Embed Size (px)
Citation preview

Renal Medullary Carcinoma: Prolonged Remission With Chemotherapy,Immunohistochemical Characterisation and Evidence of bcr/abl Rearrangement
Jens Stahlschmidt, MD,1 Catherine Cullinane, MB, BAO, BCh,1
Paul Roberts, BSc(HONS),2 and Susan V. Picton, FRCPCH3*
Background. Renal medullary carcinoma(RMC), an extremely rare tumour of the kidney,carries a dismal prognosis, with no reports todate of significant response to chemotherapy orradiotherapy. A case of this tumour in a malechild, who showed a dramatic response to che-motherapy, is described. Procedure. A detailedhistological evaluation of the tumour and cyto-genetic analysis using fluorescent in situ hy-bridisation (FISH) was carried out. The childwas treated with multiagent chemotherapy, fol-lowed by abdominal radiotherapy. Results. Adetailed histopathological and immunohisto-chemical portrait of this tumour is described,and FISH studies confirmed the presence of abcr/abl rearrangement. The child obtained
complete radiological remission following che-motherapy, although he later relapsed and diedof progressive disease despite further attemptsat treatment with chemotherapy. Conclusions.Although there are no previous reports of re-sponse of this tumour to chemotherapy, thiscase illustrates that treatment of this disease isjustified. The responses of other cases to similardrug regimens would be of interest to confirmwhether the encouraging response describedfor this case could be reproduced. Cytogeneticanalysis of other cases of RMC may clarifywhether the abnormalities seen in this case aretypical. Med. Pediatr. Oncol. 33:551–557,1999. © 1999 Wiley-Liss, Inc.
Key words: renal neoplasm; child; treatment; cytogenetics; histopathology
INTRODUCTION
Renal medullary carcinoma (RMC) is an extremelyrare primary neoplasm of the kidney, which occurs al-most exclusively in Afro-Caribbeans with sickle cell trait(SCT). It was recently described by Davis et al. [1], whoreviewed 54 tumours coded as renal cell carcinoma inpatients under 40 years of age from the Armed ForcesRegistry and found 33 cases of this tumour. Prognosiswas poor, with a mean survival of 15 weeks in the 19cases for whom follow-up information was available. Ina subsequent report Avery et al. [2] described six of thesecases in more detail. None of the patient responded toany of the chemo- and immunotherapies used. Very re-cently a number of other case reports of RMC have beenpublished [3–10], and although in some cases treatmenthas been attempted no responses to chemotherapy or ra-diotherapy have been demonstrated [6,8,10]. To ourknowledge we describe the first case in which completeclinical remission was achieved for 5 months followingsurgery and chemotherapy despite extensive metastaticdisease. In addition an immunohistochemical portraitwith the second published detailed tumour karyotype ispresented.
CASE REPORT
A 14-year-old black male of Nigerian extraction, whowas known to have SCT, presented with a 3 month his-
tory of weight loss and a 1 month history of lethargy andmalaise. During the 10 days prior to admission he devel-oped intermittent pyrexia, arthralgia, and abdominalpain. No haematuria was noted. Ultrasonography andcomputerised tomography demonstrated a mass associ-ated with the lower pole of the left kidney and lymph-adenopathy extending from the retrocrural region supe-riorly to below the aortic bifurcation inferiorly (Fig. 1a).An ultrasound-guided fine-needle aspirate of the renalmass displayed an infiltrating, poorly differentiated car-cinoma. Therefore, a laparotomy was carried out. At op-eration extensive paraaortic lymphadenopathy and asci-tes were confirmed. There was a large tumour in thelower pole of the left kidney. A left nephrouretectomyand paraaortic lymph node biopsy were carried out.
1Department of Histopathology, St. James’s University Hospital,Leeds, United Kingdom2Yorkshire Regional Cytogenetics Unit, St. James’s University Hos-pital, Leeds, United Kingdom3Department of Paediatric Oncology, St. James’s University Hospital,Leeds, United Kingdom
*Correspondence to: S.V. Picton, Department of Paediatric Oncology,Children’s Day Hospital, St. James’s University Hospital, BeckettStreet, Leeds LS9 7TF, United Kingdom.
Received 28 January 1999; Accepted 8 July 1999
Medical and Pediatric Oncology 33:551–557 (1999)
© 1999 Wiley-Liss, Inc.

Pathology
The nephrectomy specimen measured 16 × 5.5 × 4 cm.The cut surface revealed extensive replacement of thelower pole of the kidney by a greyish, fleshy lobulatedtumour measuring 7 × 6 × 6 cm. Thetumour occupiedpredominately the medulla, with extension into the pel-vicalyceal system and part of the renal sinus (Fig. 2).Small peripheral satellite lesions up to 1.2 cm extendedinto the cortex. An attached 13.5 cm length of uretershowed thickening of the periureteral tissue 3 cm fromthe pelviureteral junction over a length of 5 cm.
Histological sections were taken from standard forma-lin-fixed, paraffin-embedded tissue and stained haema-toxylin and eosin, periodic acid Schiff (PAS) stains with-out and with diastase (PASD), reticulin, Masson’s tri-chrome, and Perls. Immunohistochemical staining usedthe standard avidin-biotin technique, with a wide rangeof mostly monoclonal antibodies as listed in Table I. The
percentage of apoptotic cells (apoptotic index) wascounted in 10 high-power fields (HPF; Leitz NPL Fluotar40×). Criteria for apoptotic cells were applied as de-scribed by Kerr et al. [11] Immunohistochemical resultswere graded as follows: −, less than 1%; +, 1–25%, ++,26–50%; +++, 51–75%, ++++, 76–100%.
Histological Findings
Histological examination revealed an infiltrative,moderately to highly cellular, poorly differentiated epi-thelial tumour (Fig. 3). In its typical form it consisted ofcohesive sheets of large cells (up to 40mm) with hae-matoxophilic cytoplasm and huge, pale nuclei, some ofwhich had clear, others coarse, chromatin, Acidophilicnucleoli were conspicuous and irregular and occasionallygreater in size than erythrocytes. Focally the cells had arhabdoid cytology. The tumour appeared partly squa-moid, although prickels or keratinisation were not seen.Eosinophilic, PAS-, and PASD-positive cytoplasmic in-clusions were noted. Mitoses were readily seen, as wellas areas of necrosis. The main variant of this lesion was
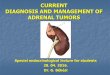
Fig. 1. A CT scan of the abdomen demonstrating the renal tumourand associated paraaortic lymphadenopathy at presentation(a) andcomplete remission following nephrectomy and six courses of chemo-therapy(b).
Fig. 2. The cut surface of the left kidney reveals replacement of thelower pole and midportion by a greyish, predominantly lobulated, andpartly infiltrating tumour. Note compression and focal infiltration ofthe renal pelvis by tumour.
552 Stahlschmidt et al.

a trabecular and loosely reticular growth pattern. Theinfiltrative margins were surrounded by dense, lympho-histiocytic cell infiltrates set in a myxoid or desmoplasticstroma. Reticulin stain revealed no increase in reticulinfibres within the tumour. The tumour focally eroded thetransitional cell epithelium of the pelviceal system. Therewas extensive and widespread invasion of blood vesselsand lymphatics, with focal extension into renal tubulesand Bowman spaces. Numerous tumour islands werefound within the pelvic fat and the renal capsule. Thethickening of the periureteral tissue was due to tumourinfiltration of the wall and vascular permeation. The cutends of ureter and renal vein were free of tumour. Theremote renal parenchyma was normal. There was no evi-dence of sickle cells. Paraaortic lymphnodes sampledwere positive for metastatic tumour.
Immunohistochemistry
Results of immunohistochemistry of this case and allpreviously published cases are summarised in Table I.
RESULTSCytogenetic Results and FISH studies
G-banded analysis of five metaphases showed a near-tetraploid clone, with between 84 and 94 chromosomes,and several consistent numerical and structural chromo-some changes (see Fig. 6): 84–94,XX,+X,−Y,−Y,+I(1)(q10),−7,−8,+I(8)(q10)x2,t(9;22)(q34;q11)x2,t(10;16)(q22;q22)x2,i(17)(q10),add(22)(q11)x2[cp5].The abnormalities thus include isochromosomes for 1q,8q (two copies), and 17q, two copies of a translocationbetween chromosomes 10 and 16, two copies of a trans-location between chromosomes 9 and 22, and two copies
of a structural rearrangement of the other two number 22chromosomes at q11.
FISH studies confirmed that the (9;22) translocationcontained a bcr/abl rearrangement of the type commonlyseen in chronic myeloid leukaemia. Furthermore, the ab-sence of a bcr signal on the other two 22 chromosomessuggests that this region is deleted in the rearrangementdescribed on G-banding as “add(22)(q11).”
Treatment and Clinical CourseThe patient was treated with six courses of the fol-
lowing chemotherapy: methotrexate 30 mg/m2, vinblas-tine 4 mg/m2, adriamycin 75 mg/m2, and cisplatin 100mg/m2. Repeat computer tomography (CT) followingthis treatment demonstrated complete radiological remis-sion, with no evidence of residual lymphadenopathy(Fig. 1b). He was then treated with abdominal radio-therapy (45 Gy) to all previous tumour sites. The childremained well and in clinical remission for a further 4months, at which time he was readmitted with nausea,vomiting, and abdominal pain. A gastrointestinal contraststudy demonstrated delayed gastric emptying and CTscanning suggested generalised thickening of the smallbowel, initially thought to be related to radiotherapy. Thesymptoms did not improve, and a repeat laparotomy wascarried out, which demonstrated widespread retroperito-neal and mesenteric lymphadenopathy and ascites sug-gestive of disease recurrence causing gastric outlet ob-struction. Biopsies of duodenum and mesentery con-firmed recurrence of tumour with widespread lymphaticinvasion, and a palliative gastrojejunostomy was carriedout. Despite second-line chemotherapy using carboplatinand etoposide there was continued disease progression,and the child died 6 weeks following relapse of diseaseand 49 weeks following diagnosis.
Fig. 3. Infiltration of undifferentiated tumourcells in irregular sheets with microcystic spacesand focally a reticular pattern (top right quad-rant). Also shown is a trabecular pattern (bot-tom right corner). The stroma is desmoplastic.H&E, ×166.
Renal Medullary Carcinoma: Diagnosis and Treatment 553

DISCUSSIONRenal carcinomas are extremely rare in children. In
adults the main differential diagnosis includes poorly dif-ferentiated invasive transitional cell carcinoma (TCC)originating in the renal pelvis, the subtypes of renal cellcarcinoma (RCC), collecting duct carcinoma, or meta-static tumour. The results of previously published studieson immunohistochemical features of RMC are presentedin Table I and compared to the results of our case. Aninteresting finding in the present case was that the CK14isotype was positive predominantly in the centre of largetumour formations. CK14 is absent in normal differenti-ated transitional epithelium in vivo [13,14] but has beendescribed in high-grade TCCs at varying site within thetumour [13] or even in tumour areas that were otherwise
not suggestive of squamous differentiation [15]. Addi-tionally, this case demonstrated circumscribed expres-sion of CK20 (Fig. 4), which is absent in normal renaltubular epithelium and in most cases of RCC, but, ifconfined to the umbrella cells in normal transitional epi-thelium, it is a marker for terminally differentiated nor-mal urothelium [15,16]. In high-grade TCCs CK20 posi-tivity is at least focally maintained [16]. The expressionof the remaining cytokeratins have been described inboth RCCs [17] and TCCs [13] and so does not help inthe differential diagnosis or in determining the origin ofthis tumour. In this case reactivity with CD15 was weakand focal with a tendency towards the outer margins ofthe tumour. The same distribution was observed byParham et al. [18] who investigated 91 TCCs of the blad-
TABLE I. Immunoreactivity for Different Monoclonal Antibodies (Otherwise Stated) in This Study and Comparison toOther Studies
AntibodyCurrentstudy Ref 1 Ref 12 Ref 9 Ref 8 Ref 5
Cytokeratin (CK) 7 ++++MNF116 (CK5/6/8/17) ++++ Keratin Ab N/S
9/10-positiveAE1/
AE3-positiveCytokeratins
N/S-positiveAE1/AE3-
positiveCAM5.2 (CK8/18) ++++ Positive PositiveCK14 + 34betaE12
(CK1/5/10/14)-negative
CK20 (Fig. 4) +Desmin − Negative NegativeAlpha-smooth muscle actin −Vimentin − Negative Positive NegativeGlial fibrillary acidic
protein−
Neurofilament protein(70/200kDa)
−
Laminin −Epithelial membrane
antigen− 4/4-Positive Positive Positive Positive Focal positivity
Myoglobin −Alpha-foetoprotein − Negative NegativePlacental alkaline
phosphatase−
Carcinoembryonic antigen − 5/8-PositiveN/S
Negative Negative
Factor VIII (polyclonal) −S100 protein − Negative NegativeHMB-45 −Neuron-specific enolase −CD (cluster differentiation
marker) 15+
CD30 −CD45 LCA − Negativep53 (DO7) +BCL-2 (Fig. 5) ++++a
Cyclin D1 +b
MIB-1 0.74–0.85c
aPositive in basal cell layer of transitional epithelium.bFocal, weak positivity throughout the urothelium.cMIB-1 staining index per 400 tumour cells.
554 Stahlschmidt et al.

der with the CD15 clone MC2. The morphology and theimmunohistochemical profile indicate that this tumour isdistinct from both RCC and TCC. In comparison topoorly differentiated types of TCC, there might be asimilarity, which, from the clinical point of view, wassupported by the good response to treatment using che-motherapy suitable for the treatment of TCC.
In the current case diffuse expression of bcl-2 (Fig. 5)was associated with expression of p53 (wild and mutanttypes) in 10% and cyclin D1 in 15–20%, of tumour cellnuclei. The MIB-1 staining index varied slightly depend-ing on the tumour architecture. It was higher in solidtumour formations (0.85), whereas yolk sac-like differ-entiated areas showed a lower staining index (0.74). Theapoptotic index ranged between 0.5% and 1%. The exactpathway of p53-mediated apoptosis is not clear. Severalstudies have shown that bcl-2 is regulated by p53 [19],and it has been shown that bcl-2 is able to antagonisep53-induced apoptosis [20]. Cyclin D1 (PRAD-1, bcl-1)overexpression has been detected in a number of neo-plasms, including TCC, and was strongly related to tu-mour differentiation. In addition, p53 expression was as-sociated with high-grade TCC, and an inverse relation-ship between p53 and cylin D1 was observed [21].
The only other published tumour karyotype also dis-played multiple structural and numerical abnormalities,including a rearrangement of chromosome 16 at q22, aswas seen in our case [2]. However, given the fact that thiscase and our own both showed multiple chromosomeabnormalities, with only the 16q abnormality in com-mon, it is difficult to make too many comparisons otherthan to note the cytogenetic complexity of this type oftumour. Perhaps the most interesting finding in our caseis the translocation between chromosome 9 and 22, giv-ing rise to two copies of the Philadelphia chromosome
and a presumed BCR/ABL rearrangement. Studies bySanchez-Garcia and Grutz using transformed murinehaematopoetic cells showed that the BCR-ABL onco-genes prevent apoptosis in these cells by inducing a bcl-2expression pathway.
The other notable cytogenetic abnormality seen here isthe structural rearrangement of the other two 22 chromo-somes not involved in the t(9;22) translocation. G-banding and FISH studies suggest the loss of at least partof q11. This is of interest in light of a number of reportsof deletion of 22q11 in malignant rhabdoid tumours[23,24]. Given the rhabdoid features described in ourcase, again it is possible to speculate that the 22q11 re-arrangement makes a direct contribution to this feature.Furthermore, given the fact that all four 22 chromosomescontain an abnormality of 22q11, it is possible that thereis a homozygous change in a gene or genes important inthe production of rhabdoid features.
In the original description of RMC, Davis et al. [1]named the tumour “the seventh sickle cell nephropathy.”In 33 of the 34 cases sickled erythrocytes were demon-strated within the renal tissue, and the patients weretherefore assumed to have SCT. The diagnosis of SCTwas confirmed in nine of these patients using haemoglo-bin electrophoresis. In our case, although the child wasknown to have SCT, no sickled erythrocytes were foundin the nephrectomy specimen. It is of interest that Davis’sgroup identified an identical tumour in a white femalewhere no sickled erythrocytes were found in the tissue,and Kalyanpur et al. [4] described another case in a whiteadolescent without sickle cell trait. It may therefore nolonger be helpful to consider this condition as a “sicklecell nephrectomy.” Davis et al. also carried out a detailedreview of the available clinical records of the 33 cases,and several notable features were highlighted. In particu-
Fig. 4. CK20 immunoreactivity of tumourcells is patchy. ×440.
Renal Medullary Carcinoma: Diagnosis and Treatment 555

lar RMC appeared to be a malignancy affecting relativelyyoung patients of African-American descent, which dis-played an extremely aggressive clinical course. All tu-mours extended beyond the renal capsule, and most weremetastatic to lymph nodes and beyond at the time ofpresentation. Although follow-up clinical informationwas not available in all cases, no patient was known tohave survived, and the mean duration of life followingsurgery was only 15 weeks. Avery et al. [2] describedfurther clinical information regarding six of these pa-tients (age range 24–36 years). All had metastatic diseaseat diagnosis and all died within 7 months of diagnosisdespite a variety of attempts at therapy. Treatments in-cluded multiagent chemotherapy regimens [cyclophos-phamide doxorubicin, and cisplatin (CAP); methotrexate,vinblastine, doxorubicin, and cisplatin (MVAC), topote-can, doxorubicin, and filgrastim], single-agent vinblas-tine,a-interferon, paclitaxel, and radiotherapy. Since thisfirst series of patients was described, nine further casereports have been published [3–10]. Interestingly all of
these and most of the Davis et al. series were right-sidetumours (Table II). Histologically all were thought to fitthe original description of RMC, and all except one wereassociated with SCT. In all cases the disease was fatal,and the durations of survival are shown in Table II. Avariety of further chemotherapy agents have been used,including 5-fluorouracil, vincristine, actinomycin, ifos-phamide, etoposide, carboplatin, and interleukin-2, but inno case has response to chemotherapy been demon-strated.
We present another case of RMC in a black child ofNigerian extraction also known to have SCT. Despiteextensive metastatic disease at presentation, this case isnotable as the first to show response to chemotherapy.Complete radiological response was demonstrated after 6courses of MVAC chemotherapy. This combination ofchemotherapy agents is used commonly in the treatmentof adults with TCC [25] and was chosen in this casebecause of the histological similarities between TCC andRMC. With the exception of one patient in the report by
Fig. 5. Cross section of proximal ureter, withtumour deposits displaying diffuse positivityfor bcl-2. Note positive expression in urothelialbasal cells. ×440.
Fig. 6. Karyotype of representative metaphase with84 chromosomes. The structurally abnormal chromo-somes are indicated with arrows. Note that only onecopy of the t(10;16) translocation is seen here. Theother four metaphases all contained two copies of thisrearrangement.
556 Stahlschmidt et al.

Davis et al., who survived 52 weeks following diagnosisand was described by the authors as having “indolentdisease,” survival was shorter in patients who were nottreated with chemotherapy or who showed no response totreatment. Although prolongation of survival and tempo-rary palliation were achieved in our patient, further at-tempts at treatment with these agents should be carriedout to determine whether this aggressive disease can becured.
REFERENCES
1. Davis CJ Jr, Mostofi FK, Sesterhenn IA. Renal medullary carci-noma. The seventh sickle cell nephropathy. Am J Surg Pathol1995;19:1–11.
2. Avery RA, Harris JE, Davis CJ Jr, et al. Renal medullary carci-noma: clinical and therapeutic aspects of a newly described tumor.Cancer 1996;78:128–132.
3. Friedrichs P, Lassen P, Canby E, Graham C. Renal medullarycarcinoma and sickle cell trait. J Urol 1997;157:1349.
4. Kalyanpur A, Schwartz DS, Fields JM, et al. Renal medulla car-cinoma in white adolescent. AJR 1997;169:1037–1038.
5. Adsay NV, deRoux SJ, Sakr W, Grignon D. Cancer as a marker ofgenetic medical disease: an unusual case of medullary carcinomaof the kidney. Am J Surg Pathol 1998;22:260–264.
6. Coogan CL, McKiel CF, Flanagan MJ, et al. Renal medullarycarcinoma in patients with sickle cell trait. Urology 1998;51:1049–1050.
7. Pickhardt PJ. Renal medullary carcinoma: an aggressive neoplasmin patients with sickle cell trait. Abdom Imaging 1998;23:531–532.
8. Larson DM, Gilstad CW, Manson GW, Henry MR. Renal med-
ullary carcinoma: report of a case with positive urinary cytology.Diagn Cytopathol 1998;18:276–279.
9. Wesche WA, Wilimas J, Khare V, Parham DM. Renal medullarycarcinoma: a potential sickle cell nephropathy of children andadolescents. Pediatr Pathol Lab Med 1998;18:97–113.
10. Pirich LM, Chou P, Walterhouse DO. Prolonged survival of apatient with sickle cell trait and metastatic renal medullary carci-noma. J Pediatr Hematol Oncol 1999;21:67–69.
11. Kerr JFR, Winterford CM, Harmon BV. Apoptosis. Its signifi-cance in cancer and cancer therapy. Cancer 1994;73:2013–2026.
12. Rodriguez-Jurado R, Gonzalez-Crussi F. Renal medullary carci-noma. J Urol Pathol 1996;4:191–203.
13. Schaafsma HE, Ramaekers FCS, van Muijen GNP, et al. Distri-bution of cytokeratin polypeptides in human transitional carcino-mas, with special emphasis on changing expression patterns dur-ing tumor progression. Am J Surg Pathol 1990;136:329–343.
14. Purkis PE, Steel JB, Mackenzie IC, et al. Antibody markers ofbasal cells in complex epithelia. J Cell Sci 1990;97:39–50.
15. Harnden P, Southgate J. Cytokeratin 14 as a marker of squamousdifferentiation in transitional cell carcinoma. J Clin Pathol 1997;50:1032–1033.
16. Moll R, Loewe A, Laufer J, Franke WW. Cytokeratin 20 in humancarcinomas. Am J Pathol 1992;140:427–447.
17. Dierick AM, Praet M, Roels H, et al. Vimentin expression of renalcell carcinoma in relation to DNA content and histological grad-ing: a combined light microscopic, immunocytochemical and cy-tophotometrical analysis. Histopathology 1991;18:315–322.
18. Parham DM, Morton K, Coghill G, et al. Expression of CD15antigen in urinary bladder transitional cell carcinoma. J ClinPathol 1990;43:541–543.
19. Korsmeyer SJ. Bcl-2: an antidote to programmed cell death. Can-cer Surv 1992;15:105–118.
20. Yang E, Korsmeyer SJ. Molecular thanatopsis: a discourse on theBCL2 family and cell death. Blood 1996;88:386–401.
21. Lee CCR, Yamamoto S, Morimura K, et al. Significance of cyclinD1 overexpression in transitional cell carcinomas of the urinarybladder and its correlation with histopathological features. Cancer1997;79:781–789.
22. Sanchez-Garcia I, Grutz G. Tumorigenic activity of the BCR-ABLoncogenes is mediated by bcl-2. Proc Natl Acad Sci USA 1995;92:5287–5291.
23. Rosty C, Martine P, Zucman J, et al. Cytogenetic and molecularanalysis of a t(1;22)(p36;q11.2) in a rhabdoid tumour with a pu-tative homozygous deletion of chromosome 22. Genes ChromCancer 1998;21:82–89.
24. Sawyer JR, Goosen LS, Swanson CM, et al. A new reciprocaltranslocation (12;22)(q24.3;q11.2–12) in a malignant rhabdoid tu-mour of the brain. Cancer Genet Cytogenet 1998;101:62–67.
25. Sternberg CN, Yagoda A, Scher HI, et al. Preliminary results ofM-VAC (methotrexate, vinblastine, doxorubicin and cisplatin) foradvanced transitional cell carcinoma of the urothelium. J Urol1985;133:402–407.
TABLE II. Summary of Previously Published Cases of RMC
ReferenceNumberof cases
Sideinvolved
Survival fromdiagnosis (weeks)
Davis et al. [1] 19 74% R 12 (Median)3–52 (range)
Friedrichs et al. [3] 1 R 20Kalyanpur et al. [4] 1 R 4Adsay et al. [5] 1 R 0Coogan et al. [6] 3 R 68
916
Pickhardt [7] 1 R 20Larson et al. [8] 1 R 9Wesche et al. [9] 1 R 4Pirich et al. [10] 1 R 60This case 1 R 49
Renal Medullary Carcinoma: Diagnosis and Treatment 557