Embed Size (px)
Citation preview

Renal cell carcinoma marker (RCC-Ma)is specific for cutaneous metastasis ofrenal cell carcinoma
Background: Renal cell carcinoma marker (RCC-Ma) is a monoclonalantibody against a normal renal proximal tubule antigen. RCC-Maexpression is relatively specific for primary clear cell renal cell carci-noma. Its expression in cutaneous metastasis of renal cell carcinoma(MRCC) and other cutaneous clear cell lesions has not been studied.Methods: One hundred and thirty-seven cutaneous clear cell lesionsincluding eight xanthomas, 32 xanthelasmas, 25 xanthogranulomas,seven balloon cell nevi, six clear cell hidradenomas, 29 sebaceousadenomas, six sebaceous epitheliomas, eight sebaceous carcinomas,and 16 MRCC were examined using immunohistochemistry for theexpression of RCC-Ma.Results: RCC-Ma was expressed in 10 of 16 (62.5%) MRCC, all withgreater than 20% of cell labeling. Of these, 4 of 10 (40%) labeled with amembranous pattern and 6 of 10 (60%) labeled with both amembranous and a cytoplasmic pattern. RCC expression was not seenin any of the other clear cell lesions (p < 0.001). Furthermore, lack ofexpression in each of the other diagnostic groups was significant wheneach group was compared with the MRCCs (p < 0.01 at least for eachgroup).Conclusions: Our study demonstrates that RCC may be a valuablecomponent of a panel of immunohistochemical markers whenevaluating cutaneous clear cell lesions.
Perna AG, Ostler DA, Ivan D, Lazar AJF, Diwan AH, Prieto VG,Reed JA. Renal cell carcinoma (RCC) marker is specific for cutaneousmetastasis of RCC.J Cutan Pathol 2007; 34: 381–385. # Blackwell Munksgaard 2006.
Ashley G. Perna1, Daniel A.Ostler2, Doina Ivan3, AlexanderJ. F. Lazar3, A. Hafeez Diwan3,Victor G. Prieto3 and Jon A. Reed1
1Department of Pathology, Baylor College ofMedicine,2Department of Pathology, University of TexasHealth Science Center, and3Departments of Pathology and Dermatology,M.D. Anderson Cancer Center, Houston,TX, USA
Ashley G. Perna, MD, Department of Pathology,Baylor College of Medicine, One Baylor Plaza,Room 286A, Houston, TX 77030, USATel: þ1 713 798 5490e-mail: [email protected]
Accepted for publication May 2, 2006
The renal cell carcinoma marker (RCC-Ma) is acommercially available mouse monoclonal antibodyproduced against a crude microsomal fraction of theproximal tubules from normal human kidney. It isspecific for an Mr 200,000 glycoprotein (Gp200,000) found in the renal proximal tubular brushborder in normal human kidney.1 RCC-Ma hasproven useful in distinguishing renal cell carcinoma(RCC) from other renal neoplasms, as 80–85% ofprimary clear cell RCC express RCC-Ma, whereasprevious studies have documented no RCC-Maexpression in 24 oncocytomas, 20 transitional cellcarcinomas, three angiomyolipomas, three meso-
blastic nephromas, and three cystic nephromas.2,3
Furthermore, RCC-Ma distinguishes RCC fromother neoplasms that can show clear cell morpho-logy and can enter into the differential diagnosis ofRCC, with no RCC-Ma staining seen in six adre-nocortical carcinomas, seven adrenocortical adeno-mas, five hemangioblastomas, and 21 hepatocellularcarcinomas.2 However, 100% (8/8) of pituitary ade-nomas, 20% (2/10) of invasive mammary ductalcarcinoma, and 29% (2/7) of testicular embryonalcarcinomas expressed RCC-Ma.2 Despite the fairlyhigh sensitivity of RCC-Ma in diagnosing primaryclear cell RCC, only 67% of visceral metastasis of
J Cutan Pathol 2007: 34: 381–385doi: 10.1111/j.1600-0560.2006.00623.xBlackwell Munksgaard. Printed in Singapore
Copyright # Blackwell Munksgaard 2006
Journal of
Cutaneous Pathology
381

clear cell RCC expressed RCC-Ma.2 To our knowl-edge, there has been no evaluation of RCC-Maexpression in cutaneous metastasis of clear cell RCC.Multiple cancers classically metastasize to the
skin, including breast carcinomas, lung carcino-mas, and RCCs.4–6 Although metastases of RCCto the skin comprise approximately 6% of cuta-neous metastases,4–7 there has been only limitedinvestigation into the immunophenotype of thesemetastatic lesions. CD10, also known as the com-mon acute lymphoblastic leukemia antigen(CALLA), is expressed in 82–94% of primaryclear cell RCC,3,8 and all the studied cases (3/3)of cutaneous metastases of RCC.9 In the skin, thereare many clear cell neoplasms of epithelial, mela-nocytic, and mesenchymal origin.10 Many of these,including balloon cell nevi (BCN), xanthomatouslesions, and clear cell hidradenoma (CCH) canmimic metastatic RCC. Particularly, xanthoma-tous lesions can show pronounced cytoplasmicclearing with loss of the classic foamy histiocyticappearance. When these xanthomatous lesions takeon a less foamy appearance, they can mimic mela-noma11 and metastatic RCC.9 Although CD10 isexpressed in some metastatic RCC to the skin, thisantibody has been shown to have limited utility indistinguishing cutaneous metastases of RCC fromother cutaneous clear cell lesions, as many cuta-neous clear cell lesions of different histogenesis alsoexpress CD10.9 To our knowledge, RCC-Maexpression has not been evaluated in cutaneousRCC metastases, BCN, xanthomatous lesions,and sebaceous neoplasms.
Materials and methods
Tissues
Formalin-fixed, paraffin-embedded tissues (n ¼ 137)were derived from the tissue archives of theDepartments of Pathology at Baylor College ofMedicine, Texas Children’s Hospital, the MichaelE. DeBakey Veterans Affairs Medical Center, andthe University of Texas M.D. Anderson CancerCenter. Specimens included cutaneous MRCC(n ¼ 16), xanthomas (CX, n ¼ 8), xanthogranulo-mas (XG, n ¼ 25), xanthelasmas (XA, n ¼ 32),BCN (n ¼ 7), CCH (n ¼ 6), sebaceous adenomas(SA, n ¼ 29), sebaceous carcinomas (SC, n ¼ 8),and sebaceous epitheliomas (SE, n ¼ 6). All tissueswere sectioned 5-mm thick and placed on positivelycharged glass slides (ProbeOn Plus, Fisher Scientific,Pittsburgh, PA).The sections were deparaffinized and rehydrated
through a graded series of ethanol. Heat-inducedepitope retrieval was performed with 10 mM Tris–HCl pH 9.0 solution. The sections were steamed for
25 min followed by cooling at room temperature for10 min in the same solution. Endogenous peroxi-dase was inhibited by treatment with 3% aqueoushydrogen peroxide for 6 min at room temperaturefollowed by a rinse with Tris-buffered saline (TBS,150 mM NaCl, 10 mM Tris–HCl pH ¼ 7.4) beforeimmunohistochemistry.
Immunohistochemistry
Deparaffinized sections were incubated with the mouseIgG monoclonal anti-RCC Ma antibody (Clone66.4.C2, Vector Laboratories Inc, Burlingame, CA)and diluted 1:10 with an antibody diluent (Dako,Carpinteria, CA) for 45 min at room temperature.After TBS washes, the primary antibody was thenfollowed by using a Mouse-Probe HRP Polymer kitMACH 3 (Biocare Medical, Walnut Creek, CA). TheMouse Probe was allowed to incubate for 20 min atroom temperature. After additional TBS washes, a3,3
0-diaminobenzidine chromogen (Dako) was applied
and incubated for 6 min at room temperature.Negative controls were performed by omitting theprimary antibody. All slides were lightly counterstainedwith hematoxylin, permanently mounted, and viewedwith a standard light microscope.Immunolabeling was scored subjectively by two
pathologists (JAR, AGP) as follows: 0, no labeling;1þ, labeling in fewer than 10% of cells; 2þ, labelingin 10–50%; and 3þ, labeling in more than 50% ofclear cells in the lesion. The pattern of labeling(membranous only vs. mixed cytoplasmic and mem-branous vs. cytoplasmic only) was also noted for allthe cases.
Statistical analysis
Comparisons of frequency of staining between diag-nostic groups were made using the w2 test with ap-value <0.05 considered to be significant.
Results
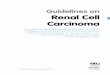
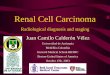
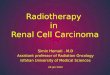
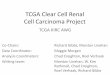
Clinical data including the diagnosis, age, gender,and anatomical site for all patients are summarizedin Table 1. RCC-Ma was expressed in 10 of 16(62.5%) cutaneous metastases of RCC. All 10 ofthese metastatic lesions showed RCC-Ma expressionin greater than 20% of cells, with seven of 10 (70%)of the positive cutaneous metastases scored as 2þ,and the remaining three of 10 (30%) scored as 3þ.Of these, four of 10 (40%) showed a predominantlymembranous pattern (Fig. 1A and B) and six of 10(60%) showed both a membranous and a cytoplas-mic pattern (Fig. 2A and B). None showed a purely
Perna et al.
382

cytoplasmic pattern. The RCC-Ma expression scoreand pattern of RCC-Ma labeling for the cutaneousMRCC are reported in Table 2.
None of the CCH, BCN, SA, SE, SC, CXs, XAs, orXG exhibited any expression of RCC-Ma. When thegroup of cutaneous metastasis of RCC was comparedwith all the other clear cell lesions, the differential
Table 1. Clinical data for cutaneous clear cell lesions
Diagnostic category (n) Age (range) Sex (M : F) Anatomic sites
Xanthomas (8) 9 months to 72 years 4:4 1 face, 1 lower extremity,2 trunk, 4 upper extremity
Xanthelasmas (32) 34–71 years 20:12 30 periorbital, 1 nose, 1 forearm
Xanthogranulomas (25) 8 months to 61 years 15:9 (1 unknown) 12 head, 5 trunk, 4 lowerextremity, 3 upper extremity,1 unknown
Balloon cell nevi (7) 5–74 years 3:4 3 back, 2 abdomen, 1 face,1 unknown
Clear cell hidradenomas (6) 31–75 years 4:2 3 upper extremity, 1 trunk,1 temple, 1 labium
Sebaceous adenomas (29) 46–90 years 20:9 25 head, 3 back, 1 shoulder,
Seceous epitheliomas (6) 50–83 years 3:3 6 Head
Sebaceous carcinomas (8) 59–91 years 4:4 7 face, 1 shoulder
Cutaneous metastasis of RCC (16) 41–79 years 9:7 10 head, 1 neck, 3 upperextremity, 1 lower extremity,1 trunk
A
B
Fig. 1. (A, B) There is prominent immunolabeling with renal cell
carcinoma marker in a predominantly membranous pattern in
these examples of metastatic renal cell carcinoma to the skin (mag-
nification �400).
A
B
Fig. 2. (A, B) In these examples of cutaneous metastasis of renal cell
carcinoma, there is both cytoplasmic and membranous labeling
with metastatic renal cell carcinoma (magnification �400).
Use of RCC-Ma to diagnose metastatic RCC to skin
383

expression of RCC-Ma in the cutaneous metastasis ofRCC was highly significant (p < 0.001). Further-more, the lack of staining in each of the other diag-nostic groups was significant when each individualgroup was compared with the MRCCs (p < 0.01 foreach group). No expression of RCC-Ma was seen innormal epidermis and normal dermal structures.
Discussion
RCC-Ma was originally raised as an antibody to anantigen found in the proximal tubule brush borderof normal human kidneys. It has been shown to be afairly specific marker for clear cell RCC, demon-strating expression in 80–85% of primary clear cellRCC and 67% of visceral metastasis of RCC. Ourstudy shows that expression of RCC-Ma is presentin 62.5% of cutaneous metastases of clear cell RCC,similar to the previously reported expression in 67%of visceral metastasis of clear cell RCC.2
Furthermore, our study shows that none of thecutaneous clear cell lesions that could potentiallymimic metastatic clear cell RCC to the skin expressRCC-Ma. Previous studies have demonstrated thatCD10 (CALLA), another antibody commonly usedin the diagnosis of primary RCC,3,8 is not as usefulin the diagnosis of cutaneous MRCC.9 CD10 isexpressed not only in cutaneous metastases of clear
cell RCC but is also expressed in CXs, XAs, juvenileXG, and some BCN and CCH.9
This study shows that RCC-Ma is highly useful ina panel of immunohistochemical markers in evaluat-ing a new cutaneous clear cell lesion, especially in apatient with a history of RCC. Table 3 summarizes asuggested panel of immunohistochemical markersand the expected results for metastatic RCC andpotential mimics, based on a review of the relevantliterature and the extensive personal experience ofthe authors with these lesions. The specificity ofRCC-Ma in identifying true metastatic RCC to theskin is excellent (100%), however, the sensitivity indetecting a RCC metastasis to the skin is poor (65%).Therefore, according to our data, a positive resultwith RCC-Ma immunohistochemistry in a cutaneousclear cell lesion is diagnostic of metastatic RCC to theskin. However, as this study demonstrates, a negativeRCC-Ma immunohistochemical result clearly doesnot exclude a diagnosis of metastatic RCC.
Acknowledgements
We thank Serrita Coleman, Angela Vogel, and Antonio Duharte in the
Baylor College of Medicine Immunohistochemistry lab for their tech-
nical assistance. This work was presented at the American Society of
Dermatopathology Annual Meeting in Seattle, WA, in October 2005.
References
1. Yoshida SM, Imam A. Monoclonal antibody to a proximal
nephrogenic renal antigen: immunohistochemical analysis of
formalin-fixed, paraffin-embedded human renal cell carcino-
mas. Cancer Res 1989; 49: 1802.
2. McGregor DK, Khurana KK, Cao C, et al. Diagnosing pri-
mary and metastatic renal cell carcinoma: the use of the mono-
clonal antibody ‘Renal Cell Carcinoma Marker’. Am J Surg
Pathol 2001; 25: 1485.
Table 2. Renal cell carcinoma marker expression score and pattern oflabeling for cutaneous metastases of renal cell carcinoma
Score Pattern
3þ 2þ 1þ 0 Membranous Cytoplasmic Both
3 7 0 6 4 0 6
Table 3. A suggested panel of immunohistochemical markers and the expected results for metastatic renal cell carcinoma to the skin (MRCC) andpotential mimics
RCC-Ma CD10 EMA AE1/AE3 CEA CD68 CK7 CK20 HMB45 S-100
MRCC3,8,9,12 þ/– þ nd* nd* nd* nd* – – nd* nd*
CX9,12–14 – þ – – – þ – – – –/þXA9,12,14 – þ – – – þ – – – –/þXG9,12,14–16 – þ – – – þ – – – –/þBCN9,12 – þ/– – – – – – – þ þCCH9,12,17–19 – þ/– þ þ þ nd þ – – –SA12,20–23 – þ/– þ þ þ/– – þ/– – – þSE12,20,23 – þ/– þ þ þ/– – þ/– – – þSC12,20–25 – þ/– þ/– þ – – þ/– – – þ
MRCC, cutaneous metastasis of renal cell carcinoma; CX, xanthoma; XA, xanthelasma; XG, xanthogranuloma; BCN, balloon cell nevus; CCH, clear cellhidradenoma; SA, sebaceous adenoma; SE, sebaceous epithelioma; SC, sebaceous carcinoma; nd, not determined.*The labeling in cutaneous metastases of renal cell carcinoma (MRCC) has not been studied with these antibodies; however, some positivity with EMAand AE1/AE3 would be expected and negativity with CEA, CD68, S-100, and HMB-45 would be expected based on the immunohistochemical resultsseen in primary clear cell RCC.
Perna et al.
384

3. Avery AK, Beckstead J, Renshaw AA, Corless CL. Use of
antibodies to RCC and CD10 in the differential diagnosis of
renal neoplasms. Am J Surg Pathol 2000; 24: 203.
4. Brownstein MH, Helwig EB. Spread of tumors to the skin.
Arch Dermatol 1973; 107: 80.
5. Brownstein MH, Helwig EB. Patterns of cutaneous metastasis.
Arch Dermatol 1972; 105: 862.
6. Brownstein MH, Helwig EB. Metastatic tumors of the skin.
Cancer 1972; 29: 1298.
7. Koga S, Tsuda S, Nishikido M, Matsua F, Saito Y, Kantake H.
Renal cell carcinoma metastatic to the skin. Anticancer Res
2000; 20: 1939.
8. Pan CC, Chen OCH, Ho DMT. The diagnostic utility of
MOC31, BerEP4, RCC marker, and CD10 in the classification
of renal cell carcinoma and renal oncocytoma: an immunohis-
tochemical analysis of 328 cases. Histopathology 2004; 45: 452.
9. Perna AG, Smith MJ, Krishnan B, Reed JA. CD10 is expressed
in cutaneous clear cell lesions of different histogenesis. J Cutan
Pathol 2005; 32: 348.
10. Suster S. Clear cell tumors of the skin. Semin Diagn Pathol
1996; 13: 40.
11. Busam KJ, Rosai J, Iversen K, Jungbluth AA.
Xanthogranulomas with inconspicuous foam cells and giant
cells mimicking malignant melanoma. Am J Surg Pathol
2000; 24: 864.
12. Ostler DA, Perna AG, Ivan D, et al. Cytokeratin 7 and 20
expression in clear cell lesions of the skin. Mod Pathol 2006; 19
(Suppl. 1): 86A.
13. Breier F, Zelger B, Reiter H, Gschnait F, Zelger BW. Papular
xanthoma: a clinicopathological study of 10 cases. J Cutan
Pathol 2002; 29: 200.
14. Tomaszewski MM, Lupton GP. Unusual expression of S-100
protein in histiocytic neoplasms. J Cutan Pathol 1998; 25: 129.
15. Dehner LP. Juvenile xanthogranulomas in the first two decades
of life: a clinicopathologic study of 174 cases with cutaneous and
extracutaneous manifestations. Am J Surg Pathol 2003; 27: 579.
16. Janssen D, Harms D. Juvenile xanthogranuloma in childhood
and adolescence: a clinicopathologic study of 129 patients
from the kiel pediatric tumor registry. Am J Surg Pathol
2005; 29: 21.
17. Satoh T, Katsumata M, Tokura Y, Iwatsuki K, Takigawa M.
Clear cell hidradenoma with whorl formation of squamoid
cells: immunohistochemical and electron microscopic studies.
J Am Acad Dermatol 1989; 21: 271.
18. Grossniklaus HE, Knight SH. Eccrine acrospiroma (clear cell
hidradenoma) of the eyelid. Immunohistochemical and ultra-
structural features. Ophthalmology 1991; 98: 347.
19. Biernat W, Kordek R, Wozniak L. Phenotypic heterogeneity of
nodular hidradenoma. Immunohistochemical analysis with
emphasis on cytokeratin expression. Am J Dermatopathol
1996; 18: 592.
20. Bayer-Garner IB, Givens V, Smoller B. Immunohistochemical
staining for androgen receptors: a sensitive marker of sebaceous
differentiation. Am J Dermatopathol 1999; 21: 426.
21. Johnson JS, Lee JA, Cotton DW, Lee WR, Parsons MA.
Dimorphic immunohistochemical staining in ocular sebaceous
neoplasms: a useful diagnostic aid. Eye 1999; 13: 104.
22. Metze D, Soyer HP, Zelger B, et al. Expression of a glycopro-
tein of the carcinoembryonic antigen family in normal and
neoplastic sebaceous glands. Limited role of carcinoembryonic
antigen as a sweat gland marker. J Am Acad Dermatol 1996;
34: 735.
23. Bieniek R, Lazar AJF, Lyle S. Keratin 15 stem cell marker and
other immunohistochemical characteristics of sebaceous neo-
plasms. Mod Pathol 2006; 19 (Suppl. 1): 77A.
24. Ansai S, Hashimoto H, Aoki T, Hozumi Y, Aso K. A histo-
chemical and immunohistochemical study of extra-ocular
sebaceous carcinoma. Histopathology 1993; 22: 127.
25. Ansai S, Katagata Y, Yoshikawa K, et al. An immunohisto-
chemical study of sebaceous carcinoma with anti-keratin
monoclonal antibodies: comparison with other skin cancers.
J Dermatol 1994; 21: 553.
Use of RCC-Ma to diagnose metastatic RCC to skin
385