Embed Size (px)
Citation preview

Correspondence and communications 833
causes it to disappear on clinical exam over the ensuingweeks.
Conclusions
Fat necrosis is a minor, but bothersome and worrisomecomplication of autologous breast reconstruction. It hasclassically been managed by surgical excision or liposuc-tion, which can introduce new scars and cause contourdeformities. The great advantage of this new method ofneedle aeration is that the nodules soften so that theydon’t have to be surgically removed as in all the otherreported methods of treatment, thus maintaining anacceptable breast contour with a minimally invasive, safe,and effective technique.
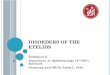
Figure 1 Nodular BCC of the lower eyelid. Lesion extendsmore laterally than is at first apparent
Acknowledgements
None.
Conflict of interest statement
The authors have no conflicts of interest.
References
1. Peeters WJ, Nanhekhan L, Van Ongeval C, et al. Fat necrosis indeep inferior epigastric perforator flaps: an ultrasound-basedreview of 202 cases. Plast Reconstr Surg 2009;124:1754e8.
2. Caterson SA, Tobias AM, Slavin SA, et al. Ultrasound-assistedliposuction as a treatment of fat necrosis after deep inferiorepigastric perforator flap breast reconstruction: a case report.Ann Plast Surg 2008;60:614e7.
Shareef JandaliLouis P. Bucky
Division of Plastic Surgery, University of PennsylvaniaHealth System, 3400 Spruce St., 10 Penn Tower,
Philadelphia, Pennsylvania PA 19104, USAE-mail address: [email protected]
ª 2010 British Association of Plastic, Reconstructive and AestheticSurgeons. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.bjps.2010.10.022
Reply to: Guidelines forreconstruction of the eyelids andcanthal regions. J Plast ReconstrAesthet Surg 2010;63(9):1420e1433
Sir,
DOI of original article: 10.1016/j.bjps.2009.05.035.
Mathijssen and van der Meulen must be congratulated onthe thoroughness of their literature review and the depthof their experience in periorbital reconstruction is beyondquestion.1 However, in one paragraph the authors statethat “Leaving a defect to heal through secondary intention(the so-called laissez faire technique) is never indicatedin the periorbital area, as contour deformity or contrac-ture was repeatedly encountered . This method onlyworks well for concave surfaces, such as the forehead orthe malar prominence.”
To say this technique is never indicated is overlydogmatic. In a recent paper, 2 four patients were describedin whom secondary intention healing most certainly wasindicated and, although unconventional, proved to be theideal treatment for their circumstances. A further case isdescribed below:
A 70 year old gentleman presented with a nodular basalcell carcinoma involving the margin of the lower eyelid(Figure 1).
Surgical excision was advised. The options of complexreconstruction or secondary intention healing werediscussed with the patient and the latter course wasdecided upon. The tumour was more extensive laterallythan first appeared, and also extended towards the inferior
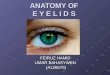
Figure 2 Immediate post-operative appearance
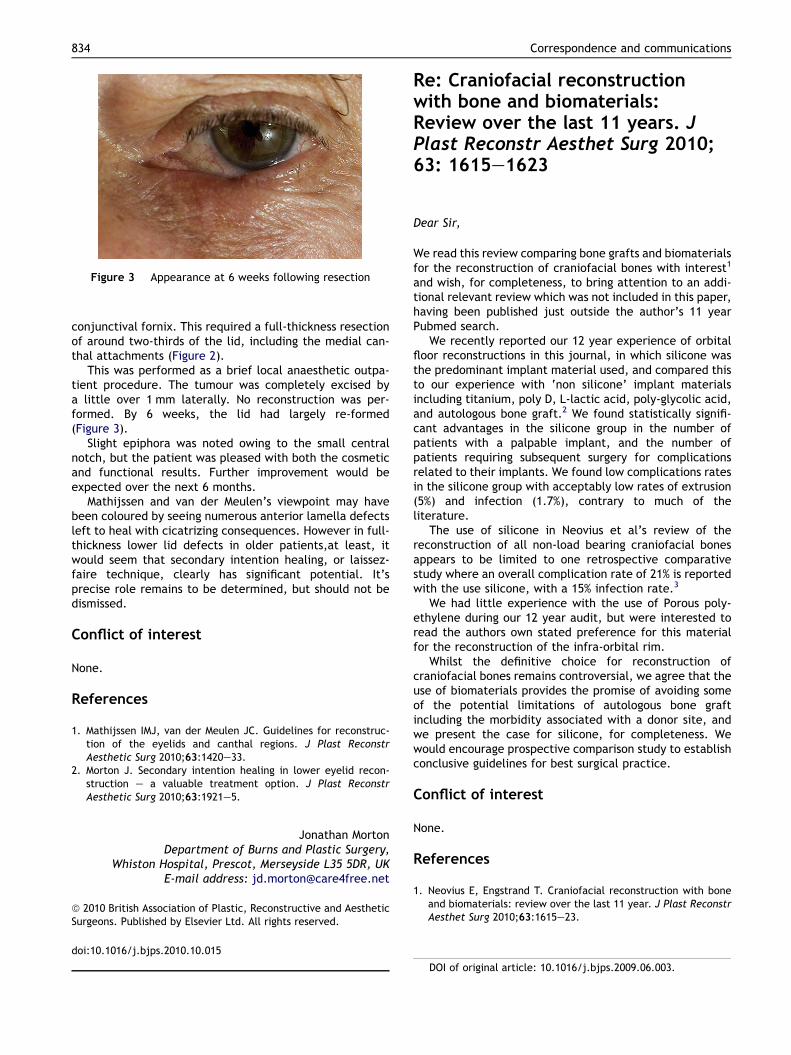
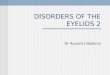
Figure 3 Appearance at 6 weeks following resection
DOI of original article: 10.1016/j.bjps.2009.06.003.
834 Correspondence and communications
conjunctival fornix. This required a full-thickness resectionof around two-thirds of the lid, including the medial can-thal attachments (Figure 2).
This was performed as a brief local anaesthetic outpa-tient procedure. The tumour was completely excised bya little over 1 mm laterally. No reconstruction was per-formed. By 6 weeks, the lid had largely re-formed(Figure 3).
Slight epiphora was noted owing to the small centralnotch, but the patient was pleased with both the cosmeticand functional results. Further improvement would beexpected over the next 6 months.
Mathijssen and van der Meulen’s viewpoint may havebeen coloured by seeing numerous anterior lamella defectsleft to heal with cicatrizing consequences. However in full-thickness lower lid defects in older patients,at least, itwould seem that secondary intention healing, or laissez-faire technique, clearly has significant potential. It’sprecise role remains to be determined, but should not bedismissed.
Conflict of interest
None.
References
1. Mathijssen IMJ, van der Meulen JC. Guidelines for reconstruc-tion of the eyelids and canthal regions. J Plast ReconstrAesthetic Surg 2010;63:1420e33.
2. Morton J. Secondary intention healing in lower eyelid recon-struction e a valuable treatment option. J Plast ReconstrAesthetic Surg 2010;63:1921e5.
Jonathan MortonDepartment of Burns and Plastic Surgery,
Whiston Hospital, Prescot, Merseyside L35 5DR, UKE-mail address: [email protected]
ª 2010 British Association of Plastic, Reconstructive and AestheticSurgeons. Published by Elsevier Ltd. All rights reserved.
doi:10.1016/j.bjps.2010.10.015
Re: Craniofacial reconstructionwith bone and biomaterials:Review over the last 11 years. JPlast Reconstr Aesthet Surg 2010;63: 1615e1623
Dear Sir,
We read this review comparing bone grafts and biomaterialsfor the reconstruction of craniofacial bones with interest1
and wish, for completeness, to bring attention to an addi-tional relevant review which was not included in this paper,having been published just outside the author’s 11 yearPubmed search.
We recently reported our 12 year experience of orbitalfloor reconstructions in this journal, in which silicone wasthe predominant implant material used, and compared thisto our experience with ‘non silicone’ implant materialsincluding titanium, poly D, L-lactic acid, poly-glycolic acid,and autologous bone graft.2 We found statistically signifi-cant advantages in the silicone group in the number ofpatients with a palpable implant, and the number ofpatients requiring subsequent surgery for complicationsrelated to their implants. We found low complications ratesin the silicone group with acceptably low rates of extrusion(5%) and infection (1.7%), contrary to much of theliterature.
The use of silicone in Neovius et al’s review of thereconstruction of all non-load bearing craniofacial bonesappears to be limited to one retrospective comparativestudy where an overall complication rate of 21% is reportedwith the use silicone, with a 15% infection rate.3
We had little experience with the use of Porous poly-ethylene during our 12 year audit, but were interested toread the authors own stated preference for this materialfor the reconstruction of the infra-orbital rim.
Whilst the definitive choice for reconstruction ofcraniofacial bones remains controversial, we agree that theuse of biomaterials provides the promise of avoiding someof the potential limitations of autologous bone graftincluding the morbidity associated with a donor site, andwe present the case for silicone, for completeness. Wewould encourage prospective comparison study to establishconclusive guidelines for best surgical practice.
Conflict of interest
None.
References
1. Neovius E, Engstrand T. Craniofacial reconstruction with boneand biomaterials: review over the last 11 year. J Plast ReconstrAesthet Surg 2010;63:1615e23.