-
8/11/2019 Renal Pathology Blok 13
1/71
Disease of the urinary
system
Rohadi
Lab PA FK UNRAM
-
8/11/2019 Renal Pathology Blok 13
2/71
Kidney Anatomy:
-
8/11/2019 Renal Pathology Blok 13
3/71
Kidney Histology :
-
8/11/2019 Renal Pathology Blok 13
4/71
Kidney Histology
-
8/11/2019 Renal Pathology Blok 13
5/71
Kidney Histology
-
8/11/2019 Renal Pathology Blok 13
6/71
Classification of urinary
system disease
Congenital
Infeksi : Parenchim, Interstial Nephritis
Glomerulo Nephritis
Vascular disorder :
Hipertensive Neprosclerosis
-A.C.N.( Acut Cortical Necrosis)
-A.T.N.( Acut Tubular Necrosis )
-Infark Ginjal
-
8/11/2019 Renal Pathology Blok 13
7/71
SINDROME PD KELAINAN GINJAL
Neprotic Syndrome
Nepritic Syndrome
A.R.F.( Acut Renal Failure)
C.R.F ( Chronic Renal Failure )
Hidroneprosis +Hidrocalices
Calculi renalis ( Batu Ginjal )
Tumor-tumor ginjal dan kandung kemih
Benign Tumor
Malignant tumor
-
8/11/2019 Renal Pathology Blok 13
8/71
Preparat yang ada :
1. TCC
2. TBC Ginjal
3. Pyelonefrosis Khronis
4. PNC
5. Nerfrolitiasis
6. Pyelitis Chronic
7. Nefroblastoma
8. Glomerulonefritis
Kronis
9. Renal Cell Ca
10. Squamous Cell CaGinjal
-
8/11/2019 Renal Pathology Blok 13
9/71
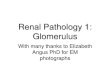
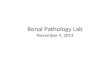
TBC Ginjal
Renal tuberculosis. Photograph of a cut gross specimen shows
multiple,
predominantly peripheral, white tuberculous granulomas
throughout the kidney.
-
8/11/2019 Renal Pathology Blok 13
10/71
TBC Ginjal
-
8/11/2019 Renal Pathology Blok 13
11/71
Normal
Proliferative
Post strepto
-
8/11/2019 Renal Pathology Blok 13
12/71
-
8/11/2019 Renal Pathology Blok 13
13/71
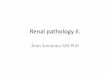
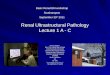
Chronic glomerulonephritis
Chronic glomerulonephritisrepresents the end-stage of all
glomerulonephritis with unfavorable evolution. This general
(glomerular,vascular and interstitial) affection constitutes the
so-called "end stage
kidney". In most cases, it is associated with systemic
hypertension.
a kidney with chronic glomerulonephritis. The cortex has
largely
turned to scar tissue and there is a poor demarcation
between
cortex and medulla due to the glomerular scarring.
h l l h
-
8/11/2019 Renal Pathology Blok 13
14/71
Chronic glomerulonephritisThe majority of the glomeruli are
affected.
Depending on the stage of the disease,
they may present different degrees of
hyalinization (hyalinosclerosis - totalreplacement of glomeruli
and Bowmann's
space with hyaline). The hyaline is an
amorphous material, pink, homogenous,
resulted from combination of plasma
proteins, increased mesangial matrix and
collagen. Totally hyalinised glomeruli are
atrophic (smaller), lacking capillaries,
hence these glomeruli are non-functional.
Few glomeruli may still present changes
which permit to discern the etiology of
chronic glomerulonephritis. Obstruction ofblood flow will
produce secondary tubular
atrophy, interstitial fibrosis and thickening
of the arterial wall by hyaline deposits. In
the interstitium is present an abundant
inflammatory infiltrate (mostly with
lymphocytes).
-
8/11/2019 Renal Pathology Blok 13
15/71
Chronic glomerulonephritis
-
8/11/2019 Renal Pathology Blok 13
16/71
Chronic glomerulonephritis
Functional nephrons have dilated tubules, often with hyaline
casts in the lumens.
-
8/11/2019 Renal Pathology Blok 13
17/71
Pyelonephrosis
An absolute term for any disease of the pelvis
of the kidney. ... Origin: pyelo-+ G. Nephros,
kidney, + -osis,
-
8/11/2019 Renal Pathology Blok 13
18/71
Acute pyelonephritis
route of invasion :
via blood stream
ascending route
obstructive
non-obstructive
role of vesicoureteral reflux and infected urine
-
8/11/2019 Renal Pathology Blok 13
19/71
PYELONEPHRITIS ACUTA
Makroskopis :
-.Uni/Bilateral
-. Ginjal>> Kapsul meregang
- Abses kecil sub kaps,Pelvis hyperemis
granuler.
-URINE : PURULENT
Mikroskopis :
-Gambaran Abses
Akibat: Resolusi, Chronic Pyel., Supp, Bisa +
-
8/11/2019 Renal Pathology Blok 13
20/71
Septicemia-
Microabscess
-
8/11/2019 Renal Pathology Blok 13
21/71
Septicemia-Microabscess
-
8/11/2019 Renal Pathology Blok 13
22/71
-
8/11/2019 Renal Pathology Blok 13
23/71
-
8/11/2019 Renal Pathology Blok 13
24/71
-
8/11/2019 Renal Pathology Blok 13
25/71
-
8/11/2019 Renal Pathology Blok 13
26/71
CHRONIC PYELONEPHRITIS
Makroskopis : Ginjal Mengecil
Kapsul melekat, menebal( parut) Cortex tipis
Batas dg medulla kabur,warna pucat
Medulla mengkerut
Pelvis menebal fibrotik,pucat Calyces melebar
Vasculer prominent
-
8/11/2019 Renal Pathology Blok 13
27/71
CHRONIC PYELONEPHRITIS
Mikroskopis :
Parenchym : Kelompok jar.parut.
Tubulus : Delatasi,epit.atrofi : berisi bahan albominus (koloid/
Tiroidisasi)
Asal : Dr.proses inf ringan,lama,berkelanj.
-Pyelo.Acut Berulang
-
8/11/2019 Renal Pathology Blok 13
28/71
PNC
You can see the stones, dark red and rough. They have plugged
the renal
collecting system and dilated the calyces. Stasis of urine and
the presence of the
inert stones themselves both promote infection. This in turn can
make the stones
grow larger.
-
8/11/2019 Renal Pathology Blok 13
29/71
-
8/11/2019 Renal Pathology Blok 13
30/71
-
8/11/2019 Renal Pathology Blok 13
31/71
-
8/11/2019 Renal Pathology Blok 13
32/71
Microscopic View of PNC
1. scarring and shrinking of the renal tubules, with the
glomerulus spared.In contrast to rapidly progressive
glomerulonephritis, the scar is outside
Bowman's capsule.
2. a group of tubules filled with cast protein and distended
from scar
contraction. The unwary may mistake this for thyroid.
-
8/11/2019 Renal Pathology Blok 13
33/71
Urolithiasis :
-
8/11/2019 Renal Pathology Blok 13
34/71
Urolithiasis:
-
8/11/2019 Renal Pathology Blok 13
35/71
NEPHROLITHIASIS
-
8/11/2019 Renal Pathology Blok 13
36/71
Staghorn Calculus:
-
8/11/2019 Renal Pathology Blok 13
37/71
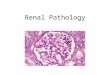
NEPHROLITHIASIS
Top left: Retention of calcium oxalate crystals in the renal
tubules after kidney
transplantation. Top right: Close-up image of calcium oxalate
crystals plugging the renal
tubules of a primary hyperoxaluria patient with end-stage renal
failure. Obstruction of the
renal tubules leads to tubular necrosis and loss of the total
nephron mass. In preterm
infants, tubular nephrocalcinosis may lead to reduced renal
function in adulthood, while in
renal transplant patients it may have a negative impact on
long-term graft survival.
-
8/11/2019 Renal Pathology Blok 13
38/71
Hidronefrosis
-
8/11/2019 Renal Pathology Blok 13
39/71
Urolithiasis with hydronephrosis:
-
8/11/2019 Renal Pathology Blok 13
40/71
Hidronefrosis
Obstructive uropathy; form a continuousspectrum from minor
changes of blunting
of the renal papillae to severe from where
kidney converted into a multiseptate sac
with paper-thin walls.
-
8/11/2019 Renal Pathology Blok 13
41/71
Hidronefrosis
1. Thinning renal parenchyma with residual large renal vessels
in the hilum;
note dilated renal pelvis with flattened epithelia.
2. Sclerosis of glomeruli with atrophic tubules; note renal
pelvis with flattened
epithelia.
-
8/11/2019 Renal Pathology Blok 13
42/71
TUMOR GINJAL
Benigna : Adenoma
Hamartoma
Haemangioma
Lipoma,Angiomio lipoma,Fibro
ma, liomyoma.
Maligna : Adeno Ca, Grawits tu, Willm Tu,Sarcoma
-
8/11/2019 Renal Pathology Blok 13
43/71
Renal carcinoma(renal cell carcinoma, clear cell carcinoma,
grawit tumor )
Definition:
Renal carcinoma is a malignant tumor, it
is originate from renal tubule
epithelium . 80
90 %. Age : 60
70 th.
Risk Factor : Smoking
-
8/11/2019 Renal Pathology Blok 13
44/71
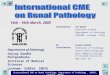
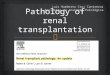
RCC
This renal cell
carcinoma is very large,
as indicated by the 15
cm ruler. A portion ofnormal kidney
protrudes at the lower
center. This patient was
a physician himself andjust didn't have any
early symptoms.
-
8/11/2019 Renal Pathology Blok 13
45/71
RCC (GRAWITS TUMOR)
Morfologi : Makros
Tumor besar 3-15 cm
Pd irisan : Kuningabu2 dg area kis
tik & perdrhn prominent
Ada satelit nodul
Bisa meluas : Ke Collect Tub---Calyces-------Pelvis---
Ureter
-
8/11/2019 Renal Pathology Blok 13
46/71
Pathology
Grossly :
Nodular, might have a pseudo
capsula, usually on the upperpole of the kidney; yellowcolored,
hemorrhagic andnecrotic
-
8/11/2019 Renal Pathology Blok 13
47/71
Slide 21.72
-
8/11/2019 Renal Pathology Blok 13
48/71
-
8/11/2019 Renal Pathology Blok 13
49/71
Microscopic View :The cancer cells are clear (lipid and
glycogen deposition), nuclei notbig, nucleus-cytoplasm ratio
not
large. Cancer cells arrange nest-
like or gland-like. Stroma is scanty.
-
8/11/2019 Renal Pathology Blok 13
50/71
-
8/11/2019 Renal Pathology Blok 13
51/71
Slide 21.73
Renal Cell Carcinoma
-
8/11/2019 Renal Pathology Blok 13
52/71
Renal Cell Carcinoma:
Incidence:
Etiology:
Clinical
Features:
Lab:
Path:
Clinical
Course:
Cells of proximal convoluted tubule. Risk
factors are smoking, obesity, analgesic
abuse.
Hematuria*, flank pain, palpable mass.
Frequently metastasize (lungs, bone, skin,
liver, brain).Gross or microscopic hematuria.
Specific Dx by radiographic techniques.
5-yr. survival 40%. Poor prognosis with
metastases.
Gross: Large yellow mass with hemorrhage
and necrosis. Invade renal vein.
Micro: Usually clear or granular cells with
little anaplasia. Other histologic variants
(great mimicker).
5th
and 6th
decades, most commonprimary renal malignancy.
Treatment: Chemotherapy, surgery, immunotherapy.
Synonyms: Hypernephroma, clear cell carcinoma.
-
8/11/2019 Renal Pathology Blok 13
53/71
Squamous Cell Carcinoma Ginjal
-
8/11/2019 Renal Pathology Blok 13
54/71
Squamous Cell Carcinoma Ginjal
The tumor is moderately differentiated with
formation of abundant keratin pearls
-
8/11/2019 Renal Pathology Blok 13
55/71
Nephroblastoma(embryonal adenosarcoma, wilmstumor)
Nephroblastoma is a malignant
tumor, it originate fromembryonal cell (Nephroblast).
Usually is seen in the children,
very common.
-
8/11/2019 Renal Pathology Blok 13
56/71
WILMS TUMOR("nephroblastoma"): One of thecommonest pediatric
solidtumors (peak age 1-4 years).Wilms tumor
microscopicallyresembles the primitive
nephrogenic zone of the fetalkidney, with primitiveglomeruloid
structures and acellular stroma. Wilms tumor isassociated with
mutationsinvolving the WT1 tumorsuppressor gene on chromosome
11. This neoplasm is verytreatable with an excellentprognosis
and >80% cure rateoverall.
-
8/11/2019 Renal Pathology Blok 13
57/71
WILMS TUMOR
Makroskopis :
Tumor berukuran bbrp Cmsangat
besar
Warna putih abu2
Homogen dlm kapsel ginjal
Tampak area nekrosis & perdrhn
-
8/11/2019 Renal Pathology Blok 13
58/71
WILMS TUMOR
Mikroskopis :
1. Jaringan ikat
2. Blastema
3. Komp.Epit.yg dpt membent.strt.Tub,
Glomerulus ( Abortive Glom. )
Salah satu komponen bisa dominant
-
8/11/2019 Renal Pathology Blok 13
59/71
Microscopic View :
Two components:adenocarcinoma
fibrosarcoma
Sometime tumor cell would formglomerulus-like or tubule-like
structures.
Sometime having some well differentiated
cartilage
-
8/11/2019 Renal Pathology Blok 13
60/71
WILM TUMOR
Wil T
-
8/11/2019 Renal Pathology Blok 13
61/71
Wilms Tumor
Incidence:
Etiology:
Clinical
Features:
Lab:
Path:
Clinical
Course:
Embryonic renal tissue (metanephric
blastema). Genetic abnormalities.
Palpable abdominal mass. Abdominal
pain, fever, anorexia, nausea/vomiting.
Hematuria.
No specific clinical laboratory findings.Diagnosis by
radiographic techniques.
5-yr. Survival 80%. Metastases to lung,
liver, bone, brain.
Gross: Solitary/multiple cystic mass,
sharply delineated. Soft, bulging, gray-
white with focal hemorrhage and necrosis.
Micro: Triphasic mesenchymal stroma,
tubules, and solid areas (blastema).
Primitive glomeruli, skeletal muscle,cartilage, bone, etc.
(embryonic tissues)
Most common renal tumor of
childhood. Peak age - 2.5 - 3.5 years.
Treatment: Prompt resection with chemotherapy
radiotherapy.
Synonyms: Nephroblastoma.
-
8/11/2019 Renal Pathology Blok 13
62/71
Carcinoma of Bladder
Transitional cell carcinoma of bladder
Definition
Transitional cell carcinoma of
bladder is a malignant tumor. It
originate from transitional cell ofbladder. It occupy 90% of
cases in
carcinoma of bladder.
-
8/11/2019 Renal Pathology Blok 13
63/71
Pathology
. Grossly:
Usually it is a papillary tumor with
slender or broad pedicle,
sometime it show cauliflower-likeor polypous, sometime it is
flat.
-
8/11/2019 Renal Pathology Blok 13
64/71
-
8/11/2019 Renal Pathology Blok 13
65/71
TCC Bladder
-
8/11/2019 Renal Pathology Blok 13
66/71
TCC Bladder
These tumors showmore architectural
disorder and nuclear
atypia than Grade 1
tumors. The nuclear
size, shape, polarity,
and chromatin show
greater variability.Mitoses are still
infrequent.
-
8/11/2019 Renal Pathology Blok 13
67/71
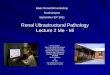
TCC Bladder
Another look at grade 1 papillaryurothelial carcinoma. These
patients are at risk of developing
recurrent tumors which may be
of higher grade. This entity is
considered synonymous withpapillary urothelial neoplasm of
low malignant potentialin the
1998 WHO/ISUP Classification of
papillary urothelial neoplasms.
-
8/11/2019 Renal Pathology Blok 13
68/71
-
8/11/2019 Renal Pathology Blok 13
69/71
-
8/11/2019 Renal Pathology Blok 13
70/71
-
8/11/2019 Renal Pathology Blok 13
71/71