Embed Size (px)
Citation preview

Patricia Patterson
Replacing a human heart
o the world, it was a medical landmark-the first permanent implantation of an artificial heart in T a human patient. Yet to the operating mom
nurses who participated, it was a natural part of working on the heart service at the University of Utah Hospital in Salt Lake City.
b n g before surgery waa scheduled on Dec 2 for
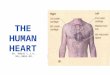
The operating room stan was prepared for the unprecedented procedure. (Wwm by Brad Nelson, UniverSdy d Utah Medicat center.)
AORN Journal, Febncrrry 1983. Vol37. No 2 183

During the implant operation, Diane Karsten, RN (right), was the circulating nurse and Gayle Baldwin, RN, scrubbed.
Barney Clark, DDS, two nurses knew they would be in the operating mom for this unprecedented case. Diane Karsten, RN, who circulated, had been working for three years with surgeon William C DeVries, MD. Scrub nurse Gayle Baldwin, RN, had been employed on the cardiovascular service ever since graduating from nursing school a year and a half previously.
Both nurses had been on a team that implanted mechanical hearts in two cadavers, and they had observed at least four or five procedures on animals dur- ing the year preceding the first human operation. The entire team had done its first dry run for an artificial heart more
Patrlcla Patterson is associate editor of the AORN Journal.
than a year before Dr Clark’s surgery. There were two more dry runs as they awaited the first patient.
For Colleen O’Connor, RN, operating mom supervisor, the dry runs were es- sential in anticipating the many details the procedure required. “Every piece of equipment, including the cameras, was in the mom and moved as it would be
184 AORN Journal, February 1983, Vol37, No 2

When the procedure was rescheduled for Wednesday evening, the OR nurses were ready. They knew what was needed, and setting up the room took them about one-half hour.
when the patient came in and when he left,” she said. “All personnel were in there and knew what was expected.
“We even had an orderly act as the patient and attached the artificial heart
to the outside of his chest. Then we hooked up the heart’s cords to the drive unit 50 we would know exactly how the cords would go. At the end, we moved him over to the intensive care unit
AORN Journal, February 1983, Vol37, No 2 185

(ICU) and put the equipment with him in the room.
“And that’s exactly the way it went during the real operation,” she added with satisfaction. The meticulous plan- ning and experience resulted in a smoothly run surgery.
Soon after Dr Clark had arrived at the hospital on Monday, Nov 29, from his home in Seattle, a six-member evalua- tion committee considered whether he was an appropriate candidate for the surgery. (See related article.) For the operation to go forward, they all would have to agree. They evaluated Dr Clark that night and met the next morning at a confidential session. The vote was unanimous in favor of the surgery. The operation was scheduled for Thursday, Dec 2, at 8 am.
The process for informing Dr Clark about his surgery was highly structured and carefully planned. He was required to read a long consent form, discuss the procedure thoroughly with Dr DeVries, and then to sign the form twice 24 hours apart.
But as Dr Clark slipped toward death Wednesday evening, Dr DeVries de- cided surgery could not wait until the next morning. The patient’s cardiac output was 1 L, and the physicians were concerned he might have a stroke or decline to the point where the heart im- plant would do no good.
His condition had been deteriorating rapidly ever since he had arrived in Salt Lake City. He was suffering from con- gestive heart failure due to cardio- myopathy. At 61, he was 11 years too old for the heart transplant program at Stanford (Calif) University Medical Center. Medication wa8 no longer effec- tive. Without the surgery, death was certain.
The housekeeping staff had been standing by. At 8 pm, OConnor had them prepare the room. Then a local TV station moved in its cameras and
Heart’s design has replaceable parts The artificial heart’s modular design proved itself both during the original surgery and the replacement operation Dec 14 when a ventricle had to be replaced. Surgeons simply snapped the defective part off and attached a spare. The heart was developed by Robert K Jarvik, MD.
The ventricles are easily popped onto connectors sutured to the aorta, the pulmonary artery, and the atria. The two blood vessels have sleeves of vascular graft material, and the atria have cuffs. The connectors are said to work “like Tupperware.”
The heart is pumped by compressed air that enters the chest through two catheters connected to the external drive unit. The air comes into diaphragms in the ventricles, which expand and push the blood out. The airtight diaphragms are separated from the rest of the chamber by four layers of polyurethane 116,000 of an inch thick separated by a dry graphite powder.
Supported on an aluminum base, the ventricles are made of a molded polyurethane called Biomer. The plastic is so fine that it appears smooth under an electron microscope, and thus is compatible with the blood.
The heart‘s rate can be regulated manually. Two weeks after the original surgery, the device was set at 75 beats per minute, and the cardiac output was at a normal level of 7 L per minute. At 130/80, Dr Clark’s blood pressure was within the normal range.
about the same as the heart of a 20-year-old man. It will fit comfortably into the chest of an average man, but the current model is too big for most women.
the heart system h a s safety alarms and a back-up mechanism. Those attending the patient would have three or four minutes to switch to the back-up system in case it is needed.
The artificial heart weighs 280 g, which is
In case of mechanical or electrical failure,
186 AORN Journal, February 1983, Vol37, No 2

AORN Journal, Februuty 1983, Vol37, No 2 189

wires. OR nurses Karsten and Baldwin were able to set up quickly. “We knew what we needed, so it only took us a half hour,” Karsten commented. The room was ready.
From the standpoint of security and traffic control, the timing was right. At that late hour, few other procedures were underway. Security personnel were stationed at all entrances to the suite, and no one was admitted to the area without identification.
OConnor stayed in the room near the door to keep out curious onlookers. In all, 26 people were in the room, includ- ing the surgical team, auxiliary per- sonnel, and cameramen. They had ex- pected 18.
Soon after 10 pm, Dr Clark was wheeled in and transferred onto the OR bed. The staff marveled at his quiet strength. The anesthesiologist told Dr Clark that he would not be able to give him preoperative medication because of the condition of his heart. “We’re asking you to help us by just being totally re- laxed,” he said.
“He became so relaxed, I thought he was asleep, but he continued to answer questions,” OConnor commented.
Preparing the patient and adminis- tering anesthesia took an hour. The anesthesiologist chose Fentanyl as the anesthetic agent. About 11:30 pm, the team opened the chest and began can- nulation for cardiopulmonary bypass. Because Dr Clark was a cardiomyopathy patient who would have an implant, no cardioplegia was needed.
After the patient was placed on bypass, Dr DeVries began dissecting the two ventricles, which the heart prosthesis would replace. The two atria were left. The surgeon passed the dis- sected heart to Baldwin, who handed it off to Karsten, who placed it on the back table. Soft and mushy, it continued to quiver.
“I found myself staring at it,” O’Con-
nor said. Baldwin said that doing the cadaver
cases had prepared her for the shock of holding the excised heart. “When we first did it on a cadaver, I realized, ‘This is the heart-the point of no return.’ I’m glad I had the cadaver experience first.” The specimen was picked up by the pathology department for special biop- sies. Now the remaining heart and blood
vessels could be prepared to receive the implant. To the aorta and pulmonary artery, the surgeon sutured sleeves made of vascular grait material (Fig 1). Cuffs were sewn to the atria. Both the vascular sleeves and the cuffs had spe- cially designed flanges that the artifi- cial heart would be snapped onto.
The connectors work “like Tupper- ware,” Karsten explained. In fact, Robert K Jarvik, MD, the artificial heart’s inventor, was said to have got- ten the idea aRer his wife attended a Tupperware party. The snap-off design enables surgeons to change the pros- thesis easily in case of mechanical prob- lems. That feature would prove to be important later in this procedure and again 13 days later, when the mitral valve cracked.
Suturing the graft material in place was tricky because Dr Clark’s tissues were fragile due to previous cortico- steroid therapy. Dr DeVries had to be very gentle, taking small bites with the needle. He sewed over and over to tighten the graR and keep the suture line from bleeding. The surgeon used 2-0 polypropylene on the aorta and 3-0 polypropylene on the cuffs. “It was just regular vascular suture,” Karsten noted.
The patient was ready to receive his new heart. Waiting on the back table, the implant had been gas sterilized. A back-up prosthesis was also prepared in case it was needed. Since the device was not made of foreign protein, no immu-
190 AORN Journal, February 1983, Vol37, No 2

Dr Clark is transferred to the operating room bed. He was so ill that the anesthesiologist informed him he could not administer preoperative medication.
nosuppression was needed. The heart had been treated with thrombin, and Karsten filled it with heparinized saline to keep it wet inside.
Dr DeVries snapped the prosthesis in place. He aspirated air by inserting a needle into two ports on the heart de- signed for that purpose. The patient was taken off bypass, and the machine that drives the heart was started. So far so good. But there was a problem. A valve in the leR ventricle was sticking. They would have to back up.
Again, the patient was placed on the heart-lung machine. Because of the im- plant’s clever design, Dr DeVries was able to disconnect the leR ventricle and replace it with a new left ventricle from the reserve prosthesis. Although replac- ing the defective part was easy, the process extended the surgery by about two or three hours. The time was needed to take him on and off bypass as well as
to repair a tear in the atrium. Cardiopulmonary bypass was ended
once again. The heart’s drive unit was turned on. “When they turned those pumps on, and the heart worked, you could hear a big sigh of relief,” Karsten said. “I turned and looked at Colleen. It was like a breath of fresh air. Everybody had instant energy.”
The 7% hour procedure was over. It was now 7 am. Dr Clark would be taken directly to a specially designed room in the ICU. Deciding who would transport him was not difficult.
“We all went,” Karsten laughed. In the ICU, Dr Clark had one RN as-
signed only to him for each shift. Unlike other cardiac surgery patients, Dr Clark does not require electrocardio- graph monitoring. “He has a flat ECG,” Karsten pointed out, since there is no heart muscle to send signals to the monitor. Rather, his heart function is
AORN Journal, Februnty 1983. Vol37, No 2 191

monitored by the technicians responsi- ble for the drive unit. Soon after sur- gery, his cardiac output had increased to 7.5 to 8 L per minute, and his blood pressure was within the normal range.
All went well at first. Then complica- tions began developing. The surgical consent form had been explicit about this possibility. The risks included mechanical malfunction or failure of the device itself, as well as infection and other complications of complex cardiac surgery.
On Saturday, two days after the im- plant procedure, Dr Clark developed subcutaneous emphysema as air es- caped through blebs in the lungs. The blebs were closed in a nonemergency operation that day, and a chest tube was reinserted. These were a complication of the chest surgery, unrelated to the arti- ficial heart.
Other immediate complications were acute tubular necrosis, which was tem- porary, and seizures of an uncertain cause, which occurred on Tuesday, five days after the heart surgery. The sei- zures lasted more than two hours. After the seizure episode, he appeared to be recovering slowly but steadily. He was still on a respirator, which was being removed for brief periods.
The first crisis with the artificial heart itself came Dec 14, almost two weeks after the original surgery. Dr Clark’s blood pressure dropped sud- denly, and he was rushed back to the operating room. Again, Karsten circu- lated and Baldwin scrubbed. When the surgeons opened the chest, they found the mitral valve had cracked. The heart’s modular design again proved valuable, as Dr DeVries pulled off the left ventricle and connected a new part. Spare implants had been sterilized and kept in reserve. Of the two- to three- hour surgery, replacing the ventricle took only about 25 minutes.
As he entered his third week with the
Surgical consent is rigorous process Barney Clark went into surgery knowing there were no guarantees. He knew the artifical heart was experimental and could fail. He knew the longest an animal had lived with the device was nine months. He was aware his mobility would be severely restricted. He also knew there was no alternative but death.
artificial heart through an elaborate protocol. After being referred to the University of Utah, he was screened by a six-member evaluation committee. They had to vote unanimously in favor of selecting him as a candidate.
Chaired by William C DeVries, MD, chairman of thoracic and cardiovascular surgery, who would perform the operation, the panel also included two cardiologists, a social worker, a psychiatrist, and a nurse. Helen Kee, RN, assistant hospital administrator and director of nursing service, represented nursing. She also coordinated the hospital’s planning for this special patient.
Since Dr Clark was gravely ill, the committee met with him immediately and took their vote the next morning. It was unanimous.
“suffering from chronic nonoperable end-stage progressive congestive heart failure.” This is the profile for New York Heart Association Class IV patients. He was to have been in this condition for at least eight weeks, showing no improvement. The life span for these patients is generally considered to be six months or less.
From Dr Clark’s background, the panel knew he came from a stable home situation. His life history showed a pattern of psychological stability and determination. As a dentist, he had a background that would enable him to understand the disease process and the mechanics of the artificial heart system. He had no other
Dr Clark was fully informed about the
The research criteria required that he be
192 AORN Journal, February 1983, Vol37, No 2




















![The human heart [recovered]](https://img.pdfslide.us/doc/110x75/58ae95681a28abdf068b64df/the-human-heart-recovered.jpg)
