Embed Size (px)
Citation preview

Renal Anatomy
800,000 to 1 million nephrons / kidney
• initial filtering component – renal corpuscle
• tubule extending from renal corpuscle to collecting ducts
Renal corpuscle forms filtrate of blood free of cells and protein
Filtrate leaves and enters tubule – as it flows through the tubule, substances are exchanged
Fluid remaining at the end of each nephron combines in collecting ducts – leaves as urine
Renal corpuscle:
• interconnected capillary loops – glomerulus
• supplied with blood from afferent arteriole
• glomerulus protrudes into Bowman’s capsule
• as blood flows through glomerulus, 1/5 of plasma filters into Bowman’s capsule
• remaining blood leaves through efferent arteriole

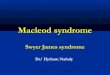
A – Renal corpuscleB – Proximal tubuleC – Distal convoluted tubuleD – Juxtaglomerular apparatus1. Basement membrane (Basal lamina)2. Bowman's capsule – parietal layer3. Bowman's capsule – visceral layer3a. Pedicels (podocytes)3b. Podocyte4. Bowman's space (urinary space)5a. Mesangium – Intraglomerular cell5b. Mesangium – Extraglomerular cell6. Granular cells (Juxtaglomerular cells)7. Macula densa8. Myocytes (smooth muscle)9. Afferent arteriole10. Glomerulus Capillaries11. Efferent arteriole
Renal Corpuscle

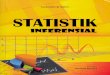
A. The endothelial cells of the glomerulusB. Glomerular basement membraneC. Podocytes
Renal Corpuscle

Renal Corpuscle

Membranous Glomerulonephritis
Progressive disease thought to occur as a result of autoimmunity – 85% of cases are idiopathic
Disease can also occur secondary to other autoimmune diseases (eg. systemic lupus erythematosus) or
through inflammation in response to bacterial / viral infection.
Symptoms:
• Edema
• Foamy appearance of urine
• Frequent urination
• High blood pressure
Membranous glomerulonephritis is the most common cause of nephrotic syndrome in Caucasians (20-
35%).

Membranous Glomerulonephritis - Pathology
Characterized by subepithelial immune deposits - presence of immunoglobulins, complement, and
membrane attack complex (MAC) (C5b-9)
Immune complexes serve as a trigger for the complement cascade and formation of the MAC – but
what triggers Ab formation ?

Membranous Glomerulonephritis - Pathology
Characterized by subepithelial immune deposits - presence of immunoglobulins, complement, and
membrane attack complex (MAC) (C5b-9)
Immune complexes serve as a trigger for the complement cascade and formation of the MAC – but
what triggers Ab formation ?
Serum samples from 26 of 37 patients (70%) with idiopathic but not secondary membranous
nephropathy specifically identified a 185-kD glycoprotein in nonreduced glomerular extract.
Reactive serum specimens recognized recombinant PLA2R and bound the 185-kD glomerular protein.
PLA2R was expressed in podocytes in normal human glomeruli and colocalized with IgG4 in immune
deposits in glomeruli of patients with membranous nephropathy. IgG eluted from such deposits in
patients with idiopathic membranous nephropathy, but not in those with lupus membranous or IgA
nephropathy, recognized PLA2R. (N Engl J Med. 2009 Jul 2;361(1):11-21)

Membrane Attack Complex (MAC)

Membrane Attack Complex
What happens ?
• Lysis of glomerular epithelial cells
• Stimulates release of proteases and reactive O2 species that induce further cell damage
• Capillary walls become more porous, increasing the amount of fluid that can enter Bowman’s capsule
• Inhibitor of nephrin is released, decreasing the selectivity of filtration through podocytes.

Membranous Glomerulonephritis – Clinical Features
Any thoughts on clinical / laboratory features?

Membranous Glomerulonephritis – Clinical Features
Any thoughts on clinical / laboratory features?
Proteinuria is generally in nephrotic range and can be massive (>10 g/24h) (corresponding hypoproteinemia)
Hypoalbuminemia
Hypercholesterolemia
Microhematuria is common and macrohematuria is unusual
No hypocomplementemia (at least in idiopathic forms) and in many cases increased levels of MAC (C5b-C9)

Membranous Glomerulonephritis – Clinical Features
Any thoughts on clinical / laboratory features?
Proteinuria is generally in nephrotic range and can be massive (>10 g/24h) (corresponding hypoproteinemia)
Hypoalbuminemia
Hypercholesterolemia
Microhematuria is common and macrohematuria is unusual
No hypocomplementemia (at least in idiopathic forms) and in many cases increased levels of MAC (C5b-C9)
The reason for most of these changes should be obvious – why do patients present with hypercholesterolemia ?
• triglycerides are normally cleared by the liver and other organs not the kidney• mechanism is unknown but enzymes involved in fatty acid metabolism are not as active• one route could be that an enzyme inhibitor that is normally cleared by the kidney can accumulate

Membranous Glomerulonephritis – Outcomes
Prognosis
~25% of patients have partial or complete remission (with 1/3 of those having recurrence)50% will lack any proteinuria or impairment of renal function
A small percentage will have rapid loss of renal function, possibly leading to death.
Varying outcomes with no obvious differences in pathology make treatment options difficult.

Membranous Glomerulonephritis – Outcomes
Prognosis
~25% of patients have partial or complete remission (with 1/3 of those having recurrence)50% will lack any proteinuria or impairment of renal function
A small percentage will have rapid loss of renal function, possibly leading to death.
Varying outcomes with no obvious differences in pathology make treatment options difficult.
Treatment
Corticosteroids and other immunosuppresants – limited use with variable data on the effectiveness• Side effects of immunosuppresants may be more dangerous than the underlying disease
• Calcineurin inhibitors (CNIs) induce remission of proteinuria in most nephrotic patient 60% of patients become treatment dependent and are at risk of chronic nephrotoxicity

Membranous Glomerulonephritis – Outcomes
Is Rituximab the answer?
- Humanized monoclonal antibody designed to target the cellular protein, CD20
- CD20 is found on the surface of all mature B cells – involved in the progression of B cells in to plasma cells, which produce high quantities of antibodies (but actual role is unknown)
- Rituixmab causes B cells to undergo programmed cell death, allowing new, less-reactive B cells to develop in the bone marrow.
- Destroys memory B cells, those responsible for recognising previous exposure to an antigen.

Membranous Glomerulonephritis – Outcomes
Is Rituximab the answer?
Design: Thirteen patients with membranous glomerulonephritis , normal renal function, and proven dependence on calcineurin inhibitors , despite previous treatment with other immunosuppressant drugs,
received a single trial of four weekly doses of rituximab (375 mg/m2).

Membranous Glomerulonephritis – Outcomes
Is Rituximab the answer?
Design: Thirteen patients with membranous glomerulonephritis , normal renal function, and proven dependence on calcineurin inhibitors , despite previous treatment with other immunosuppressant drugs,
received a single trial of four weekly doses of rituximab (375 mg/m2).
Outcome measures: the percentage of patients with CNI withdrawal and no evidence of relapse and the percentage of patients with complete or partial remission 30 mo after CNI withdrawal.

Membranous Glomerulonephritis – Outcomes
Is Rituximab the answer? Clin J Am Soc Nephrol. 2009 Jun;4(6):1083-8. Epub 2009 May 28
Design: Thirteen patients with membranous glomerulonephritis , normal renal function, and proven dependence on calcineurin inhibitors , despite previous treatment with other immunosuppressant drugs,
received a single trial of four weekly doses of rituximab (375 mg/m2).
Outcome measures: the percentage of patients with CNI withdrawal and no evidence of relapse and the percentage of patients with complete or partial remission 30 mo after CNI withdrawal.
Results: After rituximab, proteinuria decreased significantly (2.5 ± 0,76 basal versus 0.85 ± 0.17 at 6 mo;
p = .0003)
CNIs and other immunosuppressant drugs could be withdrawn in all patients with no evidence of relapse.
After CNI withdrawal, glomerular filtration rate increased significantly (90.3 ± 15 basal to 106.4 ± 20 at 3 mo with a mean increase of 15.3% [range 0–20]).
Three patients suffered a relapse of nephrotic proteinuria 19, 23, and 28 mo after rituximab treatment; all
were successfully treated with a second course of rituximab.
At 30 mo, all patients were in remission.