Embed Size (px)
Citation preview

RENAL VENOUS THROMBOSIS IN THE NEWBORNBY
MARGARET L. FALLON, M.B., Ch.B.(From the Birmingham Children's Hospital)
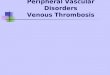
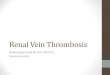
Thrombosis of the renal vein was first describedby Rayer in 1837. This was followed in 1877 byHutinel's account of forty-two cases of renalthrombosis, in thirty of which the condition wasbilateral. Abeshouse (1945), in reviewing 228 casesof renal thrombosis of all varieties, found ninety-eight of these in children less than a year old, andof this total ninety occurred in infants during thefirst two months of life. Barenburg et al. (1941)reported five cases in a series of twenty-fivenecropsies carried out on infants with gastro-enteritis-a figure which suggests a rather bighincidence in this selected group of cases. At theBirmingham Children's Hospital over a period offive years and out of a total of 1,430 routine post-mortem examinations, six instances of renalhaemorrhagic infarction were found. In four ofthese cases the main renal trunk was thrombosed.In the remaining two cases the thrombosis wasconfined to the interlobular veins and was thereforedetected only on microscopic examination (figs. Iand 3). A survey of the literature was made byMorison in 1945, with particular reference to renalthrombosis and infarction in the newborn, and heincludes a description of a series of fatal cases.
Renal thrombosis may be primary, that is, thethrombotic process originates within the renalvenous system; or secondary, resulting fromextension of a thrombus along the vena cava ortributaries of the renal vein. This latter variety israre in childhood. Sandblom (1948) has further sub-divided the cases arising during the neonatal period.
1. A primary, rare form with no obvious etiolcgy,and predominating urinary symptoms.
2. The usual variety encountered in infancy,which is secondary to infection with dehydraticn,and in which the urinary chapges are minimal.Ante-mortem diagncsis cf the condition is rare,
due probably to the rapid dissolution which almostinvariably follows the onset of symptoms. A caseof unilateral thrombosis, of his first type, wasdescribed by Sandblom (1948), in which nephrectomyappeared to be a life-saving measure in a five-day-oldinfant. Campbell and Matthews (1942) hadpreviously described two similar cases with recovery
following nephrectomy. One of these was unique inthat a correct pre-operative diagnosis was made.So far as can be ascertained, there is no authentic
account in the literature of survival followingbilateral renal venous thrombosis. Such a case ishere recorded, with the notes of two fatal cases.
Case RecordsCase 1. W.K., a full-term male infant, weight
7 lb. 4 oz., was delivered with forceps on March 24,1948. He made good progress until the twelfthday, when he became drowsy, fed reluctantly, anddeveloped diarrhoea. His condition deterioratedrapidly during the next four days, the diarrhoeaincreased, and all feeds were refused during thetwenty-four hours before his admission to hospitalon April 9, 1948. He was by now extremelycollapsed, the temperature being 100- F., thepulse 160, and respiration 40 per minute. Hisweight had fallen to 5 lb. 7 oz.; the features weresunken; the colour was ashen, and the extremitieswere cyanosed; the fontanelle was depressed;respirations were shallow and distressed. Pusdischarged from a forceps wound over the rightparietal region. No enlargement of the abdomenwas detected. The child was put into an oxygen tentand intravenous administration of plasma and salinewas begun. Penicillin was given intramuscularly atthree-hourly intervals. Oral fluids were withheldduring the first two days.
Progress. No urine was passed until eighteenhours after admission, when a few cubic centimetresof almost pure blood was collected. The respira-tions became laboured; both kidneys were nowconsiderably enlarged, the left kidney more than theright. During the following forty-eight hours thecondition deteriorated. The stools became wateryand offensive, numbering between eight and tena day. Gross haematuria persisted. The size ofthe kidneys by this time had increased even moreand the abdomen had become distended. On thefourth day after admission the respiratory rate roseto 65 a minute and there was marked dyspnoea,presumably related to the uraemia, since the bloodurea had reached the high level of 329 mg. per100 ml.By the seventh day the scalp infection had
resolved and the urine was macroscopically clear.The blood urea level had fallen to 292 mg. per
125 9
copyright. on F
ebruary 5, 2020 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.24.118.125 on 1 June 1949. Dow
nloaded from

ARCHIVES OF DISEASE IN CHILDHOOD
100 ml. Weak breast milk feeds, an ounce at atime, were now tolerated. The diarrhoea improvedgradually but the condition of the child remainedcritical until towards the end of the second week.Then definite improvement set in. He gainedweight; the stools became normal, and the size ofthe kidneys decreased. The blood urea fell to62 mg. per 100 ml. By the end of the third weekthe left kidney was still somewhat enlarged but theright was no longer palpable. The urine was nowmicroscopically clear. He was discharged fromhospital six weeks after admission in good generalcondition. The left kidney was still palpable. Theurine was clear and the blood urea was 52 mg. per100 ml. Weight on discharge was 7 lb. 4 oz.His condition was reviewed at the age of four
months. Intravenous pyelography showed a normalpelvic shadow with normal excretion on both sides.The blood urea level was then 41 mg. per 100 ml.,and clinical examination was negative.
DIAGNOSIS. Although post-mortem examinationor laparotomy are the only means of establishingan absolute diagnosis, a clinical diagnosis ofbilateral renal thrombosis mav reasonably beaccepted in this case on the following grounds:
1. The occurrence of frank haematuria in theabsence of urinary infection. The urine remainedsterile and free from pus throughout the acutephase of the illness. The haematuria persisted untilthe end of the third week in spite of adequate dosagewith vitamin K at the onset. A diagnosis ofhaemorrhagic disease of the newborn could thereforebe excluded. It has been shown that infants withrenal haemorrhage resulting from birth injuryinvariably succumb within the first twenty-four hoursof life (Cruikshank, 1930).
2. Gross enlargement of the kidneys with theirsubsequent return to normal size. This, along withintravenous pyelography at a later date, eliminatedthe possibility of a congenital condition.
3. The high degree of renal insufficiencyindicated by the uraemia.Two outstanding features of the case described
are: first, the remarkably high blood urea levelattained; secondly, the return of the kidneys toapparently normal function within a few weeks,following such gross enlargement with almostcomplete suppression of function. So complete wasthe recovery that it seams probable that bothrecanalization of the thrombi within the renal veinor its tributaries, together with the development ofa collateral circulation from the extrarenal veins,were the factors responsible.
This case is unusual in that it had the presentingsigns and symptoms of both groups described bySandblom.
Case 2. A male infant was admitted to hospitalon the twelfth day with a history of failure to gainweight since birth and gastro-enteritis of twenty-fourhours' duration. He was semi-comatose. The urine
contained a moderate amount of albumin. Theprothrombin time was 30 seconds (control18 seconds). Death occurred three days later.Autopsy revealed an enlarged right kidney which
was grossly congested. The right renal vein wasdistended and contained a recent thrombus whichfilled the whole renal vein and extended into theinferior vena cava. The lungs showed patchyconsolidation. Both middle ears contained pus.
Case 3. A female infant aged four weeks becamefretful and sleepless on the day before admission.The stools were watery. The child succumbed thefollowing day. Post-mortem examination showed ahaemorrhagic infarction of the whole right kidneyand of the lower pole of the left kidney. Recentthrombi were present in both main renal veinsand in the longitudinal sinus.
Case 4. A prematurely born female infant wasadmitted to hospital on the first day of life. Thebirth weight was 2 lb. 7 oz. The general conditionwas feeble, and there was respiratory distress.Death occurred eighteen hours after delivery. Atautopsy the lungs were found to be almost com-pletely airless. There were numerous asphyxialsubepicardial haemorrhages. The heart and greatvessels were normal. The liver was grossly con-gested. Both kidneys showed areas of earlyhaemorrhagic infarctions, 2 to 5 mm. in diameter.There were multiple subarachnoid haemorrhagesover the cerebellum. The cerebral venous sinuseswere normal.
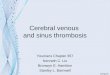
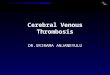
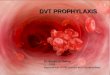
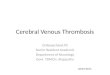
HISToLoGY. The medulla showed gross conges-tion but no necrosis. In the cortex there were areasof haemorrhagic infarction. In some places therenal parenchyma was completely replaced by redcells and numerous white blood cells. In otherareas there was only disintegration of the tubularepithelium, the first convoluted tubules being moreaffected than the convoluted and Henle loops. Theglomeruli were better preserved than the tubules(fig. 2). In several places thrombosis of the smallveins was seen. Some were completely obstructed.In others a layer of hyalinized platelet thrombus wasseen lining the wall of the vein (fig. 3).
EtiologySepsis and dehydration were the probable
precipitating factors in the first and second casesdescribed. In the third case dehydration was theonly cause of thrombosis. Focal infection has beenshown to be a frequent accompaniment of renalthrombosis, and in Case 1 the scalp infection maywell have given rise to bacteraemia or septicaemia.The occurrence of dehydration, in conjunction withthe normal relatively low venous pressure in thenewborn, predisposes to thrombosis and accountsin part for the high incidence of the condition duringthe neonatal period.Case 4 is unusual in that both infection and
dehydration were absent. The thrombosis in thisinstance was presumably caused by the asphyxiated
126copyright.
on February 5, 2020 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.24.118.125 on 1 June 1949. D
ownloaded from

RENAL VENOUS THROMBOSIS IN THE NEWBORN
FiG. I -Thrombosis ofrenal vein in one ofsix cases discussed.x 120.
FIG. 2.-Ha1morrhagicinfarctio of realcortex in Case 4.x 120.
127copyright.
on February 5, 2020 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.24.118.125 on 1 June 1949. D
ownloaded from

128 ARCHIVES OF DISEASE IN CHILDHOOD
condition of the infant, which resulted in generalvenous congestion with stagnation. This etiologycontrasts with cases hitherto described. Cruikshank(1930) in an analysis of eight hundred neonataldeaths, was unable to demonstrate any relationshipbetween maturity, birth asphyxia, or marasmus andrenal (as opposed to intracranial) thromboses.Toxaemia per se has not been proved to play any
significant part in the process.
TreabnentIt is of interest that in Campbell's two cases
treated surgically the prothrombin level, pre-operatively, was well below the average normal lowlevel at that period of life. He advocates theadministration of vitamin K in such cases. InCase 2, referred to earlier by the author, the pro-thrombin time was found, forty-eight bours beforedeath, to be 30 seconds, a figure which may also beregarded as low, especially in view of the fact that10 ml. ofwhole blood had been given intramuscularlyon the day before admission to hospital.As pointed out earlier, vitamin K did not influence
the haematuria in Case I here reported. It ispossible that the raising of the protbrombin level
FE4r,0 ~~O
lb ~ ~ t
FIG. 3.-Earlyvthrombosis ofa small renal vein in Case 4. x 480.
may, in fact, increase the risk of an extendingthrombosis. It would seem reasonable, therefore,to avoid the use of vitamin K in any case of renalthrombosis which is to be treated medically, unlessthe child shows a general haemorrhagic tendency.
Since the diagnosis of renal thrombosis is usuallyretrospective, there has been no opportunity forobserving the effect of the anti-coagulant drugs.The place of surgery in the treatment of renal
thrombosis requires further consideration. Marshalland Whapham (1936) describe a case conforming toSandblom's first group, in which the thrombosis isbilateral, and many similar cases are to be found inthe literature. When a decision is made to removea kidney in which thrombosis is suspected, a graverisk is being taken, since the possibility of a throm-botic process already having started in the otherkidney is considerable. Unless there is a suppura-tive condition within the affected kidney it is difficultto foresee that nephrectomy, during the acute phase,will be of any benefit.The criterion for surgery would appear to be,
therefore, a heavily infected urine in a case ofunilateral thrombosis.The treatment of renal venous thrombosis may
be summarized as follows:1. Surgical treatment: nephrectomy is of value
in certain selected cases of unilateral thrombosis.2. Medical treatment: this should be directed
towards (a) the relief of dehydration; (b) treatmentof co-existing focal infection; (c) the prevention ortreatment of urinary infection.
The literature concerning renal thrombosis isbriefly reviewed.A case of bilateral thrombosis with recovery is
described in detail. Three fatal cases are described,including one of interlobular thrombosis due toneonatal asphyxia. The diagnosis, etiology, andtreatment of the condition are discussed.
I wish to thank Dr. Frances Braid for her helpfuladvice and criticism in the preparation of this paper,Professor A. V. Neale for permission to include twoof the cases, and Dr. H. S. Baar for post-mortemdetails, histology, and microphotographs.
REFERENCESAbeshouse, B. S. (1945). Urol. Cutan. Rev., 49, 661.Barenburg, L. H., Greenstein, N. M., Levy, W., and
Rosenbluth, S. B. (1941). Amer. J. Dis. Child.,62, 362.
Campbell, M. F., and Matthews, W. F. (1942). 1.Paediat., 20, 604.
Cruikshank, J. N. (1930). No. 145. Spec. Rep. Ser.,med. Res. Coun., London.
Hutinel, V. (1877). Thesis. Paris. No. 230.Marshall, S., and Whapham, E. (1936). Lancet. 2, 428.Morison, J. E. (1945). Arch. Dis. Childh., 20, 129.Rayer, P. (183741). Traite des Maladies des Reins,
Paris, 2, 268: 3, 590.Sandblom, P. H. (1948). Acta paediatr. Stockh., 35,
160.
copyright. on F
ebruary 5, 2020 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.24.118.125 on 1 June 1949. Dow
nloaded from