Embed Size (px)
Citation preview

Replacing animal experiments:choices, chances and challengesGill Langley,1* Tom Evans,2 Stephen T. Holgate,3 and Anthony Jones4
SummaryReplacing animal procedures with methods such as cellsand tissues in vitro, volunteer studies, physicochemicaltechniques and computer modelling, is driven by legisla-tive, scientific and moral imperatives. Non-animal ap-proaches are now considered as advanced methods thatcan overcome many of the limitations of animal experi-ments. In testingmedicines andchemicals, in vitro assayshave spared hundreds of thousands of animals. Incontrast, academic animal use continues to rise and theconcept of replacement seems less well accepted inuniversity research. Even so, some animal procedureshave been replaced in neurological, reproductive anddentistry research and progress is being made in fieldssuch as respiratory illnesses, pain and sepsis. Systematicreviews of the transferability of animal data to the clinicalsetting may encourage a fresh look for novel non-animalmethods and, as mainstream funding becomes available,more advances in replacement are expected. BioEssays29:918–926, 2007.� 2007 Wiley Periodicals, Inc.
Introduction
Public disquiet about animal experiments has a long history
and has intensified in the last two decades. Concern focuses
primarily on the suffering caused to sentient animals, both
during experiments and by the nature of confinement in a
laboratory setting. Critics also point out that the validity of
animal experiments is often assumed rather than proven(1)
and that they are very demanding in costs and time. Animal
research policies that command both public and scientific
support remain elusive and a 30-year downward trend in
numbers of experiments is reversing.
A key emerging solution is the development of novel or
adapted research and testing methods that not only avoid
animal use, but can replace animal experiments. As part of the
internationally accepted Three Rs concept (replace, reduce
and refine animal experiments), the development of replace-
ment techniques is neither new nor untried: since 1986,
national(2) and European(3) legislation has required that
equivalent non-animal techniques must be used in place of
experiments on animals. In the USA, a similar imperative
operates at the institutional level. In the European Union,
the Commission and Member States have a further legislative
duty to encourage research into methods that could achieve
equivalent research objectives, but using fewer animals or
none at all. For this reason, the European Centre for the
Validation of Alternative Methods (ECVAM) was created in
1991, and has successfully validated more than 18 full or
partial replacement methods, eight of which have already
gained regulatory acceptance.
To promote the Three Rs, in 2004 the British government
established the National Centre for the Replacement, Reduc-
tion and Refinement of Animals in Research, whose ultimate
aim is the replacement of all animal experiments. There are
similar centres in Germany, Austria, the Netherlands, Japan
and elsewhere. There is a growing acceptance that non-
animal research methods are advanced techniques, having
potential to improve scientific andmedical progresswith fewer
demands on time and finance. As the British government has
said, ‘‘. . .alternative methods are often, in reality, ‘advanced
methods’ broadening the scope and overcoming some of the
limitations of existing animal models.’’(4)
This review discusses the origins and applications of some
successful replacementmethods already used in fundamental
medical research and in regulatory testing, and looks to three
fields of research (sepsis, respiratory disease and pain) for
chances to further replace animal experiments and to the
future for upcoming developments.
Replacing animal procedures—significant
successes
Replacing animal procedures is a well-established concept in
industry, especially in the pharmaceutical, chemical and
1Dr Hadwen Trust for Humane Research, Hitchin, Hertfordshire, UK.2Division of Immunology, Infection and Inflammation, University of
Glasgow, UK.3Infection, Inflammation and Repair Division, School of Medicine,
University of Southampton, Hampshire, UK.4Human Pain Research Group, Manchester University, Rheumatic
Diseases Centre, Clinical Sciences Building, Hope Hospital, Salford,
UK.
Tom Evans is in receipt of a Grant from the Dr Hadwen Trust.
*Correspondence to: Gill Langley, Dr Hadwen Trust, 84A Tilehouse
Street, Hitchin, Herts. SG5 2DY, UK.
E-mail: [email protected]
DOI 10.1002/bies.20628
Published online in Wiley InterScience (www.interscience.wiley.com).
918 BioEssays 29.9 BioEssays 29:918–926, � 2007 Wiley Periodicals, Inc.
Abbreviations: ECVAM, European Centre for the Validation of
Alternative Methods; Three Rs, the replacement, reduction and
refinement of animal procedures; FE, finite element; TMS, transcranial
magnetic stimulation; PET, positron emission tomography; COPD,
chronic obstructive pulmonary disease.
Challenges

cosmetics sectors, but seems less well known in academia.
Animal experiments conducted by industry in Britain have
fallen significantly over several years, but those carried out by
universities and medical schools have risen by 52% in the last
decade.(5) The following successful examples of replacement
havebeenselected frommany, to illustrate different routes and
reasons for the development and implementation of replace-
ment methods.
Regulatory testing of medicines and chemicalsSafety or quality testing of medicines or chemicals are areas
where the replacement of animal-based methods has wide
currency, both in industry and the regulatory authorities.
In the regulatory arena, new tests are validated by an
internationally agreed, formal process.(6) Several replacement
techniques have been successfully validated and approved.
Since 2000, three in vitro or synthetic methods have gained
regulatory acceptance for testing chemical corrosivity: the rat
skin assay and human skin model assay and the Corrositex
model(7) have replaced severe in vivo tests on rabbits. The cell-
based neutral red uptake assay for photo-irritancy is accepted
internationally, avoiding tests on mice.(8) Data from the in vitro
method of assessing skin penetration of drugs, pesticides and
chemicals are accepted worldwide, replacingmany studies on
rodents. In 2007, ECVAM endorsed two in vitro tests using
human skin models as replacements for in vivo skin irritation
tests on rabbits.
Other techniques have beenvalidated scientifically and are
in the regulatory pipeline, such as new in vitro pyrogenicity
assays. Parenteral medicines must be tested for pyrogens to
exclude the possibility of bacterial contamination. The original
in vivo test, introduced in the 1940s, measures fever response
by a rectal probe in rabbits restrained in stocks. Some animals
may suffer fever, respiratory problems, organ failure or fatal
shock. The test’s detection limit is above the human fever
threshold; it is time-consuming and costly, and unsuitable for
important new therapeutic areas such as cellular products.(9)
A secondmethod, conducted ex vivo on blood samples from
horseshoe crabs (Limulus polyphemus), was first developed in
the 1970s. Although its range is limited, between 1988 and
1998, the Limulus assay led to a decrease from 78,000 to 9,500
in the annual number of rabbit tests carried out in Britain.
An understanding of the mechanisms of the human fever
reaction, together with advances in cell biology techniques,
prompted the development of new in vitro pyrogenicity tests
usinghumanbloodcells.Basedon theactivation ofmonocytes
in response to pyrogens, the new assays, now fully validated
by ECVAM, avoid problems of species-specificity and are
more sensitive, more accurate, quicker and more cost-
effective.(10) They detect a wider range of pyrogens than the
Limulus test, and are being adapted for use with medical
devices and for environmental air pollutants; yet few people
believed earlier that a complex function such as fever could be
transferred to the ‘test tube’. The European Commission
estimates that more than 200 laboratories worldwide are
already implementing the in vitro methods, which will replace
some 200,000 rabbit tests a year in Europe alone.
In the manufacture and quality control of vaccines and
biological medicines, hundreds of thousands of animals
worldwide have been spared by the introduction of cell-based
methods. Historical cases enable a clearer analysis of causes
and outcomes, from a longer-term perspective. Examples
include testing for residual toxicity of diphtheria vaccine(11) and
potency testing of yellow fever vaccine. The original potency
test for yellow fever vaccine, comprising intracerebral inocu-
lation of immune serum and virus in mice, was introduced in
the 1950s. This lethal dose method was never fully stand-
ardised and had poor reproducibility, attributed to varying
sensitivities to the virus inmice of different ages, to differences
in the route of virus introduction, and to the type of animal
serumused.(12) In the late 1970s, a cell culture assaybasedon
plaque formation to detect neutralising antibodies was found
to be more practical, sensitive and reproducible,(13) finally
replacing an estimated 1,500 mice each year.
Physicochemical techniques, such as colorimetric assays
and high-performance liquid chromatography, have been
introduced as quality control tests for biological medicines.
Digitalis used to be routinely tested for potency on pigeons and
guinea pigs, by a lethal method involving intravenous injection.
In the late 1980s, this was replaced by a chemical colorimetric
assay which directly measured the content of digitoxin.
Similarly, the mouse convulsion method, by which every batch
of insulin was originally tested on 600 mice per sample, was
first refined and eventually replaced by high-performance
liquid chromatography. This was introduced as amore precise
technique(14) and accepted as a replacement by the British
Pharmacopoeia in 1990.(15) Chromatographic assays also
replaced animal bioassays for growth hormone, oxytocin and
lypressin.
In most examples pre-dating the late 1980s, the develop-
ment of non-animal assays was driven by dissatisfaction with
existing animal tests and the need for improved precision,
range or reproducibility.(12–14) The replacement techniques
werealso less costlyandproduced faster results. In the caseof
cosmetics and chemicals, high-profile consumer campaigns
have driven the pace and European directives have now
mandated or facilitated the replacement of animal-based
methods.(16,17) In the last decade or so, as the Three Rs
concept has gained widespread currency, a concern to spare
animals from suffering has become an increasingly powerful
driver for additional efforts to replace them.(18)
Computer simulations in medical research:fetoplacental physiology and orthodonticsAnimal models of human fetoplacental physiology are of
limited value, due to the species specificity of features such as
Challenges
BioEssays 29.9 919

(1) placental structure, permeability and blood flows, (2)
responses to hypoxia, (3) amniotic vascularisation, and (4)
amniotic fluid composition and dynamics.(19,20) This is
particularly so in the case of twin–twin transfusion syn-
drome,(21) a serious condition in which identical twins receive
unequal vascular supplies in the uterus.
The limitations of animal studies prompted the develop-
ment of computer models, based originally on clinical
measurements of fetal growth rates, phenotypic features
and weight discordance, obtained using ultrasound. Colour or
power Doppler imaging of blood flows and vascular anasto-
moses in pregnant women provided further data, as did in vitro
and ex vivo human organ and tissue studies, such as placental
dye injection and microscopy.
The first models addressed the causes of pregnancy-
induced hypertension and pre-eclampsia. By 1995 they had
successfully explained the mechanism underlying the diagnos-
tic ‘notch’ in uterine artery blood flow in women at risk of pre-
eclampsia.(22) In pinpointing the cause as an abnormality in
artery wall elasticity, the computer simulations overturned the
previous hypothesis. Mathematical modelling also demon-
strated howan imbalance in someanastomoses in the placenta
leads to twin–twin transfusion syndrome,(23) revealing the links
between fetofetal transfusion and amniotic fluid imbalance, the
hallmark of the syndrome. This finding led to a test to predict
women’s susceptibility and provided a rationale for classifying
severity so that optimal treatments could be selected.(24)
The models continue to improve and provide important
insights into the physiology of human pregnancy. They now
incorporate features such as imbalances in chorionic vascu-
lature,(25) fetal fluid dynamics, fetoplacental growth and
circulatory alterations, fetal heart failure and aspects of the
rennin–angiotensin system.(26) These developments are
expected to clarify the progression of conditions such as
twin–twin transfusion syndrome, and help determine the
efficacy of current and potential therapies.
Finite element (FE) analysis is a technique borrowed from
engineering. It is a theoretical approach in which a structure is
mathematically modelled by subdividing it into a mesh of
elements, bounded by sets of nodes. Computational proce-
dures are used to determine effects such as strains and
stresses caused byapplied loads. These are thenvisualised to
identify their magnitude and precise locations in the structure.
Since 1973, when it was introduced into dental biomechanical
research, FE analysis has been very widely applied in studies
of dental materials, oral and maxillofacial surgery, orthodon-
tics, dental restorations and more.(27) It is used to predict,
quantitatively and in three dimensions, the stresses and
strains imposed on tissues of the teeth and jaws, to help
assess the safety and efficacy of dental treatments and
appliances (see Fig. 1).
Based on the known structural properties of human tooth,
bone and ligament, and of dental materials such as ceramic
and titanium, FE analysis allows simulations of the outcomes
of corrective treatments, in terms of fracture properties,
stresses and strains at junctions, bond strengths, influences
of thermal or mechanical loads and failure problems.
A recent example is a FE-based computer model of a
titanium screw developed for implantation into the jawbone as
an anchor for applying orthodontic pressure.(28) A simulation
of the screwand surrounding bone predicted the displacement
causedwhen corrective pressurewas applied to the implanted
screw. Themodel showed the highest stresseswould be at the
neck of the screw, and in the bone at the level of the first screw
thread. The results suggested that the screw would provide
adequate anchorage, and helped to inform clinical decisions
about the best use of the implant.
Some animal experiments conducted in dentistry research
are invasive, long term and cause significant suffering.(29)
However, morphological and biomechanical dissimilarities
between species mean that animal studies may provide only
a ‘‘crude indication of the likely biomechanical consequences
in patients’’.(30) Ideally, FE models should be informed by and
validated using human data.(31)
Simulations can generate important insights: for example,
FE modelling of a human tooth and ligament under load,
validated using data from a human volunteer study, revealed
that the periodontal ligament was the location of the largest
strains. This suggested that initial tooth displacement is
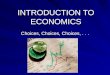
Figure 1. Finite element-based three-dimensional simula-
tion of bone adaptation around a screwthread implant. The
colour scale represents predicted variations in bone density in
response to the implant. Density is directly related to bone
strength and, after implant insertion, evolves by a damage/
repair process that continues until a mechanobiological
equilibrium is reached. Computer simulations can give deep
insight into the complex feedback mechanisms and various
parameters involved, predicting the rate of osseointegration
and hence durability of the implant, over more than 80 days.
With permission from Georges Limbert and John Middleton.
Challenges
920 BioEssays 29.9

mediatedvia the ligament rather than bycellular remodelling in
the bone.(32)
The widespread use of FE simulations in dentistry has
replacedsomeanimal experiments, particularly in researching
novel orthodontic appliances and materials, and in cases
where competing hypotheses would otherwise have been
explored using animal models.
Transcranial magnetic stimulation in functionalbrain researchTranscranial magnetic stimulation (TMS) is a technique used
in functional brain research which, applied to human volun-
teers, is widely accepted as a replacement for some invasive
experiments on non-human primates.(33) Using a coil, TMS
applies to the head amagnetic field which, by inducing random
neural activity, transientlyandsafelydisrupts a targetedareaof
the brain. This creates a ‘virtual lesion’ and during the tens of
milliseconds (or more) of disruption, volunteers perform
cognitive, visual or other tasks to determine the effect of the
‘lesion’ on their normal performance. The usual function of that
part of the brain can thus be inferred.
Magnetic stimulation of the human nervous system was
originally conceived in the mid-1980s(34) as a technique for
clinical assessment of central nervous function (especially
motor function), in patients with conditions such as multiple
sclerosis and demyelinating neuropathy. The conventional
method used painful electrical stimulation through the skin.
Magnetic stimulation, by contrast, was painless and suitable
both for clinical assessment and research.(35) The technique
was developed in human volunteers, by comparison of
magnetic versus electrical stimulation in the same individu-
als.(36) Experiments using dogs and primates were also
conducted(37) although not from a need to demonstrate safety
or to validate the technique, since these studies had already
been conducted with humans.
The research applications of TMS have since expanded
beyond motor function to include central visual and cognitive
processing aswell as cortical development and plasticity. As a
virtual lesioningmethod, it can demonstrate whether or not an
area of the human brain is actually necessary for a certain
function, rather than merely correlating neural activity with an
outcome, as is the case with functional magnetic resonance
imaging or positron emission tomography (PET) studies. TMS
combines good spatial and temporal resolutions, and has a
number of advantages in functional brain research.(38)
Compared to animal lesioning experiments, TMS is
superior in providing a chronology of activity in several brain
areas and the ability to use within-subject controls. It permits
analysis of a lesion effectwithout the complicationof functional
re-organisation, which occurs after brain lesioning in conven-
tional animal experiments. The spatial resolution of TMS does
not compare with cell-level experiments using electrodes in
animals. But in cognitive psychology research, for example,
with a systems-level focus, some experts believe that human
functional studies could provide virtually all the information
needed. This would replacemany experiments on non-human
primates.(38) Being safe and non-invasive, TMS has opened
the door to a wide range of human brain studies(39) without the
complications of species variations.(40)
Replacing animal procedures—further
opportunities
Three areas of medical research—sepsis, respiratory illness
and pain—have been selected to illustrate where significant
progress is being made in replacing animal experiments.
In each area, experiments may involve substantial animal
suffering, therapeutic breakthroughs are urgently needed;
and the validity of the animal models has been criticised.
Research into sepsisSepsis is a complex host response to severe infection.(41)
Despite considerable advances in intensive care treatment
and thedevelopment ofmoreeffectiveantibiotics, themortality
of this condition remains about 20–50%. An estimated 31,000
patients were admitted with sepsis to Intensive Care Units in
2004 in England,Wales andNorthern Ireland, of whom14,000
died before discharge, a mortality rate of 45%.(42) There is a
major need to developnew therapies targetedat this condition.
Animals have been used extensively to study the patho-
physiologyof sepsis, and asmodels for the disease to test new
therapies as they are developed.(43) Two major classes of
model have been developed. Compounds derived from
microbes, such as the bacterial component lipopolysacchar-
ide, canbe used tomimicmanyof the features of sepsis, and in
a high enough dose these are fatal. Alternatively, experimental
infections with live microbes are used to establish systemic
infection and the development of sepsis.
Both thesemodels producemajor physiological changes in
the animals used and can be rated substantially severe in
Britain by the Home Office, which regulates animal experi-
ments. Animal models have provided a large body of evidence
to establish the major pathophysiological mechanisms that
operate during sepsis, and as a springboard in the develop-
ment of new therapies. However, they are imperfect models.
There are important differences in the responses of different
animals, including humans, to sepsis. For example, rodents,
the most-utilised species in such work, are about 1,000-fold
more resistant to the toxic effects of lipopolysaccharide than
humans.(44) Additionally, there have been a number of high-
profile experimental treatments that have worked well in
animal models but failed in clinical trials.(45)
Given these ethical and scientific concerns, there is a need
to replace and refine animalmodels in the study of sepsis, both
to reduce animal suffering and to improve the predictive power
of models in developing new therapies for human sepsis. The
complex nature of sepsis represents a real challenge to
Challenges
BioEssays 29.9 921

develop alternatives to animal experimentation that will
provide meaningful biological information. However, given
the lack of success of animal models of sepsis in predicting
outcome in humans(45) there is a real need to develop better
models to predict this. There are a number of approaches that
hold promise for the future.
The in vitro tools of molecular and cellular biology will still
providemuch important information in the future. The ability to
manipulate such systems in a controlled fashion allows firm
inferences to be drawn and new hypotheses tested. Newer
methods of cell culture using three-dimensional supports hold
promiseas better models of tissue function (seeFig. 2),(46) and
advances in stem cell biology may well allow quite complex
tissues to be constructed entirely in vitro. Similarly, progress
being made in computer modelling of sepsis may also allow
modelling of septic processes without the use of animals.(47)
The last 50 years have seen a considerable decline in the
field of clinical experimentationwith human subjects. Although
the growth of much greater control over human studies is to
be welcomed, it seems this has led to a decline in such
approaches, both in living patients and in material removed
for subsequent in vitro analysis. Both these approaches can
shed considerable light on the pathophysiology of sepsis. For
example, studies investigating blood flow in human volunteers
have investigated the mechanisms underlying venodilatation
following cytokine administration, shedding light on the role of
nitric oxide in living humans.(48)
An important study used biopsies from children with
meningococcal sepsis to study the role of the anticoagulant
proteinC in sepsis.(49) The finding that endothelial activation of
protein C was impaired in this setting helped underpin the
development of activated protein C as a therapy of sepsis with
some demonstrable benefit. This is a concrete example where
data derived directly from human studies have aided in the
development of a useful therapy. Similarly, muscle biopsies
taken from septic patients demonstrated severemitochondrial
dysfunction, suggesting novel targets for therapeutic inter-
vention.(50) A greater use of human subjects and material in
sepsis research could contribute to the reduction of animal
experimentation, while providing mechanistic insights into this
serious medical problem.
Research into respiratory diseasesThemajority of diseases affecting the lung are environmental in
origin, whether produced by infectious, immunological or
toxicological mechanisms. The conducting airway and alveolar
epithelium, with the surface area of a tennis court, provides the
interface between the external environment and the internal
tissue milieu which, if disturbed, leads to tissue damage and
disease. The epithelium serves a barrier function both physi-
cally, by excluding environmental insults, and functionally
through the release of several bioactive molecules and a range
ofmetabolic activities to protect against or inactivate chemicals.
New therapeutic agents are needed for asthmaand chronic
obstructive pulmonary disease (COPD), but animal models
are limited because of structural and physiological differences
in the airways ofmice and humans.(51) These two diseases are
good examples of environmentally associated disorders that
reveal themselves through increased genetic susceptibility
and a range of environmental insults e.g. tobacco smoke,
allergens, chemicals and infectious agents.(52) In both
diseases, there are major changes in structure and function
of the epithelium. The epithelium also expresses many
candidate susceptibility genes for these diseases, identified
by positional cloning. For example, in asthma, a strong
association has been found with polymorphisms of several
genes that are preferentially expressed in the epithelium.(53)
Based on gene–environmental interactions, it has been
possible to reproduce some of the characteristics of asthma
and COPD using tissue engineering. Epithelial cells brushed
from the airways of volunteers at fibreoptic bronchoscopy can
be cultured to confluence in tissue culture over 2–3 weeks.
These provide a resource for investigating basal character-
istics as well as responses on exposure to pertinent stimuli,
e.g. air pollutants,(54) tobacco smoke,(55) viruses.(56,57) Epi-
thelium reconstituted in vitro from asthmatic patients exhibits
increased permeability due to reduced formation of tight
junctions, and increased susceptibility to oxidant pollutants. It
is also more susceptible to damage by common cold viruses
(due to reduced b- and l-interferon production).
In the case of COPD, epithelial cells at baseline and
following exposure to tobacco smoke extract also exhibit
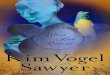
Figure 2. Renal tubule grown in vitro. Human primary renal
tubule epithelial cells were grown in a three-dimensional
collagen matrix in the presence of hepatocyte growth factor
to encourage tubulogenesis. The cells were fixed and stained
for the actin-associated protein ezrin (green), which is
concentrated in the brush border (arrowheads) facing a central
tubular lumen (L). Such three-dimensional cell cultures can be
used to study tissue damage in sepsis. Bar is 50 mm.
Challenges
922 BioEssays 29.9

markers of injuryand repair that occur invitro in theairwaycells
of patients, but not in those fromnormal volunteers. The profile
of protective oxidant genes expressed by epithelial cells from
COPD patients at baseline and when exposed to tobacco
smoke extract also map onto disease severity in vivo.(55) As in
asthma, epithelial cells cultured from COPD patients also
exhibit increased sensitivity to the damaging effects of
common cold viruses that might explain why such patients
are more vulnerable to virus-induced exacerbations. In both
conditions, the disease-related phenotypes persist in tissue
culture over several passages, suggesting that they are
primary rather than secondary abnormalities.(57)
Building upon the in vitro monolayer system, it has been
possible to produce a fully differentiated airway epithelium
by growing cells on inserts and, after they have formed
monolayers, bringing the cells up to the air/liquid interface.(58)
On removal of growth factors and addition of retinoic acid,
these cells differentiate after 3–4 weeks into a fully stratified
epithelium with functional ciliated and mucus-secreting goblet
cells. If grown in the presence of the pro-asthmatic cytokine IL-
13, a high proportion of the columnar cells transform into
goblet cells with evidence of active mucus secretion.(59)
Differentiated epithelial cells grown from asthmatic airways
behave differently from those of normal airways in their defi-
cient formation of tight junctions, accompanied by a parallel
reduction in transepithelial electrical resistance indicating a
more ‘leaky’ epithelium (STH, unpublished observations).
Since these cell culture systems maintain aspects of
disease phenotypes, they can be used to look for novel
molecular targets using genomic and proteomic platforms.
They can also be used as test systems for novel therapeutics
such as human recombinant b-interferon in restoring resist-
ance to the common cold virus.(56) Taken together, these
studies provide a solid basis of utilising airway epithelial
cultures from well-phenotyped patients, to discover novel
therapeutic targets and test new therapeutics for these
diseaseswhere there is an urgent need for greater innovation.
Computer simulations have also been used to explore
mechanisms of asthma pathology and predict the efficacy of
potential treatments, helping further to replace some animal
experiments.(60)
Research into painPain canonly be described andconfirmed inhumans in termsof
an integratedsensory, affectiveandmotivational experience.(61)
Although most pain is generated by activation of specialised
nerve endings (nociceptors), pain can also result from damage
to the nervous system or from psychological stress.
Functional brain imaging experiments in volunteers have
demonstrated a matrix of higher cortical centres implicated in
the complex cognitive integration that results in pain.(62,63)
Some of these higher centres, such as the cingulate cortex,
are poorly developed in many non-primates.
The assumption that discoveries can be easily transferred
from one species to another has to be challenged by a long list
of drugs that are effective at reducing nociceptive responses in
animals, but have failed as analgesics in clinical trials. The
challenge now is to determine how we can develop new and
safe analgesics more efficiently.
Animalmodels have provided uswith key information about
the detailed anatomical connections of nociceptive path-
ways(64,65) and potential physiological mechanisms of pain
perception.(66–68) However, the focus of studies in animals has
been on nociception within structures downstream of the
brain stem. Animal models of pain have been well reviewed
recently.(69) Generally, animal behaviour is observed, or
responses in the nervous system are recorded, whilst a
noxious stimulus is applied before and after some kind of
physiological intervention. The main problem with the inter-
pretation of animal models is that behavioural observations
are limited to motor responses and these cannot easily be
extrapolated to a change in pain experience. Animal pain
models can therefore only yield some possible clues to
potential mechanisms of pain in humans.
Pain is perceived as a result of integrated activity of well-
defined brain structures and there are two main systems: the
medial and lateral pain systems. Functional brain imaging
studies in humans have provided substantial information
about how these structures contribute to normal and abnormal
human pain perception in volunteers and patients (see
Fig. 3).(62,63) For instance, PETstudies that indirectly measure
synaptic activity in the brain have been used to establish that
the medial and lateral pain systems are mainly concerned
with emotional pain processing (e.g. unpleasantness), and
sensory-discriminative processing (e.g. pain localisation),
respectively.(70) Using a different PET technique that images
receptor binding on neurons, it has been possible to measure
changes in activity of natural pain-killers called endorphins,
in different types of chronic pain.(71,72) Complementary
approaches include post-mortem tissue analysis, which
provides a single ‘snapshot’ of chemical differences in
peripheral and central neurons (e.g. spinal cord), in relation
to sensory abnormalities in patients with pain due to nerve
damage.(73)
The challenge is to use these different types of information
to develop new therapies for painmore effectively.We suggest
some approaches to achieve this. First, there needs to be a
shift from anatomical-, disease- and time-based classification
of pain to a more physiological definition of clinical pain
syndromes, using physiological methods such as functional
brain imaging techniques. This can be achieved by careful
physiological and psychological measurement in patients with
different types of pain syndrome. For instance, we (AJ) have
recently identified an inability to alter the way that they attend
to pain in patientswith a type of widespread chronic pain called
fibromyalgia.(74)
Challenges
BioEssays 29.9 923

To achieve a more physiological approach to pain classi-
fication, it will be necessary to identify the normal physio-
logical(70,71) and pathophysiological mechanisms of pain
perception.(75,76) For example, PET studies have shown a
selective reduction in receptors for natural opiates in thebrains
of patients with severe pain due to stroke.(76) Such studies
require substantial investment and greater collaboration
between the pharmaceutical industry and academia.
Following identification ofmechanisms in humans, targeted
drug development should be narrowly based on modulation
of those mechanisms. Having identified and measured the
pathophysiological mechanisms, proof-of-concept trials will
be much more cost-effective. Preferably no drug should be
developed without establishing that it reaches the target organ
in humans, prior to clinical trials. In many cases, this can be
achieved using molecular imaging e.g. PET.
In summary, techniques exist to begin to reclassify human
pain physiologically and to identify candidate pathophysiolog-
ical mechanisms in volunteers. By working back from these
mechanisms to drug development, some animal experiments
maybe replaced. This is not beyond currentmolecular imaging
capacities but will require a sea-change in the way we think
about pain.
Where next?
The drive to replace animal procedures has historically involved
humaneand scientific aspects, and this is still so. Acceptance of
the capacityof animals toexperience pain anddistressprovides
a growing impetus for progress, most apparent in regulatory
testing where non-animal method development has been
embraced by toxicologists, legislators and regulators. Individual
scientists concerned about animal use have made a significant
impact in particular fields, such as vaccine testing.
Dissatisfaction with the quality of animal data remains a
powerful motivator for change, and the search for superior
alternatives is increasingly attracting government funds.
The European Commission now supports a programme of
research to replace animal-based toxicology, and promotes
this as a contribution to the quality of science and the safety of
consumers as well as preventing animal suffering.
In academia, with an emphasis more on fundamental
medical research, change has been slower. There are several
reasons: (1) open-ended research questions are perceived as
being more difficult to pursue without animal experiments, (2)
there are few avenues for consumer pressure to be exerted,
and (3) academic research is less shaped by legislative and
regulatory initiatives. However, recent systematic reviews of
the translation of animal research into clinical benefit may well
signal a change.
Several such reviews have demonstrated that animal
studies were poorly predictive of human outcomes. In
particular, discordances were found in animal and human
data for (1) corticosteroids in head injury, (2) anti-fibrinolytics in
bleeding, (3) tirilazad for stroke,(77) and (4) neuroprotective
drugs in stroke.(78) A systematic review of 76 highly cited
animal studies published in seven leading journals, found that
only 37% translated into successful human trials.(79) In these
articles and others, one of the key questions is whether the
animal models sufficiently mimic the human diseases.
Change is on itsway. Legislative developments, such as the
new chemical regulatory framework in the European Union,
and the revision of European legislation on animal experi-
ments, may force the pace. The perception that research to
replace animals is a niche field is gradually being overcome,
and ideally the replacement concept will become embedded
in mainstream journals. In the USA, the Interagency
Figure 3. Sections of brain areas at 4 mm and 6 mm demonstrating increased activation within the areas of the medial pain system in
patientswith arthritic pain (AP) condition (AP - EP), compared to the experimental pain (EP) condition (EP - AP). pACC, perigenual anterior
cingulate cortex; aMCC, anterior mid-cingulate cortex; PCC, posterior cingulate cortex; SGC, subgenual cingulate cortex.
Challenges
924 BioEssays 29.9

Coordinating Committee on the Validation of Alternative
Methods has just drafted a five-year plan to develop and
validate alternatives to animal experiments; and Japan
established a centre for alternative methods in 2005. Major
funders such as the Wellcome Trust are taking their first
tentative steps to support this research. Influential organisa-
tions such as the Royal Society(80) and the Nuffield Council on
Bioethics(81) increasingly acknowledge, in their publications,
the limitations of animal data in medical research.
Replacing animal experiments is a cultural challenge
requiring flexibility and openness to new ideas, and a scientific
challenge needing a fresh, cross-disciplinary approach. The
research needed also has potential to boost science, improve
medical progress and better protect the safety of patients and
consumers.
Acknowledgments
We are very grateful for assistance from Nevil Chimon and
Alison Watson, and to Georges Limbert and John Middleton
for permission to reproduce Figure 1.
References1. Animal Procedures Committee. 2003. Review of Cost-Benefit Assess-
ment in the Use of Animals in Research London: Home Office.
2. Anon. 1986. Animals (Scientific Procedures) Act 1986, Section 5 (5)
London: HMSO.
3. Council Directive 86/609/EEC of 24 November 1986 on the approxima-
tion of laws, regulations and administrative provisions of the Member
States regarding the protection of animals used for experimental and
other purposes. Official J Eur Comm L358:1–29.
4. The Government Reply to the Report of the House of Lords Select
Committee on Animals in Scientific Procedures, Session 2001–2002.
Presented to Parliament by the Secretary of State for the Home
Department, January 2003. Cm. 5729.
5. Home Office. 2006. Statistics of Scientific Procedures on Living Animals
Great Britain 2005. Cm. 6877 London: The Stationery Office.
6. OECD. 2005. Guidance document no. 34 on the validation and
international acceptance of new or updated test methods for hazard
assessment. OECD Series on Testing and Assessment. ENV/JM/MONO
(2005)14. Paris: OECD.
7. Commission Directive 2000/33/EC of 25 April 2000 adapting to technical
progress for the 27th time Council Directive 67/548/EEC on the
approximation of laws, regulations and administrative provisions relating
to the classification, packaging and labelling of dangerous substances.
Official J Eur Comm L136:90.
8. Guidance for Industry on Photosafety Testing. 2003. Food and Drug
Administration Center for Drug Evaluation and Research Maryland: FDA.
9. Dhruvakumar S, Stephens ML, Sandusky CB, Leary S. 2006. Public
Comments to the US NTP Interagency Center for the Evaluation of
Alternative Toxicological Methods (NICEATM), on the Peer Panel
Evaluation of in vitro Pyrogenicity Testing Methods http://iccvam.niehs.
nih.gov/methods/pyrodocs/pyrocomm.htm (accessed January 2007).
10. Hoffmann S, Peterbauer A, Schindler S, Fennrich S, Poole S, et al. 2005.
International validation of novel pyrogen tests based on human
monocytoid cells. J Immunol Methods 298:161–173.
11. Hendriksen CFM, Garthoff B, Aggerbeck H, Bruckner L, Castle P, et al.
1994. Alternatives to Animal Testing in the Quality Control of Immuno-
biologicals: Current Status and Future Prospects. ATLA 22:420–434.
12. World Health Organization. 1993. The Immunological Basis for Immuni-
zation Series, Module 8: Yellow Fever. WHO/EPI/GEN/93.18 Geneva:
WHO. p 2–3.
13. World Health Organization Expert Committee on Biological Stand-
ardization. 1979. Thirtieth Report, Technical Report Series. 638. Geneva:
WHO. p 19–20.
14. Anon. 1985. Reduction of the use of animals in the development and
control of biological products. Lancet 2:900–902.
15. British Pharmacopoeia 1988, Addendum. 1990. Insulin preparations
London: HMSO. p 1279–1280.
16. Directive 2003/15/EC of the European Parliament and of the Council of
27 February 2003 amending Council Directive 76/768/EEC on the
approximation of the laws of the Member States relating to cosmetic
products. Official J Eur Comm L66:26–35.
17. Regulation (EC) No 1907/2006 of the European Parliament and of the
Council of 18 December 2006 concerning the Registration, Evaluation,
Authorisation and Restriction of Chemicals (REACH), establishing a
European Chemicals Agency, amending Directive 1999/45/EC and
repealing Council Regulation (EEC) No. 793/93 and Commission
Regulation (EC) No. 1488/94 as well as Council Directive 76/769/EEC
and Commission Directives 91/155/EEC, 93/67/EEC, 93/105/EC and
2000/21/EC. Official J Eur Union L396:1–849.
18. Hendriksen CFM. 2002. Refinement, reduction and replacement of
animal use for regulatory testing: current best scientific practices
from the evaluation of safety and potency of biologicals. ILAR J 43
(suppl.):S43–S48.
19. Schroder HJ. 1995. Comparative aspects of placental exchange
functions. Eur J Obstet Gynecol Reprod Biol 63:81–90.
20. Albuquerque CA, Nijland MJ, Ross MG. 1999. Human and ovine
amniotic fluid composition differences: implications for fluid dynamics.
J Matern Fetal Med 8:123–129.
21. Umur A, van Gemert MJC, Ross MG. 2001. Amniotic fluid and
hemodynamic model in monochorionic twin pregnancies and twin-twin
transfusion syndrome. Am J Physiol Regulat Integr Comp Physiol
280:R1499–R1509.
22. Talbert DG. 1995. Uterine flow velocity waveform shape as an indicator
of maternal and placental development failure mechanisms: a model-
based synthesizing approach. Ultrasound Obstet Gynecol 6:261–271.
23. Talbert DG, Bajoria R, Sepulveda W, Bower S, Fisk NM. 1996.
Hydrostatic and osmotic pressure gradients produce manifestations of
fetofetal transfusion syndrome in a computerized model of monochorial
twin pregnancy. Am J Obstet Gynecol 174:598–608.
24. Tan TYT, Taylor MJO, Wee LY, Vanderheyden T, Wimalasundera R, et al.
2004. Doppler for artery-artery anastomosis and stage-independent
survival in twin-twin transfusion. Obstet Gynecol 103:1174–1180.
25. Denbow ML, Talbert D, Fisk NM. 2006. Determinants of flow along
arterio-arterial anastomoses in monochorionic placentae by dynamic
computer modelling of chorionic plate vasculature. Prenat Diagn
26:433–442.
26. van den Wijngaard JPHM, Umur A, Krediet RT, Ross MG, van Gemert
MJC. 2005. Modeling a hydropic recipient twin in twin-twin transfusion
syndrome. Am J Physiol Regul Integr Comp Physiol 288:R799–R814.
27. Mackerle J. 2004. Finite element modelling and simulations in dentistry: a
bibliography 1990–2003. Comp Methods Biomech Biomed Eng 7:277–
303.
28. Gallas MM, Abeleira MT, Fernandez JR, Burguera M. 2005. Three-
dimensional numerical simulation of dental implants as orthodontic
anchorage. Eur J Orthod 27:12–16.
29. Huja SS, Rao J, Struckhoff JA, Beck FM, Litsky AS. 2006. Biomechanical
and histomorphometric analyses of monocortical screws at placement
and 6 weeks postinsertion. J Oral Implantol 32:110–116.
30. Jones ML, Hickman J, Middleton J, Volp C. 2001. A validated finite
element method study of orthodontic tooth movement in the human
subject. J Orthod 28:29–38.
31. Cattaneo PM, Dalstra M, Melsen B. 2005. The finite element method: a
tool to study orthodontic tooth movement. J Dent Res 84:428–433.
32. Middleton J, Jones M, Wilson A. 1996. The role of the periodontal
ligament in bone modeling: the initial development of a time-dependent
finite element model. Am J Orthod Dentofacial Orthop 109:155–162.
33. Anon. 2006. Primates in Medical Research London: Medical Research
Council and Wellcome Trust. p 16.
34. Barker AT, Jalinous R, Freeston IL. 1985. Non-invasive magnetic
stimulation of the human motor cortex. Lancet 1:1106–1107.
Challenges
BioEssays 29.9 925

35. Hess CW, Mills KR, Murray NMF. 1986. Responses in small hand
muscles from magnetic stimulation of the human brain. J Physiol
388:397–419.
36. Schriefer TN, Mills KR, Murray NM, Hess CW. 1988. Evaluation of
proximal facial nerve conduction by transcranial magnetic stimulation. J
Neurol Neurosurg Psychiat 51:60–66.
37. Estrem SA, Haghighi S, Levy WJ, Wertheimer R, Kendall M. 1988. Motor-
evoked potentials of facial musculature in dogs. Laryngoscope 98:1012–
1015.
38. Langley G, Harding G, Hawkins P, Jones A, Newman C. et al. 2000.
Volunteer studies replacing animal experiments in brain research. ATLA
28:315–331.
39. Tunik E, Frey SH, Grafton ST. 2005. Virtual lesions of the anterior
intraparietal area disrupt goal-dependent on-line adjustments of grasp.
Nat Neurosci 8:505–511.
40. Orban GA, Claeys K, Nelissen K, Smans R, Sunaert S. et al. 2006.
Mapping the parietal cortex of human and non-human primates.
Neuropsychologia 44:2647–2667.
41. Cohen J. 2002. The immunopathogenesis of sepsis. Nature 420:885–
891.
42. Harrison DA, Welch CA, Eddleston JM. 2006. The epidemiology of
severe sepsis in England, Wales and Northern Ireland, 1996 to
2004: secondary analysis of a high quality clinical database, the
ICNARC Case Mix Programme. Database Crit Care 10:R42.
43. Marshall JC, Deitch E, Moldawer LL, Opal S, Redl H, et al. 2005.
Preclinical models of shock and sepsis: what can they tell us? Shock 24
(Suppl 1):1–6.
44. Galanos C, Freudenberg MA. 1993. Mechanisms of endotoxin shock and
endotoxin hypersensitivity. Immunobiol 187:346–356.
45. Zanotti S, Kumar A, Kumar A. 2002. Cytokine modulation in sepsis and
septic shock. Expert Opin Investig Drugs 11:1061–1075.
46. O’Brien LE, Zegers MM, Mostov KE. 2002. Opinion: Building epithelial
architecture: insights from three-dimensional culture models. Nat Rev
Mol Cell Biol 3:531–537.
47. Vodovotz Y, Chow CC, Bartels J, Lagoa C, Prince JM, et al. 2006. In
silico models of acute inflammation in animals. Shock 26:235–244.
48. Bhagat K, Hingorani AD, Palacios M, Charles IG, Vallance P. 1999.
Cytokine-induced venodilatation in humans in vivo: eNOS masquerading
as iNOS. Cardiovasc Res 41:754–764.
49. Faust SN, Levin M, Harrison OB, Goldin RD, Lockhart MS, et al. 2001.
Dysfunction of endothelial protein C activation in severe meningococcal
sepsis. New Engl J Med 345:408–416.
50. Brealey D, Brand M, Hargreaves I, Heales S, Land J, et al. 2002.
Association between mitochondrial dysfunction and severity and out-
come of septic shock. Lancet 360:219–223.
51. Mallia P, Johnston SL. 2005. Mechanisms and experimental models of
chronic obstructive pulmonary disease exacerbations. Proc Am Thorac
Soc 2:361–366.
52. Martinez FD. 2007. Gene-environment interactions in asthma: with
apologies to William of Ockham. Proc Am Thorac Soc 4:26–31.
53. Holgate ST. 2006. Susceptibility genes in severe asthma. Curr Allergy
Asthma Rep 6:345–348.
54. Bucchieri F, Puddicombe SM, Lordan JL, Richter A, Buchanan D, et al.
2002. Asthmatic bronchial epithelium is more susceptible to oxidant-
induced apoptosis. Am J Respir Cell Mol Biol 27:179–185.
55. Pierrou S, Broberg P, O’Donnell R, Pawlowski K, Virtala R, et al. 2006.
Expression of genes involved in oxidative stress responses in airway
epithelial cells of COPD smokers. Am J Respir Crit Care Med 175:577–
586.
56. Wark PA, Johnston SL, Bucchieri F, Powell R, Puddicombe S, et al. 2005.
Asthmatic bronchial epithelial cells have a deficient innate immune
response to infection with rhinovirus. J Exp Med 201:937–947.
57. Contoli M, Message SD, Laza-Stanca V, Edwards MR, Wark PA, et al.
2006. Role of deficient type III interferon-lambda production in asthma
exacerbations. Nat Med 12:1023–1026.
58. Vermeer PD, Panko L, Karp P, Lee JH, Zabner J. 2006. Differentiation of
human airway epithelia is dependent on erb B2. Am J Physiol Lung Cell
Mol Physiol 291:L175–L180.
59. Kondo M, Tamaoki J, Takeyama K, Nakata J, Nagai A. 2002. Interleukin-
13 induced goblet cell differentiation in primary cell culture from guinea
pig tracheal epithelium. Am J Respir Cell Mol Biol 27:536–541.
60. Lewis AK, Paterson T, Leong CC, Defranoux N, Holgate ST, et al. 2001.
The roles of cells and mediators in a computer model of chronic asthma.
Int Arch Allergy Immunol 124:282–286.
61. Melzack R, Casey KL. 1968. Sensory, motivational, and central control
determinants of pain. In Kenshalo DR editor The Skin Senses. Spring-
field: CC Thomas. p 423-439.
62. Jones AKP, Kulkarni B, Derbyshire SWG. 2003. Pain mechanisms and
their disorders. In Frackowiak R, Jones T, editors. Br Med Bull Oxford:
Oxford University Press. p 83–93.
63. Treede RD, Kenshalo DR, Gracely RH, Jones AKP. 1999. The cortical
representation of pain. Pain 79:105–111.
64. Apkarian AV, Hodge CJ. 1989. Primate spinothalamic pathways: III.
Thalamic terminations of the dorsolateral and ventral spinothalamic
pathways. J Comp Neurol 288:493–511.
65. Vogt BA, Rosene DL, Pandya DN. 1979. Thalamic and cortical afferents
differentiate anterior from posterior cingulate cortex in the monkey.
Science 204:205–207.
66. Le Bars D, Bouhassira D, Villanueva L. 1995. Opioids and diffuse
noxious inhibitory control (DNIC) in the rat. In Bromm B, Desmedt J,
editors. Pain and Brain: From Nociception to Cognition New York: Raven
Press Ltd. p 517–539.
67. Suzuki R, Morcuende S, Webber M, Hunt SP, Dickenson AH. 2002.
Superficial NK1-expressing neurons control spinal excitability through
activation of descending pathways. Nat Neurosci 5:1319–1326.
68. Woolf CJ. 1994. A new strategy for the treatment of inflammatory pain.
Prevention or elimination of central sensitization. Drugs 47 (Suppl 5):1–9.
69. Wang LX, Wang ZJ. 2003. Animal and cellular models of chronic pain.
Adv Drug Deliv Rev 55:949–965.
70. Kulkarni B, Bentley DE, Elliott R, Youell P, Watson A, et al. 2005. Attention
to pain localization and unpleasantness discriminates the functions of the
medial and lateral pain systems. Eur J Neurosci 21:3133–3142.
71. Jones AK, Kitchen ND, Watabe H, Cunningham VJ, Jones T, et al. 1999.
Measurement of changes in opioid receptor binding in vivo during
trigeminal neuralgic pain using [11C] diprenorphine and positron
emission tomography. J Cereb Blood Flow Metab 19:803–808.
72. Jones AKP, Cunningham VJ, Ha-Kawa S, Fujiwara T, Luthra SK, et al.
1994. Changes in central opioid receptor binding in relation to
inflammation and pain in patients with rheumatoid arthritis. Br J
Rheumatol 33:909–916.
73. Yiangou Y, Facer P, Durrenberger P, Chessell IP, Naylor A, et al. 2006.
COX-2, CB2 and P2X7-immunoreactivities are increased in activated
microglial cells/macrophages of multiple sclerosis and amyotrophic
lateral sclerosis spinal cord. BMC Neurol 6:12.
74. Kulkarni B, Boger E, Watson A, Elliott R, Bentley DE, et al. 2005.
Attentional dysfunction in fibromyalgia. Rheumatol 44:94.
75. Gracely RH, Geisser ME, Giesecke T, Grant MA, Petzke F, et al. 2004.
Pain catastrophizing and neural responses to pain among persons with
fibromyalgia. Brain 127:835–843.
76. Jones AKP, Watabe H, Cunningham VJ, Jones T. 2004. Cerebral
decreases in opioid receptor binding in patients with central neuropathic
pain measured by [11C]diprenorphine binding and PET. Eur J Pain
8:479–485.
77. Perel P, Roberts I, Sena E, Wheble P, Briscoe C, et al. 2006. Comparison
of treatment effects between animal experiments and clinical trials: a
systematic review. BMJ doi:10.1136/bmj.39048.407928.BE.
78. O’Collins VE, Macleod MR, Donnan GA, Horky LL, van der Worp BH,
et al. 2006. 1,026 experimental treatments in acute stroke. Ann Neurol
59:467–477.
79. Hackam DG, Redelmeier DA. 2006. Translation of research evidence
from animals to humans. JAMA 296:1731–1732.
80. Royal Society. 2006. Royal Society policy document 17/06. In Expert
Scientific Group on Phase One Clinical Trials, Interim Report Appendix
11.4, Stakeholder written submissions. p 333–334.
81. Nuffield Council on Bioethics. 2005. The Ethics of Research Involving
Animals London: Nuffield Council on Bioethics. p 180–181.
Challenges
926 BioEssays 29.9