Embed Size (px)
Citation preview

Capitol University
College of Nursing
Cagayan de Oro City
A Case Study Presented to
Col. Josephine I. Domingo
In Partial Fulfillment of RLE 6 Hospital Rotation
“Renal Stone”
Submitted by:
Catherine P. Galos, Ica Nyll Nashra T. Gamba, Xylas John D. Garcia,
Kristian Paul M. Geromo, Mark Lenndon S. Intong, Maria Angela H. Hinautan,
Farah Jane Y. Hinoyog, Joana Mae T. Labanen, Sidney B. Jadman,
Brian Anthony N. Guylan, Joe Dennis Y. Jamero
January 20, 2010

Table of Contents
I. Introduction…………………………………………………………1
II. Client’s Profile……………………………………………………..3
III. Anatomy and Physiology………………………………………..5
IV. Pathophysiology…………………………………………………..8
V. Laboratory Results……………………………………………….10
VI. Nursing Care plan………………………………………………..13
VII. Drug Study………………………………………………………….14
VIII. Discharge Plan……………………………………………………..15
IX. Learning Experience………………………………………………17
1

I. Introduction
We can say that life is one of the most wonderful gift that God has given to us.
We are being obliged to take good care of it, but in some instance we cannot guarantee
that we can take good care of it. Because of in adequate information, no individual
wants to harm themselves intentionally or unintentionally.
Our kidney is one of the most important part of our study because without it we
can say that an individual will be useless because the kidney act as a filter for blood
making urine and removing waste products from the body. It also helps regulate
electrolyte levels that are important for our body function.
Our patient case is renal stone. A kidney stone is a solid piece of materials that
forms in a kidney out of substances in the urine. A stone may stay in the kidney or break
loose and travel down the urinary tract. A small stone may pass all the way out of the
body without causing too much pain.
A large stone may get stuck in a ureter, the bladder or the urethra. A problem
stone can block the flow of urine and cause great pain.
The kidney acts as a filter for blood, making urine and removing waste products
from the body. It also helps regulate electrolyte levels that are important for body
function. Urine drains from the kidney into the bladder through a narrow tube called the
ureter. When the bladder fills and there is an urge to urinate, the bladder empties
through the urethra, a much wider tube than the ureter.
In some people, chemicals crystallize in the urine and form the beginning or
nidus, of a kidney stone. These stones are very tiny when they form, smaller than a
grain of sand, but gradually can grow over time to a 1/10 of an inch or larger.
Urolithiasis is the term that refers to the presence of stones in the urinary tract, while
nephrolithiasis refers to kidney stones. The size of the stone doesn’t matter as much as
where it is located.
When the stone sits in the kidney, it rarely causes problems, but when it falls into
the ureter, it acts like a dam. As the kidney continues to function and make urine,
pressure builds up behind the stone and causes the kidney to swell. This pressure is
what causes the pain of a kidney stone, but it also helps push the stone along the
course of the ureter. When the stone enters the bladder, the obstruction in the ureter is
relieved and the symptoms of a kidney stone are resolved.
2

There is no consensus as to why kidney stones form but some of the probable
causes are the following: Heredity, some people are more susceptible to forming kidney
stones and heredity may play a role. The majority of kidney stones are made of calcium
and hypercalciura (high levels of calcium in the urine) is a risk factor. The predisposition
to high levels of calcium in the urine may be passed on from generation to generation.
Some rare heredity diseases also predispose some people to form kidney stones.
Examples include people with renal tubular acidosis and people with problems
metabolizing a variety of chemicals including cystine (an amino acids), oxalate (a type
of salt), and uric acid (as in gout).
The group selects this case because we were alarm of the growing number of
patient suffered from this disease. What are the factors that lead to this kind of disease.
We want to gain information so that we could apply this to our field of profession. What
are the accurate nursing skills needed to help the client recover, to get well live in a
healthy lifestyle and more so to gain further information of the disease process.
3

II. Clients Profile
Patient X is a 31 years old Filipino male, married, a Roman Catholic and was
born on December 30, 1978. Patient’s X is a Philippi line Military Army. He is presently
residing at Butuan City. His chief complaint is Right Flank and Hypergastric pain. With
previous hospitalization were polyps both nostrils and other help problem is
hypertension.
Functional Health Patterns
The patient has no history of smoking, only drinking alcohol and cola. He is
allergy of mongo and fish.
Nutritional and Metabolic Patterns
The fluid intake of water is about 6-8 glasses a day. He also eat fruits and
vegetables and with good appetite. There are no food and diet restrictions and there are
no any conditions of difficulty of eating and chewing.
Elimination Pattern
Patient X used to void 3-4 a day with light yellow colored urine and defecate once
a day with brown colored stool and without discomfort.
Activity-Exercise Pattern
Patient X used to exercise like walking and jogging.
Self-Perception and Self Concept Pattern
Patient X feels normal to his self and God fearing.
Role – Relationship Pattern
Patient X is a married man, and lives with his wife and child. His family felt
worried about his condition.
Sexuality – reproductive Pattern
Patients X has no problem with his sexual life and his wife are not using any
contraceptives.
Coping – Stress tolerance Pattern
4

Patient X is taking vitamin such as Enervon C. and, he manage his stress on
sleeping at least 6 hours.
Value – Belief Pattern
Patient X is a roman catholic and he has strong faith and belief to God. He went
to church with his family.
Physical Assessment
Upon assessing patient X has a black complexion, smooth skin, black and thick
hair. With no abnormal conditions on senses.
5

III. Anatomy and Physiology
6

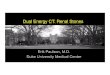
The Human Renal System
The human renal system is made up of two kidneys, two ureters, the urinary
bladder, and the urethra. In addition to the production of urine the renal system has
many other functions.
One quarter to one fifth of cardiac output passes through the kidneys at all times.
This means that the kidneys filter approximately 1.2 liters of blood every minute. It is
therefore not surprising that even slight abnormalities of renal function quickly lead to
electrolyte disturbances. If untreated death will occur.
The Kidneys
The kidneys are two bean shaped organs of the renal system located on the
posterior wall of the abdomen one on each side of the vertebral column at the level of
the twelfth rib. The left kidney is slightly higher than the right. Human kidneys are richly
supplied with blood vessels which give them their reddish brown color. The kidneys
measure about 10cm in length and, 5cm in breadth and about 2.5 cm in thickness.
The kidneys are protected by three highly specialized layers of protective tissues.
The outer layer consists mainly of connective tissue which protects the kidneys from
trauma and infection. This layer is often called the renal fascia or fibrous membrane.
The technical name for this layer is the renal capsule. The next layer (second layer from
the exterior) is called the fascia and it makes a fibrous capsule around the kidneys. This
layer connects the kidneys to the abdominal wall. The inner most layer is made up of
adipose tissue and is essentially a layer of fatty tissue which forms a protective
cushions the kidney; and the renal capsule (fibrous sac) surrounds the kidney and
protects it from trauma and infection.
Causes
Kidney stones are deposits of mineral salts, called calculi, in the kidney. These stones
can pass into the ureter, the narrow tube that connects the kidneys to the bladder. This
can cause Urolithiasis. Urolithiasis refers to the condition of having calculi in the urinary
tract (which also includes the kidneys), which may form or pass into the urinary bladder.

7
What is going on in the body?
Kidney stones occur when the urine has a high level of minerals that form stones. Most
kidney stones are made from calcium. Minerals such as uric acid and oxalate may also
form stones. These stones can irritate kidney tissue and block urine flow. Kidney stones
typically leave the body by passage in the urine stream, and many stones are formed
and passed without causing symptoms. If stones grow to sufficient size before passage
on the order of at least 2-3—millimeters they can cause obstruction of the ureter. The
resulting obstruction causes dilation or stretching of the upper ureter and renal pelvis
(the part of the kidney where the urine collects before entering the ureter) as well as
muscle spasm of the ureter, trying to move the stone. This leads to pain, most
commonly felt in the flank, lower abdomen and groin (a condition called renal colic).
Renal colic can be associated with nausea and vomiting. There can be blood in the
urine, visible with the naked eye or under the microscope (macroscopic or microscopic
hematuria) due to damage to the lining of the urinary tract.
What are the causes and risks of the condition?
Kidney stones are caused by an accumulation of mineral salts, with calcium
being the most common. People with kidney stones may first have dysfunction or
damage to some of the collecting tubes in the kidney. Factors that increase the risk of
stone formation include the following: abnormalities in metabolism of a mineral, such as
uric acid, diet high in a mineral, such as calcium, hereditary factors, inadequate fluid
intake , lack of kidney stone inhibitors, such as magnesium, in the urine, and living in a
hot, dry climate.
What are the signs and symptoms of the condition?
Some stones can grow to be very large without causing symptoms. Flank pain is a
common symptom of kidney stones. Flank pain occurs on one side of the back near the
lower ribs. If stones have passed into the ureter, the person may have groin pain. Pain
may also radiate down the lower side of the abdomen. A kidney stone may cause blood
in the urine, nausea, and vomiting

8
IV Phatophysiology

9

10
V. Laboratory Results and Diagnostic Procedure
The following are the results for the laboratory examination on Complete Blood Count,
Hematology Report, Urinalysis and Fecalysis.
A laboratory test is a medical procedure in which a sample of blood, urine, or
other tissues or substances in the body is checked for certain features. Such tests are
often used as part of a routine checkup to identify possible changes in a person’s health
before any symptoms appear. Laboratory tests also play an important role in diagnosis
when a person has symptoms. In addition, tests may be used to help plan a patient’s
treatment, evaluate the response to treatment, or monitor the course of the disease over
time.
Complete Blood Count
Test Result Reference Value Unit
Hgb 15.0 11.7 – 14.5 g/L
Hct 45.0 34.1 – 44.3 gm%
WBC Count 13,550 5,000 – 10, 000
Platelet Count 204,000 150 000 – 450 000
The differential WBC count (percent of the total contributed by each type of
white cell) is determined by counting the number of each type found in a total of one
hundred cells counted. It also increases in acute infections & trauma, values decrease
in diabetes mellitus, anemias and following cancer chemotherapy.
Hematology Report
Test Result Reference Value Unit
Neutrophils 70 45 – 70 %
Lympocytes 22 18 – 45 %
Eosinophils 06 2 -3 %
Monocytes 02 4- 8 %

11
Neutrophils are the primary white blood cells responsible for fighting infections.
High levels of neutrophils indicate infection. Low levels can indicate sepsis. The
neutrophils are concentrated in the area of infection or are rapidly being used, leaving
less circulating in the blood.
Lymphocyte are also responsible for fighting infection and also develop
antibodies to protect the body against future attacks. High levels of lymphocytes can
indicate infection, viral disease or certain cancers such as lymphosarcom.
Monocytes recognize a variety of microorganisms, especially gram-negative
bacteria. Activated monocytes turn into macrophages that can engulf and destroy
microorganisms and secrete a variety of cytokines that modulate the activity of other
leukocytes.
Eosinophils decrease in steroid therapy, increase in leukemia & parasitic
infection.
URINALYSIS
Color: Yellow
WBC: 0-2/hpf
Transparency: St. Terbid
RBC: plenty/hpf
Sugar and albumin: MG
Specific gravity: 1.025
Med. Tech/ Date of exam: 28Dec’09
Pathologist: Ramon M. Nery, MD
FECALYSIS
Color: brown
Character: Soft
Parasites found: no ova or parasite seen
Med. Tech/ Date of exam: 30 Dec’09
Pathologist: Ramon M. Nery, MD

12
Ultrasound of the KUB
There is no disparity in the size of kidneys. The right measures about 10.3 x 4.7 x
4.6 cms, with cortical thickness of 1.6 cm. While the left measures about 10.9 x 4.7 x
4.2 cms. With cortical thickness of 2.0 cm. There is mild pole measuring about 4.6 mm.
the right ureter is also mildly dilated with two lithiais in the distal portion measuring
about 6.4 mm. The left central echo complex is intact. No mass is seen.
The urinary bladder is unremarkable. The prostrate gland is normal in size
measuring about 2.8 x 4.3 x 30 cms. No focal mass lesion is seen.
Impression:
Nephrolithiasis with mild uretero hydronephrosis due to lithiasis in the distal
ureter, right normal, left kidney, urinary bladder and prostate gland (19.4 g)

13
VI. Nursing Care Plan

14
VII. Drug Study

15
VIII. Health Teachings / Discharge Plan
Methods
Medication:
Explain to the patient the purpose. Schedule dosage
and route of administration of any prescribe drugs, as
well as it’s side effects to report to the physician and
nurse
Economy
Encoraude cleients to increase fluid intake
Advice the patient about the importance of deversional activities
Discuss with client’s belief about health and reasons for not
following prescribed plan of care
Encourage verbalizations of feelings about pain
Treatment
Explain to the patient and his significant others the mode of
treatment/regimen, its purpose and the normal feelings of sensations
that are likely, as well as any procedural care.
Health Teachings
Encourage regular exercise
Increase fluid intake at least 8 – 10 glasses a day
Promote comfortable environment
Instruct patient on how to take care his complain/illness upon onset
of pain to prevent further complications

16
Out Patient Follow-Up
Stress the important for follow up check up upon onset of pain
Provide information about additional learning experience
Diet
Low salt diet
Low fat diet
Spiritual
Stress out the importance of visiting the church, attending mass
praying to nourish not only mind but also the soul

17
IX. Learning Experience
Doing this case study, it has given the group a lot of lessons and a lot of
experiential learning. Lessons gained pointed out the importance of caring for a patient
with different kinds of illnesses specially patients who have renal stone. We’ve also
learned how to handle these situations and interventions and coherent evaluations.
Utmost, learning experiences taught the group the values of discipline, punctuality,
patience, cooperation, perseverance and not to mention the deep interpersonal
bonding that led to trusting relationship towards the group members, to our P.C.I. and
the our C.I. as well.
We would like to take this opportunity to thank all the people involved in progress
and making of this case study. We also want to thank the friendly and ever so helpful
staff of Camp Evangelista Station Hospital; to our PCI for being so good and kind to
help us and of course, our warmest, sincere thanks to our clinical instructor, Col.
Josephine Domingo, RN, for always guiding us to do the right thing to give our best to
serve our patients and their needs. It has been truly a great and educational
experience. A lot has been learned and hoped we still could remember this throughout
the years.
During our first exposure to the Medical and Surgical Ward, it made our
experience productive and wonderful. We were expecting it to be very difficult and
daunting but the people around the area made it easier and fun for us to learn new
things. Making the atmosphere casual but maintaining professionalism made it
conducive to learn, eager as for us.
In the future, it has certainly inspired us to seriously consider specialize
ourselves working in the Camp Evangelista Station Hospital, it is both challenging and
a profound experience consoling with patients through their emotional and physical
needs. Moreover, hearing from registered experienced nurses that it must be a truly
liberating and exhilarating but quite humble to save someone’s life in their most dire
hour of need.