Embed Size (px)
Citation preview

Renal medicine for the FinalFRCA
Aleksandra NowickaST7, UHCW08.05.2019

Acute kidney injury

Acute kidney Injury
Acute kidney injury (AKI) - a syndrome of abrupt decline in renal excretory and homeostatic function. This results in:
• bloodstream accumulation of products of nitrogenous metabolism
• failure to regulate– body fluid volume
– electrolyte concentrations
– Acid - base balance

Definition – KIDGO 2012
• An absolute increase in serum creatinine of ≥ 0.3 mg/dL (≥ 26.4 μmol)
• A percentage increase in serum creatinine of ≥ 150% (>1.5 fold from baseline)
• A reduction in urine output (< 0.5 ml/kg/hour for > 6 hours)

Continuing Education in Anaesthesia Critical Care & Pain, Volume 15, Issue 4, August 2015, Pages 213–218, https://doi.org/10.1093/bjaceaccp/mku030
The content of this slide may be subject to copyright: please see the slide notes for details.
Fig 1 Steady-state SCr plotted vs GFR in a 70-yr-old white male.

Continuing Education in Anaesthesia Critical Care & Pain, Volume 15, Issue 4, August 2015, Pages 213–218, https://doi.org/10.1093/bjaceaccp/mku030
The content of this slide may be subject to copyright: please see the slide notes for details.
Fig 2 Predicted change in normal GFR and SCr with age in a white
female. The same creatinine is associated with ...

Incidence
• Varies according to the sensitivity of definition
• ∼10% of all acute care hospitalizations
• 50% of patients admitted to intensive care units
• 7.5% patients with normal renal function undergoing non-cardiac surgery

AKI staging by KIDGO 2012
Serum creatinine criteria Urine output criteria
1 Increase in serum creatinine of ≥0.3 mg/dl (≥26.4 µmol/l)
or increase to ≥150% to 200% from baseline
<0.5 ml/kg/h for >6
hours
2 Increase in serum creatinine to >200% to 300% from
baseline
<0.5 ml/kg/h for > 12
hours
3 Increase in serum creatinine to >300% from baseline or
serum creatinine ≥4.0 mg/dl (≥354 µmol/l) with an acute
increase of ≥0.5 mg/dl (44 µmol/l) or
receiving renal replacement therapy
<0.3 ml/kg/h for 24
hours or anuria for 12
hours

Causes

Acute tubular necrosis
• Tubule cell damage and death
• Acute ischemic or toxic event (drug toxicity, intrarenal vasoconstriction and intratubularobstruction)

ATN Pathophysiology
• Hypoperfusion/ ischaemia/ inflammation/ toxins initiate cell injury
• Reduction in GFR– Reduced filtration due to hypoperfusion
– Casts and debris obstructing the tubule lumen, causing back-leak of filtrate through the damaged epithelium
• Inflammatory process causing further cellnecrosis, vasoconstriction and hypoperfusion

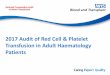
ATN Pathophysiology
Maintenance phase• Tubuloglomerular feedback - constriction of
afferent arterioles• stabilization of GFR at a very low level, and it
typically lasts 1-2 weeks. • Complications e.g. uremicRecovery phase• Regeneration of tubular epithelial cells• Abnormal diuresis occurs• Salt and water loss and volume depletion

Continuing Education in Anaesthesia Critical Care & Pain, Volume 15, Issue 4, August 2015, Pages 213–218,
https://doi.org/10.1093/bjaceaccp/mku030
The content of this slide may be subject to copyright: please see the slide notes for details.
Fig 3 Clinical course of AKI.

Chronic kidney disease

CKD
• Risk factor for serious postoperative complications
– Acute renal failure
– Cardiovascular complications
• Increased morbidity and mortality

Pathogenesis

Staging


Pathophysiology
Renal injury
Hyperfiltration and hypertrophy
Increased glomerular capillary pressuredamages capillaries
Secondary focal and segmentalglomerulosclerosis
Global gromerulosclerosis

Other factors causing progressive renalinjury
• Systemic hypertension• Uncontrolled diabetes• Proteinuria (in addition to being a marker of CKD) • Nephrotoxins (NSAIDs, intravenous contrast media) • Decreased perfusion (severe dehydration or episodes
of shock) • Episodes of AKI• Hyperlipidemia• Hyperphosphatemia with calcium phosphate
deposition• Smoking

Renal failure - pathophysiology

Cardiovascular• Systemic hypertension
– sodium and water retention – RAA activation
• Accelerated atherosclerosis and IHD– Low grade inflammation– Dyslipidemia
• Left ventricular hypertrophy and failure– Pressure overload: HTN– Volume overload – sodium/water retention; fistula– Anaemia
• Metastatic calcific valve lesions – Aortic calcification and aortic stenosis – Mitral calcification

Cardiovascular
• Conduction abnormalities – 2nd and 3rd degree AV block– Myocardial fibrosis – calcification in conduction system
• Sudden death from acute cardiac arrhythmias – IHD– Electrolyte imbalance
• Bacterial endocarditis • Haemorrhagic uraemic pericarditis is now uncommon
and occurs in patients receiving inadequate dialysis. • Postoperative pulmonary complications – atelectasis,
infection, fluid overload

Haemostasis and coagulation
• INR, APTT and platelet count usually normal• Tendency to excessive bleeding in the peri-operative period• Derranged platelet activity - decreased adhesiveness and
aggregation• Platelet dysfunction is not corrected by platelet transfusion
but can be improved by dialysis.• Rapid improvements in coagulation require the use of
pooled cryoprecipitate or DDAVP (which enhances release of von Willebrand factor)
• Bleeding tendency exacerbated by anaemia• Implications on regional anaesthetic techniques

Haemostasis and coagulation
There is also a tendency towards hypercoagulation
TEG studies show increase in all aspects of coagulation:
• Initial fibrin formation
• Fibrin–platelet interaction
• Qualitative platelet function

Anemia
• Decreased renal synthesis of erythropoietin- no reticulocyte response
• Normochromic normocytic anemia• Starts early in the course of the disease• Other causes
– Chronic blood loss: Uremia-induced platelet dysfunction enhances bleeding tendency
– Secondary hyperparathyroidism – Inflammation – Nutritional deficiency – Accumulation of inhibitors of erythropoiesis

Metabolic acidosis
• Normal anion gap - kidneys unable to produce enough ammonia in the proximal tubules to excrete the endogenous acid into the urine in the form of ammonium.
• In stage 5 CKD, accumulation of phosphates, sulfates, and other organic anions are the cause of the increase in anion gap.

Effects of acidosis
• Reduced ability to compensate for respiratory acidosis• Depression of myocardial contractility and reduced cardiac output• Altered drug distribution and efficacy• Negative effects on protein balance:
– Negative nitrogen balance – Increased protein degradation – Increased essential amino acid oxidation – Reduced albumin synthesis – Lack of adaptation to a low-protein diet
• Malnutrition, loss of lean body mass, and muscle weakness• Rapid progression of kidney disease• Renal osteodystrophy - bone acts as a buffer for excess acid
resultaning in loss of mineral

Salt- and water-handling abnormalities
• Clinically manifested when the GFR falls to less than 10-15 mL/min/1.73 m², when compensatory mechanisms become exhausted
• Failure of sodium and free-water excretion • Extracellular volume expansion and volume
overload– peripheral edema – pulmonary edema– hypertension
• At a higher GFR, excess sodium and water intake could result in a similar picture

Hyperkalemia
• Usually only develops when GFR falls to less than 20-25 mL/min/1.73 m²
• Sooner with potassium-rich diet or low serum aldosterone levels
• Common sources of low aldosterone levels are DM, ACE inhibitors, NSAIDs, beta-blockers
• Can be aggravated by an extracellular shift of potassium (acidemia or lack of insulin)
• Increased GI tract potassium excretion in CKD

Magnesium
• Handled by the kidney much like potassium
• Reduced excretion may causehypermagnesaemia, muscle weakness and potentiate non-depolarising muscle relaxants


Immune function
• Sepsis is a leading cause of death
• Inhibitionof cell-mediated immunity and humoral defence
• Little improvement following dialysis.
• Increased production of proinflammatory cytokines
• Superficial infections are common in fistula andcatheter sites
• Wound healing is poor
• Increased incidence of hepatitis C infection inpatients on haemodialysis

Gastrointestinal abnormalities
• Anorexia, nausea and vomiting
• Malnutrition
• GI bleeding (urea is a mucosal irritant)
• Gastric emptying is delayed, residual volume increased and pH lowered
• Peptic ulcer disease most patients take PPIs

Neurological abnormalities
• Wide spectrum of CNS changes. for example, from mild personality alterations to asterixis (i.e. lapse of posture, usually manifested by bilateral flapping tremor), myoclonus, encephalopathy and convulsions.
• Peripheralneuropathy– Common in advanced stages
– Initially ‚glove and stocking’ sensory loss
– Progresses to motor changes
• Autonomic neuropathy - delayed gastric emptying, postural hypotensionand silent myocardial ischaemia

Endocrine disturbances
• Changes in parathyroid function
• Impaired glucose tolerance; but reducedrequirement for exogenous insulin in diabetics, probably related to the reduced metabolism of insulin by the failing kidney
• Abnormalities of temperature regulation with reduced basal metabolic rate and a tendency to hypothermia. This is may be important when assessing fever.

Pharmacokinetic changes • Highly protein bound drugs
– Hypoalbuminaemia and acidosis increase free-drug availability– Doses of benzodiazepines and thiopental should be reduced by 30–50%.
• Propofol - pharmacodynamics unchanged • Highly ionised, lipid-insoluble drugs
– Elimination partially or completely dependent on renal excretion– Duration of action of a single loading dose will be dependent on redistribution rather than
excretion
• Renaly excreted hepatic metabolites may have far greater activity than the parent drug (morphine-6-glucuronide) or significant side-effects (nor-pethidine).
• Volatile anaesthetic agents– Elimination unaffected.– metabolism of sevoflurane will theoretically produce nephrotoxic fluoride ions
• Atracurium and cisatracurium are obvious choices for muscle relaxation but limited doses of vecuronium and rocuronium are acceptable alternatives.
• Plasma cholinesterase activity is not affected.• Anticholinesterases and anticholinergic agents – prolonged excretion.• Local anaesthetics
– Reduced duration of action– Maximum doses should be reduced by 25% (reduced protein binding and a lower CNS seizure
threshold)

Residual renal function in dialysispatients
24 h urine volume >100 ml
• Lower mortality risk
• Reduced intradialytic weight gain
• Improved solute clearance

Renal replacement therapy

Diffusion
• Haemodialysis• Fluid in the dialysis
compartment moves in a counter-current direction
• It is also possible for solutes (e.g. bicarbonate) to move in the opposite direction (e.g. from dialysate to blood)
• Better for small molecules(urea, creatinine, aminoacids)

Convection
• Pressure gradient is set up across the dialysis filter
• Water is pushed across the membrane and carries dissolved solutes with it; this is known as the solvent drag
• Ultrafiltration - the movement of fluid across the membrane as a result of this transmembrane pressure
• Convection - the process by which solutes move across the membrane is
• Good for small and largerparticles (Vit B12, vancomycin, B2 microglobulin, cytokines, complement)

Mechanisms of RRT
• Peritoneal dialysis,
• Intermittent haemdialysis (IHD)
• Continuous renal replacement therapy (CRRT)
– Continuous veno-venous haemofiltration (CVVH)
– Continuous veno-venous haemodialysis (CVVHD)
– Continuous veno-venous haemodiafiltration(CVVHDF)
• Renal transplant

Continuous RRT

BJA Education, Volume 17, Issue 3, March 2017, Pages 88–93, https://doi.org/10.1093/bjaed/mkw070
The content of this slide may be subject to copyright: please see the slide notes for details.
Fig 1 Circuit components. Continuous renal replacement therapy
requires a central double-lumen veno-venous ...

CVVH
• Blood flow rates - 100–200 ml/min• Replacement fluid infused into the blood with
the use of a replacement pump
• About 2 litres of ultrafiltrate removed each hour• Either all or part of the ultrafiltrate is replaced,
depending on the desired overall fluid balance

CVVHD
• Dialysate includes a buffer (acetic acid or bicarbonate) and essential electrolytes• Diffusion occurs down concentration gradients allowing rapid equilibration of
solutes across the membrane• Counter-current flow system is to maintain a waste-solute concentration gradient

CVVHDF
• Hybrid function
• Replacement and dialysate fluids are required - this is achieved with the same fluid solution

SCUF
• Slow continuous ultrafiltration
• Ultrafiltrate is formed at a rate of less than 300 ml/hour
• Replacement fluid is not infused.
• It can be useful when there is volume overload, but no solute accumulation (e.g. congestive cardiac failure).

Anticoagulation
• Coagulation cascade activated by contact with extracorporeal circuit
• Anticoagulation prolongs the life of filter– Systemic
• Heparin• LMWH• Prostacyclin
– Regional• Citrate• Heparin/protamine
– Endogenous coagulopathy

Dose
• Effective volume of effluent/kg/hr
• Optimal dose unknown
• Usually 25 - 50 ml/kg/hr

Indications for CRRT on ITU
• The criteria for initiating therapy include: – Hyperkalaemia (potassium >6.5 mmol l−1 or rapidly rising)
– Refractory fluid overload
– Metabolic acidosis
– Certain drug and alcohol intoxications
– Signs of uraemia, such as pericarditis or encephalopathy
– Temperature control; sepsis
• Criteria are based on expert opinion rather than evidence arising from randomized controlled trials
• Consider the severity of other organ failure and the trajectory of the patient’s illness

Intermittent haemodialysis
• Uses diffusion to remove solutes from plasma but can be combined with ultrafiltration to remove fluid.
• Blood and dialysis fluid are circulated in a counter-current fashion, but no replacement fluid is reinfused.
• Vas-cath (untunnelled or tunneled) A-V fistula or graft
• High dialysate flows (300-400 mls/min)
• Dialysate mixed from water and concentrate
• 3-4 hours
• Volume removed quickly, large fluid shifts, hypotension
• Increased brain water content

Peritoneal dialysis• Diffusion• Intraperitoneal catheter• Glucose rich dialysate inserted
and removed after dwell time• Most patients are on
continuous ambulatory PD • Three dialysate changes/day +
an overnight dwell• Problems
– Limited solute clearance– Peritonitis risk– Hyperglycemia– Protein loss– Interference with diaphragmatic
function