Embed Size (px)
Citation preview

Report of the 2010 Global NGO Deworming Inventory
Children Without Worms
Submitted to WHO STAG Working Group on Access to Essential Medicines
April 17, 2012
Executive Summary
The Preventive Chemotherapy (PCT) Databank, managed by the World Health Organization (WHO), is
the primary repository for records of annual treatments conducted globally to control soil-transmitted
helminthiasis (STH). Ministries of Health provide reports on STH treatments conducted in their countries
to the WHO for inclusion into the Databank. Non-governmental organizations (NGOs) often provide
treatments for STH in multiple countries. However, the reporting mechanisms for incorporating NGO-
delivered STH treatments into the Databank are not well-defined, and the extent of the gap in treatment
reporting is not well understood.
The Global NGO Deworming Inventory was created to quantify the gap in annual reporting of
treatments conducted by NGOs targeting school-age children at risk for STH. In 2010, the Inventory was
carried out by Children Without Worms (CWW) to capture treatments in 2009. In 2011, CWW once
again carried out the Inventory for the purpose of identifying “unique treatments” conducted by NGOs
in 2010 that had not previously been reported to WHO for inclusion in the PCT databank.
NGOs reported 65.4 million STH treatments to the 2010 Inventory that were not delivered as part of the
Program to Eliminate Lymphatic Filariasis (PELF), 25% of the 260.7 million treatments in the WHO PCT
databank for 2010. Of these 65.4 million treatments, the 2010 Inventory identified 23.3 million (35.6%)
that had not previously been reported to WHO via Ministries of Health and were therefore considered
“unique” to the Inventory. The 23.3 million unique treatments identified by the Inventory represent
8.9% of all non-PELF STH treatments in children reported to the PCT databank. Of these, 7.2 million
treatments were identified in pre-school-age children (PSAC), representing 4.9% of all non-PELF STH
treatments reported to the PCT databank for this age group, and 16.1 million treatments were identified
in school-age children (SAC), 14.2%. Of all unique treatments identified via the Inventory, 93% of
unique treatments of pre-school-age children and 97% of unique treatments of school-age children
came from countries which had not submitted STH reports to WHO.
The NGO Deworming Inventory has provided a complementary approach to collecting data on STH
treatments for 2009 and 2010 by estimating the treatment reporting gap for the inclusion of NGO-
administered treatments for STH into the WHO’s PCT Databank. Low response rate, uncertain data
quality, and imprecise case definitions limit the robustness of these findings. The Inventory results
highlight the need to strengthen the reporting mechanisms for non-PELF STH treatments between
Ministries of Health and the WHO, and to devise strategies to ensure that NGO-delivered treatments are
integrated into Ministry of Health reports.

2
Background
In 2001, World Health Assembly (WHA) Resolution 54.19 set forth recommendations for the control of
soil-transmitted helminthiasis (STH) through regular administration of preventive chemotherapy (PCT)
to at least 75% of all school-age children at risk of STH-related morbidity by the year 2010. This goal
equates to treating at least 457 million1 school-age children annually, in many areas twice per year. To
track progress towards this goal, the WHO PCT databank2 compiles annual deworming treatment data
from Ministries of Health (MOHs). However, the PCT Databank does not typically receive treatment data
from non-governmental organizations (NGOs), which often provide deworming treatment to at-risk
populations as a component of child/community health campaigns.
The Global NGO Deworming Inventory (hereafter referred to as the Inventory) has been created to
address this data gap. Specifically, the objectives of the Inventory are to:
1. Capture and collate data on NGO deworming treatments into a centralized, reliable database
that can be integrated with the WHO PCT databank;
2. Enumerate the extent and scope of NGO deworming activities worldwide; 3. Provide a platform for sharing information on country-level treatment activities amongst
deworming programs.
In 2010, the WHO Working Group on Access to Assured-Quality Essential Medicines for Neglected
Tropical Diseases (WGA) requested Children Without Worms (CWW) to survey and compile deworming
data from NGOs worldwide via the Inventory. In the first Inventory, CWW compiled available treatment
reports from NGOs that conducted deworming of school-age children in 2009. The development of the
2009 Inventory, including the establishment of partnerships, creation of treatment reporting forms, and
development of communications and outreach strategies is described in reports available at
http://www.deworminginventory.org/reports. The 2009 Inventory identified 18.5 million treatments3
for STH using albendazole or mebendazole4 that had not been reported previously to WHO by either
Ministries of Health or NGOs. These treatments uniquely captured by the Inventory were subsequently
added to the PCT databank and represented approximately 17% of 107 million reported STH treatments
of school-age children in 2009 that were not delivered as part of the Program to Eliminate Lymphatic
Filariasis (PELF) 5. These results, along with other information gathered by the Inventory such as regional
1 WHO Weekly Epidemiological Record, No. 25, 2011, 86, 257–268. http://www.who.int/wer
2 http://www.who.int/neglected_diseases/preventive_chemotherapy/sth/en/index.html
3 54.8 million SAC treatments with only albendazole or mebendazole were reported to the 2009 Inventory; 18.5
million (33.8%) of these treatments were previously unreported to WHO. An additional 8.1 million treatments with ivermectin, DEC, or praziquantel—alone or in combination with mebendazole or albendazole—were reported to the 2009 Inventory. 4 An additional 2.3 million treatments using combinations of praziquantel, ivermectin, DEC, mebendazole or
albendazole that had not previously been reported to the WHO were also identified via the 2009 Inventory, for a total of 20.8 million unique treatments identified. For the purposes of this report, treatments identified via the Inventory that co-targeted STH in conjunction with lymphatic filariasis or schistosomiasis treatments are excluded. 5 107 million treatments of school-age children with either albendazole or mebendazole alone were reported,
representing the total number of treatments for STH that were not co-administered with another drug for treatment of lymphatic filariasis or schistosomiasis. (PCT Databank administrator)

3
deworming activities, were compiled and made available on
http://www.deworminginventory.org/reports. Presentations on the Inventory were given at the WHO
STAG WGA in April 2011 and M&E Workgroup meetings and to the CORE Group Annual Meeting in May
2011. Links to a PowerPoint presentation were provided on the websites of partners, including RTI and
USAID. The purpose of the presentation was to raise awareness of the project and its results.
WGA Recommendations from the 2009 Inventory
The following section outlines actions taken by CWW to implement recommendations of the WGA
following the 2009 Inventory.
Recommendation 1: The Inventory should be continued, and NGOs need to be encouraged to
participate in the Inventory and record treatment data.
The Inventory was repeated in 2010 in accordance with this recommendation. In addition to
encouraging participation in the Inventory from targeted NGOs, CWW utilized the Inventory as a tool to
advocate for the collection of robust data on deworming treatments. Save the Children’s School Health
and Nutrition team worked with CWW to modify their treatment reporting form after identifying gaps in
data requested by the Inventory and previous treatment reports provided by Save the Children. The new
version of Save the Children’s deworming treatment reporting form will be utilized in 2012 by country
offices. This collaborative effort is an example of how NGOs can modify their data collection processes
to facilitate sharing data with the WHO PCT database.
Recommendation 2: WHO should send letters to Regional WHO focal points and Ministries of Health,
informing them of the results of the Inventory and encouraging them to collaborate with NGO
implementing deworming activities in their country.
CWW sent multiple requests via email for assistance in identifying and verifying NGOs operating in all
WHO regions. The PAHO office provided substantial support by directly and repeatedly contacting NGOs
operating in Latin America and the Caribbean to encourage their participation in the 2010 Inventory.
Recommendation 3: CWW should survey NGOs that did not participate in the 2009 Inventory to
determine how to increase future participation.
CWW carried out a survey in July 2011 to evaluate the 2009 data submission process, assess the
usefulness of the Inventory website and available reports, and gauge interest in participation in the 2010
Inventory. One hundred eighty-six individuals from 90 organizations that were targeted for the 2009
Inventory were contacted via email requesting their participation in the survey. After multiple email
follow-up attempts, six responses were received, representing participation from 4% of organizations
solicited.
Of these six responding organizations, four had participated in the 2009 Inventory, and two indicated
they were not aware of the activity and therefore had not participated. The four organizations that
participated in the 2009 Inventory rated the data submission process as “easy” (n=2) or “somewhat

4
easy” (n=2). All six organizations that participated in the survey indicated they intended to participate in
the 2010 Inventory. Suggestions were provided to improve the Inventory, such as establishing a
designated reporting mechanism and contact person within each country to link NGO and MOH
treatment data, and to improve the coordination of reporting among NGO deworming programs.
No suggestions were made for substantial changes to the Inventory data collection process.
Methods
Data collection
The 2010 Inventory was conducted using the same methods that were used for the 2009 Inventory.6
The Inventory treatment reporting form was revised based on lessons learned from the 2009 data
collection process; these changes are listed in Table 1. The inclusion of additional data elements was
intended to better identify overlapping treatments between the Inventory and the PCT databank. Two
data elements were removed from the 2010 Inventory. First, the disease(s) targeted was no longer
requested, as this information could be inferred from the drugs used in treatment. Second, information
on previous year treatments and upcoming year treatment plans was deemed unnecessary.
NGOs targeted for the 2010 Inventory included those participating in the 2009 Inventory7, along with an
additional 30 organizations that had been identified since the 2009 Inventory using the same methods.
Contact information was updated through online research and direct contacts. A total of 120
organizations were contacted by email and phone to solicit participation in the 2010 Inventory.
Organizations were contacted multiple times via phone and email beginning in June 2011, and outreach
was concluded in December 2011. In addition to direct contacts, the invitation to participate in the
Inventory was widely disseminated by key partners (CORE, InterAction, USAID, RTI, GNNTD, Deworm the
World, SCI) via mailing lists, website postings, and social media platforms.
In addition to surveying NGOs that conducted deworming treatments in 2010, the Inventory surveyed
non-implementing NGOs that donated deworming drugs to implementing partners. These NGOs were
provided the same instructions and forms as implementing NGOs, but were not expected to complete
the treatment reporting data fields.
6 2009 Global NGO Deworming Inventory Final Report; www.deworminginventory.org/reports
7 From the 2009 NGO Deworming Inventory Final Report: “An online search was conducted using key words and
phrases such as deworming, mass drug administration, antiparasitic treatment for children, helminth control, etc, to identify relevant programs. Once organizations were identified, they were contacted to obtain accurate contact information for the person(s) responsible for the deworming program. In addition to the online search, key partners were also asked to help identify deworming programs in the countries in which they work.”

5
The 2009 Inventory had excluded organizations that dewormed fewer than 50,000 individuals annually
in an effort to simplify the data collection process8. However, this restriction was lifted for the 2010
Inventory as it was apparent from 2009 results that relatively few participating organizations fell below
the exclusion threshold. It was also decided that there was value in capturing all deworming treatments
reported to the Inventory, and that excluding data based on threshold criteria might result in the loss of
useful information.
Validation
The data validation process began with CWW reviewing the online submissions by NGOs to ensure that
treatment reports included the critical data elements requested (country, district, population treated,
drug(s) used, treatment figures, number of treatment rounds.) Where necessary, organizations were
contacted to clarify any questions and gaps in the data submitted. Following this initial review and
cleaning of the data, treatment figures for each NGO were compiled at the country level and, where
possible, at the district level.
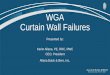
The PCT Databank administrator participated in the validation of Inventory data to assess which NGO-
conducted treatments captured via the Inventory might be considered “unique,” i.e. not previously
reported to the WHO by either Ministries of Health or NGOs and therefore, not already included in the
PCT Databank records for 2010. Figure 1 illustrates the reporting streams by which treatment figures are
channeled to the WHO PCT Databank.
Definitions
“Definitely unique treatments” were defined as treatments reported to the Inventory by NGOs (pathway
2 in figure 1) in countries for which WHO received no STH treatment reports, either from Ministries of
Health (pathway 2) or from the NGOs directly (pathway 3).
“Possibly unique treatments” were defined as treatments reported to the Inventory by NGOs (pathway
2 in Figure 1) that were not included in the reports that the Ministry of Health submitted to the WHO PCT
Databank (pathway 1b). Ministries of Health do not typically disaggregate treatments by the name of
the NGO that administered them. Therefore, to determine if NGO treatments had already been
included in Ministry of Health reports to the WHO PCT databank, WHO asked Ministries of Health to
review the dates, districts, age group treated, and number of treatments reported by NGOs to the
Inventory and compare them with those reported by the Ministry. Because duplicate reporting could
not always be ruled out, these treatments are considered possibly, but not definitively, unique.
8 From the 2009 NGO Deworming Inventory Final Report: “All organizations were asked to complete an online
survey. If programs provided treatment to more than 50,000 children in one country and had only country-level treatment data, they were asked to provide national-level treatment data via the online survey. Programs that treated fewer than 50,000 children were not asked to provide further information (this equated to four organizations). If programs provided treatment to more than 50,000 children and had sub-national level treatment data, they were asked to download the excel-based treatment reporting form and provide district level treatment data.”

6
For brevity, the terms “unique” and “possibly unique” are considered together as “unique” for the
remainder of the analysis and discussion, except where noted in the text.
Results
Of the 120 NGOs surveyed, 19 (15.8%) provided data for either treatments or for donations to other
implementing NGOs in 2010 (Table 2).
Eight organizations provided data via the Excel treatment reporting form; eight organizations submitted
their own treatment reporting forms, and three organizations submitted treatment data in the body of
an email.
Treatment figures from one NGO were included as a result of having removed the 2009 requirement
that excluded organizations that dewormed fewer than 50,000 individuals annually.
Treatments with albendazole and another drug, such as ivermectin or DEC, were reported to the
Inventory despite these combined treatments being administered primarily for treatment of lymphatic
filariasis, with deworming occurring as a co-benefit of the administration of albendazole. Treatments
with only praziquantel were also reported, along with combined treatments administering praziquantel
with a benzimidazole (albendazole or mebendazole) for combined targeting of schistosomiasis and STH
(Table 3).
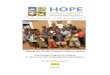
The analysis was restricted to treatments targeting STH, using albendazole or mebendazole alone, i.e.,
not in combination with another drug. Therefore, treatments that were co-administered with another
drug for lymphatic filariasis and/or schistosomiasis were excluded from the analysis (Figure 2).
Regional Distribution of Non-PELF STH Treatments Reported to the Inventory
More than half of the countries for which NGOs reported treatments to the Inventory were in Africa
(Figure 3).
Gaps in treatment reporting identified by the Inventory: Unique treatments
Unique treatments
Of the 65.4 million treatments identified by the Inventory for pre-school- and school-age children using
albendazole or mebendazole only (i.e., non-PELF treatments), 23.3 million (35.6%) had not previously
been reported to the WHO for inclusion in the PCT databank, and were therefore categorized as unique.
Of these 23.3 million unique treatments, 7.2 million were identified in pre-school-age children (11% of
all treatment reports for this group received by the Inventory) and 16.1 million in school-age children
(24.6% of all treatment reports for this age group received by the Inventory).
Definitely unique treatments
Of the 16.1 million unique treatments identified for SAC, 15.6 million (97%) were reported to the
Inventory from countries for which WHO had received no non-PELF STH reports from the Ministry of

7
Health. These treatments were considered as definitely unique. For PSAC, this figure was 6.7 million
(93%).
Possibly unique treatments
The remaining unique treatments in the Inventory were considered possibly unique. In these cases,
Ministries of Health had reported non-PELF STH treatments to the WHO PCT databank but further
investigation revealed that some NGO treatments had not been included in the Ministry of Health
report.9 For SAC, 518,049 possibly unique treatments were identified (3% of all unique SAC treatments
identified via the Inventory. For PSAC, this figure was 500,000 treatments (7% of all unique PSAC
treatments identified via the Inventory).
Contribution of unique treatments to overall STH treatments in the PCT Databank
The 23.3 million unique treatments identified by the Inventory represent 8.9% of all non-PELF STH
treatments in children reported to the PCT databank in 2010. For PSAC this proportion is 4.9%,
compared to 14.2% for SAC.
Regional distribution of unique treatments
The region with the greatest contribution of unique treatments (PSAC and SAC combined) was Africa.
The Southeast Asia region provided the majority of unique SAC treatments, and the Africa region
provided the majority of unique PSAC treatments (Figures 4, 5, and 6).
Regional and country-level differences in the percentage of unique treatments identified via the
Inventory are shown in Tables 4 and 5, respectively.
Discussion
The 2010 Inventory indicates that NGOs delivered at least 65.4 million treatments for STH with
albendazole or mebendazole only to pre-school- and school-age children in 2010. This represents 25%
of the estimated 260.7 million non-PELF treatments for STH reported to WHO. Thus, at a global level,
NGOs deliver a substantial percentage of all non-PELF global deworming treatments.
9 1.1 million unique treatments of pre-school and school-age children combined (4.7% of all unique treatments)
were identified through cross-checking reports submitted by NGOs to both the WHO and the Inventory. Two
organizations (Save the Children and SCI) submitted treatment reports to both the WHO and the Inventory. These
reports were compared to one another, and discrepancies identified between the reports submitted to WHO and
the Inventory by Save the Children. (No discrepancies were found between reports submitted by SCI to WHO and
the Inventory). Save the Children staff was asked to confirm treatment figures with their country offices and
provide verified figures. The reasons for the discrepancies in reporting were late/updated reporting figures being
received from country offices, and errors in calculation. As a result of this cross-check, 1.1 million additional
treatments were identified that had not previously been reported to WHO for inclusion in the PCT Databank.

8
Of the 65.4 million treatments reported to the Inventory, 23.3 (35.6%) were considered ‘unique’ –
reported only to the Inventory – and were added to the PCT databank. Among SAC, for whom data
were available for both 2009 and 2010 inventories, the proportion of treatments identified as unique
was 17% and 14.2%, respectively. These data suggest that the reporting gap is fairly stable, or at least
not increasing, over the two-year period.
Considerable regional variation was observed. The proportion of all treatments that were classified as
unique was highest in Southeast Asia (92%), a figure that was driven by the data from Bangladesh. The
Americas had the second-highest ratio of unique to non-unique treatments; this was likely a result of
extensive outreach to NGOs in the region by the PAHO office. No treatments were reported from the
European region; this is a departure from the 2009 Inventory, which received 645,024 treatments, all of
which were all unique.
Eight NGOs provided all of the unique treatment figures captured by the Inventory (Table 6). Two NGOs
(Children Without Worms and Deworm the World) provided 75% of all unique SAC treatment figures.
Five NGOs provided the remainder of unique SAC treatments (range: <1 – 11%.) One NGO (Helen Keller
International) provided more than 80% of all unique PSAC treatments reported to the Inventory.
The NGO that contributed the highest number of unique SAC treatments to the PCT databank, Children
Without Worms, submitted treatment data for SAC in Bangladesh—also the country with the highest
number of unique SAC treatments captured via the Inventory. Deworm the World, which contributed
the second-highest number of unique SAC treatments, submitted treatments from Cote d’Ivoire, Guinea,
Gambia, India, Madagascar, Mali, and Sao Tome. These countries represent 4,046,710 million (25%) of
all unique SAC treatments identified via the Inventory. The treatment figures from Helen Keller
International came from Tanzania, where over 80% of the unique PSAC treatments identified via the
Inventory were administered.
While the intention of the Inventory was to identify treatment reporting gaps between the NGOs and
Ministries, 93% of all unique PSAC treatments and 97% of all unique SAC treatments reported to the
Inventory came from countries for which WHO had not received STH treatment reports from the
Ministries of Health. This suggests that the Inventory is primarily identifying a treatment reporting gap
between country governments and WHO, rather than between NGOs and Ministries of Health. For the
Ministries of Health that did not report non-PELF treatments to WHO, it is not clear in all cases whether
they received treatment reports from the NGOs. Therefore, reporting from NGOs to Ministries of Health
may also need to be enhanced.
Limitations
The strength of the conclusions that can be drawn from the 2010 Inventory is limited by several factors.
Low response rate
First, despite repeated attempts to contact NGOs (an estimated 800 hours of staff time), the response
rate to the Inventory was extraordinarily low. Thus, the inventory may have under-estimated the global

9
scope of NGO involvement in deworming. The reasons for the reduced number of submissions to the
2010 Inventory (20) compared to 2009 (24), despite significantly enhanced efforts to solicit reports, are
unclear, but may include the following:
1. Lack of resources to commit to completing the Inventory form.
During the July 2011 survey to assess the 2009 Inventory results, the staff from some NGOs targeted by
the Inventory told CWW that they didn’t have time or staff capacity to complete the Inventory.
2. Possibly fewer NGOs involved in deworming in 2010.
The increased donations of mebendazole and albendazole announced by Johnson & Johnson and
GlaxoSmithKline in 2010 may have led to reductions in deworming programs led by NGOs. In addition,
changes in the laws for valuing gift-in-kind contributions10 beginning in mid-2009 have required
organizations that previously valued donated deworming medications as high as $9.07 per pill to
decrease the value to 35 cents per pill, drastically reducing the amount of revenue that could be claimed
by these organizations.11 This decreased valuation might have led to fewer organizations involved in
deworming in 2010. Further, integration of deworming treatments into national neglected tropical
disease (NTD) control programs led by Ministries of Health might have resulted in a decrease in
deworming treatments being independently conducted by NGOs. Integration of NTD control may be
mitigating the issue of NGOs conducting deworming programs outside of the government’s control or
awareness, and resulting in reporting of these treatments by NGOs to the Ministries of Health and, from
there to the PCT databank.
3. Lack of recognition of the value of treatment reporting; lack of treatment data.
A primary purpose of data collection is to enable effective use of data by stakeholders. However, the
NGOs that participated in the 2009 Inventory did not have timely access to the Inventory results, which
were posted on the NGO Inventory website in mid-2011, and were therefore unable to utilize the data
to which they contributed.
At its inception, the Inventory project was considered as a possible mechanism for better coordination
of deworming efforts led by NGOs. However, the Inventory collects data on the previous year’s activities
and the subsequent delay in publication of reports have made it unrealistic to expect NGOs to utilize
Inventory reports to coordinate their deworming activities. (To illustrate this example, consider that the
2010 Inventory contained treatment figures from 2009 that were collected and analyzed in late 2010,
and these data were not made available to the public until June 2011. This time-lag meant that NGOs
were already conducting their 2011 deworming campaigns by the time information on where other
NGOs were operating became available. Similarly, the 2010 Inventory reports will not be available until
the second quarter of 2012, at which time many NGOs will already have planned and begun their annual
deworming activities for the year.)
10
Financial Accounting Standards Board Statement No. 157. http://www.fasb.org/summary/stsum157.shtml 11
“Aid Charities’ Accounting Practices Draw Criticism.” Caroline Preston, The Chronicle of Philanthropy, Sep. 18, 2011.

10
In addition to a lack of recognition of the value of treatment reporting, it is probable that incomplete
treatment recording by some NGOs further impacts the ability to accurately measure the number of
treatments conducted in a given year. Some NGOs do not accurately or consistently record treatment
data when conducting deworming campaigns. Small NGOs and faith-based missions might conduct
deworming as a supplement to larger projects or programs, and therefore keeping accurate records of
this activity might be low priority. Smaller groups might lack the capacity to effectively record treatment
data, and choose instead to allocate their resources to implementation and other activities; this also
occurs for larger NGOs operating with limited budgets and staff.
4. Lack of buy-in for the Inventory project across sectors
As the administrators of the Inventory, CWW engaged with multiple partners to promote the project.
Response and support from key partners in the Inventory was mixed; treatment data were not received
from several key partners or only received after months of reminders. Lack of responsiveness from key
partners raises questions about whether the Inventory project could serve as a rallying point for the STH
control community. The level of success of the Inventory project in achieving aim three (making links
between NGOs conducting deworming and thereby strengthening the sense of partnership amongst
NGOs conducting deworming is uncertain12.
“Possibly unique” treatments
While 500,000 PSAC treatments and 518,049 SAC treatments reported to the Inventory were identified
as possibly unique treatments, it is likely that some of these might duplicate treatments reported by
MOH. MOH reports to WHO generally do not provide the names of NGOs that delivered the treatments
being reported to WHO, which limits the cross-checking that can be done to verify the uniqueness of
treatments reported to the Inventory.
Duplicate accounting of tablets
There is a strong possibility of duplicate reporting of the number of tablets donated for deworming by
the six NGOs that provided these data to the Inventory. This is inherent in the complex donation and
treatment chain among multiple NGOs. An example of this duplicate reporting was uncovered during
the data solicitation phase of the Inventory. An NGO called The Worm Project donated approximately 3
million tablets of albendazole to various other NGOs in Honduras. One of these NGOs, The MAMA
Project, in turn donated approximately 63,000 tablets of albendazole received from the Worm Project to
other local NGOs for distribution. However, both the Worm Project and the MAMA Project reported the
12
Circumstantial evidence may indicate the project succeeded in raising awareness of how individual NGO activities fit into the global landscape of STH control. The efforts of CWW to solicit participation by phone and email undoubtedly raised awareness of the project and engaged multiple NGOs. The Inventory website was another tool for engaging the NGO deworming community; tracking of visits to the Inventory website reveals that www.deworminginventory.org received 1,900 page views by 672 unique visitors from 74 countries between June and December 2011. Further examination of visits shows that 18% of visitors accessed the site via a search engine, indicating that knowledge of the Inventory can be gained via independent searches by individuals seeking information on deworming. Overall, the extent of awareness of the Inventory amongst NGOs conducting deworming remains unclear and would require further exploration to assess fully.

11
amounts of albendazole they had donated to other NGOs in Honduras (3 million and 63,000,
respectively), thereby double-counting 63,000 tablets. In this case, we are aware of the duplicate
accounting for the donated drugs received. However, given the complicated and inconsistent nature of
accounting for deworming drugs sent from larger organizations to smaller organizations, we cannot be
certain that duplication of reporting for donated tablets has not occurred elsewhere in the Inventory.
Without accounting for such duplicate reporting, the involvement of NGOs in deworming activities may
be over-estimated by the Inventory if counting of donated tablets is used as a proxy measure.
Unknown universe of NGOs involved in deworming
The Inventory is not a comprehensive listing of all treatments conducted by NGOs in a given year. The
sensitivity of the Inventory to detect NGO treatments has not been determined, but is certainly less than
100%. The activities of NGOs that did not respond to the Inventory or chose not to participate were not
captured, and NGOs that are conducting deworming but were unknown to CWW would naturally not be
included. Therefore, the Inventory cannot be relied upon as a comprehensive account of NGO
deworming activities, nor could it serve as a comprehensive “mop-up” tool for capturing all STH
treatments not reported directly to the WHO.
Recommendations
1. Strengthen reporting mechanisms for non-PELF STH treatments between Ministries of Health and the
WHO. The 2010 Inventory identified specific countries and regions where this reporting can be
strengthened.
2. Enhance reporting by NGOs to Ministries of Health at the country level. Robust reporting mechanisms
should be developed to provide country governments with full awareness of the treatments carried out
in-country by NGOs, which should then be incorporated into national non-PELF deworming treatment
reports for the WHO.
3. Reduce resources for any continuation of the Inventory. The 2010 Inventory project required
significant human resources (approximately 1,600 staff-hours in total for two CWW staff members and
approximately 60 hours for the PCT Databank administrator). Results from two consecutive years were
similar, suggesting no important trends. The overall contribution of unique treatments identified by the
inventory to the total reported to WHO was modest (9%). The response rate among NGOs and
participation by partners was low. Further, data from the 2010 Inventory provide insight on where the
reporting gap is greatest and how to address it. Continuation of the Inventory as the same level of effort
does not appear to be warranted.

12
Table 1. Data elements included in Global NGO Deworming Inventory treatment reporting form.
Information requested in 2010 and 2009 Inventory forms
• Organization name and contact information; • Target countries/districts; • Target populations per district (age-disaggregated); • Number of treatment rounds per year; • Number people treated per district at last treatment round (age-disaggregated); • Drugs used for treatment (albendazole, mebendazole, other).
New information requested in 2010 Inventory form
Implementing partners;
Age-disaggregated population of targeted districts;
STH prevalence of targeted districts;
Number of individuals targeted for deworming treatments, disaggregated by age
(children under five years of age, and children between the ages of five and 15);
Number of adults (>15 years) treated;
Number of deworming drugs provided for targeted districts and drug source.
Information requested in 2009 Inventory form removed from 2010 form
• Disease(s) targeted (STH, lymphatic filariasis, schistosomiasis.)
• Level of deworming in previous year and anticipated level for coming year.

13
Table 2. 2010 Global NGO Deworming Inventory response figures
Characteristic No. (%) organizations
Organizations surveyed 120
Organizations responding 20 (16.6%)
Type of data submitted
Treatment only 14 (11.7%)
Donation only* 4 (3.3%)
Treatment and Donation* 2 (1.7%)
Year of response
2010 only 5 (4.2%)
2009 and 2010 15 (12.5%)
Also reported directly to WHO (pathway 3 in Figure 1) **
2 (1.7%)
*Donation data are not included in the analyses or results below. Only treatment figures reported to the Inventory
were incorporated into the analysis. See Figure 2 for more information on the inclusion pathway for data received
via the 2010 Inventory.
** No NGOs reported directly to WHO that also didn’t report to the Inventory

14
Table 3. Treatments reported to the 2010 Inventory, by drug or drug combination
Drug(s) Used Preschool-Age Children School-Age Children # of NGOs reporting treatments All treatments
reported to Inventory (% of total)
No. (%) unique treatments
All treatments reported to Inventory (% of total)
No. (%) unique treatments
Albendazole (ALB) alone
2,705,130 (15%)
297,362 (11%) 5,780,075 (10%)
2,566,550 (44.9%)
10 (63%)*
Mebendazole (MEB) alone
15,750,467 (85%)
6,940,870 (43.8%)
41,136,950 (71%)
13,516,029 (32.8%)
8 (50%)*
Praziquantel (PZQ)
0 0 3,588,744 (6%) 0 2 (13%)
Ivermectin (IVM) + ALB
0 0 3,354,559 (5.8%)
0 1 (6%)
IVM or DEC + ALB
0 0 955,952 (1.6%) 0 1 (6%)
PZQ + ALB 0 0 2,023,437 (3.5%)
0 1 (6%)
PZQ + MEB 0 0 1,030,182 (1.7%)
0 2 (13%)
All treatments
18,455,597 7,238,232 (39%) 57,869,899 16,082,579 (28%)
16
* Some NGOs reported both albendazole-only and mebendazole-only treatments.

15
Table 4. Proportion of Unique treatments reported to the Inventory, by region
Region Treatments Reported to WHO
No. (%) treatments uniquely reported to Inventory
Proportion of all unique treatments contributed by this region
Africa (AFR) 40,063,819 11,513,591 28.7% 49.4%
Americas (AMR) 5,911,186 2,673,372 45.2% 11.5%
Eastern Mediterranean (EMR)
1,164,245 0 0.0% 0.0%
Europe (EUR) 0 0 0 0
Southeast Asia (SEAR) 8,924,406 8,194,583 91.8% 35.1%
Western Pacific (WPR) 9,308,967 939,265 10.1% 4.0%
Total 65.4 million 23.3 million 35.6% 100%

16
Table 5. Unique PSAC and SAC treatments contributed to the Inventory, by Country
Country (Region) Unique PSAC Treatments
Unique SAC Treatments
Bangladesh (SEAR) 0 8,060,000 (50.1%)
Cote d'Ivoire (AFR) 0 1,181,600 (7.3%)
Dominican Republic* (AMR) 984 (<1%) 2,791 (<1%)
El Salvador (AMR) 210,820 (2.9%) 106,324 (<1%)
Ethiopia (AFR) 0 1,098,241 (6.8%)
Gambia (AFR) 39,163 (<1%) 226,320 (1.4%)
Guatemala (AMR) 238,909 (3.3%) 294,094 (1.8%)
Guinea (AFR) 429,557 (5.9%) 1,954,555 (12.2%)
Honduras (AMR) 0 1,155,502 (7.2%)
India (SEAR) 0 134,583 (<1%)
Madagascar* (AFR) 0 374,898 (2.3%)
Mali (AFR) 2,531 (<1%) 154,709 (1%)
Nicaragua* (AMR) 139,140 (1.9%) 140,360 (<1%)
Peru (AMR) 105,542 (1.5%) 278,906 (1.7%)
Philippines (WPR) 39,614 (<1%) 899,651 (5.6%)
Sao Tome (AFR) 3,459 (<1%) 20,045 (<1%)
Tanzania (AFR) 6,028,513 (83.3%) 0
All Countries 7,238,232 (100%) 16,082,579 (100%)
* Country Ministry of Health provided reports to WHO for number of SAC treated in 2010 with
albendazole or mebendazole only (non-PELF).

17
Table 6. Unique PSAC and SAC treatments contributed to the Inventory, by NGO
Reporting NGO Number (%) of PSAC unique treatments reported
Number (%) of SAC unique treatments reported
Change a Life International 85,558 (1.2%) 203,692 (1.3%)
Children Without Worms 0 8,060,000 (50.1%)
Deworm the World 474,710 (6.6%) 4,046,710 (25.2%)
Helen Keller International 6,028,513 (83.3%) 0
INMED Partnerships for Children 19,984 (<1%) 75,214 (<1%)
Operation Blessing International 588,869 (8.1%) 1,696,280 (10.5%)
Save the Children 984 (<1%) 1,101,032 (6.8%)
University of the Philippines 39,614 (<1%) 899,651 (5.6%)
All NGOs 7,238,232 16,082,579

18
Figure 1. Reporting Channels for STH Treatments Conducted by NGOs
1b 2b
3
1a 2a
3. NGOs
report to
WHO Ministries of Health Inventory
NGO
WHO PCT Databank
1b. Ministries of Health
include NGO treatments in
their reports to WHO
2b. CWW provides NGO treatment
reports in the Inventory to WHO
2a: NGOs report to the Inventory 1a: NGOs report to Ministries of Health

19
Figure 2. Inclusion pathway for data received via the 2010 Inventory
All Reports Received
Treatments for Lymphatic
Filariasis (Albendazole +
Ivermectin/DEC)
Treatments for
Schistosomiasis
(Praziquantel alone or with
Albendazole/Mebendazole)
Treatment Data Only
Treatments for Soil-Transmitted
Helminthiasis (Mebendazole or
Albendazole)
Excluded
Excluded
Excluded
Reports of drugs donated (no
treatment data)
20 NGOs provided reports
6 NGOs reported
82.2 mil tablets
3 NGOs reported
4.3 mil SAC treatments
0 PSAC treatments
16 NGOs reported 76.4 mil treatments
- 57.9 mil SAC treatments
- 18.5 mil PSAC treatments
3 NGOs reported
6.6 mil SAC treatments
0 PSAC treatments
14 NGOs reported 65.4 mil treatments
- 46.9 mil SAC treatments
- 18.5 mil PSAC treatments

20
Figure 3. Regional distribution of countries reporting STH treatments (including pre-school-age children,
school-age children, and adults) to 2010 Inventory
20
10
2
3
3
Regional Distribution of Countries for which Treatments for STH with Albendazole or
Mebendazole (all ages) were Reported to 2010 Inventory Africa (AFR)
Americas (AMR)
Eastern Mediterranean(EMR)
Southeast Asia (SEAR)
Western Pacific (WPR)

21
Figure 4. Treatments by region of pre-school-age and school-age children with albendazole only or
mebendazole only captured by the 2010 Inventory
Africa(AFR)
Americas(AMR)
EasternMediterra
nean(EMR)
SoutheastAsia (SEAR)
WesternPacific(WPR)
Unique 11,513,591 2,673,372 0 8,194,583 939,265
Not unique 28,550,228 3,237,814 1,164,245 729,823 8,369,702
0
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
30,000,000
35,000,000
40,000,000
45,000,000
Number of Treatments of Pre-
School-age and School-age Children
Reported to the 2010 Inventory
Treatments of Pre-School-age and School-Age Children Treatments with Albendazole or
Mebendazole Captured by the 2010 Inventory

22
Figure 5. Treatments by region of school-age children with albendazole only or mebendazole only
captured by the 2010 Inventory
Africa(AFR)
Americas(AMR)
EasternMediterra
nean(EMR)
SoutheastAsia (SEAR)
WesternPacific(WPR)
Unique 5,010,368 1,977,977 0 8,194,583 899,651
Not unique 19,607,675 2,737,311 1,164,245 712,569 6,612,646
0
5,000,000
10,000,000
15,000,000
20,000,000
25,000,000
30,000,000
Number of Treatments of
School-age Children Reported to 2010
Inventory
Treatments of School-age Children (SAC) for STH with Albendazole or Mebendazole Captured by the 2010
Inventory

23
Figure 6. Treatments by region of pre-school-age children with albendazole only or mebendazole only
captured by the 2010 Inventory
Africa(AFR)
Americas(AMR)
EasternMediterra
nean(EMR)
SoutheastAsia (SEAR)
WesternPacific(WPR)
Unique 6,503,223 695,395 0 0 39,614
Not unique 8,942,553 500,503 0 17,254 1,757,056
0
2,000,000
4,000,000
6,000,000
8,000,000
10,000,000
12,000,000
14,000,000
16,000,000
18,000,000
Number of Treatments of Pre-
School-age Children Reported to the 2010 Inventory
Treatments of Pre-School-Age Children (PSAC) for STH with Albendazole or Mebendazole Captured
by the 2010 Inventory