Embed Size (px)
Citation preview

NATURE REVIEWS | RHEUMATOLOGY VOLUME 11 | JANUARY 2015 | 21
Department of Biomedical Engineering (E.A.M., J.C.H.), Department of Orthopaedic Surgery (K.A.A.), University of California Davis, One Shields Avenue, Davis, CA 95616, USA.Department of Orthopaedic Surgery and Musculoskeletal Trauma, University of Thessaly, Biopolis, Larisa 41110, Greece (K.N.M.). Department of Orthopaedic Surgery, Brigham and Women’s Hospital, Harvard Medical School, 75 Francis Street, Boston, MA 02115, USA (A.H.G.).
Correspondence to: K.A.A. athanasiou@ ucdavis.edu
Repair and tissue engineering techniques for articular cartilageEleftherios A. Makris, Andreas H. Gomoll, Konstantinos N. Malizos, Jerry C. Hu and Kyriacos A. Athanasiou
Abstract | Chondral and osteochondral lesions due to injury or other pathology commonly result in the development of osteoarthritis, eventually leading to progressive total joint destruction. Although current progress suggests that biologic agents can delay the advancement of deterioration, such drugs are incapable of promoting tissue restoration. The limited ability of articular cartilage to regenerate renders joint arthroplasty an unavoidable surgical intervention. This Review describes current, widely used clinical repair techniques for resurfacing articular cartilage defects; short-term and long-term clinical outcomes of these techniques are discussed. Also reviewed is a developmental pipeline of acellular and cellular regenerative products and techniques that could revolutionize joint care over the next decade by promoting the development of functional articular cartilage. Acellular products typically consist of collagen or hyaluronic-acid-based materials, whereas cellular techniques use either primary cells or stem cells, with or without scaffolds. Central to these efforts is the prominent role that tissue engineering has in translating biological technology into clinical products; therefore, concomitant regulatory processes are also discussed.
Makris, E. A. et al. Nat. Rev. Rheumatol. 11, 21–34 (2015); published online 23 September 2014; doi:10.1038/nrrheum.2014.157
IntroductionThe management of articular cartilage defects is one of the most challenging clinical problems for orthopaedic surgeons. Articular cartilage, a highly organized tissue with substantial durability, has a limited intrinsic healing capacity. Damage from trauma or degenerative pathol-ogy frequently results in gradual tissue deterioration, leading to debilitating joint pain, functional impairment and degenerative arthritis.1 Currently, the standard surgi-cal intervention for end-stage degenerative joint pathol-ogy is total joint replacement. Early surgical intervention for symptomatic cartilage lesions, including osteotomy and autologous osteochondral graft transplantation, has been suggested to restore normal joint congruity and minimize further joint deterioration.2 Often, these tech-niques are not long-term clinical solutions, prompting the development of regenerative medicine and tissue engineering approaches to restore articular cartilage. Strategies include cell-based (with or without scaffolds) or whole-tissue transplantation techniques.
In this Review, we discuss the basic science, indica-tions, advantages, shortcomings and outcomes of inter-ventions for cartilage healing. The goal is to provide an evidence-based assessment for the treatment of articu-lar cartilage pathology by reviewing the literature, with particular focus on the clinical outcomes of prospective randomized controlled trials (Table 1). Moreover, we discuss current prospective tissue engineering trials for cartilage repair, with an emphasis on cell sources, the
clinical aspects of cell administration, the use of mesen-chymal stem cells (MSCs), growth-factor-based therapies and cell-free, implantation-based therapies. Finally, the scien tific and regulatory challenges in translating these approaches to clinical practice are discussed.
Present repair techniquesMicrofractureMicrofracture was introduced to the clinic after other bone-marrow-stimulation techniques were used in the late 1980s and early 1990s to penetrate subchondral bone. This technique enhances migration of MSCs from bone marrow to the site of a cartilage defect (Figure 1a–c); however, microfracture often results in the formation of fibrocartilage that is biochemically and biomechani-cally inferior to hyaline articular cartilage.3,4 A case series study has shown that without the mechanical robustness of hyaline tissue, the repair tissue is vulner-able to mechanical joint forces and typically deteriorates ~18–24 months after surgery, as shown by the modified Cincinnati Rating System for knee and International Cartilage Repair Society (ICRS) scores postoperatively, compared with baseline scores (Box 1).4 Such deteriora-tion is particularly evident when treating large defects or those located in the patellofemoral joint.4 Furthermore, owing to the penetration of the subchondral bone, intra-lesional osteophytes develop in 20–50% of cases.5 The altered biomechanics of the sclerotic bone might be the cause of a threefold-to-sevenfold increase in the failure rate of autologous chondrocyte implantation (ACI) when performed after prior microfracture.6,7 Specific indica-tions have, therefore, been proposed for performing this
Competing interestsA.H.G. declares that he consults for Sanofi S.A. The other authors declare no competing interests.
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

22 | JANUARY 2015 | VOLUME 11 www.nature.com/nrrheum
technique in cartilage lesions. These indications are based on the size, depth and location of the lesion in the joint, as well as the patient’s age and BMI (Figure 2). Although the FDA and many clinicians still consider microfracture to be the gold standard for cartilage repair, prospective comparative studies show that microfracture might delay cartilage degeneration only in the short-term; more than 5 years after surgery, treatment failure can be expected regardless of the size of the lesion.8,9 A detailed descrip-tion of the indications, clinical application, rehabilitation and outcomes of the standard microfracture procedure has been reviewed elsewhere,10 and is outside the scope of this article. However, a brief understanding of this technique is important, as microfracture has become a ubiquitous approach to surgical regeneration of cartilage, the shortcomings of which have ultimately spurred the development of procedures that aim to fully regenerate articular cartilage.
Autologous chondrocyte implantationThe inconsistent outcomes of microfracture prompted the development of ACI. To perform this technique, a full-thickness sample from a low-weight-bearing region of the joint is collected by biopsy punch during a first arthro-scopic operation to provide a chondrocyte population that is then expanded in vitro, yielding ~12–48 million cells. During a second operation the chondrocytes are implanted into the debrided cartilage defect and covered by a membrane (Figure 1d). This technique has two major benefits: using a patient’s own cells avoids potential immune complications or viral infections from transplant-ing allogeneic cells or foreign materials; and as opposed to autologous osteochondral implantation, the small biopsy minimizes complications for the chondrocy te donor.11,12
Positive clinical and functional outcomes of ACI have been confirmed by clinical trials.13–15 Long-term case series with >10 years follow-up have demonstrated that ACI is an effective and durable treatment for large (>4 cm2) knee cartilage lesions.13,14 Other clinical trials have reported similar results,16,17 highlighting the benefits
Key points
■ The limited ability of articular cartilage to regenerate has prompted the development of cell-based tissue engineering techniques, such as autologous chondrocyte implantation
■ The complexity of autologous chondrocyte implantation and contraindications in wide clinical application have driven the development of matrix-assisted chondrocyte implantation, which uses scaffolds to provide mechanical stability and support chondrogenesis
■ To improve neotissue formation, graft maturation and biomechanical integrity, cells can be cultured in vitro before implantation on 3D matrices with exogenous stimuli, such as growth factors
■ Biomaterials such as collagen type I and III membranes are also used in cell-free approaches to enhance cartilage’s innate regenerative capacity by functioning as scaffolds for resident progenitor cells
■ Scaffold-free, cell-based techniques to form biomimetic neotissues, which can avoid disadvantages of scaffold use such as limited biocompatibility and release of degradation byproducts, are now in development
■ Despite promising results and advances in cartilage tissue engineering, translation into clinical practice has not yet been achieved, as many challenges remain to be resolved
of combining ACI with a corrective osteotomy.18 Whether ACI is superior to other standard treatments in prospec-tive randomized controlled clinical trials, however, is controversial. A study comparing ACI to autologous osteochondral transplantation (mosaicplasty) found ACI to have superior clinical results 10 years postopera-tively;19 other studies demonstrated superior outcomes for ACI when compared with microfracture for the treatment of cartilage defects >3 cm2 in size.20,21 Studies of ACI and microfracture for smaller defects, however, have found similar clinical and radiographically evident out comes,22 although ACI has been associated with improved structural repair.12,23 Additional large-scale prospective random ized studies with a long-term follow-up are necessary to identify and understand the clinical criteria, indications and contraindications for when ACI might provide superior clinical outcomes over less inva-sive and costly techniques, such as microfracture. Ideally, functional evaluation should be supplemented by charac-terization of neotissue with sophisticated imaging or arthroscopic techniques.
ACI has three major drawbacks: two operations are needed; a long recovery time (6–12 months) is required to ensure neotissue maturation and achieve improved clinical scores from baseline; and ACI is a multistage, com plex procedure. The most frequently reported adverse event after ACI, using a periosteal flap to seal the implanted cells in the cartilage defect, is hyper trophy of the flap.24 Therefore, alternative approaches utilize artificial ma trices such as porcine membranes consist-ing of mixtures of collagen types I and III or hyaluronic acid scaffolds.25–27 However, these materials increase the likelihood of an immune reaction to the allogeneic scaf-fold, and their use is currently considered off-label in the USA. Preliminary studies have also shown that autolo-gous chondrocytes ‘dedifferentiate’ into fibrochondro-cytes in culture.28 However, other work shows they can redifferentiate and express chondrocytic markers after being reintroduced into a 3D in vitro culture system.29 To standardize clinical outcomes of ACI, patient-specific and cartilage defect-specific factors have been established to generate a treatment algorithm that improves the likeli-hood of a successful outcome (Figure 2). Nevertheless, large-scale cohort studies are needed to further in vestigate the cost-effectiveness of ACI.
Overall, ACI has proven beneficial for treating cartilage defects, but more research needs to be done to develop biomechanically stable matrices, to achieve faster matura-tion of the neotissue and better integration with the host tissue. Furthermore, work is required to standardize and optimize the technique and the post-surgery functional evaluation so that surgeon and patient biases do not affect the functional outcome.
Scaffold-based techniquesThe lack of a supportive scaffold material to guide matrix synthesis and organization might, in part, account for the outcome variability across patient populations treated with chondrocyte implantation techniques. Ex vivo studies have shown that successful cartilage regeneration
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 11 | JANUARY 2015 | 23
Table 1 | Randomized controlled trials comparing cartilage regeneration techniques
Study Treatments Follow-up (months)
Clinical outcome Comments
Wong et al.65
(2013)Bone marrow MSCs + HA + microfracture (n = 28)HA + microfracture (n = 28)
24 The bone marrow MSC-treated group were significantly better in IKDC (P = 0.001), Lysholm (P = 0.016), Tegner (P = 0.021) and MOCART (P <0.001) scores
Larger mean lesion size in the MSC-recipient group (6.0 cm2) than in the control group (3.5 cm2)
Stanish et al.100
(2013)BST-CarGel® (n = 41)Microfracture (n = 39)
12 MRI showed greater lesion filling (P = 0.011) and better hyaline cartilage-like MRI T2 values (P = 0.033) in the BST-CarGel® group than the microfracture group
WOMAC showed equivalent improvement in both groups
Saw et al.77
(2013)Subchondral drilling + HA + PBSCs (n = 25)Subchondral drilling + HA (n = 25)
18 PBSC group had significantly better ICRS II histological scores (P = 0.022) and MRI morphological scores (P = 0.013)
No significant difference in the mean 24-month IKDC scores between the control and intervention groups
Patel et al.96
(2013)PRP (1 injection; n = 52)PRP (2 injections; n = 50)Normal saline (1 injection; n = 46)
6 Both PRP-treated groups had better WOMAC questionnaire results (P <0.001) than the normal saline group; a single dose of PRP is as effective as two PRP injections to alleviate symptoms in OA
The results slightly deteriorated 6 months after surgery in both PRP treated groups
Gudas et al.9
(2013)OAT–ACL (n = 34)Microfracture–ACL (n = 34)Debridement–ACL (n = 34)IAC–ACL (n = 34)
36 The IAC–ACL group’s IKDC subjective knee evaluation was significantly better than that of the OAT–ACL group (P = 0.043)The OAT–ACL group’s IKDC subjective knee evaluation was significantly better than that of the microfracture-ACL group (P = 0.024) and debridement-ACL group (P = 0.018)
No significant difference between the microfracture–ACL and debridement-ACL group IKDC subjective scores (P = 0.058)
Filardo et al.102
(2012) PRP (n = 54)HA (n = 55)
12 No significant differences in IKDC, EQ-VAS, Tegner and KOOS scores between the groups
For middle-aged patients with moderate signs of osteoarthritis, PRP was nonsuperior to hyaluronic acid injections
Crawford et al.49
(2012)NeoCart (n = 21)Microfracture (n = 9)
24 Improvement in the NeoCart group was significantly better (P <0.05) than in the microfracture group for KOOS pain, IKDC, KOOS sports, VAS pain and the KOOS quality of life scores
Significantly more NeoCart-treated patients (P = 0.013) responded to therapy at 6, and 12 months and the trend continued at 24 months
Bentley et al.19
(2012) ACI (n = 58)Mosaicplasty (n = 42)
120 The functional outcome (Modified Cincinnati knee score and the Stanmore-Bentley functional rating system) was greater for ACI than for mosaicplasty (P = 0.02)
Repair failed within 10 years of surgery in 10 of 58 (17%) patients in the ACI group and 23 of 42 (55%) in the mosaicplasty group (P <0.001)
Vanlauwe et al.113
(2011)CCI (n = 51)Microfracture (n = 61)
60 CCI and microfracture were comparable for the KOOS and oKOOS scores; in the early treatment group CCI was statistically significant (P = 0.026) and clinically better than microfracture
Treatment failures were comparable (n = 7 in CCI vs n = 10 in microfracture), although microfracture failures tended to occur earlier
Cole et al.88
(2011) CAIS (n = 20)Microfracture (n = 9)
24 No differences in the number of adverse events (SF-36) between CAIS and microfracture groupsThe IKDC and KOOS scores of the CAIS groups were significantly (P <0.05) higher than the microfracture group
Differences between the 2 groups in fill of the graft bed, tissue integration, or presence of subchondral cysts were not detected by imaging analysis
Basad et al.20
(2010) MACI (n = 40)Microfracture (n = 20)
24 MACI was significantly more effective than microfracture according to the Lysholm (P = 0.005), Tegner (P = 0.04), ICRS patient (P = 0.03), and ICRS surgeon (P = 0.02) scores
MACI was superior to microfracture in the treatment of large (>4 cm2), symptomatic articular defects
Zeifang et al.35
(2010)MACI (n = 11)ACI (n = 10)
24 No differences in the IKDC (P = 0.4994), Tegner Activity (P = 0.1043) scores and SF-36 (P = 0.4063) of ACI and MACI techniquesLysholm and Gillquist scores at 12 months (P = 0.0449) and 24 months (P = 0.0487) favoured ACI
MOCART revealed no significant difference between the 2 groups (P = 0.692)
Van Assche et al.22
(2010)ACI (n = 34)Microfracture (n = 33)
24 ACI had similar overall functional outcomes to microfracture
ACI resulted in slower recovery at 9 and 12 months compared with microfracture
Abbreviations: ACI, autologous chondrocyte implantation; ACL, anterior cruciate ligament; CAIS, cartilage autograft implantation system; CCI, characterized chondrocyte implantation; EQ-VAS, EuroQol-visual analogue scale; HA, hyaluronic acid; IAC, intact articular cartilage; ICRS, International Cartilage Repair Society; IKDC, international knee documentation committee; KOOS, knee injury and osteoarthritis outcome score; MACI, matrix-assisted chondrocyte implantation; MSC, mesenchymal stem cell; OA, osteoarthritis; OAT, osteochondral autologous transplantation; oKOOS, overall knee injury and osteoarthritis outcome score; PBSC, peripheral blood stem cell; PRP, platelet-rich plasma; SF-36, short form-36; WOMAC, Western Ontario and McMaster osteoarthritis index.
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

24 | JANUARY 2015 | VOLUME 11 www.nature.com/nrrheum
is dependent both on the chondrocyte proliferation rate and on the differentiation capacity of stem cells within a tissue-engineered 3D matrix, a structure that acts as a cell carrier to maintain and support the crucial charac-teristics of the tissue.30 The second generation of ACI has therefore focused on the development of scaffold-based approaches for delivering chondrocytes to the carti-lage defect site. Scaffold-based approaches have major advantages to sc affold-free techniques: these advantages include, increased control to better fill the cartilage defect; fewer donor site complications; a less technically chal-lenging procedure; and shorter postoperative recovery time due to increased graft stability. Additionally, because the chondrocytes are cultured in a 3D environment, they are less prone to dedifferentiation and therefore produce a more hyaline-like cartilage.31 Furthermore, in vitro culture prior to implantation might help to maintain quality control of scaffold-based repair.
MACIMatrix-induced autologous chondrocyte implantation (MACI) is the most common scaffold-plus-cell-based cartilage repair technique currently in clinical prac-tice. Similar to ACI, MACI requires two surgical proce-dures. The first surgery collects autologous tissue from which the patient’s chondrocytes are isolated. Once iso-lated, the cell population is expanded in vitro and then seeded for 3 days on an absorbable porcine-derived mixed collagen (type I and III) membrane prior to implantation. These membranes are specifically engineered to promote chondrocyte infiltration on one side and low friction on the other. To implant the cell-seeded scaffold a mini- arthrotomy exposes and debrides the lesion, after which the matrix is implanted and secured using fibrin glue,
with the cell-laden side facing the sub chondral bone and the low-friction surface facing the joint cavity (Figure 1e).
Although case series of MACI have had promising clinical and histological results,32,33 the superiority of MACI over existing techniques remains unproven. One of the few prospective randomized clinical trials to assess MACI found comparable clinical, arthroscopic and histo-logical outcomes between MACI-treated or ACI-treated patients;34 however, the MACI-treated group had a lower rate of hypertrophy of the graft. Another study reported no differences in International Knee Documentation Committee (IKDC) scores, Tegner activity scores or the Short Form-36 from patients 24 months after undergoing either MACI or ACI; however, Lysholm and Guillquist knee functionality scores showed better efficacy of the ACI technique than MACI (Box 1).35 A separate study found outcomes to be better with MACI than micro-fracture for patients with large (>4 cm2) defects 2 years after surgery.20 Overall, these studies found MACI to have similar, if not superior, functional outcomes to either ACI or microfracture in a follow-up study after ≥2 years. Although MACI is technically attractive in terms of reproducibility, safety, surgical simplicity and reducing invasiveness and intraoperative time, the expense of the technique warrants further investigation. Large prospec-tive randomized trials with long follow-up periods are also necessary to identify clinical criteria, indications and contraindications to optimize the performance of this technique.
Hyaluronic-acid-based scaffoldsHyaluronic-acid-based scaffolds are another means of implanting chondrocytes within a 3D biodegradable environment. Similar to collagen-derived matrices, the
a
c d e
bFemur
Articularcartilage
Lesion
Medial collateral ligament
Lateralcollateralligament
Fibula Tibia
Anteriorcruciateligament
Posteriorcruciateligament
Medialmeniscus
Lateralmeniscus
Autologous chondrocyte
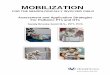
Figure 1 | Cartilage regeneration techniques. a | A full-thickness focal chondral lesion. b | The lesion is debrided to ensure healthy, stable margins for integration of the host tissue with the neotissue. c | Microfracture. Channels are created using a 45° awl, spaced 3–4 mm apart, and 3–4 mm deep to penetrate the subchondral bone, allowing MSCs to migrate from the marrow to the cartilage defect. d | ACI. The debrided lesion is filled with 12–48 million autologous chondrocytes and covered with a periosteal flap or mixed collagen type I and type III membrane. e | MACI. The autologous chondrocyte population is expanded in vitro and then seeded for 3 days onto an absorbable 3D (collagen types I and III or hyaluronic acid) matrix prior to implantation. The cell-seeded scaffold is then secured into the lesion with fibrin glue. Abbreviations: ACI, autologous chondrocyte implantation; MACI, matrix-assisted autologous chondrocyte implantation; MSC, mesenchymal stem cell.
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 11 | JANUARY 2015 | 25
hyaluronic-acid-based scaffold is intended to promote and maintain the chondrocytic phenotype and col-lagen type II synthesis during in vitro culture, as well as after implantation (Figure 1e).36 Although, ex vivo studies have reported that the degradation rate of these ma terials can be tailored to match the rate of the synthe-sis of extra cellular matrix (ECM) by the cells to aid in
integration with the defect site,36,37 this finding has not been confirm ed in long-term follow-up clinical studies.
Treating cartilage defects with autologous chondro-cytes delivered with a hyaluronic-acid-based scaffold has shown promise. In case series, hyaline-like cartilage has been shown to develop ~1 year after implantation,27,38 and improved functional and health-related quality of life outcomes have been reported 3 years after implantation, compared with baseline.27 A prospective cohort study, evaluating athletes treated with either hyaluronic-acid-based MACI or microfracture, found com parable out-comes in ICRS, IKDC and Tegner scores (Box 1) between the two groups 2 years postoperatively.38 However, better IKDC scores were detected 7.5 years after operation in the hyaluronic-acid-based MACI group than in the group treated with microfracture. Interestingly, athletes treated by microfracture required at least 8 months of recovery before returning to the field, whereas those receiving hyaluronic-acid-based MACI required 12.5 months.38 Thus, although hyaluronic-acid-based MACI ultimately has better clinical outcomes than microfracture, longer rehabilitation is required. In a small cohort study, statis-tically significant differences were not found in the functional outcomes or the histological and immuno-histochemical composition of hyaluronic-acid-based and fibrin-based scaffolds (both seeded with chondrocytes) 1 year after implantation.39 Although scaffold-based ACI for cartilage regeneration is approved in Europe, and FDA approval is currently pending in the USA, well-designed comparative studies with long follow-up periods are needed to confirm the potential therapeutic and e conomic benefits.
Future regenerative approachesEx vivo chondrocyte-seeded scaffoldsDespite the technical advantages of MACI, clinical studies have revealed the functional outcomes to be similar to
Box 1 | Tools to evaluate joint function, cartilage repair and quality of life
■ American Orthopaedic Foot & Ankle Society (AOFAS) score: evaluates and monitors the progress of patients after foot and ankle surgery
■ Ankle Osteoarthritis Scale (AOS) score: is a visual analogue, self-administered instrument to measure disability and pain from ankle osteoarthritis
■ Cincinnati knee rating scale: evaluates functional status of a degenerative knee based on symptoms, sports activity, daily activities and clinical parameters
■ EuroQol visual analogue scale (EQ-VAS): records the patient’s self-rated health on a visual analogue scale and records a quantitative measure of health
■ Guillquist knee scoring scale: provides a functional scoring scale for follow-up of knee ligament surgery, concentrating primarily on knee stability
■ International Cartilage Repair Society (ICRS) score: provides macroscopic evaluation of cartilage repair
■ International Knee Documentation Committee (IKDC) subjective knee evaluation form: detects improvement or deterioration in function, symptoms and activities due to knee impairment
■ Knee injury and Osteoarthritis Outcome Score (KOOS): evaluates patients’ opinions about their knee and associated problems over short-term and long-term follow up (1 week to decades)
■ Lysholm knee scoring scale: evaluates outcomes of knee ligament surgery, particularly symptoms of instability
■ Modified Cincinnati rating system: requires patient input only; provides user with an overall score as well as symptom and functional subscores
■ Short Form-36 (SF-36): evaluates health status and determines the cost-effectiveness of a treatment in health economics analyses
■ Tegner activity score: provides a standardized method to evaluate work and sport activities; complements the Lysholm scale, based on observations that limitations in function scores (Lysholm) might be masked by a decrease in activity
■ Western Ontario and McMaster Universities osteoarthritis index (WOMAC): assesses the course of disease and response to treatment in patients with degenerative hip or knee pathology
Patello-femoral
joint
Femoralcondyle
<2–3 cm
≥2–3 cm
<2–3 cm
≥2–3 cm
Lesion location Lesion size Primary treatment options
Secondary treatment options
High demand Low demandAssessment
1 Malalignment2 Meniscal de�ciency3 Ligament insuf�ciency
1 Microfracture*2 Osteochondral autograft transplantation*
1 Microfracture*2 Autologous chondrocyte implantation
1 Microfracture*2 Autologous chondrocyte implantation
1 Osteochondral allograft*2 Autologous chondrocyte implantation*3 Microfracture4 Osteochondral autograft transplantation
1 Microfracture*2 Osteochondral autograft transplantation*
1 Osteochondral allograft*2 Autologous chondrocyte implantation*
1 Osteochondral allograft*2 Autologous chondrocyte implantation*
1 Autologous chondrocyte implantation*2 Osteochondral autograft transplantation3 Osteochondral allograft
1 Autologous chondrocyte implantation*2 Osteochondral allograft*3 Osteochondral autograft
1 Rehabilitation2 Patellofemoral alignment
Figure 2 | Algorithm for treatment of cartilage defects. If rehabilitation is not a viable option for a patient with a symptomatic cartilage lesion, the surgeon should assess both the size and location of the defect, determine whether the patient desires a more active (high demand) or sedentary (low demand) lifestyle, and consider if the patient has undergone previous cartilage repair treatments. *Recommended treatment options for a given situation.115
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

26 | JANUARY 2015 | VOLUME 11 www.nature.com/nrrheum
those of ACI.34,35 A plausible explanation is that after chondrocyte seeding, the collagen matrices are implanted into the patient within 3 days, leaving the MACI neotissue implant immature and therefore vulnerable. To improve the efficacy of such tissue engineering procedures, novel approaches are in development (Figure 3) to introduce autologous chondrocytes into a 3D matrix and culture them in vitro for longer periods, typically 4–6 weeks. During this time, articular chondrocytes produce their own ECM components within the 3D environ ment, resulting in an implant with biochemical integrity simi-lar to healthy articular cartilage. Surgical techniques similar to those established for MACI are used to engi-neer and implant the tissue. The enhanced mechanical robustness of the neotissue after long-term ex vivo 3D culture makes implants structurally and functionally more mature than MACI-based implants and, thus, potentially able to withstand normal joint loads earlier
post-implantation. This robust neotissue might improve short-term and long-term functional outcomes for patients, and ex vivo and preclinical outcomes are promis-ing,40–42 although comparative clinical studies are needed to confirm this hypothesis. Also imperative is to inves-tigate methods to form a stable interface between the implant and host tissue environment; a low integration potential raises the failure rate of the technique.43
Although in vitro culture of autologous chondrocyte-seeded 3D matrices might result in robust chondral implants, time alone is not enough to promote suffi-cient maturation of the engineered tissue. Researchers have therefore sought exogenous chondrocyte stimuli analogous to those that promote biomechanically robust implants in vivo. Walking, for example, can create loads of ~4–5 times body weight on normal human knee car-tilage.44 Chondrocytes respond to high mechanical loads by proliferating and producing ECM.45 Thus, exogenous
Cell-free scaffold
Intra-articular injection of bone marrow MSCs
Scaffold-free techniques
dc
Cellular scaffold
Particulated allografts
f
Cell slurry
a b
e
Hyaluronic acid
MSC
Engineered neotissue
Figure 3 | New tissue engineering techniques for treating cartilage lesions. a | Technically mimicking ACI, a debrided chondral lesion is filled with bone-marrow-derived or chondroinduced MSCs, not autologous chondrocytes, and covered with a collagen type I/III membrane. b | Intra-articular injection of MSCs with or without injectable matrices is a single-stage procedure. c | AMIC is a cell-free, scaffold-based single surgery. Microfracture releases blood and bone marrow MSCs, then collagen type I/III, hyaluronic acid or fibrin matrix are sutured or glued into the defect. d | MACI uses scaffolds plus either primary articular chondrocytes or bone-marrow-derived MSCs. e | Neotissue can be formed by combining particulated native cartilage with fibrin glue. Limited autodigestion of ECM releases superficial chondrocytes, which then produce additional ECM that integrates the cartilage particles and fills the defect. f | Scaffold-free techniques include a self-assembling process or chondrospheres. Without a scaffold to interrupt cell–cell signalling and stress shielding, cells are able to respond to stimuli and promote integration of neotisssue ECM with the surrounding tissue. Resulting neotissue is thought to be a bioactive microenvironment. Abbreviations: ACI, autologous chondrocyte implantation; AMIC, autologous matrix-induced chondrogenesis; ECM, extracellular matrix; MACI, matrix-induced autologous chondrocyte implantation; MSC, mesenchymal stem cell.
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 11 | JANUARY 2015 | 27
mechanical stimulation has been applied to cell-laden matrices in vitro, in the form of either hydrostatic pres-sure40 or dynamic compression,41 to improve matrix maturation and the function of neotissues. Research has also identified growth factors that help chondro-cytes to maintain their phenotype and ability to produce ECM. The most important growth factors widely used in cartilage regeneration and tissue engineering ex vivo studies are transforming growth factor β (TGF-β) family members, particularly TGF-β1 and TGF-β3.46 In vitro tissue engineering studies have confirmed that TGF-β stimulation helps maintain the native chondrocyte pheno type, enhances the biochemical composition and functional properties of the neotissue, and promotes the development of implants that exhibit structure–function relationships similar to native articular cartilage.40,41,47 Despite extensive research in this field, there is no general consensus regarding the optimal type, level and applica-tion time of growth factor and mechanical stimulation, or for combinations of these factors, to develop robust hyaline-like tissues. The array of treatment possibilities complicates and thereby increases the cost of research in this field.
Only a few human clinical reports on the outcomes of autologous chondrocyte-laden, engineered scaffold-based approaches to cartilage regeneration are available. In an FDA phase I clinical trial, eight patients were implanted with tissue-engineered, autologous- chondrocyte-seeded, collagen type I scaffolds, which were subjected to hydro-static pressure prior to surgery.48 After 1 year, cartilage defects in seven of eight patients had almost completely filled with a mature, organized repair-tissue. These prom-ising results led to a phase II clinical trial, which found that the technique had a similar safety profile as microfracture and had better clinical outcomes in most functional scores 2 years after implantation.49 Although immune reactions to the collagen scaffold were not found in this study, long-term studies should evaluate this potential.
Alternative cell and tissue sourcesCurrent cell-based clinical practices for treating articular cartilage defects and degeneration only utilize autologous chondrocytes. Despite efforts to recapitulate the in vivo environment with 3D culture, bioreactors, and exogenous mechanical and biochemical stimulation, a repair tissue with native hyaline cartilage properties has yet to be pro-duced. Thus, in an effort to avoid some of the drawbacks associated with autologous chondrocyte therapy, methods have developed using stem cells, many of which are c urrently in a queue for FDA approval for clinical studies.
Bone marrow MSCsOf the various types of stem cell in the body, MSCs derived from bone marrow have many advantages for clinical use. They are comparatively easy to isolate and proliferate, allowing for the potential to obtain them from donors and to store them in readily available cell banks. Furthermore, extensive preclinical work in vitro and in vivo confirmed by clinical trials has found that human bone marrow MSCs are capable of differentiating
into both cartilage50–53 and bone,54 meriting their use for regeneration of both osteochondral and chondral defects. Specifically, bone marrow MSCs derived from patients with advanced osteoarthritis were shown ex vivo to produce proteoglycan and collagen type II and to main-tain a chondrocytic phenotype in a scaffold in the pres-ence of TGF-β1.55,56 Another beneficial trait is their ability to selectively migrate to diseased tissues and organs, where they have been found to secrete T-cell-suppressive cytokines57,58 known to be important for allotransplanta-tion and xenotransplantation.59 In the case of cartilage repair, bone marrow MSCs might enable a targeted repair system that promotes trophic effects through the release of synthetic, proliferative and regenerative factors directly into chondral lesions.60 By creating a regenerative envi-ronment with the release of chemotactic factors,61 bone marrow MSCs might also drive endogenous stem cells to enter the cartilage defect and aid in the regeneration of damaged tissue.
Preliminary human clinical studies have investigated the cartilage regenerative potential of injected human bone marrow MSCs (Figure 3a,b,d). In a case series, four patients with osteoarthritis were treated each with a single injection of bone marrow MSCs into the knee; 1 year after the patients had decreased pain and improved joint mobility without any adverse effects.62 Good clinical and functional results were also reported in a similar case series at a 6-month follow-up.63–65 Despite the potential application of bone marrow MSCs, much remains to be investigated: such as, the number of cells required to pro-mote cartilage regeneration; whether one or more injec-tions are required to reach the desired effect; the optimal time-window for these injections; and the long-term safety of the technique. Finally, prospective controlled studies with long-term follow-up are needed to inves-tigate the therapeutic potential of bone marrow MSC in jection versus established cartilage repair techniques.
ACI-like and MACI-like strategies can use bone marrow MSCs in conjunction with scaffolds, as opposed to autologous chondrocytes (Figure 3d). Many clinical case series have used cultured bone marrow MSCs seeded into collagen scaffolds for the treatment of symptomatic cartilage defects.52,66,67 Most of these studies, which have been with a small number of patients, have reported good results less than 1 year after implantation. In a large-scale observational cohort study, 72 patients with cartilaginous lesions were treated with either ACI or bone marrow MSC implantation covered with a periosteal patch.53 The stem cells were found to treat the chondral defects as effec-tively as ACI in terms of 2-year postoperative clinical and functional outcomes. More importantly, the bone marrow MSC treatment was less expensive than ACI, avoided the risk of donor site morbidity and did not require an addi-tional operation to obtain the cells. However, pain from the surgical site from which bone marrow MSCs were harvested, along with other potential adverse effects of the additional surgical intervention, are concerns meriting further investigation.
Overall, the positive outcomes of these studies accen-tuate the potential of bone marrow MSC therapy for
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

28 | JANUARY 2015 | VOLUME 11 www.nature.com/nrrheum
cartilage repair. However, it remains to be seen how these techniques compare with more established procedures in comparative clinical studies, and further research is necessary to understand the feasibility of their clinical application. The potential benefit of preimplantation dif-ferentiation of bone marrow MSCs with growth factors or other biophysical or biomechanical stimuli that promote phenotypic change and stability also warrants addi-tional investigation. As MSCs are multi potent, studies to confirm the safety of transplanting them are also needed. Finally, future studies should directly compare bone marrow MSCs with other stem cells for their ability to regenerate cartilage.
Other MSC sourcesMost cartilage regeneration work using MSCs has been with bone-marrow-derived cells. Bone marrow aspiration, although painful, is an established method. However, stem cells can be derived from other sources, including adipose tissue, muscle, corticocancellous bone, synovium, periosteum and umbilical cord.68 Human adipose-derived stem cells are the most readily acces-sible, and in vitro studies have shown these cells to have a similar proliferative profile and differentiation capac-ity to bone marrow MSCs.69,70 Adipose-derived stem cells have been regarded as an ‘ideal’ cell source due to our ability to isolate them in comparatively large quan-tities, their nonimmunogenic and anti-inflammatory properties,71 minimal ethical considerations associated with their use and, compared with stem cells from other sources, their capacity for proliferation and differentia-tion is less likely to be affected by a person’s age.72 The clinical feasibility and safety of human adipose-derived MSCs to treat degenerative cartilage pathology was investigated in a case series by injecting the cells into the osteoarthritic knee joint of elderly patients (mean age 70.3 years, range 65–80 years) in combination with arthroscopic lavage.73 The treatment resulted in improved physical function, cartilage healing and pain reduction; however, this technique has some of the same problems as bone marrow MSC joint injections: these problems include the number of cells required to promote cartilage regeneration; whether one or more injections are required to reach the desired effect; the optimal time-window for these injections; and the long-term safety of the technique. In addition, quantitative evidence of improvement, for example with biopsy or MRI, is needed.
The chondrogenic potential of stem cells from other sources has also been studied; autologous peripheral blood stem cells (PBSCs) have been the most clini-cally investigated, albeit primarily in case series.74–76 A random ized trial investigated articular cartilage regen-eration in patients aged 18–50 years with knee chondral lesions (ICRS grade 3 and grade 4 lesions) treated with arthroscopic subchondral drilling followed by post-operative intra-articular injections of hyaluronic acid, with or without PBSCs. The study found the PBSC group had improved quality of cartilage as shown in the ICRS visual assessment scale histology score and an
MRI-based morphological score over those of the control group 18 months after injection.77 In vitro, synovial-derived stem cells have a better chondrogenic potential than stem cells from other sources,78,79 as shown by the develop ment of hyaline-like neotissue when they are seeded onto scaffolds,80 although clinical studies using these cells have not yet been conducted. Multilineage dermal stem cells have also been isolated and have a high capacity for in vitro chondroinduction in a cartilage tissue engineering study.81 Much in vitro work remains to be done to understand the chondrogenic potential of stem cells and to optimize chondrocyte differentiation. Future preclinical and comparative clinical studies will hopefully answer the many questions concerning the benefits, clini-cal applicability and cost-effectiveness of these cells, and they might identify indications and criteria for their use in cartilage healing.
Induced pluripotent stem cellsInduced pluripotent stem cells (iPSCs) also show pro-mise for chondrogenic application in the clinic. These cells have the ability to differentiate in vitro into either cartilage51,82 or bone.83,84 The expression of chondrogenic markers in human iPSCs was shown to be either com-parable or superior to bone marrow MSCs,51 whereas the quality of cartilage repair tissue formed by either human iPSC pellets or a human iPSC–alginate hydro-gel in a rat osteochondral defect model was substantially better than the tissue formed in empty defects or defects filled with alginate hydrogel.51,82 In an in vitro study, iPSCs derived from reprogrammed human synovial cells of patients with advanced osteoarthritis were used to generate mesenchymal lineage cells, such as chondro-cytes and osteoblasts.84 Despite these promising results, several questions remain to be answered: these ques-tions pertain to the chondrogenic efficacy of these cells; optimal practices for isolating, differentiating and puri-fying them ex vivo; the undesired genetic modifications of most reprogramming protocols, and the potential of teratogenesis or other in vivo tissue malformations; and validation of iPSC-based therapies by the FDA and the European Medicines Agency. Although much remains to be understood, the enormous potential of iPSCs for treating cartilage degeneration merits future studies to address these uncertainties.
Fresh and particulated allograftsAside from cell-based methods, fresh osteochondral allo-grafts, as well as particulated cartilage allografts, have been used to fill cartilage defects and promote regenera-tion (Figure 3e). An advantage of using allograft tissues is that they are not regulated by the FDA, and thus bypass costly and time-consuming clinical trials. Fresh osteo-chondral allograft transplantation has had positive clini-cal benefits for young, active individuals. Clinical results have found that these grafts last 1–25 years, depending on graft chondrocyte viability and mechanical stability of the host–graft interface; when such criteria were met, histological evaluation consistently detected hyaline repair tissue.85
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 11 | JANUARY 2015 | 29
Particulated cartilage allografts, on the other hand, are the focus of fewer scientific publications. These grafts are formed by combining particulated cartilage with a fibrin glue to form a construct that is then placed into the cartilage defect. Limited autodigestion of the ECM releases superficial chondrocytes, which produce addi-tional ECM that integrate the cartilage particles, filling the defect. Clinical experience with this technique is limited to short-term (2–year follow-up) studies, most of which are case reports and case series demonstrat-ing feasibility, safety and efficacy, with improvements in subjective patient clinical scores and MRI evidence of good defect filling.86,87 An alternative approach to intro-ducing autologous cartilage fragments into the cartilage defect utilizes a scaffold-based technique. Specifically, in a single surgery, hyaline cartilage is arthroscopically harvested from a low load-bearing region of the joint, mechanically minced and then glued onto a synthetic, absorbable scaffold before transplantation into the car-tilage defect. In a prospective clinical safety study, this novel autologous scaffold-based allograft procedure was compared with microfracture; clinical and imaging results showed the scaffold-based approach resulted in better functional outcomes, better cartilage develop-ment and fewer adverse events.88 A larger prospective controlled study investigating the mechanical integrity of neotissue formed with this technique, by quantita-tive MRI techniques and second-look arthroscopy, was stopped by the sponsor due to the difficulty in adhering to strict FDA inclusion criteria.89 Future studies should correlate structural changes (as measured by quanti-tative MRI techniques or established morphological methods) with either clinician-based evaluation scales or patient-reported outcome as sessment tools.
Novel cell-free biomaterialsAlthough autologous chondrocytes and MSC-based techniques offer much promise for articular cartilage repair, methods for extracting, proliferating and differ-entiating cells are both timely and costly. Furthermore, because MACI-based and hyaluronic-acid-scaffold-based techniques are cellular, the FDA might consider them both as a medical device and as biological, resulting in long and expensive regulatory approval. These regula-tory advantages thereby enhance interest in these cell-free material-based products for cartilage regeneration and repair.
AMICAutologous matrix-induced chondrogenesis (AMIC) is a cell-free technique that can be performed in a single surgery (Figure 3c). To perform AMIC, a mini- arthrotomy exposes and cleans the defect site, then microfracture releases both blood and bone marrow containing MSCs, and finally a mixed collagen type I and type III matrix is sutured or glued into the cartilage defect.90 The implanted collagen matrix is thought to sta-bilize the resulting blood clot, helping to promote early mechanical stability and cartilage regeneration. Case series have found AMIC to be both safe and effective
in treating full-thickness cartilage defects.91–94 In one study, patients followed-up for as long as 5 years had substantial improvements in Tegner, Lysholm, ICRS, and Cincinatti scores (Box 1) as early as 12 months after surgery.93 Furthermore, MRI revealed moderate-to-complete filling of all chondral defects. In another AMIC study, a biphasic osteochondral biodegradable scaffold consisting of calcium triphosphate in the osseous region and poly(lactic-co-glycolic acid) in the cartilaginous region was used to treat full-thickness ankle cartilage defects.94 At a 1 year follow-up, American Orthopaedic Foot & Ankle Society and Ankle Osteoarthritis Scale clinical scores (Box 1) were increased in all six patients compared with preoperative values. Interestingly, the observed clinical outcomes in AMIC-treated patients did not correlate with age, BMI or the number of previ-ous orthopaedic operations of these patients. The small number of cases in these studies, the short follow-up and not having control groups might explain the lack of such correlations. The simplicity and cost-effectiveness of AMIC merits further studies to identify the quality of neocartilage formation, the reproducibility of the data and any potential pitfalls associated with the technique.
Active in situ approachesA novel approach to enhance cartilage repair with AMIC is to deliver growth factors that selectively recruit and stimulate MSCs from the subchondral bone marrow into cell-free scaffolds. Such growth factors can be tai-lored to also activate chondrocytes in the surrounding healthy tissue to help remodel the repair tissue filling the c artilage defect.
Implanting polymer-based materials combined with autologous serum or platelet-rich plasma and hyaluro-nic acid after initial microfracture of a defect has been proposed as a novel strategy for active in situ AMIC.95 Autologous serum and platelet-rich plasma can recruit bone marrow MSCs from the underlying subchondral bone,96 and hyaluronic acid might help the bone marrow MSCs differentiate into a chondrocytic phenotype.97 A clinical trial found 52 patients receiving this treat-ment had improved patient-reported Knee injury and Osteoarthritis Outcome Scores (KOOS) 1 year after surgery, compared with their preoperative status (Box 1), and defects were shown, by histological analysis, to be filled with a hyaline-like repair tissue.98 However, con-trolled trials with a longer follow-up period are needed to confirm these data and prove that the neotissue is dura ble. In another method, chitosan in a glycerol phos-phate buffer is mixed with freshly drawn autologous whole blood to form a clot.99 A multicentre, random-ized comparative clinical trial found that 1 year after operation a combined treatment of chitosan–glycerol phosphate and microfracture resulted in greater lesion filling and a su perior quality of repair tissue than micro-fracture alone.100 However, no significant differences in the functional outcomes were detected between the groups at follow-up. Given that fibrocartilage formed after microfracture starts to deteriorate as soon as 2 years after surgery,4 longer follow-up studies of the functional
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

30 | JANUARY 2015 | VOLUME 11 www.nature.com/nrrheum
outcomes are needed to investigate the potential benefits of these active in situ AMIC techniques.
Knowledge of the dose dependence and tissue specificity of MSC chemoattractants, including bone morphogenetic
proteins, whole blood serum, chemokines and platelet-rich plasma could be used as part of an active in situ AMIC cartilage repair strategy.101,102 Potentially, these treatments could be tailored for a specific condition and anato-mical location. Although most of these treatments are FDA-approved and are immediately available for clinical application, well-designed preclinical studies followed by controlled clinical trials are first needed to investigate their effectiveness. Additionally, growth factors belonging to the TGF-β superfamily, as well as insulin-like growth factors, platelet-derived growth factors and pro-epidermal growth factor, have been shown to enhance stem cell chemotactic migration.103 Methods could therefore be developed to combine both growth factors and MSC chemoattractants to further promote cartilage regeneration by tailoring their release in a controlled manner, for example on the surface of matrices or within nanoparticles.104
Scaffold-free approachesSelf-assembling processAlthough several tissue engineering approaches for car-tilage repair forgo the use of either cells or exogenous stimulation, another option is a self-assembling process that requires no scaffold (Figure 3f).105 Without a scaffold to interrupt cell–cell signalling and stress shielding, the neotissue microenvironment might be more bioactive, enhancing the response to stimulation and integration with surrounding tissue (Box 2). Ex vivo studies found that stimulation of self-assembled articular cartilage with exogenous (hypoxia, growth factors, crosslinking agents) and biomechanical (hydrostatic pressure) stimulation pro-motes the development of robust neotissue with similar functional properties as native cartilage.106–108 These studies also found that scaffold-free neotissue is capable of both integration and in vivo maturation.109 When compared with scaffold-based techniques, the scaffold-free neotissue had superior mechanical properties and a higher percentage of ECM.110 Thus, scaffold-free neo-tissue is a promising new development in the generation of highly bioactive implants to enhance cartilage repair.
ChondrospheresAnother scaffold-free technology for articular cartilage regeneration is based on generating spheroids of autolo-gous chondrocytes (chondrospheres) for implantation (Figure 3f). In a minipig cartilage defect model, these spheroids adhered and integrated with full-thickness cartilage defects and produced cartilaginous ECM.111 The clinical efficacy of chondrospheres is currently being investigated in a phase III controlled clinical trial in Europe;112 the preliminary human clinical outcomes have not yet been published. Another scaffold-free technol-ogy is to utilize juvenile allogeneic chondrocytes. These cells have been shown to have a stronger and more stable chondrogenic activity in vitro than human adult cells and can avoid immunological responses and form hyaline-like tissue when grafted into goat cartilage defects.113,114 A phase III clinical trial comparing this technology with microfracture is ongoing; clinical data from this trial are not yet available.
Box 2 | Cell response to mechanical load
Bone and cartilage can adapt to external loads. In bone, this phenomenon is known as Wolff’s Law, the theory that if the tissue is exposed to loading, it will remodel to become stronger and better able to withstand the load. Likewise, when load is taken away, the tissue will become weaker, as it is metabolically ‘taxing’ to maintain a greater tissue mass. Such remodelling occurs at the cellular level via mechanotransductive signalling. A load (or lack of load) will transmit through the matrix of the tissue and convert into a biochemical signal, alerting cells to either produce more, or catabolize existing, extracellular matrix. Cells receive these signals through surface receptors and also alert neighbouring cells. Exogenous materials used in scaffold-based tissue engineering approaches might interrupt the flow of this mechanotransductive signalling cascade, shielding cells from the effects of local stresses and hindering cell–cell signalling. Currently scaffold-free tissue engineering approaches are being developed to help preserve the natural balance between external loading environment and internal tissue architecture.
AutologousAllogeneic
MSCsiPSCs
Biomechanical stimulation
Growth factorsProteinsSerum
ChemokinesPlatelet-rich plasma
SyntheticHydrogel
ECM component ■ Collagen■ GAG
Tissue-derived ■ Decellularized matrix
Scaffold-freeapproaches
■ Articular cartilageself-assembly
■ Chondrospheres
Cells Signals
Scaffolds
MACIEx vivo
3D culture
Cell-freescaffolds■ AMIC
Figure 4 | The tissue engineering paradigm. Cells, signals and scaffolds are the major elements of tissue engineering approaches to cartilage repair. For this purpose, many different cell sources (autologous cells, allogeneic cells or stem cells) have been tested in vitro. Neotissue has been cultured ex vivo with various stimuli and chemicals to enhance synthesis and chondrogenic potential. To further improve the integrity of neotissues, scaffolds have been used to create a 3D environment to maintain the phenotype of cells, carry integrated cells in vivo, and to recruit cells from the host environment. Combinations of these factors drive the three major cartilage engineering strategies that exist: cell-free, scaffold-based implants that promote cell recruitment with chemoattractants; cell-seeded scaffolds that mimic the structure of native tissues; and scaffold-free, cell-based biomimetic techniques. Abbreviations: AMIC, autologous matrix-induced chondrogenesis; ECM, extracellular matrix; GAG, glycosaminoglycans; MACI, matrix-assisted autologous chondrocyte implantation.
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 11 | JANUARY 2015 | 31
ConclusionsThis Review focuses on the basic science, indications, advantages, limitations and outcomes of current and future cartilage regeneration strategies. Emphasis is on tissue engineering approaches because such techniques are the basis for the next generation of cartilage regen-eration technology. Specifically, tissue engineering aims to develop biomimetic tissues that recapitulate the bio-logical, structural and functional features of native carti-lage, increasing the ability of implants to withstand and adapt to the highly loaded environment of the knee. Such strategies are needed, not only to stop the progression of cartilage degeneration, but also to improve long-term functional outcomes for patients. These novel bio mi-metic solutions might help treat an increasing number of individuals with cartilage pathology, as well as limit the e conomic burden.
Despite the efforts discussed, the generation of truly biomimetic chondral and osteochondral replacements is elusive; however, technological development in many areas is rapid (Figure 4). For example, tissue engineer-ing approaches using a variety of cell sources, including autologous, allogeneic, xenogeneic and stem cells, have yielded repair tissues with hyaline-like characteristics, thereby decreasing pain and in many cases delaying joint degeneration. Although a ‘gold standard’ cell source has yet to be identified, stem cells stand out in terms of their availability and minimization or lack of donor morbid-ity. Furthermore, the combination of tissue engineering with both biochemical and biomechanical exogenous stimulation has resulted in repair tissues with even better hyaline-like properties. Tissue-engineered, cell-free scaf-folds, as well as cell-based, scaffold-free approaches offer even further hope for the treatment of cartilage repair.
Overall, a technology has yet to be developed that satis-fies the fundamental requirements of successful cartilage healing, namely, one that embodies the appropriate struc-ture–function relationship, ECM organization, bioactivity and surgical logistics. To address these criteria, work must be done to improve not only the mechanical properties of the tissue, but also to shape and organize neotissue development so that it better mimics native morpho-genesis. Furthermore, emphasis must be placed on the degradation characteristics of scaffold-based approaches to ensure degradation rates match tissue regeneration. In cell-based applications, a thorough understanding of how to maintain the chondrocytic phenotype of autologous and allogeneic chondrocytes, and how to foster complete chondrogenic differentiation of stem cells, must be estab-lished. Once technologies are able to pass these criteria,
stringent manufacturing methods that ensure reproduci-bility of the resulting implants and long-term functional clinical outcomes in humans will need to be developed. Standardization of the approval process should also be streamlined across countries; current practices in Europe allow faster translation of promising technologies than the FDA.
Crucial to these endeavours is the development of better animal models of cartilage damage for in vivo test ing prior to clinical application in well-designed, pro spective, random ized controlled clinical trials. Further more, such clinical studies should compare novel technologies to current ‘gold standard’ clinical approaches. The result-ing repair tissue must also be subjected to rigorous bio-chemical and biomechanical evaluation to deter mine how similar the regenerative tissue is to native tissue. What quantifies a robust, hyaline-like repair tissue, and what threshold of such quantifiable characteristics is neces sary for successful clinical outcomes must be clearly determined. Use of noninvasive, quantitative measures both before and after surgery is important to understand long-term clinical trial outcomes. Such information will be critical to determine which technologies result in regenerative tissue that truly recreates the st ructure–function relationship of healthy, native articular carti lage. Equally important, measures should be taken to deter-mine the appropriate indications, contraindications, patient selection criteria, surgical practices and reha-bilitation protocols for each technology. Importantly, the necessity of minimizing health-care costs must also be seriously considered. All-in-all, much work is required to develop truly bio mimetic cartilage regenerative therapies, but we are closer than ever to making such a concept a clinical reality.
Review criteria
We searched for original articles focusing on cartilage repair and regeneration in MEDLINE, PubMed, Embase and the Cochrane Controlled Trials Register, published 2000–2014. The search terms alone and in combination were “cartilage repair”, “cartilage regeneration”, “cartilage randomized controlled trials”, “cartilage cohorts”, “cartilage systematic reviews”, “cartilage scaffolds”, “engineered cartilage”, “chondrocyte tissue engineering”, “stem cells and chondrocyte” and “chondrocyte and growth factors”. Preliminary searches were undertaken in March 2014 and were updated in May 2014. All publications identified were English-language, full-text papers. We also searched the reference lists of identified articles for additional publications.
1. Lories, R. J. & Luyten, F. P. The bone–cartilage unit in osteoarthritis. Nat. Rev. Rheumatol. 7, 43–49 (2011).
2. Moran, C. J. et al. Restoration of articular cartilage. J. Bone Joint Surg. Am. 96, 336–344 (2014).
3. Bae, D. K., Yoon, K. H. & Song, S. J. Cartilage healing after microfracture in osteoarthritic knees. Arthroscopy 22, 367–374 (2006).
4. Kreuz, P. C. et al. Results after microfracture of full-thickness chondral defects in different
compartments in the knee. Osteoarthritis Cartilage 14, 1119–1125 (2006).
5. Mithoefer, K., McAdams, T., Williams, R. J., Kreuz, P. C. & Mandelbaum, B. R. Clinical efficacy of the microfracture technique for articular cartilage repair in the knee: an evidence-based systematic analysis. Am. J. Sports Med. 37, 2053–2063 (2009).
6. Minas, T., Gomoll, A. H., Rosenberger, R., Royce, R. O. & Bryant, T. Increased failure rate of autologous chondrocyte implantation after
previous treatment with marrow stimulation techniques. Am. J. Sports Med. 37, 902–908 (2009).
7. Pestka, J. M., Bode, G., Salzmann, G., Südkamp, N. P. & Niemeyer, P. Clinical outcome of autologous chondrocyte implantation for failed microfracture treatment of full-thickness cartilage defects of the knee joint. Am. J. Sports Med. 40, 325–331 (2011).
8. Goyal, D. et al. Evidence-based status of microfracture technique: a systematic review
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

32 | JANUARY 2015 | VOLUME 11 www.nature.com/nrrheum
of level I and II studies. Arthroscopy 29, 1579–1588 (2013).
9. Gudas, R. et al. Comparison of osteochondral autologous transplantation, microfracture, or debridement techniques in articular cartilage lesions associated with anterior cruciate ligament injury: a prospective study with a 3-year follow-up. Arthroscopy 29, 89–97 (2013).
10. Gomoll, A. H. Microfracture and augments. J. Knee Surg. 25, 9–15 (2012).
11. Saris, D. B. et al. Treatment of symptomatic cartilage defects of the knee: characterized chondrocyte implantation results in better clinical outcome at 36 months in a randomized trial compared to microfracture. Am. J. Sports Med. 37 (Suppl. 1), 10S–19S (2009).
12. Saris, D. B. et al. Characterized chondrocyte implantation results in better structural repair when treating symptomatic cartilage defects of the knee in a randomized controlled trial versus microfracture. Am. J. Sports Med. 36, 235–246 (2008).
13. Peterson, L., Vasiliadis, H. S., Brittberg, M. & Lindahl, A. Autologous chondrocyte implantation: a long-term follow-up. Am. J. Sports Med. 38, 1117–1124 (2010).
14. Minas, T., Von Keudell, A., Bryant, T. & Gomoll, A. H. The John Insall Award: a minimum 10-year outcome study of autologous chondrocyte implantation. Clin. Orthop. Relat. Res. 472, 41–51 (2014).
15. Behery, O. A., Harris, J. D., Karnes, J. M., Siston, R. A. & Flanigan, D. C. Factors influencing the outcome of autologous chondrocyte implantation: a systematic review. J. Knee Surg. 26, 203–211 (2013).
16. Filardo, G., Kon, E., Di Martino, A., Iacono, F. & Marcacci, M. Arthroscopic second-generation autologous chondrocyte implantation: a prospective 7-year follow-up study. Am. J. Sports Med. 39, 2153–2160 (2011).
17. Macmull, S. et al. Autologous chondrocyte implantation in the adolescent knee. Am. J. Sports Med. 39, 1723–1730 (2011).
18. Trinh, T. Q., Harris, J. D., Siston, R. A. & Flanigan, D. C. Improved outcomes with combined autologous chondrocyte implantation and patellofemoral osteotomy versus isolated autologous chondrocyte implantation. Arthroscopy 29, 566–574 (2013).
19. Bentley, G. et al. Minimum ten-year results of a prospective randomised study of autologous chondrocyte implantation versus mosaicplasty for symptomatic articular cartilage lesions of the knee. J. Bone Joint Surg. Br. 94, 504–509 (2012).
20. Basad, E., Ishaque, B., Bachmann, G., Stürz, H. & Steinmeyer, J. Matrix-induced autologous chondrocyte implantation versus microfracture in the treatment of cartilage defects of the knee: a 2-year randomised study. Knee Surg. Sports Traumatol. Arthrosc. 18, 519–527 (2010).
21. Saris, D. et al. Matrix-applied characterized autologous cultured chondrocytes versus microfracture: two-year follow-up of a prospective randomized trial. Am. J. Sports Med. (2014).
22. Van Assche, D. et al. Autologous chondrocyte implantation versus microfracture for knee cartilage injury: a prospective randomized trial, with 2-year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 18, 486–495 (2010).
23. Knutsen, G. et al. A randomized trial comparing autologous chondrocyte implantation with microfracture. Findings at five years. J. Bone Joint Surg. Am. 89, 2105–2112 (2007).
24. Peterson, L. et al. Two- to 9-year outcome after autologous chondrocyte transplantation of the knee. Clin. Orthop. Relat. Res. 374, 212–234 (2000).
25. Gooding, C. R. et al. A prospective, randomised study comparing two techniques of autologous chondrocyte implantation for osteochondral defects in the knee: Periosteum covered versus type I/III collagen covered. Knee 13, 203–210 (2006).
26. Gomoll, A. H., Probst, C., Farr, J., Cole, B. J. & Minas, T. Use of a type I/III bilayer collagen membrane decreases reoperation rates for symptomatic hypertrophy after autologous chondrocyte implantation. Am. J. Sports Med. 37 (Suppl. 1), 20S–23S (2009).
27. Marcacci, M. et al. Articular cartilage engineering with Hyalograft C: 3-year clinical results. Clin. Orthop. Relat. Res. 435, 96–105 (2005).
28. Darling, E. M. & Athanasiou, K. A. Rapid phenotypic changes in passaged articular chondrocyte subpopulations. J. Orthop. Res. 23, 425–432 (2005).
29. Martinez, I., Elvenes, J., Olsen, R., Bertheussen, K. & Johansen, O. Redifferentiation of in vitro expanded adult articular chondrocytes by combining the hanging-drop cultivation method with hypoxic environment. Cell Transplant. 17, 987–996 (2008).
30. Grigolo, B. et al. Evidence for redifferentiation of human chondrocytes grown on a hyaluronan-based biomaterial (HYAff 11): molecular, immunohistochemical and ultrastructural analysis. Biomaterials 23, 1187–1195 (2002).
31. Caron, M. M. et al. Redifferentiation of dedifferentiated human articular chondrocytes: comparison of 2D and 3D cultures. Osteoarthritis Cartilage 20, 1170–1178 (2012).
32. Marlovits, S. et al. Clinical and radiological outcomes 5 years after matrix-induced autologous chondrocyte implantation in patients with symptomatic, traumatic chondral defects. Am. J. Sports Med. 40, 2273–2280 (2012).
33. Zheng, M. H. et al. Matrix-induced autologous chondrocyte implantation (MACI): biological and histological assessment. Tissue Eng. 13, 737–746 (2007).
34. Bartlett, W. et al. Autologous chondrocyte implantation versus matrix-induced autologous chondrocyte implantation for osteochondral defects of the knee: a prospective, randomised study. J. Bone Joint Surg. Br. 87, 640–645 (2005).
35. Zeifang, F. et al. Autologous chondrocyte implantation using the original periosteum-cover technique versus matrix-associated autologous chondrocyte implantation: a randomized clinical trial. Am. J. Sports Med. 38, 924–933 (2010).
36. Bian, L. et al. Enhanced MSC chondrogenesis following delivery of TGF-β3 from alginate microspheres within hyaluronic acid hydrogels in vitro and in vivo. Biomaterials 32, 6425–6434 (2011).
37. Chung, C., Beecham, M., Mauck, R. L. & Burdick, J. A. The influence of degradation characteristics of hyaluronic acid hydrogels on in vitro neocartilage formation by mesenchymal stem cells. Biomaterials 30, 4287–4296 (2009).
38. Kon, E. et al. Articular cartilage treatment in high-level male soccer players: a prospective comparative study of arthroscopic second-generation autologous chondrocyte implantation versus microfracture. Am. J. Sports Med. 39, 2549–2557 (2011).
39. Horák, M. et al. Comparison of the cellular composition of two different chondrocyte- seeded biomaterials and the results of their
transplantation in humans. Folia Biol. (Praha) 60, 1–9 (2014).
40. Tatsumura, M., Sakane, M., Ochiai, N. & Mizuno, S. Off-loading of cyclic hydrostatic pressure promotes production of extracellular matrix by chondrocytes. Cells Tissues Organs 198, 405–413 (2014).
41. Jeon, J. E., Schrobback, K., Hutmacher, D. W. & Klein, T. J. Dynamic compression improves biosynthesis of human zonal chondrocytes from osteoarthritis patients. Osteoarthritis Cartilage 20, 906–915 (2012).
42. Lee, C. H. et al. Regeneration of the articular surface of the rabbit synovial joint by cell homing: a proof of concept study. Lancet 376, 440–448 (2010).
43. Khan, I. M., Gilbert, S. J., Singhrao, S. K., Duance, V. C. & Archer, C. W. Cartilage integration: evaluation of the reasons for failure of integration during cartilage repair. A review. Eur. Cell. Mater. 16, 26–39 (2008).
44. Harrington, I. J. A bioengineering analysis of force actions at the knee in normal and pathological gait. Biomed. Eng. 11, 167–172 (1976).
45. Appelman, T. P., Mizrahi, J., Elisseeff, J. H. & Seliktar, D. The influence of biological motifs and dynamic mechanical stimulation in hydrogel scaffold systems on the phenotype of chondrocytes. Biomaterials 32, 1508–1516 (2011).
46. Ringe, J., Burmester, G. R. & Sittinger, M. Regenerative medicine in rheumatic disease-progress in tissue engineering. Nat. Rev. Rheumatol. 8, 493–498 (2012).
47. O’Conor, C. J., Leddy, H. A., Benefield, H. C., Liedtke, W. B. & Guilak, F. TRPV4-mediated mechanotransduction regulates the metabolic response of chondrocytes to dynamic loading. Proc. Natl Acad. Sci. USA 111, 1316–1321 (2014).
48. Crawford, D. C., Heveran, C. M., Cannon, W. D. Jr, Foo, L. F. & Potter, H. G. An autologous cartilage tissue implant NeoCart for treatment of grade III chondral injury to the distal femur: prospective clinical safety trial at 2 years. Am. J. Sports Med. 37, 1334–1343 (2009).
49. Crawford, D. C., DeBerardino, T. M. & Williams, R. J. 3rd. NeoCart, an autologous cartilage tissue implant, compared with microfracture for treatment of distal femoral cartilage lesions: an FDA phase-II prospective, randomized clinical trial after two years. J. Bone Joint Surg. Am. 94, 979–989 (2012).
50. de Vries-van Melle, M. L. et al. Chondrogenic differentiation of human bone marrow-derived mesenchymal stem cells in a simulated osteochondral environment is hydrogel dependent. Eur. Cell. Mater. 27, 112–123; discussion 123 (2014).
51. Ko, J. Y., Kim, K. I., Park, S. & Im, G. I. In vitro chondrogenesis and in vivo repair of osteochondral defect with human induced pluripotent stem cells. Biomaterials 35, 3571–3581 (2014).
52. Wakitani, S. et al. Human autologous culture expanded bone marrow mesenchymal cell transplantation for repair of cartilage defects in osteoarthritic knees. Osteoarthritis Cartilage 10, 199–206 (2002).
53. Nejadnik, H., Hui, J. H., Feng Choong, E. P., Tai, B. C. & Lee, E. H. Autologous bone marrow-derived mesenchymal stem cells versus autologous chondrocyte implantation: an observational cohort study. Am. J. Sports Med. 38, 1110–1116 (2010).
54. Quarto, R. et al. Repair of large bone defects with the use of autologous bone marrow
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

NATURE REVIEWS | RHEUMATOLOGY VOLUME 11 | JANUARY 2015 | 33
stromal cells. N. Engl. J. Med. 344, 385–386 (2001).
55. Kafienah, W. et al. Three-dimensional cartilage tissue engineering using adult stem cells from osteoarthritis patients. Arthritis Rheum. 56, 177–187 (2007).
56. Ringe, J. & Sittinger, M. Tissue engineering in the rheumatic diseases. Arthritis Res. Ther. 11, 211 (2009).
57. Krampera, M. et al. Role for interferon-γ in the immunomodulatory activity of human bone marrow mesenchymal stem cells. Stem Cells 24, 386–398 (2006).
58. Singer, N. G. & Caplan, A. I. Mesenchymal stem cells: mechanisms of inflammation. Annu. Rev. Pathol. 6, 457–478 (2011).
59. Liechty, K. W. et al. Human mesenchymal stem cells engraft and demonstrate site-specific differentiation after in utero transplantation in sheep. Nat. Med. 6, 1282–1286 (2000).
60. Wu, L., Prins, H. J., Helder, M. N., van Blitterswijk, C. A. & Karperien, M. Trophic effects of mesenchymal stem cells in chondrocyte co-cultures are independent of culture conditions and cell sources. Tissue Eng. Part A 18, 1542–1551 (2012).
61. Caplan, A. I. Adult mesenchymal stem cells for tissue engineering versus regenerative medicine. J. Cell Physiol. 213, 341–347 (2007).
62. Davatchi, F., Abdollahi, B. S., Mohyeddin, M., Shahram, F. & Nikbin, B. Mesenchymal stem cell therapy for knee osteoarthritis. Preliminary report of four patients. Int. J. Rheum. Dis. 14, 211–215 (2011).
63. Centeno, C. J. et al. Increased knee cartilage volume in degenerative joint disease using percutaneously implanted, autologous mesenchymal stem cells. Pain Physician 11, 343–353 (2008).
64. Emadedin, M. et al. Intra-articular injection of autologous mesenchymal stem cells in six patients with knee osteoarthritis. Arch. Iran. Med. 15, 422–428 (2012).
65. Wong, K. L. et al. Injectable cultured bone marrow-derived mesenchymal stem cells in varus knees with cartilage defects undergoing high tibial osteotomy: a prospective, randomized controlled clinical trial with 2 years’ follow-up. Arthroscopy 29, 2020–2028 (2013).
66. Kuroda, R. et al. Treatment of a full-thickness articular cartilage defect in the femoral condyle of an athlete with autologous bone-marrow stromal cells. Osteoarthritis Cartilage 15, 226–231 (2007).
67. Wakitani, S. et al. Autologous bone marrow stromal cell transplantation for repair of full-thickness articular cartilage defects in human patellae: two case reports. Cell Transplant. 13, 595–600 (2004).
68. Mohal, J. S., Tailor, H. D. & Khan, W. S. Sources of adult mesenchymal stem cells and their applicability for musculoskeletal applications. Curr. Stem Cell Res. Ther. 7, 103–109 (2012).
69. Mehlhorn, A. T. et al. Differential effects of BMP-2 and TGF-β1 on chondrogenic differentiation of adipose derived stem cells. Cell Prolif. 40, 809–823 (2007).
70. Wang, Y. H. et al. Characterization and evaluation of the differentiation ability of human adipose-derived stem cells growing in scaffold-free suspension culture. Cytotherapy 16, 485–495 (2014).
71. Manferdini, C. et al. Adipose-derived mesenchymal stem cells exert antiinflammatory effects on chondrocytes and synoviocytes from osteoarthritis patients through prostaglandin E2. Arthritis Rheum. 65, 1271–1281 (2013).
72. Parker, A. M. & Katz, A. J. Adipose-derived stem cells for the regeneration of damaged tissues. Expert Opin. Biol. Ther. 6, 567–578 (2006).
73. Koh, Y. G., Choi, Y. J., Kwon, S. K., Kim, Y. S. & Yeo, J. E. Clinical results and second-look arthroscopic findings after treatment with adipose-derived stem cells for knee osteoarthritis. Knee Surg. Sports Traumatol. Arthrosc. http:// dx.doi.org/10.1007/s00167-013-2807-2.
74. Fu, W. L. et al. Repair of large full-thickness cartilage defect by activating endogenous peripheral blood stem cells and autologous periosteum flap transplantation combined with patellofemoral realignment. Knee 21, 609–612 (2014).
75. Turajane, T. et al. Combination of intra-articular autologous activated peripheral blood stem cells with growth factor addition/ preservation and hyaluronic acid in conjunction with arthroscopic microdrilling mesenchymal cell stimulation Improves quality of life and regenerates articular cartilage in early osteoarthritic knee disease. J. Med. Assoc. Thai. 96, 580–588 (2013).
76. Saw, K. Y. et al. Articular cartilage regeneration with autologous peripheral blood progenitor cells and hyaluronic acid after arthroscopic subchondral drilling: a report of 5 cases with histology. Arthroscopy 27, 493–506 (2011).
77. Saw, K. Y. et al. Articular cartilage regeneration with autologous peripheral blood stem cells versus hyaluronic acid: a randomized controlled trial. Arthroscopy 29, 684–694 (2013).
78. Mendelson, A. et al. Chondrogenesis by chemotactic homing of synovium, bone marrow, and adipose stem cells in vitro. FASEB J. 25, 3496–3504 (2011).
79. Sakaguchi, Y., Sekiya, I., Yagishita, K. & Muneta, T. Comparison of human stem cells derived from various mesenchymal tissues: superiority of synovium as a cell source. Arthritis Rheum. 52, 2521–2529 (2005).
80. Shao, Z. et al. Surface modification on polycaprolactone electrospun mesh and human decalcified bone scaffold with synovium-derived mesenchymal stem cells-affinity peptide for tissue engineering. J. Biomed. Mater. Res. A http://dx.doi.org/doi:10.1002/jbm.a.35177.
81. Sanchez-Adams, J. & Athanasiou, K. A. Dermis isolated adult stem cells for cartilage tissue engineering. Biomaterials 33, 109–119 (2012).
82. Diekman, B. O. et al. Cartilage tissue engineering using differentiated and purified induced pluripotent stem cells. Proc. Natl Acad. Sci. USA 109, 19172–19177 (2012).
83. Park, S. & Im, G. I. Embryonic stem cells and induced pluripotent stem cells for skeletal regeneration. Tissue Eng. Part B Rev. http://dx.doi.org/10.1089/ten.teb.2013.0530.
84. Kim, M. J. et al. Generation of human induced pluripotent stem cells from osteoarthritis patient-derived synovial cells. Arthritis Rheum. 63, 3010–3021 (2011).
85. Gross, A. E. et al. Fresh osteochondral allografts for posttraumatic knee defects: long-term followup. Clin. Orthop. Relat. Res. 466, 1863–1870 (2008).
86. Bonner, K. F., Daner, W. & Yao, J. Q. 2-year postoperative evaluation of a patient with a symptomatic full-thickness patellar cartilage defect repaired with particulated juvenile cartilage tissue. J. Knee Surg. 23, 109–114 (2010).
87. Farr, J., Cole, B. J., Sherman, S. & Karas, V. Particulated articular cartilage: CAIS and DeNovo NT. J. Knee Surg. 25, 23–29 (2012).
88. Cole, B. J. et al. Outcomes after a single-stage procedure for cell-based cartilage repair:
a prospective clinical safety trial with 2-year follow-up. Am. J. Sports Med. 39, 1170–1179 (2011).
89. US National Library of Medicine. ClinicalTrials.gov [online], http://clinicaltrials.gov/ct2/show/NCT00881023 (2014).
90. Benthien, J. P. & Behrens, P. The treatment of chondral and osteochondral defects of the knee with autologous matrix-induced chondrogenesis (AMIC): method description and recent developments. Knee Surg. Sports Traumatol. Arthrosc. 19, 1316–1319 (2011).
91. Kusano, T. et al. Treatment of isolated chondral and osteochondral defects in the knee by autologous matrix-induced chondrogenesis (AMIC). Knee Surg. Sports Traumatol. Arthrosc. 20, 2109–2115 (2012).
92. Gille, J. et al. Outcome of Autologous Matrix Induced Chondrogenesis (AMIC) in cartilage knee surgery: data of the AMIC Registry. Arch. Orthop. Trauma Surg. 133, 87–93 (2013).
93. Gille, J. et al. Mid-term results of Autologous matrix-Induced Chondrogenesis for treatment of focal cartilage defects in the knee. Knee Surg. Sports Traumatol. Arthrosc. 18, 1456–1464 (2010).
94. Pearce, C. J., Gartner, L. E., Mitchell, A. & Calder, J. D. Synthetic osteochondral grafting of ankle osteochondral lesions. Foot Ankle Surg. 18, 114–118 (2012).
95. Patrascu, J. M., Freymann, U., Kaps, C. & Poenaru, D. V. Repair of a post-traumatic cartilage defect with a cell-free polymer-based cartilage implant: a follow-up at two years by MRI and histological review. J. Bone Joint Surg. Br. 92, 1160–1163 (2010).
96. Patel, S., Dhillon, M. S., Aggarwal, S., Marwaha, N. & Jain, A. Treatment with platelet-rich plasma is more effective than placebo for knee osteoarthritis: a prospective, double-blind, randomized trial. Am. J. Sports Med. 41, 356–364 (2013).
97. Patrascu, J. M. et al. Polyglycolic acid-hyaluronan scaffolds loaded with bone marrow-derived mesenchymal stem cells show chondrogenic differentiation in vitro and cartilage repair in the rabbit model. J. Biomed. Mater. Res. B Appl. Biomater. 101, 1310–1320 (2013).
98. Siclari, A., Mascaro, G., Gentili, C., Cancedda, R. & Boux, E. A cell-free scaffold-based cartilage repair provides improved function hyaline-like repair at one year. Clin. Orthop. Relat. Res. 470, 910–919 (2012).
99. Buschmann, M. D., Hoemann, C. D., Hurtig, M. B. & Shive, M. S. in Cartilage Repair Strategies Vol. 1 Ch. 7 (ed. Williams, R. J.) 85–104 (Humana Press, 2007).
100. Stanish, W. D. et al. Novel scaffold-based BST-CarGel treatment results in superior cartilage repair compared with microfracture in a randomized controlled trial. J. Bone Joint Surg. Am. 95, 1640–1650 (2013).
101. Richter, W. Mesenchymal stem cells and cartilage in situ regeneration. J. Intern. Med. 266, 390–405 (2009).
102. Filardo, G. et al. Platelet-rich plasma vs hyaluronic acid to treat knee degenerative pathology: study design and preliminary results of a randomized controlled trial. BMC Musculoskelet. Disord. 13, 229 (2012).
103. Ponte, A. L. et al. The in vitro migration capacity of human bone marrow mesenchymal stem cells: comparison of chemokine and growth factor chemotactic activities. Stem Cells 25, 1737–1745 (2007).
104. Lim, S. M. et al. Dual growth factor-releasing nanoparticle/hydrogel system for cartilage
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved

34 | JANUARY 2015 | VOLUME 11 www.nature.com/nrrheum
tissue engineering. J. Mater. Sci. Mater. Med. 21, 2593–2600 (2010).
105. Huey, D. J., Hu, J. C. & Athanasiou, K. A. Unlike bone, cartilage regeneration remains elusive. Science 338, 917–921 (2012).
106. Makris, E. A., Hu, J. C. & Athanasiou, K. A. Hypoxia-induced collagen crosslinking as a mechanism for enhancing mechanical properties of engineered articular cartilage. Osteoarthritis Cartilage 21, 634–641 (2013).
107. Makris, E. A., MacBarb, R. F., Responte, D. J., Hu, J. C. & Athanasiou, K. A. A copper sulfate and hydroxylysine treatment regimen for enhancing collagen cross-linking and biomechanical properties in engineered neocartilage. FASEB J. 27, 2421–2430 (2013).
108. Gunja, N. J., Uthamanthil, R. K. & Athanasiou, K. A. Effects of TGF-β1 and hydrostatic pressure on meniscus cell-seeded scaffolds. Biomaterials 30, 565–573 (2009).
109. Makris, E. A., MacBarb, R. F., Paschos, N. K., Hu, J. C. & Athanasiou, K. A. Combined use of chondroitinase-ABC, TGF-β1, and collagen crosslinking agent lysyl oxidase to engineer functional neotissues for fibrocartilage repair. Biomaterials 35, 6787–6796 (2014).
110. Aufderheide, A. C. & Athanasiou, K. A. Assessment of a bovine co-culture, scaffold-free method for growing meniscus-shaped constructs. Tissue Eng. 13, 2195–2205 (2007).
111. Meyer, U. et al. Cartilage defect regeneration by ex vivo engineered autologous microtissue —preliminary results. In Vivo 26, 251–257 (2012).
112. US National Library of Medicine. ClinicalTrials.gov [online], http://clinicaltrials.gov/show/NCT01222559 (2014).
113. Adkisson, H. D. et al. The potential of human allogeneic juvenile chondrocytes for restoration of articular cartilage. Am. J. Sports Med. 38, 1324–1333 (2010).
114. Vanlauwe, J. et al. Five-year outcome of characterized chondrocyte implantation versus microfracture for symptomatic cartilage defects of the knee: early treatment matters. Am. J. Sports Med. 39, 2566–2574 (2011).
115. Cole, B. J., Pascual-Garrido, C. & Grumet, R. C. Surgical management of articular cartilage defects in the knee. J. Bone Joint Surg. Am. 91, 1778–1790 (2009).
AcknowledgementsThe authors acknowledge funding from NIH R01 AR061496, NIH R01 DE019666, NIH R01 DE015038, and the California Institute for Regenerative Medicine (CIRM) TR3-05709.
Author contributionsAll authors contributed equally to researching data for the article, substantially contributing to discussion of content, writing and review/editing of the manuscript before submission.
REVIEWS
© 2015 Macmillan Publishers Limited. All rights reserved