-
8/18/2019 RENAL US
1/76
Diana Pancu, MD
RENAL ULTRASOUND
-
8/18/2019 RENAL US
2/76
Right: with biopsy needleLeft: prostate showing a hypoechoic
Lesion suspicious for cancer
-
8/18/2019 RENAL US
3/76
-
8/18/2019 RENAL US
4/76
Objectives
• Clinical indications for performing ED renal !
• "pproach to performing the ! study• #ormal anatomy
• "bnormal findings
• Clinical $mpact
-
8/18/2019 RENAL US
5/76
Clinical Indications for ED
Renal Ultrasound
• Suspected renal colic
% Colic&y flan& pain radiating to
groin % 'ematuria
• Clinical question
% Presence of hydronephrosis % "bsence of
other pathology (""")
-
8/18/2019 RENAL US
6/76
!erfor"in# t$e Stud%
• Patient preparation:
% none
• *ransducer: +-M'. or +/ M'.
% /- M'. for thin patient
• Patient positioning
% !upine
% Posterior obli0ue, lateral decubitus, prone
-
8/18/2019 RENAL US
7/76
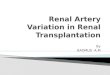
Anato"%
• 1idneys are retroperitoneal, *23 4 L5
• Right &idney is lower than the left &idney
• Right &idney is posterio4inferior to li6er 7
gallbladder
• Left &idney is inferior4medial to the spleen
• "drenal glands are superior, anterior,
medial to each &idney
-
8/18/2019 RENAL US
8/76
$ 8 C
" 9
R * "
Celiac
ais
!M"
Renal artery
Renal 6ein
&epatic
'eins
Right&idney
Left
&idney
Liver
!pleen
-
8/18/2019 RENAL US
9/76
Renal Scannin# Approac$es
-
8/18/2019 RENAL US
10/76
Approac$ to Scannin#
• Right &idney scanningapproach: anterior,
lateral, posterior
• Li6er is the acoustic
window
• Left &idney: re0uires a posterior
approach, through the spleen
• "ir4filled bowel impedes
anterior scanning
$
LI'ER STO(AC&
S ! L E E N
I'C
AORTA) )
S
-
8/18/2019 RENAL US
11/76
Anato"%
• ;423 cm long, 54/ cm wide, +45 cm thic& •
-
8/18/2019 RENAL US
12/76
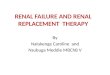
R enal arter%
Renal vein
Ureter
Renal capsule Corte*
(edullar% p%ra"ids
(inor
Cal%*
)idne% Anato"%
(edulla
Sinus
(ajor
Cal%*
-
8/18/2019 RENAL US
13/76
Sono#rap$ic Appearance
• reters are normally not seen
• Renal pel6is is blac& when 6isible
• Renal sinus is echogenic due to fat
• Medullary pyramids are hypoechoic
• Corte is mid4gray, less echogenic thanli6er or spleen
• Capsule is smooth and echogenic
-
8/18/2019 RENAL US
14/76
Ri#$t )idne% Lon# A*is
-
8/18/2019 RENAL US
15/76
Li6er
Diaphragm
!inus
Corte
Anterior
!osterior
Superior Inferior
Ri#$t )idne% Lon# A*is
-
8/18/2019 RENAL US
16/76
Ri#$t )idne% S$ort A*is
-
8/18/2019 RENAL US
17/76
Ri#$t )idne% S$ort A*is
8ertebral
?ody
R 1idney
"ortaRenal a
-
8/18/2019 RENAL US
18/76
Left )idne% Lon# A*is
-
8/18/2019 RENAL US
19/76
Left )idne% Lon# A*is
Anterior
!osterior
Superior Inferior
!pleen
1idney
Rib
S$ado+
-
8/18/2019 RENAL US
20/76
Left )idne% S$ort A*is
-
8/18/2019 RENAL US
21/76
Left )idne% S$ort A*is
Anterior
!osterior
Ri#$t LeftLi6er
!pleen
L 1idney
-
8/18/2019 RENAL US
22/76
Co""on !itfalls in
Renal Scannin#
• @ailure to scan both &idneys
• Mista&ing prominent renal pyramids forhydronephrosis
• Mista&ing prominent pyramids for cysts
• Confusing normal renal arteries for the
ureter
-
8/18/2019 RENAL US
23/76
Co""on !itfalls in
Renal Scannin#
• @ailure to scan through the bladder to search
for stone at the uretero46esicular >unction
• $nability to 6isuali.e left &idney due to
anterior probe placement• @ailure to scan the aorta in suspected
renal
colic
-
8/18/2019 RENAL US
24/76
Nor"al 'ariants
• Dro"edar% $u"ps
% Lateral &idney bulge, same echogenicity as the
corte
• &%pertrop$ied colu"n of ,ertin
% Cortical tissue indents the renal sinus
• Double collectin# s%ste"
% !inus di6ided by a hypertrophied column of
?ertin
• &orses$oe -idne%
% 1idneys are connected, usually at the lower
pole
• Renal ectopia
% 9ne or both &idneys outside the normal renal
fossa
-
8/18/2019 RENAL US
25/76
Clinical Indications
./ Obstructive Uropat$%
-
8/18/2019 RENAL US
26/76
Nep$rolit$iasis
• 23A of the ! population
• $ncidence of renal colic is +A with /-Arecurrence within 2-
years
– Manthey DE. Emerg Med Clin North Am.2001;19(3):
633-54
-
8/18/2019 RENAL US
27/76
Radio#rap$ic (odalities
Radio#rap$%
• B3A !ensiti6ity, BA !pecificity
% !harma R#, !hah $,
-
8/18/2019 RENAL US
28/76
Radio#rap$ic (odalities
I'! vs/ US
• Prospecti6e study, / patients
% !inclair D, Filson !, *oi ", et al "nn Emerg
Med 2://B4//;, 2;;
ULTRASOUND
Sensitivity=85%Specifcity=92%
IVPSensitivity=90%Specifcity=94%
-
8/18/2019 RENAL US
29/76
Radio#rap$ic (odalities
ED Ultrasound 0 )U, vs/ I'!
• Prospecti6e study, 2- patients
Sensitivity = 97%Specifcity = 59%
'enderson, !, et al: Acad Emerg Med 2;;G/:BBB4B2
Sensitivity = 97%Specifcity = 59%
PPV = 81% NPV = 92%
-
8/18/2019 RENAL US
30/76
Radio#rap$ic (odalities
&elical CT1 2old Standard
• "ccurate, fast, no contrast• $dentifies presence and
si3e of stone
• Location of stone• Le6el of obstruction
• 9ther sources of pain
-
8/18/2019 RENAL US
31/76
Stone on CT
• sually 6isuali.ed
• #ot 6isuali.ed
% !tone is etremely small H 2 mm
% !tone is of relati6ely low C* attenuation:
$ndina6ir stones
% !tone ecluded from imaging due to
respiratory6ariation
-
8/18/2019 RENAL US
32/76
&elical CT
Secondar% 4indin#sSensitivit%• reteral dilatation ;-A
• Perinephric stranding 3A• Collecting system
dilatation +A
• Renal enlargement 2A
Specificit%• reral dilatation ;+A
• Perinephric stranding ;+A• Collecting system
dilatation ;5A
• Renal enlargement ;A
!mith "R "m Roentgenol 2B:22-;4222+, 2;;B
-
8/18/2019 RENAL US
33/76
Location of Stone
• + patients
• Rate of spontaneous stone passage• 33A for proimal ureteral
stones
• 5BA for midureteral stones
• 2A for distal ureteral stones
% Morse R J Urol 2;;2G 25/:3B+43B/
-
8/18/2019 RENAL US
34/76
5idt$ of Stone
• /3- patients
• Rate of spontaneous stone passage % 2--A for stones
that were 2 mm or smaller in width
% ;-A for stones 3 to + mm
% -A for stones that were 5 mm
% //A for stones that were / mm
% +/A for stones that were B mm % 3/A for
stones that were mm
% 23A for stones that were mm• eno " rology 2;G
2-:/554/5B
-
8/18/2019 RENAL US
35/76
Radio#rap$ic (odalities
Ultrasound•
@ast• Can identify other causes of pain
• !afe in pregnant patients, children
-
8/18/2019 RENAL US
36/76
&%dronep$rosis
Dilatation of the urinary tract at any le6el
secondary to intrinsic and or etrinsic
obstruction to urine flow
-
8/18/2019 RENAL US
37/76
&%dronep$rosis
• Intrinsic6 acquired % Renal lit$iasis
% #eoplasm (renal, ureteral, bladder)
% Papillary necrosis
% reterocele
% ?lood clot
% #eurogenic bladder
% "nticholinergics
% Pregnancy, P$D, uterine prolapse)
% Diuretics
% 8esico4ureteral reflu
% Diabetes insipidus
• Intrinsic6 con#enital
% !tenosis (ureteral,
urethral, meatal)
% "dynamic ureter
% !pinal cord defects
% Duplication of the
ureter
% reterocele
-
8/18/2019 RENAL US
38/76
&%dronep$rosis in Renal Colic
!mith "R "m Roentgenol 2;;BG 2B:22-;4222+
Sensitivity = 90%
Specifcity = 93%
PPV = 92%
NPV = 90%
Dalrymple rol 2;;G 2/;:+/45-
Sensitivity = 87%
Specifcity = 90%
PPV = 90%
NPV = 89%
-
8/18/2019 RENAL US
39/76
Obstructive Uropat$%
2radin# S%ste" 1 Subjective• Mild
% Minimal separation of calyces
• Moderate % Dilation of ma>or and minor calyceal
system
• Severe % Mar&ed dilation of the renal pel6is and
thinningof the renal parenchyma
-
8/18/2019 RENAL US
40/76
Ran#e of &%dronep$rosis
Nor"al (ild (oderate Severe
-
8/18/2019 RENAL US
41/76
(ild &%dronep$rosis
)idne% Liver
2,
-
8/18/2019 RENAL US
42/76
(oderate 1 Severe
&%dronep$rosis
Liver
)idne%
Dilated pelvis
2,
-
8/18/2019 RENAL US
43/76
Renal !at$olo#%
./ Renal C%sts
-
8/18/2019 RENAL US
44/76
Renal C%sts
• "rise in the renal corte, commonly single rather
than multiple
• Cysts do not communicateG hydronephrosis does
• !hape is round or o6al
• Echo free
• !harp interface between the mass and renal tissue
• Large renal cysts may be mista&en for aortic
aneurysms
-
8/18/2019 RENAL US
45/76
Renal C%sts
Li6er
1idney
Cyst
!catter 3-
?owel
-
8/18/2019 RENAL US
46/76
!roble"s 7 !itfalls
• Mista&ing cysts for hydronephrosis
• Mista&ing cysts for aortic aneurysm
-
8/18/2019 RENAL US
47/76
Case !resentation
• 5- yo male presents with complaints of
recent se6ere headaches, diaphoresis,
and palpitations
• PE anious male
% ?P 32-I23- 'R 25/ RR 2 * ;; % Physical
eam otherwise normal
-
8/18/2019 RENAL US
48/76
Ultrasound of )idne%s
Li6er
Diaphragm
1idney
(ass
Rib
S$ado+
-
8/18/2019 RENAL US
49/76
Case Develop"ent
• *he patient was managed with alpha and
beta4adrenergic bloc&ing agents
• rine studies re6ealed ele6atedmetanepherine and catecholamine
le6els
• *he patient was diagnosed with
pheochromocytoma
-
8/18/2019 RENAL US
50/76
8/ Renal (asses
Renal !at$olo#%
-
8/18/2019 RENAL US
51/76
Renal (asses
• ltrasound 6isuali.es most solid and cystic renal masses
• ?eyond scope of EM ultrasound
• "ppearance
% $rregular borders % Poorly defined
interfaces between mass and &idney
• Comple masses
% Comple ultrasonic appearance
% Cysts or solid masses may represent infection or
hemorrhage
% May ha6e fluid le6els
-
8/18/2019 RENAL US
52/76
Case !resentation
• +/ year old male with history of Crohn=s presents
with sudden onset of right flan& pain 'e is
nauseated and has 6omited a few times 'ereports hematuria and
denies fe6er, dysuria,
abdominal pain
-
8/18/2019 RENAL US
53/76
!$%sical E*a"
Joung man in moderate distress from pain
• ?P 23/IB 'R 22- * ;
• Lungs: clear to ascultation• 'eart: *achycardia without
murmur
• "bdomen: soft, non4tender, normal bowel
sounds• ?ac&: right costo46ertebral angle tenderness
on percussion
-
8/18/2019 RENAL US
54/76
Renal Ultrasound
Ri#$t )idne% Left )idne%
-
8/18/2019 RENAL US
55/76
Ultrasound
T$in !arenc$%"a
Dilated Cal%cesDistinct S$ado+
Ec$o#enic
Structure
-
8/18/2019 RENAL US
56/76
CT Results
• ?ilateral !taghorn Calculi
• ?ilateral moderate hydronephrosis
• Right sided + mm stone at the 8
-
8/18/2019 RENAL US
57/76
Su""ar% 7 Ta-e1&o"e !oints
• ! is an ad>unct in the e6aluation of
patients with suspected renal colic % E6aluate
&idneys
% E6aluate aorta
• !can both &idneys
-
8/18/2019 RENAL US
58/76
Renal
ltrasound
!te6e
-
8/18/2019 RENAL US
59/76
RE#"L "#"*9MJ
RENAL
CORTE9
(EDULLA
(A:OR
CAL;CES
RENAL
!EL'IS
RENAL
(EDULLAR;
!;RA(ID
RENAL
CA!SULEURETER
(INOR
CAL;9
RENAL
COLU(N
-
8/18/2019 RENAL US
60/76
RENAL SONO2RA!&;
• !aired retroperitoneal or#ans• Renal sinus1 dense central
ec$oes due to
renal fat
% Contains• Collectin# s%ste" cal%ces6 infundibula6 7
part of
renal pelvis
% bifid s%ste" seen as t+o separate lobulations
• Renal vessels renal $iliu"• L%"p$atics
• 4at
• 4ibrous tissues
-
8/18/2019 RENAL US
61/76
RE#"L !$#!• Central area of the &idney
from the medial border
• ?ounded by fat
% anteriorly and posteriorly byfibrous sheath
&nown as
-
8/18/2019 RENAL US
62/76
RENAL SONO2RA!&;
• Renal parenc$%"a 1 8 parts corte* 7 "edulla %
t$ic-est at t$e renal poles
• Corte* located bet+een capsule 7 "edulla % lo+ level
unifor" ec$oes % less ec$o#enic t$an liver 7
spleen % Colu"ns of ,ertin < colu"ns of cortical
tissue located bet+een p%ra"ids
Kcan enlar#e 7 "i"ic a "ass
K nor"al variant• "edulla
% variable in si3e but avera#e adult -idne% "easures
=1.8 c" in len#t$> ?1@ c" in +idt$> 8/A1?/B c" in
t$ic-ness
% renal volu"e is esti"ated b% +ater displace"ent
• ' < B/?= * len#t$ * +idt$ * anterior posteriordi"ension
-
8/18/2019 RENAL US
63/76
RENAL SONO2RA!&;
•Renal parenc$%"a 1 8 parts corte* 7
"edulla
% (edulla• !%ra"ids 1 trian#ular or rounded
$%poec$oic areas
• Rounded 3ones of decreasedec$o#enicit% bet+een corte* 7renal
sinus
• Specular ec$oes interspersed att$e junction of t$e corte*
7
"edulla represents arcuate
arteries 7 veins C-no+n as
cortico"edullar% junctionD
-
8/18/2019 RENAL US
64/76
RENAL SONO2RA!&;
• 8ascular echange
% renal arteries
• come off of aorta 4 can be multiple• right renal artery (RR")
4 seen posterior to I'C in
sa#ittal plane
% renal 6eins
• come off of $8C
• left renal 6ein (LR8) 4 seen between !M" 7 aorta
in the trans6erse plane
RE#"L "R*ERJ
-
8/18/2019 RENAL US
65/76
-
8/18/2019 RENAL US
66/76
RENAL SONO2RA!&;
• Renal anatomy
% &idney is co6ered by a true capsule
% &idney is surrounded by perinephric
fat % fat is bounded anteriorly 7 posteriorly by
fibrous sheath 4
-
8/18/2019 RENAL US
67/76
LE@* RE#"L "R*ERJ and 8ein
LRA
LR'
RENAL SONO2RA!&;
-
8/18/2019 RENAL US
68/76
RENAL SONO2RA!&;
• Congenital 6ariations
% fetal lobulations
% dromedary hump
% agenesis
% ectopic
• cross4fused ectopic 4 both located on same side and
usually connected
% horseshoe 4 isthmus of tissue that connects
both&idneys
% pel6ic &idney 4 fails to migrate from
pel6ic area
during embryology
-
8/18/2019 RENAL US
69/76
RENAL SONO2RA!&;
• Physiology 4 + functions
% filtration
% reabsorbtion % tubular secretions
• Essential lab 6alues
% ?# 4 ?lood rea #itrogen
% Creatinine
RENAL SONO2RA!&;
-
8/18/2019 RENAL US
70/76
RENAL SONO2RA!&;
• $ndications for sonography eam % hydronephrosis
% non 6isuali.ation on I'! eam
% e6aluation of flan& masses
% a6oidance of contrast agent ("llergy to
$8Pcontrast)
% decreased or poor renal function
% e6aluation of abscess
% e6aluation of renal transplant
% e6aluation of urinary bladder
% hematuria 7 or flan& pain
RENAL SONO2RA!&;
-
8/18/2019 RENAL US
71/76
• $maging techni0ue 4 no prep necessary
% patient position 4 obli0ue 7 decubitus
positions
wor& the best
% LP9 I use li6er for acoustic window for
imaging the right % Rt Lateral ducubitus best position
for left
&idney 4 use spleen
% techni0ue setting• highest fre0uency possible that
allows for proper
penetration
% gain settings are 6itally important
RENAL SONO2RA!&;
-
8/18/2019 RENAL US
72/76
RENAL SONO2RA!&;
• $maging techni0ue 4 Complete study
% must be bilateral 7 include the bladder
% multiple planes including sagittal 7
trans6erse % scan superior to inferior and medial to
lateral to
be assured you scan the entire &idney
% compare cortical density to that of the
li6er % if hydronephrosis 4 try to demonstrate the
ureter
-
8/18/2019 RENAL US
73/76
RENAL SONO2RA!&;
• $maging techni0ue 4 if malignancy is suggested
you must scan 7 sur6ey for in6ol6ement of:
% $8C % Renal 6eins
% Li6er
% Retroperitonium
RENAL SONO2RA!&;
-
8/18/2019 RENAL US
74/76
RENAL SONO2RA!&;
• reters
% arise as budli&e outgrowths from the
mesonephric
or Folffian ducts
% a6erage si.e +- cm long / mm in diameter
% courses retroperitoneal to the bladder
?ladder thin walled, smooth 7 uniform /mm in
diameter
loo& for abnormal densities or interruptions of
the
wall
6olume trans6erse "P length
-
8/18/2019 RENAL US
75/76
"DRE#"L
-
8/18/2019 RENAL US
76/76
"DRE#"L