Embed Size (px)
Citation preview

Renal Dysfunction in Heart Failure Patients with Preserved versus Reduced
Ejection Fraction: Impact of the New CKD-EPI Formula
McAlister et al: Renal Dysfunction in Heart Failure
Finlay A. McAlister,1 MD MSc; Justin Ezekowitz,2 MB BCh MSc; Luigi Tarantini,3 MD;
Iain Squire, MB ChB MD4; Michel Komajda, MD5; Antoni Bayes-Genis, MD6;
Israel Gotsman, MD7; Gillian Whalley, PhD8,9; Nikki Earle, BSc9; Katrina K. Poppe, PhD9;
Robert N. Doughty,9 MD; For the Meta-analysis Global Group in Chronic Heart Failure
(MAGGIC) Investigators
The Divisions of 1General Internal Medicine and 2Cardiology, University of Alberta, Edmonton, Canada; 3The Department of Cardiology, San Martino Hospital, Belluno, Italy; 4The University of Leicester, and NIHR Biomedical Research Unit, Glenfield Hospital, Leicester, United Kingdom; 5The Pitie Salpetriere Hospital Cardiovascular Division, Paris, France; 6Hospital Universitari Germans Trias i Pujol, Department of Medicine, UAB, Barcelona, Spain; 7The Heart Institute, Hadassah University Hospital, Jerusalem, Israel; 8UniTec, Auckland, New Zealand; 9Department of Medicine, The University of Auckland, New Zealand
Correspondence to Dr. F. McAlister, 2F1.21 WMC, University of Alberta Hospital 8440 112 Street, Edmonton, Alberta, Canada T6G 2R7 Tele: (780) 407-1657 Fax: (780) 407-3132 E-mail: [email protected] Journal Subject Codes: Cardio-renal physiology/ pathophysiology, Epidemiology, Congestive heart failure
nnnnnnnivivivivivivivererererererersisisisisisisitytytytytytyty o o ooooof f fffff AlAlAlAlAlAlAlbbbbbbbBelllllllllllununuuuuu o,o,,,,, IIII IIItatatatatataalylylylylylyly;;;;; ; ; 4444444
HR Biomedical Research Unit, Glenfield Hospital, Leicesterhe Salpetriere Hospital Cardiovascular Division, Paris, Francen SU Nd
HR Biomedical Research Unit, Glenfield Hospital, Leicesterhe Salpetriere Hospital Cardiovascular Division, Paris, Francens Trias i Pujol, Department of Medicine, UAB, Barcelona, SUniversity Hospital, Jerusalem, Israel; 8UniTec, Auckland, Ndicine, The University of Auckland, New Zealand
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
arch 25, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on M
arch 25, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

Abstract
Background—Prior studies in heart failure have used the Modification of Diet in Renal Disease
(MDRD) equation to estimate Glomerular Filtration Rate (eGFR). The Chronic Kidney Disease
– Epidemiology Collaboration Group equation (CKD-EPI) more accurately estimates GFR than
the MDRD when compared against the radionuclide gold standard. The prevalence and
prognostic import of renal dysfunction in HF if the CKD-EPI equation is used rather than the
MDRD is uncertain.
Methods and Results—We used individual patient data from 25 prospective studies to stratify
heart failure patients by eGFR using the CKD-EPI and the MDRD equations and examined
survival across eGFR strata. In 20 754 patients (15 962 with reduced ejection fraction [HF-REF]
and 4792 with preserved ejection fraction [HF-PEF], mean age 68 years, 151 [95%CI 146-155]
deaths per 1000 patient-years), 10 589 (51%) had eGFR < 60 ml/min using the MDRD equation
and 11 422 (55%) using the CKD-EPI equation. Using the CKD-EPI equation resulted in 3760
(18%) patients being re-classified into different eGFR risk strata; 3089 (82%) were placed in a
lower eGFR category and exhibited higher all-cause mortality rates (net reclassification
improvement with CKD-EPI 3.7%, 95% CI 1.5% to 5.9%). Reduced eGFR was a stronger
predictor of all-cause mortality in HF-REF than HF-PEF.
Conclusions—Use of the CKD-EPI equation rather than the MDRD to calculate eGFR leads to
higher estimates of renal dysfunction in heart failure and more accurate categorization of
mortality risk. Renal function is more closely related to outcomes in HF-REF than in HF-PEF.
Key Words: renal function, heart failure, prognosis
uced ejection frfrrrrraa
88 yeyeeeeeeararararararars,s,s,ssss 1 11111151515151515151 [ [ [ [ [ [ [95959595959595
ent-years), 10 589 (51%) had eGFR < 60 ml/min using the M
s e
g e
r f
CKD-EPI 3.7%, 95% CI 1.5% to 5.9%). Reduced eGFR was
ent-years), 10 589 (51%) had eGFR < 60 ml/min using the M
sing the CKD-EPI equation. Using the CKD-EPI equation re
g re-classified into different eGFR risk strata; 3089 (82%) wet
ry and exhibited higher all-cause mortality rates (net reclassif
CKD-EPI 3.7%, 95% CI 1.5% to 5.9%). Reduced eGFR was
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

It is well recognized that renal dysfunction is common in patients with heart failure (HF)
and is an adverse prognostic factor.1-8 While prior studies examining the prevalence and
prognostic import of renal dysfunction in HF have used the Modification of Diet in Renal
Disease (MDRD) equation to estimate Glomerular Filtration Rate (eGFR),9 recent studies
comparing MDRD-generated eGFRs against radionuclide gold standards have demonstrated that
the MDRD systematically underestimates true eGFR, particularly in those with an eGFR >60.10
Thus, studies using the MDRD equation to calculate eGFRs may overestimate the prevalence of
renal dysfunction in study participants.11 In clinical practice, patients misclassified as having
renal dysfunction may be exposed to potential harms since such patients are often treated with
lower doses of drugs and diagnostic tests using contrast media are avoided.
In 2009, the Chronic Kidney Disease – Epidemiology Collaboration Group developed,
and validated in 8254 patients, a new equation (CKD-EPI) for estimating GFR which is more
accurate than the MDRD when compared against the radionuclide gold standard.12 However,
few patients in the CKD-EPI validation studies had HF and the true prevalence and prognostic
import of renal dysfunction in HF if the CKD-EPI equation is used rather than the MDRD is
uncertain. In addition, it is unknown whether renal dysfunction prevalence and prognostic
importance differs between HF patients with reduced ejection fraction (HF-REF) and those with
preserved ejection fraction (HF-PEF). In particular, there is debate about whether risk truly
increases at eGFR < 60 ml/min or whether lower eGFR levels might be a more appropriate cut-
point to identify at-risk individuals since most patients with HF are elderly and eGFR declines
with age.11
Thus, we designed this study to examine the frequency of renal dysfunction in HF
patients using the CKD-EPI and the MDRD formulae, and to examine the association between
renal dysfunction and mortality in patients with HF-REF and HF-PEF.
re avovovovovovovoidididididididededededededed.. .
u
54 patients, a new equation (CKD-EPI) for estimating GFR w
D
CKD EPI lid i di h d HF d h l
Chronic Kidney Disease – Epidemiology Collaboration Grou
54 patients, a new equation (CKD-EPI) for estimating GFR w
DRD when compared against the radionuclide gold standard
CKD EPI lid i di h d HF d h l
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Methods
The methods, including details about study selection criteria and the flow of included
studies, and main results of the MAGGIC meta-analysis have been described in full elsewhere.13
For this analysis, we pooled individual patient data from the 25 studies in the MAGGIC meta-
analysis (2 pharmacotherapy RCTs, 4 management strategy RCTs and 19 observational studies)
that included data on serum creatinines and collected all-cause mortality outcomes prospectively
in HF patients and did not restrict their study entry criteria by left ventricular ejection fraction
(LVEF). The meta-analysis protocol was approved by The University of Auckland Human
Subjects Ethics Committee. Data (including demographics, comorbidities, therapy, symptom
status, clinical variables, laboratory variables, and outcome) from the individual studies were re-
coded into a uniform format at the Central Coordinating Centre at the University of Auckland
and incorporated into one database.
For this analysis, HF-PEF was pre-specified as baseline LVEF 50% and we defined
renal dysfunction as eGFR < 60 ml/min, corresponding to National Kidney Foundation Kidney
Disease Outcomes Quality Initiative (NKF KDOQI) stages 3 and 4 kidney disease.14 Covariates
were all defined at baseline, including anemia (hemoglobin less than 120g/L in women and
130g/L in men). We calculated eGFR by two methods. For the MDRD equation, none of the
studies used isotope dilution to measure creatinine and thus we used 186 x (serum creat) -1.154 x
age (yrs) -0.203 x (0.742 if female) x (1.212 if black). For the CKD-EPI equation, we used eGFR=
141 x min (SCr/k,1)a, x max (SCr/k,1)-1.209 x 0.993Age x [1.159 if Black], where Scr is serum
creatinine, k is 0.7 for females and 0.9 for males, a is -0.329 for females and -0.411 for males,
min indicates the minimum of Scr/ k or 1, and max indicates the maximum of Scr/ k or 1.
Data are described as mean (standard deviation) unless otherwise stated. Tests for linear
trend were constructed from orthogonal contrasts for continuous variables and using the
m thehehehehehehe i iiiiiindndndndndndndivivivivivivividididididididuauauauauauauallllll l
m y
y d
GFR 60 l/ i di N i l Kid F
m format at the Central Coordinating Centre at the University
o one database.
ysis, HF-PEF was pre-specified as baseline LVEF 50% and
GFR 60 l/ i di N i l Kid F
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Cochran-Armitage Trend Test for ordered categorical data. Confidence intervals around person
time rates were calculated using Miettinen’s exact test (www.openepi.com, accessed September
19 2011). Areas under the receiver operating characteristics (ROC) curve (AUC) were compared
using the ROCCONTRAST option of Logistic regression procedure of SAS. The Cox
proportional hazard of time to all cause death within 3 years from baseline study visit was used
to model the hazard of varying degrees of renal dysfunction (strata generated using the MDRD
and the CKD-EPI formulae separately), adjusted for age, sex, ischemic etiology, anemia,
hypertension, diabetes, and atrial fibrillation and stratified by study. The variables chosen for the
model were selected for clinical relevance - data were available for these variables in more than
94% of the patients in this analysis. Models were constructed from those individuals with
complete data for each model. No imputation of missing data was employed. Unless otherwise
stated, the procedures of SAS v9.2 (SAS Institute Inc) were used for all analyses. All tests were
two-tailed and P<0.05 was considered significant.
Results
In 20754 patients with heart failure (15962 with HF-REF and 4792 with HF-PEF, mean
age 68 years, 66% men), all-cause mortality was 24% over median follow-up of 2.0 years (150.5
[95%CI 146.3-154.7] deaths per 1000 patient-years). There were 136.7 (95%CI 128.2-145.7)
deaths per 1000 patient-years in those with HF-PEF and 154.1 (95% CI 149.4-158.9) deaths per
1000 patient-years in those with HF-REF.
Patients with HF-REF were more likely to be male and to have ischemic etiology and
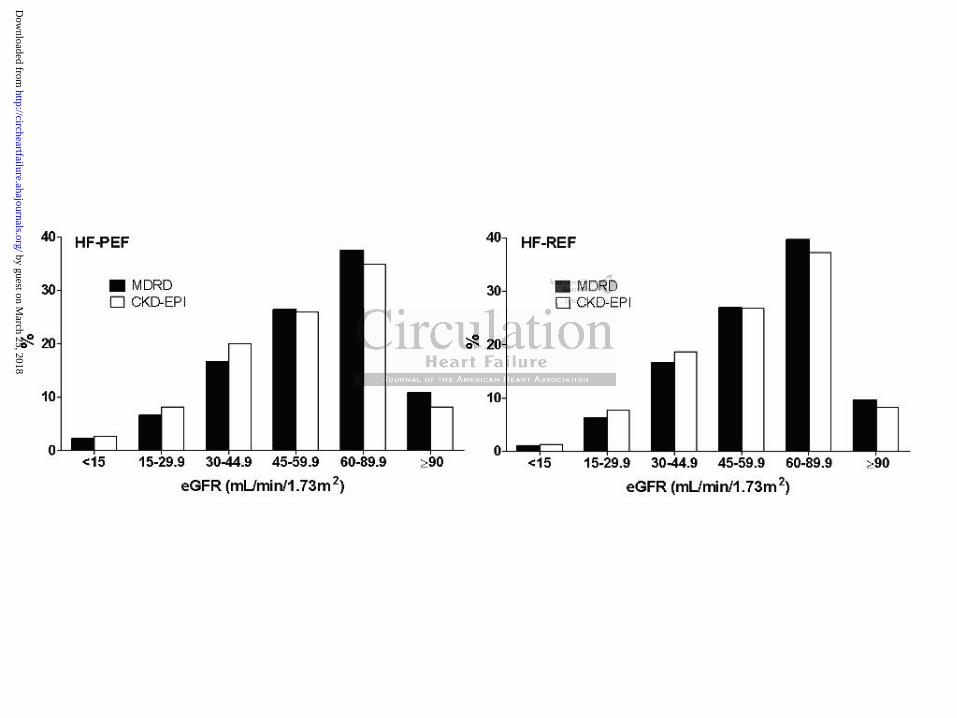
diabetes mellitus (Table 1, comparisons done using Chi-square tests). The distribution of eGFR
was similar in patients with HF-PEF and in those with HF-REF (Figure 1). Patients with lower
om thththththththososososososose e eeeee ininininininindididididididivivivivivivividdddddd
a U
e s
0
ach model. No imputation of missing data was employed. U
es of SAS v9.2 (SAS Institute Inc) were used for all analyses
05 was considered significant.
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

eGFRs exhibited worse HF symptom status, higher comorbidity burdens, and lower use of
cardiovascular medications (Table 1, all p<0.001).
Using the MDRD equation, 10589 (51%) had eGFR < 60 ml/min (meeting the National
Kidney Foundation KDOQI definition of stage 3 or 4 kidney disease); using the CKD-EPI
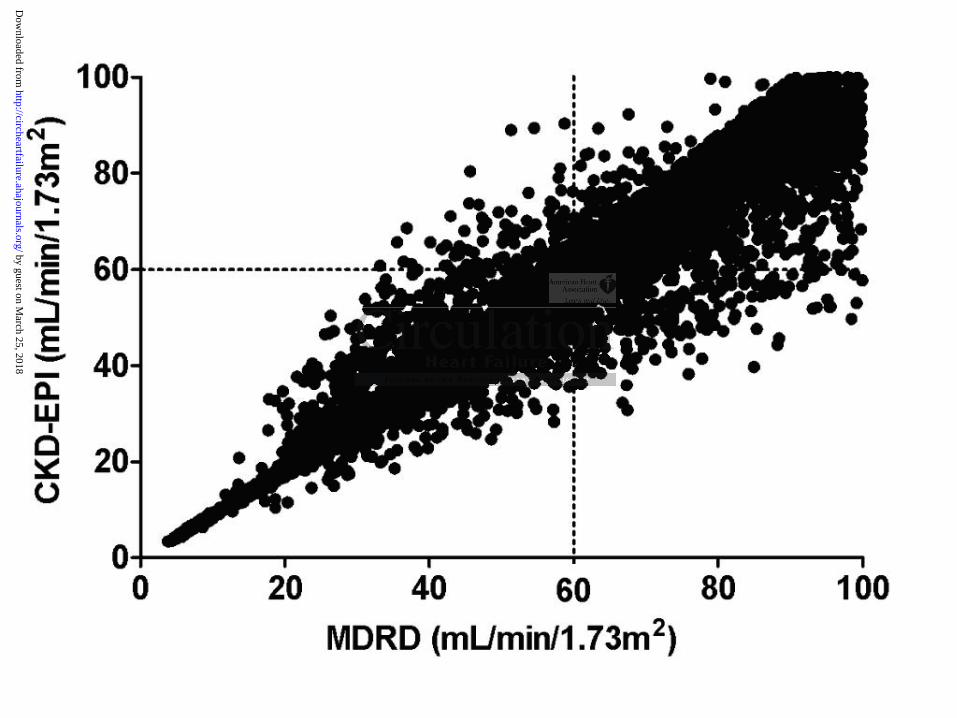
equation, 11422 (55%) patients had eGFR < 60 ml/min (Figure 1). However, using the CKD-
EPI formula resulted in 3760 (18%) patients being reclassified between KDOQI categories
(Table 2, Figure 2), with reclassification occurring across all categories of eGFR. Eighteen
percent (671) of those reclassified were placed in a higher eGFR category with CKD-EPI than
with MDRD (i.e. they were reclassified to a lower risk group); the remaining 3089 (82%) were
placed in a lower eGFR category with CKD-EPI than MDRD (i.e. they were reclassified to a
higher risk group). Although the CKD-EPI equation and the MDRD equation demonstrated
similar discrimination in predicting all-cause mortality in heart failure patients, the CKD-EPI
derived eGFR performed statistically significantly better than the model using MDRD (Table 3),
and review of the misclassification matrix (Table 2) does confirm that the all-cause mortality
rates in the reclassified patients more closely reflected their CKD-EPI risk categorization than
their MDRD-based risk stratification (net reclassification improvement 3.7%, 95% CI 1.5% to
5.9%).
While the adjusted Cox proportional hazards ratio (HR) for the association between renal
dysfunction and mortality in patients with HF-REF increased sequentially as eGFR declined
below 60 ml/min (Figure 3a), the association was less evident in HF-PEF, where there were
fewer patients and lower event rates in each category (Figure 3b, p value for interaction between
EF groups 0.048). Indeed, perusal of the aHR in Figures 3a and 3b reveals that renal dysfunction
was a stronger predictor of all-cause mortality in patients with HF-REF than HF-PEF. Of note,
the HR were adjusted for age, sex, etiology, and presence/absence of anemia, atrial fibrillation,
e. ththhhhhheyeyeyeyeyeyey w wwwwwwererererererere e eeeee rerererererereccclclclclcl
A e
o t
r M
i l ifi i i (T bl 2) d fi h h ll
Although the CKD-EPI equation and the MDRD equation de
on in predicting all-cause mortality in heart failure patients, t
rmed statistically significantly better than the model using M
i l ifi i i (T bl 2) d fi h h ll
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

hypertension, or diabetes, were stratified by study, and the adjusted HR were almost identical
when baseline medication use was included in the models (data not shown). The association
between gradients of CKD-EPI defined eGFR and mortality was similar irrespective of age
(Figure 4).
Discussion
This large meta analysis based upon individual patient data from over 20,000 individuals
confirms previous reports of greater symptom burden, reduced likelihood of being prescribed
evidence based therapies, and poorer adjusted survival in patients with renal dysfunction and
heart failure.7,15
An important novel finding in our study is that use of the CKD-EPI equation to estimate
GFR rather than the MDRD increases the apparent prevalence of renal dysfunction in both HF-
PEF and HF-REF patients. This is contrary to prior studies conducted in healthier and younger
patient populations which suggested higher prevalence of renal dysfunction using the MDRD
compared to the CKD-EPI equation.9-12,16,17,18 However, our data are consistent with a recent
report from the Nijmegen Biomedical Study which found that the CKD-EPI formula provided
lower estimates of GFR than the MDRD in older subjects.19 Thus, impaired renal function is
even more common in HF than previously appreciated. Indeed, our study may even have
underestimated the prevalence of renal dysfunction as we did not have data on albuminuria,
cystatin C, or rate of decline in eGFR, all of which are indicators of renal dysfunction which may
not be apparent in patients with eGFR still in the “normal” range.20-23 Although the Kidney
Early Evaluation Program investigators reported that only 30% of the 2455 patients with heart
failure in their cohort had CKD-EPI eGFR < 60,18 the diagnosis of heart failure in KEEP was
based on self-report and their cohort was substantially younger than ours.
nt novel finding in our study is that use of the CKD-EPI equa
i
a
hi h d hi h l f l d f i i
nt novel finding in our study is that use of the CKD-EPI equa
MDRD increases the apparent prevalence of renal dysfuncti
atients. This is contrary to prior studies conducted in healthi
hi h d hi h l f l d f i i
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

A second important observation from the current analysis is that eGFR is a stronger
predictor of all-cause mortality in HF-REF than HF-PEF, and for any given eGFR category,
mortality is higher in patients with HF-REF than in patients with HF-PEF. The stronger
relationship between mortality and eGFR in HF-REF emphasizes the relevance of the cardiorenal
syndrome to prognosis of these patients. Indeed, it is likely that reduction in eGFR is a marker
for reduced cardiac output, which is a more important prognostic factor in patients with HF-REF
than HF-PEF. Further, competing mortality risks from comorbid conditions such as cancer and
chronic obstructive lung disease are likely to play a larger role in prognosis in HF-PEF.24
Although our study reports on a large, well categorized, and heterogeneous cohort of HF
patients who are similar to other population-based HF cohorts,25 there are some limitations to our
study. For one, we only have renal function and covariate data at baseline. Use of a single
baseline serum creatinine to calculate each patient’s eGFR (by either the MDRD or the CKD-EPI
equations) may overestimate the prevalence of kidney disease.11,26 However, this would have
introduced a null bias into our study, leading to an underestimation of the magnitude of the
association between renal dysfunction and outcomes, and a recent report from the QICKD Study
reported that using 2 eGFR measurements at least 3 months apart rather than just a single
measurement only reduced the prevalence estimates for CKD by about 1%.27 Second, we do not
have any data on unmeasured covariates such as body mass index, levels of BNP, parathyroid
hormone, C-reactive protein, or cholesterol; studies comparing these levels in patients
with/without renal dysfunction and the effects of interventions on these levels and subsequent
clinical outcomes are clearly needed. However, we did adjust for anemia in our multivariable
analyses and have shown in a cohort of 754 patients followed at a specialized heart failure clinic
(in whom we had hemoglobin data) that renal insufficiency is an independent prognostic factor,
even after adjusting for hemoglobin values.7 In the same vein, we do not have data on other
thehererererererere a aaaaaarerererererere ssss sssomomomomomomome e ee e e e lllllll
only have renal function and covariate data at baseline. Use
t D
r i
i d l di d i i f h i
only have renal function and covariate data at baseline. Use
tinine to calculate each patient’s eGFR (by either the MDRD
restimate the prevalence of kidney disease.11,26 However, thi
i d l di d i i f h i
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

renal function metrics such as albuminuria22 , rate of change in eGFR,28 or cystatin C levels21,29
which appear to be prognostically important in patients regardless of eGFR level; however, this
mimics clinical practice in that the vast majority of HF patients are managed without access to
cystatin C levels. Finally, we acknowledge that there is variability between laboratories in
measurement of serum creatinines prior to the introduction of isotope-dilution mass spectrometry
standardization in the mid-2000s; however, this variability was shown to predominantly
introduce error at higher eGFR levels (ie. greater than 60) which were not the focus of our study.
In conclusion, despite the above limitations, our study does demonstrate that reduced
renal function is even more common than previously appreciated in HF, regardless of ejection
fraction. We have also confirmed that reduced eGFR is a stronger predictor of death in patients
with HF-REF than in patients with HF-PEF. Finally, mirroring the findings from the Kidney
Early Evaluation Program in subjects at high risk of kidney disease,18 we have demonstrated that
in patients with HF, use of the CKD-EPI formula to estimate GFR appears to offer better
mortality risk stratification than the MDRD formula.
er prprprprprprpredededededededicicicicicicictototototototor r rrrrr ofofofofofofof d d d d ddd
n m
o
f
fi i h h MDRD f l
n patients with HF-PEF. Finally, mirroring the findings from
ogram in subjects at high risk of kidney disease,18 we have d
use of the CKD-EPI formula to estimate GFR appears to offmm
fi i h h MDRD f l
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Sources of Funding
FAM and JAE are supported by salary awards from Alberta Innovates-Health Solutions; KKP is
supported by a Research Fellowship from the New Zealand Heart Foundation, RND holds the
New Zealand Heart Foundation Chair in Heart Health. The MAGGIC meta-analysis was
supported by grants from the New Zealand National Heart Foundation, The University of
Auckland and The University of Glasgow. These sponsors had no role in the design, conduct,
data management and analysis; or in the manuscript preparation or review; or in the authorization
for submission.
Disclosures
None.
References 1. Dries DL, Exner DV, Domanski MJ, Greenberg B, Stevenson LW. The prognostic
implications of renal insufficiency in asymptomatic and symptomatic patients with left
ventricular systolic dysfunction. J Am Coll Cardiol. 2000;35:681-9.
2. Hillege HL, Girbes AR, de Kam PJ, Boomsma F, de Zeeuw D, Charlesworth A, Hampton
JR, van Veldhuisen DJ. Renal function, neurohormonal activation, and survival in
patients with chronic heart failure. Circulation. 2000;102:203-10.
3. Al-Ahmad A, Rand WM, Manjunath G, Konstam MA, Salem DN, Levey AS, Sarnak MJ.
Reduced kidney function and anemia as risk factors for mortality in patients with left
ventricular dysfunction. J Am Coll Cardiol. 2001;38:955-62.
4. Mahon NG, Blackstone EH, Francis GS, Starling RC, Young JB, Lauer MS. The
prognostic value of estimated creatinine clearance alongside functional capacity in
DV D ki MJ G b B S LW Th
References
DV D ki MJ G b B S LW Th
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

ambulatory patients with chronic congestive heart failure. J Am Coll Cardiol.
2002;40:1106-13.
5. Kearney MT, Fox KA, Lee AJ, Prescott RJ, Shah AM, Batin PD, Baig W, Lindsay S,
Callahan TS, Shell WE, Eckberg DL, Zaman AG, Williams S, Neilson JM, Nolan J.
Predicting death due to progressive heart failure in patients with mild-to-moderate
chronic heart failure. J Am Coll Cardiol. 2002;40:1801-8.
6. McClellan WM, Flanders WD, Langston RD, Jurkovitz C, Presley R. Anemia and renal
insufficiency are independent risk factors for death among patients with congestive heart
failure admitted to community hospitals: A population-based study. J Am Soc Nephrol.
2002;13:1928-36.
7. McAlister FA, Ezekowitz J, Tonelli MR, Armstrong PW. Renal insufficiency and heart
failure: prognostic and therapeutic implications from a prospective cohort study.
Circulation. 2004;109:1004-9.
8. Ezekowitz JA, McAlister FA, Humphries K, Norris CM, Tonelli M, Ghali WA, for the
APPROACH Investigators. The association among renal insufficiency,
pharmacotherapy, and outcomes in 6427 patients with heart failure and coronary artery
disease. J Am Coll Cardiol. 2004;44:1587-92.
9. Levey AS, Bosch JP, Lewis JB, Greene T, Rogers N, Roth D. A more accurate method
to estimate glomerular filtration rate from serum creatinine: a new prediction equation.
Modification of Diet in Renal Disease Study Group. Ann Intern Med. 1999;130:461-70.
10. Bostom AG, Kronenberg F, Ritz E. Predictive performance of renal function equations
for patients with chronic kidney disease and normal serum creatinine levels. J Am Soc
Nephrol. 2002;13:2140-4.
A i
g v
A M Ali FA H h i K N i CM T lli M Gh
A, Ezekowitz J, Tonelli MR, Armstrong PW. Renal insuffi
gnostic and therapeutic implications from a prospectiv
2004;109:1004-9.
A M Ali FA H h i K N i CM T lli M Gh
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

11. Glassock RJ, Winearls C. An epidemic of chronic kidney disease: fact or fiction?
Nephrol Dial Transplant. 2008;23:1117-21.
12. Levey AS, Stevens LA, Schmid CH, Zhang Y, Castro AF, Feldman HI, Kusek JW,
Eggers P, van Lente F, Greene T, Coresh J. A new equation to estimate glomerular
filtration rate. Ann Intern Med. 2009;150:604-612.
13. Meta-analysis Global Group in Chronic Heart Failure (MAGGIC) Investigators. The
Survival of Patients with Heart Failure with Preserved or Reduced Left Ventricular
Ejection Fraction: an Individual Patient Data Meta-analysis. Eur Heart J. 2011;Aug 6
[Epub ahead of print] doi:10.1093/eurheartj/ehr254
14. National Kidney Foundation. Kidney Disease Outcomes Quality Initiative. Clinical
practice guidelines for chronic kidney disease: evaluation, classification, and
stratification. Am J Kidney Dis. 2002;39(Suppl 1):s1-s266.
15. McCullough PA. Cardiorenal risk: an important clinical intersection. Rev Cardiovasc
Med. 2002;3:71-6.
16. Carter JL, Stevens PE, Irving JE, Lamb EJ. Estimating glomerular filtration rate:
comparison of the CKD-EPI and MDRD equations in a large UK cohort with particular
emphasis on the effect of age. Q J Med. 2011;104:839-847.
17. White SL, Polkinghorne KR, Atkins RC, Chadban SJ. Comparison of the prevalence and
mortality risk of CKD in Austraila using the CKD Epidemiology Collaboration (CKD-
EPI) and Modification of Diet in Renal Disease (MDRD) Study GFR estimating
equations: The AusDiab (Australian Diabetes, Obesity, and Lifestyle) Study. Am J
Kidney Dis. 2010;55:660-670.
18. Stevens LA, Li S, Tamura MK, Chen SC, Vassalotti JA, Norris KC, Whaley-Connell AT,
Bakris GL, McCullough PA. Comparison of the CKD Epidemiology Collaboration
QQuauauauauauaualililililililitytytytytytyty I IIIIIInininininininitititititititiatatatatatatativiviviviviviv
delines for chronic kidney disease: evaluation, classification,
e
71 6
delines for chronic kidney disease: evaluation, classification,
. Am J Kidney Dis. 2002;39(Suppl 1):s1-s266.
PA. Cardiorenal risk: an important clinical intersection. Re
71 6
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

(CKD-EPI) and Modification of Diet in Renal Disease (MDRD) Study Equations: Risk
factors for and complications of CKD and mortality in the Kidney Early Evaluation
Program (KEEP). Am J Kidney Dis 2011;57 (Suppl 2):S9-S16.
19. van den Brand JA, van Boekel GA, Willems HL, Kiemeney LA, den Heijer M, Wetzels
JF. Introduction of the CKD-EPI equation to estimate glomerular filtration rate in a
Caucasian population. Nephrol Dial Transplant. Nephrol Dial Transplant. 2011;26:3176-
81
20. Tonelli M, Muntner P, Lloyd A, Manns BJ, James MT, Klarenbach S, Quinn RR, Wiebe
N, Hemmelgarn BR, for the Alberta Kidney Disease Network. Using proteinuria and
estimated glomerular filtration rate to classify risk in patients with chronic kidney
disease. A cohort study. Ann Intern Med. 2011;154:12-21.
21. Peralta CA, Shlipak MG, Judd S, Cushman M, McClellan W, Zakai NA, Safford MM,
Zhang X, Muntner P, Warnock D. Detection of chronic kidney disease with creatinine,
cystatin C, and urine albumin-to-creatinine ratio and association with progression to end-
stage renal disease and mortality. JAMA. 2011;305:1545-52.
22. Chronic Kidney Disease Prognosis Consortium. Association of estimated glomerular
filtration rate and albuminuria with all-cause and cardiovascular mortality in general
population cohorts: a collaborative meta-analysis. Lancet. 2010;375:2073-81.
23. Shlipak MG, Katz R, Kestenbaum B, Siscovick D, Fried L, Newman A, Rifkin D, Sarnak
MJ. Rapid decline of kidney function increases cardiovascular risk in the elderly. J Am
Soc Nephrol. 2009;20:2625-30.
24. O’Hare AM, Bertenthal D, Covinsky KE, Landefeld CS, Sen S, Mehta K, Steinman MA,
Borzecki A, Walter LC. Mortality risk stratification in chronic kidney disease: one size
for all ages? J Am Soc Nephrol. 2006;17:846-53.
ents s sssss wiwiwiwiwiwiwiththththththth c cccccchrhrhrhrhrhrhronononononononiiiiiii
Shlipak MG, Judd S, Cushman M, McClellan W, Zakai NA,
u w
d i lb i i i i d i i i h
ohort study. Ann Intern Med. 2011;154:12-21.
Shlipak MG, Judd S, Cushman M, McClellan W, Zakai NA,
untner P, Warnock D. Detection of chronic kidney disease w
d i lb i i i i d i i i h
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

25. Krum H, Gilbert RE. Demographics and concomitant disorders in heart failure. Lancet.
2003;362:147-58.
26. Eriksen BO, Ingebretsen OC. In chronic kidney disease staging the use of the chronicity
criterion affects prognosis and the rate of progression. Kidney Int. 2007;72:1242-48.
27. de Lusignan S, Tomson C, Harris K, van Vlymen J, Gallagher J. Creatinine fluctuation
has a greater effect than the formula to estimate glomerular filtration rate on the
prevalence of chronic kidney disease. Nephron Clin Prac. 2011;117:213-214.
28. Rusinaru D, Buiciuc O, Houpe D, Tribouilloy C. Renal function and long-term survival
after hospital discharge in heart failure with preserved ejection fraction. Int J Cardiol
2011;147:278-282.
29. Lee M, Saver JL, Huang WH, Chow J, Chang KH, Ovbiagele B. Impact of elevated
cystatin C level on cardiovascular disease risk in predominantly high cardiovascular risk
populations. A meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3:675-683.
t
v d
r JL, Huang WH, Chow J, Chang KH, Ovbiagele B. Impact
vel on cardiovascular disease risk in predominantly high card
A meta-analysis. Circ Cardiovasc Qual Outcomes. 2010;3
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Table 1. Characteristics of patients, stratified by eGFR calculated using the CKD-EPI formula
HF-PEF (n=4792) HF-REF (n=15962)
eGFR <15 15-29.9 30-44.9 45-59.9 60-89.9 90 p value <15 15-29.9 30-44.9 45-59.9 60-89.9 90 p value
N 129 390 959 1248 1674 392 203 1238 2977 4278 5942 1324
Age, yrs (SD) 73 (13) 77 (10) 77 (9) 73 (10) 68 (11) 56 (12) <.0001 70 (13) 75 (9) 73 (9) 69 (10) 63 (11) 53 (12) <.0001
Women, % 61 61 63 57 43 37 <.0001 42 42 37 30 21 18 <.0001
Medical history:
Hypertension 66 66 58 56 50 48 <.0001 68 52 42 37 33 29 <.0001
MI 21 28 28 26 27 20 0.274 38 54 55 55 49 41 <.0001
Atrial fibrillation 28 30 27 27 23 14 <.0001 19 21 21 18 15 12 <.0001
Diabetes 35 33 28 23 21 21 <.0001 39 32 27 22 20 18 <.0001
Ischemic etiology 47 41 45 46 41 37 0.014 56 62 62 63 57 48 <.0001
Anaemia 73 64 50 39 34 34 <.0001 73 69 54 44 35 28 <.0001
Medication
ACEi or ARB 54 59 67 68 65 60 0.685 69 78 88 91 91 92 <.0001
Beta-blocker 26 31 33 35 38 36 0.0005 37 33 34 35 41 44 <.0001
Diuretic 74 84 87 82 78 70 <.0001 69 90 90 84 79 69 <.0001
Spironolactone 15 20 20 19 16 16 0.052 10 28 28 29 26 23 0.351
Digoxin 24 25 31 32 29 29 0.379 25 39 44 47 45 47 <.0001
Clinical status NYHA class (I+II/III+IV) 59/41 59/41 65/35 72/28 75/25 75/25 <.0001 47/53 46/54 53/47 59/41 67/33 75/25 <.0001
Heart rate, bpm 85 (24) 80 (20) 80 (23) 81 (22) 81 (23) 82 (22) 0.457 82 (17) 80 (18) 81 (19) 81 (19) 81 (19) 82 (19) 0.781
SBP, mmHg 146 (42) 142 (31) 143 (27) 144 (28) 142 (26) 139 (27) 0.074 138 (30) 131 (28) 129 (25) 128 (23) 127 (22) 126 (22) <.0001
DBP, mmHg 80 (21) 75 (16) 78(16) 80 (14) 80 (14) 80 (16) 0.080 78 (17) 75 (13) 75 (13) 76 (13) 77 (13) 78 (14) 0.388 LVEF % (median, IQR) 59 (54,62) 60 (54,64) 59 (54,64) 60 (68,90) 60 (55,63) 60 (56,63) 0.683 36
(27, 41) 31
(23, 38) 30 (23,38) 30 (23, 38) 31 (24,38) 32 (25,39) 0.036
All-cause deaths 38 156 234 216 242 55 <.0001 72 590 1066 1139 1031 148 <.0001 Mortality rate (per 1000 patient years)
346.7
307.6
182.4
117.1
92.4
105.9
<.0001 441.3
378.9
233.5
151.9
98.3
74.3
<.0001
33333339 9 9 9 9 9 9 3333333
5666 641 37 0.014 56 6
34 34 <.0001 73 6
7
3
41 37 0.014 56 6
34 34 <.0001 73 6
65 60 0.685 69 7
38 36 0.0005 37 3
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Table 2. Comparison of all-cause mortality rates (expressed as incidence per 1000 person years) in MDRD and CKD-EPI defined subgroups
CKD-EPI eGFR MDRD eGFR 90 60-89.9 45-59.9 30-44.9 15-29.9 <15
Reclassification
90, n
Mortality rate (95% CI)
1489
83.7 (72.1, 96.7)
539
103.9 (85.8, 124.9)
24
80.6 (29.5, 178.6)
0 -
0 -
0 -
563/2052 (27.4%)
563 downward
60-89.9, n
Mortality rate
226
64.7 (42.4, 94.8)
6862
95.8 (90.3, 101.6)
984
143.0 (126.4,161.1)
41
228.0 (143.2,346.0)
0 -
0 -
1251/8113 (15.4%)
1025 downward 226 upward
45-59.9, n
Mortality rate
1
-
199
101.2 (74.2, 135.1)
4356
141.9 (133.4,150.9)
993
204.9 (18.3, 228.7)
8
42.0 (3.10, 207.4)
0 -
1201/5557 (21.6%)
1001 downward 200 upward
30-44.9, n
Mortality rate
0 -
16
274.6 (139.5,489.5)
156
236.1 (186.7,294.7)
2837
226.8 (212.6,241.8)
441
307.2 (265.1,354.0)
0 -
613/3450 (17.8%)
441 downward 172 upward
15-29.9, n
Mortality rate
0 -
0 -
6
238.9 (60.8, 650.2)
65
274.4 (196.1,374.3)
1177
388.4 (357.2,421.7)
59
541.1 (369.2,767.0)
130/1307 (9.9%)
59 downward 71 upward
<15, n
Mortality rate
0 -
0 -
0 -
0
-
2
782.1 (131.1,2584.0)
273
369.6 (295.4, 456.5)
2/275 (0.7%)
2 upward
Reclassification downward = eGFR risk strata lower with CKD-EPI than with MDRD Reclassification upward = eGFR risk strata higher with CKD-EPI than with MDRD
88888884356 993 8
7
156 2837
4356
141.9 (133.4,150.9)
993
204.9 (18.3, 228.7)
8
42.0 (3.10, 207
441
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Table 3. Area under the curve for all cause mortality at 3 years after adjustment for age and gender
Equation Whole group HF-REF HF-PEF
CKD-EPI 0.644 (0.635, 0.653) 0.652 (0.636, 0.656) 0.621 (0.616, 0.626)
MDRD 0.634 (0.626, 0.644) 0.646 (0.636, 0.656) 0.598 (0.592, 0.603)
p value <0.0001 <0.0001 <0.0001
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Figure Legends
Figure 1. Comparison of eGFR distributions using the MDRD and CKD-EPI formulae in
patients with HF-REF and HF-PEF
Figure 2. Reclassification plot
Figure 3a. Association between CKD-EPI defined eGFR categories and all-cause mortality
in heart failure patients with reduced ejection fraction.
Legend: Hazard ratios adjusted for age, sex, ischemic etiology, anemia, hypertension, diabetes,
or atrial fibrillation, and stratified by study
Figure 3b. Association between CKD-EPI defined eGFR categories and all-cause mortality
in heart failure patients with preserved ejection fraction.
Legend: Hazard ratios adjusted for age, sex, ischemic etiology, anemia, hypertension, diabetes,
or atrial fibrillation, and stratified by study
Figure 4. Mortality rates by age group and CKD-EPI defined eGFR categories
gggggggorororororororieieieieieieiessss s ss ananananananand d ddddd alalalalalalall-l-l-l-l-l-l-ccccccc
tients with preserved ejection fraction
o n
y rates by age group and CKD EPI defined eGFR categor
tients with preserved ejection fraction.
os adjusted for age, sex, ischemic etiology, anemia, hyperten
and stratified by study
y rates by age group and CKD-EPI defined eGFR categor
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

0
100
200
300
400
500
600
700
Dea
ths/
1,00
0pa
tient
year
s
Age Group
CKD-EPI (ml/min/1.73m )
>7565-75
55-65<55
<1515-30
30-4545-60
60-90>90
CKD EPI (ml/min/1.73m)2
AgeGro
up (yrs)
Deaths/1,000patie
ntyears by guest on M
arch 25, 2018http://circheartfailure.ahajournals.org/
Dow
nloaded from

DoughtyBayes-Genis, Israel Gotsman, Gillian Whalley, Nikki Earle, Katrina K. Poppe and Robert N. Finlay A. McAlister, Justin A. Ezekowitz, Luigi Tarantini, Iain Squire, Michel Komajda, Antoni
Impact of the New CKD-EPI FormulaRenal Dysfunction in Heart Failure Patients with Preserved versus Reduced Ejection Fraction:
Print ISSN: 1941-3289. Online ISSN: 1941-3297 Copyright © 2012 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Circulation: Heart Failure published online March 22, 2012;Circ Heart Fail.
http://circheartfailure.ahajournals.org/content/early/2012/03/22/CIRCHEARTFAILURE.111.966242World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circheartfailure.ahajournals.org/content/suppl/2012/03/22/CIRCHEARTFAILURE.111.966242.DC1Data Supplement (unedited) at:
http://circheartfailure.ahajournals.org//subscriptions/
is online at: Circulation: Heart Failure Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
click Request Permissions in the middle column of the Web page under Services. Further information about thisEditorial Office. Once the online version of the published article for which permission is being requested is located,
can be obtained via RightsLink, a service of the Copyright Clearance Center, not theCirculation: Heart Failure Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on March 25, 2018
http://circheartfailure.ahajournals.org/D
ownloaded from

Supplemental Material Acknowledgements for the MAGGIC meta-analysis MAGGIC Executive Group: C Berry, RN Doughty, C Granger, L Køber, B Massie, F
McAlister, J McMurray, S Pocock, K Poppe, K Swedberg, J Somaratne, GA Whalley.
MAGGIC Steering Group: The Steering Group included investigators from the original studies
that provided individual patient data: A Ahmed, B Andersson, A Bayes-Genis, C Berry, M
Cowie, R Cubbon, RN Doughty, J Ezekowitz, J Gonzalez-Juanatey, M Gorini, I Gotsman, L
Grigorian-Shamagian, M Guazzi, M Kearney, L Køber, M Komajda, A di Lenarda, M Lenzen, D
Lucci, S Macín, B Madsen, A Maggioni, M Martínez-Sellés, F McAlister, F Oliva, K Poppe, M
Rich, M Richards, M Senni, I Squire, G Taffet, L Tarantini, C Tribouilloy, R Troughton, H
Tsutsui, GA Whalley.
MAGGIC Coordinating Centre: RN Doughty, N Earle, K Perera, K Poppe, GA Whalley, The
University of Auckland, New Zealand.
MAGGIC Statistical Group: J Dobson, GD Gamble, S Pocock, K Poppe.
The MAGGIC Studies and Investigators. The following investigators kindly provided the individual patient data from their studies: AHFMS: RN Doughty, G Whalley; Andersson (2 datasets): B Andersson, C Hall; BATTLESCARRED & Richards: AM Richards, R Troughton, J Lainchbury; Berry: C Berry, K Hogg, J Norrie, K Stevenson, M Brett, J McMurray; CHARM: MA Pfeffer, K Swedberg, CB Granger, P Held, JJV McMurray, EL Michelson, B Olofsson, J Östergren, S Yusuf for the CHARM Investigators and Committees; Diamond & ECHOS: L Køber, C Torp-Pedersen; DIG Trial: DIG limited access data, Ali Ahmed; Euro HF Survey: MJ Lenzen, WJM Scholte op Reimer, E Boersma, PJMJ Vantrimpont, F Follath, K Swedberg, J Cleland, M Komajda: Gotsman; I Gotsman, D Zwas, D Planer, T Azaz-Livshits, D Admon, C Lotan, A Keren: Grigorian-Shamagian; L Grigorian-Shamagian, A Varela-Roman, P Mazón-Ramos, P Rigeiro-Veloso, MA Bandin-Dieguez, JR Gonzalez-Juanatey; Guazzi: M Guazzi, J Myers, R Arena; Heart Failure Clinic Edmonton: FA McAlister, J Ezekowitz, PW Armstrong, Bibiana Cujec , Ian Paterson; Hillingdon: MR Cowie, DA Wood, AJS Coats, SG Thompson, V Suresh, PA Poole-Wilson, GC Sutton; HOLA: M Martínez-Sellés, JAG Robles, L Prieto, MD Muñoa, E Frades, O Díaz-Castro, J Almendral; Italian HF Registry (IN-CHF): L Tarantini, P Faggiano, M Senni, D Lucci, D Bertoli, M Porcu, C Opasich, L Tavazzi, AP Maggioni; Kirk: V Kirk, M Bay, J Parner, K Krogsgaard, TM Herzog, S Boesgaard, C Hassager, OW Nielsen, J Aldershvile, H Nielsen L Kober; Macin: SM Macín, ER Perna, JP Cimbaro Canella, P Alvarenga, R Pantich, N Ríos, EF Farias, JR Badaracco; Madsen: BK Madsen, JF Hansen, KH Stokholm, J Brons, D Husum, LS Mortensen; MUSIC: A Bayes-Genis, R Vazquez, T Puig, C Fernandez-Palomeque, A Bardají, D Pascual-Figal, J Ordoñez-Llanos, M Valdes, A Gabarrus, R Pavon, L Pastor, JR Gonzalez-Juanatey, J Almendral, M Fiol,V Nieto, C Macaya, J Cinca, A Bayes de Luna; Newton: JD Newton, HM Blackledge, IB Squire; NPC I: SP Wright, GA Whalley, RN Doughty; Rich (dataset 1): R Kerzner, BF Gage, KE Freedland, MW Rich; Rich

(dataset 2): BC Huynh, A Rovner, KE Freedland, RM Carney, MW Rich; Taffet: GE Taffet, TA Teasdale, AJ Bleyer, NJ Kutka, RJ Luchi; Tribouilloy: C Tribouilloy, D Rusinaru, H Mahjoub, V Soulière, F Lévy, M Peltier; Tsutsui: H Tsutsui, M Tsuchihashi, A Takeshita; UK Heart Study: PA MacCarthy, MT Kearney, R Cubbon, J Nolan, AJ Lee, RJ Prescott, AM Shah, WP Brooksby, KAA Fox; Varela-Roman: A Varela-Roman, JR Gonzalez-Juanatey, P Basante, R Trillo, J Garcia-Seara, JL Martinez-Sande, F Gude.





























