Embed Size (px)
Citation preview

RECONSTRUCTION CONUNDRUM
Repair of an Alar Defect
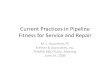
A healthy, 44-year-old white man was referred forMohs micrographic surgery of a biopsy-proven basalcell carcinoma of the left ala. At presentation, thepatient had a nodular plaque measuring 0.6�0.5 cmwith ill-defined clinical borders of the left ala. Giventhe critical anatomic location and ill-defined borders,Mohs micrographic surgery was indicated. The tumorwas subsequently extirpated in two stages using theMohs technique producing a surgical defect measuring
1.4� 1.0 cm in greatest dimension. The resultant sur-gical defect extended into the subcutaneous tissue ofthe left ala but did not perforate into the nasal vesti-bule (Figure 1). Reconstructive options consideredincluded second intention healing, full-thickness skingraft, composite graft, island pedicle flap, and a two-stage interpolation flap. As a dermatologic surgeon,how would you address this patient’s surgical defect toyield the optimum functional and aesthetic restoration?
r 2003 by the American Society for Dermatologic Surgery, Inc. � Published by Blackwell Publishing, Inc.ISSN: 1076-0512/03/$15.00/0 � Dermatol Surg 2003;29:1089–1091
Figure1.

Resolution
After tumor extirpation in which accurate surgicalmargins have been assured to be negative, thedermatologic surgeon is frequently confronted withsoft-tissue defects of the nasal ala. The paramountreconstruction goal includes restoring function if lostor preserving function if maintained. This must beallied with a reconstructive option that produceselegant cosmetic results with concomitant little mor-bidity in a cost-effective fashion.
The topographic complexity of the nasal ala hasfrequently challenged the dermatologic surgeon. In thisparticular instance, the defect was rather small andwas not full thickness. However, the close proximity tothe free alar margin has produced a surgical defect ofmoderate complexity. The reconstructive surgeon mustclearly understand the aesthetic importance of thisarea of the nose and the poor tolerance for alarmovement in achieving excellent cosmetic results. Ifthe ala is displaced upward, suboptimal results andpatient dissatisfaction may result. The reconstructivesurgeon must also consider the anatomy of the nasalvalve and the patency of the nasal airway whenreconstructing defects in this anatomic location.
Although second intention healing may producenice results in the more concave areas of the ala(around the alar groove), it is not a viable option inthis case. Predictable wound contraction wouldundoubtedly produce elevation of the free alar marginand a poor end cosmetic result. The close proximity ofthe caudad margin of this surgical defect to the freealar rim must be carefully considered. In my opinion, afull-thickness skin graft obtained from a suitabledonor site (e.g., the conchal bowl) would in this caseprove not only inadequate to fill the contour defect butalso may allow for cephalic alar retraction. A
composite graft of skin and perichondrium or skin,perichondrium, and cartilage may have been used toreconstruct this surgical defect. A composite graft mayyield less retraction during a postoperative period. Acomposite graft containing an underlying strut ofcartilage may have been harvested from the conchalfloor to repair this surgical defect. However, in myexperience, the viability of the composite grafts foralar defects is significantly less predictable than that ofrandom pattern cutaneous flaps.
For surgical defects of this type, random patternflaps prove unsurpassed in matching the qualities ofmissing skin and soft tissue and their ability to restorethe complex topography of this anatomic subunit.Local flaps obtained from the lower nasal sidewall orlateral portion of the ala (bilobed transposition flap-medial base and island pedicle flap, respectively)would prove difficult in this particular situation. Theseflaps rely on some degree of secondary movement toachieve surgical closure and would place an inordinaterisk on distortion of the alar margin. For this reason, Ithought that the best reconstructive option was a two-staged interpolation flap (Figure 2). This is a randompattern cutaneous flap that is based somewhat on thevasculature of the angular artery, a branch of the facialartery. These interpolation flaps, if done with surgicalprecision, are typically robust flaps. The cheekinterpolation flap traditionally has a donor site at ornear the midpoint of the melolabial fold. This allowsthe result of the donor scar to be placed carefullywithin the melolabial fold, assisting in scar camou-flage. However, this is problematic for several reasons.In men, the interpolation flap may frequently trans-pose course terminal hair onto the ala, resulting in anobvious cosmetic problem. Secondary ablative proce-dures or laser-assisted hair removal may improve thecosmetic results but add yet another stage to the
Figure2. Figure 3.
1090 COOK: RECONSTRUCTION CONUNDRUM Dermatol Surg 29:10:October 2003

reconstructive efforts. Furthermore, for larger alardefects, the harvesting of the melolabial flap from thecheek as traditionally described may result in conspic-uous flattening of the cheek and subtle asymmetry ofthe melolabial folds, an aesthetic result that somepatients may find displeasing. For these reasons, Ichose to change convention and place the donor sitealong the paranasal cheek at the junction of theaesthetic subunits of the lateral nasal dorsum andmedial cheek. The resultant donor scar will hidecarefully in this aesthetic boundary. This flap lacks thecourse terminal hair of the lower face, and the donorsite may be easily closed by advancing the cheek to fillthe surgical defect.
When performing this flap, it is of paramountimportance to preserve the vascular integrity at thebase of the flap. Careful undermining in a deepersubcutaneous plane will preserve this vascular pedicle.The flap is then trimmed to meet the size of thesurgical defect of the ala and sutured into place. Thedonor site is appropriately closed in this case, as notedby sliding the cheek medially to the border of theaesthetic subunit. Sutures are removed in 5 days, andthe flap is allowed to mature for 3 weeks from the dateof the initial surgery. At this time, the pedicle istransected. The flap skin is then thinned and inset tofill the surgical defect and is sutured into place. Thereconstructive surgeon at this point may wish toextend the surgical defect to encompass the entire
remnant of the aesthetic unit. Sutures from thesecondary procedure are removed at 7 days. Thepatient is then followed carefully to observe for anypostoperative complications, although they rarelyoccur with this particular flap. In this case, the endaesthetic result was nice, and no additional surgicalprocedures were performed (Figure 3).
Conundrum Keys
� Care must be taken to maintain or restore alarfunction and form.
� Two-staged interpolation flaps offer the advantagesof closely matching skin, contour restoration, andavoidance of scarring and distortion caused byincorrectly designed adjacent flaps.
� The inferiorly based paranasal cheek interpolationflap has the advantage of avoiding transfer ofterminal hair to the nose and distortion of thelower cheek and is easily camouflaged at the borderof the aesthetic units of nasal sidewall and cheek.
JOEL COOK, MDDepartment of Dermatology
Medical University ofSouth CarolinaCharleston, SC
Dermatol Surg 29:10:October 2003 COOK: RECONSTRUCTION CONUNDRUM 1091