Embed Size (px)
Citation preview

www.mjms.usm.my © Penerbit Universiti Sains Malaysia, 2011 For permission, please email:[email protected]
Abstract Foreignbodiesareacommonproblemseeninotolaryngologicalpractice.Ofthereportedforeignbodies,metallic foreignbodiesarea rareentity.Oneof the least commoncomplicationsofforeignbodyingestionispenetrationandmigration.Wedescribeacaseofamigratingmetallicforeignbodyina50-year-oldwomanwithahistoryofaccidentalingestioncausingodynophagia.Inthepresentcase,theforeignbodymigratedextraluminallyintothecarotidsheath.Ourreviewofliteraturerevealedthatfewsuchcaseshavebeenreported.
Keywords:: foreign bodies, foreign-body migration, medical imaging, metals, neck, otolyngology; head neck
Introduction
Ingestedforeignbodies(FBs)areacommonproblem encountered in otolaryngologicalpractice(1).However,onlyasmallnumberofFBsperforatethewalloftheaero-digestivetract,andan even smaller fractionmigrate extraluminally(2). Although a migrating foreign body mayremainquiescent,theymaycauselife-threateningsuppurative or vascular complications; hence,location and removal is essential. Removal ofembedded FBs can be quite challenging andfrustrating because location of the FB is oftenquitedifficult. We present a case report of a migratingmetallicforeignbodythatwasfoundtobepresentlateraltothecarotidsheath,witharelevantreviewoftheliterature.
Case Report
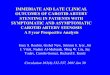
A 50-year-old female presented to theOtolaryngologyOutpatientDepartment,StJohn’sMedical College and Hospital (a tertiary carecentreinBangalore,SouthIndia)withcomplaintsof a pricking sensation inher throat for 4days.Shehadbeenexaminedatadistricthospital,andserial radiographs were taken, which showed aforeign body in the right retropharyngeal area.Thepatientwasreferredtoourcentreforfurthermanagement.An initial radiograph taken at thetimeofadmissionconfirmedthepresenceoftheforeign body in the right retropharyngeal area(Figure1). A rigid Hopkins endoscopy showedcongestionintheregionofthevallecula,withno
foreignbody(FB),castingdoubtonextraluminalmigration. Computed tomography (CT) of theneck with contrast showed the presence of aforeignbody in the right lateralpharyngealwall(Figure2). A careful search was made for theforeign body under general anaesthesia withintraoperativeradiographicaid.TheFBcouldnot
Case Report Metallic Foreign Body Penetrating the Carotid Sheath: A Case Report
Hemanth Vamanshankar, Arun B nair, Nandakumar rajan
Department of Otolaryngology and Head and Neck Surgery, St Johns Medical College and Hospital, Bangalore, 560034, India
Submitted: 6Jul2010Accepted: 27Aug2010
Figure1:Foreignbodyvisualisedonaradiographatthetimeofadmission.
72Malaysian J Med Sci. Jan-Mar 2011; 18(1): 72-75

Case Report |Metallicforeignbodypenetratingthecarotidsheath
www.mjms.usm.my 73
Figure 2: Computed tomography imageshowing the foreign body in thelateralpharyngealwall.
belocated;thus,anopenlateralcervicalapproachwas used. Two needles were placed below theskinintheneck,andintra-operativeradiographsweretakentolocatetheforeignbody(Figure3).An oblique incision was made from the hyoidbone to the thyroid cartilage, and the lateralpharyngeal wall was exposed. Another attemptwas made to visualise the foreign body usingdirect laryngoscope-assisted trans-illuminationfrom the oral cavity. This again proved to beunsuccessful. On further neck exploration, the foreignbody(ametallicwire)wasfoundtobeembeddedinthecarotidsheath(Figure4)andwasremoved(Figure5).Theneckwoundwasclosedinlayers,and a size 16 nasogastric tube was passed. Thepatient’spost-operativerecoverywasuneventful,exceptforthroatpain,whichpersistedfor2weekspost-operatively.
Discussion Impaction of foreign bodies in the upperaero-digestivetracthasbeenreportedsinceearlyhistory.Foreignbodiescanbelodgedinthetonsils,
thebaseofthetongue,pyriformthefossa,andthecervicaloesophagus.Onlyrarelydoforeignbodiespenetratethewalloftheaero-digestivetract,andeven more rarely do they migrate into the softtissueandvisceraofneck(3). Larger and sharper FBs get stuck in thepharynx or oesophagus, causing symptoms thatrequire their removal by oesophagoscopy. Inthe pharynx, FBs usually become lodged in thevallecula or lymphoid tissue, particularly thehypertrophiedtonsilortonguebase.ThoseFBsintheoesophaguscommonlyremainstuckbelowtheupperoesophagealsphincter.Foreignbodiesthataresharperandthosethataremorehorizontallyorientedhaveahigherchanceofpenetratingthewalloftheaero-digestivetract(4). The possible mechanisms for penetrationof foreign bodies include a combination ofoesophageal peristalsis and neckmovements orcarelessmanoeuvresusedwhentryingtoremoveit, for example, using fingers for balloons (4,5).Foreign bodiesmay also introduce bacteria intothesofttissueoftheneckandcausesuppurativecomplications such as parapharyngeal orretropharyngealabscess(2). A barium swallow is of limited value inlocating migrated foreign bodies but can beuseful in detecting oesophageal leaks (5). Themost commonly used tool for foreign bodyidentification is radiography of the soft tissuesoftheneck.However,imagesoftheforeignbodyand calcified cartilage of the upper airway mayoverlap, making location of the foreign bodydifficult. Thus, radiographs lack sensitivity indiagnosis (2,6). A CT scan of the neck utilising1-mmcuts is the investigativemethodofchoice.CT scans are invaluable in confirming the exactlocationoftheforeignbodyanditsrelationshiptothevitalstructuresintheneck. However, CT scans are not without theirdrawbacks. The soft tissues of the neck aremobile in relation to thebonyandcartilaginousstructures;thus,atthetimeofsurgery,theforeignbodymay not be situated exactly as where it isseenintheCT,asinourcase(1,5). Direct laryngoscopy may be done forconfirmation.Afindingofoedema, lacerationorulcerationondirectlaryngoscopyshouldraisethelevel of suspicion of a penetrating foreign body(2).Explorationandremovaloftheforeignbodyvia anexternal approach is recommended if theforeign body is confirmed to be extraluminal.Surgerymaybesupplementedwithintraoperativeradiography for accurate location of the foreignbody.However,due to theirpoor imagequality,intraoperativeradiographsarenotroutinelyused,

74 www.mjms.usm.my
Malaysian J Med Sci. Jan-Mar 2011; 18(1):72-75
buttheycomeinhandyasalastresortincasesinwhichtheforeignbodycannotbefoundafteranextensivesearch(2). Foreignbodyfixationtoorganwallsmayleadtoperioesophagitisorperipharyngitis,whichcanresultinanabscess.Perforationmayleadtofever,chestpain,subcutaneousemphysema,dyspnoea,and dysphagia. Migrating foreign bodies mayrupturelargevesselssuchasthecarotidoraorta,and foreign bodies can damage neighbouringorganssuchasthethyroidgland.Insomecases,the longdurationof symptomsmaybe theonlyhint of the presence of an intraluminal foreignbody(4).
Conclusion Ourcasehighlightstheneedforahighindexof suspicion todetectperforationandmigrationofaningestedforeignbodyintothesofttissuesoftheneck.Promptdiagnosis isneededtopreventthehighmorbidity thatcanoccur insuchcases.Themajorityof theupperaero-digestive foreignbodies are intraluminal and can be removed byendoscopy;therefore,itiscosteffectivetodoCTscansincasesofforeignbodiesthatcouldnotbelocatedandremovedendoscopicallyor inwhichthe symptoms have persisted for long duration.A systemic approach to neck exploration via an
Figure3:(a)Needlesplacedbelowtheskintohelplocatetheforeignbody.(b)Foreignbodywiththetwoneedlesseenonanintraoperativeradiograph.
Figure4:Foreignbodyfoundembeddedinthecarotidsheath.
Figure5:Foreignbodypost-removal.
a b

Case Report |Metallicforeignbodypenetratingthecarotidsheath
www.mjms.usm.my 75
externalapproach,withtheuseofintraoperativeradiography, will decrease the chances of anunsuccessfulexploration.
Authors’ Contributions
Conceptionanddesign:HVDraftingofthearticle:ABNFinalapprovalofthearticle:NR
Correspondence
DrArunBNairDLO(RajivGandhiUniversityofHealthSciences)DepartmentofOtolaryngologyStJohnsMedicalCollegeandHospitalBangalore560034IndiaTel:+918022065346Fax:+918025530070Email:[email protected]
References
1. ChungSM,KimHS,ParkEH.Migratingpharyngealforeign bodies: A series of four cases of saw-toothed fish bones. Eur Arch Otorhinolaryngol.2008;265(9):1125-1129.
2. Sreetharan SS, Prepageran N, Satwant S. Unusualmigratoryforeignbodyintheneck.Singapore Med J.2004;45(10):487-488.
3. Al-Sebeih K, Volvoda M, Sobeih A, Al-Sihan M.Perforating and migrating pharyngoesophagealforeignbodies:Aseriesof5patients.Ear Nose Throat J.2006Sep;85(9):600-603.
4. Mamede RC, Amaral F, Raimundo DG, FreitasLC, Ricz HM, Mello-Filho FV. Do foreign bodiesmigratethroughthebodytowardstheheart? Braz J Otorhinolaryngol.2009;75(2):195-199.
5. Lu PKS, Brett RH, Aw CY, Singh R. MigratingOesophageal Foreign Body—An Unusual Case.Singapore Med J.2000;41(2):77-79.
6. Masuda M, Honda T, Hayashida M, Samejima Y,YumotoE.Acaseofmigratoryfishboneinthethyroidgland.Auris Nasus Larynx.2006;33(1):113-116.