Embed Size (px)
Citation preview

Renal FailureRenal Failure

Renal FailureRenal Failure Results when kidney’s cannot remove Results when kidney’s cannot remove
wastes or perform regulatory functionswastes or perform regulatory functions Systemic disorder resulting from many Systemic disorder resulting from many
different causesdifferent causes ARF :ARF : Reversible syndrome that results in Reversible syndrome that results in
decreased GFR and oliguria (Fast & Days )decreased GFR and oliguria (Fast & Days ) CRF :CRF : Progressive ( Slow & Years ); Progressive ( Slow & Years );
Irreversible deterioration of renal function Irreversible deterioration of renal function resulting in azotemiaresulting in azotemia
Both types result in loss of ability to maintain normal Both types result in loss of ability to maintain normal volume and composition of body fluidsvolume and composition of body fluids

Assessment of Renal Assessment of Renal FunctionFunction
Glomerular Filtration Rate (GFR)Glomerular Filtration Rate (GFR) = The volume of water filtered from the plasma = The volume of water filtered from the plasma
per unit of time.per unit of time. Gives a rough measure of the number of Gives a rough measure of the number of
functioning nephronsfunctioning nephrons
Normal GFR:Normal GFR: Men: 130 mL/min./1.73m2Men: 130 mL/min./1.73m2 Women: 120 mL/min./1.73m2Women: 120 mL/min./1.73m2
Cannot be measured directly, so we use Cannot be measured directly, so we use creatininecreatinine and and creatinine clearancecreatinine clearance to to estimate.estimate.

Assessment of Renal Assessment of Renal FunctionFunction
CreatinineCreatinine As plasma creatinine increases, the As plasma creatinine increases, the
GFR exponentially decreases.GFR exponentially decreases. Limitations to estimate GFR:Limitations to estimate GFR:
Patients with decrease in muscle mass,, Patients with decrease in muscle mass,, malnutrition, advanced age, may have malnutrition, advanced age, may have low/normal creatinine despite underlying low/normal creatinine despite underlying kidney diseasekidney disease
Medications may artificially elevate creatinine:Medications may artificially elevate creatinine: Trimethroprim Trimethroprim CimetidineCimetidine

Assessment of Renal Assessment of Renal FunctionFunction
Creatinine ClearanceCreatinine Clearance Best way to estimate GFRBest way to estimate GFR GFR = (creatinine clearance) x (body GFR = (creatinine clearance) x (body
surface area in msurface area in m22/1.73)/1.73) Ways to measure:Ways to measure:
24-hour urine creatinine:24-hour urine creatinine: Creatinine clearance = (Ucr x Uvol)/ plasma CrCreatinine clearance = (Ucr x Uvol)/ plasma Cr
Cockcroft-Gault Equation:Cockcroft-Gault Equation:
(140 - age) x lean body (140 - age) x lean body weight [kg] weight [kg] CrCl (mL/min) = ——————————————— x CrCl (mL/min) = ——————————————— x 0.85 if0.85 if Cr [mg/dL] x 72 Cr [mg/dL] x 72 female female

Major causes of Kidney Major causes of Kidney FailureFailure
Prerenal DiseasePrerenal Disease Vascular DiseaseVascular Disease Glomerular DiseaseGlomerular Disease Interstitial/Tubular DiseaseInterstitial/Tubular Disease Obstructive UropathyObstructive Uropathy

Acute Renal Acute Renal FailureFailure
Relatively sudden onset of renal Relatively sudden onset of renal failure that is potentially failure that is potentially
reversiblereversible

Acute Renal FailureAcute Renal Failure An abrupt decrease in renal function sufficient to cause An abrupt decrease in renal function sufficient to cause
retention of metabolic waste such as urea and creatinine.retention of metabolic waste such as urea and creatinine. Most community acquired acute renal failure (70%) is prerenalMost community acquired acute renal failure (70%) is prerenal Most hospital acquired acute renal failure (60%) is due to Most hospital acquired acute renal failure (60%) is due to
ischemia or nephrotoxic tubular epithelial injury (acute tubular ischemia or nephrotoxic tubular epithelial injury (acute tubular necrosis).necrosis).
Mortality rate 50-70%Mortality rate 50-70% Risk factor for acute renal failureRisk factor for acute renal failure Advanced ageAdvanced age Preexisting renal parenchymal diseasePreexisting renal parenchymal disease Diabetes mellitusDiabetes mellitus Underlying cardiac or liver diseaseUnderlying cardiac or liver disease Early sign of ARF is oliguria.Early sign of ARF is oliguria.
Only seen in 2/3 of ARF pts.Only seen in 2/3 of ARF pts. Frequently have:Frequently have:
Metabolic acidosisMetabolic acidosis HyperkalemiaHyperkalemia Disturbance in body fluid homeostasisDisturbance in body fluid homeostasis Secondary effects on other organ systemsSecondary effects on other organ systems

Definition of Acute Renal Failure Definition of Acute Renal Failure Based on “Acute Kidney Injury Based on “Acute Kidney Injury
Network”Network”
StageStage Increase in Increase in Serum Serum
CreatinineCreatinine
Urine OutputUrine Output
11 1.5-2 times 1.5-2 times baseline baseline
OR OR 0.3 mg/dl 0.3 mg/dl
increase from increase from baselinebaseline
<0.5 ml/kg/h for <0.5 ml/kg/h for >6 h>6 h
22 2-3 times 2-3 times baselinebaseline
<0.5 ml/kg/h for <0.5 ml/kg/h for >12 h>12 h
33 3 times baseline 3 times baseline OR OR
0.5 mg/dl 0.5 mg/dl increase if increase if
baseline>4mg/dlbaseline>4mg/dlOROR
Any RRT given Any RRT given
<0.3 ml/kg/h for <0.3 ml/kg/h for >24 h>24 hOR OR
Anuria for >12 hAnuria for >12 h

RIFLE criteria for diagnosis of ARFRIFLE criteria for diagnosis of ARF based on The “Acute Dialysis Quality based on The “Acute Dialysis Quality
Initiative”Initiative”Increase in SIncrease in SCrCr Urine outputUrine output
RRisk of renal injuryisk of renal injury
IInjury to the kidneynjury to the kidney
FFailure of kidney ailure of kidney functionfunction
0.3 mg/dl increase0.3 mg/dl increase
2 X baseline2 X baseline
3 X baseline OR3 X baseline OR
> 0.5 mg/dl increase > 0.5 mg/dl increase if Sif SCrCr >=4 mg/dl >=4 mg/dl
< 0.5 ml/kg/hr for > < 0.5 ml/kg/hr for > 6 h6 h
< 0.5 ml/kg/hr for < 0.5 ml/kg/hr for >12h>12h
Anuria for >12 hAnuria for >12 h
LLoss of kidney oss of kidney functionfunction
EEnd-stage diseasend-stage disease
Persistent renal Persistent renal failure for > 4 weeksfailure for > 4 weeks
Persistent renal Persistent renal failure for > 3 failure for > 3 monthsmonths

Classification of ARFClassification of ARF
Acute Renal Failure
Pre-renal Intrinsic Post-renal
GlomerularInterstitial VascularTubular

Acute Renal FailureAcute Renal Failure
Pre Renal CausesPre Renal Causes
Post Renal Post Renal CausesCauses
Intrinsic Intrinsic causescauses
Tubular Interstitial Tubular Interstitial AcuteAcute Necrosis Nephritis Necrosis Nephritis GlomerulonephritisGlomerulonephritis (10% of cases) (10% of cases) (5% of cases)(5% of cases)
Ischemia Ischemia ToxinsToxins(50% of cases) (35% of (50% of cases) (35% of cases)cases)

Ischemic Acute Renal FailureIschemic Acute Renal Failure Intravascular volume depletion and hypotensionIntravascular volume depletion and hypotension Gastrointestinal, renal, dermal losses, hemorrhage, shockGastrointestinal, renal, dermal losses, hemorrhage, shock
Generalized Generalized or localized reduction in or localized reduction in renal blood flowrenal blood flow
IschemicIschemic Acute Renal FailureAcute Renal Failure
Decreased effective Decreased effective intravascular volume:intravascular volume: CHF, CHF, cirrhosis, nephrosis, peritonitiscirrhosis, nephrosis, peritonitis
Medications:Medications: ACE ACE inhibitors, NSAIDS, inhibitors, NSAIDS, radiocontrast agents, radiocontrast agents, Ampho B, CyclosporinAmpho B, Cyclosporin
Hepatorenal syndrome
Large vessel renal vascular disease: Renal artery thrombosis or embolism, Renal artery stenosis
Small vessel renal vascular disease:Small vessel renal vascular disease:Atheroembolism, vasculitis, malignant Atheroembolism, vasculitis, malignant hypertension, hypercalcemia, hypertension, hypercalcemia, transplant rejectiontransplant rejection
SepsisSepsis

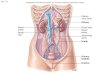
Effects of NSAIDS and ACE Effects of NSAIDS and ACE inhibitorsinhibitors
on Glomerular Hydrostatic Pressureon Glomerular Hydrostatic Pressure Prostaglandins causeProstaglandins causeafferent vaso afferent vaso dilationdilation
Locally produced AII causes efferent vaso constriction
Blocked by NSAIDS
Blocked by ACE inhibitors

Most common causes of ACUTE Most common causes of ACUTE Renal FailureRenal Failure
Prerenal Prerenal ( Community )( Community ) Acute Tubular Necrosis (ATN) – Acute Tubular Necrosis (ATN) –
( Hospitals )( Hospitals ) Acute on chronic renal failure (usually due Acute on chronic renal failure (usually due
to ATN or prerenal)to ATN or prerenal) Obstructive uropathyObstructive uropathy Glomerulonephritis/VasculitisGlomerulonephritis/Vasculitis Acute Interstitial nephritisAcute Interstitial nephritis AtheroemboliAtheroemboli

Major Disease Categories Major Disease Categories Causing ARFCausing ARF
Disease CategoryDisease Category IncidencIncidencee
Prerenal AzotemiaPrerenal Azotemia caused by acute renal caused by acute renal hypoperfusionhypoperfusion
55-60%55-60%
Intrinsic Renal AzotemiaIntrinsic Renal Azotemia caused by caused by acute diseases of renal parenchyma:acute diseases of renal parenchyma: -Large renal vessels dis.-Large renal vessels dis.
-Small renal vessels and glomerular dis.-Small renal vessels and glomerular dis.
-ATN (ischemic and toxic)-ATN (ischemic and toxic)
-Tubulo-interestitial dis.-Tubulo-interestitial dis.
-Intratubular obstruccttion-Intratubular obstruccttion
35-40%35-40%
*>90%**>90%*
Postrenal AzotemiaPostrenal Azotemia caused by acute caused by acute obstruction of the urinary tractobstruction of the urinary tract
<5%<5%

Prerenal AzotemiaPrerenal Azotemia Intravascular volume depletionIntravascular volume depletion
BBleeding, GI loss, Renal loss, Skin loss, Third leeding, GI loss, Renal loss, Skin loss, Third space lossspace loss
Decreased cardiac outputDecreased cardiac outputCHFCHF
Renal vasoconstrictionRenal vasoconstrictionLiver Disease, Sepsis, HypercalcemiaLiver Disease, Sepsis, Hypercalcemia
Pharmacologic impairment of Pharmacologic impairment of Autoregulation and GFR in specific Autoregulation and GFR in specific settingssettingsACEI in bilateral RAS, NSAIDS in any renal ACEI in bilateral RAS, NSAIDS in any renal hypoperfusion settinghypoperfusion setting

Renal Acute Renal FailureRenal Acute Renal Failure
Acute Tubular Acute Tubular Necrosis(ischaemic Necrosis(ischaemic or toxic)or toxic) [ATN] [ATN]
Interstitial nephritisInterstitial nephritis Glomerular diseaseGlomerular disease Renal Vascular Renal Vascular
DiseaseDisease MicrovascularMicrovascular VasoconstrictioVasoconstrictio
nn Tubular ObstructionTubular Obstruction
70% ATN70% ATN Drugs Drugs
(Aminoglycosides,NSA(Aminoglycosides,NSAIDs, Amphotericin)IDs, Amphotericin)
RhabdomyolysisRhabdomyolysis Iodinated contrast Iodinated contrast
agentsagents Heavy metalsHeavy metals Prolonged ischaemiaProlonged ischaemia Combination of the Combination of the
aboveabove

Intrinsic Renal AzotemiaIntrinsic Renal Azotemia Large Renal Vessel DiseaseLarge Renal Vessel Disease
Thrombo-embolic diseaseThrombo-embolic disease Renal Microvasculature and Glomerular DiseaseRenal Microvasculature and Glomerular Disease
Inflammatory:Inflammatory: glomerulonephritis, allograft rejection glomerulonephritis, allograft rejection
VasospasticVasospastic:: malignant hypertension, scleroderma crisis, pre-malignant hypertension, scleroderma crisis, pre-eclampsia, contrasteclampsia, contrastHematologicHematologic: HUS-TTP, DIC: HUS-TTP, DIC
Acute Tubular Necrosis (ATN)Acute Tubular Necrosis (ATN)IschemicIschemicToxicToxic
Tubulo-interestitial DiseaseTubulo-interestitial DiseaseAcute Interestitial Nephritis (AIN), Acute cellular allograft Acute Interestitial Nephritis (AIN), Acute cellular allograft rejection, viral (HIV, BK virus), infiltration (sarcoid)rejection, viral (HIV, BK virus), infiltration (sarcoid)
Intratubular ObstructionIntratubular Obstructionmyoglobin, hemoglobin, myeloma light chains, uric acid, tumor myoglobin, hemoglobin, myeloma light chains, uric acid, tumor lysis, drugs (indinavir, acyclovir, foscarnet, oxalate in ethylene lysis, drugs (indinavir, acyclovir, foscarnet, oxalate in ethylene glycol toxicity)glycol toxicity)

Acute Tubular NecrosisAcute Tubular Necrosis Most common form of “Renal” ARFMost common form of “Renal” ARF Tubular damage, loss of tubular function with Tubular damage, loss of tubular function with
direct effect on GFRdirect effect on GFR U/P osmol =1, U/P creatinine 10-20, UNa+ > 40 U/P osmol =1, U/P creatinine 10-20, UNa+ > 40
mmol/lmmol/l Duration days to 6 weeksDuration days to 6 weeks Oliguria most common but anuria and polyuria Oliguria most common but anuria and polyuria
possiblepossible Diuretics do not change course of ATN but can Diuretics do not change course of ATN but can
increase water excretionincrease water excretion High mortality even with dialysis (ATN High mortality even with dialysis (ATN
associated with other organ failure associated with other organ failure

Postrenal AzotemiaPostrenal Azotemia StonesStones Blood clotsBlood clots Papillary necrotic tissuePapillary necrotic tissue Urethral diseaseUrethral disease
Anatomic: Anatomic: posterior valveposterior valveFunctional: Functional: anticholinergics, L-DOPAanticholinergics, L-DOPA
Prostate diseaseProstate disease Bladder diseaseBladder disease
Anatomic:Anatomic: cancer, schistosomiasis cancer, schistosomiasisFunctional: Functional: neurogenic bladderneurogenic bladder

Urine Output in Acute Renal Urine Output in Acute Renal failurefailure
OliguriaOliguria = Daily urine output < 400 mL= Daily urine output < 400 mL When present in acute renal failure, associated When present in acute renal failure, associated
with a mortality rate of 75% (with a mortality rate of 75% (versus 25% versus 25% mortality rate in non-oliguric patients)mortality rate in non-oliguric patients)
Most deaths are associated with the underlying disease Most deaths are associated with the underlying disease process and infectious complicationsprocess and infectious complications
AnuriaAnuria No urine productionNo urine production Probably time for dialysisProbably time for dialysis

Phases of Acute Renal FailurePhases of Acute Renal Failure Phases of rapid decrease in renal Phases of rapid decrease in renal
function lead to the collection of function lead to the collection of metabolic wastes in the body.metabolic wastes in the body.
Phases include:Phases include: Oliguric Oliguric DiureticDiuretic Recovery Recovery
Acute syndrome may be reversible with Acute syndrome may be reversible with prompt intervention.prompt intervention.

Oliguric PhaseOliguric Phase1.1. Clinical picture dominated by surgical, medical Clinical picture dominated by surgical, medical
or obstetric problem causing ARFor obstetric problem causing ARF
2.2. Oliguria within 24-48 hours of initial injuryOliguria within 24-48 hours of initial injuryi.i. May take several days to develop with nephrotoxic May take several days to develop with nephrotoxic
chemicalschemicals
ii.ii. Azotemia accompanies oliguriaAzotemia accompanies oliguria
3.3. Critical to recognize, determine cause and begin Critical to recognize, determine cause and begin treatmenttreatment
4.4. Oliguria caused by acute-on-chronic RF usually Oliguria caused by acute-on-chronic RF usually easy to detect from historyeasy to detect from history
5.5. Post renal obstruction must be ruled outPost renal obstruction must be ruled out
6.6. Prerenal oliguria most common condition Prerenal oliguria most common condition leading to ARF and must be distinguished from leading to ARF and must be distinguished from ATNATN

Diuretic PhaseDiuretic Phase1.1. Begins when urine output increases to >400 Begins when urine output increases to >400
ml/dayml/day
2.2. Usually lasts 2-3 weeksUsually lasts 2-3 weeks
3.3. Urine output rarely exceeds 4 L/dayUrine output rarely exceeds 4 L/day
4.4. Caused partly by osmotic diuresis due to high Caused partly by osmotic diuresis due to high blood urea and partly by impaired ability of blood urea and partly by impaired ability of recovering tubules to conserve salts and waterrecovering tubules to conserve salts and water
5.5. May develop KMay develop K++, Na, Na++ and water deficits and water deficits
6.6. Must replace loses or deathMust replace loses or death7.7. BUN may continue to rise as clearance does not keep BUN may continue to rise as clearance does not keep
up with productionup with production
8.8. With continued diuresis azotemia gradually With continued diuresis azotemia gradually disappears and get clinical improvementdisappears and get clinical improvement

Recovery PhaseRecovery Phase1.1. Lasts up to one yearLasts up to one year
2.2. Anemia and concentrating ability gradually Anemia and concentrating ability gradually improveimprove
1.1. Some have permanent reduction in GFRSome have permanent reduction in GFR
3.3. ATN serious condition (still 50% mortality – ATN serious condition (still 50% mortality – down from 90% 30 years ago)down from 90% 30 years ago)
1.1. About 2/3 die during oliguric stage and about 1/3 About 2/3 die during oliguric stage and about 1/3 during diuretic stageduring diuretic stage
4.4. Mortality related to causeMortality related to cause1.1. 60% after surgery, crushing injuries60% after surgery, crushing injuries
2.2. 25% after CCl25% after CCl44, bad transfusion, bad transfusion
3.3. 10-15% in obstetric cases10-15% in obstetric cases
4.4. With non-oliguric ARF – 25% mortalityWith non-oliguric ARF – 25% mortality

Natural Clinical Course of ATNNatural Clinical Course of ATN Initiation Phase (hours to days)Initiation Phase (hours to days)
Continuous ischemic or toxic insultContinuous ischemic or toxic insultEvolving renal injuryEvolving renal injuryATN is potentially preventable at this timeATN is potentially preventable at this time
Maintenance Phase (typically 1-2 wks)Maintenance Phase (typically 1-2 wks)May be prolonged to 1-12 monthsMay be prolonged to 1-12 monthsEstablished renal injuryEstablished renal injuryGFR < 10 cc/min, The lowest UOPGFR < 10 cc/min, The lowest UOP
Recovery PhaseRecovery PhaseGradual increase in UOP toward post-ATN diuresisGradual increase in UOP toward post-ATN diuresis
Gradual fall in SGradual fall in SCrCr (may lag behind the onset of (may lag behind the onset of diuresis by several days)diuresis by several days)

ARF: Systemic ComplicationsARF: Systemic Complications Infections of urinary tract & lungs due to uremiaInfections of urinary tract & lungs due to uremia
Up to 70% of pts. with ARF. Up to 70% of pts. with ARF. #1 cause of ARF morbidity/mortality#1 cause of ARF morbidity/mortality
AnemiaAnemia Kidney makes EPO, Kidney makes EPO, ↓↓ EPO EPO anemia (HCT 20-30) anemia (HCT 20-30)
““33rdrd space disease” space disease” Salt and Water retention (esp. in prerenal failure)Salt and Water retention (esp. in prerenal failure) Pulmonary edema, Pleural effusion, & ascites Pulmonary edema, Pleural effusion, & ascites
HypocalcemiaHypocalcemia ↓↓ Excretion of phosphateExcretion of phosphate impaired GI absorption of Calcium. impaired GI absorption of Calcium.
HyperkalemiaHyperkalemia ↓↓ Glomerular filtration, Glomerular filtration, ↓↓ Tubular secretion Tubular secretion Malaise, nausea, and muscle weakness. Malaise, nausea, and muscle weakness. A cardiac emergencyA cardiac emergency
Metabolic Acidosis w/ Metabolic Acidosis w/ ↑↑ Anion Gap Anion Gap ↓↓ Excretion of acids & Excretion of acids & ↓↓ tubular reabsorption of bicarbonate tubular reabsorption of bicarbonate
results in metabolic acidosis with a high anion gap.results in metabolic acidosis with a high anion gap. Hypotension, Kussmaul’s respirationsHypotension, Kussmaul’s respirations

Initial Diagnostic Tools in Initial Diagnostic Tools in ARFARF
History and Physical examinationHistory and Physical examination Detailed review of the chart, drugs Detailed review of the chart, drugs
administered, procedures done, administered, procedures done, hemodynamics during the procedures.hemodynamics during the procedures.
Urinalysis (SG, PH, protein, blood, crystals, Urinalysis (SG, PH, protein, blood, crystals, infection )infection )
Urine microscopy {casts, cells (eosinophils)}Urine microscopy {casts, cells (eosinophils)} Urine Electrolytes Urine Electrolytes Renal imaging (US, CT Scan ,Retrograde Renal imaging (US, CT Scan ,Retrograde
Pyelogram )Pyelogram ) Markers of CKD (iPTH, size<9cm, anemia, Markers of CKD (iPTH, size<9cm, anemia,
high phosphate, low bicarbbonatehigh phosphate, low bicarbbonate Renal biopsyRenal biopsy

Assessing the patient with Assessing the patient with ARFARF
History:History: Cancer?Cancer? Recent Infections?Recent Infections? Blood in urine?Blood in urine? Change in urine output?Change in urine output? Flank Pain?Flank Pain? Recent bleeding?Recent bleeding? Dehydration? Diarrhea? Nausea? Dehydration? Diarrhea? Nausea?
Vomiting?Vomiting? Blurred vision? Elevated BP at home? Blurred vision? Elevated BP at home?
Elevated sugars?Elevated sugars?

Assessing the patient with ARFAssessing the patient with ARF
Family History:Family History: Cancers?Cancers? Polycystic kidney disease?Polycystic kidney disease?
Medications:Medications: Any non-compliance with diabetic or Any non-compliance with diabetic or
hypertensive meds?hypertensive meds? Any recent antibiotic use?Any recent antibiotic use? Any NSAID use?Any NSAID use?

Assessing the patient with ARF Assessing the patient with ARF Physical ExamPhysical Exam
Vital Signs:Vital Signs: Elevated BP: Concern for Elevated BP: Concern for malignant hypertensionmalignant hypertension Low BP: Concern for hypotension/hypoperfusion (Low BP: Concern for hypotension/hypoperfusion (acute acute
tubular necrosistubular necrosis)) Neuro:Neuro:
Confusion: Confusion: hypercalcemiahypercalcemia, uremia, , uremia, malignant malignant hypertension, hypertension, infection, malignancyinfection, malignancy
HEENT:HEENT: Dry mucus membranes: Concern for dehydration (Dry mucus membranes: Concern for dehydration (pre-renalpre-renal))
Abdomen:Abdomen: Ascites: Concern for liver disease (Ascites: Concern for liver disease (hepatorenal syndromehepatorenal syndrome), ),
or or nephrotic syndromenephrotic syndrome Extremities:Extremities:
Edema: Concern for Edema: Concern for nephrotic syndromenephrotic syndrome Skin:Skin:
Tight skin, sclerodactyly – Tight skin, sclerodactyly – Sclerodermal renal crisisSclerodermal renal crisis Malar rashMalar rash - Lupus - Lupus

Assessing the patient with ARFAssessing the patient with ARF Laboratory AnalysisLaboratory Analysis
Fractional Excretion of Sodium:Fractional Excretion of Sodium:
(Urine(UrineNa+Na+ x Plasma x PlasmaCreatinineCreatinine)) FEFENaNa= ______________________ x 100= ______________________ x 100
(Plasma(PlasmaNa+Na+ x Urine x UrineCreatinineCreatinine))
FEFENaNa < 1% → < 1% → Prerenal Prerenal
FEFENaNa > 2% → > 2% → ((Acute Tubular Necrosis),Acute Tubular Necrosis), obstructive uropathyobstructive uropathy
If patient receiving diuretics, can check FE of If patient receiving diuretics, can check FE of urea.urea.

Assessing the patient with ARF Assessing the patient with ARF RadiologyRadiology
Renal UltrasoundRenal Ultrasound Look for signs of hydronephrosis as sign Look for signs of hydronephrosis as sign
of obstructive uropathy.of obstructive uropathy.

Assessing the patient with ARFAssessing the patient with ARFUrinalysisUrinalysis
HematuriaHematuria Non-glomerular:Non-glomerular:
Urinary sediment: intact red blood cellsUrinary sediment: intact red blood cells Causes:Causes:
InfectionInfection CancerCancer Obstructive UropathyObstructive Uropathy
Rhabdomyolysis Rhabdomyolysis Myoglobinuria; Myoglobinuria; Hematuria with no RBCsHematuria with no RBCs
Glomerular:Glomerular: Urine sediment: dysmorphic red blood cells, red cell Urine sediment: dysmorphic red blood cells, red cell
castscasts Causes:Causes:
GlomerulonephritisGlomerulonephritis VasculitisVasculitis Atheroembolic diseaseAtheroembolic disease TTP/HUSTTP/HUS (Thombotic Microangiopathy) (Thombotic Microangiopathy)

Assessing Patient with ARFAssessing Patient with ARFUrinalysisUrinalysis (cont.)(cont.)
ProteinProtein Need microscopic urinalysis to see Need microscopic urinalysis to see
microabluminemiamicroabluminemia Can check 24-hour urine protein collectionCan check 24-hour urine protein collection
Nephrotic syndrome - ≥ 3.5 g protein in 24 hoursNephrotic syndrome - ≥ 3.5 g protein in 24 hours AlbuminuriaAlbuminuria
GlomerulonephritisGlomerulonephritis Atheroembolic diseaseAtheroembolic disease (TTP/HUS) Thrombotic microangiopathy(TTP/HUS) Thrombotic microangiopathy Nephrotic syndromeNephrotic syndrome
Tubular proteinuriaTubular proteinuria Tubular epithelial injury (acute tubular necrosis)Tubular epithelial injury (acute tubular necrosis) Interstitial nephritisInterstitial nephritis

Assessing patient with acute Assessing patient with acute renal failurerenal failure Urinary CastsUrinary Casts
Red cell castsRed cell casts GlomerulonephrGlomerulonephritisitis
VasculitisVasculitis
White Cell castsWhite Cell casts Acute Acute Interstitial Interstitial nephritisnephritis
Fatty castsFatty casts Nephrotic Nephrotic syndrome, syndrome, Minimal change Minimal change diseasedisease
Muddy Brown Muddy Brown castscasts
Acute tubular Acute tubular necrosisnecrosis

Urine Indices in ARFUrine Indices in ARF
> 500> 500 < 350< 350 < 350< 350
< 20< 20 > 40> 40 > 40> 40
> 20:1> 20:1 < 10:1< 10:1 < 10:1< 10:1
< 1%< 1%
<35%<35%>3%>3%
>55%>55%>3%>3%
>55%>55%Hyaline Hyaline
castscastsBrown, Brown,
Granular Granular casts,casts,
BlandBland
Pre Renal Intrinsic ATN
Post Renal
Uosm
Na (meq/L)
Bun/Cr (mg/dL)
FENa
Sediment
FEUrea

When to do Renal Biopsy in When to do Renal Biopsy in ARF?ARF?
If unable to discover cause of renal disease If unable to discover cause of renal disease Any evidence of glomerular diseaseAny evidence of glomerular disease
-Nephrotic range proteinuria-Nephrotic range proteinuria
-Sub-nephrotic range proteinuria with hematuria -Sub-nephrotic range proteinuria with hematuria
-RBC cast-RBC cast ARF in renal allograftARF in renal allograft Determine the prognosis and chance of Determine the prognosis and chance of
recovery of renal function in dialysis recovery of renal function in dialysis dependent ARF.dependent ARF.
Whenever potential Biopsy result can Whenever potential Biopsy result can change the management or prognosis.change the management or prognosis.

Treatment of Acute Treatment of Acute Renal FailureRenal Failure
Treat underlying causeTreat underlying cause Blood pressureBlood pressure InfectionsInfections Stop inciting medicationsStop inciting medications Nephrostomy tubes/ureteral stents if obstructionNephrostomy tubes/ureteral stents if obstruction Treat scleroderma renal crisis with ACE inhibitorTreat scleroderma renal crisis with ACE inhibitor
HydrationHydration Diuresis (Lasix)Diuresis (Lasix) Renal Replacement Therapy : Dialysis & Renal Renal Replacement Therapy : Dialysis & Renal
TransplantTransplant Pharmacologic treatments under study:Pharmacologic treatments under study:
Dopamine: no benefitDopamine: no benefit Atrial Natriuretic Peptide (ANP) or ANP-analogue (Anaritide): Atrial Natriuretic Peptide (ANP) or ANP-analogue (Anaritide):
promisingpromising

When to initiate RRT in a patient with When to initiate RRT in a patient with ARF?ARF?
1) Renal Replacement Therapy:1) Renal Replacement Therapy:Electrolytes imbalancesElectrolytes imbalancesAcid-base disturbancesAcid-base disturbancesUremic complicationsUremic complications
-Encephalopathy-Encephalopathy-Pericarditis-Pericarditis-Gastropathy -Gastropathy
2) Renal/Multiorgan Support Therapy2) Renal/Multiorgan Support Therapy-Protects other organs by improving overall body -Protects other organs by improving overall body milieu (balance of inflammatory mediators) milieu (balance of inflammatory mediators) -Allowing therapies for other organs that pt could -Allowing therapies for other organs that pt could not otherwise tolerate not otherwise tolerate
-Volume resuscitation-Volume resuscitation-Aggressive nutrition-Aggressive nutrition

3) Removal of toxic agents in overdose3) Removal of toxic agents in overdose
-Ethylene Glycol-Ethylene Glycol
-Methanol-Methanol
-Salicylates-Salicylates
-Lithium-Lithium
-Theophylline-Theophylline

Indications for HemodialysisIndications for Hemodialysis Refractory fluid overload Refractory fluid overload Hyperkalemia (plasma potassium concentration Hyperkalemia (plasma potassium concentration
>6.5 meq/L) or rapidly rising potassium levels >6.5 meq/L) or rapidly rising potassium levels Metabolic acidosis (pH less than 7.1) Metabolic acidosis (pH less than 7.1) Azotemia (BUN greater than 80 to 100 mg/dL )Azotemia (BUN greater than 80 to 100 mg/dL ) Signs of uremia, such as pericarditis, Signs of uremia, such as pericarditis,
neuropathy, or an otherwise unexplained neuropathy, or an otherwise unexplained decline in mental status decline in mental status
Severe dysnatremias (sodium concentration Severe dysnatremias (sodium concentration greater than 155 meq/L or less than 120 meq/L) greater than 155 meq/L or less than 120 meq/L)
Hyperthermia Hyperthermia Overdose with a dialyzable drug/toxin Overdose with a dialyzable drug/toxin

Chronic Renal FailureChronic Renal Failure
Chronic renal failure: Slowly progressive Chronic renal failure: Slowly progressive and non- reversible loss of kidney functionand non- reversible loss of kidney function
Uraemia:Uraemia: Metabolic outcome of chronic Metabolic outcome of chronic renal failurerenal failure
End-stage renal disease:End-stage renal disease: Requirement for Requirement for renal replacement therapyrenal replacement therapy

Chronic Kidney DiseaseChronic Kidney Disease = a GFR of < 60 for 3 months or more.= a GFR of < 60 for 3 months or more. Most common causes:Most common causes:
Diabetes MellitusDiabetes Mellitus HypertensionHypertension
Management:Management: Blood pressure control!Blood pressure control! Diabetic control!Diabetic control! Smoking cessationSmoking cessation Dietary protein restrictionDietary protein restriction Phosphorus lowering drugs/ Calcium replacementPhosphorus lowering drugs/ Calcium replacement
Most patients have some degree of hyperparathyroidismMost patients have some degree of hyperparathyroidism Erythropoietin replacementErythropoietin replacement
Start when Hgb < 10 g/dLStart when Hgb < 10 g/dL Bicarbonate therapy for acidosisBicarbonate therapy for acidosis Dialysis?Dialysis?

Stages of Chronic Kidney Stages of Chronic Kidney DiseaseDisease
StageStage DescriptionDescription GFR (mL/min/1.73 GFR (mL/min/1.73 m2)m2)
11 Kidney damage with Kidney damage with normal or increased normal or increased GFRGFR
≥ ≥ 9090
22 Kidney damage with Kidney damage with mildly decreased GFRmildly decreased GFR
60-8960-89
33 Moderately decreased Moderately decreased GFRGFR
30-5930-59
44 Severely decreased GFRSeverely decreased GFR 15-2915-29
55 Kidney Failure ( ESRD )Kidney Failure ( ESRD ) < 15< 15


Chronic Renal Failure
Factors causing progression
•Sustaining primary disease
•Systemic hypertension
• Proteinuria
• Nephrocalcinosis
• Dyslipidaemia
• Imbalance between renal energy demands and
supply
Progression of Chronic Renal Failure

What is ESRD?What is ESRD?
The deterioration of nephrons resulting in loss of The deterioration of nephrons resulting in loss of ability to excrete wastes, concentrate urine, and ability to excrete wastes, concentrate urine, and regulate electrolytes. regulate electrolytes.
Occurs as Occurs as chronic or acute renal failurechronic or acute renal failure progressing to the point where function is less progressing to the point where function is less than 15% of normal. than 15% of normal.
Function is so low that without dialysis or Function is so low that without dialysis or kidney transplantation, death will occur from kidney transplantation, death will occur from accumulation of fluids and waste products in accumulation of fluids and waste products in the body.the body.
ESRD almost always follows chronic kidney ESRD almost always follows chronic kidney failure, which may exist for 10 - 20 years or failure, which may exist for 10 - 20 years or more before progression to ESRD.more before progression to ESRD.

Chronic Renal FailureCommon causes of ESRD
Percentage incidencePercentage incidence
Diabetes mellitusDiabetes mellitus 5050
GlumerulonephritisGlumerulonephritis 1010
HypertensionHypertension 2020
Polycycstic kidney Polycycstic kidney diseasedisease
55
Vesicouretic refluxVesicouretic reflux 55
Analgesic nephropahtyAnalgesic nephropahty 55
OtherOther 55

CausesCauses
Hypertension
Congestive Heart Failure
Diabetes (most common cause)
Chronic Glomerulonephritis

CausesCauses
Aminoglycoside nephrotoxicity (Gentamycin)
IV contrast medium
Long term use of NSAIDS

CausesCauses
Nephrolithiasis
Prostate Cancer

CausesCauses
Systemic Lupus Erythrematosus
Polycystic Kidney Disease
Amyloidosis
Atherosclerosis

Chronic Renal FailureMain
consequencesMechanisMechanismm
ExampleExample ConsequenceConsequence
Decreased Decreased excretionexcretion
Uraemic toxinsUraemic toxins
Salt and waterSalt and water
PhosphatePhosphate
AcidAcid
PotassiumPotassium
Uraemic syndromeUraemic syndrome
Volume overload, Volume overload, hypertensionhypertension
HyperparathyroidismHyperparathyroidism
Metabolic acidoseMetabolic acidose
HyperkalaemiaHyperkalaemia
Decreased Decreased biosynthesbiosynthes
isis
ErythropoietinErythropoietin
Activation of Activation of vitamin Dvitamin D
AnaemiaAnaemia
Osteomalacia, Osteomalacia, HyperparathyroidismHyperparathyroidism
Altered Altered metabolismetabolis
mm
DyslipidaemiaDyslipidaemia
Sex hormonesSex hormonesAtherogenesisAtherogenesis
Abnormal reproductive Abnormal reproductive functionfunction


Symptoms of ESRDSymptoms of ESRD
Unintentional weight loss Nausea or vomiting
FatigueHeadache
Generalized itching Greatly decreased urine output
Easy bruising or bleeding Decreased alertness
drowsiness, somnolence, lethargy confusion, delirium , coma
Muscle twitching or cramps Seizures
Increased skin pigmentation Skin may appear yellow or brown
Nail abnormalities Decreased sensation in the hands, feet, or other areas

Chronic Renal Failure : Treatment
1. Differentiate from ARF
2. Establish aetiology
3. Establish severity
4. Treat reversible factors
5. Treat complication
6. Changes in lifestyle
7. Avoid or treat factors causing progression
8. Dialysis
9. Transplantation

TreatmentTreatment
Diseases that cause or result from Diseases that cause or result from chronic renal failure must be controlled.chronic renal failure must be controlled.
Hypertension, congestive heart failure, Hypertension, congestive heart failure, urinary tract infections, kidney stones, urinary tract infections, kidney stones, obstructions of the urinary tract, obstructions of the urinary tract, glomerulonephritis, and other disorders glomerulonephritis, and other disorders should be treated appropriatelyshould be treated appropriately
Dialysis or kidney transplantation are the Dialysis or kidney transplantation are the only treatments for ESRDonly treatments for ESRD

Pre-Dialysis TreatmentPre-Dialysis Treatment1.1. Maintain normal electrolytes Maintain normal electrolytes
2.2. Potassium, calcium, phosphate are major Potassium, calcium, phosphate are major electrolytes affected in CRF electrolytes affected in CRF
3.3. ACE inhibitors may be acceptable in many ACE inhibitors may be acceptable in many patients with creatinine >3.0mg/dL patients with creatinine >3.0mg/dL
4.4. ACE inhibitors may slow the progression of ACE inhibitors may slow the progression of diabetic and non-diabetic renal disease , diabetic and non-diabetic renal disease , Reduce or discontinue other renal toxins Reduce or discontinue other renal toxins (including NSAIDS) (including NSAIDS)
5.5. Diuretics (eg. furosemide) may help maintain Diuretics (eg. furosemide) may help maintain potassium in normal range potassium in normal range
6.6. Renal diet including high calcium and low Renal diet including high calcium and low phosphatephosphate

Permanent Vascular AccessPermanent Vascular Access

DialysisDialysis Method of removing toxic substances from the blood. Method of removing toxic substances from the blood.Blood is diverted from the access through a filter. The Blood is diverted from the access through a filter. The
blood flows counter-current to a special solution called the blood flows counter-current to a special solution called the dialysate. The electrolyte imbalances and toxins in the dialysate. The electrolyte imbalances and toxins in the
blood are corrected and returned to the body.blood are corrected and returned to the body.Peritoneal
Hemodialysis

HemodialysisHemodialysis
Works by circulating the blood, Works by circulating the blood, from an access in the body, from an access in the body, through a semi-permeable filter through a semi-permeable filter in the dialysis machine that in the dialysis machine that helps remove toxins. The helps remove toxins. The cleansed blood is then returned cleansed blood is then returned to the body. to the body.
Typically, most patients undergo Typically, most patients undergo hemodialysis for three sessions hemodialysis for three sessions every week. Each session lasts every week. Each session lasts 3-4 hours3-4 hours
Patients on hemodialysis are Patients on hemodialysis are always always heparinized heparinized to prevent to prevent clotting of the AV access.clotting of the AV access.
Indicated in chronic tx and Indicated in chronic tx and obese patientsobese patients

Hemodialysis : Indications Hemodialysis : Indications
1)1) Uremia - azotemia with symptoms and/or Uremia - azotemia with symptoms and/or signs signs
2)2) Severe Hyperkalemia Severe Hyperkalemia
3)3) Volume Overload - usually with congestive Volume Overload - usually with congestive heart failure (pulmonary edema) heart failure (pulmonary edema)
4)4) Toxin Removal - ethylene glycol poisoning, Toxin Removal - ethylene glycol poisoning, theophylline overdose, etc. theophylline overdose, etc.
5)5) An arterio-venous fistula in the arm is An arterio-venous fistula in the arm is created surgically created surgically
6)6) Catheters are inserted into the fistula for Catheters are inserted into the fistula for blood flow to dialysis machineblood flow to dialysis machine

Complications of HemodialysisComplications of Hemodialysis
Dialysis disequilibrium syndromeDialysis disequilibrium syndrome Infectious diseasesInfectious diseases Hepatitis B and C infectionsHepatitis B and C infections HIV exposure—poses some risk for HIV exposure—poses some risk for
patients undergoing dialysispatients undergoing dialysis

PeritonealPeritoneal Works by using the body's peritoneal membrane, Works by using the body's peritoneal membrane,
inside the abdomen, as a semi-permeable inside the abdomen, as a semi-permeable membrane.membrane.
Solutions that help to remove toxins are infused Solutions that help to remove toxins are infused in, remain in the abdomen for a certain time in, remain in the abdomen for a certain time period, and are eventually drained out. period, and are eventually drained out.
This can be done at home on a continuous basis. This can be done at home on a continuous basis. (CAPD )(CAPD )
Indicated in patients with ARF, require occasional Indicated in patients with ARF, require occasional dialysis, or those who are young and have the dialysis, or those who are young and have the capability of doing this at home.capability of doing this at home.
Types of peritoneal dialysis:Types of peritoneal dialysis: Continuous ambulatory peritonealContinuous ambulatory peritoneal Automated peritonealAutomated peritoneal Intermittent peritonealIntermittent peritoneal Continuous-cycle peritonealContinuous-cycle peritoneal

ComplicationsComplications
PeritonitisPeritonitis PainPain Exit site and tunnel infectionsExit site and tunnel infections Poor dialysate flowPoor dialysate flow Dialysate leakageDialysate leakage Other complicationsOther complications

Renal TransplantationRenal Transplantation
Candidate selection criteriaCandidate selection criteria DonorsDonors Preoperative carePreoperative care Immunologic studiesImmunologic studies Surgical teamSurgical team Operative procedureOperative procedure


Renal FailureDifferentiation between ARF & CRF
AcuteAcute ChronicChronic
HistoryHistory Short (days-week)Short (days-week)Long Long (month-years)(month-years)
Haemoglobin concentrationHaemoglobin concentration NormalNormal LowLow
Renal sizeRenal size NormalNormal ReducedReduced
Renal osteodystrophyRenal osteodystrophy AbsentAbsent PresentPresent
Peripheral neuropathyPeripheral neuropathy AbsentAbsent PresentPresent
Serum Creatinine Serum Creatinine concentrationconcentration
Acute reversible Acute reversible increaseincrease
Chronic Chronic irreversible irreversible

Acute Interstitial/Tubular Acute Interstitial/Tubular DiseaseDisease
Acute Tubular NecrosisAcute Tubular Necrosis:: One of the most causes of acute renal failure in hospitalized One of the most causes of acute renal failure in hospitalized
patientspatients Causes:Causes:
Hypotension, SepsisHypotension, Sepsis Toxins: Aminoglycosides, Amphotericin,, Pentamadine, Toxins: Aminoglycosides, Amphotericin,, Pentamadine, IV IV
contrastcontrast Rhabdomyolysis Rhabdomyolysis (heme-pigments are toxins)(heme-pigments are toxins)
Urine sediment: Urine sediment: muddy brown granularmuddy brown granular castscasts Acute Interstitial NephritisAcute Interstitial Nephritis::
Causes:Causes: Drugs: Antibiotics, Proton-pump inhibitors, Drugs: Antibiotics, Proton-pump inhibitors, NSAIDSNSAIDS, ,
allopurinolallopurinol Infections: Legionella, LeptospirosisInfections: Legionella, Leptospirosis Auto-immune disordersAuto-immune disorders
Urine sediment: Urine sediment: urine eosinophils urine eosinophils (but not always (but not always present),present), white blood cells, red blood cells, white cell castswhite blood cells, red blood cells, white cell casts
Cast NephropathyCast Nephropathy – Multiple Myeloma – Multiple Myeloma Tubular casts – PAS-negative, and PAS-positive (Tamm-Horsefall Tubular casts – PAS-negative, and PAS-positive (Tamm-Horsefall
mucoprotein)mucoprotein)

Chronic Interstitial Tubular Chronic Interstitial Tubular DiseaseDisease
Polycystic Kidney DiseasePolycystic Kidney Disease HypercalcemiaHypercalcemia Autoimmune disordersAutoimmune disorders
SarcoidosisSarcoidosis Sjögren’s syndromeSjögren’s syndrome

Increase in Creatinine without Increase in Creatinine without ARFARF
Inhibition of tubular creatinine Inhibition of tubular creatinine secretionsecretion
Trimethoprim, Cimetidine, ProbenecidTrimethoprim, Cimetidine, Probenecid
Interference with creatinine assays in Interference with creatinine assays in the lab (false elevation)the lab (false elevation)
glucose, acetoacetate, ascorbic acid, glucose, acetoacetate, ascorbic acid, cefoxitincefoxitin
flucytosineflucytosine

Increase in BUN without ARFIncrease in BUN without ARF
Increased productionIncreased production
GI BleedingGI Bleeding
Catabolic states (Prolonged ICU stay)Catabolic states (Prolonged ICU stay)
CorticosteroidsCorticosteroids
Protein loads (TPN-Albumin infusion)Protein loads (TPN-Albumin infusion)

New Biomarkers in ARFNew Biomarkers in ARFAlternatives to Serum CreatinineAlternatives to Serum Creatinine
Urinary Neutrophil Gelatinase-Associated Urinary Neutrophil Gelatinase-Associated Lipocalin (NGAL)Lipocalin (NGAL)
Urinary Interleukin 18Urinary Interleukin 18
Urinary Kidney Injury Molecule 1 (KIM-1)Urinary Kidney Injury Molecule 1 (KIM-1)

Is there a role for Dopamine in prevention Is there a role for Dopamine in prevention or treatment of ARF in ICU setting?or treatment of ARF in ICU setting?
Clinical Outcomes:Clinical Outcomes: No effect on mortalityNo effect on mortality No effect on the need for or incidence of Renal No effect on the need for or incidence of Renal
Replacement Therapy (RRT)Replacement Therapy (RRT)
Renal Physiologic Outcomes:Renal Physiologic Outcomes: Diuretic effect and increased creatinine clearance Diuretic effect and increased creatinine clearance
on the first day which was not significant on the on the first day which was not significant on the following days.following days.
Adverse effect:Adverse effect: on the immune, respiratory, and endocrine system. on the immune, respiratory, and endocrine system.

Role of ANP analogues in ARF ?Role of ANP analogues in ARF ?
61 patients in 2 cardiothoracic ICU with post-op 61 patients in 2 cardiothoracic ICU with post-op ARF assigned to receive recombinent ANP ARF assigned to receive recombinent ANP (50ng/kg/min) or placebo(50ng/kg/min) or placebo
The need for RRT before day 21 after The need for RRT before day 21 after development of ARF was significantly lower in development of ARF was significantly lower in ANP group (21% vs 47%)ANP group (21% vs 47%)
The need for RRT or death after day 21 was The need for RRT or death after day 21 was significantly lower in ANP group (28% vs 57%)significantly lower in ANP group (28% vs 57%)

Is there a role for Fenoldepam in prevention Is there a role for Fenoldepam in prevention or treatment of AKI in ICU setting?or treatment of AKI in ICU setting?
Dopamine-1 receptor agonist, lack of Dopamine-Dopamine-1 receptor agonist, lack of Dopamine-2, and alpha-1 receptor effect, make it a 2, and alpha-1 receptor effect, make it a potentially safer drug than Dopamine!potentially safer drug than Dopamine!
Reduces in hospital mortality and the need for Reduces in hospital mortality and the need for RRT in ARFRRT in ARF
Reverses renal hypoperfusion more effectively Reverses renal hypoperfusion more effectively than renal dose Dopaminethan renal dose Dopamine
So far so good specially in cardiothoracic ICU So far so good specially in cardiothoracic ICU patients, awaiting more powered trials in other patients, awaiting more powered trials in other groups! groups!

Is there a role for diuretics in the treatment Is there a role for diuretics in the treatment of ARF in ICU setting?of ARF in ICU setting?
PICARDPICARD Study: Study:
Cohort study of 552 pts in 4 UC hospitals:Cohort study of 552 pts in 4 UC hospitals:
Odds Ratio Odds Ratio
In-hospital MortalityIn-hospital Mortality 1.771.77
Non-recovery of renal functionNon-recovery of renal function 1.681.68
Improved urine output and shorter duration of RRT Improved urine output and shorter duration of RRT (none has clinical relevance in ICU pts)(none has clinical relevance in ICU pts)
But diuretics continue to be used for volume control But diuretics continue to be used for volume control in ARF in ICU setting!in ARF in ICU setting!

CRRT vs SLEDCRRT vs SLED (Sustained low efficiency dialysis) (Sustained low efficiency dialysis)
SLED became popular because of CRRT SLED became popular because of CRRT disadvantages:disadvantages: Expensive, continuous pt immobilization, need for specialized Expensive, continuous pt immobilization, need for specialized
machines and pre-mixed commercial solutions, and machines and pre-mixed commercial solutions, and anticoagulationanticoagulation
Only 2 small studies compared these 2 in Only 2 small studies compared these 2 in hemodynamically unstable pts with ARFhemodynamically unstable pts with ARF
They did not see significant differences in They did not see significant differences in hemodynamic parameters and solute clearancehemodynamic parameters and solute clearance
They did not look at any patient-relevant They did not look at any patient-relevant outcomes, so the jury is still out thereoutcomes, so the jury is still out there

Overall conclusion on RRT modality Overall conclusion on RRT modality benefit in ARFbenefit in ARF
CRRT does not confer a survival advantage as CRRT does not confer a survival advantage as compared to IHDcompared to IHD
SLED may replace CRRT although there is no SLED may replace CRRT although there is no outcome benefit study up to this dateoutcome benefit study up to this date
There is limited data regarding the ideal timing There is limited data regarding the ideal timing of RRT initiation and the preferred mode of of RRT initiation and the preferred mode of solute clearancesolute clearance
No evidence to support a more intensive strategy No evidence to support a more intensive strategy of RRT in the setting of AKIof RRT in the setting of AKI