Embed Size (px)
Citation preview

J
O
Rp
SRa
b
a
ARR1AA
KIVAPO
1
olaTt
SoS
MT
(c
2h
ARTICLE IN PRESSG ModelOMSMP-248; No. of Pages 5
Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology xxx (2014) xxx–xxx
Contents lists available at ScienceDirect
Journal of Oral and Maxillofacial Surgery,Medicine, and Pathology
j o ur nal ho me pa ge: www.elsev ier .com/ locate / jomsmp
riginal Research
emoval of maxillary teeth with buccal 4% Articaine without usingalatal anesthesia—A comparative double blind study
aravanan Kandasamy (MDS, MOMS RCPS (Glasgow))a,∗, Rethish Elangovan (MDS)b,eena Rachel John (MDS)b, Nantha Kumar Cb
Department of Oral & Maxillofacial Surgery, Vinayaka Mission’s Sankaracharya Dental College & Hospital, Salem 636308, Tamilnadu, IndiaSalem Soudeswari Arts College, P M P Nagar, Maniyanur, Salem 636010, Tamilnadu, India
r t i c l e i n f o
rticle history:eceived 11 October 2013eceived in revised form8 November 2013ccepted 6 December 2013vailable online xxx
eywords:nfiltrationestibular diffusionrticainealatal injectionral surgery
a b s t r a c t
Objective: The aim of the present study was to evaluate and compare the property of vestibular to palatalbony diffusion of Articaine with that of lignocaine in the maxilla for the removal of maxillary teeth withoutthe need for palatal injection.Materials and methods: The study group (A) had 1.7 ml of 4% Articaine hydrochloride with adrenaline1:100,000. The Articaine anesthetic agent was injected into the buccal vestibule by simple infiltrationmethod along the long axis of the corresponding tooth. The patients were allowed to wait for 10 min. Thecontrol group (L) had 1.7 ml of lignocaine 2% with adrenaline 1:80,000. The parameters like pain duringinjection, objective symptom of numbness, pain during flap elevation, and pain during tooth extractionand the frequency of reanesthesia required were evaluated and marked by a different person. The painwas evaluated using the 0–100 mm VAS scale with descriptors on each end from NO PAIN to ABSOLUTEPAIN.Statistical analysis used: Chi square test was used.Results: Among the study group (A), 98.28% (114) patients had objective symptom of numbness on probingshowing statistically significant p value (0.001). The complete control group (L) necessitating reanesthe-
sia. 106 (91.38%) patients of the study group (A) required no reanesthesia showing statistically significantresult (p value: 0.001).Conclusion: The results of this study indicate that Articaine hydrochloride 4% with epinephrine 1:100,000produce more effective buccal vestibule–palatal anesthesia (91.38%) than the 2% lignocaine with 1:80,000.MS, A
© 2013 Asian AO. Introduction
Pain associated with administration of local anesthesia prior toral surgical procedures has been researched since the advent ofocal anesthetic agents. Among the different techniques of local
Please cite this article in press as: Kandasamy S, et al. Removal of
anesthesia—A comparative double blind study. J Oral Maxillofac Surg M
nesthetic administration, palatal anesthetia are the most painful.he reason being the adherence of the palatal mucoperiosteum tohe bone, hence minimal space for deposition of the local anesthetic
� AsianAOMS: Asian Association of Oral and Maxillofacial Surgeons; ASOMP: Asianociety of Oral and Maxillofacial Pathology; JSOP: Japanese Society of Oral Pathol-gy; JSOMS: Japanese Society of Oral and Maxillofacial Surgeons; JSOM: Japaneseociety of Oral Medicine; JAMI: Japanese Academy of Maxillofacial Implants.∗ Corresponding author at: Department of Oral & Maxillofacial Surgery, Vinayakaission’s Sankaracharya Dental College & Hospital, Salem 636308, Tamilnadu, India.
el.: +91 94430 94802.E-mail addresses: saran [email protected] (S. Kandasamy), [email protected]
R. Elangovan), [email protected] (R.R. John), [email protected] (N.K. C).
212-5558/$ – see front matter © 2013 Asian AOMS, ASOMP, JSOP, JSOMS, JSOM, and JAMttp://dx.doi.org/10.1016/j.ajoms.2013.12.001
SOMP, JSOP, JSOMS, JSOM, and JAMI. Published by Elsevier Ltd. All rightsreserved.�
solution, leading to pain due to separation of the mucoperiosteumfrom bone by the deposited solution [1]. A number of techniqueshave been advocated to reduce the pain of intra oral palatal injec-tions, which includes topical anesthetic application, topical coolingof palate, computerized injection systems, pressure administration,eutectic mixture of local anesthetics (EMLA), and transcutaneouselectronic nerve stimulation (TENS). Although these adjunctivetechniques have been described to reduce the pain during thepalatal injection, they have not yet gained universal acceptance[2].
Maxillary tooth removal without palatal anesthesia has been thetopic of much research. Among the local anesthetics, Lidocaine isthe “gold standard” drug. Articaine is gaining popularly as an effi-cient local anesthetic due to its safety and potency [3]. The longduration of action of Articaine and its superior diffusion through
maxillary teeth with buccal 4% Articaine without using palataled Pathol (2014), http://dx.doi.org/10.1016/j.ajoms.2013.12.001
bony tissue makes Articaine superior to other local anesthetics,hence maxillary buccal infiltration with Articaine provided ade-quate palatal soft tissue anesthesia, obviating the need for a painfulpalatal injection [4,5].
I. Published by Elsevier Ltd. All rights reserved.�

ING ModelJ
2 ial Sur
ttt
2
t
2
bS(i
2
sofpercHmowrtfamt
2
ftv2ma
2
hate
ld1bnod
the age group of 15–65 yrs and the mean age was 41.18 yrs (Table 1and Fig. 1).
Among the study group (A), 98.28% (114) patients had objectivesymptom of numbness on (Table 2) probing showing statistically
Table 1Male and female comparison between the 2 groups.
Drug Sex Chi square p
Male Female
N % N %
ARTICLEOMSMP-248; No. of Pages 5
S. Kandasamy et al. / Journal of Oral and Maxillofac
So the aim of this present study was to evaluate and comparehe buccal vestibular to palatal bony diffusion of 4% Articaine withhat of 2% lignocaine in the maxilla during the removal of maxillaryeeth without the need for palatal injection.
. Materials and methods
The report of the methodology used in the study conforms tohe Consolidated Standards of Reporting Trials statement.
.1. Trial design
This was a single-centered, balanced randomization, dou-le blinded, parallel-group study conducted in the Maxillofacialurgery Department, Vinayaka Missions University Hospital, SalemTamil Nadu, India). No changes to the trial design were made dur-ng the study.
.2. Participants
The potential study participants were examined by a singleurgeon at recruitment who was not involved in the follow-upf research subjects. Ethical approval for this study was obtainedrom the ethics committee at Vinayaka Missions University Hos-ital, Salem (Tamil Nadu, India). A member of the research teamxplained the study protocol, and written informed consent wasecorded from all eligible subjects. The study was performed inompliance with Good Clinical Practice and the Declaration ofelsinki (most recent revision, 2000). Institutional ethical com-ittee approval and informed consent from all volunteers was
btained. The patients who were included in the study were thoseith maxillary teeth that were grossly destroyed by caries, infected
oot stumps, impacted maxillary 3rd molars or therapeutic extrac-ion of premolars. The number of teeth requiring removal variedrom one to three. The exclusion criteria were patients who werellergic to local anesthetics, those with teeth showing even slightobility, pregnant women and also the patients with severe sys-
emic diseases contraindicating extractions.
.3. Study setting
A total of 227 patients (102 male, 125 female) of age rangingrom 15 to 65, who underwent extractions of maxillary teeth inhe Dept. of Oral & Maxillofacial Surgery, Vinayaka Missions Uni-ersity, Salem, Tamil Nadu, India, from January 2012 to February012 were included in the study. The Maxillofacial Surgery Depart-ent receives patients from over a wide geographic area within
nd around the city of Salem.
.4. Interventions
The study group (A) were administered 1.7 ml of 4% Articaineydrochloride with adrenaline 1:100,000. The Articaine anestheticgent was injected into the buccal vestibule by simple infiltra-ion method along the long axis of the corresponding tooth to bextracted.
For cases involving multiple (maximum three) extractions, theocal anesthetic was infiltrated into the buccal vestibule of the mid-le tooth. The patients were allowed to wait for 10 min. After the0 min waiting period, the effect of local anesthetic was checked
Please cite this article in press as: Kandasamy S, et al. Removal of
anesthesia—A comparative double blind study. J Oral Maxillofac Surg M
oth subjectively and objectively. The objective symptom of numb-ess was tested using a sharp probe on the palatal gingival aspectf the corresponding tooth to be extracted. The extraction proce-ure was performed by the same surgeon who administered the
PRESSgery, Medicine, and Pathology xxx (2014) xxx–xxx
local anesthetic. The control group (L) were administered 1.7 ml oflignocaine 2% with adrenaline 1:80,000 in a similar manner.
2.5. Outcomes
If the patient complained of pain during flap evaluation, then thelocal anesthetic solution was given on the palatal side. The param-eters like pain during injection, objective symptom of numbness,pain during flap elevation, and pain during tooth extraction and thefrequency of reanesthesia required were evaluated and marked bya different person. The pain was evaluated using the 0–100 mm VASscale ranging from 0 for NO PAIN to 100 for ABSOLUTE PAIN.
2.6. Sample size
The study group comprised of a total of 116 individuals of which55 were males and 61 were females. The control group had a totalof 111 individuals with 47 males and 64 females. The numberof patients requiring multiple extractions was 30. The number ofpatients requiring single tooth extraction was 197.
2.7. Randomization
The participants were allocated into the study or the controlgroups randomly using lot method. The envelopes containing (A)and (L) were sealed.
2.8. Blinding
The surgeons and the participants were blinded to their allo-cation to the Articaine (A) study or the lignocaine (L) controlgroup. The observers performing the assessment of the objectivesymptoms were blind to the surgical outcome. Furthermore, theinvestigators who carried out the assessment were blind to theallocation of the patient to the (A) or (L) group. The study is thus adouble blinded one.
2.9. Statistical methods
The collected data were statistically analyzed using SPSS 11.5for Windows (IBM SPSS, Chicago, IL). Descriptive statistics wereused to summarize all measurements. p values less than .05 wereconsidered statistically significant.
3. Results
The number of patients involved in the study group (A) was 116,of which 55 were males and 61 were females. The patients werewithin the age ranging from 15 to 65 yrs with a mean age groupbeing 41.08 yrs. The number of patients involved in the controlgroup (L) was 111, of which 47 were males, 64 were females, within
maxillary teeth with buccal 4% Articaine without using palataled Pathol (2014), http://dx.doi.org/10.1016/j.ajoms.2013.12.001
Study group (A) 55 47.41 61 52.590.59 0.443Control group (L) 47 42.34 64 57.66
Total 102 44.93 125 55.07

ARTICLE IN PRESSG ModelJOMSMP-248; No. of Pages 5
S. Kandasamy et al. / Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology xxx (2014) xxx–xxx 3
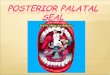
no of subjects reported in the study
period = 1876
No of subjects for maxillary teeth removal = 97 3
No of su bjects excluded from the
study as per exclusion criter ia = 61 5
No of subjects referred for further inves�ga �ons = 11 3
No of subjects includ ed in the stud y as per criter ia = 24 5
No of subject s no t interested in
par� cipa� ng the stud y = 18
No of su bjects too k part in the study =
227
No of subj ects in the stud y group (A) = 11 6
no of subj ects involve d in the
contr ol group = 11 1
No of subjects for mandibular tee th =
903
Fig. 1. Diagram showing patient allocation.
Table 2Comparison of objective symptom between the study group and control group.
Drug Objective symptoms Total Chi square p
Yes No N
N % N %
Study group (A) 114 98.28 2 1.72 116219.14 <0.001**
Control group (L) 111 100.00 111
sp
flt
dtpter(
TC
Total 114 50.22 113
** p value is significant.
ignificant p value (0.001). In the control group (L), 100% com-lained of pain on probing.
Only 10 patients in the study group (A), i.e. 8.62% had pain duringap elevation requiring reanesthesia (Table 3). On the other hand,he complete control group (L) needed reanesthesia (Table 4).
Those patients who had marked pain during flap elevation anduring extraction procedure who required reanesthesia were givenhe appropriate anesthetic on the palatal side and the extractionrocedure was completed. Meticulous care was taken to see that
Please cite this article in press as: Kandasamy S, et al. Removal of
anesthesia—A comparative double blind study. J Oral Maxillofac Surg M
he patients included in this study underwent smooth and painlessxtraction procedure.106 (91.38%) patients of the study group (A)equired no reanesthesia which was statistically significant resultp value: 0.001).
able 3omparison of pain during flap elevation between the study and control groups.
Drug Pain during flap elevation
Yes No
N % N
Study group (A) 10 8.62 106
Control group (L) 110 99.10 1
Total 120 52.86 107
** p value is significant.
49.78 227
4. Discussion
Pain is a protective mechanism of the body to tissue injurycaused by different stimulations [6]. Dental pain is usually acuteinflammatory in nature and it compels the patient to seek profes-sional help [6]. Reduction of pain has been the subject of continuousresearch in the field of oral and maxillofacial surgery. Intra oper-ative and postoperative pain varying in intensity and durationmay affect a patient during an oral surgical procedure. Therefore,
maxillary teeth with buccal 4% Articaine without using palataled Pathol (2014), http://dx.doi.org/10.1016/j.ajoms.2013.12.001
a method to decrease or eliminate pain has its usefulness justi-fied. The number of local anesthetic agents available has improvedthe interest in research on dental pain control. The concept oflocal anesthetic action is based on hindering the generation and
Total Chi square p
N
%
91.38 116186.35 <0.001**
0.90 111
47.14 227

ARTICLE IN PRESSG ModelJOMSMP-248; No. of Pages 5
4 S. Kandasamy et al. / Journal of Oral and Maxillofacial Surgery, Medicine, and Pathology xxx (2014) xxx–xxx
Table 4Comparison of reanesthesia requirement between the study and control groups.
Drug Reanesthesia Total Chi square p
Yes No N
N % N %
Study group (A) 10 8.62 106 91.38 116190.29 <0.001**
Control group (L) 111 100.00 111
Total 121 53.30 106 46.70 227
cdtcs
lbliettemlost
maupipvsato
lavauto
c1f(ssw
cwect
** p value is significant.
onduction of nerve impulses. Thus, the impulse is aborted, hin-ered from reaching the brain and is not interpreted as pain byhe patient. The availability of number of local anesthetic agents toontrol intra operative and post-operative pain has led to severaltudies comparing the efficacy of one over the other [7].
Till date, lignocaine continues to be considered the standardocal anesthetic drug of choice that has been consistently usedy many dentists. For the extraction of maxillary teeth, it is abso-
utely necessary that palatal infiltration or block be given. Palatalnjections are very painful. Many patients felt pain during injectionven after the application of surface anesthesia palatally prior tohe injection. The palatal mucosal binding to its underlying perios-eum and its abundant nerve supply makes injections to the palatextremely painful. The pain can also be caused by the displace-ent of mucoperiosteum. Articaine is emerging as an outstanding
ocal anesthetic indicated for dental procedures and control of post-perative pain [8]. When we used Articaine hydrochloride in ourtudy, the patients never complained of severe pain. Only 8.62% ofhe patients complained of pain, which required reanesthesia.
The administration of local anesthetics into skin or oral mucousembrane is frequently uncomfortable [2]. Many factors are
ttributed to this discomfort, including the speed of injection, vol-me of solution, density of tissue and psychologic factors. The acidicH of the anesthetic solutions plays a significant role in provok-
ng discomfort during local anesthetic administration. The pH oflain local anesthetic solution like lignocaine is approximately 5.5;asoconstrictor containing solution is about 4.5. The addition ofubstances such as sodium bicarbonate or carbon dioxide to thenesthetic that alkalinize the solution makes the drug administra-ion more comfortable. Also at a higher pH, anesthetic have a rapidnset of action and greater potency [9].
The chemical structure of Articaine is different from that of otherocal anesthetics due to the substitution of the aromatic ring with
thiophenic ring, and the presence of an additional ester ring, pro-ides Articaine with increased liposolubility and intrinsic potency,s well as greater plasma protein binding versus other commonlysed local anesthetic [10]. These differential characteristics are inurn clinically reflected by a shorter latency and increased durationf anesthesia, as well as superior bony tissue diffusion.
In 1993, Vähätalo et al. [11] conducted a double blind study toompare the anesthetic properties of Articaine hydrochloride with:200,000 epinephrine and Lidocaine with 1:80,000 epinephrineor maxillary infiltration anesthesia. The latency time was 187 s±66) for Articaine and 201 s (±88) for lignocaine and there were notatistically significant difference in onset and duration of anesthe-ia between Articaine with epinephrine 1:200,000 and lignocaineith epinephrine 1:80,000.
In 2001, Malamed et al. [12] compared the safety and effi-acy of 4% Articaine with epinephrine 1:100,000 with 2% Lidocaine
Please cite this article in press as: Kandasamy S, et al. Removal of
anesthesia—A comparative double blind study. J Oral Maxillofac Surg M
ith epinephrine 1:100,000 and found that 4% Articaine withpinephrine 1:100,000 was well tolerated and also provided clini-ally effective pain relief during most dental procedures and had aime of onset and duration of anesthesia appropriate for clinical use
and comparable to those observed for other commercially availablelocal anesthetics.
Fan et al. in 2009 [4], compared Articaine with lignocaine inmaxillary extractions in 71 patients and concluded that the routineuse of a palatal injection for the removal of permanent maxillaryteeth may not be required when Articaine hydrochloride is used asthe local anesthetic. The time limit was 5 min for the initiation ofthe procedure.
In 2009, Lima-Júnior et al. [5] evaluated the vestibularpalatal diffusion of 4% Articaine with epinephrine 1:100,000 and1:200,000, in impacted maxillary third molar extractions, with-out palatal injection. They concluded that Articaine 4% withepinephrine 1:100,000 produced more effective buccal vestibule-palatal anesthesia than 1:200,000 solution, when an interval of10 min is allowed between the administration of the anesthetic andthe initiation of the surgery.
Katyal [13] in 2010 did meta-analysis on the systematic reviewto compare the efficacy and safety of Articaine with lignocainein maxillary and mandibular infiltrations and block anesthesiain patients presenting for routine dental treatments and con-cluded that Articaine is more effective than lignocaine in providinganesthetic success in the first molar region for routine dental proce-dures, although they did not recommend its use in children under4 years of age, since no data exists to support such usage.
Sreekumar and Bhargava [14] in 2011 conducted a study tocompare the onset and duration of action of soft tissue and pul-pal anesthesia with three volumes 0.6 ml, 0.9 ml and 1.2 ml of4% Articaine with 1:100,000 epinephrine in maxillary anesthesiaand found that maxillary infiltration anesthesia with Articaine andepinephrine had a faster onset, a greater success rate and a longerduration with volume of 1.7 ml.
The duration of the effect of an anesthetic is proportional to itsdegree of protein binding [12]. However, the duration of the effectof the local anesthetic is also dependent on the injection site orconcentration of vasoconstrictor present in the anesthetic solution,among other factors. Articaine presents one of the greatest proteinbinding percentages of all amide local anesthetics, comparable onlyto ultra-long action substances such as bupivacaine, ropivacaineand etidocaine.
A number of techniques may be used to reduce the painof intra oral injections, including topical anesthetic application,topical cooling of palate, computerized injection systems, pres-sure administration, eutectic mixture of local anesthetics (EMLA),and transcutaneous electronic nerve stimulation (TENS). Althoughthese numbers of adjunctive techniques have been described toreduce discomfort or pain, they are expensive, complex, and timeconsuming procedures and patients still experience discomfortduring palatal injection [2].
In our study, only 10 patients (8.62%) in the study group (A) had
maxillary teeth with buccal 4% Articaine without using palataled Pathol (2014), http://dx.doi.org/10.1016/j.ajoms.2013.12.001
pain during flap elevation out of 116 patients, which was statis-tically significant p value (0.001). On the other hand, the controlgroup (L) had 99.1% patients who complained of pain during flapelevation. One patient in the control group (L) had no pain during

ING ModelJ
ial Sur
tpg8Ai
5
4v1adispw
F
E
C
A
s
[
[
[
[
[14] Sreekumar K, Bhargava D. Comparison of onset and duration of actionof soft tissue and pulpal anaesthesia with three volumes of 4% arti-
ARTICLEOMSMP-248; No. of Pages 5
S. Kandasamy et al. / Journal of Oral and Maxillofac
he flap elevation but later complained of pain during the extractionrocedure necessitating reanesthesia. Thus the complete controlroup (L) had 100% reanesthesia whereas in the study group, only.62% (10 out of 116) needed reanesthesia. This result showed thatrticaine is superior to lignocaine as observed in the previous stud-
es [4,5,12,13].
. Conclusion
The results of this study indicate that Articaine hydrochloride% with epinephrine 1:100,000 produced more effective buccalestibule–palatal anesthesia (91.38%) than the 2% lignocaine with:80,000, when an interval of 10 min was allowed between thedministration of the anesthetic and the initiation of the proce-ure. From our study, we conclude that Articaine 4% is superior
n comparison to 2% lignocaine and possess the characteristics ofuperior bony diffusion and there is no absolute necessity to usealatal infiltration for the removal of maxillary teeth in accordanceith previous studies.
unding
None.
thical approval
Approval obtained.
ompeting interest
None declared.
Please cite this article in press as: Kandasamy S, et al. Removal of
anesthesia—A comparative double blind study. J Oral Maxillofac Surg M
cknowledgement
The authors would like to thank the principal of Vinayaka Mis-ions Sankaracharya Dental College, Salem for their support.
PRESSgery, Medicine, and Pathology xxx (2014) xxx–xxx 5
References
[1] McArdle BF. Painless palatal anesthesia. J Am Dent Assoc 1997;128(5):647.
[2] Uckan S, Dayangac E, Araz K. Is permanent maxillary tooth removal with-out palatal injection possible? Oral Surg Oral Med Oral Pathol Oral RadiolEndod 2006;102(December (6)):733–5. Epub 2006 March 20. Erratum in: OralSurg Oral Med Oral Pathol Oral Radiol Endod 2007;103(April (4)):580. PMID:17138173.
[3] Malamed SF, Gagnon S, Leblanc D. Efficacy of articaine: a new amide localanesthetic. J Am Dent Assoc 2000;131:635–42.
[4] Fan S, Chen WL, Yang ZH, Huang ZQ. Comparison of the efficiencies ofpermanent maxillary tooth removal performed with single buccal infiltra-tion versus routine buccal and palatal injection. Oral Surg Oral Med OralPathol Oral Radiol Endod 2009;107(March (3)):359–63. Epub 2008 November8.
[5] Lima-Júnior JL, Dias-Ribeiro E, de Araújo TN, Ferreira-Rocha J, Honfi-Junior ES,Sarmento CFM, et al. Evaluation of the buccal vestibule-palatal diffusion of 4%articaine hydrochloride in impacted maxillary third molar extractions. MedOral Patol Oral Cir Bucal 2009;14:E129–32.
[6] Hunter JP, Simmonds MJ. Pain: putting the whole person at the centre. Physio-ther Can 2010;62:1–8.
[7] Silva LC, Santos TD, Santos JA, Maia MC, Mendonc a CG. Articaine versus lido-caine for third molar surgery: a randomized clinical study. Med Oral Patol OralCir Bucal 2012;17(January (1)):e140–5.
[8] Isen DA. Articaine: pharmacology and clinical use of a recently approved localanesthetic. Dent Today 2000;19:72–7.
[9] Reed KL, Malamed SF, Fonner AM. Local anesthesia: Part 2.Technical considerations. Anesth Prog 2012;59(Fall (3)):127–36,http://dx.doi.org/10.2344/0003-3006-59.3.127, quiz 137. Review. PMID:23050753.
10] Hawkins JM, Moore PA. Local anaesthesia: advances in agents and techniques.Dent Clin North Am 2002;46:719–32.
11] Vähätalo K, Antila H, Lehtinen R. Articaine and lidocaine for maxillary infiltra-tion anaesthesia. Anesth Prog 1993;40:114–6.
12] Malamed SF, Gagnon S, Leblanc D. Articaine hydrochloride: a study of the safetyof a new amide local anesthetic. J Am Dent Assoc 2001;132:177–85.
13] Katyal V. The efficacy and safety of articaine versus lignocaine in dentaltreatments: a meta-analysis. J Dent 2009;38(April (4)):307–17. Epub 2010December 16.
maxillary teeth with buccal 4% Articaine without using palataled Pathol (2014), http://dx.doi.org/10.1016/j.ajoms.2013.12.001
caine with 1:100,000 epinephrine in maxillary infiltration anaesthesia.Oral Maxillofac Surg 2011;15(December (4)):195–9. Epub 2011 May18.