office for Europe AMC Net-work, a common tool now exists for presenting drug utilization data with the aim of improving drug use. Efforts will continue and specific support to individual countries will be provided as a follow-up to this workshop.
4 ATC: the Anatomical, Therapeutic Chemical Classification is a system for the classification of medicinal products according to their primary active substance and area of impact; DDD: Defined Daily Dose is an average dose per day for a medicine used in adults.
25MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Main discussion points1. Discussion focused on the purpose and use of
ATC/DDD, and ATC/DDD for fixed dose combi-nation drugs.
2. The quality improvement circle (collection of data, audit against guidelines, perform interven-tion and observe changes) was discussed along with the importance of providing feedback: (i) locally to prescribers and other relevant health professionals; (ii) nationally to assess changes in the health care system; and (iii) cross-nationally to compare countries.
26
Programme H 27 FEBRUARY FIFTH WHO REGIONAL OFFICE FOR EUROPE AMC NETWORK MEETING
SESSION FACILITATORS
Ms Angela Carp Dr Arno Müller Professor Brian Godman Ms Hanne Bak Pedersen Dr Klaus Weist Ms Lilit Ghazaryan Mr Umut Gurpinar Ms Vesela Radonjic
The final session discussed AMC data from countries that participate in the WHO Regional Office for Europe AMC Network, in order to identify current trends and plan the next phase of collaboration.
Work on gathering wholesale data is ongoing and data from 2012 to 2013 is currently in the valida-tion stage. Analysis will be carried out over the coming months; however, validated data from five network countries was available for discussion at the workshop.
ECDC also shared data from the European Sur-veillance of Antimicrobial Consumption Network (ESAC-Net) and presented outcomes from a recent meeting of the Advisory Committee on Antimicro-bial Resistance and Healthcare Associated Infec-tion (ARHAI). Close collaboration with ECDC has been instrumental in creating the data collected so far, as the method used by the AMC Network is very similar to that of ESAC-Net. ECDC has also assisted with the comparison of data across coun-tries in Europe, and participants of the workshop
27MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
expressed their satisfaction with the collaboration between ECDC and the AMC Network.
During the workshop it was agreed to set up an AMC help-desk in order to support new members of the Network. The Health Technologies and Pharmaceu-ticals (HTP) programme of the Regional Office will coordinate this together with partners.
It was also agreed that the analysis of data from 2011, 2012 and 2013 should be published be-fore the end of 2015. In relation to this work, collaboration with the European Drug Utilization Group (EuroDURG) is established and during the
workshop a member of the EuroDURG Executive Committee discussed recent AMC-related studies and suggested options for collaboration in pub-lishing the findings.
The call for 2014 data will be launched in September 2015 and the next network meeting is scheduled for 9–10 September 2015.
Specific follow-up on findings from the network will be addressed individually at the country lev-el, with the support of the HTP programme and in collaboration with the AMR programme at the Regional Office.
28
Country AMR activity poster session
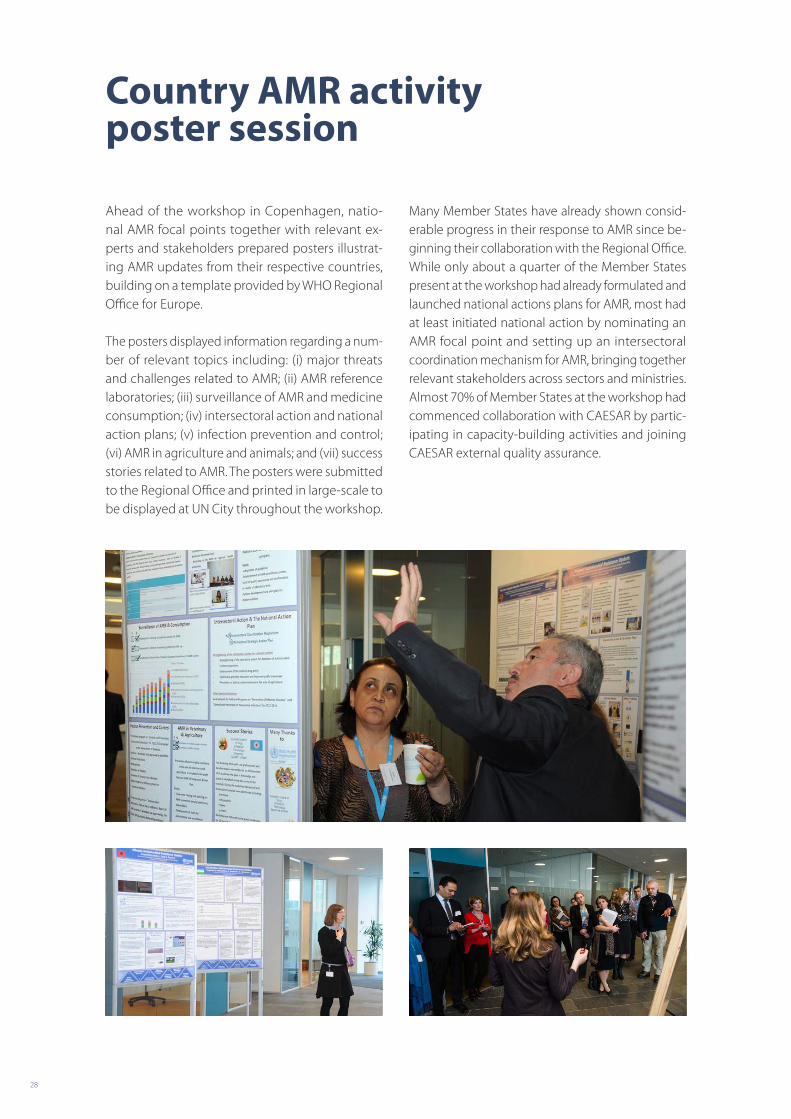
Ahead of the workshop in Copenhagen, na tio- nal AMR focal points together with relevant ex-perts and stakeholders prepared posters illustrat-ing AMR updates from their respective countries, building on a template provided by WHO Regional Office for Europe.
The posters displayed information regarding a num-ber of relevant topics including: (i) major threats and challenges related to AMR; (ii) AMR reference laboratories; (iii) surveillance of AMR and medicine consumption; (iv) intersectoral action and national action plans; (v) infection prevention and control; (vi) AMR in agriculture and animals; and (vii) success stories related to AMR. The posters were submitted to the Regional Office and printed in large-scale to be displayed at UN City throughout the workshop.
Many Member States have already shown consid-erable progress in their response to AMR since be-ginning their collaboration with the Regional Office. While only about a quarter of the Member States present at the workshop had already formulated and launched national actions plans for AMR, most had at least initiated national action by nominating an AMR focal point and setting up an intersectoral coordination mechanism for AMR, bringing together relevant stakeholders across sectors and ministries. Almost 70% of Member States at the workshop had commenced collaboration with CAESAR by partic-ipating in capacity-building activities and joining CAESAR external quality assurance.
29MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Feedback from workshop participants
Forty-eight participants from 19 countries provided structured feedback on the workshop. More than 85% found that the event responded very or extremely well to their expectations, and a similar proportion stated that their knowledge on AMR and related top-ics covered by the workshop had improved a great deal as a result of the event. Almost all respondents found that the content presented throughout the workshop was very relevant for their job.
“Very informative and interactive workshop! It has strengthened intercountry communica-tion and teamwork. Thank you very much and good luck with initiatives and programmes!”
“Thank you for the invitation to participate, and for the opportunity to share my views. Such workshops are really very useful!”
“I think it would be good to pay more attention to the next steps regarding antibiotic resistance awareness campaigns and to discuss the pos-sibility of the publication of the main results of the campaigns that have already taken place.”
“It would be nice, at the next meeting, if you could invite more people from the policy level, for them to hear what the recommen-dations are.”
“The growth of antibiotic resistance is becom-ing a global event. The greatest threat today is the rapid spread of carbapenemase among Enterobacteriaceae, mainly in Klebsiella spp. To counter growing antibiotic resistance is possible only by joint efforts.”
30
Annex 1. List of workshop participants
Albania Admir Malaj Gentian Kasmi Iris Hoxha Lindita Molla Silva Tafaj
Armenia Hasmik Martirosyan Kristina Gyurjyan Lilit Ghazaryan Nune Kotsinyan Nune Krishchyan
Azerbaijan Nazifa Mursalova Rahila Aliyeva Sanubar Salimova Vafa Abilova
Belarus Elena Kacherouskaya Elena Nosova Halina Pyshnik Leonid Titov
Bosnia and Herzegovina Aida Pitic Amela Dedeic-Ljubovic Antonija Verhaz Ljubica Bojanic Pava Dimitrijevic Tijana Spasojevic
The former Yugoslav Republic of Macedonia Aspazija Sofijanova Biljana Kakaraskoska Boceska Golubinka Bosevska
Country Name
31MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Kristina Hristova Neda Milevska Nikola Panovksi Verica Ivanovska
Georgia Irma Korinteli Karaman Pagava Lile Malania Maia Lomtadze Paata Imnadze
Kazakhstan Aigul Shagaltayeva Dinagul Bayesheva Larissa Makalkina Zeynegul Shakenova
Kyrgyzstan Baktygul Kambaralieva Damira Ashyralieva Gulbara Kulushova Talantbek Arstankulov
Republic of Moldova Angela Carp Ludmila Bumakov Olga Burduniuc Radu Cojocaru Rodica Scutelnic
Montenegro Goran Markovic Lidija Cizmovic Ljubica Pejakov Milena Lopicic
Country Name
32
Russian Federation Roman S. Kozlov Sergei Popov
Serbia Branka Terzic Milena Vasic Snezana Jovanovic Vesela Radonjic Zora Jelesic
Tajikistan Azamjon Mirzoev Khurshed Khabibov Nargis Maqsudova Nukra Sinavbarova
Turkey Serap Süzük Umut Emre Gürpinar
Ukraine Aidyn Salmanov Larysa Iakovlieva Olga Golubovska Tetyana Glushkevich
Uzbekistan Abror Kasimov Aybek Khodiev Gulnora Abdukhalilova Iskandar Mavlyanov Muhabbat Ibragimova
Country Name
33MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Annex 2. List of workshop observers
Anna Lubimova
Amrita Sankaranarayanan
Arianit Jakupi
Arsim Kurti
Dennis Raka
Lars Blad
Lul Raka
Casper Larsen
Lotte Stig Nørgaard
Shaip Krasniqui
Susanne Kaae
34
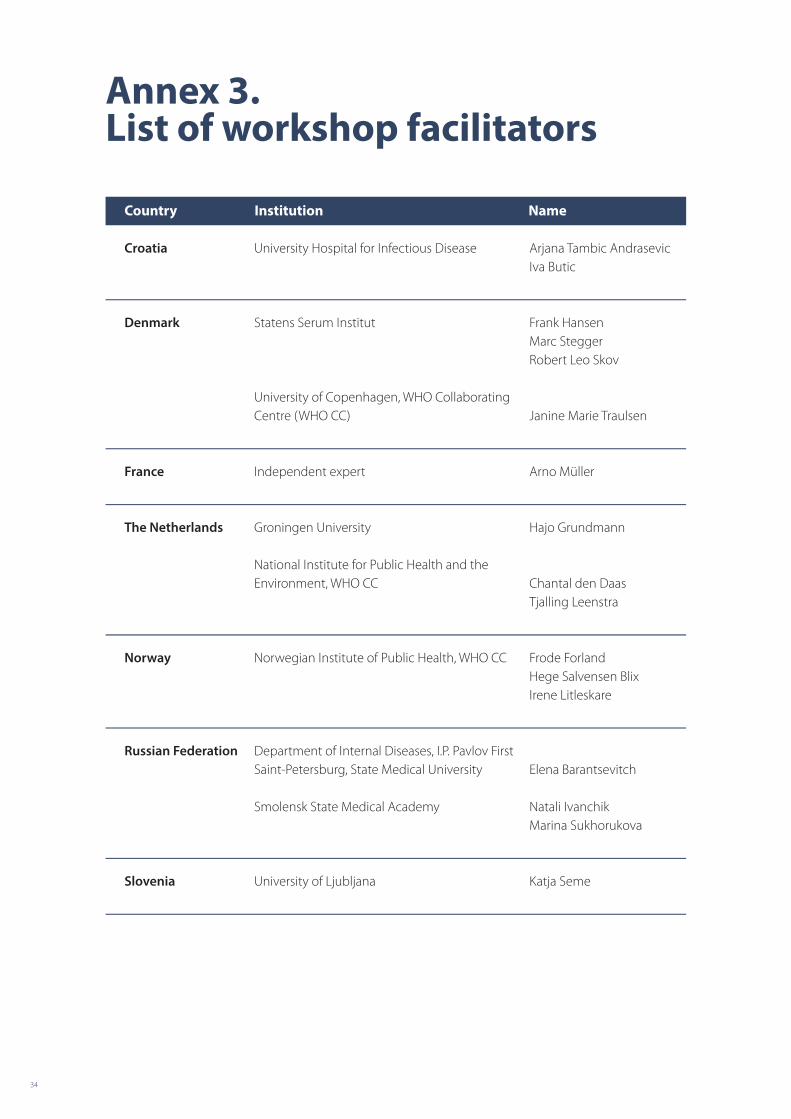
Annex 3. List of workshop facilitators
Croatia University Hospital for Infectious Disease Arjana Tambic AndrasevicIva Butic
Denmark Statens Serum Institut Frank HansenMarc SteggerRobert Leo Skov
University of Copenhagen, WHO Collaborating Centre (WHO CC) Janine Marie Traulsen
France Independent expert Arno Müller
The Netherlands Groningen University Hajo Grundmann
National Institute for Public Health and the Environment, WHO CC
Chantal den DaasTjalling Leenstra
Norway Norwegian Institute of Public Health, WHO CC Frode ForlandHege Salvensen BlixIrene Litleskare
Russian Federation Department of Internal Diseases, I.P. Pavlov First Saint-Petersburg, State Medical University
Elena Barantsevitch
Smolensk State Medical Academy Natali IvanchikMarina Sukhorukova
Slovenia University of Ljubljana Katja Seme
Country Institution Name
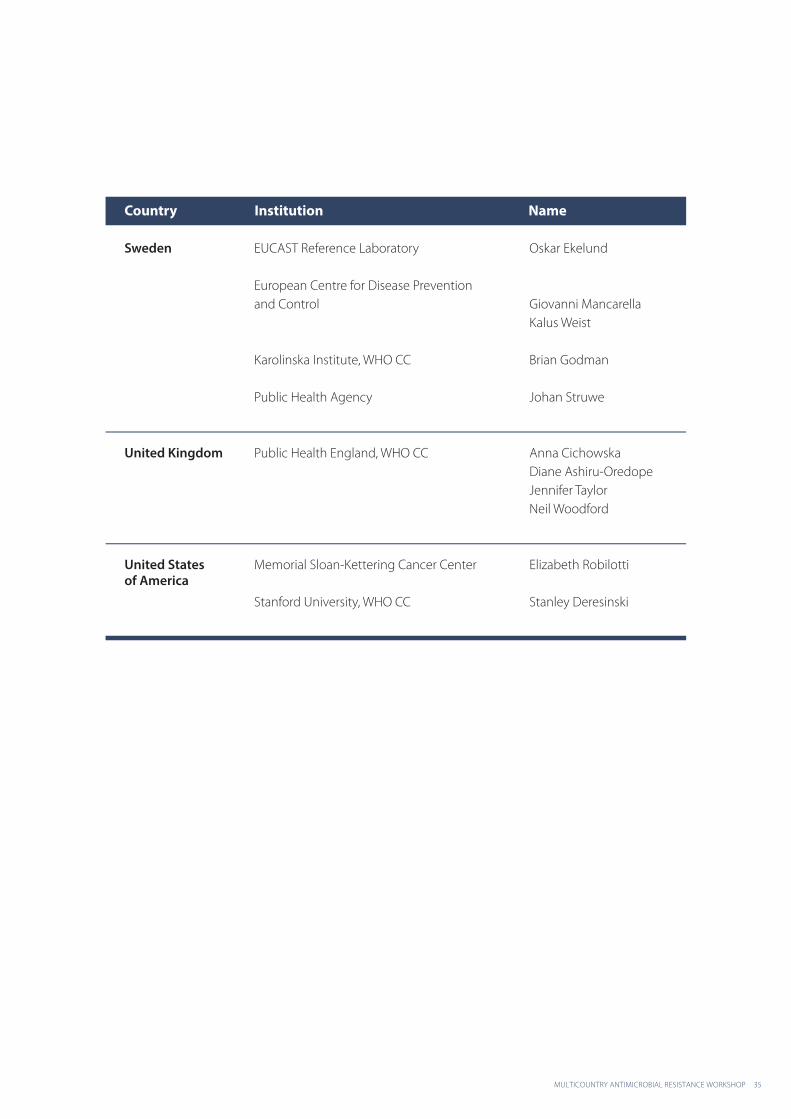
35MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Sweden EUCAST Reference Laboratory Oskar Ekelund
European Centre for Disease Prevention and Control Giovanni Mancarella
Kalus Weist
Karolinska Institute, WHO CC Brian Godman
Public Health Agency Johan Struwe
United Kingdom Public Health England, WHO CC Anna CichowskaDiane Ashiru-OredopeJennifer TaylorNeil Woodford
United Statesof America
Memorial Sloan-Kettering Cancer Center Elizabeth Robilotti
Stanford University, WHO CC Stanley Deresinski
Country Institution Name
36
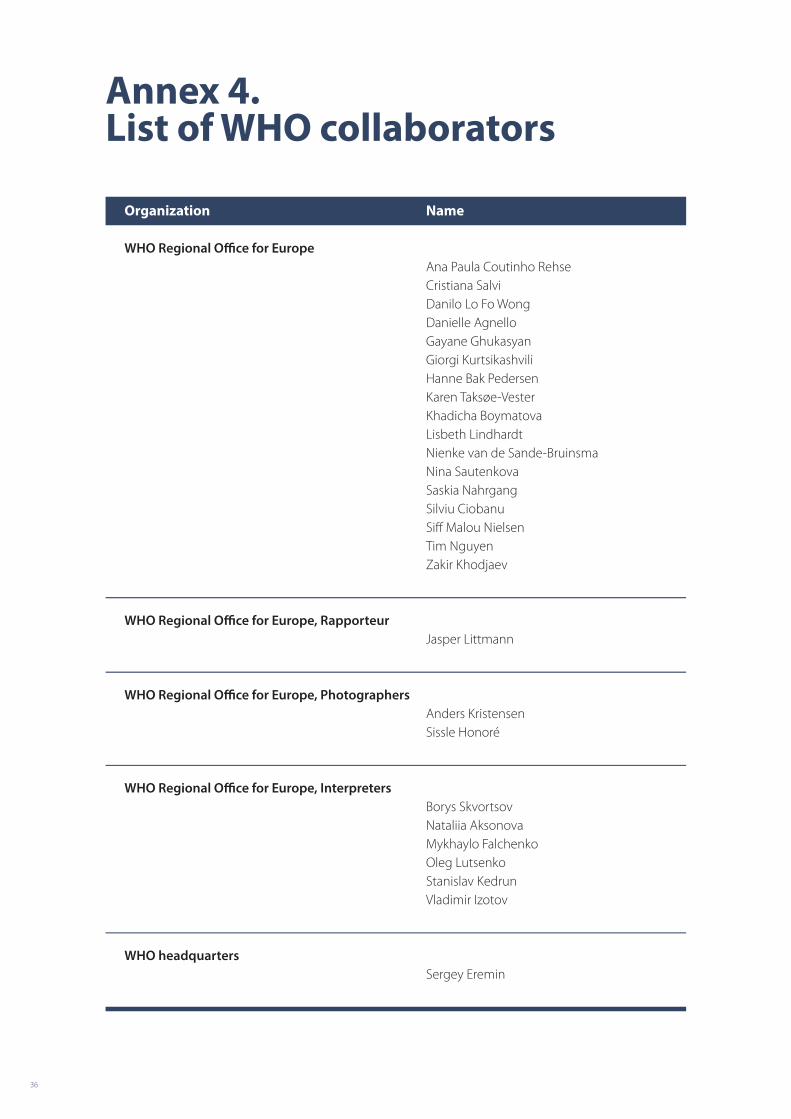
Annex 4. List of WHO collaborators
WHO Regional Office for Europe Ana Paula Coutinho Rehse Cristiana Salvi Danilo Lo Fo Wong Danielle Agnello Gayane Ghukasyan Giorgi Kurtsikashvili Hanne Bak Pedersen Karen Taksøe-Vester Khadicha Boymatova Lisbeth Lindhardt Nienke van de Sande-Bruinsma Nina Sautenkova Saskia Nahrgang Silviu Ciobanu Siff Malou Nielsen Tim Nguyen Zakir Khodjaev
WHO Regional Office for Europe, Rapporteur Jasper Littmann
WHO Regional Office for Europe, Photographers Anders Kristensen Sissle Honoré
WHO Regional Office for Europe, Interpreters Borys Skvortsov Nataliia Aksonova Mykhaylo Falchenko Oleg Lutsenko Stanislav Kedrun Vladimir Izotov
WHO headquarters Sergey Eremin
Organization Name

37MULTICOUNTRY ANTIMICROBIAL RESISTANCE WORKSHOP
Annex 5. Workshop agenda overview
Date TimeMedical micro-
biologists
Hospital clinicans,
ID doctors, national focal
points
Awareness campaign grantees
Pharmacists
Monday 23 February
Arrival Arrival
Tuesday 24 February
08:00 Bus to SSI
Arrival Arrival
09:00 – 12:00Programme A:
Laboratory Workshop
Programme B: Use of Antimicro-
bial MedicineLunch break
13:00 – 17:00
17:30 Bus to Admiral Hotel
Wednesday 25 February
08:00 Bus to UN City
08:00 Bus to SSI
09:00 – 11:30 Programme A: Laboratory Workshop
Programme C: Principles of AMSProgramme B:
Use of Antimicro- bial Medicine11:30 – 12:00
12:00 – 13:00 Lunch at UN City
13:00 – 17:00 Programme D: Plenary Session
17:30 – 20:00 Reception at UN City
20:00 Bus to the hotel Return to the hotel
Thursday 26 February
08:15 Bus to UN City
09:00 – 12:00Programme E:
AMS and the Multidisciplinary Team
Programme F: AMR
Awareness Campaigns
Programme G: ATC/DDD Course
12:00 – 13:00 Lunch Poster Presentations (displayed)
13:00 – 17:00Programme E:
AMS and the Multidisciplinary Team
Programme F: AMR
Awareness Campaigns
Programme G: ATC/DDD Course
17:30 Departure Return to the hotel
Friday 27 February 09:00 – 17:00
Programme H: Review and Discussion
The WHO Regional Office for Europe
The World Health Organization (WHO) is a specialized agency of the United Nations created in 1948 with the primary responsibility for international health matters and public health. The WHO Regional Office for Europe is one of six regional offices throughout the world, each with its own programme geared to the particular health conditions of the countries it serves.
Member States
AlbaniaAndorraArmeniaAustriaAzerbaijanBelarusBelgiumBosnia and HerzegovinaBulgariaCroatiaCyprusCzech RepublicDenmarkEstoniaFinlandFranceGeorgiaGermanyGreeceHungaryIcelandIrelandIsraelItalyKazakhstanKyrgyzstanLatviaLithuaniaLuxembourgMaltaMonacoMontenegroNetherlandsNorwayPolandPortugalRepublic of MoldovaRomaniaRussian FederationSan MarinoSerbiaSlovakiaSloveniaSpainSwedenSwitzerlandTajikistanThe former Yugoslav Republic of MacedoniaTurkeyTurkmenistanUkraineUnited KingdomUzbekistan
World Health OrganizationRegional Office for EuropeUN City, Marmorvej 51, DK-2100 Copenhagen Ø, DenmarkTel.: +45 45 33 70 00 Fax: +45 45 33 70 01 Email: [email protected]: www.euro.who.int