Embed Size (px)
Citation preview

ORIGINAL ARTICLE
Renal replacement therapy in the ICU: comparison of clinicalfeatures and outcomes of patients with acute kidney injuryand dialysis-dependent end-stage renal disease
Turkay Akbas • Sait Karakurt • Serhan Tuglular
Received: 4 December 2013 / Accepted: 31 August 2014
� Japanese Society of Nephrology 2014
Summary
Background The goal of this study is to study clinical
features and outcomes of the patients who had renal
replacement therapy (RRT) in the intensive care unit (ICU)
between 2000 and 2007.
Methods We retrospectively studied 222 patients.
Results Overall ICU mortality and invasive mechanical
ventilation (IMV) rates were 58.1 and 61.3 %. The mean
APACHE II score was 27.6 ± 8.3. Chronic dialysis (CD)
patients formed 45.5 % of the study population. Acute
kidney injury (AKI) patients had higher rates of IMV (73
vs. 51.5 %, p = 0.002), cancer (27.8 vs. 7.9 %, p B 0.001)
and mortality (67.8 vs. 50.5 %, p = 0.010) than CD
patients. AKI patients with normal kidney function (NKF)
before ICU admission had poorer prognosis than acute-on-
chronic kidney disease (CKD) and CD patients (78.6, 51
and 50.5 %, respectively, p B 0.001). Multivariate analysis
showed that IMV (OR, 14.8; 95 % CI, 5.47–40.05;
p B 0.001) and having NKF before hospitalization (OR,
2.8; 95 % CI, 1.04–7.37; p = 0.041) were predictors of
overall ICU mortality. Additionally, IMV is found as a
prognostic factor for both AKI (OR, 18.7; 95 % CI,
4.48–77.72; p B 0.001) and CD patients (OR, 8.14; 95 %
CI, 2.01–33.04; p = 0.003), but APACHE II score is
meaningful only for CD patients (OR, 1.13; 95 % CI,
1.02–1.26; p = 0.024). The areas under the ROC curves
for APACHE II score were 0.52 (95 % CI, 0.39–0.66) for
AKI and 0.78 (95 % CI, 0.55–0.89) for CD patients.
Conclusion The observed ICU mortality among patients
requiring RRT is high and IMV is associated with mor-
tality. AKI patients have increased mortality compared to
CD patients. AKI patients with past NKF have poorer
prognosis than acute-on-CKD and CD patients.
Keywords Acute kidney injury � End-stage kidney
disease � Intensive care unit � Renal replacement therapy
Introduction
Renal replacement therapy (RRT) is a commonly used
therapy modality among critically ill patients. The aim of
dialysis is, except for intoxication and hypervolemia,
generally to support renal function in those patients who
develop acute kidney injury (AKI) during their intensive
care unit (ICU) stay or to do regular dialysis of those
patients on chronic dialysis (CD) programs admitted to the
ICU. End-stage renal disease (ESRD) patients consist of
1.3–5.8 % of all admissions to the ICU [1–4] and it was
displayed that 2–20 % of ESRD patients require ICU
admission every year [3, 5]. The main causes of ICU
admission in ESRD patients are infection, bleeding and
cardiovascular events [1, 5–7]. Mortality rate among these
patients is reported to be between 9 and 54 % [1, 3–10].
AKI occurs in 1–50 % of all critically ill patients,
depending on the population studied and criteria used to
T. Akbas (&)
Department of Internal Medicine and Critical Care Unit, School
of Medicine, Marmara University, Istanbul, Turkey
e-mail: [email protected]
T. Akbas
Fevzi Cakmak Mahallesi, Mimar Sinan Caddesi, No:41 Ust
Kaynarca, Pendik, Istanbul 34899, Turkey
S. Karakurt
Department of Pulmonary and Critical Care Medicine, School of
Medicine, Marmara University, Istanbul, Turkey
S. Tuglular
Department of Nephrology, School of Medicine, Marmara
University, Istanbul, Turkey
123
Clin Exp Nephrol
DOI 10.1007/s10157-014-1028-4

define it [8, 11–13]. The rate of RRT among AKI patients
is reported to be between 11 and 70 % [8, 11, 12, 14, 15].
The main reason for development of AKI is sepsis which is
followed by major surgery [11, 14, 15]. Generally, AKI is a
part of multiorgan failures and shows poor prognosis.
Mortality of AKI ranges from 23 to 64 % [8, 11–15].
In this study, we will first describe demographical and
clinical features of the patients who had RRT during their
ICU stay. Then, we will describe and compare demo-
graphical and clinical characteristics of the CD and AKI
patients, ending with a comparison of the mortality rate
between the two groups.
Materials and methods
The study population consisted of all patients who had any
type of RRT after admission to the medical ICU of Mar-
mara University Hospital between 2000 and 2007. The
university hospital had 280 beds where the medical ICU
occupied 8 beds among a total of 21 adult ICU beds
(medical, anesthesia and coronary ICU). Nearly 12,000
patients/year were admitted to the hospital where around
260 patients/year admitted to the medical ICU during the
study period. The university hospital has an actively
working dialysis unit with 20 beds and works as a reference
hospital for health-related problems of dialysis-dependent
patients. We reviewed the past records of the patients
through the computer database and medical notes of the
ICU and dialysis unit of the hospital. The patients were
admitted to the ICU from the emergency service or other
wards of the hospital except ten patients from the operation
room. Of the ten patients, nine were on CD and eight had
the operation of renal transplantation. In the event of
multiple admissions, only the initial ICU admission was
accepted. Exclusion criterion was being less than 18 years
old. The study was approved by Ethics Committee of
Marmara University (09.2013.0253).
Data elements included demographics, admission diag-
nosis, comorbidity, Acute Physiologic and Chronic Health
Evaluation (APACHE) II score, need of mechanical venti-
lation (MV), presence of organ failure, development of
hypotension during RRT (systolic blood pressure
\90 mmHg after two successive measurements were con-
sidered as hypotension), type of dialysis, length of ICU stay
(LOS), ICU mortality and cause of mortality. The APACHE
II score was calculated by using the worst values within the
first 24 h of admission to the ICU. MV included noninvasive
MV (NIMV) and invasive MV (IMV). Individual organ
failures were defined as the sequential organ failure assess-
ment score C2 points for each system [12].
A diagnosis of infection included admissions for pri-
marily sepsis-related diagnosis. These were lung,
gastrointestinal, urinary tract, central nervous system, soft
tissue, and catheter-related infections. A cardiac diagnosis
encompassed cardiogenic shock, heart failure, acute myo-
cardial infarction, hypervolemia, cardiac arrest, and rhythm
problems. A hepatic diagnosis included admission with
chronic/active hepatic failure. A diagnosis of hemorrhage
described any bleeding. A diagnosis of epilepsy included
status epilepticus and uncontrolled seizures. Vasculitis
comprised patients who had immune suppressive therapy
or plasmapheresis due to vasculitis-related organ failures.
Uremia included those patients who were admitted to the
ICU with acute deterioration of renal function due to any
cause and CD patients who required urgent RRT due to any
reason. COPD exacerbation described patients with COPD
who had MV support because of respiratory failure.
The baseline serum creatinine levels of the patients were
retrieved from the hospital computer database or medical
files 3 months before the ICU admission; otherwise, the
lowest serum creatinine levels during the admission were
considered. Patients’ previous renal functions were cate-
gorized into three groups: patients who had a documented
history of chronic kidney disease (CKD) or whose glo-
merular filtration rates were \60 ml/min, as calculated by
MDRD using baseline serum creatinine levels, were
accepted as patients with CKD stages 2–5 [16]. Develop-
ment of AKI in those patients was named as acute-on-
CKD. Patients being chronically dialysis-dependent prior
to ICU admission were put into CKD stage 5D [16].
Patients who had normal baseline serum creatinine levels
were accepted as patients with normal kidney function
(NKF). Comorbidities were extrapolated from patients’
medical notes.
All patients requiring dialysis in this study were evalu-
ated and managed by the nephrology department of the
hospital. RRT was either intermittent hemodialysis (IHD),
or continuous venovenous hemodialysis (CVVHD), or
peritoneal dialysis (PD). IHD was employed for hemody-
namically stable patients, while CVVHD was used pri-
marily for patients who were hemodynamically unstable.
Some patients received two modalities (IHD-CVVHD or
PD-IHD). In this case, the last modality used was accepted.
Patients who were on PD before ICU admission had PD
unless contraindicated due to peritonitis, catheter-related
problems or other technical problems. Types of dialysis,
number of dialysis sessions and dialysis prescriptions were
arranged based on outpatient therapy and current status of
the patients.
Statistical analysis
Normally distributed continuous variables were analyzed
by the Student’s t or ANOVA tests and results were
expressed as means with standard deviations (SD).
Clin Exp Nephrol
123

Continuous variables without normal distribution (age and
LOS) were reported as medians with interquartile ranges
and compared using the Mann–Whitney U or Kruskal–
Wallis tests. Categorical variables were expressed as pro-
portions and compared with the Chi-square test. Multi-
variate analysis was performed using logistic regression
with mortality as the dependent outcome variable. The
variables yielding p values\0.15 by univariate analysis or
considered clinically important were entered in a backward
multivariate logistic regression, with goodness of fit
determined by the method of Hosmer–Lemeshow. When
the degree of correlation between the variables entered in
the multiple regression equation is high, the regression
model can produce incorrect variance estimates and may
give a misleading interpretation of the model. To address
the problem of multicolinearity, a correlation matrix was
used to asses the overlap between the data. A high spear-
men correlation (r [ 0.5) indicates that the data highly
correlate with each other. One way of mitigating the
harmful effects of multicolinearity is to delete the offend-
ing variables from the regression model [17]. The receiver
operating characteristic (ROC) curve analysis was used to
determine the performance of APACHE II probability of
death. p \ 0.05 was considered as statistically significant.
Results
During the 7-year period, 222 patients (M/F, 113/109;
median age 66 (53–73), range 19–91) had extracorporeal
dialysis support. The baseline characteristics of the patients
are listed in Table 1. The predominant reasons for admis-
sion were infection, cardiac problems and bleeding. The
mean APPACHE II score was 27.6 ± 8.3 and 45.5 % of
the patients were on CD. The rates of NIMV and IMV were
30.4 and 61.3 %, respectively. Organ system failure data
were obtained for 112 patients where 59.8 % of them had
non-renal organ system failures. The data of LOS was
reached in 61 patients and the median LOS was 6 (2–19.5)
days. Thirteen patients (5.8 %) had IHD at first, but then
switched to CVVHD due to hemodynamic instability and
all of them except one died. One septic patient had PD
initially then, followed by IHD because of technical
problems. Renal-transplant patients had RRT because of
allograft nephropathy. The data of blood pressure during
dialysis session was obtained for 45 patients where 44 % of
them experienced hypotension. Overall observed ICU
mortality was 58.1 %. The mean APACHE II score and
rates of CVVHD, IMV, non-renal organ system failure,
AKI, history of chronic liver disease and hypotension
during RRT were significantly high in nonsurvivors
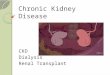
(Table 2). All surgical patients survived. Mortality
increased with the number of organ system failures,
Table 1 Characteristics of 222 patients who had RRT in the ICU
Sex, n (% men) 113 (50.9)
Age, median (25–75 percentiles) 66 (53-73)
Primary diagnosis, n (%)
Infection 94 (42.3)
Cardiac disease 44 (19.8)
Bleeding 22 (9.9)
Uremia 16 (7.1)
Postoperative follow-up 10 (4.5)
Epilepsy 9 (4.1)
Hepatic failure 6 (2.7)
Othersa 21 (9.6)
Comorbidity, n (%)
CVD 113 (50.9)
DM 68 (30.6)
Cancer 40 (18.0)
COPD 19 (8.6)
Liver disease 19 (8.6)
APACHE II, mean (SD) 27.6 (8.3)
IMV, n (%) 136 (61.3)
NIMV, n (%) 67 (30.2)
Type of dialysis, n (%)
IHD 156 (70.3)
CVVHD 53 (23.9)
PD 13 (5.8)
Dialysis indication, n (%)
Regular dialysis 74 (33.3)
Sepsis-related AKI 59 (26.6)
Uremiab 59 (26.6)
Hypervolemia 25 (11.2)
Hyperkalemia 4 (1.8)
Intoxicationc 1 (0.5)
Mortality, n (%) 129 (58.1)
Cause of mortality, n (%)
Sepsis 106 (82.2)
Cardiac disease 13 (10.1)
Liver failure 6 (4.7)
Bleeding 4 (3)
APACHE acute physiologic and chronic health evaluation, CVD
cardiovascular disease, COPD chronic obstructive pulmonary disease,
DM diabetes mellitus, CVVHD continuous venovenous haemodialy-
sis, ICU intensive care unit, IHD intermittent haemodialysis, IMV
invasive mechanical ventilation, NIMV noninvasive mechanical
ventilation, n number, PD peritoneal dialysis, RRT renal replacement
treatment, SD standard deviationa Others include vasculitis (7), COPD exacerbation (7), pancreatitis
(4), intoxication (2) and HELLP syndrome (1)b Uremia describes indication of RRT due to worsening of kidney
function for any reason except for sepsis for AKI patients and defines
urgent dialysis due to any cause except for hyperkalemia for CD
patientsc One CD patient with the diagnosis of intoxication had normal
regular dialysis during ICU stay
Clin Exp Nephrol
123

reaching 88 % after C3 organ system failures (Fig. 1).
Patients with organ failures had high APACHE II scores
(organ failure?, 30.4 ± 8.6; no organ failure, 24.9 ± 8.2;
p = 0.005).
Among 121 patients who had RRT first time in the ICU,
six patients had extracorporeal dialysis support because of
heart failure-related volume overload (5) and intoxication
(1). The remaining 115 (51.8 %) patients were accepted as
AKI. When we compared AKI patients with CD patients,
the rates of respiratory failure, IMV, cancer and mortality
were found to be significantly high in AKI patients
(Table 3). All AKI patients who were admitted to the ICU
with the diagnosis of liver failure except one died. When
the patients were analyzed according to past renal function,
Table 2 Demographic and
clinical characteristics of
survivors and nonsurvivors
Bold values indicate statistically
significant results
AKI acute kidney injury,
APACHE acute physiologic and
chronic health evaluation, CVD
cardiovascular disease, CD
chronic dialysis, COPD chronic
obstructive pulmonary disease,
DM diabetes mellitus, CVVHD
continuous venovenous
haemodialysis, IHD intermittent
haemodialysis, IMV invasive
mechanical ventilation, LOS
length of ICU stay, NIMV
noninvasive mechanical
ventilation, N/A not applicable,
n number, PD peritoneal
dialysis, SD standard deviationa Others include vasculitis (7),
COPD exacerbation (7),
pancreatitis (4), intoxication (2)
and HELLP syndrome (1)b LOS covers 61 patientsc Hypotension during dialysis
session encloses 45 patientsd Non-renal organ failure
covers 112 patientse Uremia describes indication
of RRT due to worsening of
kidney function for any reason
except for sepsis for AKI
patients and defines urgent
dialysis due to any cause except
for hyperkalemia for CD
patientsf One CD patient with the
diagnosis of intoxication had
normal regular dialysis during
ICU stay
Parameters Alive (n = 93) Dead (n = 129) p
Sex, % men 55.9 47.3 0.20
Age, median (25–75 percentiles) 66 (52–73) 66 (56–73) 0.47
APACHE II, mean (SD) 24.9 (7.1) 29.6 (8.7) 0.001
Primary diagnosis (%)
Infection 24.7 55 N/A
Cardiac disease 28 14
Bleeding 14 7
Uremia 9.5 5.3
Postoperative follow-up 10.8 0
Epilepsy 4.3 3.9
Hepatic failure 0 4.7
Othersa 8.7 10.1
Comorbidity (%)
CVD 53.8 48.8 0.46
DM 34.4 27.9 0.30
Cancer 14 20.9 0.18
COPD 4.3 11.6 0.054
Liver disease 1.1 14 <0.001
IMV (%) 24.7 87.6 <0.001
NIMV (%) 28 31.8 0.54
LOS, median (25–75 percentiles)b 5 (3–14) 9 (2–21) 0.56
Hypotension, n (%)c 6 (20.7) 14 (87.5) <0.001
Type of renal disease (%)
AKI 32.2 67.8 0.010
CD 49.5 50.5
Non-renal organ failure, (%)d
Respiratory 31.5 89.1 <0.001
Cardiovascular 20 86.4 <0.001
Haematologic 5.8 49.2 <0.001
Hepatic 5.8 27.4 0.002
Neurologic 3.8 35.5 <0.001
Type of dialysis (%)
IHD 88.2 57.3 <0.001
CVVHD 3.2 38.8
PD 8.6 3.9
Dialysis indication (%)
Regular dialysis 35.5 31.8 N/A
Sepsis-related AKI 4.3 42.6
Uremiae 33.4 21.7
Hypervolemia 22.5 3.1
Hyperkalemia 3.2 0.8
Intoxicationf 1.1 0
Clin Exp Nephrol
123

AKI patients with previous NKF had higher rates of
chronic liver disease, respiratory failure, IMV and mor-
tality than acute-on-CKD and CD patients (Table 4).
The following variables were entered into the backward
logistic regression model: comorbidities, IMV, age, sex,
APACHE II and past kidney function. Hypotension during
RRT and non-renal organ system failure were not put into
the system due to limited number of the patients. No cor-
relation was encountered between variables. The indepen-
dent predictors of overall ICU mortality were IMV [odds
ratio (OR), 14.8; 95 % CI, 5.47–40.05; p B 0.001] and
presence of NKF before ICU admission (OR, 2.8; 95 % CI,
1.04–7.37; p = 0.041; Hosmer–Lemeshow goodness of fit
v2: 10.59, p = 0.226) (Table 5). After analyzing variables
according to AKI and CD, IMV emerged to be a risk factor
of mortality for both AKI (OR, 18.7; 95 % CI, 4.48–77.72;
p B 0.001) and CD patients (OR, 8.14; 95 % CI,
2.01–33.04; p = 0.003; Hosmer–Lemeshow goodness of
fit v2:9.05, p = 0.249), but APACHE II score was impor-
tant only for CD patients (OR, 1.13; 95 % CI, 1.02–1.26;
p = 0.024; Hosmer–Lemeshow goodness of fit v2:10.71;
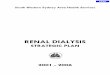
p = 0.218). The areas under the ROC curves for APACHE
II score were 0.78 (95 % CI, 0.55–0.89; p = 0.004) for CD
and 0.52 (95 % CI, 0.39–0.66; p = 0.69) for AKI patients
(Figs. 2, 3).
Discussion
Although APACHE II scores were similar between AKI
and CD patients, more AKI patients died than did CD
patients. The result is similar to other studies which showed
higher mortality for AKI patients than CD patients [1, 7, 8,
18–20]. AKI develops in critically ill patients usually in the
context of multiple organ dysfunctions; it shows the
severity of the disease [1, 15, 21]. The rate of MV is high
among AKI patients and studies reported that respiratory
failure requiring MV is a key risk for mortality in these
patients as demonstrated also in our study [11, 18, 19].
Another reason for having high mortality in our AKI
patients was the inclusion of patients with medical condi-
tions. Mortality rate of patients with AKI in medical
diagnosis was reported higher than surgical diagnosis [14,
19, 20]. These patients are more likely to have severe
diseases and need other organ supports like MV and
vasopressors.
The mortality rate of our dialysis-dependent ESRD
patients was higher than other studies [1, 3–8, 22]. This
could be due to admission of severely ill patients, consid-
ering high rate of IMV and mean APACHE II score in our
patients. The studies that reported high mortality in ESRD
patients had rates of MV higher than 50 % [9, 18]. Addi-
tionally, MV was displayed as a mortality predictor for
ESRD patients [1, 18, 19, 23]. We, as well, displayed that
IMV was associated with an eightfold risk of mortality in
CD patients. The other reason for having high mortality
could be due to inclusion of more patients with medical
reasons. Admission for a medical as opposed to a surgical
reason is associated with a worse outcome among ESRD
patients [4, 9, 10, 20]. It was reported that ICU mortality
rate was 61 % for CD patients admitted for medical rea-
sons in comparison to CD patients admitted for surgical
reasons which had 19 % of mortality [9]. In our study, 9 %
of CD patients were admitted to the ICU after elective
surgeries and none of them died.
In this study, the mortality rate of AKI patients with
NKF before ICU admission was higher than acute-on-CKD
and CD patients. Although APACHE II scores were not
different between these three groups, those with past NFK
had high respiratory failure and IMV rates which actually
show the severity of the disease and impact of respiratory
failure on mortality mentioned above. Any critical illness
severe enough to result in AKI requiring RRT in those
patients with earlier NKF would be associated with par-
ticularly high mortality reported also by Walcher et al.
[18].
In the present study, more than 50 % of AKI patients
had the diagnosis of infection and sepsis was found as a
main cause for mortality. Sepsis, a highly prevalent syn-
drome that prompts admission to ICU, is a leading pre-
cipitant of AKI. Between 50 and 80 % of AKI is
considered associated with sepsis and presence of sepsis is
correlated with the severity of AKI and mortality as also
seen in our study [7, 11, 15, 18]. Infection is also reported
as the principal admission diagnosis and mortality reason
in ESRD patients admitted to ICU [6, 7, 24]. This can be
because of high susceptibility of ESRD patients to infec-
tion due in part to the acquired immune deficiency state of
Fig. 1 The relationship between the number of non-renal organ
system failures and mortality among all patients who had RRT in the
ICU
Clin Exp Nephrol
123

uremia, advanced age, comorbid conditions such as DM,
and frequent and repetitive exposure to potential infectious
risk factors during the normal course of dialysis therapy
[25]. In this study, primary admission and mortality diag-
noses were, as well, infection in CD patients.
When we compared patients according to comorbidities,
cancer was found to be more common in AKI patients.
AKI, frequently seen in critically ill cancer patients,
reported to be between 32 and 54 % [26, 27], and 32 % of
them had RRT during ICU stay [27]. Although mortality in
Table 3 Differences between
AKI and CD patients
Bold values indicate statistically
significant results
AKI acute kidney injury,
APACHE acute physiologic and
chronic health evaluation, CVD
cardiovascular disease, CD
chronic dialysis, COPD chronic
obstructive pulmonary disease,
DM diabetes mellitus, CVVHD
continuous venovenous
haemodialysis, IHD intermittent
haemodialysis, IMV invasive
mechanical ventilation, LOS
length of ICU stay, NIMV
noninvasive mechanical
ventilation, N/A not applicable,
n number, PD peritoneal
dialysis, SD standard deviationa Others include vasculitis (7),
COPD exacerbation (7),
pancreatitis (4), intoxication (1)
and HELLP syndrome (1)b LOS covers 59 patientsc Hypotension during dialysis
session encloses 42 patientsd Non-renal organ system
failure covers 106 patientse Uremia describes indication
of RRT due to worsening of
kidney function for any reason
except for sepsis for AKI
patients and defines urgent
dialysis due to any cause except
for hyperkalemia for CD
patients
Parameters AKI (n = 115) CD (n = 101) p
Sex, % men 53 49.5 0.60
Age, median (25–75 percentiles) 67 (55–74) 65 (53–72) 0.09
APACHE II, mean (SD) 27.8 (7.9) 27.5 (9) 0.50
Admission diagnosis (%)
Infection 54.8 30.7 N/A
Cardiac disease 9.6 27.6
Bleeding 7.8 12.9
Uremia 12.1 2
Postoperative follow-up 0.9 8.9
Epilepsy 0 8.9
Hepatic failure 5.2 0
Othersa 9.6 9
Comorbidity (%)
CVD 48.7 51.5 0.68
DM 31.3 29.7 0.79
Cancer 27.8 7.9 <0.001
COPD 9.6 6.9 0.48
Liver disease 11.3 5.9 0.16
NIMV (%) 32.2 25.7 0.29
IMV (%) 73 51.5 0.002
LOS, median (25–75 percentiles)b 8 (2–21) 4.5 (2–20) 0.65
Hypotension, n (%)c 11 (50) 9 (45) 0.74
Non-renal organ failure, (%)d
Respiratory 55.4 76.5 0.001
Cardiovascular 55.4 61.7 0.49
Haematologic 33.9 26.4 0.39
Hepatic 23.2 13.2 0.17
Neurological 22.2 21.4 0.92
Type of dialysis (%)
IHD 67 72.2 N/A
CVVHD 33 14.9
PD 0 12.9
Dialysis indication (%)
Regular dialysis 0 73.2 N/A
Sepsis-related AKI 50.4 0
Uremiae 40.1 13.9
Hypervolemia 7.8 10.9
Hyperkalemia 1.7 2
Mortality (%) 67.8 50.5 0.010
Cause of mortality (%)
Sepsis 89.8 70.6 N/A
Cardiac disease 1.3 23.5
Liver failure 7.6 0
Bleeding 1.3 5.9
Clin Exp Nephrol
123

cancer patients with AKI requiring RRT was reported
between 64 and 78 % [27, 28], the presence of cancer was
not able to be shown as a prognostic factor [28], except for
uncontrolled cancers [27]. Likewise, we failed to show
cancer as an important mortality predictor in the multi-
variate analysis although it was significant in the univariate
Table 4 Comparison of the
patients according to past
kidney function
Bold values indicate statistically
significant results
APACHE acute physiologic and
chronic health evaluation, CVD
cardiovascular disease, CKD
chronic kidney disease, COPD
chronic obstructive pulmonary
disease, DM diabetes mellitus,
D dialysis, IMV invasive
mechanical ventilation, LOS
length of ICU stay, NIMV
noninvasive mechanical
ventilation, NKF normal kidney
function, N/A not applicable,
n number, SD standard
deviationa LOS covers 59 patientsb Hypotension during dialysis
session includes 42 patientsc Non-renal organ system
failure encloses 106 patients
Parameters NKF
(n = 70)
CKD stages 2–5
(n = 45)
CKD stage 5D
(n = 101)
p
Sex, % men 52.9 53.1 49.5 0.87
Age, median (25–75
percentiles)
65.5 (52–73) 70 (64.5–75) 65 (53–72) 0.048
APACHE II,mean (SD) 27.9 (8.5) 27.7 (6.9) 27.5 (9) 0.95
Comorbidity (%)
CVD 41.4 60 51.5 0.14
DM 22.9 44.4 29.7 0.048
Cancer 25.7 31.1 7.9 0.001
COPD 7.1 13.3 6.9 0.39
Liver disease 15.7 4.4 5.9 0.044
NIMV (%) 32.9 31.1 25.7 0.57
IMV (%) 77.1 66.7 51.5 0.002
LOS, median (25–75
percentiles)a10 (2–22) 6 (4–14) 4.5 (2–20) 0.583
Hypotension, n (%)b 8 (50) 3 (50) 9 (45) 0.94
Non-renal organ failure (%)c
Respiratory 84.3 64.4 55.4 <0.001
Cardiovascular 55.6 55 61.7 0.788
Haematologic 36.1 29.4 26.4 0.61
Hepatic 28.2 11.8 13.2 0.13
Neurological 24.3 17.6 21.4 0.85
Mortality (%) 78.6 51.1 50.5 <0.001
Cause of mortality (%)
Sepsis 87.2 95.7 70.6 N/A
Cardiac disease 1.8 0 23.5
Liver failure 9.2 4.3 0
Bleeding 1.8 0 5.9
Table 5 Results of multivariate models
Variables B p Odds ratio (95 % CI)
All patients
Liver disease 2.212 0.069 9.13 (0.84–98.81)
COPD 1.945 0.108 6.99 (0.65–75.10)
IMV 2.695 \0.001 14.81 (5.47–40.05)
NKF 1.019 0.041 2.77 (1.04–7.37)
APACHE II 0.064 0.053 1.06 (0.99–1.13)
AKI patients
IMV 2.927 \0.001 18.66 (4.48–77.72)
CD patients
IMV 2.097 0.003 8.14 (2.01–33.04)
APACHE II 0.125 0.024 1.13 (1.02–1.26)
AKI acute kidney injury, APACHE acute physiologic and chronic
health evaluation, CVD cardiovascular disease, CD chronic dialysis,
COPD chronic obstructive pulmonary disease, CI confidence interval,
IMV invasive mechanical ventilation, NKF normal kidney function
Fig. 2 The ROC curve for sensitivity and specificity of APACHE II
score in ESRD patients [0.78 (95 % CI 0.55–0.89); p = 0.004]
Clin Exp Nephrol
123

analysis. In this study, all AKI patients who were admitted
to the ICU with liver failure except one died. This was
because of having severely ill patients. The development of
AKI in these patients is a poor prognostic criterion with
reported mortality rates of between 52 and 91 % [29, 30].
Another reason for having high mortality could be through
failures in providing a liver-transplant for the patients due
to the shortage of organs and less transplant units. Mor-
tality was demonstrated to be 98 % in liver failure patients
who had CVVHD but no liver transplantation [31].
The primary limitation of this study is its retrospective
design conducted at a single medical center and its small
sample size. As such, the results might lack wider appli-
cability. Second, we did not examine AKI patients who did
not require RRT and patients without AKI. Therefore, we
can not generalize our findings to all ICU patients. Third,
information available from the early ICU database was not
sufficient to allow full collection of data on variables of
organ failure systems, LOS and hypotension during RRT.
This could be a reason for failing to show a difference
between AKI and CD patients along these variables.
Fourth, due to insufficient database, we could not study
hospital mortality, hospital LOS and renal survival for AKI
patients at the time of hospital discharge. Thus, the out-
comes for the patients after ICU discharge are unknown.
In conclusion, we have shown that overall mortality is
high among patients requiring RRT in the ICU. Although
disease severity score is the same between AKI and CD
patients, the rates of IMV and mortality are significantly
high in AKI patients. AKI patients with NKF before ICU
admission have an increased risk of dying than do patients
with acute-on-CKD and CD patients. IMV is an important
prognostic predictor for both AKI and CD patients,
whereas APACHE II is displayed as important only for CD
patients.
Acknowledgments We thank Dr. Pınar Ay, M.D., Assoc. Prof. of
Health Care and Statistic at Marmara University, School of Medicine,
for his help with the statistical analysis. T. Akbas designed the study,
gathered the raw data of the study and contributed to the writing of
the paper. Sait Karakurt helped the study design, reviewed the paper
and contributed to the writing of the manuscript. Serhan Tuglular
designed the study, reviewed the paper and contributed to the writing
of the manuscript. All authors read, edited and ultimately approved
the final manuscript.
Conflict of interest All authors have declared that no conflict of
interest exists.
References
1. Strijack B, Mojica J, Sood M, et al. Outcomes of chronic dialysis
patients admitted to the intensive care unit. J Am Soc Nephrol.
2009;20:2441–7.
2. Metnitz PGH, Moreno RP, Almeida E, et al. SAPS 3—from
evaluation of the patient to evaluation of the intensive care unit.
Part 1: objectives, methods and cohort description. Intensive Care
Med. 2005;31:1336–44.
3. Uchino S, Morimatsu H, Bellomo R, Silvester W, Cole L. End-
stage renal failure patients requiring renal replacement therapy in
the intensive care unit: incidence, clinical features, and outcome.
Blood Purif. 2003;21:170–5.
4. Hutchison CA, Crowe AV, Stevens PE, Harrison DA, Lipkin
GW. Case mix, outcome and activity for patients admitted to
intensive care units requiring chronic renal dialysis: a secondary
analysis of the ICNARC Case Mix Programme Database. Crit
Care. 2007;11:R50.
5. Dara SI, Bekele A, Bajwa AA, Albright RC. Outcome of patients
with end-stage renal disease admitted to the intensive care unit.
Mayo Clin Proc. 2004;79:1385–90.
6. Manhes G, Heng AE, Aublet-Cuvelier B, Gazuy N, Deteix P,
Souweine B. Clinical features and outcome of chronic dialysis
patients admitted to an intensive care unit. Nephrol Dial Trans-
plant. 2005;20:1127–33.
7. Rocha E, Soares M, Valente C, et al. Outcomes of critically ill
patients with acute kidney injury and end-stage renal disease
requiring renal replacement therapy: a case-control study.
Nephrol Dial Transplant. 2009;24:1924–30.
8. Clermont G, Acker CG, Angus DC, Sirio CA, Pinsky MR,
Johnson JP. Renal failure in the ICU: comparison of the impact of
acute renal failure and end-stage renal disease on ICU outcomes.
Kidney Int. 2002;62:986–96.
9. Chapman RJ, Templeton M, Ashworth S, Broomhead R, McLean
A, Brett SJ. Long-term survival of chronic dialysis patients fol-
lowing survival from an episode of multiple-organ failure. Crit
Care. 2009;13:R65.
10. Allegretti AS, Steele DJ, David-Kasdan JA, Bajwa E, Niles JL,
Bhan I. Continuous renal replacement therapy outcomes in acute
kidney injury and end stage renal disease: a cohort study. Crit
Care. 2013;17:R109.
11. Uchino S, Kellum JA, Bellomo R, et al. Acute renal failure in
critically ill patients: a multinational, multicenter study. JAMA.
2005;294:813–8.
12. De Mendonca A, Vincent JL, Suter PM, et al. Acute renal failure
in the ICU: risk factors and outcome evaluated by the SOFA
score. Intensive Care Med. 2000;26:915–21.
Fig. 3 The ROC curve for sensitivity and specificity of APACHE II
score in AKI patients [0.52 (95 % CI, 0.39–0.66); p = 0.69]
Clin Exp Nephrol
123

13. Chertow GM, Levy EM, Hammermeister KE, Grover F, Daley J.
Independent association between acute renal failure and mortality
following cardiac surgery. Am J Med. 1998;104:343–8.
14. Abosaif NY, Tolba YA, Heap M, Russell J, El Nahas AM. The
outcome of acute renal failure in the intensive care unit according
to RIFLE: model application, sensitivity, and predictability. Am J
Kidney Dis. 2005;46:1038–48.
15. Avasthi G, Sandhu JS, Mohindra K. Acute renal failure in
medical and surgical intensive care units—a one year prospective
study. Ren Fail. 2003;25:105–13.
16. Levey AS, Eckardt KU, Tsukamoto Y, et al. Definition and
classification of chronic kidney disease: a position statement from
kidney disease: improving global outcomes (KDIGO). Kidney
Int. 2005;67:2089–100.
17. Van Steen K, Curran D, Kramer J, et al. Multicollinearity in
prognostic factor analyses using the EORTC QLQ-C30: identi-
fication and impact on model selection. Statist Med. 2002;21:
3865–84.
18. Walcher A, Faubel S, Keniston A, Dennen P. In critically ill
patients requiring CRRT, AKI is associated with increased
respiratory failure and death versus ESRD. Ren Fail. 2011;33:
935–42.
19. Ostermann M, Chang R. Renal failure in the intensive care unit:
acute kidney injury compared to end-stage renal failure. Crit
Care. 2008;12:432–3.
20. Bagshaw SM, Mortis G, Doing CJ, Godinez-Luna T, Fick GH,
Laupland KB. One-year mortality in critically ill patients by
severity of kidney dysfunction: a population-based assessment.
Am J Kidney Dis. 2006;48:402–9.
21. Steinvall I, Bak Z, Sjoberg F. Acute kidney injury is common,
parallels organ dysfunction or failure, and carries appreciable
mortality in patients with major burns: a prospective exploratory
cohort study. Crit Care. 2008;12:R124.
22. Senthuran S, Bandeshe H, Ranganathan D, Boots R. Outcomes
for dialysis patients with end-stage renal failure admitted to an
intensive care unit or high dependency unit. Med J Aust.
2008;188:292–5.
23. Juneja D, Prabhu MV, Gopal PB, Mohan S, Spridhar G, Nayak
KS. Outcome of patients with end stage renal disease admitted to
an intensive care unit in India. Ren Fail. 2010;32:69–73.
24. Sood MM, Miller L, Komenda P, et al. Long-term outcomes of
end-stage renal disease patients admitted to the ICU. Nephrol
Dial Transplant. 2011;26:2965–70.
25. Arulkumaran N, Annear NMP, Singer M. Patients with end-stage
renal disease admitted to the intensive care unit: systematic
review. Br J Anaesth. 2013;110:13–20.
26. Liborio AB, Abreu KL, Silva GB Jr, et al. Predicting hospital
mortality in critically ill cancer patients according to acute kidney
injury severity. Oncology. 2011;80:160–6.
27. Soares M, Salluh JI, Carvalho MS, Darmon M, Rocco JR, Spector
N. Prognosis of critically ill patients with cancer and acute renal
dysfunction. J Clin Oncol. 2006;24:4003–10.
28. Maccariello E, Valente C, Nogueira L, et al. Outcomes of cancer
and non-cancer patients with kidney injury and need of renal
replacement therapy admitted to general intensive care units.
Nephrol Dial Transplant. 2011;26:537–43.
29. De Carvalho JR, Villela-Nogueira CA, Luiz RR, et al. Acute
kidney injury network criteria as a predictor of hospital mortality
in cirrhotic patients with ascites. J Clin Gastroenterol.
2012;46:e21–6.
30. Cholongitas E, Senzolo M, Patch D, Shaw S, O’Beirne J, Bur-
roughs AK. Cirrhotics admitted to intensive care unit: the impact
of acute renal failure on mortality. Eur J Gastroenterol Hepatol.
2009;21:744–50.
31. Fraley DS, Burr R, Bernardini J, Angus D, Kramer DJ, Johnson
JP. Impact of acute renal failure on mortality in end-stage liver
disease with or without transplantation. Kidney Int. 1998;54:
518–24.
Clin Exp Nephrol
123
![REVISED ORDINANCE GOVERNING …rguhs.ac.in/cdc/alliednew140709/BMLT.pdf6. Bachelor of Science in. Renal Dialysis Technology [ BSc. Renal Dialysis Technology] 7. Bachelor of Science](https://img.pdfslide.us/doc/110x75/5ae3fea87f8b9a7b218dcfe8/revised-ordinance-governing-rguhsacincdcalliednew140709bmltpdf6-bachelor.jpg)