Embed Size (px)
DESCRIPTION
Renal artery stenosis
Citation preview

Diagnosis of Renovascular Hypertension
Cholatip Pongskul


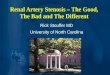
Characteristics of atherosclerotic and fibromuscular dysplasia
Variable Atherosclerotic Fibromuscular dysplasia
Age at presentation Older(>50 yr) Usually young(<40 yr)
Sex Either Usually female
Lesion location Ostial, proximal, middle Middle or distal
BP response to revascularization
Unclear Normotensive in most patients

Atherosclerotic Fibromuscular dysplasia
Elderly>50 Younger<40,femaleResponse to correction

Pathophysiology of renal artery stenosis

Who should be tested for renovascular hypertension?
• 45-year-old man, uremia, BP 160/90 mmHg, proteinuria, kidney 8.5, 8 cm
• 70-year-old man, smoker, hypertension, dyslipidemia, presented with pulmonary edema, Cr=1.4 mg/dl
• 60-year-old woman with pulmonary edema, BP 180/100 mmHg, Cr=1.2 mg/dl

Who Should be tested

What testShould be performed

How
to interpret the result

Who
• Onset of severe hypertension after 55• Unexplained deterioration of kidney function
– Rising > 50%, 1 week, ACEI• Severe hypertension in diffuse atherosclerosis• Severe hypertension with asymmetry kidney >
1.5 cm• Severe hypertension with flash pulmonary
edema, refractory CHF• Systolic-diastolic bruit at one side

Test or not test?
• Medication is effective in renovascular hypertension
• Who will benefit from correction?
• Testing associated with potential risk• Correction procedure associated with
morbidity/mortality

Test should be performed in patient with high likelihood of benefit
from procedure

High likelihood of benefit from procedure
• Short duration• Failure of medical Rx, in patient with high
likelihood of renovascular hypertension• Intolerance to optimal medical therapy• Progressive renal failure• Suspected fibromuscular dysplasia• Recurrent flash pulmonary edema

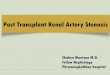
Gold Renal angiography
More than 50% stenosis

Other tests• Duplex sonography• CT angiogram• MRA

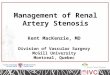
Duplex doppler sonography
Functional and anatomical
Peak200 cm/sec

Peak systolic velocitySensitivity 85, specificity 92%Positive predictive value 84%
Positive test: more informative than negative test

Resistive index(1-end diastolic velocity)/PSV
Predict outcome after revascularization

Limitation
Time consuming operator dependent

Obese patient

CT angiography

Excellent sensitivity and specificityLimitation in distal stenosis (FMD)

Magnetic resonance angiography

MRA• Almost 100% sensitivity!• Nephrogenic systemic
fibrosis?

Functional assessment

Captopril renography: less commonly usedLittle predictive value
Not for screening test!

Selecting a diagnostic test
• Local availability• Expertise with each technique• Renal insufficiency?

Who
New onset HT>55 yrDeterioration GFRAsymmetry kidneyFlash pulmonary edema
Test
Failure medicalFMD?Progressive renalfailure
Benefit fromcorrection